

Abstract
Introduction:
Stroke-related smartphone applications (apps) present enormous potential for stroke management as apps become increasingly prevalent in China. However, there is no comprehensive study reported about the currents status of stroke-related apps available to adopt in Chinese app market. The aim of this study is to assess the current status of stroke-related apps available to adopt in China.
Materials and Methods:
Using Stroke-related keywords written in either Chinese or English, the top 6 most prevalent apps online stores in China were searched from June to August 2018, including android market, 360 app market, wan dou jia, baidu mobile app, ying yong bao, apple app store. The basic features of selected apps were analyzed based on operating system, cost, target people, engagement, online interaction, release date, size, popularity, and usefulness. The information accountability of selected apps was evaluated with the Silberg scale. The functionality of selected apps targeting stroke patients at home were reviewed by researchers.
Results:
Our study showed that the downloads of stroke-related apps from android platform and the engagement of health professionals in apps development were critically insufficient. And most apps didn’t offer a platform to facilitate online interaction with health professional. The information accountability of apps also presented a huge room for improvement. The average Silberg score of 127 apps was 3.5 (out of 9) with most apps not disclosing sponsorship, authors’ affiliations, credentials, and sources or references of information. Few apps were modified in the past months. What's more, although the apps targeting stroke patients at home have covered 9 functionalities, most apps had only a simple functionality.
Conclusion:
This study identified areas for improvement concerning information accountability of stroke-related apps available for adoption in China and reviewed functionality of apps targeting stroke patients at home. The findings might guide the development for stroke-related apps in China in the future.
Keywords: apps, China, information accountability, Silberg scale, stroke
1. Introduction
By the end of 2015, the total number of mobile phone users in China reached 1.3 billion.[1] And among all mobile phone users, about 668 million Chinese were smartphone users by of the first quarter of 2017.[2] A global survey also showed that the rate of smartphone penetration in China has grown exponentially and reached 58% in 2015, and 71% in 2017.[3,4]
The widespread usage of smartphone has sparked a boom in apps development. In spite of being known since 2008, numerous apps have been released on the android play store or apple app store.[5] In China, the number of apps on the third-party app stores and apple store (China) also has exceeded 2.48 and 1.78 million, respectively, by the end of August 2018.[6] Meanwhile, health-related apps are booming. By the end of 2017, the number of health-related apps worldwide has over 0.325 million, up about 0.078 million from 2016.[7] The proliferation of health-related apps has changed the way of seeking health-related information, suggestions, and instruction for people. For example, 42% of American smartphone owners used at least one fitness app, and 18% of such users used a health/wellness coaching service in 2016.[8] Additionally, 53.7% of Chinese inpatients with chronic diseases were willing to use a physical activity app.[9] The huge user demands, positively policy supports, and widely available network connections features for smartphone apps have also prompted high engagement for developer. According to the research2 guidance,[7] almost 84,000 developers have been involved in developing health-related apps by the end of 2017, up 45% from 2016. With health-related apps becoming commonly used, the opportunities for management of health-related diseases will grow, in particular chronic diseases. These changes bring potential clinical advantages, but also expose new risks.[10]
On one hand, the widespread development and usage for apps offer new pathways to manage chronic diseases, especially stroke. It is reported that there were almost 25.7 million stroke survivors worldwide.[11] In the United States, on average, someone has a stroke every 40 seconds.[12] In China, the incident and mortality rates of stroke have declined,[13] but the absolute number of people affected by stroke is still increasing significantly.[14] By the end of December 2016, Chinese stroke survivors were almost 13 million.[15] In addition, Słomka et al[16] reported that hemostatic abnormalities is a pivotal event in the pathophysiology of ischemic stroke. However, some risk factors of stroke, such as hypertension, heart disease, diabetes, obesity and insulin resistance, smoking, alcohol abuse, dyslipidemia, etc, could be intervened by apps for a better outcome. Evidences showed that the stroke-related apps shortened the admission time, improved rehabilitation outcome, promoted long-term care quality, and the satisfaction of patients.[17–19] For example, “Care for stroke” app could provide a better education than face-to-face education for stroke patients with physical disabilities.[20] On the other hand, currently the development of health-related apps isn’t in parallel with the relevant regulation and standardization for information quality of apps. A systematic review showed that most Chinese health-related apps lacked regulatory oversight, and content quality was uneven.[21] Kao and Liebovitz[22] also found that one of most common barriers for which consumer health apps provided low-cost, around-the-clock access to high-quality health information for end users on a global scale was limited evidence-based literature. More seriously, most apps developed based on industry promotion and economic benefits were not consistent with consumer needs and professionals requirements, and thus the efficacy, safety, and scientific of apps were worrisome. For instance, Dubey et al[23] found 52.7% stroke-related apps were developed by non-health care agencies. Huckvale et al[10] showed that 66% of accredited health and wellness apps sending identifying information over the Internet did not use encryption and 20% did not have a privacy policy. Therefore, concerns have arisen that the accountability of information offered by health-related apps may not be very well.
