

Abstract
Objectives.
To determine how individual difference (age, cognition, and hearing) and risk presentation (audio frequency, speed, and organization) variables affect viewing of direct-to-consumer (DTC) prescription drug television ads.
Methods.
Participants (N = 1,075) from four age groups across the adult lifespan took an in-person hearing examination, watched a DTC television ad, and responded to survey questions.
Results.
Increased age was related to reduced cognition and hearing ability, as well as lower ad comprehension and risk recall. Greater speed and more complex organization of the ad’s risk information lowered risk recall and claim recognition. Audio frequency had no effect. Cognitive abilities mediated the relationship between age and risk recall.
Discussion.
Older adults are likely to have more difficulty recalling and understanding the risks presented in DTC television ads. Risk information can be presented in ways that facilitate or inhibit recall and recognition among individuals across the lifespan.
Keywords: direct-to-consumer advertising, risk information, aging, hearing, cognition
Older adults use proportionally more prescription drugs (Kantor, Rehm, Hass, Chan, & Giovannucci, 2015) and watch more television (Depp, Schkade, Thompson, & Jeste, 2010) than their younger counterparts, yielding relatively high exposure levels to direct-to-consumer (DTC) prescription drug promotion. Older adults also face increasing problems with hearing and cognition, although many of these issues are overcome by compensatory strategies (Wingfield & Tun, 2001). Finally, older adults are more likely to experience adverse drug reactions when taking prescription medications (Lavan & Gallagher, 2016). The current paper explores 1) whether variations in promotional content disproportionately affect older adults, for whom prescription drugs are particularly relevant, and 2) the aural and cognitive demands of DTC television promotion.
The communication of information involves, in part, the abilities and motivations of the audience, and the characteristics of the message (Wingfield, McCoy, Peelle, Tun, & Cox, 2006). As people age, they experience decrements in hearing (Gates & Mills, 2005; Lin, 2012) and cognitive abilities (Craik, 2007). Pichora-Fuller and colleagues (2015) note robust associations between hearing, cognitive abilities, and aging in their recent review. For example, older adults often cannot hear high frequency sounds (Arvin, Prepageran, & Raman, 2013), process input in complex situations (Wingfield, Stine, Lahar, & Aberdeen, 1988), or maintain abilities during divided tasks (McDowd & Craik, 1988) as well as younger adults. They also expend more effort to understand speech in background noise (Desjardins & Doherty, 2013; Heyl & Wahl, 2012). Thus, in this study, we expected older individuals to have higher levels of hearing loss and cognitive decline (Hypothesis 1a).
Previous studies have shown that older adults with compromised hearing have difficulty understanding television (Lormore & Stephens,1994; Voeks, Gallagher, Langer, & Drinka, 1993) and those with hearing devices find television noises to be bothersome (Skagerstrand, Stenfelt, Arlinger, & Wikstrom, 2014). Older adults hold several compensatory abilities that improve information processing, such as relying on contextual cues (Pichora-Fuller, 2008; Humes, Burk, Coughlin, Busey, & Strauser, 2007; Wingfield & Tun, 2001); however, these compensatory strategies may not fully eliminate the impacts of hearing and cognitive disparities. Based on the large volume of literature associating aging, hearing loss, and cognitive decline (Gallacher, 2004; Martini, Castiglione, Bovo, Vallesi, & Gabelli, 2014), as well as their effects on processing televised information (Lormore & Stephens,1994; Southwell et al., 2010; Voeks, Gallagher, Langer, & Drinka, 1993), we predict that older individuals will experience lower recall and comprehension of DTC ads compared with younger individuals (Hypothesis 1b).
In addition to individual difference variables, characteristics of television ads themselves likely influence the understanding of information in those ads. DTC ads are unique among television ads because the U.S. Food and Drug Administration (FDA) requires a major statement of the product’s most serious and frequent risks in the audio or the audio and visual components of the ad. For several products, this involves a substantial recitation of medical or technical terms. A recent content analysis (Sullivan, Aikin, & Poehlman, 2017) showed 96% of ads contained at least one medical term in the major statement, with an average of three terms per ad.
Varying the presentation of the major statement, we examined the implications for viewer recall and comprehension of risk information presented auditorily. In this study, we manipulated 1) the audio frequency, 2) the speed, and 3) the organizational complexity of the major statement voiceover. How information is presented in the auditory channel may be particularly relevant to viewers with hearing or cognitive deficits. We operationalized these manipulations in a realistic DTC television ad, which promoted a fictitious high cholesterol medication, “Votrea.” First, we varied the audio frequency of the major statement. The most naturalistic manipulation of auditory frequency in DTC ads is to vary the gender of the speaker because generally female voices have a higher frequency than male voices (Titze, 2000) and advertisers use both.
Past research on comprehension of speech with different frequencies is mixed; a study using all female participants showed that they remembered information better when the voiceover was female rather than male (Glinert & Shommer, 2008), but another study showed that audio frequency had only a small effect on responses to televised alcohol warnings (Slater, Karan, Rouner, & Walters, 2002). Older adults have more difficulty with higher audio frequencies relative to lower frequencies (Arvin et al., 2011). In one study, 8.5% of individuals aged 20a-29 had difficulty hearing high audio frequencies whereas 77% of individuals aged 60-69 had the same difficulty (Agrawal, Platz, & Niparko, 2008). Thus, we predict that older adults will have more difficulty with higher frequencies, represented here by a female voice, than with lower frequencies, represented by a male voice (Hypothesis 2a).
