

Importance:
Recent reports identify that among hospitalized coronavirus disease 2019 patients, 30% require ICU care. Understanding ICU resource needs remains an essential component of meeting current and projected needs of critically ill coronavirus disease 2019 patients.
Objectives:
This study queried U.S. ICU clinician perspectives on challenging aspects of care in managing coronavirus disease 2019 patients, current and anticipated resource demands, and personal stress.
Design, Setting, and Participants:
Using a descriptive survey methodology, an anonymous web-based survey was administered from April 7, 2020, to April 22, 2020 (email and newsletter) to query members of U.S. national critical care organizations.
Measurements and Main Results:
Through a 16-item descriptive questionnaire, ICU clinician perceptions were assessed regarding current and emerging critical ICU needs in managing the severe acute respiratory syndrome coronavirus 2 infected patients, resource levels, concerns about being exposed to severe acute respiratory syndrome coronavirus 2, and perceived level of personal stress. A total of 9,120 ICU clinicians responded to the survey, representing all 50 U.S. states, with 4,106 (56.9%) working in states with 20,000 or more coronavirus disease 2019 cases. The 7,317 respondents who indicated their profession included ICU nurses (n = 6,731, 91.3%), advanced practice providers (nurse practitioners and physician assistants; n = 334, 4.5%), physicians (n = 212, 2.9%), respiratory therapists (n = 31, 0.4%), and pharmacists (n = 30, 0.4%). A majority (n = 6,510, 88%) reported having cared for a patient with presumed or confirmed coronavirus disease 2019. The most critical ICU needs identified were personal protective equipment, specifically N95 respirator availability, and ICU staffing. Minimizing healthcare worker virus exposure during care was believed to be the most challenging aspect of coronavirus disease 2019 patient care (n = 2,323, 30.9%). Nurses report a high level of concern about exposing family members to severe acute respiratory syndrome coronavirus 2 (median score of 10 on 0–10 scale). Similarly, the level of concern reached the maximum score of 10 in ICU clinicians who had provided care to coronavirus disease 2019 patients.
Conclusions:
This national ICU clinician survey identifies continued concerns regarding personal protective equipment supplies with the chief issue being N95 respirator availability. As the pandemic continues, ICU clinicians anticipate a number of limited resources that may impact ICU care including personnel, capacity, and surge potential, as well as staff and subsequent family members exposure to severe acute respiratory syndrome coronavirus 2. These persistent concerns greatly magnify personal stress, offering a therapeutic target for professional organization and facility intervention efforts.
Keywords: coronavirus disease 2019, critical care, critical care clinician, intensive care unit, intensive care unit clinician, pandemic
Despite mitigation and containment measures, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) continues to spread across the globe. At present, over 5.8 million cases have been identified and are accompanied by over 362,000 deaths worldwide (1). Despite increasing test availability, many consider these numbers to remain underestimates of the actual global disease burden. Recent reports identify that up to 14% of coronavirus disease 2019 (COVID-19) cases require hospitalization and treatment in the ICU. Among hospitalized patients, 30% require ICU care and 29% or more of those in the ICU require mechanical ventilation (2, 3). Understanding ICU resource needs remains an essential component in meeting current and projected needs of critically ill patients and healthcare workers during a pandemic such as COVID-19. Establishing and managing surge capacity, ICU team staffing, infection and prevention control measures, clinical care pathways, scarce resource allocation, goals of care, ethical challenges, and staff well-being all merit specific attention as each domain is stressed by pandemic care (4).
