

To the Editor:
We would like to describe a follow-up study that illustrates the ability of aerosol and droplets to be generated in intraocular surgery performed on a model eye. We have previously demonstrated that aerosol can be generated in an open chamber system with phacoemulsification but not vitrectomy [1].
We used both the Bausch and Lomb Stellaris PC and Alcon Constellation platform to simulate aerosol generation in intraocular surgery using an Advanced Cataract model eye from Phillips Studio (Bristol, UK). Fluorescein dye was injected into the anterior chamber. Using a black background and dark room, a blue light was used to allow better visualisation of aerosol and droplet formation. Videos were taken to visualise aerosol/droplet generated [2, 3].
We found that in a tightly sealed cornea wound, it was possible to prevent visible aerosol formation in phacoemulsification. However, with a leaky wound, aerosol could be seen to be generated from phacoemulsification [2]. (Fig. 1a) In vitrectomy, there was no evidence of visible aerosol or droplet formation using a 25 gauge sealed trocar [3]. When conducting air exchange, there was droplet formation at the trocar exit especially when the silicone seal for the trocar was removed or damaged. At air gas exchange, droplets could also be seen when a 25 gauge needle was passed through the sclera at the hub end opening of the needle. (Fig. 1b) No visible aerosol was observed in any of the vitrectomy steps using the model eye.
Fig. 1. Aerosol and droplet generation in model eye.
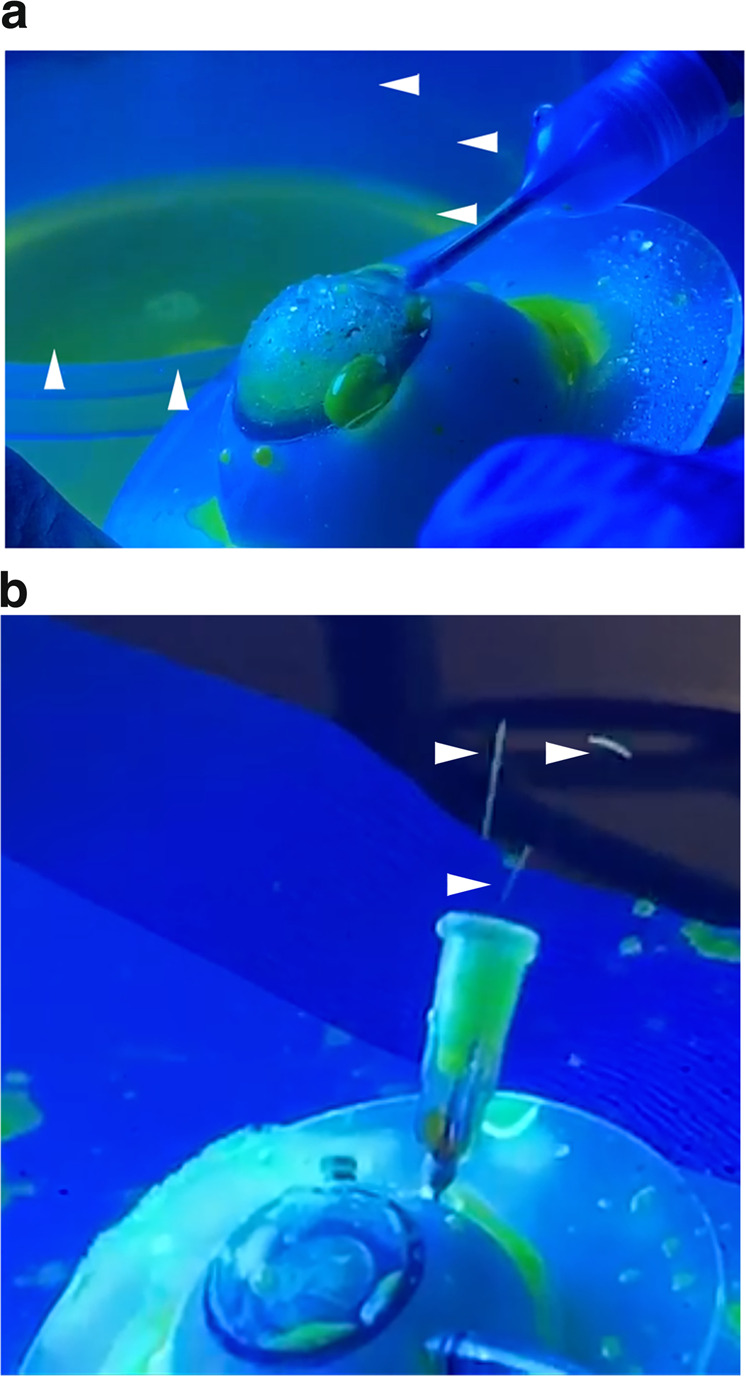
a Aerosol generated with phacoemulsification hand piece in model eye: arrows denote aerosol. b Droplet seen at hub of 25 gauge needle with air gas exchange: arrows denote droplets.
Our attempts of visualising aerosol depend on the sensitivity of the camera. Smaller amounts of bioaerosols which can be less than 10 microns require sophisticated instrumentation to detect [4]. Therefore, small quantities of aerosol which were not detected using our methodology may still be present. Further consideration must be taken in relation to the amount of virus required to cause disease and the presence of virus in ocular tissue. Due to the virucidal activity of iodine and the routine preoperative povidone iodine preparation in intraocular surgery, the presence of virus in the conjunctival sac is likely to be low [5]. There are also no reports of coronavirus detected in aqueous and vitreous humour in the literature thus far. Therefore, risk of disease transmission in intraocular surgery may be minimal if care is taken in constructing the wound during phacoemulsification.
Compliance with ethical standards
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Wong R, Bannerjee P, Kumaran N. Aerosol generating procedures in intraocular surgery. Eye. 2020. 10.1038/s41433-020-0997-7. [DOI] [PMC free article] [PubMed]
- 2.Wong R, Dellaversana G, Kumaran N. Aerosol generation in ophthalmic procedures: Part 2 using model eye. 2020. https://youtu.be/bGNezVnj01M. Accessed 15 May 2020.
- 3.Wong R, Bannerjee P, Kumaran N. Aerosol generation in ophthalmic procedures: Part 3 using model eye. 2020. https://youtu.be/qztIA–W0qU. Accessed 15 May 2020.
- 4.Pan YL. Detection and characterization of biological and other organic-carbon aerosol particles in atmosphere using fluorescence. J Quant Spectroc Ra. 2015;150:12–35. doi: 10.1016/j.jqsrt.2014.06.007. [DOI] [Google Scholar]
- 5.Eggers M, Eickmann M, Zorn J. Rapid and effective virucidal activity of povidone-iodine against Middle East respiratory syndrome coronavirus (MERS-CoV) and modified vaccinia virus ankara (MVA) Infect Dis Ther. 2015;4:491–501. doi: 10.1007/s40121-015-0091-9. [DOI] [PMC free article] [PubMed] [Google Scholar]