Recently, some researchers have presented the information accountability of apps targeting various health problems, such as chronic kidney disease, smoking cessation.[24,25] Lambert et al[24] and Cheng et al[25] also assessed the information accountability of cardiovascular disease apps applied in the Chinese market. However, there is no comprehensive study reported about information accountability of stroke-related apps available to adopt in China. Therefore, further assessing the information accountability of stroke-related apps available for adoption in China is of prime importance for developing a safe app for stroke management.
What's more, apps have been widely served to chronic disease management for patients in the community, such as people with Parkinson disease or cancer.[27,28] The stroke-related apps are also no exception. For example, apps targeting stroke patients at home could promote communication between user and health professionals, regardless of their space or time.[27,28] However, there is no studies done to identify the functionality of apps targeting stroke patients at home in Chinese app market, although a study reviewed the stroke-related apps extracted from play store.[23] It's therefore essential for researchers to explore the current functionality of apps targeting stroke patients at home, which will influence to design an optimal and practical app as a novel method to replace face-to-face follow-up for patients with stroke at home.
In this paper, the overarching aim of our study was to assess the current status of stroke-related apps available to adopt in China. The key objectives were to identify common characteristics of stroke-related apps; assess information accountability of stroke-related apps; review current functionality of apps targeting stroke patients at home.
2. Materials and methods
2.1. Selection of apps
Using the following terms as the search keywords: “stroke,” “apoplexy,” “cerebral hemorrhage,” “cerebral infarction,” “hemiplegia,” “cerebral vascular accident,” “cerebral vascular disease,” “CVA” written either in English or Chinese. Apps were searched on the leading platforms from the top 6 most widely used apps stores in China from April to September 2018. A cumulative total of 1846 apps were yielded initially by search. After reviewing the information of the retrieved apps, 1543 apps were excluded as they aren’t related to stroke, including information provided by apps which were not related to stroke or target people that were not only stroke-related people (e.g., Target users include stroke patients and other chronic patients). Then a further review led to the removal of 158 duplicates. A total of 145 apps were identified to download. Whereas during the installation and application, 18 apps which didn’t run normally were excluded from the study. Finally, a total of 127 relevant apps were analyzed, with 64 apps from the Android (50%), 43 apps from the iOS (34%), and 20 apps from both Android and iOS (16%). The details for the exclusion of apps are included in Fig. 1. If both a Chinese and an English version were available on the store, both versions were adopted for further evaluation. Each app was adopted and analyzed independently by 2 researchers onto a Huawei Glory 8 (for the android platform) or i-phone 6S (for the iOS platform) smartphone.
Figure 1.
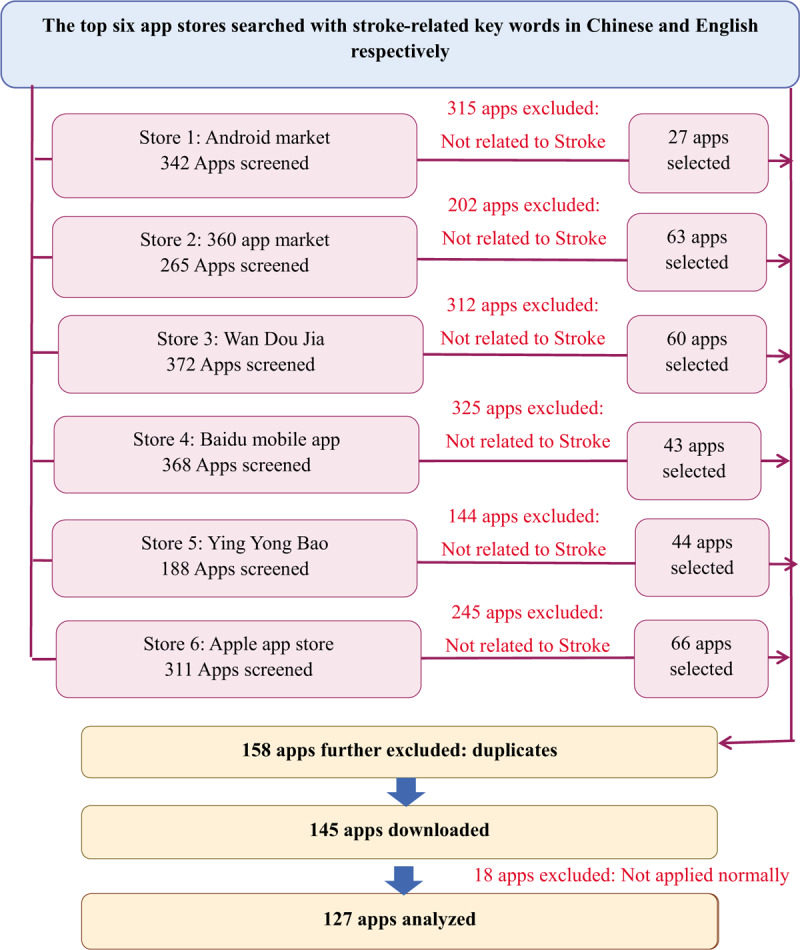
Flow chart of the selection process of apps.