The Society of Critical Care Medicine (SCCM), a multiprofessional organization representing physicians, nurses, pharmacists, respiratory therapists, and other ICU clinicians, launched a series of COVID-19 focused rapid cycle surveys to obtain essential information related to critically ill patient care during the COVID-19 pandemic. The first survey, conducted between March 18, 2020, and March 25, 2020, discovered that while critical care capacity was being augmented, the majority of respondents (n = 4,547, 93.9%) anticipated ICU personal protective equipment (PPE) shortages based upon their current user profile. Chief reported concerns included ICU resource shortages including supplies, therapeutic agents, beds, and staff as well as concerns regarding large volume patient surge leading to facility and ICU overcrowding (5). In order to assess evolving ICU-relevant aspects of COVID-19 pandemic care, a second survey was created and disseminated. This follow-up survey focused on critical areas of need, ICU clinician perceptions of emerging issues in patient management, as well as personal—as opposed to system—concerns.
MATERIALS AND METHODS
A descriptive survey methodology design was used. Data were obtained using a national web-based anonymous survey over a 2-week period between April 7, 2020, and April 22, 2020. The survey targeted members of the Critical Care Societies Collaborative, a grouping of four major U.S. critical care professional organizations including the American Association of Critical-Care Nurses, the American College of Chest Physicians, the American Thoracic Society, and the SCCM. Collectively these organizations represent over 150,000 critical care professionals including physicians, advanced practice providers, nurses, respiratory therapists, pharmacists, and other healthcare clinicians.
The 16-item questionnaire assessed ICU clinician perceptions of key resource challenges in providing patient care, clinician concerns about exposure to SARS-CoV-2, anticipated future limitations, and their perceived level of personal stress. Current resource concerns were assessed in three descending tiers of priority. Active concerns were then followed by inquiry into clinician’s perceptions of potentially anticipated future shortages. The survey was created using SurveyMonkey (San Mateo, CA) and distributed via email and newsletter invitation.
