

Abstract
Purpose of Review
Heart failure with preserved ejection fraction (HFpEF) is a relatively new disease entity used in medical terminology; however, both the number of patients and its clinical significance are growing. HFpEF used to be seen as a mild condition; however, the symptoms and quality of life of the patients are comparable to those with reduced ejection fraction. The disease is much more complex than previously thought. In this article, information surrounding the etiology, diagnosis, prognosis, and possible therapeutic options of HFpEF are reviewed and summarized.
Recent Findings
It has recently been proposed that heart failure (HF) is rather a heterogeneous syndrome with a spectrum of overlapping and distinct characteristics. HFpEF itself can be distilled into different phenotypes based on the underlying biology. The etiological factors of HFpEF are unclear; however, systemic low-grade inflammation and microvascular damage as a consequence of comorbidities associated with endothelial dysfunction, oxidative stress, myocardial remodeling, and fibrosis are considered to play a crucial role in the pathogenesis of a disease. The H2FPEF score and the HFpEF nomogram are recently validated highly sensitive tools employed for risk assessment of subclinical heart failure.
Summary
Despite numerous studies, there is still no evidence-based pharmacotherapy for HFpEF and the mortality and morbidity associated with HFpEF remain high. A better understanding of the etiological factors, the impact of comorbidities, the phenotypes of the disease, and implementation of machine learning algorithms may play a key role in the development of future therapeutic strategies.
Keywords: HFpEF, Heart failure, Diastolic dysfunction, Heart failure with preserved ejection fraction, Preserved left ventricular function
Introduction
The spectrum of disorders involving myocardial dysfunction with typical signs and symptoms has since been referred to as heart failure (HF) [1, 2]. Echocardiographic parameters, i.e., ejection fraction (EF), have been used for subclassification of this complex clinical entity: heart failure with reduced EF (HFrEF; EF < 40%), mid-range EF (HFmrEF; EF 41–49%), and preserved EF (HFpEF; EF ≥ 50%) have all been recognized as different points on the continuum of heart failure disorders [3].
Heart failure has been increasingly recognized as an epidemic and various possible etiologies have now been identified. These include coronary artery disease, valvular heart disease, hypertension, cardiomyopathies, and adverse effects of drugs and toxins [3]. In developing and developed countries, heart failure incidence continues to rise, accounting for most cases of HF in the developed world [2, 3]. HFpEF was discovered by Dr. Luchi et al., who in 1982 described a group of patients with typical heart failure symptoms and associated preserved (≥ 50%) left ventricular ejection fraction (LVEF) [4]. Recently, HFpEF has been defined by the European Society of Cardiology (ESC) as preserved left ventricular EF (LVEF ≥ 50%), with evidence of diastolic dysfunction or structural heart disease, in the context of classic signs and symptoms of heart failure and elevated natriuretic peptides [3, 5].
The complex interplay between various factors involved in the etiopathogenesis and potentiation of heart failure has sparked a new drive for heart failure classification based on various (molecular and biochemical) parameters and biomarker profiles [6, 7•]. Indeed, the inter- and intra-observer reliability of LVEF has been noted to vary markedly, thus diminishing the clinical utility of LVEF for diagnostic and prognostic purposes [7•]. However, the terms HFrEF, HFmrEF, and HFpEF will be used in our descriptions for simplicity.
Prevalence and Demographics
The prevalence of HF is estimated to be 1.1–5.5% in the general population [8]. It is a common cause of hospitalization. Those who are diagnosed with HFpEF represent about a third to one-half of the total number of HF patients [9–11]. Current data suggests that there is a shift in the type of heart failure patients are likely to be diagnosed with. Epidemiological data revealed that the prevalence of HFpEF relative to HFrEF is increasing at a rate of 1% per year, indicating that HFpEF is becoming the most common type of HF [8]. The highest rate of HFpEF is among the elderly; however, the younger subgroup of patients (< 65-year-old) accounts for 40% of all total cases [9, 12]. HFpEF affects more women than men, suggesting that gender may play a major role in disease evolution [13]. On the other hand, incidence rates are similar across all races and ethnicities [14]. Although patients with HFpEF have a lower risk of death than patients with HFrEF (HR 0.62, 95% CI 0.46–0.85), regardless of age, gender, or etiology of HF, absolute mortality is still high [15].
