

Abstract
Adenoid hypertrophy is one of the common causes of upper airway obstruction in children. It usually presents with sleep-related breathing disorders and associated findings generally occur around the age of 4 years. However, the development of acute upper airway obstruction due to adenoid hypertrophy is extremely rare. Acute upper airway obstruction due to adenoid hypertrophy in a patient aged under 1 year is an extremely unexpected condition. The aim of this case report was to contribute to the literature by reporting the presence of adenoid hypertrophy causing severe acute airway obstruction leading to endotracheal intubation in a 7-month-old male patient.
Keywords: Adenoids, adenoidectomy, nasopharynx, pediatrics, respiratory insufficiency
Abstract
Adenoid hipertrofisi, çocuklardaki üst havayolu tıkanıklığının en sık görülen sebeplerinden biridir. Genellikle dört yaş civarında, uyku ile ilişkili solunum bozukluğu ve benzeri belirtiler ile ortaya çıkar. Buna karşın, adenoid hipertrofisi nedeniyle akut üst solunum yolu tıkanıklığı görülmesi çok ender bir durumdur. Özellikle bir yaşın altındaki bir hastada bu durumun görülmesi son derece nadirdir. Bu yazının amacı, adenoid hipertrofisi nedeniyle endotrakeal entübasyon gerektirecek kadar ağır akut üst solunum yolu obstrüksiyonu olan yedi aylık erkek hastayı sunarak dizine katkı sağlamaktır.
Introduction
Adenoid tissue and palatine tonsils constitute two of the four parts of Waldeyer’s ring, which is located in the pharyngeus (1). Adenoid tissue growing in response to antigenic stimulus is encountered in early childhood, and gradually tends to shrink after reaching the largest size at an average age of 5 years. Palatine tonsils also grow until an average age of 4 years, due to frequent infections and then begin to shrink (2). Adenoidectomy and tonsillectomy are performed to remove upper airway resistance when adenoid tissue and palatine tonsils are overgrown and cause upper airway obstruction (UAO) findings (1, 2).
Sleep-related breathing disorder accompanied by apnea is one of the definitive indications for adenoidectomy and tonsillectomy (3). Adenoidectomy and tonsillectomy are usually performed in the same operation, but can also be performed at different times. This decision may vary upon the clinical findings of the patient (4). Sleep-related breathing disorder due to adenotonsillar hypertrophy (ATH) is often seen in children aged 4–5 years, because at this age, the adenoid tissue and palatine tonsils have reached their largest size (2). If untreated, ATH can lead to serious conditions such as maxillofacial anomalies, pulmonary hypertension and cor pulmonale, and in extremely rare cases, acute UAO (3).
The aim of this report was to contribute to the literature by presenting and discussing a 7-month-old male patient with adenoid hypertrophy (AH) that led to severe UAO requiring endotracheal intubation, a condition that would not immediately come to mind among the causes of acute UAO in infants aged under one year.
Case
A 7-month-old male patient was referred to the pediatric emergency department with respiratory distress. The respiratory rate was 45 breaths/minute and there was no fever. The patient had severe respiratory distress, inspiratory stridor, and suprasternal withdrawal. On physical examination, the palatine tonsils were observed to be grade 3 hypertrophic but with no active infection, expirium was prolonged, and there was no abnormal heart rhythm, additional sounds or murmur. The arterial blood gas measurements were pH: 7.25, O2SAT: 80%, PCO2: 63.7, PO2: 69.1. Hemoglobin was 11 g/dL on the complete blood count, and the biochemical analysis, electrocardiogram, and posterior-anterior chest radiography were normal. The patient was immediately connected to BiPAP, but endotracheal intubation was urgently performed due to increased respiratory distress and decreased oxygen and increased carbon dioxide. The patient was then transferred to the pediatric intensive care unit (PICU). Informed consent was obtained from the patient’s parents.
When the hemodynamic status stabilized in the PICU, the patient was taken to the operating room and an upper and lower respiratory system examination was performed under general anesthesia. A flexible fiberoptic airway examination revealed adenoid tissue completely filling the nasopharynx, and laryngeal structures were normal (Fig. 1). Bronchoscopy examination showed no pathology such as foreign body, subglottic cyst, web or stenosis that could have led to airway obstruction. Adenoidectomy was performed and the patient was transferred to the PICU (Fig. 2). A dramatic improvement was observed, and the patient was extubated one day after the surgery. After observation for three days in the otorhinolaryngology department, the patient was discharged in a stable condition.
Figure 1.
