

Abstract
Children with HIV have an increased risk of developing Kaposi Sarcoma (KS) and non-Hodgkin lymphoma (NHL) compared to HIV-negative children. We compiled currently published epidemiologic data on KS and NHL among children in sub-Saharan Africa (SSA). Among countries with available data, the median incidence of KS was 2.05/100,000 in the general pediatric population and 67.35/100,000 among HIV-infected children. The median incidence of NHL was 1.98/100,000 among the general pediatric population, while data on NHL incidence among HIV-infected children was lacking. Larger regional studies are needed to better address the dearth of epidemiologic information on pediatric KS and NHL in SSA.
Keywords: pediatric, epidemiology, Kaposi sarcoma, non-Hodgkin lymphoma, Africa
Introduction
Among populations in high-income countries, the annual incidence of new pediatric cancer is 13-16 cases per 100,000 children under the age of 15 with leukemia being the most common diagnosis.[1,2] Children infected with human immunodeficiency virus (HIV) have higher rates of cancer than children who are HIV-uninfected for both HIV-related malignancies and non-HIV-related malignancies.[3,4] Worldwide, approximately 200,000 children and adolescents are diagnosed with cancer every year and 80% of them live in low- and middle-income countries (LMIC).[5] In many LMIC, less than 25% of children with cancer survive, constituting 90% of all pediatric cancer deaths.[6]
The majority of children infected with HIV reside in sub-Saharan Africa (SSA).[7] Individuals with HIV have an estimated 100-fold increased risk of developing Kaposi Sarcoma (KS) or non-Hodgkin lymphoma (NHL) in comparison to individuals who are not HIV-uninfected,[8] earning these cancers the designation of AIDS-defining malignancies.[9–13] KS is associated with co-infection with human herpesvirus-8 (HHV-8) and is the most common HIV-associated malignancy worldwide and the most frequently diagnosed cancer in many African nations.[14–16] NHL is associated with co-infection with Epstein-Barr Virus (EBV) and is the most common malignancy among children throughout many regions of Africa.[17, 18]
There are many challenges to the diagnosis and management of HIV-associated malignancies among children and adolescents in SSA including delayed presentation for care or missed diagnoses.[19, 20] Moreover, there are still many countries in SSA that do not offer cancer services for children.[21] In countries in SSA that offer childhood cancer services, clear consensus treatment guidelines are lacking.[22]
Despite the increased risk of malignancy among children and adolescents with HIV/AIDS, there is a dearth of research on the epidemiology of pediatric KS and NHL in SSA. The lack of national cancer registries, under-reporting, and limited diagnostic capabilities make accurate epidemiological data collection challenging.[23] This review aims to compile currently available incidence and prevalence data on KS and NHL among children and adolescents in SSA and to map geographical burden of disease.
Methods
PubMed and Google Scholar were searched using key words “pediatric,” or “childhood,” “Kaposi sarcoma,” “Burkitt lymphoma” or “Non-Hodgkin lymphoma,” and “Africa” or the respective country name for each of the 48 countries in sub-Saharan Africa. Authors CAR, EMK, and HL evaluated the available literature for documentation of the incidence and prevalence of KS and NHL in SSA among children and adolescents. No restriction was placed on the language of publication, although all included studies were written in English. Only peer-reviewed journals were considered. No attempt was made to identify unpublished studies or conference abstracts, which are often based on preliminary analyses.
Studies were included if they were published between January 1, 1995 and December 31, 2014 and reported KS or NHL incidence or prevalence for children aged 0–18 years in a SSA country. For studies that did not explicitly state prevalence, it was calculated by dividing total cases of KS or NHL by total study population. General pediatric population was defined as including both HIV-infected and HIV-uninfected children and adolescents as some studies did not explicitly state HIV prevalence in their study population. Data were normalized to have a denominator of 100,000 for consistent reporting. Where possible, the text of manuscripts was searched to identify the method of diagnosis. Maps illustrating relative incidence and prevalence were created using ArcGIS version 10.0 (Environmental Systems Research Institute, Redlands, CA, USA).
Results
One hundred and forty-two studies were found to have relevant titles or key words and were evaluated. Twenty-two studies met inclusion criteria. Of the 48 countries in SSA, only 15 (31%) were represented in reports of the epidemiology of KS and NHL among children and adolescents.
Fifteen studies reported epidemiological data for KS (Table I). The median incidence of KS among general pediatric populations was 2.05/100,000 children per year while the median incidence among HIV-infected pediatric populations was 67.35/100,000 children per year. The median prevalence of KS in HIV-infected pediatric populations was 1,513/100,000. There were 16 studies reporting the epidemiology of NHL in SSA (Table II). The median incidence of NHL among the general pediatric population was 1.98/100,000. There were no studies reporting the incidence of NHL among HIV-infected children and adolescents.
TABLE I.