Etiology
The etiology and pathophysiology of HFpEF are still being uncovered. Firstly, the etiological factors affecting HFpEF and HFrEF seem to be different [16]. The Framingham Heart Study suggests that the classification of HF be made depending on the underlying cause of the disease: coronary artery disease, valvular heart disease, hypertension, or other causes [16, 17]. Patients with HFpEF are more likely to have valvular heart disease, hypertension, and atrial fibrillation (p = 0.05, p < 0.001, and p < 0.001, respectively). On the contrary, patients with HFpEF are less likely to have a myocardial infarction or left bundle branch block (LBBB) (OR 0.21, 95% CI, 0.10–0.46, p < 0.001). Compared to patients with HFrEF, patients with HFpEF have significantly higher blood pressure (p = 0.04), lower resting heart rate, and lower levels of potassium in the plasma [16]. Many studies point out that patients with HFpEF are usually older women with hypertension [15, 16, 18, 19]. Indeed, arterial hypertension is one of the main factors leading to increased stiffness of blood vessels and increased afterload of LV [20].
Furthermore, comorbidities seem to play a pivotal role in the pathophysiology of HFpEF. The most common are obesity, diabetes, atrial fibrillation, metabolic syndrome, chronic obstructive pulmonary disease, sleep-disordered breathing, renal dysfunction, and anemia [7•, 21–27]. Aging seems to have a great impact as well [10, 28, 29].
Although the pathophysiology of HFpEF is yet to be understood, systemic low-grade inflammation, mediated through tumor necrosis factor (TNF) alpha and transforming growth factor (TGF) beta 1, was proposed as a cause of disease [18, 30]. However, the degree of diffuse myocardial fibrosis is not related to the severity of impairment of diastolic function in HFpEF [31]. Microvascular dysfunction induces systemic inflammation which is present before the clinical symptoms [18, 32]. It is mediated by microRNAs and the formation of different miRNA [18, 33]. Furthermore, the intrinsic cardiomyocyte phenotype is distinct in HFpEF and HFrEF. Research by Curl et al. indicates that hypertrophic heart rat (HHR) shows a significantly elevated calcium (Ca2+) operating level and increased L-type calcium channel current, which contrasts with the suppressed Ca2+ cycling state typical for HFrEF [34].
Clinical Manifestations
The initial presenting symptoms of HFpEF may be included in the broad category of heart failure. Dyspnea is the most common manifesting symptom among them. Shortness of breath can manifest in various ways, whether it be upon exertion or at rest as in paroxysmal nocturnal dyspnea or orthopnea. Other non-specific symptoms such as fatigue are present. The typical heart failure symptoms such as ankle edema and jugular venous distention are often not present. Other possible presentations include decreased exercise tolerance, chest pain, or discomfort.
Diagnosis
The H2FPEF score and the HFpEF nomogram are recently validated highly sensitive tools employed for risk assessment of subclinical heart failure. These tools are based on clinical and echocardiographic parameters, including body mass index (BMI) > 30 kg/m2 (H); use of 2 or more antihypertensive medications (H); the presence of atrial fibrillation (F); pulmonary hypertension (pulmonary artery systolic pressure > 35 mmHg) (P); elderly with an age > 60 years (E); and elevated filling pressures (E/e′ > 9) (F). The H2FPEF score determines the probability of HFpEF by assigning a number for each item (Fig. 1) [35•]. Although formerly designated as heart failure with diastolic dysfunction, HFpEF may occur in the absence of signs of diastolic dysfunction, and as such evidence/presence of diastolic dysfunction is not required for the diagnosis [36].
Fig. 1.