RESULTS
A total of 9,120 ICU clinicians completed the survey. A total of 7,371 respondents indicated their profession, including ICU nurses (n = 6,731, 91.3%), advanced practice providers (nurse practitioners and physician assistants; n = 334, 4.5%), physicians (n = 212, 2.9%), respiratory therapists (n = 31, 0.4%), and pharmacists (n = 30, 0.4%) and an “other” category which included certified registered nurse anesthetists, emergency medicine flight personnel, ICU medical and nursing directors, trainees in graduate medical education, dieticians, and nursing and medical students (n = 33, 0.4%) (Table 1). All responding clinicians worked in critical care settings in the United States including Puerto Rico.
Respondents worked in community (n = 5,752, 63.2%), academic (n = 2,589, 28.5%), government (n = 420, 4.6%), or other healthcare settings including private, rural, critical access, or telehealth facilities (n = 338, 3.7%). Employment locations included metropolitan and urban with a population more than 50,000 (n = 6,319, 69.5%), micropolitan and urban with a population of 10,000–50,000 (n = 2,186, 24.0%), and rural with a populations fewer than 10,000 (n = 588, 6.5%) (Table 1).
Table 1.
ICU Clinician Demographics
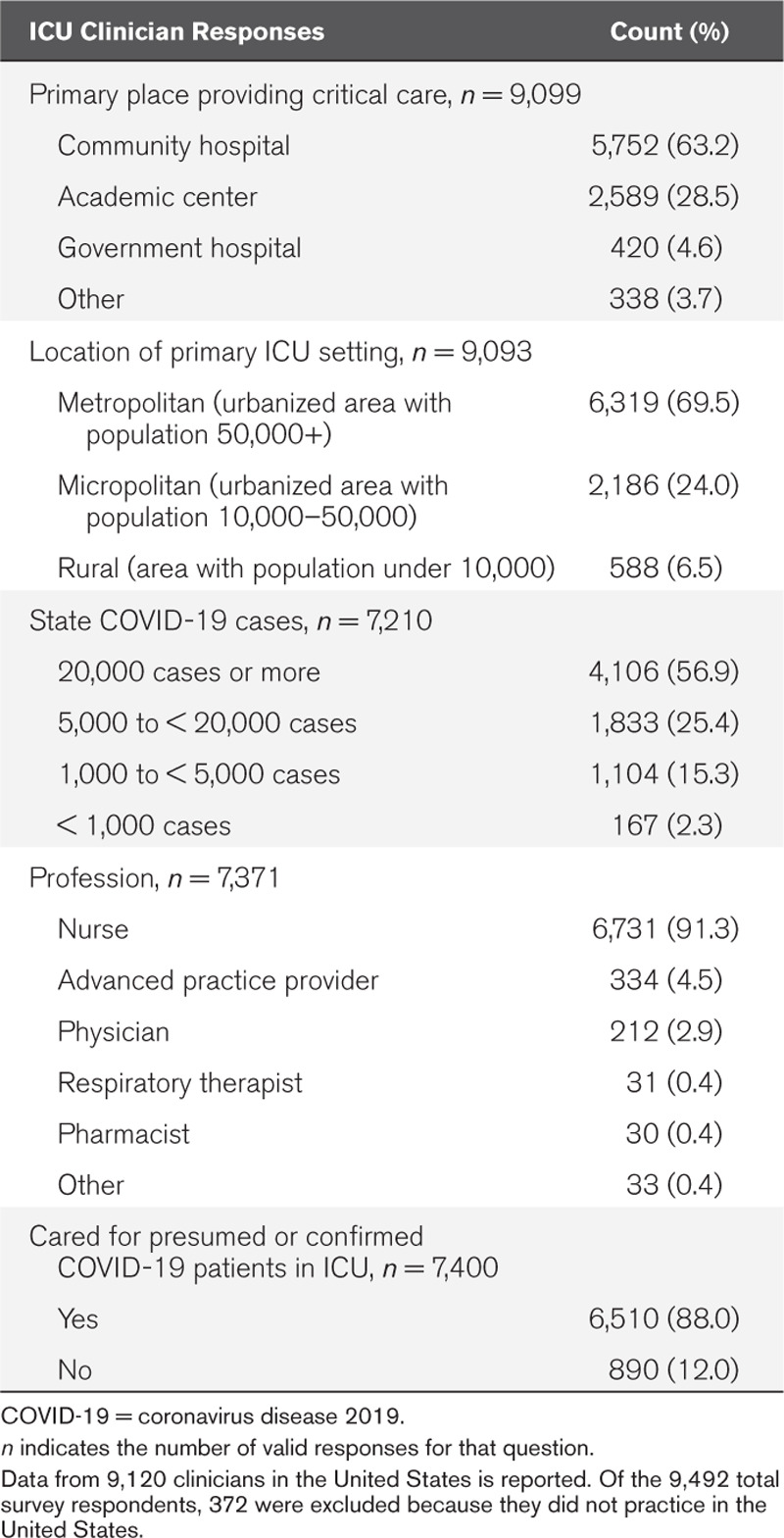
The majority (n = 6,510, 88%) reported having cared for a patient with presumed or confirmed COVID-19 (Fig. 1). A total of 4,106 (56.9%) respondents work in states with 20,000 or more COVID-19 cases, while 1,833 (25.4%) were in states with 5,000 to 20,000 cases, and 1,104 (15.3%) were in states with fewer than 5,000 cases at the time of the survey responses (Table 1 and Fig. 2).
Figure 1.
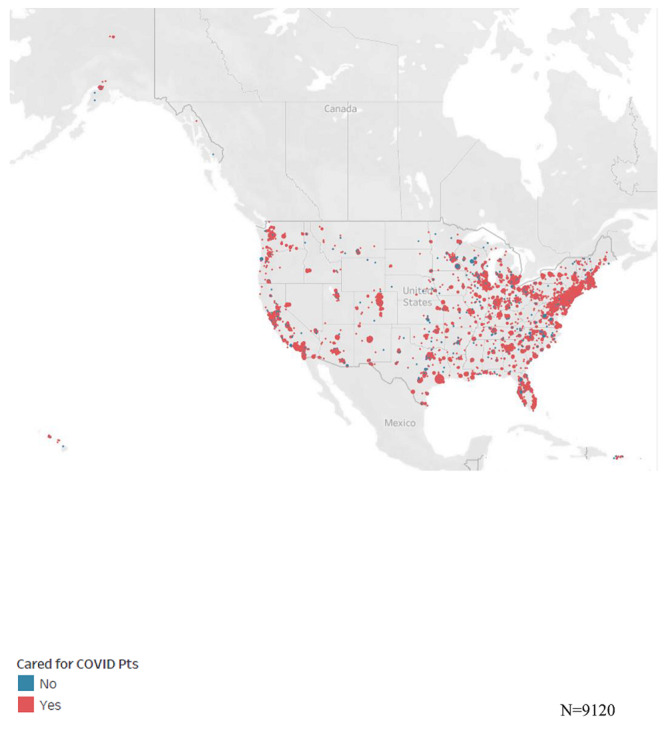
ICU clinician respondents and reports of caring for suspected or confirmed coronavirus disease 2019 (COVID-19) patients (n = 9,120).