2.2. Characteristics of Chinese stroke-related apps
Each app was categorized and analyzed based on operating system, cost, target people, the engagement of health professionals in the development, online health professionals’ interaction, release date, size, popularity, and usefulness. Refer to Dubey research,[23] the detailed classification criteria are as follows.
-
1.
Operating system: apps were classified based on the running system of apps.
-
(1)
IOS: the running systems is only iOS;
-
(2)
Android: the running systems is only android;
-
(3)
Both: the running systems are both iOS and android.
-
(1)
-
2.
Cost: apps were classified based on cost/free of download.
-
(1)
Free: apps were downloaded free of cost;
-
(2)
Paid: apps were downloaded after making payment.
-
(1)
-
3.
Target people: apps were classified based on people for whom the apps were designed.
-
(1)
General population: these apps were those which could be utilized by the general population for education, primary prevention, risk assessment, and first-aid of stroke;
-
(2)
Health professionals: these apps were those which could be utilized by health professionals for disease guidance, clinical information, case discussion, recent advances, and peer communication in the hospital/clinic/research laboratory;
-
(3)
Stroke patients at home: these apps were those which could be utilized by stroke patients at home for education, secondary prevention, home care, and stroke management;
-
(4)
Other: these apps were those which could be utilized by stroke patients in hospital or caregivers.
-
(1)
-
4.
The engagement of health professionals in apps development: apps were classified on the basis that whether the developing of apps had the engagement of health professionals;
-
(1)
Yes: the developer of apps contained medical associations, medical universities/medical schools, pharmaceutical companies, hospitals, research associations or medical journals; Or apps were also managed by doctors, nurses, researchers, or other health workers;
-
(2)
No: the developer of apps didn’t contain the above-mentioned organizations or apps weren’t managed by the above-mentioned people.
-
(1)
-
5.
Online interaction with health professionals: apps were classified on the basis that whether user could online interaction with health professionals via apps;
-
(1)
Yes: they apps were those apps which had the function of online interaction and could online communication via text, voice, or video with the above-mentioned organizations and people.
-
(2)
No: they were those apps which hadn’t the function of online interaction or could online communication without the above-mentioned organizations and people.
-
(1)
-
6.
Release date: apps were assessed based on the release date of apps released by developers;
-
7.
Size: apps were assessed based on the size of apps released by developers;
-
8.
Popularity: apps were divided into 4 groups based on the total frequency of downloads from 6 apps store;
-
(1)
<1000 times;
-
(2)
≥1000 times but <5000 times;
-
(3)
≥5000 times but <10,000 times;
-
(4)
≥10,000 times.
-
(1)
-
9.
Usefulness: apps were classified based on user rating released by apps stores.
-
(1)
Not useful: user rating was <2 stars;
-
(2)
Moderately useful: user rating was 2–3 stars;
-
(3)
Very useful: user rating was >3 stars.
-
(1)
2.3. Evaluation of information accountability for apps
Up to date, there remains no standardized evaluation tool that has been recommended by the guidelines for rating of the apps information accountability. The Silberg scale adapted by Griffiths and Christensen[29] was applied. This scale was originally extensively used to determine online health information quality.[30] Recently, researchers used it to assess information accountability of apps towards cardiovascular disease and postnatal depression.[26,31] It's a total of 9-point, which assesses 4 domains, including authorship, attribution, disclosure, and currency. A total score ranges from 0 to 9 (1 point for each item if present) with higher scores reflecting better information accountability.
2.4. Assessment of functionality for apps targeting stroke patients at home
Two researchers independently analyzed functionality for selected apps targeting stroke patients at home. Extracted the functionality of each app and then reviewed functionality coverage of whole apps targeting stroke patients at home in Chinese app market.
2.5. Data analysis
All statistical analysis were done using IBM SPSS Statistics 22.0 for Windows. The mean, and standard deviation were used to describe the Silberg scale scores and size of stroke-related apps. Numbers and percentages were calculated to describe basic characteristics (except size) and functions for apps. Notably, the popularity of apps were only analyzed for the android apps, as the frequency of downloads from iPhone apps are still unavailable.
2.6. Ethical considerations
This study was approved by the ethics committee of the Nursing College of Zhengzhou University.