Second, DTC television ads vary in voiceover speed, which often increases when the major statement is read (Sullivan et al., 2017). Among adults over 60 with hearing loss, Jenstad and Souza (2007) found participants’ speech recognition scores were lower in conditions of rapid speech versus normal speech. Wingfield et al. (2006) examined the speech rate of lists of sentences by compressing the sentences to 80%, 65%, and 50% of their regular rate. They found that as speech rate increased, comprehension declined. We manipulated major statement speed by varying how many seconds the major statement voiceover lasted. Based on Wingfield et al., we predicted that viewers would have lower recall and comprehension in the faster version (Hypothesis 2b).
Finally, the major statement in DTC ads can be organized simply or complexly, depending on the ordering and juxtaposition of words and language flow. Sullivan et al. (2017) found 32% of major statements contained passive voice, 18% contained syntactic ambiguity, and 8% contained double negatives, all characteristics that increase speech complexity. Moreover, major statements contained an average of 15.60 words per sentence, 6.68 sentences, and 20.50 risk concepts. Previous researchers have used their own definitions of speech complexity, such as the subject- or object-focus of six-word sentences (Wingfield et al., 2006), or the average number of words per sentence (Letowski & Poch, 1996). Wingfield et al. found that for simple sentences, speed, age, and hearing ability did not reduce comprehension of sentences below 85%. However, for complex sentences, speed, age, and hearing made comprehension more difficult, such that the most compromised group (older adult hearing-impaired individuals at 50% speech compression rate), only understood 50% of the content.
We manipulated the organization of the major statement in the mock DTC ad by varying the sentence structure within the major statement script to be simple versus complex. Based on Wingfield et al. (2006), we predicted that greater organizational complexity would result in lower recall and comprehension (Hypothesis 2c).
In addition to examining individual difference (age, hearing and cognitive abilities) and risk presentation (audio frequency, speed, organizational complexity) variables to determine effects on recall and processing of information in a fictitious DTC prescription drug ad, we also examined their interactions. For example, we expected that higher speeds and more complex organization would interact with age to produce more marked effects in older adult groups (Hypothesis 3).
Finally, because we manipulated the risk information portion of the ad – the major statement –we pursued a mediation analysis to understand participants’ recall of risk information. Specifically, we predicted hearing and cognitive abilities would play a mediating role between age and recall of the risk information in a DTC prescription drug ad Hypothesis 4).
Overall, we investigated numerous factors that may influence the real life DTC viewing experiences of adults across a variety of ages. To examine these questions, we conducted objective hearing evaluations, showed each participant one version of a mock DTC television ad, and measured their memory and perceptions of the ad information.
Method
Participants
Participants were 1,075 individuals evenly distributed across four age groups (18-25 years [Young Adults; YA]; 40-49 years [Middle-aged Adults; MA]; 60-74 years [Young-Old Adults; YO]; 75 years or older [Old-Old Adults; OO]). Participants were excluded if they did not fit into one of the age groups, had health care or marketing backgrounds, had participated in market research interviews in the previous 3 months, participated in the study’s pretest, or did not read and speak English. About half of participants in each of the age groups were male. The percentage of college-educated participants differed across groups: 35.9% in the YA group, 69.6% in the MA group, 59.1% in the YO groups, and 61.0% in the OO group. Finally, the majority of participants in each age group were White: 63.3% in the YA group, 65.9% in the MA group, 78.3% in the YO group, and 93.9% in the OO age group. About 20% of participants in the YA, MA, and YO age groups were Black; only 3% of participants in the OO age group were Black.
Design
This study used a 4 × 2 × 2 × 2 factorial design with factors including the four age groups mentioned above and three characteristics of the major statement voiceover: audio frequency (low vs. high), speed (low vs. high), and organization (simple vs. complex). All manipulations were designed to reasonably mimic what is currently shown in DTC ads (Sullivan et al., 2017). Thus, audio frequency was defined by the gender of the speaker. The major statement was 36-39 seconds in the low speed condition and 26-28 seconds in the high speed condition, depending on complexity. We defined two levels of major statement complexity based on: 1) sentence structure, 2) whether pronouns and antecedents were separated in text, 3) whether words required clarification from later words, and 4) number of commas in a list of words.
Procedure
Data collection occurred at a market research facility in Raleigh, North Carolina during April and May of 2017. After consent procedures, each participant answered one hearing question on a tablet: “Do you feel you have a hearing loss?” (yes, no; Sindhusake et al., 2001). Next, trained audiologists conducted objective hearing tests including otoscopy, visual inspection, and pure-tone testing. Participants removed hearing assistance devices during the hearing test but replaced them before the next part of the assessment. Participants were dismissed if audiologists observed conditions that were likely to affect results (e.g., excessive cerumen) or indicated active infection (e.g., drainage). Hearing was measured for everyone who could have at least one ear tested.