Studies Included in the Review of the Epidemiology of Kaposi Sarcoma Among Children and Adolescents in sub-Saharan Africa.
| Author, Year Published | Study Year(s) | Location | Pediatric Study Sample Size (N) | Incidence of Kaposi sarcoma among children per patient-years | HIV-specific population | Prevalence of Kaposi sarcoma among children | HIV-specific population | Method of Diagnosis |
|---|---|---|---|---|---|---|---|---|
| Mbulaiteye, et al.[24], (2006) | 1989-2002 | Kampala, Uganda | 407 | 160/100,000 | Yes | -- | -- | Not described |
| Chintu, et al.[25], (1995) | 1980-1992 | Lusaka, Zambia | Population estimate | 75.7/100,000 | Yes | 0.04/100,000 | No | Histopathology |
| Rohner, et al.[26], (2014) | 2004-2010 | Southern Africa (Botswana, Malawi, Lesotho, South Africa, Zambia, Mozambique, Zimbabwe) | 13,859 | 59/100,000 | Yes | -- | -- | Both clinical and histopathology |
| Ziegler, et al.[27], (1996) | 1992-1993 | Entebbe, Uganda | Population estimate | 8/100,000 | Yes | -- | -- | Histopathology |
| Parkin, et al.[28], (2010) | 1991-1995 | Kampala, Uganda | Population estimate | 6.26/100,000 | No | -- | -- | Histopathology |
| Wabinga, et al.[29], (2000) | 1991-1997 | Kyadondo County, Uganda | Population estimate | 5.35/100,000 | No | -- | -- | Histopathology |
| Parkin, et al.[28], (2010) | 2002-2006 | Kampala, Uganda | Population estimate | 4.46/100,000 | No | -- | -- | Histopathology |
| Carreira, et al.[30], (2014) | 2009-2010 | Beira, Mozambique | Population estimate | 2.85/100,000 | No | -- | -- | Histopathology |
| Meireles, et al.[31], (2014) | 2007 | Maputo City, Mozambique | Population estimate | 2.05/100,000 | No | -- | -- | Not described |
| Chokunonga, et al.[32], (2014) | 2010-2012 | Harare, Zimbabwe | Population estimate | 1.47/100,000 | No | -- | -- | Both clinical and histopathology |
| Echimane, et al.[33], (2000) | 1995-1997 | Abijan, Ivory Coast | Population estimate | 0.1/100,000 | No | -- | -- | Both clinical and histopathology |
| Makata, et al.[34], (1996) | 1979-1994 | Nakuru, Kisumu, and Eldoret, Kenya | Population estimate | 0.09/100,000 | No | -- | -- | Histopathology |
| Athale, et al.[35], (1995) | 1981-1991 | Lusaka, Zambia | Population estimate | 0.03/100,000 | No | -- | -- | Histopathology |
| Cox, et al.[36], (2013) | 2003-2009 | Lilongwe, Malawi | 2,241 | -- | -- | 3,200/100,000 | Yes | Both clinical and histopathology |
| Tukei, et al.[37], (2011) | 2004-2008 | Kampala, Uganda | 6,530 | -- | -- | 1,513/100,000 | Yes | Histopathology |
| Ahmed, et. al.[38], (2012) | 1998-2007 | Zaria, Nigeria | 885 | -- | -- | 680/100,000 | Yes | Histopathology |
| Median Sample Size* | 2,241 | |||||||
| Median Incidence (General Population) | 2.05/100,000 | N/A | ||||||
| Median Incidence (HIV-infected Population) | 67.4/100,000 | 1,513/100,000 |
Among studies with reported denominators.
TABLE II.
Studies Included in the Review of the Epidemiology of Non-Hodgkin Lymphoma Among Children and Adolescents in sub-Saharan Africa.
| Author, Year Published | Study Year(s) | Location | Pediatric Study Sample Size (N) | Incidence of non-Hodgkin lymphoma among children per patient-years | HIV-specific population | Prevalence of non-Hodgkin lymphoma among children | HIV-specific population | Method of Diagnosis |
|---|---|---|---|---|---|---|---|---|
| Parkin, et al.[28], (2010) | 2002-2006 | Kampala, Uganda | Population estimate | 6.79/100,000 | No | -- | -- | Histopathology |
| Parkin, et al.[28], (2010) | 1991-1995 | Kampala, Uganda | Population estimate | 4.22/100,000 | No | -- | -- | Histopathology |
| Wright, et al.[39], (2009) | 2003-2006 | Northwest Province, Cameroon | Population estimate | 5.9/100,000 | No | -- | -- | Both clinical and histopathology |
| Wabinga, et al.[29], (2000) | 1991-1997 | Kyadondo County, Uganda | Population estimate | 5.57/100,000 | No | -- | -- | Histopathology |
| Lewis, et al.[40], (2012) | 2003-2010 | Northwest Province, Cameroon | Population estimate | 4.54/100,000 | No | -- | -- | Not described |