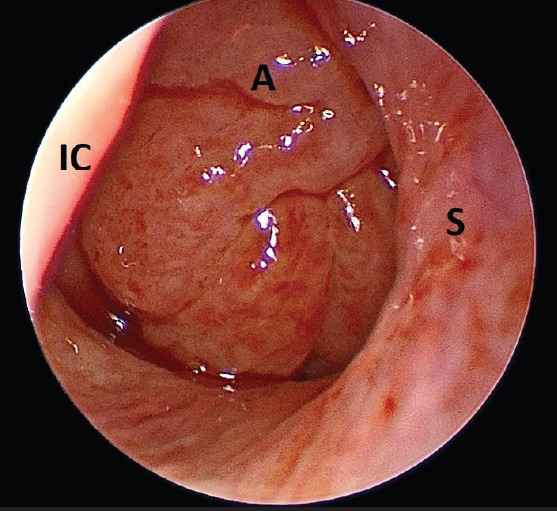
The image shows the adenoid tissue completely filling the nasopharynx on flexible fiberoptic examination of the right nasal cavity. A: Adenoid tissue; IC: Inferior concha; S: Nasal septum
Figure 2.

The image shows the surgical specimen of adenoid tissue approximately 2.5 cm in size
After 6 months without any symptoms, tonsillectomy was planned for the patient because of sleeping with an open mouth, snoring, and obstructive sleep apnea (OSA). Informed consent was obtained from the patient’s parents. At 14 months of age, the patient underwent tonsillectomy and nasopharynx examination under general anesthesia. On flexible fiberoptic examination, there was no adenoid tissue on the nasopharynx (Fig. 3). The patient was transferred to the PICU for postoperative controlled extubation, after which he was monitored in the otorhinolaryngology department, and no complications were observed. The patient was discharged with no complications, and no respiratory distress was observed in the post-operative 6-month follow-up examination.
Figure 3.
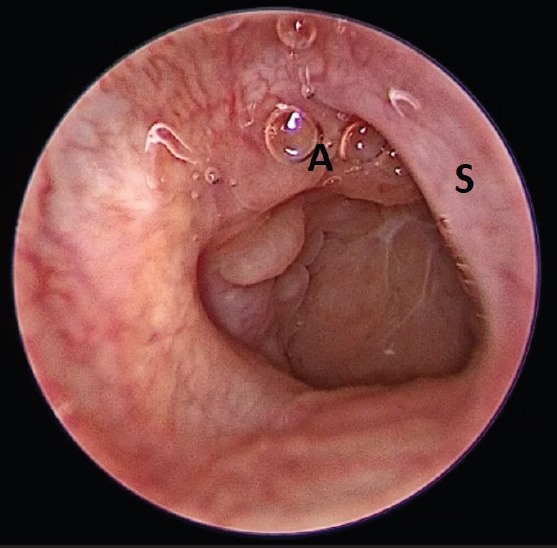
The image shows no adenoid tissue in the nasopharynx on flexible fiberoptic examination of the right nasal cavity. A: Adenoid tissue; S: Nasal septum
Discussion
In the pediatric population, the causes of acute UAO are classified as infectious and non-infectious (5). The most common infectious causes are laryngotracheitis, acute epiglottitis, bacterial tracheitis, laryngeal diphtheria, retropharyngeal abscess, tonsillar/peritonsillar abscess, Ludwig’s angina, and infectious mononucleosis. Non-infectious causes include airway foreign body, angioneurotic edema, airway trauma (penetrating/blunt), airway burns (caustic/thermal), vocal cord paralysis, and vocal cord dysfunction (5). Adenotonsillar hypertrophy as a cause of chronic UAO and acute UAO due to ATH is very rarely seen (6, 7). There is a limited number of articles reporting this condition in the literature.
There are no definitive criteria for emergency adenotonsillectomy (AT). Liang et al. (3) defined the need for urgent AT as severe OSA with associated hypoxemia unresponsive to oxygen. Brouillette et al. (8) used overnight oximetry studies to determine the urgency of AT and children with three or more desaturation events below 80% were considered as having severe OSA. Therefore, they suggested that urgent AT should be performed to these patients within 48 hours of the oximetry study. However, there are no criteria for emergency AT for ATH, which may lead to severe acute UAO requiring endotracheal intubation within hours. In this situation, there is no clear definition in the literature for the timing of surgical intervention.
Sdralis et al. (9) reported that they performed early AT in 17 children with acute UAO due to acute tonsillitis during a 15-year period, and the youngest of these children was aged 13 months old. Coyle et al. (6) reported that emergency hot AT was performed due to difficulty in breathing and desaturations of 77% in a 5-month-old male patient who had been recommended for elective AT for sleep-related breathing disorder at 8 months. In addition, there are reports of severe morbidities developing due to AH. Khirani et al. (10) reported life-threatening OSA caused by AH in an infant with Noonan syndrome. Adenoid hypertrophy alone may not explain the life-threatening OSA in this patient because Noonan syndrome is characterized by distinctive facial deformities, short stature, chest deformity, and congenital heart disease, so these accompanying pathologies may also facilitate the development of respiratory distress in these patients. Following the adenoidectomy, the respiratory disturbance was reported to improve. Malbora et al. (7) reported a 6-year-old male with transient cortical blindness associated with hypercapnia as a result of extremely enlarged adenoid tissue. Urgent AT was performed and no complications or findings such as visual or respiratory disturbances were reported at the 1-month postoperative follow-up examination.