Figure 2.
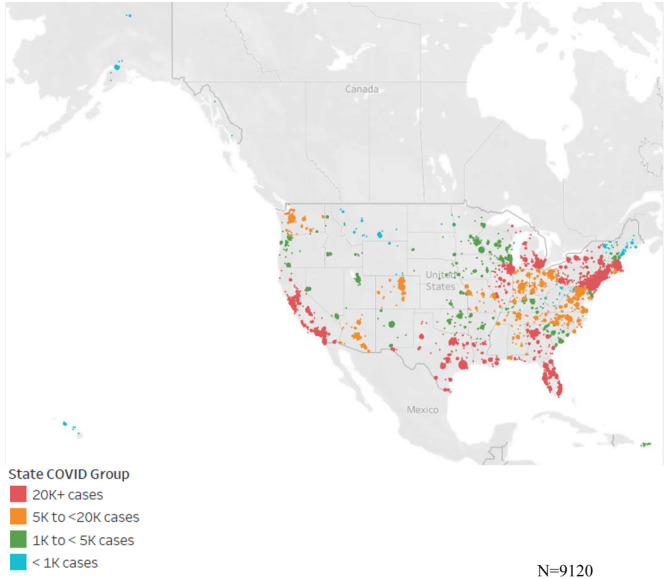
ICU clinician respondents based on the state number of confirmed coronavirus disease 2019 (COVID-19) patients.
Current Resource Challenges
The perceived need for both PPE masks (N95 respirators) (n = 2,896, 38%) and ICU staffing shortages (n = 1,614, 21.2%) exceeded all other resource challenges. Other critical needs included remaining current with regard to evolving management strategies (n = 399, 5.2%), delays in obtaining laboratory results of COVID-19 testing (n = 779, 10.2%), airborne infection isolation room (AIIR) capacity (n = 362, 4.8%), and overcoming shortages of critical ICU medications including sedatives, analgesics, and neuromuscular blocking agents (n = 299, 3.9%; Table 2 and Fig. 3).
Figure 3.

ICU critical needs for coronavirus disease 2019 (COVID-19) pandemic. PPE = personal protective equipment.
N95 respirators and ICU staffing consistently remained the most pressing concern for clinicians regardless of whether they had cared for a presumed or confirmed COVID-19 positive patient (37.3% N95 respirators, 22.6% staffing), or had not provided such care (43% N95 respirators, 12.5% staffing). This pattern remained durable regardless of the number of COVID-19 cases in the state as well.
Less frequent concerns were raised regarding ICU bed capacity (n = 272, 3.6%) and PPE gowns (n = 266, 3.5%). Infrequent concerns were noted for PPE gloves, hand sanitizing gel, non-ICU staffing, and curiously, ventilator availability (all 1% or less).
Anticipated Future Limitations
With ongoing pandemic care, ICU clinicians identified a number of resources they believed are likely to become limited, even if they were not currently limited. Anticipated limitations included personnel (n = 3,734, 40.9%), therapeutic agents (n = 3,320, 36.4%), ICU bed capacity especially related to surge potential (n = 3,292, 36.1%), AIIR availability (n = 2,868, 31.4%), institution provided care strategy updates (n = 2,087, 22.9%), and invasive ventilators (n = 2,254, 24.7%) (Table 2).
