

Key Points
Question
Are levels of outdoor artificial light at night associated with adolescent sleep patterns and past-year mental disorder?
Findings
In a cross-sectional, nationally representative survey of US adolescents, higher levels of outdoor artificial light at night, measured via satellite, were associated with later weeknight bedtimes; those in the lowest quartile of nighttime light reported the longest weeknight sleep durations. Adolescents in areas with greater levels of nighttime light also had higher prevalence of past-year mood and anxiety disorders.
Meaning
Future studies of adolescent mental and sleep health should consider contextual-level measures of light at night, in addition to individual-level exposure.
This cross-sectional study combines data from satellites and the National Comorbidity Survey–Adolescent Supplement to measure the association of outdoor artificial light at night with self-reported sleep duration and past-year anxiety and mood disorders in adolescents.
Abstract
Importance
Indoor nighttime light exposure influences sleep and circadian rhythms and is known to affect mood-associated brain circuits in animals. However, little is known about the association between levels of nighttime outdoor light and sleep and mental health in the population, especially among adolescents.
Objective
To estimate associations of outdoor artificial light at night (ALAN) with sleep patterns and past-year mental disorder among US adolescents.
Design, Setting, and Participants
This population-based, cross-sectional study of US adolescents used the National Comorbidity Survey–Adolescent Supplement, a nationally representative cross-sectional survey conducted from February 2001 through January 2004. A probability sample of adolescents aged 13 to 18 years was included. Analyses were conducted between February 2019 and April 2020.
Exposures
Levels of outdoor ALAN, measured by satellite, with means calculated within census block groups. ALAN values were transformed into units of radiance (nW/cm2/sr).
Main Outcomes and Measures
Self-reported habitual sleep patterns (weeknight bedtime, weeknight sleep duration, weekend bedtime delay, and weekend oversleep) and past-year mood, anxiety, behavior, and substance use disorders, measured via an in-person structured diagnostic interview. Parent-reported information was included in behavior disorder diagnoses.
Results
Among 10 123 adolescents (4953 boys [51.3%]; mean [SE] age, 15.2 [0.06] years [weighted]; 6483 for behavior disorder outcomes), ALAN was positively associated with indicators of social disadvantage, such as racial/ethnic minority status (median [IQR] ALAN: white adolescents, 12.96 [30.51] nW/cm2/sr; Hispanic adolescents: 38.54 [47.84] nW/cm2/sr; non-Hispanic black adolescents: 37.39 [51.88] nW/cm2/sr; adolescents of other races/ethnicities: 30.94 [49.93] nW/cm2/sr; P < .001) and lower family income (median [IQR] ALAN by family income-to-poverty ratio ≤1.5: 26.76 [52.48] nW/cm2/sr; >6: 21.46 [34.38] nW/cm2/sr; P = .005). After adjustment for several sociodemographic characteristics, as well as area-level population density and socioeconomic status, this study found that higher ALAN levels were associated with later weeknight bedtime, and those in the lowest quartile of ALAN reported the longest weeknight sleep duration. Those in the highest quartile of ALAN went to bed 29 (95% CI, 15-43) minutes later and reported 11 (95% CI, 19-2) fewer minutes of sleep than those in the lowest quartile. ALAN was also positively associated with prevalence of past-year mood and anxiety disorder: each median absolute deviation increase in ALAN was associated with 1.07 (95% CI, 1.00-1.14) times the odds of mood disorder and 1.10 (95% CI, 1.05-1.16) times the odds of anxiety disorder. Further analyses revealed associations with bipolar disorder (odds ratio [OR], 1.19 [95% CI, 1.05-1.35]), specific phobias (OR, 1.18 [95% CI, 1.11-1.26]), and major depressive disorder or dysthymia (OR, 1.07 [95% CI, 1.00-1.15]). Among adolescent girls, differences in weeknight bedtime by ALAN (third and fourth quartiles vs first quartile) were greater with increasing years since menarche (F3, 8.15; P < .001).
Conclusions and Relevance
In this study, area-level outdoor ALAN was associated with less favorable sleep patterns and mood and anxiety disorder in adolescents. Future studies should elucidate whether interventions to reduce exposure to ALAN may positively affect mental and sleep health.
Introduction
Disturbances in daily rhythms of sleep and activity have long been observed in individuals with mental disorders, especially mood disorders.1 This association is thought to be bidirectional, and not simply because of an effect of mental disorder on daily rhythms. For example, prospective high-risk studies have identified sleep disturbances as an early antecedent of bipolar disorder.2 A longitudinal community study of youths demonstrated prospective bidirectional associations between sleep problems and anxiety disorder, with sleep problems associated with subsequent anxiety disorder and vice versa.3 Furthermore, among people with bipolar disorder, disturbances to behavioral rhythms often precede mood episodes,4 and changes in activity levels were found to drive changes in mood over time.5
Daily rhythms are primarily driven by the light-dark cycle, which is the body’s major source of information about the time of day.6 The secretion of melatonin begins at dark and is strongly inhibited by exposure to light. Light is also the primary driver of the innate circadian rhythms of cellular and genetic processes. Light information is transmitted through retinal pathways to the suprachiasmatic nucleus, which acts as the body’s central clock and helps to synchronize peripheral clocks with the environment. It is thought that exposure to light at night increases disease risk by contributing to dysregulation and desynchronization of behavioral and biological daily rhythms.7,8
In 2012, the American Medical Association issued a policy statement9,10 citing concerns about the health outcomes of nighttime lighting, including mood disorders. Multiple lines of evidence support the idea that aberrant light exposure may negatively affect mood. Studies using animal models have shown that light affects depressionlike and anxietylike behaviors and have begun to elucidate neural mechanisms for these outcomes.11,12,13 In addition, human studies measuring exposure to indoor artificial light at night (ALAN) have documented associations with mental health.14,15,16,17 Moreover, light therapy has long been used as a treatment for mood disorder.18,19
In addition to individual-level indoor exposure, exposure to outdoor ALAN at the contextual level may influence mental health. Several community-based and population-based studies have demonstrated associations between outdoor ALAN and sleep patterns.20,21,22,23,24 ALAN has also gained attention as a risk factor for chronic diseases, particularly cancer and obesity.20,25,26 To our knowledge, only 1 prior study27 has focused on the association between outdoor ALAN and mental health at the population level. This study, conducted among a representative sample of South Korean adults, showed that those living in districts with higher levels of outdoor ALAN were more likely to report depressive symptoms and suicidal ideation or attempt.27 In the current study, we leverage data from a nationally representative sample of US adolescents to estimate associations of outdoor ALAN with sleep patterns and mental disorder, including broad disorder classes as well as individual disorders, in the past year. We focus on adolescents because of evidence that mental disorders commonly emerge during adolescence28 and evidence from animal studies that indicates that early exposure to ALAN may have long-lasting effects.29,30 As a secondary aim, we assessed whether associations differed by sex and age (among adolescent boys) or pubertal maturation (among adolescent girls).31,32
Methods
Sample
We used data from the National Comorbidity Survey–Adolescent Supplement (NCS-A), a nationally representative cross-sectional survey of adolescents residing in the contiguous US that was conducted from February 2001 through January 2004.33 A complex sampling design with dual household and school sampling frames was used. Adolescents in the NCS-A were sampled from across the US, from the same counties as adults in the NCS–Replication, a nationally representative survey of US adults.34 A total of 10 123 adolescents aged 13 to 18 years participated, with an overall response rate of 75.6%. In-person interviews assessing mental disorders and a range of individual, familial, and contextual characteristics were administered in adolescents’ homes by trained lay interviewers.35 In addition, parents or guardians were mailed a parent self-administered questionnaire (PSAQ), data from which are available for 6483 adolescents. The NCS-A’s procedures were approved by the human subjects committees of Harvard Medical School and the University of Michigan. Written informed consent and assent were obtained from parents and adolescents, respectively. This study was determined not human subjects research by the National Institutes of Health Office of Institutional Review Board Operations.