3. Results
3.1. Characteristics of stroke-related apps
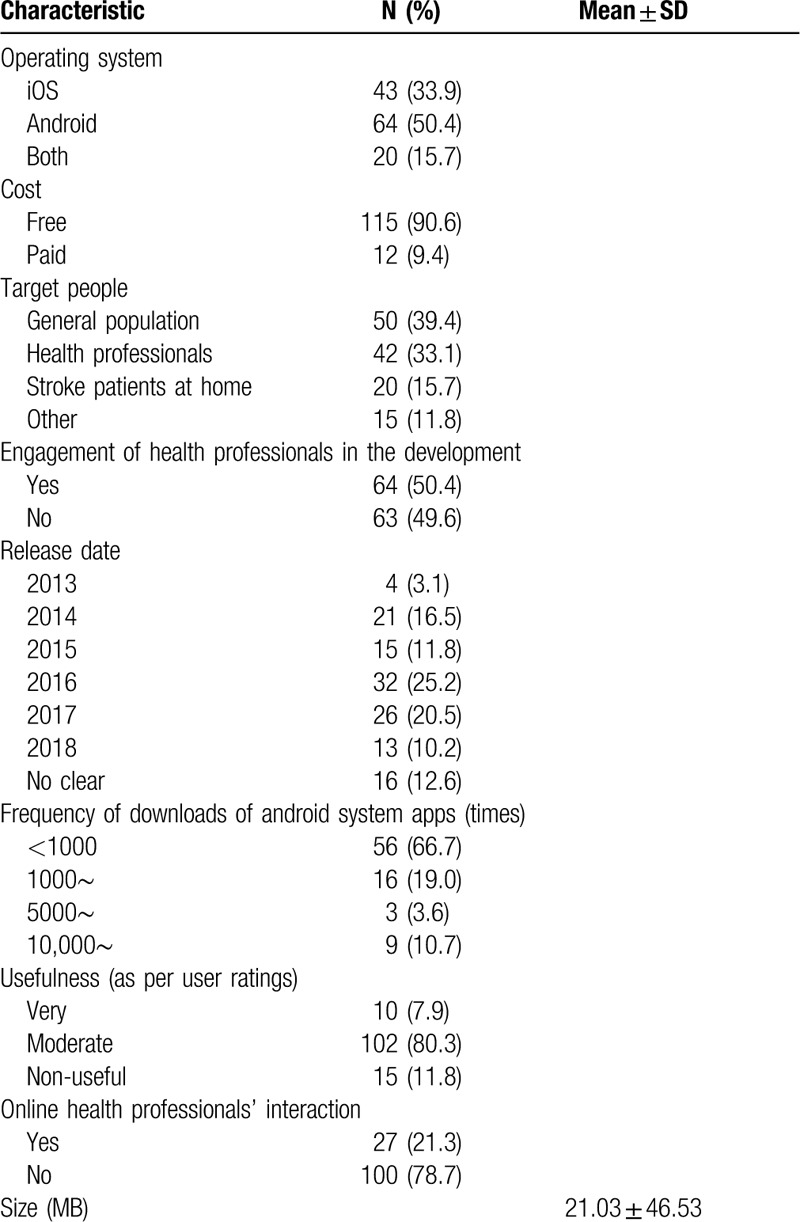
The descriptions of apps collected were performed in Table 1. Out of 127 apps, about 91% were available free of cost. About 39% of apps for the general population, about one-third (42, 33%) are for health professionals, only a small proportion (20, 16%) was designed for stroke patients at home. The stroke-related apps first appear in 2013 in China, and the largest number of apps released (32, 25%) was in 2017. The average size of apps was 21.03 MB. What's more, approximately 8% of apps were rated very useful by users, about 80% were moderately useful and the remaining (12%, 15) were non-useful. Notably, only 11% of android apps were downloaded >10,000 times, whereas 86% of android apps were downloaded <5000 times. And about half of the apps were developed without the engagement of health professionals, about 79% of apps did not have online health professionals’ interaction.
Table 1.
Characteristics of stroke-related apps.
3.2. Information accountability of stroke-related apps
The evaluation of information accountability for stroke-related apps is shown in Table 2. Out of a total of 9 scores, the mean Silberg score of 127 apps was 3.5 with an SD of 1.61, the majority of apps (92, 72%) scored at most 4 and <4% of apps had a score >7.
Table 2.
Mean Silberg scores of each dimension and the number of apps per subitem.
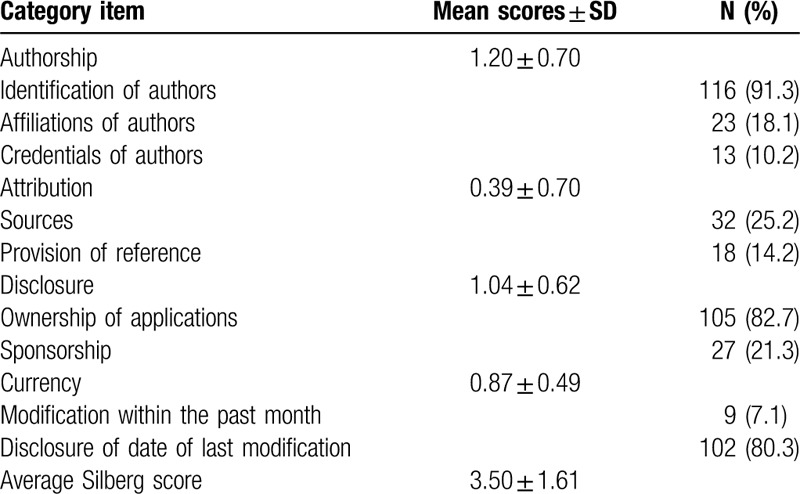
The average score of each dimension was low, ranging from 0.39 out of 2 for attribution and 1.20 out of 3 for authorship. In respect of authorship, although authors’ identification was provided for >90% of apps, only about 18% of apps identified authors’ affiliations and few-offered author's credentials (10%). With regard to attribution, only about 25% of apps indicated sources of information, and <15% of apps provided references for information. As for disclosure, about 83% of apps was disclosed the ownership of apps, but full and prominent disclosure of the sponsorship or competing interests only accounted for 21% of apps. In relation to currency, <8% of apps were updated within the past month, although dates of last modification were disclosed for 80% of apps (Table 2).