| Aka, et al.[41], (2012) | 2000-2009 | Mwanza, Tanzania | Population estimate | 4.2/100,000 | No | -- | -- | Clinical |
| Orem, et al.[42], (2007) | 1993-1997 | Kyadondo County, Uganda | Population estimate | 3.9/100,000 | No | -- | -- | Not described |
| Parkin, et al.[43], (1998) | 1980s | Kampala, Uganda | Population estimate | 3.6/100,000 | No | -- | -- | Both clinical and histopathology |
| Parkin, et al.[43], (1998) | 1980s | Blantyre, Malawi | Population estimate | 3.6/100,000 | No | -- | -- | Both clinical and histopathology |
| Ogwang, et al.[44], (2008) | 1997-2006 | Northern Uganda | Population estimate | 2.4/100,000 | No | -- | -- | Cytology or histopathology |
| Rainey, et al.[45], (2007) | 1999-2004 | Kisumu, Kenya | Population estimate | 2.15/100,000 | No | -- | -- | Both clinical and histopathology |
| Parkin, et al.[43], (1998) | 1980s | Ibadan, Nigeria | Population estimate | 1.8/100,000 | No | -- | -- | Both clinical and histopathology |
| Echimane, et al.[33], (2000) | 1995-1997 | Abijan, Ivory Coast | Population estimate | 1.4/100,000 | No | -- | -- | Both clinical and histopathology |
| Orem, et al.[42], (2007) | Not specified | Brazzaville,Congo | Population estimate | 1.1/100,000 | No | -- | -- | Not described |
| Orem, et al.[42], (2007) | 1997-1998 | The Gambia | Population estimate | 0.97/100,000 | No | -- | -- | Not described |
| Chokunonga, et al.[32], (2014) | 2010-2012 | Harare, Zimbabwe | Population estimate | 0.91/100,000 | No | -- | -- | Both clinical and histopathology |
| Mwanda, et al.[46], (2004) | 1997-1999 | Nairobi, Kenya | Population estimate | 0.83/100,000 | No | -- | -- | Histopathology |
| Orem, et al.[42], (2007) | Not specified | South Africa | Population estimate | 0.8/100,000 | No | -- | -- | Not described |
| Rainey, et al.[47], (2007) | 1988-1997 | Nairobi, Kenya | Population estimate | 0.61/100 000 | No | -- | -- | Both clinical and histopathology |
| Parkin, et al.[43], (1998) | 1980s | Namibia | Population estimate | 0.2/100,000 | No | -- | -- | Both clinical and histopathology |
| Makata, et al.[34], (1996) | 1979-1994 | Nakuru, Kisumu, and Eldoret, Kenya | Population estimate | 0.19/100,000 | No | -- | -- | Histopathology |
| Parkin, et al.[43], (1998) | 1980s | Mali | Population estimate | 0.17/100,000 | No | -- | -- | Both clinical and histopathology |
| Tukei, et al.[37], (2011) | 2004-2008 | Kampala, Uganda | 6,530 | -- | -- | 155/100,000 | Yes | Histopathology |
| Chintu, et al.[25], (1995) | 1980-1992 | Lusaka, Zambia | Population estimate | -- | -- | 7.1/100,000 | No | Histopathology |
| Median Incidence (General Population) | 1.98/100,000 |
Figures 1A and 1B illustrate the epidemiology of KS among children and adolescents in SSA from studies evaluated in this review. Figures 2A and 2B display the epidemiology of NHL from the published studies that were reviewed.
Figure 1.
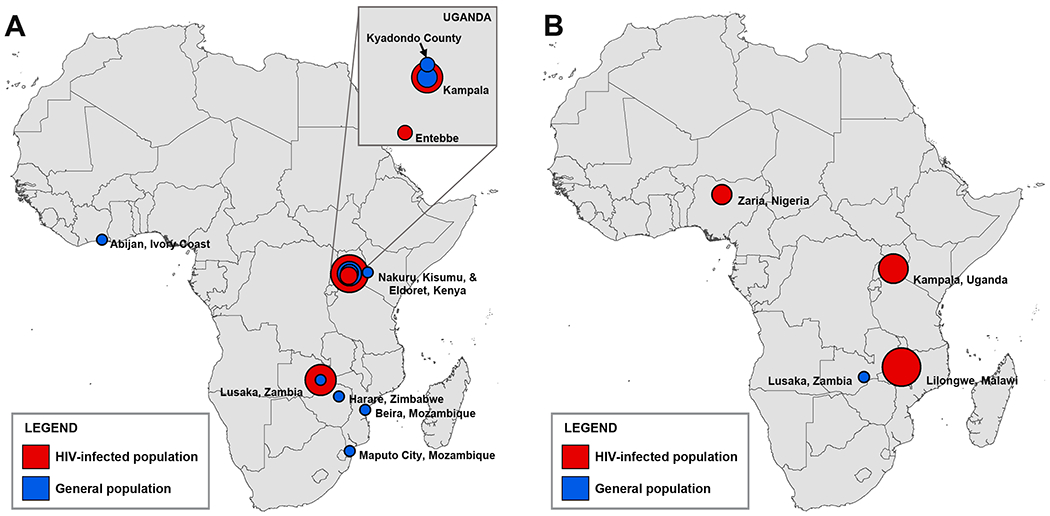
Pediatric Kaposi Sarcoma (KS) incidence (A) and prevalence (B) in sub-Saharan Africa as reported in this review. The size of the symbol indicates the relative size of the estimate, with smaller symbols representing lower relative incidence or prevalence and larger symbols representing higher relative incidence or prevalence. The KS incidence in panel A ranges from 0.03[35] to 160 per 100,000[24]. The KS prevalence in panel B ranges from 0.04[25] to 3,200 per 100,000[36].
Figure 2.
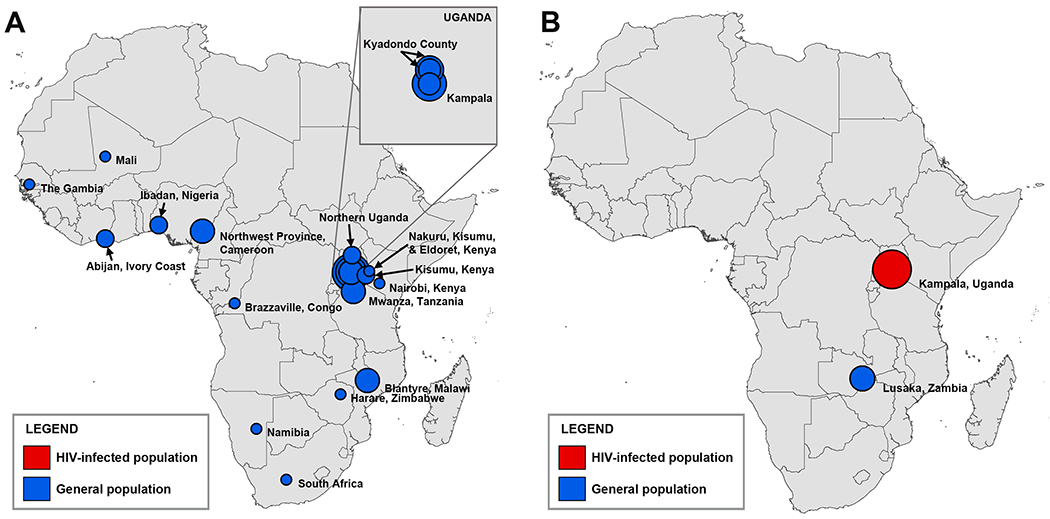
Pediatric Non-Hodgkin Lymphoma (NHL) incidence (A) and prevalence (B) in sub-Saharan Africa as reported in the literature reviewed. The size of the symbol indicates the relative size of the estimate, with smaller symbols representing lower relative incidence or prevalence and larger symbols representing higher relative incidence or prevalence. The NHL incidence in panel A ranges from 0.17[43] to 6.79 per 100,000[28]. The NHL prevalence in panel B ranges from 7.1[25] to 155 per 100,000[37].