Participants were randomly assigned to watch one of eight versions of a realistic television ad for a fictitious high cholesterol medication, Votrea. The major statement of risks was modeled on existing product ads and contained a series of risks of the fictitious Votrea, including pregnancy and liver disease contraindications, muscle pain, tiredness, and joint pain. Participants watched the ad twice while listening via noise-cancelling headphones. Study staff preset the laptop volume to an average level, but participants could adjust the volume. Participants then completed a survey.
The study received approval from the relevant Institutional Review Boards.
Measures
Hearing ability was measured by audiological examination pure-tone testing. We calculated a hearing score for each ear using the pure tone average (PTA) and high-frequency pure tone average (HPTA) scores according to the gradients described by the World Health Organization (WHO, 2015): (1) no hearing loss: PTA and HPTA are ≤25 dB; (2) mild: PTA or HPTA is 26-40 dB; (3) moderate: PTA or HPTA is 41-60 dB; (4) severe: PTA or HPTA is 61-80 dB; and (5) profound: PTA or HPTA is >81 dB. Our final hearing ability variable reflected hearing in the better ear and was based on the same five WHO gradients.
Only three respondents had profound hearing loss, so we collapsed the last two categories (profound/severe). Higher scores indicate greater hearing loss.
Cognitive ability was measured with the Letter Digit Substitution Test (LDST; van der Elst, van Boxtel, van Breukelen, & Jolles, 2007), a substitution test that relies less on memory. As a whole, substitution tests have been shown to be good indicators of general brain dysfunction and the LDST was validated as a performance indicator of cognitive function (Lezak, 1995; Southwell et al., 2018). Specifically, in two parts, we gave participants 60 seconds to replace 125 randomized letters with appropriate digits as quickly and accurately as possible and recorded the number of correct substitutions. Higher scores indicated greater cognitive ability.
Recall
Risk recall.
We asked participants to list as many side effects as they could remember. We coded responses and summed the number of correct risks listed (0-12 ).
Benefit recall.
We asked participants to list as many benefits as they could remember. We coded responses and summed the number of correct benefits listed (0-2).
Main message recall.
We asked participants what the main message of the ad was. We coded responses as correct when they included any part of the concept that Votrea reduces bad cholesterol to normal levels for people with common risk factors for heart disease (correct/incorrect).
Two trained coders independently coded the open-ended responses for risk, benefit, and main message recall. Intercoder reliability was assessed during the pretest, and all inconsistencies were resolved (Krippendorf’s alpha ≥ .75).
Claim recognition
We listed four claims that were present in the ad (one benefit and three risks), and four claims that were not (three false side effects and “none of the above”), and asked participants to select all claims that were presented in the ad. We created a claim recognition score that ranged from 0 to 4.
Ad comprehension
We listed four statements (one correct and three foils) and asked participants to select the statement that best summarized the information from the ad. The correct item was, “Votrea is a treatment for bad cholesterol, but not all people with bad cholesterol should take Votrea. Votrea has both common and uncommon side effects.” We created a dichotomous variable to reflect correct/incorrect ad comprehension.
Additional Measures
We measured demographic variables of age, sex, race, ethnicity, and education. Although not discussed here, for exploratory purposes we asked questions about risk perceptions, confidence in memory, drug attitudes, behavioral intentions, brand recognition, speech recognition, self-reported hearing loss, and self-reported cognition.
Analysis
First, we assessed the impact of age on hearing ability, using ordinal regression, and on cognitive ability, using ordinary least squared regression. We then conducted several stepwise regressions (ordinary least squares regression for continuous outcomes and logistic regression for dichotomous outcomes) to examine the main effects and interaction effects of age and ad characteristics on recall, claim recognition, and ad comprehension. In the first step of the analysis, we entered the four-category age variable (with OO as the reference group), followed in the second step by the variables related to risk presentation (audio frequency, speed, and major statement organization) and then in the third step by the interactions between age and each of the three ad risk presentation factors. We also explored regression models where step one and two remained the same, but in step three we entered the two-way interactions between audio frequency and speed, audio frequency and major statement organization, and speed and major statement organization respectively, followed by the three-way interaction between the three risk presentation factors in the fourth step. Because none of these interactions were significant, we report only main effects.
Finally, we conducted a path analysis to further understand the relationships between ad characteristics, age, hearing loss, cognitive ability, and risk recall. The analysis followed a two-step approach in which we fit two structural equation models. In the first model, we assessed whether each of the ad characteristics had a main effect on risk recall while at the same time assessing the potential main effect of age and the potential mediation role of hearing and cognitive ability on that age-risk recall relationship (Figure 1). With the second model, we explored the potential moderating role of hearing loss and cognitive ability on the relationships between the three ad characteristics and risk recall by adding moderation paths to the simple model (Figure 2). We tested each model using the robust maximum likelihood estimation method in PROC CALIS (SAS Enterprise Guide Version 7.1) to acknowledge the ordinal nature of the hearing loss variable. We excluded those with missing self-reported age data (n = 11). To assess model fit, we examined the coefficients for Root Mean Square Error of Approximation (RMSEA), Standardized Root Mean Square Residual (SRMR), and Bentler Comparative Fit Index (CFI). We assumed the cutoff for good model fit to be RMSEA < 0.06, SRMR < 0.08 and CFI > 0.95 (Hu & Bentler, 1999). We report the unstandardized coefficients and p-values for the direct, indirect, and moderation effects.