3.3. Functionality of apps targeting stroke patients at home
As shown in Fig. 2, 20 apps targeting stroke patients at home contained 9 functional domains for stroke management. The top 3 functions were “provision of information,” “rehabilitation guidance,” and “psychological support.” Whereas few apps concerned on “control of risk factors,” “modification of lifestyle,” or “management of post-stroke symptom.” Notably, over half of apps included just 1 key functional domain. Surprisingly, none of the apps contained all functions domains listed in this record.
Figure 2.
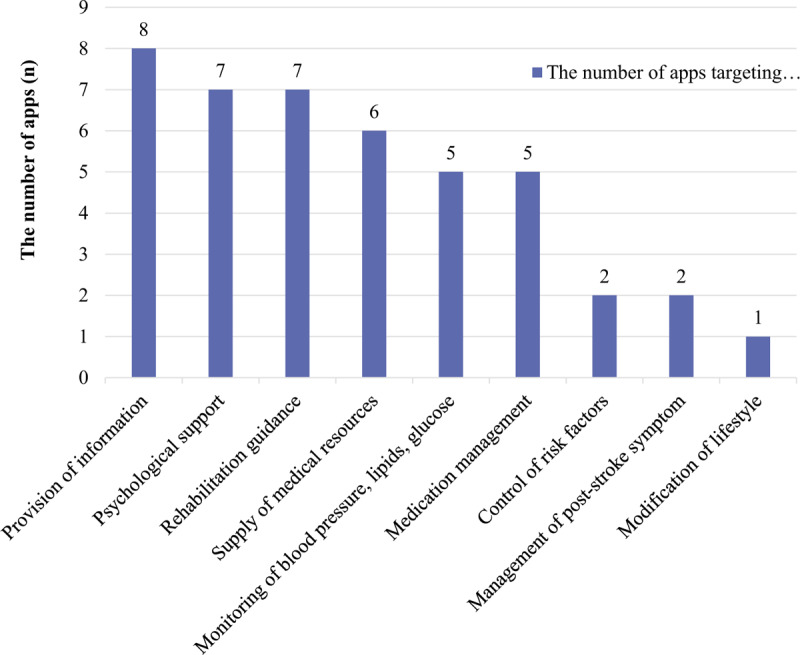
The functions coverage of apps targeting stroke patients at home.
4. Discussion
The study identified basic characteristics and information accountability for stroke-related apps available for adoption in China as well as reviewed functionality for apps targeting stroke patients at home.
Three key outcomes have arisen from our study. First, the accountability of information provided by most stroke-related apps was generally deficient. Second, the frequency of downloads in android platform and health professionals engagement in apps development were critically insufficient. Moreover, the vast majority of stroke-related apps didn’t offer a platform to facilitate online interaction with health professionals. Third, the functionality of apps targeting stroke patients at home were 9 areas, and the 3 most common of which were “provision of information,” “rehabilitation guidance,” and “psychological support.” While most app had a single function.
It is the first study that analyzed the information accountability of stroke-related apps available to adopt in the Chinese market. Our findings found that the average Silberg score of 127 stroke-related apps was 3.5 (out of a maximum score of 9). Of the 127 apps, 57 were rated above average score. Surprisingly, this mean score is apparently higher than what were analyzed in other studies, where 14 postnatal depression apps and 151 cardiovascular disease apps scored 3.0 and 2.9, respectively.[26,31] Nevertheless, it's lower in comparison to previously published study in which 39 bariatric surgery apps scored 4.0.[32] This scores acquired from our analysis could be on account that current stroke-related apps are less likely to offer these core pieces of information, including authors’ affiliations or credentials, information sources or references, sponsorship as well as updates within the past month. Corresponding with our results, prior studies also reported poor score in authors’ affiliations and credentials, sources, and references, update within the past month. For example, Jeon et al[33] and Zhang et al[32] reported the disclosure of authors’ credentials, references, and sponsorship were only 4.8%, 9.0%, and 10.3%, respectively.
Based on the above review, it's apparent that most of the apps are short of several aspects of information and hence the resultant scores are low. This might be due to the lacking in the engagement of health professionals or limited screen size of smartphone.[26,32] It also might be associated with the lack of governmental regulatory body on information quality. In July 2017, the most prominent regulatory body—the FDA—announced a new approach to approving digital health solutions which is digital products released by preselected companies would not have to go through a regulatory process for each of their product releases. This could act as a blueprint for more countries to follow.[7,34] The American Heart Association also proposed recommendations about how to stroke care via telehealth, and it highlighted telehealth must have these peculiarities for ensuring patient better access to high-quality stroke care, including safety, timeliness, effectiveness, efficiency, equality, and patient-centered.[35] Nevertheless, a review reported that stroke-related apps targeting health professionals were more scientifically valid than apps targeting general people.[23] Therefore, in order to improve accountability of information of stroke-related apps, not only the regulatory body need to be reformed, but also apps users, especially patients should be cognizant that not all apps were scientifically valid and need to consult their health professionals about availability of information gained from any app before applying apps to clinical practice.