Measures
Mental Disorder
Mental disorders were assessed during in-person interviews using a modified version of the World Health Organization Composite International Diagnostic Interview version 3.0, a fully structured, lay-administered instrument that generates psychiatric diagnoses according to DSM-IV criteria.35,36,37 Here we considered 4 broad classes of past-year mental disorder: mood (major depressive disorder, dysthymia, and bipolar I and II disorders), anxiety (agoraphobia without panic, specific phobia, social phobia, generalized anxiety disorder, panic disorder, posttraumatic stress disorder, and separation anxiety disorder), substance use (alcohol and drug abuse and dependence), and behavior (conduct disorder, oppositional defiant disorder, and attention-deficit/hyperactivity disorder). Mood, anxiety, and substance use disorder diagnoses were based on adolescent interviews alone. To maximize validity, diagnoses of conduct disorder and oppositional defiant disorder were based on both adolescent and parent reports, combined using an or rule at the symptom level, while diagnoses of attention-deficit/hyperactivity disorder were based on parent reports alone.38,39
Sleep Patterns
During the interview, adolescents were asked what time they usually go to bed on weeknights and weekends, and how many hours of sleep they usually get on weeknights and weekends. From this, we derived 4 sleep patterns: weeknight bedtime, weeknight sleep duration, weekend bedtime delay (weekend bedtime minus weeknight bedtime), and weekend oversleep (weekend sleep duration minus weeknight sleep duration). The first 2 measures captured mean sleep patterns, while the second 2 captured day-to-day variability in sleep patterns. These patterns have been studied previously in association with mental health and contextual exposures in the NCS-A.40,41,42
Adolescent-reported sleep patterns contained anomalous reports that were likely spurious (eg, a weekend sleep duration of 24 hours). To mitigate the influence of spurious reports, observations outside of 3 SDs were omitted prior to calculating sleep patterns (weeknight bedtime: 223 individuals; weeknight sleep duration: 62 individuals; weekend bedtime: 400 individuals; weekend sleep duration: 63 individuals). Total rates of missingness were 2.5% (n = 252) for weeknight bedtime, 1.0% (n = 105) for weeknight sleep duration, 7.1% (n = 719) for weekend bedtime delay, and 2.3% (n = 233) for weekend oversleep. The larger proportion of missingness for weekend bedtime delay was in part because of omission of observations from 251 adolescents who reported going to bed at noon on weekends. Sensitivity analyses that (1) included all reports and (2) recoded bedtimes of noon as midnight did not meaningfully change the results and are presented in the eTable 3 and eTable 4 in the Supplement.
Outdoor ALAN
Outdoor ALAN information was derived from satellite imagery data maintained by the National Oceanic and Atmospheric Administration’s Earth Observation Group.43 Data are from the US Defense Meteorological Satellite Program’s Operational Linescan System Nighttime Lights Time Series, which provides annual composite estimates based on continuous sampling of the Earth’s surface with daily global coverage. These composites are based on observations that exclude clouds, sunlight, moonlight, glare, and brief events, such as fires.44 We used the Defense Meteorological Satellite Program Global Radiance Calibrated Nighttime Lights high-dynamic range data, which captures increased variability within urban and suburban areas.45 Data were from the year 2000 and available at a resolution of approximately 1 km2. Mean ALAN levels for each census block group in the US according to the 2000 decennial census were calculated using ArcGIS (ESRI). ALAN values were transformed into units of radiance (nW/cm2/sr). This information was linked to participants in the NCS-A based on their census block group of residence. A census block group is a subdivision of a census tract, contains between 600 and 3000 people, and is the smallest geographical unit for which the US census collects sample data.
Covariates
Individual-level covariates included age, sex, race/ethnicity, parental education, number of siblings, number of biological parents, family income-to-poverty ratio, and immigrant generation. All covariates were categorized as in Table 1, except for age, which was modeled continuously. Area-level covariates included county-level urbanicity, region, population density, and socioeconomic status (SES). Population density (people/km2) was from the 2000 US census at the block group level. Census tract-level SES was measured using an index46 that has been used in large epidemiologic studies and applied previously in the NCS-A.47 It is derived from 6 indicators (median household income; percentage of households receiving interest, dividend, or rental income; median value of owner-occupied housing units; percentage of adults 25 years and older who completed high school; percentage of adults 25 years and older who completed college; and percentage of the persons 16 years and older with employment who held executive, managerial, or professional occupations; Table 1) that are standardized and summed to create a normally distributed summary score. Forty-eight adolescents (0.5%) lived in census tracts with missing SES indicators. Age at menarche was assessed among adolescent girls by self-report and subtracted from current age to derive years since menarche as a measure of pubertal maturation.
Table 1. Median and Interquartile Range of Outdoor Artificial Light at Night, by Participant, Family, and Area-Level Characteristicsa.
| Characteristic | No. (%) | Light at night, nW/cm2/sr, median (IQR) | P value |
|---|---|---|---|
| Age, y | |||
| 13 | 1652 (15.2) | 18.10 (42.55) | .14 |
| 14 | 2218 (21.0) | 24.08 (43.07) | |
| 15 | 1887 (20.5) | 18.68 (36.70) | |
| 16 | 2010 (21.0) | 19.62 (37.67) | |
| 17 | 1758 (16.8) | 24.13 (41.08) | |
| 18 | 598 (5.4) | 29.15 (42.09) | |
| Sex | |||
| Female | 5170 (48.8) | 21.84 (40.40) | .49 |
| Male | 4953 (51.3) | 20.80 (40.27) | |
| Race/ethnicity | |||
| Hispanic | 1914 (14.4) | 38.54 (47.84) | <.001 |
| Non-Hispanic black | 1953 (15.1) | 37.39 (51.88) | |
| Other race/ethnicity | 622 (5.0) | 30.94 (49.93) | |
| Non-Hispanic white | 5634 (65.6) | 12.96 (30.51) | |
| Urbanicity | |||
| Metropolitan | 4508 (47.5) | 37.35 (47.80) | <.001 |
| Other urban | 3304 (37.6) | 13.95 (27.82) | |
| Nonurban | 2311 (14.9) | 2.12 (3.74) | |
| Region | |||
| Northeast | 1868 (18.1) | 33.34 (75.18) | <.001 |
| Midwest | 2776 (23.3) | 23.57 (37.56) | |
| South | 3434 (36.0) | 10.79 (28.91) | |
| West | 2045 (22.6) | 28.96 (46.78) | |
| Parental education | |||
| Less than high school | 1684 (15.5) | 29.97 (55.71) | <.001 |
| High school graduation | 3081 (29.7) | 16.32 (44.11) | |
| Some college | 1998 (19.4) | 21.87 (41.02) | |
| College graduation | 3360 (35.3) | 19.84 (31.20) | |
| Family income-to-poverty ratio | |||
| ≤1.5 | 1717 (14.7) | 26.76 (52.48) | .005 |
| >1.50 to ≤3 | 2023 (19.1) | 23.23 (44.98) | |
| >3.0 to ≤6 | 3101 (31.9) | 17.96 (38.69) | |
| >6 | 3282 (34.3) | 21.46 (34.38) | |
| No. of biological parents | |||
| 0 | 971 (9.3) | 22.07 (40.89) | <.001 |
| 1 | 3797 (35.7) | 25.61 (46.35) | |
| 2 | 5355 (55.0) | 18.48 (36.60) | |
| No. of siblings | |||
| 1 | 483 (5.5) | 21.51 (42.36) | <.001 |
| 2 | 2569 (28.4) | 18.67 (37.59) | |
| 3 | 2633 (26.5) | 20.13 (38.25) | |
| ≥4 | 4438 (39.6) | 24.06 (44.46) | |
| Nativity | |||
| Not born in US | 591 (6.5) | 40.49 (45.00) | <.001 |
| 1 or 2 Parents not born in US | 1533 (13.4) | 33.30 (51.16) | |
| 1 to 4 Grandparents not born in US | 1298 (13.3) | 27.01 (43.89) | |
| Other | 6701 (66.8) | 14.58 (34.09) | |
| Area-level SES score quintile | |||
| First (lowest) | 2015 (16.5) | 41.74 (57.24) | <.001 |
| Second | 2025 (20.1) | 13.86 (43.69) | |
| Third | 2006 (19.4) | 7.96 (35.57) | |
| Fourth | 2022 (20.5) | 18.45 (31.71) | |
| Fifth (highest) | 2007 (23.5) | 24.07 (27.12) | |
| Area-level population density quintile | |||
| First (lowest) | 2026 (19.0) | 1.78 (1.33) | <.001 |
| Second | 2023 (20.6) | 7.20 (8.96) | |
| Third | 2025 (20.2) | 24.76 (21.26) | |
| Fourth | 2024 (20.5) | 36.60 (28.03) | |
| Fifth (highest) | 2025 (19.8) | 68.15 (52.02) |
Abbreviations: IQR, interquartile range; SES, socioeconomic status.
