

Dear Editor
Whether smoking links to the severity of coronavirus disease 2019 (COVID-19) is a vital topic that attracts attention recently. Six meta-analyses focusing on this issue were indexed by PubMed until 20 May 2020.1–6 Among those, the letter Lippi et al.1 published in the European Journal of Internal Medicine titled ‘Active smoking is not associated with severity of COVID-19’ was special, because it had different conclusions from the others. Although the general belief is that smokers may have more severe outcomes in COVID-19, this paper provides the opposite perspective.
There were flaws in this paper because of mistakes in data collection and led to incorrect results of meta-analysis.7 The case numbers were wrong in four out of five studies. The extent of the error is rare in academic papers. Lo et al.8 also pointed out there was a ‘null hypothesis significance testing (NHST)’ flaw in this paper, and led to the inappropriate conclusions.
In this letter, another flaw is disclosed: the results of the meta-analysis are misleading. According to Fig. 1 of the paper, the pooled odds ratio (OR) is 1.69 (95% confidence interval [CI]: 0.41–6.92). The same data are used to calculate the pooled OR by RevMan. Ver. 5.3, and the results turn out to be 1.59 (95% CI: 1.04–2.42, P = 0.03) (Fig. 1). The results should have had statistical significance.
Fig. 1.
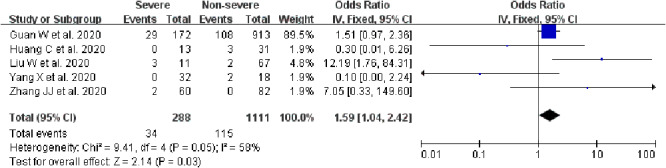
The forest plot updated according to the original data.
The results of this letter are further compared with the paper by Lippi et al.1 The ORs of individual studies are the same, except for the study by Yang et al.9 (OR, 0.11 versus 3.03). Results of this letter should be correct. This study also appears in another meta-analysis whose OR is the same as this letter.2 The weights of individual studies are also the same and indicate that Lippi et al.1 used the fixed-effects model in the meta-analysis.
The weight of the study by Yang et al.9 is small (1.9%) and could not have a significant impact on the results. The only reason the Lippi et al.1 results were so different is that they have used the pooled OR of the random effects model. In the analysis of this letter, the pooled OR of the random effects model is 1.66 (95% CI: 0.41–6.65), which is similar to Lippi et al.1 paper. Because the choice between the fixed-effects model and the random effects model dramatically changes the conclusions, they should have stated clearly the reason for the decision. They could not choose the random effects model just because they preferred a wider confidence interval and led to insignificant results.10 In any case, the forest plot in their paper is wrong because it has the results of the random effects model with the weights of the fixed-effects model.
In conclusion, Lippi et al.1 have flaws in data collection, statistical analysis and inference of conclusions. The results should have endorsed the association between smoking and the severity of COVID-19.
Conflict of Interest
None.
References
- 1. Lippi G, Henry BM. Active smoking is not associated with severity of coronavirus disease 2019 (COVID-19). Eur J Intern Med 2020;75:107–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Zhao Q, Meng M, Kumar R et al. The impact of COPD and smoking history on the severity of Covid-19: a systemic review and meta-analysis. J Med Virol 2020. doi: 10.1002/jmv.25889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Zheng Z, Peng F, Xu B et al. Risk factors of critical & mortal COVID-19 cases: a systematic literature review and meta-analysis. Review J Infect 2020;S0163-4453:30234–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Guo FR. Smoking links to the severity of Covid-19: an update of a meta-analysis. J Med Virol 2020. doi: 10.1002/jmv.25967. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Alqahtani JS, Oyelade T, Aldhahir AM et al. Prevalence, severity and mortality associated with COPD and smoking in patients with COVID-19: a rapid systematic review and meta-analysis. PLoS One 2020;15:e0233147. doi: 10.1371/journal.pone.0233147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Patanavanich R, Glantz SA. Smoking is associated with COVID-19 progression: a meta-analysis. Nicotine Tob Res 2020. doi: 10.1093/ntr/ntaa082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Guo FR. Active smoking is associated with severity of coronavirus disease 2019 (COVID-19): an update of a meta-analysis. Tob Induc Dis 2020;18(37). doi: 10.18332/tid/121915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Lo E, Lasnier B. Active smoking and severity of coronavirus disease 2019 (COVID-19): the use of significance testing leads to an erroneous conclusion. Eur J Intern Med 2020. doi: 10.1016/j.ejim.2020.05.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Yang X, Yu Y, Xu J et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med 2020. doi: 10.1016/S2213-2600(20)30079-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Umscheid CA. A primer on performing systematic reviews and meta-analyses. Clin Infect Dis 2013;57:725–34. [DOI] [PubMed] [Google Scholar]