Discussion
This review confirmed a paucity of epidemiologic information exists on pediatric KS and NHL in most SSA countries and an absence of epidemiologic data from the countries in SSA with the highest HIV prevalence (i.e., Swaziland, Botswana, and Lesotho).[48] This is consistent with the most recent World Health Organization report on the international incidence of childhood cancer.[43] While other studies have aimed to perform comprehensive analyses of the distribution of malignancies in children in SSA through querying national cancer registries,[17] a comprehensive review of primary literature showing the epidemiology of pediatric KS and NHL in SSA has not been published previously. Countries with low to middle gross domestic product have a higher incidence of cancers associated with infections compared to countries with a high gross domestic product;[49] however, a more precise epidemiology of KS and NHL among children in SSA still remains to be defined.
The expected incidence of all childhood cancers in low-income countries in children less than 15 years of age is 10.2/100,000 patient-years,[17] though this is likely an underestimate due to under-reporting of childhood malignancies. In this review, the median incidence of KS alone was much higher at 67.35/100,000 patient-years among HIV-infected populations, which is similar to the results of a recent abstract which included more than 15,000 children with HIV on antiretroviral therapy (ART) in 15 countries in Africa and found a KS incidence of 67/100,000 patient-years.[50] The incidence found in this review is nearly double the incidence of a study from the South African cohort of the same study group in which the incidence of KS was 34/100,000 patient-years.[51] In a pre-ART study covering parts of Uganda, Tanzania and the Democratic Republic of Congo, the estimated lifetime incidence of KS was as high as 1,600/100,000 patient-years.[52]
This review found a 30-fold increase in the incidence of KS reported among children and adolescents with HIV when compared to the incidence of KS among general pediatric populations in SSA, which is lower than previous estimates.[9] Though thought to be secondary to the increased seroprevalence of HHV-8, uncertainty still surrounds the reasons for the observed increase in the incidence of KS among some equatorial countries in SSA.[53,54] This review supports this finding but also draws attention to the large discrepancy in the incidence of KS among children in this region.
There is compelling evidence from studies of adult populations and predominantly from high-income countries that ART has decreased the incidence of KS and NHL among HIV-infected populations.[55–58] One study from Botswana demonstrated decreased cancer risk with ART expansion, though the median age of patients in that study was 48.[59] Studies predominantly from high-income countries point to decreases in KS and NHL among pediatric HIV-infected populations with the advent of ART.[60, 61] Similarly, this review found that studies published in the 1990s—before the advent of ART in SSA—demonstrated higher rates of KS among children and adolescents when compared to studies published in the 2000s when ART became more widely available on the continent. Moreover, a Ugandan study indicated the incidence of KS in adults decreased with each 10% increase in ART coverage.[62]
There were very few studies reporting the prevalence of NHL among children in SSA. This is likely due to the poor prognosis this diagnosis carries in SSA. NHL in SSA is most often aggressive, and is usually either cured or causes death within the first 12 to 18 months, especially in settings where targeted agents, second line therapies, and stem cell transplant are not available for patients not cured by standard first line therapy.[63] Therefore, it is likely that incidence is a more valuable metric when discussing NHL and could be why incidence is more commonly reported.
Burkitt lymphoma (BL) is the most common childhood cancer and type of NHL in endemic malaria regions in Africa, with a strong association with both malaria and EBV.[64,65] Some literature argues that this endemic form of BL has an estimated incidence as high as 5-10/100,000 patient-years.[66] Despite the expectation of a rising incidence of HIV-associated EBV-driven BL, reports from areas with high endemic BL are split, with a Ugandan study showing a clear association between HIV and endemic BL[65] and another from Malawi failing to show an effect of HIV on BL incidence.[68] In Southern Africa, where malaria is uncommon and EBV-driven sporadic BL predominates,[69] studies have not shown increased incidence of BL in HIV positive children,[25] and one study even showed an increase in overall B-cell lymphomas but a decrease in BL.[70] This is possibly due to BL being common in isolated rural areas of Africa where HIV is less prevalent.[71] However, Bohlius et al. found an incidence of NHL of 31/100,000 patient-years among children with HIV in South Africa,[51] indicating the need for future studies to better characterize BL and overall NHL among HIV-positive children throughout SSA.
Lastly, studies have suggested there is an underreporting of incidence rates of childhood malignancies in SSA, as many challenges to accurate reporting exist. These include lack of symptom recognition, incorrect diagnosis, inaccessibility to appropriate care, and inaccurate data management.[72] While most studies reviewed in this manuscript used histopathology or both clinical diagnosis and histopathology to diagnose HIV-related malignancies, histopathology remains inaccessible in many parts of SSA. A recent study comparing clinical suspicion to histopathologic diagnosis suggests that clinical suspicion of KS is suboptimal and that interpretation of histopathology can be discordant in as much as 31% of cases.[73]
This review is subject to limitations. First, data on KS in children and adolescents in some countries were reported prior to the development of comprehensive pediatric HIV programs and thus may not reflect the current incidence of KS in those locations. In addition, due to limitations in pathological confirmation, absence of pediatric cancer registries, and other causes of mortality, these data underrepresent all cases of pediatric KS and NHL in SSA.