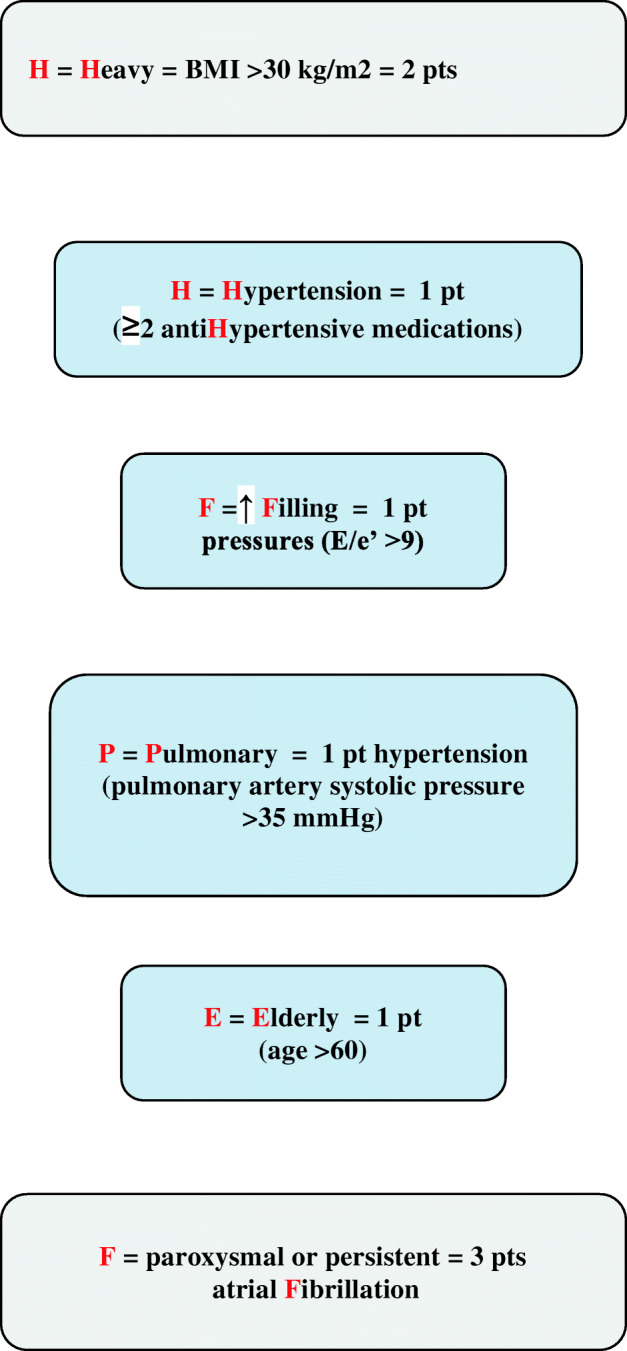
H2FPEF score used to determine the probability of HFpEF (figure created based on text from Paulus [35•])
As previously mentioned, the European Society of Cardiology (ESC) guidelines for the diagnosis of HFpEF include left ventricular EF (LVEF) ≥ 50%, evidence of either diastolic dysfunction or structural heart disease, signs and/or symptoms of heart failure, and elevated natriuretic peptides [3]. Given the complexity of HFpEF, various parameters including clinical (patient history and physical examination), biochemical (serum BNP level), hemodynamic, and radiographic data are utilized in reaching a diagnosis [37, 38]. Oftentimes exercise testing is required to confirm the diagnosis when signs of diastolic dysfunction occur only on exertion but not at rest. Nevertheless, the echocardiographic evaluation is crucial, and advanced techniques seem particularly promising. Shah et al. proposed recently that echocardiography could serve as a “digital biopsy” of the heart. Speckle-tracking echocardiography (STE) can be utilized to assess cardiomyocyte calcium homeostasis, excitation-contraction coupling, and the health of T-tubules before the onset of myocardial fibrosis [39, 40]. Furthermore, defining left atrial structure and function has recently gained importance in evaluation of LV diastolic dysfunction [41].
