

Abstract
Systemic lupus erythematosus-myositis overlap syndrome is rare with prognostic implications. Reports suggest that systemic lupus erythematosus-myositis overlap syndrome with lupus nephritis has a variable clinical outcome. We report a case of systemic lupus erythematosus-myositis overlap syndrome with lupus nephritis in a 28-year-old female, who presented with facial puffiness, proximal muscle weakness, and proteinuria.
Keywords: Overlap syndrome, proteinuria, systemic lupus erythematosus
Introduction
The term overlap syndrome includes coexistence of signs, symptoms and immunological features of two or more connective diseases occurring simultaneously.[1] Overlap syndromes of SLE with myositis, including dermatomyositis and polymyositis, are recognized clinically. 1 In contrast to myalgia which can affect nearly half of patients with systemic lupus erythematosus (SLE), SLE-myositis overlap syndrome is relatively rare. Its frequency varies from 4 to 16% in different series.[1,2]
Case Report
A 28-year-old female presented with facial puffiness and proximal muscle weakness for the last 3 months. There was no significant past medical and family history. On general examination, she had pallor with pain and swelling of bilateral ankle joints and right wrist joint. There was no dysphagia, dyspnea, mucocutaneous, or gastrointestinal symptoms. There was no significant drug history.
Her hemoglobin was 10.8 gm/dL, total leukocyte count was 2500/cumm, platelet count was 1.5 lakh/cumm and erythrocyte sedimentation rate was 90 mm at the end of the first hour. Urine analysis showed 3 + proteinuria with urine microscopy showing RBCs. The chest X-ray did not reveal any abnormality. Her serum creatinine level was 1.8 mg/dL. Immunologic work-up showed positive antinuclear antibody (ANA) and anti-double-stranded DNA antibody, anti-Smith, and anti-U1RNP. The anti-neutrophil cytoplasmic antibody, antistreptolysin O, rheumatoid factor and viral serology for hepatitis B, C, and HIV were negative. Complement C3 and C4 levels were low. Her serum creatinine phosphokinase was elevated with 2150 IU/L.
Kidney biopsy showed congested glomerular capillaries with uniform basement thickening [Figure 1a] and spikes seen in the glomerular capillary wall in the silver stain. Immunofluorescence for IgG, IgA, C3, kappa, and lambda showed a full-house pattern. [Figure 1b] A diagnosis of class V membranous lupus nephritis was made. Muscle biopsy was done from the right deltoid muscle, which showed lymphocytes infiltrating necrotic muscle fibers [Figure 1c] with evidence of lymphocytic vasculitis, thus confirming the diagnosis of myositis. Thus a final diagnosis of SLE-myositis overlap syndrome with lupus nephritis was made.
Figure 1.
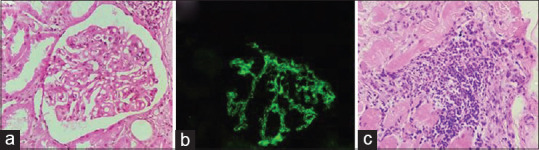
(a) Kidney biopsy showing uniform basement thickening (H and E, 100×); (b) Immunofluorescence showing full-house pattern; (c) Muscle biopsy showing lymphocytes infiltrating necrotic muscle fibers (H and E, 100×)
The patient received three pulses of intravenous methylprednisolone (1000 mg/day), with prednisone (1 mg/kg/day) on a weaning regimen, and monthly therapy of intravenous cyclophosphamide (1 g/m2). The patient tolerated the treatment well. There was complete clinical and serological remission of myositis and lupus nephritis.