Larger national or regional studies are needed to determine overall burden of disease for pediatric KS and NHL in SSA and to further elucidate the association between geographic location and KS among children. This review highlights the need for more accurate estimates of incidence and prevalence of pediatric KS and NHL and the development of high-quality registries in SSA to survey pediatric malignancies, especially among children with HIV. The authors of this manuscript, as part of the Baylor Pediatric HIV-Related Malignancy Consortium, are conducting an epidemiologic study at five pediatric HIV clinics in SSA to further elucidate the epidemiology of KS and NHL in this region.
Acknowledgements:
none
Abbreviations Key:
- KS
Kaposi sarcoma
- NHL
Non-Hodgkin lymphoma
- SSA
Sub-Saharan Africa
- HIV
Human Immunodeficiency Virus
- AIDS
Acquired Immunodeficiency Syndrome
- HHV-8
Human Herpesvirus-8
- EBV
Ebstein-Barr Virus
- LMIC
Low- and Middle-Income Countries
- ART
Antiretroviral Therapy
- BL
Burkitt Lymphoma
Footnotes
Conflict of Interest statement: the authors have no conflicts of interest.
References
- 1.Kaatsch P Epidemiology of childhood cancer. Cancer Treat Rev 2010;36:277–285. [DOI] [PubMed] [Google Scholar]
- 2.Stack M, Walsh PM, Comber H, Ryan CA, O’Lorcain P. Childhood cancer in Ireland: a population-based study. Arch Dis Child 2007;92:890–897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Patel P, Hanson DL, Sullivan PS, Novak RM, Moorman AC, Tong TC, Holmberg SD, Brooks JT; Adult and Adolescent Spectrum of Disease Project and HIV Outpatient Study Investigators. Incidence of types of cancer among HIV-infected persons compared with the general population in the United States, 1992–2003. Ann Intern Med 2008;148:728–736. [DOI] [PubMed] [Google Scholar]
- 4.Alvaro-Meca A, Micheloud D, Jensen J, Diaz A, Garcia-Alvarez M, Resino S. Epidemiologic trends of cancer diagnoses among HIV-infected children in Spain from 1997 to 2008. Pediatr Infect Dis J 2011;30:764–768. [DOI] [PubMed] [Google Scholar]
- 5.Ribeiro RC, Steliarova-Foucher E, Magrath I, Lemerle J, Eden T, Forget C, Mortara I, Tabah-Fisch I, Divino JJ, Miklavec T, Howard SC, Cavalli F. Baseline status of paediatric oncology care in ten low-income or mid-income countries receiving My Child Matters support: a descriptive study. Lancet Oncol 2008;9:721–729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rodriguez-Galindo C, Friedrich P, Morrissey L, Frazier L. Global challenges in pediatric oncology. Curr Opin Pediatr 2013;25:3–15. [DOI] [PubMed] [Google Scholar]
- 7.World Health Organization. Treatment of children living with HIV. http://www.who.int/hiv/topics/paediatric/en/ Published 2015. Accessed December 8, 2015.
- 8.Mueller BU. HIV-associated malignancies in children. AIDS Patient Care STDS 1999;13:527–533. [DOI] [PubMed] [Google Scholar]
- 9.Mbulaiteye SM, Bhatia K, Adebamowo C, Sasco AJ. HIV and cancer in Africa: mutual collaboration between HIV and cancer programs may provide timely research and public health data. Infect Agent Cancer 2011;6:16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Tanon A, Jaquet A, Ekouevi DK, Akakpo J, Adoubi I, Diomande I, Houngbe F, Zannou MD, Sasco AJ, Eholie SP, Dabis F, Bissagnene E, IeDEA West AfricaCollaboration. The spectrum of cancers in West Africa: associations with human immunodeficiency virus. PloS One 2012;7:e48108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Mbulaiteye SM, Parkin DM, Rabkin CS. Epidemiology of AIDS-related malignancies an international perspective. Hematol Oncol Clin North Am 2003;17:673–696. [DOI] [PubMed] [Google Scholar]
- 12.Gantt S, Kakuru A, Wald A, Walusansa V, Corey L, Casper C, Orem J. Clinical presentation and outcome of epidemic Kaposi sarcoma in Ugandan children. Pediatr Blood Cancer 2010;54:670–674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Casper C The increasing burden of HIV-associated malignancies in resource-limited regions. Annu Rev Med 2011;62:157–170. [DOI] [PubMed] [Google Scholar]