Figure 1.
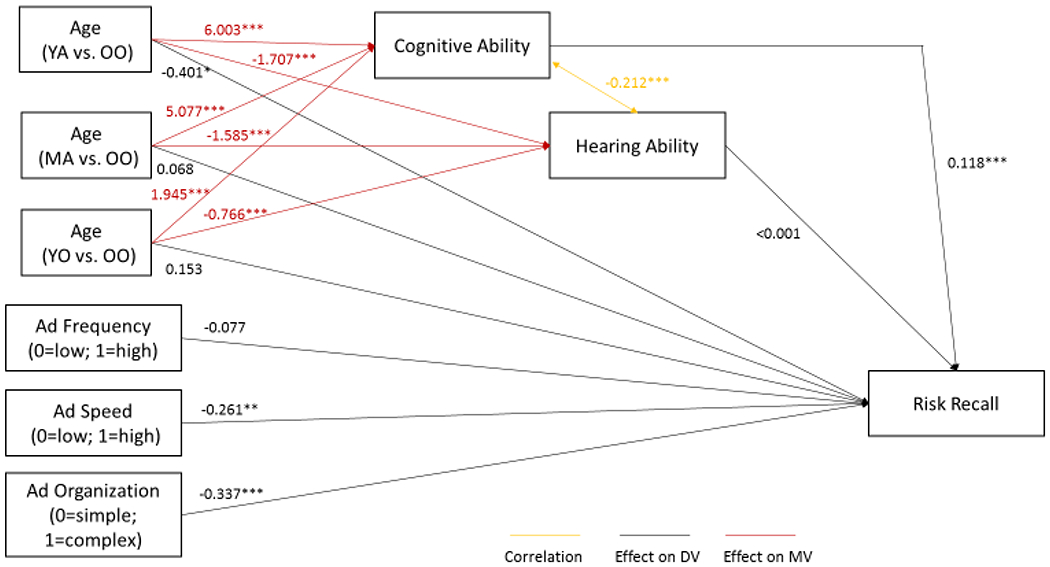
Mediation path between aging and risk recall via hearing loss and cognitive abilities.
Figure 2.
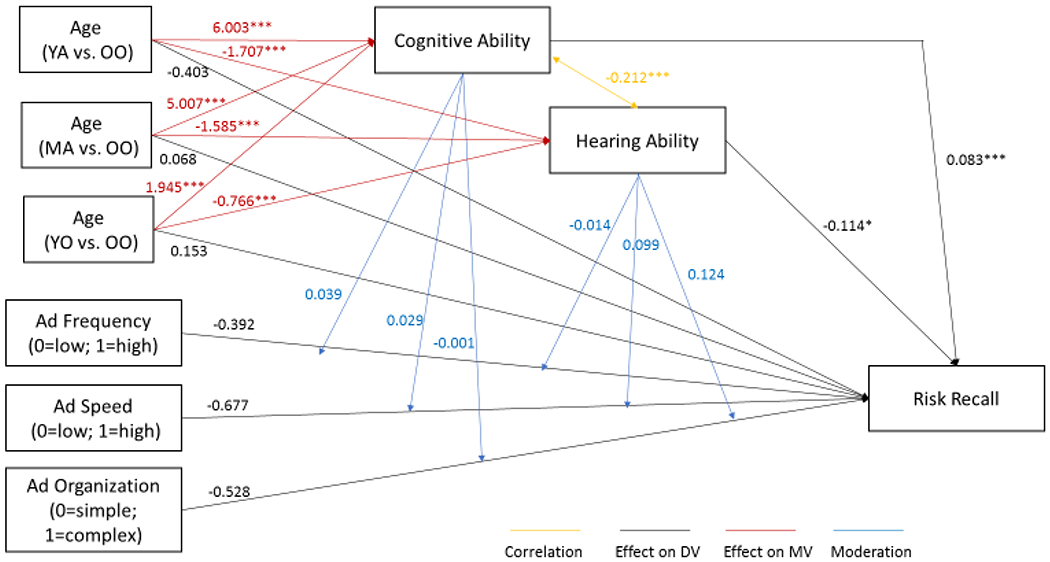
Moderation effects of cognitive and hearing ability on the relationship between age, presentation variables, and risk recall.
Results
We present four sets of results: (1) main effects of age, (2) main effects of ad characteristics, (3) interaction effects of age and ad characteristics and (4) mediation and moderation effects on risk recall.
Main Effects of Age
Hearing ability.
Results supported our hypothesis that as age group increases, hearing ability (measured as hearing loss) decreases, such that hearing ability is lowest among OO adults relative to each other age group (Hypothesis 1a). The ordinal logistic regression yielded a significant effect of age group on hearing ability (X 2= 360.58, p < .001). The planned comparisons revealed that those in the YA age group (odds ratio [OR] = 0.003, p < .001), those in the MA age group (OR = 0.02, p < .001), and those in the YO age group (OR = 0.23, p < .001) were significantly less likely to have hearing loss compared with those in the OO age group. Specifically, 98.2% of those in the YA age group, 98.6% of those in the MA age group, 40.9% of those in the YO age group, and 11.4% of those in the OO age group had no hearing loss.