Since HFpEF may also share similar clinical characteristics with valvular heart disease, pericardial disease, and high-output HF [42], diagnostic algorithms are useful in making the diagnosis of HFpEF (Fig. 2).
Fig. 2.

Diagnostic algorithm for HFpEF (figure created based on text from Huis in’t Veld et al. [38])
HFpEF Phenotypes
Phenotypic presentations of HFpEF may vary widely across patients and determine the choice of diagnostic tests and targeted management plan [39••, 43–46]. There are four clinically distinct phenotypes of HFpEF that have been recognized [47]:
Aging phenotype
Obesity phenotype
Pulmonary hypertension (PH) phenotype
Coronary artery disease (CAD) phenotype
Although this classification acknowledges the heterogeneity and need for individualized approach, the biological phenotypes seem to better describe the underlying pathomechanisms of HFpEF. Shah et al. proposed a classification created by the use of machine learning [39••, 45, 48]:
The three identified biological phenogroups are as follows:
Natriuretic peptide deficiency syndrome—younger subjects with moderate diastolic dysfunction and relatively normal BNP
Extreme cardiometabolic syndrome—obese, diabetic subjects with a high prevalence of obstructive sleep apnea
Right ventricle-cardio-abdomino-renal syndrome—older subjects with significant chronic kidney disease and cardiopulmonary comorbidities
Worse outcomes are observed in phenogroups 2 and 3.
It is generally thought that the heterogeneity in the clinical presentation of HFpEF may be explained by underlying comorbidities in individual subjects. Thus, phenogrouping enables risk stratification and the institution of better-targeted therapies as opposed to BNP-based stratification alone [45].
Differential Diagnosis
Since symptoms of HFpEF are non-specific, diagnosis might be elusive. The majority of patients complain of exertional dyspnea, which is a common cause of hospital admission. As such, there are multiple differential diagnoses to consider, including pulmonary and cardiovascular causes, or vocal cord conditions [49]. Differential diagnosis to rule out other causes of dyspnea should be based on echocardiographic examination and tissue doppler imaging [50]. Overall, clinicians should pay attention to non-specific manifestations of HFpEF and diagnose sensibly based on imaging studies.
Evaluation of Comorbidities
In recent years, a new paradigm of HFpEF has been suggested, implying that it is a very heterogeneous disease. It can be caused by comorbidities through systemic endothelial inflammation leading to structural and functional remodeling of the heart [51].
The most significant comorbidities are obesity, diabetes, metabolic syndrome, chronic obstructive pulmonary disease, sleep-disordered breathing, renal dysfunction, and anemia [7•, 21–27]. Excess visceral fat leads to increased levels of proinflammatory cytokines [52]. Hyperglycemia, hyperinsulinemia, and insulin resistance lead to mitochondrial and microvascular dysfunction, as well as autonomic neuropathy, which cause cardiac stiffness, hypertrophy, fibrosis, and eventually HF [53]. It is worth noting that proper diagnosis and an understanding of comorbidities can significantly contribute to improvement in HFpEF patients’ outcomes [27].
HFpEF and Hypertension
Chronic maladaptive neurohumoral activation leading to sustained systemic arterial hypertension has been implicated in the course of HFpEF [54]. Studies have shown that systemic hypertension is a critical determinant of outcome in HFpEF as it plays a crucial role in the onset and maintenance of a proinflammatory state, arterial stiffness, ventricular hypertrophy, titin-dependent stiffness, and dysfunction [55–57]. In patients with HFpEF, control of hypertension can induce regression of myocardial mass and improve cardiac function and relaxation as well as clinical outcomes [58, 59]. Thus, if concomitant hypertensive disease exists, it is crucial to introduce medical therapy in order to achieve lower blood pressure targets and prevent the untoward complications of increased afterload [56, 60]. According to ALLHAT trial, HFpEF patients have a more favorable prognosis than HFrEF counterparts, even among high-risk hypertensive patients [61, 62].