- 14.Phipps W, Ssewankambo F, Nguyen H, Saracino M, Wald A, Corey L, Orem J, Kambugu A, Casper C. Gender differences in clinical presentation and outcomes of epidemic Kaposi sarcoma in Uganda. PloS One 2010;5:e13936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Dal Maso L, Serraino D, Franceschi S. Epidemiology of AIDS-related tumours in developed and developing countries. Eur J Cancer 2001;37:1188–1201. [DOI] [PubMed] [Google Scholar]
- 16.Haverkos HW. Multifactorial etiology of Kaposi’ sarcoma: a hypothesis. J Biosci 2008;33:643–651. [DOI] [PubMed] [Google Scholar]
- 17.Stefan DC. Patterns of distribution of childhood cancer in Africa. J Trop Pediatr 2015;61:165–173. [DOI] [PubMed] [Google Scholar]
- 18.Mostert S, Njuguna F, Kemps L, Strother M, Aluoch L, Buziba G, Kaspers G. Epidemiology of diagnosed childhood cancer in Western Kenya. Arch Dis Child 2012;97:508–512. [DOI] [PubMed] [Google Scholar]
- 19.Stefan DC, Siemonsma F. Delay and causes of delay in the diagnosis of childhood cancer in Africa. Pediatr Blood Cancer 2011;56:80–85. [DOI] [PubMed] [Google Scholar]
- 20.Ekortarl A, Ndom P, Sacks A. A study of patients who appear with far advanced cancer at Yaounde General Hospital, Cameroon, Africa. Psychooncology 2007;16:255–257. [DOI] [PubMed] [Google Scholar]
- 21.Kruger M, Hendricks M, Davidson A, Stefan CD, van Eyssen AL, Uys R, van Zyl A, Hesseling P. Childhood cancer in Africa. Pediatr Blood Cancer 2014;61:587–592. [DOI] [PubMed] [Google Scholar]
- 22.Molyneux E, Davidson A, Orem J, Hesseling P, Balagadde-Kambugu J, Githanga J, Israels T. The management of children with Kaposi sarcoma in resource limited settings. Pediatr Blood Cancer 2013;60:538–542. [DOI] [PubMed] [Google Scholar]
- 23.Valsecchi MG, Steliarova-Foucher E. Cancer registration in developing countries: luxury or necessity? Lancet Oncol 2008;9:159–167. [DOI] [PubMed] [Google Scholar]
- 24.Mbulaiteye SM, Katabira ET, Wabinga H, Parkin DM, Virgo P, Ochai R, Workneh M, Coutinho A, Engels EA. Spectrum of cancers among HIV-infected persons in Africa: the Uganda AIDS-Cancer Registry Match Study. Int J Cancer 2006;118:985–990. [DOI] [PubMed] [Google Scholar]
- 25.Chintu C, Athale UH, Patil PS. Childhood cancers in Zambia before and after the HIV epidemic. Arch Dis Child 1995;73:100–104; discussion 4-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Rohner E, Valeri F, Maskew M, Prozesky H, Rabie H, Garone D, Dickinson D, Chimbetete C, Lumano-Mulenga P, Sikazwe I, Wyss N, Clough-Gorr KM, Egger M, Chi BH, Bohlius J. Incidence rate of Kaposi sarcoma in HIV-infected patients on antiretroviral therapy in Southern Africa: a prospective multicohort study. J Acquir Immune Defic Syndr 2014;67:547–554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ziegler JL, Katongole-Mbidde E. Kaposi’s sarcoma in childhood: an analysis of 100 cases from Uganda and relationship to HIV infection. Int J Cancer 1996;65:200–203. [DOI] [PubMed] [Google Scholar]
- 28.Parkin DM, Nambooze S, Wabwire-Mangen F, Wabinga HR. Changing cancer incidence in Kampala, Uganda, 1991–2006. Int J Cancer 2010;126:1187–1195. [DOI] [PubMed] [Google Scholar]
- 29.Wabinga HR, Parkin DM, Wabwire-Mangen F, Nambooze S. Trends in cancer incidence in Kyadondo County, Uganda, 1960–1997. Br J Cancer 2000;82:1585–1592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Carreira H, Lorenzoni C, Carrilho C, Ferro J, Sultane T, Garcia C, Amod F, Augusto O, Silva-Matos C, La Vecchia C, Lunet N. Spectrum of pediatric cancers in Mozambique: an analysis of hospital and population-based data. Pediatr Hematol Oncol 2014;31:498–508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Meireles P, Albuquerque G, Vieira M, Foia S, Ferro J, Carrilho C, Lunet N. Kaposi sarcoma incidence in Mozambique: national and regional estimates. Eur J Cancer Prev 2015;24:529–534. [DOI] [PubMed] [Google Scholar]
- 32.Zimbabwe Cancer Registry. Cancer Incidence in Harare Triennial Report. 2010-2012. http://afcrn.org/attachments/article/83/ZNCR%202012%20ANNUAL%20REPORT.pdf Published October 2014. Accessed September 10, 2015.