Cognitive ability.
Results supported our hypothesis that as age group increases, cognitive ability decreases, such that cognitive ability is lowest among OO adults relative to each other age group (Hypothesis 1a). The ANOVA analysis yielded a significant effect of age group on cognitive ability (F(3,1060) = 392.95, p < .001, η2 =.53) such that those in the YA age group (MeanYA [MYA] = 11.48, p < .001, Cohen’s d = 2.76), those in the MA age group (MMA = 10.56, p < .001, Cohen’s d = 2.22), and those in the YO age group (MYO = 7.48, p < .001, Cohen’s d = 0.88) reported significantly greater cognitive ability compared with those in the OO group (MOO = 5.48).
Recall.
We found partial support for our hypothesis that recall decreases as age group increases, such that recall is lowest relative to each other age group (Hypothesis 1b; Table 1). More participants in the MA age group reported main message recall (B = 0.64, SE = 0.27, p=0.015) than in the OO age group. Participants in the YA (B = 0.30, SE = 0.12, p = .015), MA (B = 0.67, SE = 0.12, p < .001) and YO (B = 0.39, SE = 0.12, p = .002) age groups reported significantly higher risk recall compared to those in the OO age group. We did not find significant results for benefit recall.
Table 1.
Outcome Descriptive Statistics by Age Group
| Young Adults (YA) | Middle Aged Adults (MA) | Young-Old Adults (YO) | Old-Old Adults (OO) | |
|---|---|---|---|---|
| n=270 | n=270 | n=269 | n=255 | |
| Mean (SD) | ||||
| Risk recalla | 1.90 (1.52) | 2.26 (1.51) | 1.98 (1.39) | 1.59 (1.28) |
| Benefit recallb | 0.93 (0.47) | 1.04 (0.40) | 1.01 (0.45) | 0.95 (0.37) |
| Claim recognitionc | 2.97 (0.98) | 3.10 (1.00) | 3.10 (1.00) | 3.00 (1.02) |
| n (%) | ||||
| Main message recall | 221 (81.9%) | 244 (90.4%) | 238 (88.5%) | 212 (83.1%) |
| Ad comprehension | 164 (60.7%) | 123 (45.6%) | 112 (42.0%) | 106 (41.6%) |
Possible range from 0 to 12 risks, although no participant recalled more than 7 risks.
Possible range from 0 to 2 benefits.
Possible range from 0 to 4 claims.
Claim recognition and ad comprehension.
We found partial support for our hypothesis that ad comprehension decreases as age group increases, such that claim recognition and ad comprehension are lowest among OO relative to each other age group (Hypothesis 1b; Table 1). Participants in the YA age group reported significantly better ad comprehension compared to those in the OO age group (B = 0.78, SE = 0.18, p < .001). Our claim recognition hypothesis was not supported; participants in the YA, MA and YO age groups did not report significantly different claim recognition compared to participants in the OO age group.
Main Effects of Ad Characteristics
Audio frequency of major statement.
Hypothesis 2a predicted that claim recognition and ad comprehension would be lower after exposure to a major statement using a high-frequency vs. a low-frequency voiceover. We also tested whether recall would be influenced by audio frequency. We found no significant results (Table 2).
Table 2.
Outcome Descriptive Statistics by Ad Characteristics.
| Audio Frequency of Major Statement | Speed of Major Statement | Organization of the Major Statement | ||||
|---|---|---|---|---|---|---|
| Low | High | Low | High | Simple | Complex | |
| n=530 | n=534 | n=525 | n=539 | n=533 | n=531 | |
| Mean (SD) | ||||||
| Risk recalla | 1.97 (1.47) | 1.90 (1.43) | 1.00 (0.42) | 0.96 (0.43) | 0.97 (0.45) | 0.99 (0.40) |
| Benefit recallb | 0.98 (0.43) | 0.99 (0.43) | 2.05 (1.42) | 1.82 (1.46) | 2.10 (1.49) | 1.78 (1.39) |
| Claim recognitionc | 3.05 (0.98) | 3.03 (1.02) | 3.17 (0.92) | 2.91 (1.06) | 3.16 (0.94) | 2.93 (1.04) |
| n (%) | ||||||
| Main message recall | 453 (85.5%) | 462 (86.5%) | 461 (86.5%) | 454 (85.5%) | 452 (86.1%) | 463 (85.9%) |
| Ad comprehension | 248 (46.9%) | 257 (48.2%) | 255 (47.9%) | 250 (47.2%) | 262 (50.0%) | 243 (45.2%) |
Possible range from 0 to 12 risks, although no participant recalled more than 7 risks.
Possible range from 0 to 2 benefits.
Possible range from 0 to 4 claims.
Response options range from 1-not at all confident to 5-extremely confident.
Speed of major statement.
Hypothesis 2b predicted that claim recognition and ad comprehension would be lower after exposure to a major statement using a high-speed vs. a low-speed voiceover. We also tested whether recall would be influenced by speed. Participants in the low-speed voiceover condition reported higher claim recognition (B = 0.26, SE = 0.06, p < .001), and risk recall (B = 0.24, SE = 0.09, p = .01), than those in the high-speed condition. We did not find a significant relationship between speed and ad comprehension, main message recall, or benefit recall (Table 2).