Parallel with this study's findings, the insufficient downloads of android apps was also noted in a study of smoking cessation-related apps.[25] Indeed, over 65% of stroke-related apps in android platform were downloaded <1000 times. Compared with the number of stroke survivors and smartphone owners in China, it is undoubted that the downloads, in other words, popularity of stroke-related apps were limited. One reason might be connected with patients’ acceptance of stroke-related apps. A systematic review indicated that the user's acceptance of apps might be affected by various factors and hindered to widely generalize.[36] Sun et al[37] also reported nearly half of the patients (46.3%) weren’t willing to promoting physical activities via apps. It is therefore of pertinent importance for developers or researchers to further define the reasons of lacking in downloads. Moreover, effective interventions should be designed to facilitate popularity of apps in future research.
The findings of this study showed that most stroke-related apps lacked the engagement of health professionals in apps development. This has been noticed in a number of studies.[26] An American study of 93 stroke-related apps found 47.3% of apps were associated with the engagement of health professionals in the development.[23] A Nepalese study suggested that only 7% of apps for amblyopia treatment clearly stipulated the role of health professionals in the development.[38] Research 2 guidance also reported that types of mobile health app publishers in 2017 have increased in diversity and 23% of the mobile health market are non-healthcare companies, including IT/Tech companies, consulting/research companies, and app developers/agencies.[7] However, the evidence suggested inadequate involvement of health professionals remarkably reduces the reliability of apps.[39] As a consequence, we sincerely recommended that future stroke-related apps should be jointly conceptualized by apps developers with health professionals before integrating apps into clinical practice.
The results of our study also found that only 21.3% of stroke-related apps have online interactions with health professionals. The low online health professionals’ interaction has also been found in other medical specialty apps, such as cardiovascular disease.[26] However, the eHealth Enhanced Chronic Care model (eCCM), an important theoretical model used for enhancing patient efficiency for chronic illness management by eHealth tools, emphasizes that effective online interactions is key to improving outcomes.[40] What's more, studies also showed that continuous online interactions between users and health professionals not only strengthen users–professional relationship, but also improve care satisfaction.[41,42] Whereas, it need to be noted that professionals online response time might have negative effects on users satisfaction, although our study did not report that. Above all, aside from the recommendation that there ought to be more online interaction with health professionals in the adopting process, its also crucial for health professionals to timely respond to the online interactions problems.
Our study also showed that most of apps targeting stroke patients at home had only single function. But studies found that inadequate functions would hinder user’ acceptance of apps, and further influenced successfully promotion of apps.[43] Therefore assessing the functions coverage of apps targeting home stroke patients not only enables to develop a comprehensive app for stroke management, but also improve user’ acceptance for apps.
4.1. Limitations
This study has several limitations. First, although analyzing the apps from top 6 most popular app stores, there may not encompass apps from the literature. Thus, the selected apps may be incomplete. Second, our study only analyzed the stroke-related apps downloaded and adopted; it might be more meaningful for researchers to identify the reasons why the apps were not adopted. Nevertheless, our study is the first to assess the current status of stroke-related apps available for adoption in China, including basic characteristics and information accountability of apps. Meanwhile, it is also the first to review functionality for apps targeting stroke patients at home. Future studies may consider analyzing the apps that are not applied and explore the interventions to improve their applicability.
5. Conclusion
Our study accounts for the basic characteristics and information accountability for stroke-related apps as well as functionality for apps targeting stroke patients at home available for adoption in Chinese app market. It provides insights into how to develop apps for stroke management in the future. Whereas our study show that there is a considerable room for improvement in downloads, online interaction and health professionals engagement in apps development. The information accountability for stroke-related apps also needs to be further improved for increasing confidence in user. Additionally, it's worth thinking about how to develop a comprehensive app for stroke patients at home. The implication of our study is that the development of stroke-related apps needs to consider not only popularity, reliability, and patient's satisfaction for apps, but also information accountability and functions comprehensiveness.
Acknowledgments
The authors gratefully acknowledge team members for support, and thank for professor Zhiguang Ping from School of public health, Zhengzhou University. They also want to thank for the foundation from Department of Science and Technology of Henan Province (182102310198), the Educational Department of Henan Province (2018-ZZJH-547), and the Nursing College of Zhengzhou University (2018-hlxyxk-02).
Author contributions
Applications selection: Huixia Zhang, Yongchao Zhang, Gang Chen.
Formal analysis: Huixia Zhang.
Funding acquisition: Zhenxiang Zhang.
Investigation: Yongchao Zhang, Gang Chen.
Methodology: Huixia Zhang, Zhenxiang Zhang, Beilei Lin, Yongxia Mei.
Software: Huixia Zhang, Yongxia Mei.