Artificial light at night is measured in nanowatts. The P values are from F tests from binary and multinomial logistic regressions with demographic characteristics as the dependent variables and light at night as the independent variable. Area-level SES scores were derived from 6 census indicators: median household income; percentage of households receiving interest, dividend, or rental income; median value of owner-occupied housing units; percentage of adults 25 years or older who completed high school; percentage of adults 25 years or older who completed college; and percentage of persons 16 years and older with employment who are in executive, managerial, or professional occupations.
Statistical Analysis
First, we estimated the median and interquartile range (IQR) of ALAN by sociodemographic characteristics. Second, we estimated associations between ALAN and sleep patterns using linear regression. ALAN was modeled in quartiles to allow for nonlinearity. Third, we used binary and multinomial logistic regression to estimate odds ratios (ORs) and 95% CIs for the associations between ALAN and past-year mental disorder classes. ALAN was modeled as continuous in these models, as exploratory analyses revealed that apparent nonlinearity was attributable to the most extreme values of ALAN. ALAN was standardized using the median absolute deviation from the median.48 Fourth, where associations with disorder classes were observed, we performed post hoc analyses to identify associations with individual disorders. Multinomial logistic regression was used to compare each disorder of interest with a consistent reference group while accounting for associations with other disorders. Three levels of model adjustment were used: age and sex only (model 1), additional adjustment for all sociodemographic covariates (model 2), and additional adjustment for continuous area-level SES and quadratic population density (model 3). Fifth, for outcomes of sleep patterns and mental disorder classes, we performed post hoc analyses testing for interactions of ALAN with sex and age (among adolescent boys) or years since menarche (among adolescent girls), by adding multiplicative interaction terms to model 3. Finally, we performed a sensitivity analysis controlling for season of interview. Analyses accounted for the complex sampling design and survey weights.49 Variances were estimated using Taylor series linearization. Because of the relatively low rates of missingness, missing data were handled via model-wise deletion. Analyses were conducted using SAS version 9.4 (SAS Institute) from February 2019 to April 2020.
Results
A total of 10 123 adolescents aged 13 to 18 years participated (4953 boys [51.3%]; 5634 non-Hispanic white individuals [65.6%]; mean [SE] age, 15.2 [0.06] years [weighted]), with data from the parent self-administered questionnaire available for 6483 adolescents. Median values of ALAN, by individual and area-level characteristics, are presented in Table 1. Levels of ALAN differed according to every covariate except age and sex. ALAN levels were lowest for non-Hispanic white adolescents (median [IQR], 12.96 [30.51] nW/cm2/sr; vs Hispanic adolescents: 38.54 [47.84] nW/cm2/sr; non-Hispanic black adolescents: 37.39 [51.88] nW/cm2/sr; adolescents of other races/ethnicities: 30.94 [49.93] nW/cm2/sr; P < .001), increased monotonically with urbanicity (nonurban: 2.12 [3.74] nW/cm2/sr; other urban: 13.95 [27.82] nW/cm2/sr; metropolitan: 37.35 [47.80] nW/cm2/sr; P < .001), and were highest in the Northeast (33.34 [75.18] nW/cm2/sr vs the Midwest: 23/57 [37.56] nW/cm2/sr; South: 10.79 [28.91] nW/cm2/sr; and West: 28.96 [46.78] nW/cm2/sr; P < .001). ALAN levels also differed by adolescent socioeconomic characteristics (eg, median [IQR] by family income-to-poverty ratio ≤1.5: 26.76 [52.48] nW/cm2/sr; >6: 21.46 [34.38] nW/cm2/sr; P = .005), family structure (eg, median [IQR] by number of biological parents: 0, 22.07 [40.89] nW/cm2/sr; 2, 18.48 [36.60] nW/cm2/sr; P < .001), and area-level SES (median [IQR]: first [lowest] quintile, 41.74 [57.24] nW/cm2/sr; fifth [highest] quintile, 24.07 [27.12] nW/cm2/sr; P < .001) and population density (median [IQR]: first [lowest] quintile, 1.87 [1.33]; fifth [highest] quintile, 68.15 [52.02]) (Table 1).
The Figure and eTable 1 in the Supplement show associations between quartiles of ALAN and sleep patterns. Adjusting for age and sex (model 1), ALAN was associated with weeknight bedtime (mean differences from lowest quartile of ALAN: second quartile, 14.47 [95% CI, 8.07-20.87] minutes; third quartile, 23.16 [95% CI, 15.33-31.00] minutes; highest quartile, 28.56 [95% CI, 18.82-38.30] minutes; P < .001), weeknight sleep duration (mean differences from lowest quartile of ALAN: second quartile, −17.24 [95% CI, −23.04 to −11.44] minutes; third quartile, −12.71 [95% CI, −19.29 to −6.13] minutes; highest quartile, −8.77 [95% CI, −15.29 to −2.24] minutes; P < .001), and weekend oversleep (mean differences from lowest quartile of ALAN: second quartile, 22.87 [95% CI, 10.73-35.00] minutes; third quartile, 23.31 [95% CI, 12.24-34.38] minutes; highest quartile, 14.50 [95% CI, 1.66-27.35] minutes; P < .001). Further adjustment for sociodemographic covariates reduced the magnitude of association with sleep duration (mean differences from lowest quartile of ALAN: second quartile, −13.65 [95% CI, −19.78 to −7.51] minutes; third quartile, −9.05 [95% CI, −15.58 to −2.52] minutes; highest quartile, −5.34 [95% CI, −13.60 to 2.93] minutes; P < .001) and removed the association with weekend oversleep. Under full adjustment (model 3), bedtime was progressively later as the quartile of ALAN increased; those in the highest quartile of ALAN went to bed 29 (95% CI, 15-43) minutes later than those in the lowest quartile. Sleep duration was shorter among those in the 3 highest quartiles of ALAN compared to the lowest quartile; those in the highest quartile of ALAN reported 11 (95% CI, 2-19) fewer minutes of sleep than those in the lowest quartile.
Figure. Adjusted Mean Sleep Patterns by Quartiles of Outdoor Artificial Light at Night Among US Adolescents.