HFpEF and Amyloidosis
Two types of amyloid commonly infiltrate the myocardium—immunoglobulin light chain (AL or primary systemic) amyloid and transthyretin (TTR) amyloid. Transthyretin-related amyloidoses (ATTR) may be either hereditary (caused by autosomal dominant mutations in the TTR gene) or acquired (due to misaggregation of wild-type transthyretin). ATTR amyloidosis is an increasingly common cause of HFpEF and must be excluded in patients suspected of HF [63, 64]. The amyloid is deposited in the myocardium and/or peripheral nervous system [65]. The most common cardiac symptoms are dyspnea, angina, edema, and syncope [66]. Non-cardiac manifestations include peripheral neuropathy, characterized by symptoms of neuropathic pain, numbness, and loss of muscle strength in the lower extremities. Gastrointestinal symptoms such as diarrhea and weight loss result as a consequence of autonomic neuropathy or autonomic nerve dysfunction of unknown etiology [67, 68]. Other autonomic manifestations include erectile dysfunction, orthostatic hypotension, and neurogenic bladder [69]. In addition, symptoms such as lumbar spinal stenosis may appear [70, 71]. Distal biceps tendon spontaneous rupture is also common in patients with transthyretin cardiac amyloidosis [72]. Ando et al. have also reported vitreous body inclusions of the cotton wool type, which are pathognomonic for ATTR amyloidosis [69]. Carpal tunnel syndrome (CTS) is an early presenting sign of disease, preceding the onset of HF by up to 5–9 years [73]. The prevalence of ATTR amyloidosis among patients with CTS is 7–8%, compared to 4–5% in the general population [74, 75]. CTS manifests as pain and sensory disturbances in the lateral distribution of the hand, as well as hand weakness observed in cases of severe focal neuropathy [76]. Biopsy and histopathologic analysis used to be required to identify amyloidosis. Congo red or Direct Fast Scarlet 4BS staining binds to amyloid fibrils and characteristic apple-green birefringence under polarized light microscopy is noted. However, imaging techniques as well as genetic testing are becoming increasingly important [77–79]. Echocardiography and cardiac magnetic resonance may reveal features suggestive of amyloidosis, such as thickened LV wall, atrial septum and valves, small LV cavity size, biatrial enlargement, elevated RV systolic pressure, granular sparkling appearance of the myocardial wall, pericardial effusion, restrictive filling pattern, and reduced ventricular strain with relative apical sparing pattern. However, it is not sufficient for the diagnosis [80–83]. Nuclear imaging techniques employing technetium-99 (99mTc) labeled diphosphonopropanodicarboxylic acid (99mTc-DPD), pyrophosphate (99mTc-PYP), or methylenediphosphonic acid (99mTc-MDP), once used as a bone scintigraphy, provide a novel, non-invasive diagnostic approach with relatively high sensitivity (> 90%) and specificity (86%) [84, 85]. Intense uptake of 99mTc-DPD in the myocardium with lower or absent uptake in the bones suggests ATTR amyloidosis. Positive bone scintigraphy in patients without monoclonal gammopathy characterizes 100% specificity [86]. It enables to establish the diagnosis without the need of histology [84].