Major statement organization.
Hypothesis 2c predicted that exposure to an ad with a complex organization of the major statement would produce lower recognition, comprehension, and recall relative to an ad with a simple organization of the major statement. Participants in the simple major statement organization condition reported higher claim recognition (B = 0.23, SE = 0.06, p < .001) and higher risk recall (B = 0.32, SE = 0.09, p < .001) than those in the complex major statement organization condition. We did not find a significant relationship between major statement organization and ad comprehension, main message recall, or benefit recall. (Table 2).
Moderation Effects
We did not find a significant moderation effect of age and ad characteristics on any of our outcome variables (Hypothesis 3).
Path Analysis
Mediation modeling.
We hypothesized that hearing and cognitive abilities would mediate the path between aging and the processing of DTC ads, specifically risk recall (Hypothesis 4). We manipulated the major statement of risks in the ads because this information may be critical for individuals who consider discussing a prescription drug with their healthcare providers. Thus, we expected that risk recall would be most affected and we followed up on earlier analyses with a model in which age negatively predicts risk recall via a mediation path involving cognitive ability and in which speed and major statement organization also negatively predict risk recall. This model fit the available data well:RMSEA < 0.01, SRMR = 0.01 and CFI > 0.99 (Figure 1).
Cognitive ability mediated the age-risk recall relationship. Cognitive ability appears to have been a function of age, and cognitive ability also predicted risk recall such that those with higher cognitive ability recalled more risks (B = 0.12, p < .001), controlling for ad frequency, ad organization, ad speed, age and hearing ability. The effect of age on risk recall is partly due to higher cognitive ability among the younger age groups compared to the oldest age group (YA vs. OO indirect effect = 0.71, p < .001; MA vs. OO indirect effect = 0.60, p < .001; YO vs. OO indirect effect = 0.23, p < .001).
Hearing ability did not mediate the effect of age on risk recall, p > .05. Hearing loss and cognitive ability also were negatively related to each other, B = −0.21, p < .001.
Moderation modeling.
When we tried fitting a model indicating moderation of ad characteristic effects as a function of hearing or cognitive ability, fit indices indicated a less than adequate fit with an RMSEA = 0.26, SRMR = 0.05, and CFI = 0.92 (Figure 2). We did not find support for moderation, with p > .05 for all moderation paths.
Discussion
We examined cognitive and hearing abilities across multiple adult age groups and assessed whether these abilities affected the viewing of DTC prescription drug television ads that varied in their presentation of risks. As expected, we found that age was significantly negatively related to cognitive and hearing ability. The oldest older adults tended to drop off significantly in their processing of the information. Although their hearing also declined, our analyses showed that hearing ability was not a guiding factor in this drop off. Cognitive decline played a larger role. Age was also related to main message recall, risk recall, and ad comprehension, such that younger groups tended to recall ad information better compared with the oldest group. Age was not related to claim recognition or benefit recall.
Because older adults tend to take prescription drugs and experience more adverse drug reactions, prescription drug risks are especially relevant for them. We did not assess number of hours of television watching, but based on past research (Depp et al., 2010), it is likely to be relatively high compared with other age groups. The results of our age analyses reveal that, as expected, older adults are likely to have more difficulty recalling the risks presented in DTC television ads. Thus, the communication of risk information in these televised ads to the most elderly individuals may be challenging.
We focused on risk recall in our more advanced analyses because the major statement of risks is what sets DTC ads apart from other product categories and is important for informed decision-making. This, therefore, is also the part of the ad that we manipulated, in three ways: audio frequency, speed, and organization. It is perhaps not surprising that we found no differences in risk recall or ad comprehension whether the risks were read by a male lower frequency voice or a female higher frequency voice, as hearing itself showed no effects. This is consistent with previous research (Slater et al., 2002) and indicates that regulatory resources can be focused elsewhere.
Unlike audio frequency, the speed of the major statement and its organizational complexity impacted how well participants recognized and recalled risk information. As speed and complexity increased, risk information became more difficult to recall. This result is consistent with Wingfield et al. (2006), who demonstrated this effect with six-word sentences. Surprisingly, the effects we observed did not interact with age. Moreover, when we explored a path from these ad characteristics to risk recall, we did not find that cognitive or hearing abilities moderated this relationship. In other words, increased speed and complexity had deleterious effects across the adult lifespan. These findings highlight the importance of pacing the presentation of risk information at a reasonable rate and ensuring that risk information is clear and direct and not confusingly complex.
Note that in the current study we held all other ad aspects, such as the background visuals and superimposed text on the screen, constant. There was no superimposed text on the screen during the major statement and the background visuals were calm and steady, displaying a garden scene. In reality, many DTC television ads include additional stimuli that may affect processing.
When we explored the path from aging effects to risk recall further, we found that cognitive ability, but not hearing ability, mediated the relationship between age and risk recall. This is perhaps not surprising since we allowed individuals to replace their hearing aids before watching the DTC ad, as well as turn up the volume, practices that individuals likely employ when watching television at home. Thus, our findings more realistically represent the effects of hearing loss on DTC television ad viewing. Theoretically, this mediation path – suggesting aging introduces cognitive changes that dampen memory for details at the time of memory encoding – resonates with work on fuzzy-trace theory (e.g., Reyna & Brainerd, 1995; Schneider, 2000; Southwell & Langteau, 2008). Older consumers might generate gist impressions of advertising rather than verbatim detail accounts, which affords them a general sense of ads without all the specific risk details.