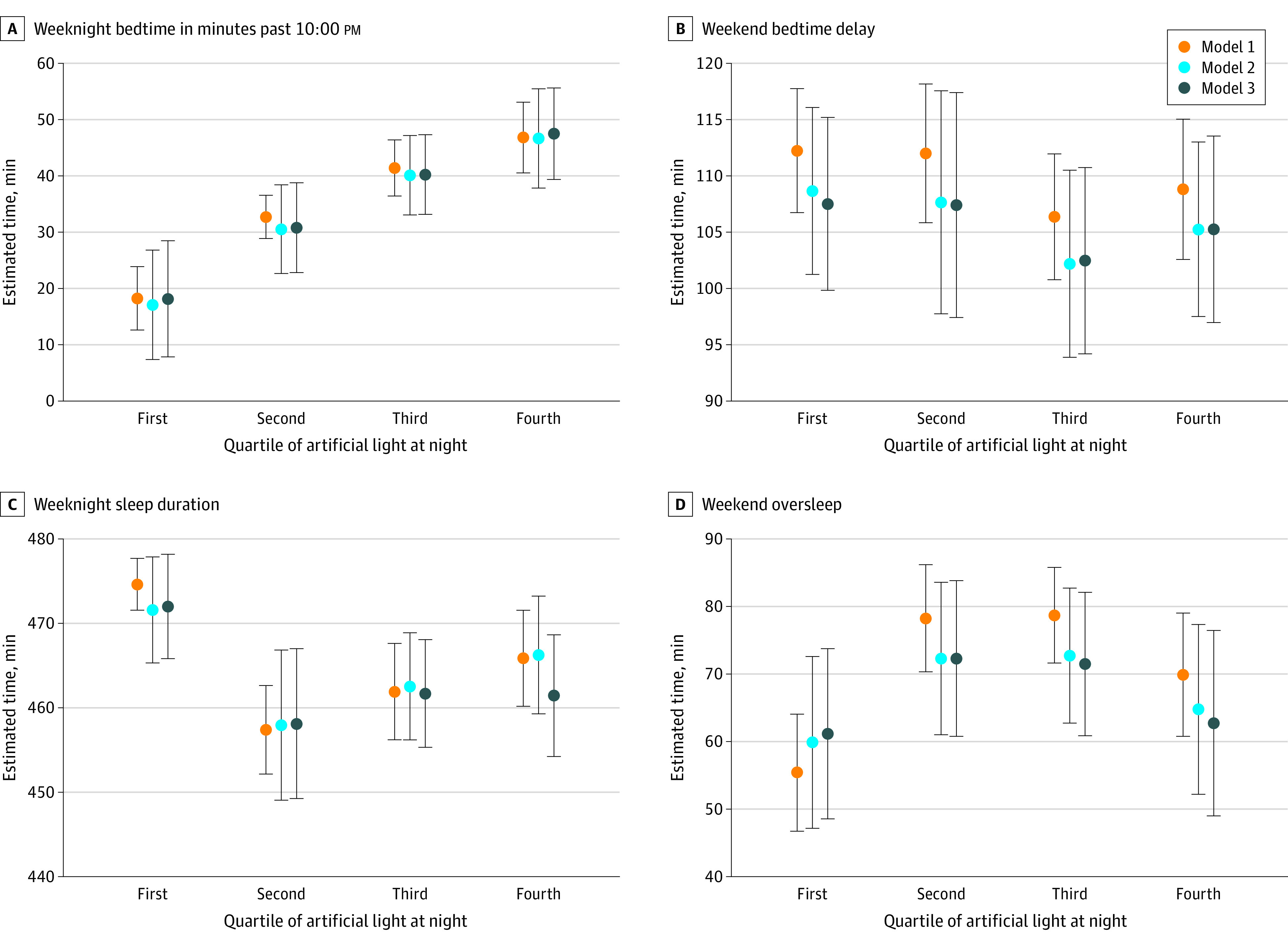
Weeknight bedtime is in minutes past 10:00 pm. Model 1 is adjusted for age and sex. Model 2 is additionally adjusted for race/ethnicity, family income, parental education, family structure, nativity, region, and urbanicity. Model 3 is additionally adjusted for census block group–level population density and census tract–level socioeconomic status. Sample sizes reflect those in eTable 1 in the Supplement. Forty-eight adolescents missing values for area-level socioeconomic status were not included in model 3. In model 3, artificial light at night was associated with weeknight bedtime and weeknight sleep duration (eTable 1 in the Supplement). Mean weeknight bedtime differed significantly between all quartiles of artificial light at night. Mean sleep duration did not differ significantly between the second through fourth quartiles of artificial light at night.
Associations between continuous ALAN and the 4 classes of past-year mental disorder are presented in Table 2. ALAN was positively associated with mood and anxiety disorder under all 3 adjustments. Adjusting for all covariates, each median absolute deviation increase in ALAN was associated with 1.07 (95% CI, 1.00-1.14) times the odds of mood disorder and 1.10 (95% CI, 1.05-1.16) times the odds of anxiety disorder.
Table 2. Associations Between Outdoor Artificial Light at Night and Classes of Mental Disorder in the Past Year Among Adolescentsa.
| Disorder class | Participants, No. | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|---|
| OR (95% CI)b | P value | OR (95% CI)c | P value | OR (95% CI)d | P value | ||
| Mood | 1021 | 1.09 (1.03-1.14) | .002 | 1.08 (1.02-1.15) | .01 | 1.07 (1.00-1.14) | .04 |
| Anxiety | 1950 | 1.09 (1.04-1.15) | .002 | 1.08 (1.03-1.13) | .003 | 1.10 (1.05-1.16) | <.001 |
| Substance | 854 | 1.03 (0.94-1.12) | .57 | 1.04 (0.93-1.16) | .50 | 1.00 (0.90-1.11) | .96 |
| Behavior | 959 | 1.08 (0.98-1.21) | .13 | 1.07 (0.95-1.21) | .25 | 1.04 (0.93-1.17) | .46 |
Abbreviations: OR, odds ratio; SES, socioeconomic status.
Artificial light at night was standardized using the median absolute deviation from the median. Numbers are unweighted. The sample size is 6483 for behavioral outcomes and 10 123 for other outcomes. Analyses accounting for comorbidity between mood and anxiety disorder showed that ORs did not significantly differ between those with mood disorder only, anxiety only, or both.
Model 1 is adjusted for age and sex.
Model 2 is additionally adjusted for race/ethnicity, family income, parental education, family structure, nativity, region, and urbanicity.
Model 3 is additionally adjusted for area-level population density and socioeconomic status. Forty-eight adolescents missing values for area-level SES were not included in model 3.
Table 3 presents post hoc analyses of individual mood and anxiety disorders. Adjusting for age and sex (model 1), ALAN was positively associated with major depressive disorder/dysthymia (odds ratio [OR], 1.11 [95% CI, 1.03-1.19]), bipolar disorder (OR, 1.11 [95% CI, 1.03-1.18]), agoraphobia (OR, 1.23 [95% CI, 1.11-1.36]), social phobia (OR, 1.08 [95% CI, 1.02-1.14]), and specific phobias (OR, 1.11 [95% CI, 1.04-1.16]). Under full adjustment (model 3), only the associations with bipolar disorder (OR, 1.19 [95% CI, 1.05-1.35]) and specific phobias (OR, 1.18 [95% CI, 1.11-1.26]) remained, although odds of major depressive disorder/dysthymia were elevated (OR, 1.07 [95% CI, 1.00-1.15]). The ORs for bipolar disorder and major depressive disorder/dysthymia did not significantly differ from one another (model 1: OR, 1.00 [95% CI, 0.90-1.11]; model 2: OR, 1.05 [95% CI, 0.93-1.17]; model 3: OR, 1.11 [95% CI, 0.96, 1.29]).
Table 3. Associations Between Outdoor Artificial Light at Night and Past-Year Mood and Anxiety Disorders Among Adolescentsa.
| Disorder | No. | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|---|
| OR (95% CI)b | P value | OR (95% CI)c,d | P value | OR (95% CI)d,e | P value | ||
| Bipolar disorder | 246 | 1.11 (1.03-1.18) | .005 | 1.14 (1.05-1.24) | .002 | 1.19 (1.05-1.35) | .006 |
| Major depressive disorder/dysthymia | 775 | 1.11 (1.03-1.19) | .005 | 1.09 (1.01-1.18) | .04 | 1.07 (1.00-1.15) | .07 |
| Agoraphobia without panic | 192 | 1.23 (1.11-1.36) | <.001 | 1.18 (1.03-1.35) | .01 | 1.05 (0.89-1.24) | .57 |
| Generalized anxiety | 63 | 1.10 (0.95-1.27) | .21 | 1.01 (.83-1.22) | .95 | 0.93 (0.68-1.26) | .63 |
| Social phobia | 516 | 1.08 (1.02-1.14) | .005 | 1.05 (0.96-1.16) | .29 | 1.06 (0.96-1.18) | .25 |
| Specific phobia | 1244 | 1.11 (1.04-1.18) | .001 | 1.12 (1.05-1.18) | <.001 | 1.18 (1.11-1.26) | <.001 |
| Panic disorder | 191 | 1.04 (0.93-1.16) | .53 | 1.04 (0.90-1.21) | .57 | 1.07 (0.85-1.33) | .57 |
| PTSD | 292 | 0.95 (0.83-1.08) | .42 | 0.91 (0.76-1.08) | .26 | 0.93 (0.80-1.08) | .35 |
| Separation anxiety | 143 | 1.12 (0.97-1.29) | .13 | 1.00 (.842-1.19) | .99 | 1.06 (0.88-1.28) | .53 |
Abbreviations: ALAN, artificial light at night; OR, odds ratio; PTSD, posttraumatic stress disorder; SES, socioeconomic status.