Table 2.
Coronavirus Disease 2019 Pandemic Care Perceptions (Overall Number of Responses = 9,120)

Clinician Concern Regarding Exposure to COVID-19
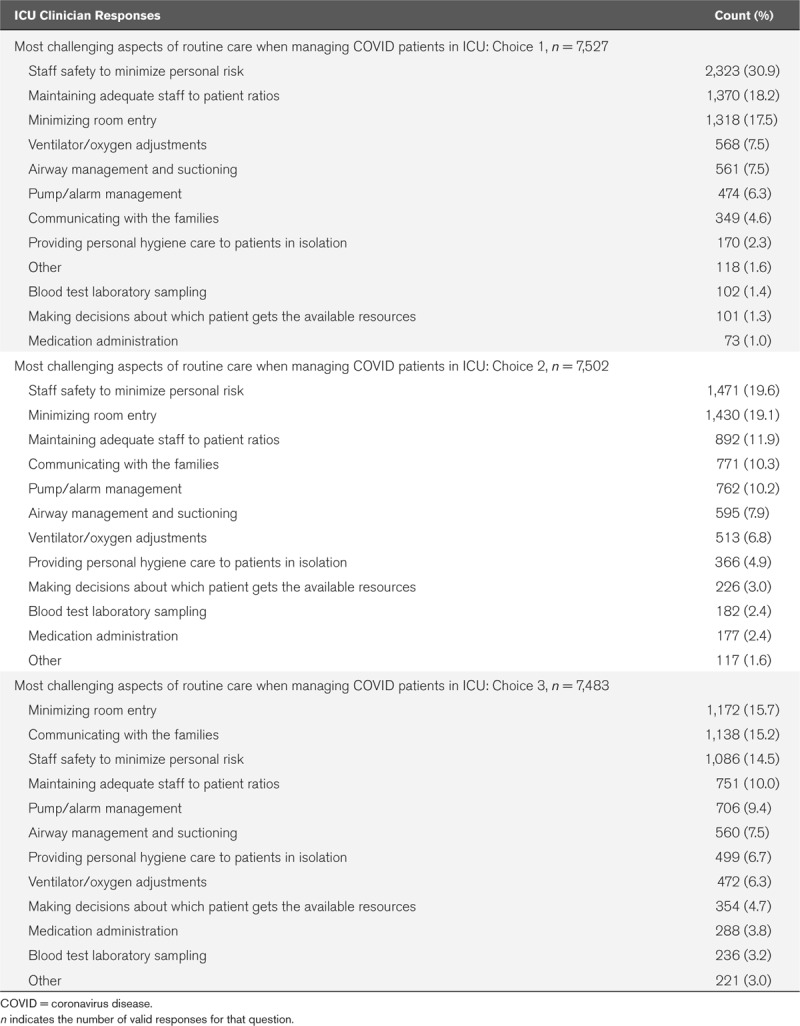
Minimizing healthcare worker virus exposure was believed to be the most challenging aspect of COVID-19 patient care (n = 2,323, 30.9%); family communication was viewed as much less challenging (n = 349, 4.6%) as was rendering decisions about resource allocation (n = 101, 1.3%). All clinicians identified staff safety to minimize personal risk as the most challenging aspect of managing COVID-19 patients in the ICU (respiratory therapists [45.2%], pharmacists [36.7%], physicians [35.7%], nurses [30.6%], and advanced practice providers [27.8%]).
Care activities perceived to bear the greatest risk of virus exposure included maintaining adequate staff to patient ratios (n = 1,370, 18.2%), minimizing the number of room entries (n = 1,318, 17.5%), ventilator and oxygen therapy management (n = 568, 7.5%), airway management including suctioning (n = 561, 7.5%), pump and monitor alarm management (n = 474, 6.3%), providing patient hygiene care (n = 170, 2.3%), obtaining blood samples (n = 102, 1.4%), and making decisions about resource allocation for patients in settings of resource constraints (n = 101, 1.3%) (Table 3).