Limitations
We did not have a representative sample and thus may be missing the important input of individuals of lower socioeconomic status and varied races and ethnicities. We also only tested one ad, so our findings may not be generalizable beyond the high cholesterol indication. More importantly, our viewing conditions may not have mimicked the natural setting of home television viewing. Participants were seated at desks separated from other individuals, and watched their designated television ad while wearing noise-cancelling headphones. Therefore, we were not able to simulate or account for other distractions that may occur during home viewing (such as other conversation or noise), and in fact eliminated these distractions by using noise-cancelling headphones. Thus, our methods potentially ensured a truer measure of the pure role of hearing in viewing DTC ads, but also may have yielded a conservative estimate of the role hearing plays in real life viewing situations. This is exacerbated by the fact that our mock ads did not contain competing visual information, as some DTC ads do. Future research should examine the influence of the variables in this study with a wider variety of participants and DTC ads and under varying viewing conditions.
Conclusions
Although the studies of cognition and hearing have a rich history in the lifespan literature, this is the first study to apply these findings to DTC prescription drug promotion. Our results show that hearing does not seem to interfere with the processing of the important risk information in these ads, but aging itself does, through the path of cognition. Thus, as age increases, cognitive abilities decline, and the ability to comprehend claims and recall risk information does also. Given that cognitive abilities are known to decrease with age, it is crucial that ads displayed on television, which are frequently viewed by older adults, and especially ads for products directed toward older individuals, convey risk information as clearly as possible.
Independently, we showed that the speed and organizational complexity of the risk presentation impacts participants’ ability to recall and recognize the risk information in these ads. Reducing the speed of the risk presentation and simplifying the organizational complexity resulted in greater risk recall across age groups. Sullivan et al. (2017) showed that the speed of the major statement in DTC ads is significantly faster than the speed in the benefit portion of the ad; our study showed that this matters. Slowing the major statement of risks and reducing its complex sentence structure are concrete approaches to improving the recall of important risk information in DTC ads. Ensuring that individuals of all ages are informed about key aspects of prescription drugs, including the risks, is critical.
References
- Agrawal Y, Platz EA, & Niparko JK (2008). Prevalence of hearing loss and differences by demographic characteristics among U.S. adults. Archives of Internal Medicine, 168, 1522–1530. [DOI] [PubMed] [Google Scholar]
- Arvin B, Prepageran N, & Raman R (2013). “High Frequency Presbycusis”: is there an earlier onset? Indian Journal of Otolaryngology & Head and Neck Surgery, 65(S3), 480–484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Craik FIM (2007). The role of cognition in age-related hearing loss. Journal of the American Academy of Audiologists, 18, 539–547. [DOI] [PubMed] [Google Scholar]
- Depp CA, Schkade DA, Thompson WK, & Jeste DV (2010). Age, affective experience, and television use. American Journal of Preventive Medicine, 39, 173–178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Desjardins JL, & Doherty KA (2013). Age-related changes in listening effort for various types of masker noises. Ear & Hearing, 34, 261–272. [DOI] [PubMed] [Google Scholar]
- Gallacher J (2004). Hearing, cognitive ability, and aging: a critical review. Reviews in Clinical Gerontology, 14, 199–209. [Google Scholar]
- Gates GA & Mills JH (2005). Presbycusis. The Lancet, 366(9491): 1111–1120. [DOI] [PubMed] [Google Scholar]
- Glinert LH, & Schommer JC (2005). Television advertisement format and the provision of risk information about prescription drug products. Research in Social and Administrative Pharmacy, 1, 185–210. [DOI] [PubMed] [Google Scholar]
- Heyl V, & Wahl H (2012). Managing daily life with age-related sensory loss: Cognitive resources gain in importance. Psychology and Aging, 27, 510–521. [DOI] [PubMed] [Google Scholar]
- Hu L, & Bentler PM (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1–55. [Google Scholar]
- Humes LE, Burk MH, Coughlin MP, Busey TA, & Strauser LE (2007). Auditory speech recognition and visual text recognition in younger and older adults: Similarities and differences between modalities and the effect of presentation rate. Journal of Speech, Language, and Hearing Research, 50, 283–303. [DOI] [PubMed] [Google Scholar]
- Jenstad LM, & Souza PE (2007). Temporal envelope changes of compression and speech rate: combined effects on recognition for older adults. Journal of Speech, Language, and Hearing Research, 50, 1123–1138. [DOI] [PubMed] [Google Scholar]