Supervision: Zhenxiang Zhang.
Writing – original draft: Huixia Zhang.
Writing – review & editing: Huixia Zhang, Tao Wang, Beilei Lin.
Footnotes
Abbreviation: apps = smartphone applications.
How to cite this article: Zhang H, Wang T, Zhang Z, Lin B, Mei Y, Zhang Y, Chen G. The current status of stroke-related smartphone applications available to adopt in China: A systematic review study. Medicine. 2020;99:27(e20656).
The authors have no conflicts of interest to disclose.
References
- [1].China Daily. China has 1.3b mobile phone users: white paper; 2016. Available at: http://usa.chinadaily.com.cn/china/2016-12/01/content_27538859.htm. (Last accessed October 17, 2018). [Google Scholar]
- [2].IiMedia. 2017–2018 China smartphone market research report; 2018. Available at: http://www.iimedia.cn/60944.html. (Last accessed October 17, 2018). [Google Scholar]
- [3].Pew Research Center. Smartphone ownership rates skyrocket in many emerging economies, but digital divide remains; 2016. Available at: http://www.pewglobal.org/2016/02/22/smartphone-ownership-rates-skyrocket-in-many-emerging-economies-but-digital-divide-remains/. (Last accessed October 17, 2018). [Google Scholar]
- [4].Pew Research Center. Social Media Use Continues to Rise in Developing Countries but Plateaus Across Developed Ones; 2018. Available at: http://www.pewglobal.org/2018/06/19/social-media-use-continues-to-rise-in-developing-countries-but-plateaus-across-developed-ones/. (Last accessed October 17, 2018). [Google Scholar]
- [5].The Statistics Portal. Number of apps available in leading app stores as of 1st quarter 2018; 2018. Available at https://www.statista.com/statistics/276623/number-of-apps-available-in-leading-app-stores/. (Last accessed November 14, 2018). [Google Scholar]
- [6].Ministry of Industry and Information Technology of the People's Republic of China. The Internet and related services sector operated smoothly from January to August 2018; 2018. Available at: http://www.miit.gov.cn/n1146312/n1146904/n1648355/c6407186/content.html. (Last accessed November 14, 2018). [Google Scholar]
- [7].Research 2Guidance. mHealth Economics 2017 - Current Status and Future Trends in Mobile Health; 2017. Available at https://research2guidance.com/product/mhealth-economics-2017-current-status-and-future-trends-in-mobile-health/. (Last accessed November 14, 2018). [Google Scholar]
- [8].Parks Associates. 42% of U.S. smartphone/tablet owners use at least one fitness app, and 18% of such users use a health/wellness coaching service; 2016. Available at: http://www.parksassociates.com/blog/article/pr-10212016. (Last accessed November 14, 2018). [Google Scholar]
- [9].Sun L, Wang Y, Greene B, et al. Facilitators and barriers to using physical activity smartphone apps among Chinese patients with chronic disease. BMC Med Inform Decis Mak 2017;17:44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Huckvale K, Prieto JT, Tilney M, et al. Unaddressed privacy risks in accredited health and wellness apps: a cross-sectional systematic assessment. BMC Med 2015;13:214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Feigin VL, Krishnamurthi RV, Parmar P, et al. Update on the global burden of ischemic and hemorrhagic stroke in 1990–2013: the GBD 2013 Study. Neuroepidemiology 2015;45:161–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Mozaffarian D, Benjamin EJ, Go AS, et al. Executive summary: heart disease and stroke statistics-2016 update. Circulation 2016;133:447–54. [DOI] [PubMed] [Google Scholar]
- [13].Yu CH, Luo LS, Li M, et al. From the global views to understand the seriousness of the burden of stroke in China. J Pub Health Prev Med 2016;27:1–5. [Google Scholar]
- [14].Krishnamurthi RV, Feigin VL, Forouzanfar MH, et al. Global and regional burden of stroke during 1990–2010: findings from the global burden of disease study 2010. Lancet Glob Health 2014;383:245–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Chen WW, Gao RL, Liu LS, et al. Chinese cardiovascular disease report 2017. Chin Circ J 2017;32:521–30. [Google Scholar]
- [16].Słomka A, Świtońska M, Sinkiewicz W, et al. Assessing circulating factor VIIa-antithrombin complexes in acute ischemic stroke: a pilot study. Clin Appl Thromb Hemost 2017;23:351–9. [DOI] [PubMed] [Google Scholar]
- [17].Sureshkumar K, Murthy G, Natarajan S, et al. Evaluation of the feasibility and acceptability of the‘care for stroke’intervention in India, a smartphone-enabled, carer-supported, educational intervention for management of disability following stroke. BMJ Open 2016;6:1–0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Zhang HX, Mei YX, Lin BL, et al. Application of home care smartphone applications in stroke patients. Chin J Rehabil Theory Pract 2018;24:913–6. [Google Scholar]
- [19].Blacquiere D, Lindsay MP, Foley N, et al. Canadian stroke best practice recommendations: telestroke best practice guidelines update 2017. Int J Stroke 2017;12:886–95. [DOI] [PubMed] [Google Scholar]