Estimates are from separate multinomial logistic regressions, with the exception of major depressive disorder/dysthymia and bipolar disorder, which were estimated in the same model. Those with no mood or anxiety disorder are the comparison group for each disorder. Numbers are unweighted. Artificial light at night was standardized using the median absolute deviation from the median. The ORs for bipolar disorder and major depressive disorder/dysthymia did not significantly differ from one another.
Model 1 is adjusted for age and sex.
Model 2 is additionally adjusted for race/ethnicity, family income, parental education, family structure, nativity, region, and urbanicity.
In the multinomial regression (models 2 and 3) for specific phobia, ALAN was not associated with other anxiety disorders (model 3: OR, 1.01 [95% CI, 0.95-1.07]). Specific phobia was the only anxiety disorder for which this was true.
Model 3 is additionally adjusted for area-level population density and socioeconomic status. Forty-eight adolescents missing values for area-level SES were not included in model 3.
There was an interaction between ALAN and years since menarche among girls, for the outcome of weeknight bedtime (F3, 8.15; P < .001; eTable 2 in the Supplement). Estimates indicated that the difference in bedtime for those in 2 highest quartiles of ALAN compared with the lowest quartile was greater with increasing years since menarche (eFigure in the Supplement). Results of sensitivity analyses (eTables 3, 4, 5, and 6 in the Supplement) were similar to the main results.
Discussion
We found that contextual-level outdoor ALAN was associated with self-reported sleep patterns and past-year mental disorder among US adolescents. After adjusting for several sociodemographic characteristics as well as area-level population density and SES, we found that adolescents living in areas with higher levels of outdoor ALAN reported later weeknight bedtime, and those in the areas with the lowest levels had longer weeknight sleep duration. Adolescents in areas with higher outdoor ALAN also had higher odds of mood and anxiety disorders in the past year. Associations with mood disorders were present for both bipolar disorder and major depressive disorder/dysthymia, while associations with anxiety disorders were driven by specific phobias. Our results are consistent with the biological role of light as a driver of circadian rhythms6 and with several studies,20,21,22,23,24 including 1 study among adolescents, demonstrating effects of ALAN on sleep patterns. They also confirm the results of a prior study of the association between ALAN and mental health among adults,27 supporting evidence from animal models that demonstrate an association of light with mood-associated behaviors.13 To our knowledge, this is the first study to show associations between outdoor ALAN and DSM-defined mental disorders.
Disturbances in sleep and circadian rhythms are well-documented in mental disorders1,50 and may be a mechanism linking ALAN to mental disorder risk. Prior work in the NCS-A demonstrated associations between sleep patterns and past-year mental disorder.42 Prospective data will be required to assess whether sleep patterns mediate the association between ALAN and mental disorder. However, prior evidence points to sleep and circadian disturbances as antecedent and possibly causal factors in mental disorder onset, especially for mood disorder.2,3,51,52 While ALAN was associated with both subtypes of mood disorders in our study, the association with bipolar disorder was especially statistically robust. This is consistent with abundant evidence that behavioral rhythms are a core feature of bipolar disorder.53 For example, hypersensitivity of melatonin suppression in response to nighttime light exposure has been suggested as an endophenotype for bipolar disorder.54
Animal models provide evidence for biological pathways that may underlie the association between ALAN and mental disorder. In mice, the retinal ganglion cells that transmit light information to the suprachiasmatic nucleus also project to mood-associated brain structures, including the newly discovered perihabenular nucleus and regions of the hypothalamus and amygdala.55,56 Exposure to dim light at night induces depressionlike behaviors in both nocturnal and diurnal rodents,13 corroborating evidence for both indirect and direct pathways to mood (ie, pathways that do and do not include disruption to sleep and circadian rhythms).13 Circadian rhythm disruption caused by ALAN could increase risk for mental disorder through a variety of mechanisms, including hypothalamic-pituitary-adrenal axis function, neurotransmission, and immune function.57
Some prior studies have suggested that effects of light may differ by sex, across the life course, and across puberty.20,25,30,31,32 We found no evidence for differences by sex, consistent with a prior study of the association of light exposure with circadian function in adolescents.32 We also did not find evidence for differences by age among adolescent boys. Among adolescent girls, the association between ALAN and bedtime was stronger among those who with a longer time since menarche. This may be explained by differences in light sensitivity, changes in personal light exposure, or both.32
We found that outdoor ALAN was strongly associated with several adolescent demographic and socioeconomic characteristics, including indicators of social disadvantage. For example, ALAN levels were higher among racial/ethnic minority adolescents, among adolescents from immigrant families, and among those with lower family incomes. Some prior studies of outdoor ALAN have noted differences according to sociodemographic characteristics.20,23,24,25 The finding of social disparities in the distribution of outdoor ALAN among US adolescents implies that adolescents who face other sources of social disadvantage, especially those in urban settings, may also be exposed to greater levels of ALAN; this may represent an additional source of physiological stress.
To our knowledge, this is the first study to report associations between ALAN and mental disorders among adolescents, associations that have potentially long-term implications for mental and physical health. There is strong evidence for both homotypic and heterotypic continuity in mental disorder across the transition from adolescence to adulthood, especially between depression and anxiety.58 Our finding that the association between ALAN and anxiety disorder was specific to specific phobias may be because of their greater prevalence, but could also be because of the developmental nature of the sample. Previous work from the World Mental Health Surveys showed that specific phobias are the factor most strongly associated with latent internalizing comorbidity and may therefore serve as a marker of youth at risk for progression to later psychopathology.59 The associations we observed between ALAN and sleep patterns also have potential long-term health implications, in that suboptimal sleep patterns have been prospectively associated with adverse physical and mental health outcomes.60,61,62,63 The importance of sleep health in other physical health outcomes, combined with known social disparities in sleep,64 have prompted calls for more research into sleep as a potential mediator of social disparities in health.65 Our results illustrate the potential utility of adopting this approach in mental health research.