- Kantor ED, Rehm CD, Haas JS, Chan AT, & Giovannucci EL (2015). Trends in prescription drug use among adults in the United States from 1999-2012. Journal of the American Medical Association, 314, 1818–1831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lavan AH, & Gallagher P (2016). Predicting risk of adverse drug reactions in older adults. Therapeutic Advances in Drug Safety, 7, 11–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Letowski T, & Poch N (1996). Comprehension of time-compressed speech: Effects of age and speech complexity. Journal of the American Association of Audiology, 7, 447–457. [PubMed] [Google Scholar]
- Lezak MD (1995). Neuropsychological Assessment (3rd Ed.). New York: Oxford University Press. [Google Scholar]
- Lin FR (2012). Hearing loss in older adults: Who’s listening? Journal of the American Medical Association, 307, 1147–1148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lormore KA, & Stephens SDG 1994. Use of the open-ended questionnaire with patients and their significant others. British Journal of Audiology, 28, 81–89. [DOI] [PubMed] [Google Scholar]
- Martini A, Castiglione A, Bovo R, Vallesi A, & Gabelli C (2014). Aging, cognitive load, dementia, and hearing loss. Audiology and Neurotology, 19(1), 2–5. [DOI] [PubMed] [Google Scholar]
- McDowd JM, & Craik FIM (1988). Effects of aging and task difficulty on divided attention performance. Journal of Experimental Psychology: Human Perception and Performance, 14, 267–280. [DOI] [PubMed] [Google Scholar]
- Pichora-Fuller MK (2008). Use of supportive context by younger and older adult listeners: Balancing bottom-up and top-down information processing. International Journal of Audiology, 47, S72–S82. [DOI] [PubMed] [Google Scholar]
- Pichora-Fuller MK, Mick P, & Reed M (2015). Hearing, cognition, and health aging: social and public health implications of the links between age-related declines in hearing and cognition. Seminars in Hearing, 36(3), 122–139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reyna VF, & Brainerd CJ (1995). Fuzzy-trace theory: An interim synthesis. Learning & Individual Differences, 7, 1–75. [Google Scholar]
- Schneider W (2000). Research on memory development: Historical trends and current themes. International Journal of Behavioral Development, 24, 407–420. [Google Scholar]
- Sindhusake D, Mitchell P, Smith W, Golding M, Newall P, Hartley D, & Rubin G (2001). Validation of self-reported hearing loss. The Blue Mountains Hearing Study. International Journal of Epidemiology, 30, 1371–1378. [DOI] [PubMed] [Google Scholar]
- Skagerstrand A, Stenfelt S, Arlinger S, Wikstrom J (2014). Sounds perceived as annoying by hearing-aid users in their daily soundscape. International Journal of Audiology, 53, 259–269. [DOI] [PubMed] [Google Scholar]
- Slater M, Karan D, Rouner D, & Walters D (2002). Effects of threatening visuals and announcer differences on responses to televised alcohol warnings. Journal of Applied Communication Research, 30, 27–49. [Google Scholar]
- Southwell BG, Gilkerson ND, Depue JB, Shelton AK, Friedenberg LM, & Koutstaal W (2010). Aging and the questionable validity of recognition-based exposure measurement. Communication Research, 37(5), 603–619. [Google Scholar]
- Southwell BG, & Langteau R (2008). Age, memory changes, and the varying utility of recognition as a media effects pathway. Communication Methods and Measures, 2(1–2), 100–114. [Google Scholar]
- Southwell BG, Parvanta SA, Johnson MM, O’Donoghue AC, Sullivan HW, Ray SE, Soloe CS, Davis CN, & McKenna N (2018). Assessing hearing and cognition challenges in consumer processing of televised risk information: Validation of self -reported measures using performance indicators. Preventive Medicine Reports, 11, 145–147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sullivan HW, Aikin KJ, & Poehlman J (2017). Communicating risk information in direct -to-consumer prescription drug television ads: A content analysis. Health Communication, DOI: 10.1080/10410236.2017.1399509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Titze IR (2000). Principles of Voice Production. Iowa City: National Center for Voice and Speech. [Google Scholar]
- van der Elst W, van Boxtel MPJ, van Breukelen GJP, & Jolles J (2007). The Letter Digit Substitution Task: Normative data for 1,858 healthy participants aged 24–81 from the Maastricht Aging Study (MAAS): Influence of age, education, and sex. Journal of Clinical and Experimental Neuropsychology, 28(6), 998–1009. [DOI] [PubMed] [Google Scholar]
- Voeks SK, Gallagher CM, Langer EH, & Drinka PJ (1993). Self-reported hearing difficulty and audiometric thresholds in nursing home residents. The Journal of Family Practice, 36, 54–58. [PubMed] [Google Scholar]
- Wingfield A, McCoy SL, Peelle JE, Tun PA, & Cox LC (2006). Effects of adult aging and hearing loss on comprehension of rapid speech varying in syntactic complexity. Journal of the American Academy of Audiology, 17, 487–497. [DOI] [PubMed] [Google Scholar]
- Wingfield A, Stine EAL, Lahar CJ, & Aberdeen JS (1988). Does the capacity of working memory change with age? Experimental Aging Research, 14, 103–107. [DOI] [PubMed] [Google Scholar]
- Wingfield A & Tun PA (2001). Spoken language comprehension in older adults: Interactions between sensory and cognitive change in normal aging. Seminars in Hearing, 22, 287–301. [Google Scholar]
- World Health Organization. (2015). World Health Organization prevention of blindness and deafness (PBD) program. Prevention of deafness and hearing impaired grades of hearing impairment. Retrieved from http://www.who.int/pbd/deafness/hearing_impairment_grades/en/.