The development of respiratory distress that progresses to endotracheal intubation due to AH in a 7-month-old child is extremely unexpected. The absence of any comorbidities in the patient also makes this case even rarer. To the best of our knowledge, there have been no previous reports of patients under the age of 1 year with similar conditions. It can be considered that the current patient had not sufficiently learned oral respiration due to his young age and that could also have contributed to the severe respiratory complaints.
Adenotonsillar hypertrophy can lead to a spectrum of findings ranging from simple UAO to life-threatening conditions (3, 4, 10). It should always be kept in mind that ATH in children may cause acute UAO.
Footnotes
Informed Consent: Informed consent was obtained from the patient’s parents.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept - U.Y., O.K.; Design - U.Y., E.K.; Supervision - S.A., M.K.; Materials - O.K, S.A.; Data Collection and/or Processing - U.Y., E.K.; Analysis and/or Interpretation - S.A., M.K.; Literature Review - U.Y., E.K.; Writing - U.Y., O.K.; Critical Review - O.K., S.A., M.K.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study has received no financial support.
Hasta Onamı: Hastanın ebeveynlerinden yazılı onam alınmıştır.
Hakem Değerlendirmesi: Dış bağımsız.
Yazar Katkıları: Fikir - U.Y., O.K.; Tasarım - U.Y., E.K.; Denetleme - S.A., M.K.; Malzemeler - O.K, S.A.; Veri Toplanması ve/veya İşlemesi - U.Y., E.K.; Analiz ve/veya Yorum - S.A., M.K.; Literatür Taraması - U.Y., E.K.; Yazıyı Yazan - U.Y., O.K.; Eleştirel İnceleme - O.K., S.A., M.K.
Çıkar Çatışması: Yazarlar çıkar çatışması bildirmemişlerdir.
Mali Destek: Yazarlar bu çalışma için mali destek almadıklarını beyan etmişlerdir.
References
- 1.Bhat VK, Shetty D, Nagaiah PH. Effects of adenoidectomy and adenotonsillectomy on the components of Waldeyer ring. Int J Otorhinolaryngol Head Neck Surg. 2017;3:290–7. [Google Scholar]
- 2.Berlucchi M, Salsi D, Valetti L, Parrinello G, Nicolai P. The role of mometasone furoate aqueous nasal spray in the treatment of adenoidal hypertrophy in the pediatric age group:preliminary results of a prospective, randomized study. Pediatrics. 2007;119:e1392–7. doi: 10.1542/peds.2006-1769. [DOI] [PubMed] [Google Scholar]
- 3.Liang C, Ruiz AG, Jensen EL, Friedman NR. Indications, clinical course, and postoperative outcomes of urgent adenotonsillectomy in children. JAMA Otolaryngol Head Neck Surg. 2015;141:236–44. doi: 10.1001/jamaoto.2014.3341. [DOI] [PubMed] [Google Scholar]
- 4.Darrow DH, Siemens C. Indications for tonsillectomy and adenoidectomy. Laryngoscope. 2002;112:6–10. doi: 10.1002/lary.5541121404. [DOI] [PubMed] [Google Scholar]
- 5.Mandal A, Kabra SK, Lodha R. Upper Airway Obstruction in Children. Indian J Pediatr. 2015;82:737–44. doi: 10.1007/s12098-015-1811-6. [DOI] [PubMed] [Google Scholar]
- 6.Coyle P, Marzouk SD, Gerolympou M, Marais J. Hot tonsillectomy for paediatric obstructive sleep apnoea. BMJ Case Rep 2014. 2014:bcr2013203378. doi: 10.1136/bcr-2013-203378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Malbora B, Malbora N, Avci Z, Olgac A, Erkan AN. A case of transient cortical blindness associated with hypercapnia as a result of extremely enlarged adenoid tissue. Ear Nose Throat J. 2015;94:E14–6. [PubMed] [Google Scholar]
- 8.Brouillette RT, Morielli A, Leimanis A, Waters KA, Luciano R, Ducharme FM. Nocturnal pulse oximetry as an abbreviated testing modality for pediatric obstructive sleep apnea. Pediatrics. 2000;105:405–12. doi: 10.1542/peds.105.2.405. [DOI] [PubMed] [Google Scholar]
- 9.Sdralis T, Berkowitz RG. Early adenotonsillectomy for relief of acute upper airway obstruction due to acute tonsillitis in children. Int J Pediatr Otorhinolaryngol. 1996;35:25–9. doi: 10.1016/0165-5876(95)01278-8. [DOI] [PubMed] [Google Scholar]
- 10.Khirani S, Leboulanger N, Ramirez A, Fauroux B. Life-threatening obstructive sleep apnea caused by adenoid hypertrophy in an infant with noonan syndrome. Case Rep Pediatr. 2012;2012:514514. doi: 10.1155/2012/514514. [DOI] [PMC free article] [PubMed] [Google Scholar]