Table 3.
Coronavirus Disease 2019 Pandemic Challenging Aspects of Care
On a scale of 0 (no concern) to 10 (maximally concerned), the aggregate median level of concern about being exposed to SARS-CoV-2 was 8, while the level of concern about exposing family members as a result of bringing the virus home was 10. The level of ICU clinician concern regarding personal exposure was a median of 8 regardless whether they had engaged in COVID-19 positive or presumed positive care. Nonetheless, a higher median score of 9 was noted from clinician respondents from states with 20,000 or more COVID-19 cases, compared to a median of 8 from respondents in states with fewer cases (Table 2).
Risk Perception and Measures Used to Limit Potential COVID-19 Transmission to Family Members
Nurses indicated a higher level of concern regarding potentially exposing family members to SARS-CoV-2 (median of 10) as a result of engaging in the care of patients with presumed or confirmed COVID-19. An only slightly reduced score was noted for advanced practice providers, physicians, and respiratory therapists (median of 9), while pharmacists scored lowest with a median of 8. The level of concern reached the maximum score of 10 in those with have provided care to patients with COVID-19. In those who have not provided care to patients with COVID-19, concern remained high with a median score of 9. Clinician concern about exposing family members to SARS-CoV-2 was also highest in respondents from states with 20,000 cases or more (median = 10) compared with 9 for respondents from states with fewer COVID-19 cases.
ICU clinicians employed a variety of measures to help reduce the risk of SARS-CoV-2 potential transmission to family members. Reported measures included changing clothes before and after work for travel home (n = 6,551, 71.8%), showering before rejoining family (n = 5,823, 63.8%), limiting or avoiding physical contact until after showering (n = 5,215, 57.2%), using alcohol-based hand sanitizer before entering their home (n = 4,650, 51%), showering and washing clothes away from family (n = 4,132, 45.3%), isolating themselves from their family members while at home (n = 1,502, 16.5%), isolating themselves from family members by living in alternate housing (n = 1,090, 12%), and wearing a mask while at home (n = 619, 6.8%) (Table 2).
Personal Stress Level
Personal stress level in ICU clinicians reportedly increased from a median pre-pandemic level of 3 to a COVID-19 pandemic level of 8 (Table 2). Engaging in the care of a presumed or confirmed COVID-19 patient increased the median stress score to 8 compared with those without similar patient care exposure who scored a 7.
DISCUSSION
These data reflect the experiences of ICU clinicians with care, resources, and exposure after the start of the COVID-19 pandemic in the United States. As such, the data are a useful follow-up to the initial survey, which uncovered concerns that were principally garnered before the pandemic had affected large portions of the United States (5). This survey’s data are instead informed by direct care and are parsed based on the density of exposure as indicated by the number of cases of COVID-19 infected patients in a region. Slightly more than half of our data flows from clinicians in states with more than 20,000 COVID-19 cases, supporting the generalizability of the findings. In keeping with the observation that the ICU team member with the greatest time-based exposure is the bedside critical care nurse, this survey predominantly reflects nursing responses.
Compared to the earlier focus regarding specific kinds of ICU resources challenges—principally revolving around the availability of mechanical ventilators—this survey underscores a different set of concerns. Those include three broad groups: PPE, staff, and therapeutic agents, with the most critical need being PPE masks (N95 respirators). This seems justified given that the global monthly requirement for gloves and masks is 76 million and 89 million, respectively, according to the World Health Organization (6). The United States was expected to need 3.5 billion N95 respirators to meet the needs for patient care at the height of the pandemic despite having only a fraction of that available in the Strategic National Stockpile (7). The Food and Drug Administration provides conservation recommendations for institutions to consider (8). Given the transmissibility of SARS-CoV-2 as a respiratory pathogen, mask shortage concerns are anticipated. Unexpectedly, the respondents to this survey did not identify ventilator shortage as an immediate concern. These data contrasts to the experience in overwhelmed sites like New York City (NYC) for whom invasive ventilator shortage has been a reality. To wit, 4,000 devices were sent from the secure national stockpile to NYC to help offset their device shortage. Our data clearly reflect the influence of non-NYC practice locations.