Limitations
These findings should be interpreted in the context of the study’s limitations and strengths. First, we lacked individual-level measures of light exposure, for which outdoor ALAN may not be a good proxy.66,67 This includes both indoor and outdoor sources of ALAN, which may be influenced by the use of blackout shades and other factors that affect how much light enters the home. However, individual ALAN exposure may be more susceptible to reverse causation. In addition, as interventions to reduce indoor ALAN exposure become more widespread (eg, nighttime light filters on personal electronics, changes to indoor lighting), outdoor sources of ALAN may become more influential. Second, the NCS-A is cross-sectional. While reverse causation between ALAN and sleep or mental health outcomes seems unlikely, longitudinal data would enable assessment of temporal associations between ALAN, sleep, and mental disorder. Third, sleep patterns were measured subjectively. However, we have no reason to believe that the error in sleep measurement is correlated with ALAN exposure. Fourth, ALAN was measured slightly before NCS-A data collection and was aggregated to the census block–group level, which could result in misclassification in very large or small census block groups. However, additional analyses (not shown) indicated weak dilution of the association between ALAN and sleep duration for interviews conducted after 2001 that did not affect interpretation. Furthermore, because US Defense Meteorological Satellite Program measurements were taken at varying times of night, and over 1 year, their composites do not necessarily reflect the maximum ALAN in an area or allow examination of temporal patterns. On the other hand, ALAN was measured objectively and independently of the outcomes. Fifth, ALAN may be a proxy for economic activity68 or other environmental exposures that are difficult to separate from ALAN in the context of a national epidemiologic study. However, as discussed, animal experiments demonstrate causal effects of ALAN on circadian rhythms and mood-associated behaviors. Sixth, we lacked measures of other personal, behavioral, and family characteristics that may influence sleep patterns,69 which may explain the lack of association with weekend bedtime delay and oversleep. Seventh, we lacked geographic information on daylight, precluding a more complete characterization of 24-hour contextual light.70,71 Eighth, our sample was not well suited to differentiating associations between ALAN and depression vs mania because of the infrequency of unipolar mania. Finally, patterns and sources of ALAN among adolescents may have changed since the NCS-A was conducted; the associations observed here may differ from what would be observed currently. However, the NCS-A provides the most current available data on prevalence of a wide array of DSM mental disorders among US adolescents.
Conclusions
In this study, we demonstrate that outdoor ALAN is associated with mental disorders and sleep patterns among US adolescents. These findings illustrate the importance of considering macrolevel indicators of light exposure in addition to individual-level light measures that are increasingly used in mental health and sleep research (eg, Figueiro et al,17 Esaki et al,72 and Obayashi et al73). Further research is needed to evaluate the role of other contextual and individual-level risk factors in the association between ALAN and mental disorder. Future studies should elucidate whether public interventions designed to reduce the brightness or spectral composition of outdoor nighttime lighting74 could benefit mental and sleep health among youth, especially those who face other sources of social disadvantage. For example, studies investigating the effects of changes in street lighting could include health outcomes, such as sleep and mood, to weigh the benefits and perceived disadvantages75 of such interventions.
eTable 1. Associations between quartiles of outdoor artificial light at night and sleep patterns among adolescents
eTable 2. Results of interaction tests between outdoor artificial light at night and sex, age among boys, and years since menarche among girls
eFigure. Predicted mean weeknight bedtimes for adolescent girls by quartile of outdoor artificial light at night, for those who are 1, 3, and 5 years post menarche
eTable 3. Associations between quartiles of outdoor artificial light at night and sleep patterns among adolescents; sensitivity analysis in which extreme reports (outside 3 standard deviations) are not excluded
eTable 4. Associations between quartiles of outdoor artificial light at night and sleep patterns among adolescents; sensitivity analysis in which bedtimes reported as 12:00 Noon are recoded as Midnight
eTable 5. Sensitivity analysis including categorical season variable in Model 3 of eTable 1
eTable 6. Sensitivity analysis including categorical season variable in Model 3 of Table 2
References
- 1.Germain A, Kupfer DJ. Circadian rhythm disturbances in depression. Hum Psychopharmacol. 2008;23(7):571-585. doi: 10.1002/hup.964 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Duffy A, Goodday S, Keown-Stoneman C, Grof P. The emergent course of bipolar disorder: observations over two decades from the canadian high-risk offspring cohort. Am J Psychiatry. 2019;176(9):720-729. doi: 10.1176/appi.ajp.2018.18040461 [DOI] [PubMed] [Google Scholar]
- 3.Shanahan L, Copeland WE, Angold A, Bondy CL, Costello EJ. Sleep problems predict and are predicted by generalized anxiety/depression and oppositional defiant disorder. J Am Acad Child Adolesc Psychiatry. 2014;53(5):550-558. doi: 10.1016/j.jaac.2013.12.029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Jackson A, Cavanagh J, Scott J. A systematic review of manic and depressive prodromes. J Affect Disord. 2003;74(3):209-217. doi: 10.1016/S0165-0327(02)00266-5 [DOI] [PubMed] [Google Scholar]
- 5.Merikangas KR, Swendsen J, Hickie IB, et al. Real-time mobile monitoring of the dynamic associations among motor activity, energy, mood, and sleep in adults with bipolar disorder. JAMA Psychiatry. 2019;76(2):190-198. doi: 10.1001/jamapsychiatry.2018.3546 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Roenneberg T, Merrow M. The circadian clock and human health. Curr Biol. 2016;26(10):R432-R443. doi: 10.1016/j.cub.2016.04.011 [DOI] [PubMed] [Google Scholar]
- 7.Cho Y, Ryu SH, Lee BR, Kim KH, Lee E, Choi J. Effects of artificial light at night on human health: a literature review of observational and experimental studies applied to exposure assessment. Chronobiol Int. 2015;32(9):1294-1310. doi: 10.3109/07420528.2015.1073158 [DOI] [PubMed] [Google Scholar]
- 8.Karatsoreos IN, Bhagat S, Bloss EB, Morrison JH, McEwen BS. Disruption of circadian clocks has ramifications for metabolism, brain, and behavior. Proc Natl Acad Sci U S A. 2011;108(4):1657-1662. doi: 10.1073/pnas.1018375108 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Stevens RG, Brainard GC, Blask DE, Lockley SW, Motta ME. Adverse health effects of nighttime lighting: comments on American Medical Association policy statement. Am J Prev Med. 2013;45(3):343-346. doi: 10.1016/j.amepre.2013.04.011 [DOI] [PubMed] [Google Scholar]
- 10.Blask DE, Brainard G, Gibbons R, Lockley S, Stevens R, Motta ME. Light Pollution: Adverse Health Effects of Nighttime Lighting, Report 4 Of The Council On Science And Public Health (A-12). American Medical Association; 2012. [Google Scholar]
- 11.Bedrosian TA, Nelson RJ. Influence of the modern light environment on mood. Mol Psychiatry. 2013;18(7):751-757. doi: 10.1038/mp.2013.70 [DOI] [PubMed] [Google Scholar]
- 12.Bedrosian TA, Nelson RJ. Timing of light exposure affects mood and brain circuits. Transl Psychiatry. 2017;7(1):e1017. doi: 10.1038/tp.2016.262 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.LeGates TA, Fernandez DC, Hattar S. Light as a central modulator of circadian rhythms, sleep and affect. Nat Rev Neurosci. 2014;15(7):443-454. doi: 10.1038/nrn3743 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Obayashi K, Saeki K, Iwamoto J, Ikada Y, Kurumatani N. Exposure to light at night and risk of depression in the elderly. J Affect Disord. 2013;151(1):331-336. doi: 10.1016/j.jad.2013.06.018 [DOI] [PubMed] [Google Scholar]