- 33.Echimane AK, Ahnoux AA, Adoubi I, Hien S, M’Bra K, D’Horpock A, Diomande M, Anongba D, Mensah-Adoh I, Parkin DM. Cancer incidence in Abidjan, Ivory Coast: first results from the cancer registry, 1995–1997. Cancer 2000;89:653–663. [DOI] [PubMed] [Google Scholar]
- 34.Makata AM, Toriyama K, Kamidigo NO, Eto H, Itakura H. The pattern of pediatric solid malignant tumors in western Kenya, east Africa, 1979-1994: an analysis based on histopathologic study. Am J Trop Hyg 1996;54:343–347. [DOI] [PubMed] [Google Scholar]
- 35.Athale UH, Patil PS, Chintu C, Elem B. Influence of HIV epidemic on the incidence of Kaposi’s sarcoma in Zambian children. J Acquir Immune Defic Syndr Hum Retrovirol 1995;8:96–100. [PubMed] [Google Scholar]
- 36.Cox CM, El-Mallawany NK, Kabue M, Kovarik C, Schutze GE, Kazembe PN, Mehta PS. Clinical characteristics and outcomes of HIV-infected children diagnosed with Kaposi sarcoma in Malawi and Botswana. Pediatr Blood Cancer 2013;60:1274–1280. [DOI] [PubMed] [Google Scholar]
- 37.Tukei VJ, Kekitiinwa A, Beasley RP. Prevalence and outcome of HIV-associated malignancies among children. AIDS 2011;25:1789–1793. [DOI] [PubMed] [Google Scholar]
- 38.Ahmed A, Bugaje MA, Babadoko AA, Ameh E. Management of AIDS-associated Kaposi’s sarcoma in Nigerian children: a case series and review of literature. J Natl Med Assoc 2012;104:385–389. [DOI] [PubMed] [Google Scholar]
- 39.Wright NJ, Hesseling PB, McCormick P, Tchintseme F. The incidence, clustering and characteristics of Burkitt lymphoma in the Northwest province of Cameroon. Trop Doct 2009;39:228–230. [DOI] [PubMed] [Google Scholar]
- 40.Lewis N, Young J, Hesseling PB, McCormick P, Wright N. Epidemiology of Burkitt’s lymphoma in Northwest Province, Cameroon, 2003-2010. Paediatr Int Child Health 2012;32:82–85. [DOI] [PubMed] [Google Scholar]
- 41.Aka P, Kawira E, Masalu N, Emmanuel B, Brubaker G, Magatti J, Mbulaiteye SM. Incidence and trends in Burkitt lymphoma in northern Tanzania from 2000 to 2009. Pediatr Blood Cancer 2012;59:1234–1238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Orem J, Mbidde EK, Lambert B, de Sanjose S, Weiderpass E. Burkitt’s lymphoma in Africa, a review of the epidemiology and etiology. Afr Health Sci 2007;7:166–175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Parkin DM, Kramarova E, Draper GJ, Masuyer E, Michaelis J, Neglia J, Qureshi S, Stiller CA, eds. (1998) International Incidence of Childhood Cancer vol. 2 IARC Scientific Publications no. 144. Lyon: International Agency for Research on Cancer. [Google Scholar]
- 44.Ogwang MD, Bhatia K, Biggar RJ, Mbulaiteye SM. Incidence and geographic distribution of endemic Burkitt lymphoma in northern Uganda revisited. Int J Cancer 2008;123:2658–2663. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Rainey JJ, Omenah D, Sumba PO, Moormann AM, Rochford R, Wilson ML. Spatial clustering of endemic Burkitt’s lymphoma in high-risk regions of Kenya. Int J Cancer 2007;120:121–127. [DOI] [PubMed] [Google Scholar]
- 46.Mwanda OW, Rochford R, Moormann AM, Macneil A, Whalen C, Wilson ML. Burkitt’s lymphoma in Kenya: geographical, age, gender and ethnic distribution. East Afr Med J 2004(8 Suppl):S68–77. [DOI] [PubMed] [Google Scholar]
- 47.Rainey JJ, Mwanda WO, Wairiumu P, Moormann AM, Wilson ML, Rochford R. Spatial distribution of Burkitt’s lymphoma in Kenya and association with malaria risk. Trop Med Int Health 2007;12:936–943. [DOI] [PubMed] [Google Scholar]
- 48.UNICEF. HIV and AIDS, Eastern and Southern Africa. http://www.unicef.org/esaro/5482_HIV_AIDS.html Accessed September 10, 2015.
- 49.Knaul FM, Adami HO, Adebamowo C, Arreola-Ornelas H, Berger AJ, Bhadelia A, Cleary J, Hunter DJ, Keating N, Mbewu A, Mendez A, Mendez O, Neal C, O’Brien M, Porter P, dos Santos Silva I, Shaheen R, Frenk J. The Global Cancer Divide: an Equity Imperative. In Closing the Cancer Divide: An Equity Imperative. Boston: Harvard University Press; 2012. [Google Scholar]
- 50.Rohner E, Bohlius J. Kaposi sarcoma incidence rate in HIV-infected children on antiretroviral therapy from Southern Africa, Europe and Asia/Pacific [abstract]. In: 10th International Conference on Cancer in Africa; 18-25 November 2015; Marrakech, Morocco Workshop abstract. [Google Scholar]
- 51.Bohlius J, Maxwell N, Spoerri A, Wainwright R, Sawry S, Poole J, Eley B, Prozesky H, Rabie H, Garone D, Technau KG, Maskew M, Davies MA, Davidson A, Stefan DC, Egger M; for the IeDEA-Southern Africa. Incidence of AIDS-defining and other cancers in HIV-postive children in South Africa: record linkage study 2016;[Epub ahead of print]. [DOI] [PMC free article] [PubMed]
- 52.Cook-Mozaffari P, Newton R, Beral V, Burkitt DP. The geographical distribution of Kaposi’s sarcoma and of lymphomas in Africa before the AIDS epidemic. Br J Cancer 1998;78:1521–1528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Dollard SC, Butler LM, Jones AM, Mermin JH, Chidzonga M, Chipato T, Shiboski CH, Brander C, Mosam A, Kiepiela P, Hladik W, Martin JN. Substantial regional differences in human herpesvirus 8 seroprevalence in sub-Saharan Africa: insights on the origin of the “Kaposi’s sarcoma belt”. Int J Cancer 2010;127:2395–2401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Sarmati L HHV-8 infection in African children. Herpes 2004;11:50–53. [PubMed] [Google Scholar]