Utilization rates for the range of ICU supplies provide insight into the tension between existing, and replenishable, supply compared to how rapidly those supplies are used. Prior to SARS-CoV-2 infected or suspected patient care, estimates may have more reflected models than empirically derived determinations. In the wake of the SARS-CoV-2 U.S. spread, anticipated supply concerns are more firmly rooted in practical experience. For this specific respondent group of principally bedside ICU team members, personnel, therapeutic agents, AIIR capacity, and ventilators were anticipated to be in short supply as pandemic care continued. Staff concerns in particular likely reflect a multiplicity of influences including patient surge compared to available staff, staff inability to work due to immune compromise, staff exhaustion, and undoubtedly, realistic concerns regarding staff exposure to, and infection by SARS-CoV-2. Exposure may lead to quarantine, and infection may lead to care within the very unit within which one previously provided care.
It is these observations, writ large across headlines and within one’s critical care unit that gives rise to near uniform concerns regarding transmission of SARS-CoV-2 to members of one’s household. Direct care activities and especially those related to airway care, as opposed to presence in the workplace, ranked highest in COVID-19 care challenges for bedside clinicians. These difficulties likely reflect care rendered while in PPE that is not worn on a daily basis prior to the pandemic. Furthermore, the need for such PPE drives fear regarding viral transmission from the healthcare worker to their household. The greater the intensity of direct care experience, the greater the concern for transmission among respondents. Reports of healthcare clinician deaths due to COVID-19 further highlight the risk to ICU clinicians (9). Unsurprisingly, nurse scores were high with regard to concerns about viral transmission. Respondent concerns regarding transmission of SARS-CoV-2 to members of one’s household are similar to those previously reported by other healthcare clinicians (10). In a recent survey of over 32,000 nurses, the American Nurses Association reported that access to PPE remains a top concern with nearly nine-out-of-10 nurses expressing fear regarding returning to work on the basis of lack of sufficient PPE (11).
Viral transmission mitigation strategies were varied but focused on common themes: reducing viral burden on clothing, immediate hygiene measures upon returning home, and some measure of distancing from family members either transient or durable. In the extreme form, some clinicians lived apart from their family members either in a separate space in the same home or at an alternate location, including in the family recreational vehicle. Although many measures seem prudent and are easy to embrace, the need to engage in those measures uniformly generates stress. This particular stress burden, which does not generally accompany usual, pre-pandemic critical care is substantially different in intensity. The impact of the duration of sustained stress on the critical care workforce merits careful surveillance, facility and professional society attention, and the articulation of mitigation and perhaps rescue strategies to preserve frontline critical care clinician health and field longevity.
The survey has several important limitations. The survey used convenience sampling and the results cannot, therefore, be generalized. Respondents may over or under-represent the population of ICU clinicians. The majority of respondents were nurses, which may decrease the applicability of the data to other members of the team. However, the reasonable concordance of nurse driven data with that of other respondents suggests that the perspectives and concerns of the ICU clinician respondents are sufficiently similar to one another. The data obtained are insufficiently granular to parse on the basis of contact or care with another healthcare worker who has contracted SARS-CoV-2 infection, or succumbed to it. There is an insufficient number of respondents to analyze data at the state and city level to glean regional variations such as the perception of ventilator shortages from within these datasets. However, this survey was not intended to assess resource numbers or shortages, but rather how clinician perceptions of resource challenges could be prioritized and what they believed is anticipatable in the future based upon their direct care experiences. We did not assess the impact of stress on clinicians, nor what measures they had embraced to reduce their stress and their effectiveness. Such inquiry will be important, however, as this is unlikely to be the last pandemic our nation faces.