- 15.Obayashi K, Saeki K, Kurumatani N. Bedroom light exposure at night and the incidence of depressive symptoms: a longitudinal study of the HEIJO-KYO Cohort. Am J Epidemiol. 2018;187(3):427-434. doi: 10.1093/aje/kwx290 [DOI] [PubMed] [Google Scholar]
- 16.Wallace-Guy GM, Kripke DF, Jean-Louis G, Langer RD, Elliott JA, Tuunainen A. Evening light exposure: implications for sleep and depression. J Am Geriatr Soc. 2002;50(4):738-739. doi: 10.1046/j.1532-5415.2002.50171.x [DOI] [PubMed] [Google Scholar]
- 17.Figueiro MG, Hunter CM, Higgins P, et al. Tailored lighting intervention for persons with dementia and caregivers living at home. Sleep Health. 2015;1(4):322-330. doi: 10.1016/j.sleh.2015.09.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Oldham MA, Ciraulo DA. Bright light therapy for depression: a review of its effects on chronobiology and the autonomic nervous system. Chronobiol Int. 2014;31(3):305-319. doi: 10.3109/07420528.2013.833935 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Terman M, Terman JS. Light therapy for seasonal and nonseasonal depression: efficacy, protocol, safety, and side effects. CNS Spectr. 2005;10(8):647-663. doi: 10.1017/S1092852900019611 [DOI] [PubMed] [Google Scholar]
- 20.Koo YS, Song JY, Joo EY, et al. Outdoor artificial light at night, obesity, and sleep health: cross-sectional analysis in the KoGES study. Chronobiol Int. 2016;33(3):301-314. doi: 10.3109/07420528.2016.1143480 [DOI] [PubMed] [Google Scholar]
- 21.Patel PC. Light pollution and insufficient sleep: evidence from the United States. Am J Hum Biol. 2019;31(6):e23300. doi: 10.1002/ajhb.23300 [DOI] [PubMed] [Google Scholar]
- 22.Vollmer C, Michel U, Randler C. Outdoor light at night (LAN) is correlated with eveningness in adolescents. Chronobiol Int. 2012;29(4):502-508. doi: 10.3109/07420528.2011.635232 [DOI] [PubMed] [Google Scholar]
- 23.Xiao Q, Gee G, Jones RR, Jia P, James P, Hale L. Cross-sectional association between outdoor artificial light at night and sleep duration in middle-to-older aged adults: The NIH-AARP Diet and Health Study. Environ Res. 2020;180:108823. doi: 10.1016/j.envres.2019.108823 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ohayon MM, Milesi C. Artificial outdoor nighttime lights associate with altered sleep behavior in the American general population. Sleep. 2016;39(6):1311-1320. doi: 10.5665/sleep.5860 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.James P, Bertrand KA, Hart JE, Schernhammer ES, Tamimi RM, Laden F. Outdoor light at night and breast cancer incidence in the Nurses’ Health Study II. Environ Health Perspect. 2017;125(8):087010. doi: 10.1289/EHP935 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Rybnikova NA, Haim A, Portnov BA. Does artificial light-at-night exposure contribute to the worldwide obesity pandemic? Int J Obes (Lond). 2016;40(5):815-823. doi: 10.1038/ijo.2015.255 [DOI] [PubMed] [Google Scholar]
- 27.Min JY, Min KB. Outdoor light at night and the prevalence of depressive symptoms and suicidal behaviors: a cross-sectional study in a nationally representative sample of Korean adults. J Affect Disord. 2018;227:199-205. doi: 10.1016/j.jad.2017.10.039 [DOI] [PubMed] [Google Scholar]
- 28.Jones PB. Adult mental health disorders and their age at onset. Br J Psychiatry Suppl. 2013;54(s54):s5-s10. doi: 10.1192/bjp.bp.112.119164 [DOI] [PubMed] [Google Scholar]
- 29.Borniger JC, McHenry ZD, Abi Salloum BA, Nelson RJ. Exposure to dim light at night during early development increases adult anxiety-like responses. Physiol Behav. 2014;133:99-106. doi: 10.1016/j.physbeh.2014.05.012 [DOI] [PubMed] [Google Scholar]
- 30.Cissé YM, Peng J, Nelson RJ. Dim light at night prior to adolescence increases adult anxiety-like behaviors. Chronobiol Int. 2016;33(10):1473-1480. doi: 10.1080/07420528.2016.1221418 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Chellappa SL, Steiner R, Oelhafen P, Cajochen C. Sex differences in light sensitivity impact on brightness perception, vigilant attention and sleep in humans. Sci Rep. 2017;7(1):14215. doi: 10.1038/s41598-017-13973-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Crowley SJ, Cain SW, Burns AC, Acebo C, Carskadon MA. Increased sensitivity of the circadian system to light in early/mid-puberty. J Clin Endocrinol Metab. 2015;100(11):4067-4073. doi: 10.1210/jc.2015-2775 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Kessler RC, Avenevoli S, Costello EJ, et al. National comorbidity survey replication adolescent supplement (NCS-A): II, overview and design. J Am Acad Child Adolesc Psychiatry. 2009;48(4):380-385. doi: 10.1097/CHI.0b013e3181999705 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kessler RC, Berglund P, Chiu WT, et al. The US National Comorbidity Survey Replication (NCS-R): design and field procedures. Int J Methods Psychiatr Res. 2004;13(2):69-92. doi: 10.1002/mpr.167 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Merikangas KR, Avenevoli S, Costello EJ, Koretz D, Kessler RC. National comorbidity survey replication adolescent supplement (NCS-A): I, background and measures. J Am Acad Child Adolesc Psychiatry. 2009;48(4):367-379. doi: 10.1097/CHI.0b013e31819996f1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Kessler RC, Akiskal HS, Angst J, et al. Validity of the assessment of bipolar spectrum disorders in the WHO CIDI 3.0. J Affect Disord. 2006;96(3):259-269. doi: 10.1016/j.jad.2006.08.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Kessler RC, Avenevoli S, Green J, et al. National comorbidity survey replication adolescent supplement (NCS-A): III, concordance of DSM-IV/CIDI diagnoses with clinical reassessments. J Am Acad Child Adolesc Psychiatry. 2009;48(4):386-399. doi: 10.1097/CHI.0b013e31819a1cbc [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Cantwell DP, Lewinsohn PM, Rohde P, Seeley JR. Correspondence between adolescent report and parent report of psychiatric diagnostic data. J Am Acad Child Adolesc Psychiatry. 1997;36(5):610-619. doi: 10.1097/00004583-199705000-00011 [DOI] [PubMed] [Google Scholar]
- 39.Grills AE, Ollendick TH. Issues in parent-child agreement: the case of structured diagnostic interviews. Clin Child Fam Psychol Rev. 2002;5(1):57-83. doi: 10.1023/A:1014573708569 [DOI] [PubMed] [Google Scholar]
- 40.Paksarian D, Rudolph KE, He JP, Merikangas KR. School start time and adolescent sleep patterns: results from the U.S. National Comorbidity Survey—adolescent supplement. Am J Public Health. 2015;105(7):1351-1357. doi: 10.2105/AJPH.2015.302619 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Rudolph KE, Shev A, Paksarian D, et al. Environmental noise and sleep and mental health outcomes in a nationally representative sample of urban US adolescents. Environ Epidemiol. 2019;3(4):e056. doi: 10.1097/EE9.0000000000000056 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Zhang J, Paksarian D, Lamers F, Hickie IB, He J, Merikangas KR. Sleep patterns and mental health correlates in US adolescents. J Pediatr. 2017;182:137-143. doi: 10.1016/j.jpeds.2016.11.007 [DOI] [PubMed] [Google Scholar]
- 43.NOAA Earth Observation Group Version 4 DMSP-OLS nighttime lights time series. Published 2020. Accessed May 29, 2020. https://ngdc.noaa.gov/eog/dmsp/downloadV4composites.html
- 44.NOAA Earth Observation Group Version 4 DMSP-OLS nighttime lights time series readme. Published 2020. Accessed May 29, 2020. https://ngdc.noaa.gov/eog/gcv4_readme.txt
- 45.Hsu FC, Baugh KE, Ghosh T, Zhizhin M, Elvidge CD. DMSP-OLS radiance calibrated nighttime lights time series with intercalibration. Remote Sens (Basel). 2015;7(2):1855-1876. doi: 10.3390/rs70201855 [DOI] [Google Scholar]
- 46.Diez-Roux AV, Kiefe CI, Jacobs DR Jr, et al. Area characteristics and individual-level socioeconomic position indicators in three population-based epidemiologic studies. Ann Epidemiol. 2001;11(6):395-405. Published correction appears in Ann Epidemiol.2001;30(4):924. doi: 10.1016/S1047-2797(01)00221-6 [DOI] [PubMed] [Google Scholar]