- 55.Orem J, Otieno MW, Remick SC. AIDS-associated cancer in developing nations. Curr Opin Oncol 2004;16:468–476. [DOI] [PubMed] [Google Scholar]
- 56.Engels EA, Biggar RJ, Hall HI, Cross H, Crutchfield A, Finch JL, Grigg R, Hylton T, Pawlish KS, McNeel TS, Goedert JJ. Cancer risk in people infected with human immunodeficiency virus in the United States. Int J Cancer 2008;123:187–194. [DOI] [PubMed] [Google Scholar]
- 57.Franceschi S, Maso LD, Rickenbach M, Polesel J, Hirschel B, Cavassini M, Bordoni A, Elzi L, Ess S, Jundt G, Mueller N, Clifford GM. Kaposi sarcoma incidence in the Swiss HIV Cohort Study before and after highly active antiretroviral therapy. Br J Cancer 2008;99:800–804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Collaboration of Observational HIV Epidemiological Research Europe (COHERE) Study Group, Bohlius J, Schmidlin K, Costagliola D, Fatkenheuer G, May M, Caro-Murillo AM, Mocroft A, Bonnet F, Clifford G, Karafoulidou A, Miro JM, Lundgren J, Chene G, Egger M. Incidence and risk factors of HIV-related non-Hodgkin’s lymphoma in the era of combination antiretroviral therapy: a European multicohort study. Antivir Ther 2009;14:1065–1074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Dryden-Peterson S, Medhin H, Kebabonye-Pusoentsi M, Seage GR 3rd, Suneja G, Kayembe MK, Mmalane M, Rebbeck T, Rider JR, Essex M, Lockman S. Cancer incidence following expansion of HIV treatment in Botswana. PLoS One 2015;10:e0135602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Chiappini E, Berti E, Gianesin K, Petrara MR, Galli L, Giaquinto C, de Martino M, De Rossi A. Pediatric human immunodeficiency virus infection and cancer in the highly active antiretroviral treatment (HAART) era. Cancer Lett 2014;347:38–45. [DOI] [PubMed] [Google Scholar]
- 61.Simard EP, Shiels MS, Bhatia K, Engels EA. Long-term cancer risk among people diagnosed with AIDS during childhood. Cancer Epidemiol Biomarkers Prev 2012;21:148–154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Mutyaba I, Phipps W, Krantz EM, Goldman JD, Nambooze S, Orem J, Wabinga HR, Casper C. A Population-Level Evaluation of the Effect of Antiretroviral Therapy on Cancer Incidence in Kyadondo County, Uganda, 1999-2008. J Acquir Immune Defic Syndr 2015;69:481–486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Stefan DC. Effect of HIV infection on the outcome of cancer therapy in children. Lancet Oncol 2014;15:e562–567. [DOI] [PubMed] [Google Scholar]
- 64.van den Bosch CA. Is endemic Burkitt’s lymphoma an alliance between three infections and a tumour promoter? Lancet Oncol 2004;5:738–746. [DOI] [PubMed] [Google Scholar]
- 65.Geser A, Brubaker G, Draper CC. Effect of a malaria suppression program on the incidence of African Burkitt’s lymphoma. Am J Epidemiol 1989;129:740–752. [DOI] [PubMed] [Google Scholar]
- 66.Traore F, Coze C, Atteby JJ, Andre N, Moreira C, Doumbe P, Ravelomanana N, Ye D, Patte C, Raquin MA, Raphael M, Lemerle J. Cyclophosphamide monotherapy in children with Burkitt lymphoma: a study from the French-African Pediatric Oncology Group (GFAOP). Pediatr Blood Cancer 2011;56:70–6. [DOI] [PubMed] [Google Scholar]
- 67.Newton R, Ziegler J, Beral V, Mbidde E, Carpenter L, Wabinga H, Mbulaiteye S, Appleby P, Reeves G, Jaffe H; Uganda Kaposi’s Sarcoma Study Group. A case control study of human immunodeficiency virus infection and cancer in adults and children residing in Kampala, Uganda. Int J Cancer 2001;92:622–627. [DOI] [PubMed] [Google Scholar]
- 68.Sinfield RL, Molyneux EM, Banda K, Borgstein E, Broadhead R, Hesseling P, Newton R, Casabonne D, Mkandawire N, Nkume H, Hodgson T, Liomba G. Spectrum and presentation of pediatric malignancies in the HIV era: experience from Blantyre, Malawi, 1998-2003. Pediatr Blood Cancer 2007;48:515–20. [DOI] [PubMed] [Google Scholar]
- 69.Stefan DC, Stones DK, Wainwright D, Kruger M, Davidson A, Poole J, Hadley GP, Forman D, Colombet M, Steliarova-Foucher E. Childhood cancer incidence in South Africa, 1987–2007. S Afr Med J 2015;105:939–947. [DOI] [PubMed] [Google Scholar]
- 70.Davidson A, Hendricks M. Experience with B-cell lymphoma at a South African centre in the HIV Era. Transfus Apher Sci 2013;49:31–39. [DOI] [PubMed] [Google Scholar]
- 71.Kamali A, Carpenter LM, Whitworth JAG, Pool R, Ruberantwari A, Ojwiya A. Seven-year trends in HIV-1 infection rates and changes in sexual behaviour among adults in rural Uganda. AIDS 2000;14:427–434. [DOI] [PubMed] [Google Scholar]
- 72.Howard SC, Metzger ML, Wilimas JA, Quintana Y, Pui CH, Robison LL, Ribeiro RC. Childhood cancer epidemiology in low-income countries. Cancer 2008;112:461–472. [DOI] [PubMed] [Google Scholar]
- 73.Amerson E, Woodruff CM, Forrestel A, Wenger M, McCalmont T, LeBoit P, Maurer T, Laker-Oketta M, Muyindike W, Bwana M, Buziba N, Busakhala N, Wools-Kaloustian K, Martin J. Accuracy of Clinical Suspicion and Pathologic Diagnosis of Kaposi Sarcoma in East Africa. J Acquir Immune Defic Syndr 2015; October 8 [Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]