CONCLUSIONS
Data garnered after ICU clinician experience with COVID-19 positive or presumed positive care identifies key priority areas for facility attention. These include PPE, specifically N95 respirators, therapeutic agents, personnel, negative pressure room supply, and ICU bed volume. High intensity concerns regarding healthcare worker safety from viral infection, and in particular, viral transmission risk to household members is common among frontline critical care clinicians. Taken together, sustained concerns regarding resource adequacy coupled with those of clinician and family member safety have substantially augmented the reported personal stress levels in those who have provided direct COVID-19 patient care. Implementing measures such as priority COVID-19 testing for healthcare workers may help to decrease the levels of personal stress and concern. Stress mitigation and healthcare worker rescue should be a priority for healthcare facilities, healthcare systems, and medical professional organizations in concert with one another.
Footnotes
Drs. Ferraro and Maves are U.S. military service members. This work was prepared as part of their official duties. The remaining authors have disclosed that they do not have any potential conflicts of interest.
REFERENCES
- 1.John Hopkins University & Medicine Coronavirus Resource Center. 2020. Available at: https://coronavirus.jhu.edu/map.html. Accessed May 29, 2020
- 2.Richardson S, Hirsch JS, Narasimhan M, et al. ; Northwell COVID-19 Research Consortium: Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the NewYork City area. JAMA 2020; 323:2052–2059 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Myers LC, Parodi SM, Escobar GJ, et al. Characteristics of hospitalized adults with COVID-19 in an integrated health care system in California. JAMA 2020; 323:2195–2198 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Griffin KM, Karas MG, Ivascu NS, et al. Hospital preparedness for COVID-19: A practical guide from a critical care perspective. Am J Respir Crit Care Med 2020; 201:1337–1344 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kaplan LJ, Kleinpell R, Maves RC, et al. Critical care clinician reports on coronavirus disease 2019: Results from a national survey of 4,875 ICU providers. Crit Care Explor 2020; 2:e0125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.World Health Organization: Shortage of Personal Protective Equipment Endangering Health Workers Worldwide. 2020. Available at: https://www.who.int/news-room/detail/03-03-2020-shortage-of-personal-protective-equipment-endangering-health-workers-worldwide. Accessed May 2, 2020.
- 7.United States House of Representatives Committee on Oversight and Reform: Shortages of Personal Protective Equipment. 2020. Available at: https://oversight.house.gov/sites/democrats.oversight.house.gov/files/2020-03-21.CBM%20SFL%20JR%20Rouda%20GEC%20to%20HHS%20re%20PPE%20%281%29.pdf. Accessed May 2, 2020
- 8.U.S. Food and Drug Administration: Surgical Mask and Gown Conservation Strategies - Letter to Health Care Providers. 2020. Available at: https://www.fda.gov/medical-devices/letters-health-care-providers/surgical-mask-and-gown-conservation-strategies-letter-health-careproviders. Accessed May 2, 2020
- 9.Cook T, Kursumovic E, Lennane S. Exclusive: Deaths of NHS Staff From Covid-19 Analyzed. Health Serv J 2020. 2020. Available at: https://www.hsj.co.uk/exclusive-deaths-of-nhs-staff-from-covid-19-analysed/7027471.article. Accessed May 2, 2020
- 10.California Health Care Foundation: COVID-19 Tracking Poll: More Critical Care Doctors Report Sufficient Protective Gear and Tests. 2020. Available at: https://www.chcf.org/blog/covid-19-tracking-poll-moredoctors-report-sufficient-protective-gear-tests/. Accessed May 2, 2020
- 11.American Nurses Association: National COVID-19 Nursing Survey. 2020. Available at: https://www.nursingworld.org/news/news-releases/2020/survey-nurses-fear-going-to-work-due-tolack-of-protection-from-virus-more-than-32k-nurses-share-experience-from-the-front-lines/. Accessed May 2, 2020