- 47.Rudolph KE, Stuart EA, Glass TA, Merikangas KR. Neighborhood disadvantage in context: the influence of urbanicity on the association between neighborhood disadvantage and adolescent emotional disorders. Soc Psychiatry Psychiatr Epidemiol. 2014;49(3):467-475. doi: 10.1007/s00127-013-0725-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Greenland S, Maclure M, Schlesselman JJ, Poole C, Morgenstern H. Standardized regression coefficients: a further critique and review of some alternatives. Epidemiology. 1991;2(5):387-392. doi: 10.1097/00001648-199109000-00015 [DOI] [PubMed] [Google Scholar]
- 49.Kessler RC, Avenevoli S, Costello EJ, et al. Design and field procedures in the US National Comorbidity Survey Replication Adolescent Supplement (NCS-A). Int J Methods Psychiatr Res. 2009;18(2):69-83. doi: 10.1002/mpr.279 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Ford DE, Kamerow DB. Epidemiologic study of sleep disturbances and psychiatric disorders: an opportunity for prevention? JAMA. 1989;262(11):1479-1484. doi: 10.1001/jama.1989.03430110069030 [DOI] [PubMed] [Google Scholar]
- 51.Murray G, Harvey A. Circadian rhythms and sleep in bipolar disorder. Bipolar Disord. 2010;12(5):459-472. doi: 10.1111/j.1399-5618.2010.00843.x [DOI] [PubMed] [Google Scholar]
- 52.Soehner AM, Bertocci MA, Levenson JC, et al. Longitudinal associations between sleep patterns and psychiatric symptom severity in high-risk and community comparison youth. J Am Acad Child Adolesc Psychiatry. 2019;58(6):608-617. doi: 10.1016/j.jaac.2018.09.448 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Gonzalez R. The relationship between bipolar disorder and biological rhythms. J Clin Psychiatry. 2014;75(4):e323-e331. doi: 10.4088/JCP.13r08507 [DOI] [PubMed] [Google Scholar]
- 54.Hallam KT, Olver JS, Chambers V, Begg DP, McGrath C, Norman TR. The heritability of melatonin secretion and sensitivity to bright nocturnal light in twins. Psychoneuroendocrinology. 2006;31(7):867-875. doi: 10.1016/j.psyneuen.2006.04.004 [DOI] [PubMed] [Google Scholar]
- 55.Hattar S, Kumar M, Park A, et al. Central projections of melanopsin-expressing retinal ganglion cells in the mouse. J Comp Neurol. 2006;497(3):326-349. doi: 10.1002/cne.20970 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Fernandez DC, Fogerson PM, Lazzerini Ospri L, et al. Light affects mood and learning through distinct retina-brain pathways. Cell. 2018;175(1):71-84.e18. doi: 10.1016/j.cell.2018.08.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.McClung CA. How might circadian rhythms control mood? Let me count the ways.... Biol Psychiatry. 2013;74(4):242-249. doi: 10.1016/j.biopsych.2013.02.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Copeland WE, Adair CE, Smetanin P, et al. Diagnostic transitions from childhood to adolescence to early adulthood. J Child Psychol Psychiatry. 2013;54(7):791-799. doi: 10.1111/jcpp.12062 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Kessler RC, Ormel J, Petukhova M, et al. Development of lifetime comorbidity in the World Health Organization world mental health surveys. Arch Gen Psychiatry. 2011;68(1):90-100. doi: 10.1001/archgenpsychiatry.2010.180 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Zhai L, Zhang H, Zhang D. Sleep duration and depression among adults: a meta-analysis of prospective studies. Depress Anxiety. 2015;32(9):664-670. doi: 10.1002/da.22386 [DOI] [PubMed] [Google Scholar]
- 61.Sivertsen B, Lallukka T, Salo P, et al. Insomnia as a risk factor for ill health: results from the large population-based prospective HUNT study in Norway. J Sleep Res. 2014;23(2):124-132. doi: 10.1111/jsr.12102 [DOI] [PubMed] [Google Scholar]
- 62.Gangwisch JE, Malaspina D, Babiss LA, et al. Short sleep duration as a risk factor for hypercholesterolemia: analyses of the National Longitudinal Study of Adolescent Health. Sleep. 2010;33(7):956-961. doi: 10.1093/sleep/33.7.956 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Wong MM, Brower KJ. The prospective relationship between sleep problems and suicidal behavior in the National Longitudinal Study of Adolescent Health. J Psychiatr Res. 2012;46(7):953-959. doi: 10.1016/j.jpsychires.2012.04.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Jackson CL, Redline S, Emmons KM. Sleep as a potential fundamental contributor to disparities in cardiovascular health. Annu Rev Public Health. 2015;36:417-440. doi: 10.1146/annurev-publhealth-031914-122838 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Laposky AD, Van Cauter E, Diez-Roux AV. Reducing health disparities: the role of sleep deficiency and sleep disorders. Sleep Med. 2016;18:3-6. doi: 10.1016/j.sleep.2015.01.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Huss A, van Wel L, Bogaards L, et al. Shedding some light in the dark—a comparison of personal measurements with satellite-based estimates of exposure to light at night among children in the Netherlands. Environ Health Perspect. 2019;127(6):67001. doi: 10.1289/EHP3431 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Rea MS, Brons JA, Figueiro MG. Measurements of light at night (LAN) for a sample of female school teachers. Chronobiol Int. 2011;28(8):673-680. doi: 10.3109/07420528.2011.602198 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Mellander C, Lobo J, Stolarick K, Matheson Z. Night-time light data: A good proxy measure for economic activity? PLoS One. 2015;10(10):e0139779. doi: 10.1371/journal.pone.0139779 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Johnson DA, Billings ME, Hale L. Environmental determinants of insufficient sleep and sleep disorders: implications for population health. Curr Epidemiol Rep. 2018;5(2):61-69. doi: 10.1007/s40471-018-0139-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Bauer M, Glenn T, Alda M, et al. Influence of light exposure during early life on the age of onset of bipolar disorder. J Psychiatr Res. 2015;64:1-8. doi: 10.1016/j.jpsychires.2015.03.013 [DOI] [PubMed] [Google Scholar]
- 71.Smolensky MH, Sackett-Lundeen LL, Portaluppi F. Nocturnal Light Pollution and Underexposure to Daytime Sunlight: Complementary Mechanisms of Circadian Disruption and Related Diseases. Taylor & Francis; 2015. [DOI] [PubMed] [Google Scholar]
- 72.Esaki Y, Kitajima T, Obayashi K, Saeki K, Fujita K, Iwata N. Light exposure at night and sleep quality in bipolar disorder: the APPLE cohort study. J Affect Disord. 2019;257:314-320. doi: 10.1016/j.jad.2019.07.031 [DOI] [PubMed] [Google Scholar]
- 73.Obayashi K, Saeki K, Kurumatani N. Association between light exposure at night and insomnia in the general elderly population: the HEIJO-KYO cohort. Chronobiol Int. 2014;31(9):976-982. doi: 10.3109/07420528.2014.937491 [DOI] [PubMed] [Google Scholar]
- 74.Maierová L. Public lighting, public health, 2018; VII Lighting Conference of the Visegrad Countries (Lumen V4), Trebic. Published 2018. Accessed June 5, 2020. https://ieeexplore.ieee.org/abstract/document/8521032
- 75.Green J, Perkins C, Steinbach R, Edwards P. Reduced street lighting at night and health: a rapid appraisal of public views in England and Wales. Health Place. 2015;34:171-180. doi: 10.1016/j.healthplace.2015.05.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eTable 1. Associations between quartiles of outdoor artificial light at night and sleep patterns among adolescents
eTable 2. Results of interaction tests between outdoor artificial light at night and sex, age among boys, and years since menarche among girls
eFigure. Predicted mean weeknight bedtimes for adolescent girls by quartile of outdoor artificial light at night, for those who are 1, 3, and 5 years post menarche
eTable 3. Associations between quartiles of outdoor artificial light at night and sleep patterns among adolescents; sensitivity analysis in which extreme reports (outside 3 standard deviations) are not excluded
eTable 4. Associations between quartiles of outdoor artificial light at night and sleep patterns among adolescents; sensitivity analysis in which bedtimes reported as 12:00 Noon are recoded as Midnight
eTable 5. Sensitivity analysis including categorical season variable in Model 3 of eTable 1
eTable 6. Sensitivity analysis including categorical season variable in Model 3 of Table 2