Discussion
It is difficult to distinguish myositis associated with SLE from myalgia occurring in patients with SLE. Generally, true myositis differs slightly in its clinical presentation with younger age of onset.[3] All SLE-myositis overlap syndrome patients are female.[1,2] Almost all of these patients present with symptoms of proximal weakness.[4] Studies have shown that these patients have more propensities to develop alopecia, oral ulcers, erosive joint disease, and pulmonary disease.[3] However, there is no significant increase in the incidence of lupus nephritis in SLE-myositis overlap syndrome.[3] Raised serum creatine kinase is found to correspond with underlying myositis in patients with SLE.[4] Furthermore, the presence of myositis specific antibodies such as anti-U1RNP, anti-Ro/SSA, anti-La/SSB, anti-Sm or anti-PM-Scl is suggestive of an overlap myositis.[1,4] Myositis, lymphocytic vasculitis, type II muscle, atrophy, vessel wall thickening, and vacuolar myopathy are various histopathological findings observed in the muscle biopsies of patients with SLE.[3] However, histopathological findings of lymphocytic vasculitis and/or myositis are confirmatory of true myositis in SLE.[4]
Treatment can prove difficult as both conditions respond to a variety of immunosuppressive and cytotoxic agents. Corticosteroids were used usually as first-line therapy and additional immunosuppressive agents such as cyclophosphamide, methotrexate, rituximab, and mycophenolate mofetil have been used with varying degrees of clinical response and remission rates.[1,5]
There are conflicting reports regarding the prognosis of SLE-myositis overlap syndrome. Some reports suggest that it follows a benign course, while others suggest no difference between them in terms of morbidity and response to therapy.[1,2] Again another study suggests that those with SLE-myositis overlap syndrome have a poorer outcome with early death.[3] Although myositis in SLE responds well to corticosteroids, the association of pulmonary involvement leads to early mortality with increase standardized mortality ratio compared to SLE alone. This indicates poor prognosis with SLE-myositis overlap syndrome.[6] In the present case, the patient responded well to treatment with complete clinical and serological remission of myositis and lupus nephritis.
SLE has an incidence of 3–4 in 100,000 populations per year in India and is commonly encountered autoimmune disease by the family physicians.[7] Lupus nephritis is a form of glomerulonephritis that constitutes one of the most severe organ manifestations of SLE.[8] Other than lupus nephritis and infection, the physicians should also be vigilant about overlap syndromes with myositis including dermatomyositis and polymyositis. The data on the subset of SLE-associated overlap syndrome is scarce however these may require aggressive therapy with a poorer prognosis.[6] Thus, while following up on a case of SLE, family physicians should be aware of these complications so as to initiate timely investigations and medical interventions.
Conclusion
SLE is an important cause of morbidity as encountered by family physicians. The most dreaded complication of SLE remains lupus nephritis causing a significant increase in the mortality rate. Other than lupus nephritis, the physicians should also be aware of the overlap syndromes with myositis in SLE, which have a poorer prognosis and may require aggressive therapy.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his/her consent for his/her images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity. A per the institute guidelines, ethical clearance is not required for case reports.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Maazoun F, Frikha F, Snoussi M, Kaddour N, Masmoudi H, Bahloul Z. Systemic lupus erythematosus-myositis overlap syndrome: report of 6 cases. Clin Pract. 2011;1:e89. doi: 10.4081/cp.2011.e89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Garton MJ, Isenberg DA. Clinical features of lupus myositis versus idiopathic myositis: A review of 30 cases. Br J Rheumatol. 1997;36:1067–74. doi: 10.1093/rheumatology/36.10.1067. [DOI] [PubMed] [Google Scholar]
- 3.Dayal NA, Isenberg DA. SLE/myositis overlap: Are the manifestations of SLE different in overlap disease? Lupus. 2002;11:293–8. doi: 10.1191/0961203302lu186oa. [DOI] [PubMed] [Google Scholar]
- 4.Lim LM, Abdul-Wahab R, Lowe J, Powell RJ. Muscle biopsy abnormalities in systemic lupus erythematosus: correlation with clinical and laboratory parameters. Ann Rheum Dis. 1994;53:178–82. doi: 10.1136/ard.53.3.178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Miller JB, Paik JJ. Overlap syndromes in inflammatory myopathies. Curr Treat Options in Rheum. 2017;3:289–98. [Google Scholar]
- 6.Shah S, Chengappa K G, Negi VS. Systemic lupus erythematosus and overlap: A clinician perspective. Clin Dermatol Rev. 2019;3:12–7. [Google Scholar]
- 7.Bharath G, Kumar P, Makkar N, Singla P, Soneja M, Biswas A, et al. Mortality in systemic lupus erythematosus at a teaching hospital in India: A 5-year retrospective study. J Family Med Prim Care. 2019;8:2511–5. doi: 10.4103/jfmpc.jfmpc_362_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Anders H, Saxena R, Zhao M, Parodis I, Salmon JE, Mohan C. Lupus nephritis. Nat Rev Dis Primers. 2020;6:7. doi: 10.1038/s41572-019-0141-9. [DOI] [PubMed] [Google Scholar]