- [20].Sureshkumar K, Murthy GVS, Munuswamy S, et al. ‘Care for Stroke’, a web-based, smartphone-enabled educational intervention for management of physical disabilities following stroke: feasibility in the Indian context. BMJ Innov 2015;1:127–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Wei XY, Cui Y, Zhou HL, et al. System evaluation and analysis on intelligent health application. J Med Inform 2017;38:8–12. [Google Scholar]
- [22].Kao C, Liebovitz DM. Consumer mobile health apps: current state, barriers, and future directions. PMR 2017;9:S106–15. [DOI] [PubMed] [Google Scholar]
- [23].Dubey D, Amritphale A, Sawhney A, et al. Smart phone applications as a source of information on stroke. J Stroke 2014;16:86–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Lambert K, Mullan J, Mansfield K, et al. Should we recommend renal diet–related apps to our patients? An evaluation of the quality and health literacy demand of renal diet–related mobile applications. J Ren Nutr 2017;27:430–8. [DOI] [PubMed] [Google Scholar]
- [25].Cheng F, Xu J, Su C, et al. Content analysis of smartphone apps for smoking cessation in China. JMIR Mhealth Uhealth 2017;5:e93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Xiao Q, Lu S, Wang Y, et al. Current status of cardiovascular disease-related smartphone apps downloadable in China. Telemed J E Health 2017;23:219–25. [DOI] [PubMed] [Google Scholar]
- [27].Bernardini S, Cianfrocca C, Maioni M, et al. A mobile app for the remote monitoring and assistance of patients with Parkinson's disease and their caregivers. Conf Proc IEEE Eng Med Biol Soc 2018;2018:2909–12. [DOI] [PubMed] [Google Scholar]
- [28].Akechi T, Yamaguchi T, Uchida M, et al. Smartphone problem-solving and behavioural activation therapy to reduce fear of recurrence among patients with breast cancer (Smartphone Intervention to LEssen fear of cancer recurrence: SMILE project): protocol for a randomised controlled trial. BMJ Open 2018;8:e24794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Griffiths KM, Christensen H. Quality of web based information on treatment of depression: cross sectional survey. BMJ 2000;321:1511–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Silberg WM, Lundberg GD, Musacchio RA. Assessing, controlling, and assuring the quality of medical information on the Internet: Caveant lector et viewor--Let the reader and viewer beware. JAMA 1997;277:1244–5. [PubMed] [Google Scholar]
- [31].Zhang MW, Ho RC, Loh A, et al. Current status of postnatal depression smartphone applications available on application stores: an information quality analysis. BMJ Open 2017;7:e15655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Zhang MW, Ho RC, Hawa R, et al. Analysis of the information quality of bariatric surgery smartphone applications using the silberg scale. Obes Surg 2016;26:163–8. [DOI] [PubMed] [Google Scholar]
- [33].Jeon E, Park H, Min YH, et al. Analysis of the information quality of Korean obesity-management smartphone applications. Healthc Inform Res 2014;20:23–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].FDA. Mobile Medical Applications; 2016. Available at: https://www.fda.gov/MedicalDevices/DigitalHealth/MobileMedicalApplications/default.htm#a. (Last accessed November 25, 2018). [Google Scholar]
- [35].Schwamm LH, Chumbler N, Brown E, et al. Recommendations for the implementation of telehealth in cardiovascular and stroke care: a policy statement from the American heart association. Circulation 2017;135:e24–44. [DOI] [PubMed] [Google Scholar]
- [36].Wang WJ, Hong JF, Zhang T, et al. A review of acceptance status of mobile health management in patients with chronic diseases. Chin J Nurs 2017;52:1265–8. [Google Scholar]
- [37].Sun L, Jiao C, Wang Y, et al. A survey on the willingness to use physical activity smartphone applications (Apps) in patients with chronic diseases. Stud Health Technol Inform 2016;225:1032–3. [PubMed] [Google Scholar]
- [38].Paudel N. Smartphone applications for amblyopia treatment: a review of current apps and professional involvement. Telemed J E Health 2018;24:797–802. [DOI] [PubMed] [Google Scholar]
- [39].Zhou HY, Hu YP. The investigation and analysis of Chinese pharmacy related applications based on apple App Store. Strait Pharm J 2015;27:262–3. [Google Scholar]
- [40].Gee PM, Greenwood DA, Paterniti DA, et al. The eHealth enhanced chronic care model: a theory derivation approach. J Med Internet Res 2015;17:86–108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41].Yao H, Chang H, Wang XJ, et al. The study of improving patients’ quality of life with mild to moderate stroke by mobile phone APP. Chin Nurs Manag 2017;17:103–7. [Google Scholar]
- [42].Chang H, Qiao YC, Meng Q, et al. System building of continued health service for stroke patients based on the APP information system. Chin Nurs Manag 2016;16:1269–72. [Google Scholar]
- [43].Zhang HX, Liang LL, Wang YL, et al. Acceptance of smartphone application for home patients with stroke. Chin J Rehabil Theory Pract 2018;24:824–7. [Google Scholar]