Treatment
There is no evidence that medications, which are known to be effective at alleviating symptom burden and reducing mortality in patients with HFrEF, are equally effective for patients with HFpEF. It may be due to the disparateness of the disease as well as multifactorial pathophysiology of the disease [87]. The number of available clinical trials on the treatment of HFpEF is finite. Currently, angiotensin-converting enzyme blockers (ACEIs), angiotensin receptor blockers (ARBs), calcium channel blockers (CCBs), and beta-blockers are given to these patients, although trials with perindopril, candesartan, irbesartan, and nebivolol did not show a clear advantage over placebo [88–93]. On the contrary, spironolactone may be effective in HFpEF treatment. The TOPCAT randomized double-blinded study had as its aim to determine what effect spironolactone would have on HFpEF in regard to mortality. It was found that it did not impact the time until first hospitalization for HF exacerbation nor did it have an influence on mortality. Post hoc analysis of the TOPCAT study showed however that the hospitalization rate of patients randomized to spironolactone was reduced by 17%. The authors of the study go on to state that clinicians wanting to utilize spironolactone in the subpopulation of HF patients should be cognizant of the potential for hyperkalemia and increased serum creatinine, necessitating regular monitoring while on therapy [94]. Although sacubitril/valsartan is highly beneficial in the treatment of HFrEF patients, the PARAGON-HF trial revealed that it does not significantly lower the rate of total hospitalizations for heart failure and death from cardiovascular causes among these patients [95]. It has been hypothesized that the administration of short-term nitrate or inorganic nitrite may promote nitric oxide signaling, thus enhancing aerobic ability in patients with HFpEF. However, the administration of inhaled inorganic nitrite for 4 weeks, compared to placebo, also did not result in significant improvement in exercise capacity [96]. On the other hand, according to Nochioka et al., the treatment of HFpEF with statins reduces mortality [97]. Recent data reveal that anti-diabetic and anti-inflammatory drugs, anti-fibrotic and high-density lipoprotein-raising strategies, microRNases, mitochondrial-targeted anti-oxidants, and therapeutic options may be promising, although these warrant further investigations [98].
Interestingly, therapy with chlorthalidone has been found to prevent the occurrence of new-onset HFpEF in hypertensive patients [61]. Furthermore, in those subjects, ACEIs have shown promising results, namely lower blood pressure, decreased frequency of HF-related hospitalizations, improved exercise capacity, and diastolic function [56, 99].
The treatment of TTR amyloidosis is based on tafamidis, a drug that has been approved for use in patients with TTR polyneuropathy. In this condition, it has a significant impact on reducing symptoms and stabilizing TTR tetramers, and has been well-tolerated [100]. Findings from the ATTR-ACT study on ATTR cardiomyopathy show that tafamidis is associated with reduced mortality and cardiovascular-related hospitalizations. There are major benefits from the treatment if used in the early stage of the disease because of a reduction in the decline in functional capacity [101].
Emphasis is now being placed on the benefit of exercise therapy for patients with heart failure. This is in direct response to exercise intolerance being the primary symptom of patients with chronic HF and a major factor decreasing quality of life (QOL) in these patients [102]. Studies comparing endurance training in patients with HFpEF and HFrEF have shown a 19% improvement in peak VO2 in HFpEF after 12 weeks of exercise therapy. In contrast, no improvement was observed in the group with HFrEF [103]. The InterAtrial Shunt Device (IASD®), which reduces the elevated left atrial pressures, may also be promising [104, 105].
Due to the complex pathophysiology of HFpEF, multiple treatment strategies are still needed and will be required to target specific mechanisms of disease. As described in the Framingham Heart and the Cardiovascular Health Studies, the incidence of HFrEF has been declining (p = 0.0029), while the incidence of HFpEF is on the rise (p < 0.001). These trends were noticed from 1990 to 2009 [106]. It is necessary to discover the pathomechanisms responsible for this divergent trend. Until we are familiar with the pathways involved in this multifactorial disease, we can only recommend medications for our patients, which are known to work in other subtypes of HF. Needless to say, therefore, the treatment of comorbidities is of utmost importance. Recent data suggest that heart failure disease management programs may improve mortality, number of hospitalizations, self-care, and quality of life [107, 108]. However, it must be emphasized that there is currently no evidence-based therapy for HFpEF [109].
Prognosis
Some sources report that both HF groups have similar outcomes, prognosis, and survival [8, 9, 110, 111]. On the contrary, the other studies point out that patients with HFpEF have a much better prognosis than patients with HFrEF [112, 113]. Somaratne et al. suggest that the survival rate of people with HFpEF is 50% higher compared to patients with HFrEF [114]. Although survival in HFrEF has significantly improved over the past decade, the prognosis of patients with HFpEF has not shown any notable change within the same time period despite the use of similar pharmacotherapy. The annual mortality of HFpEF patients in the USA is 8–12% [115]. In a major observational study, 5-year survival rate of HFpEF patients after hospitalization for HF was only 35–40%. Lack of evidence-based therapeutic strategies may play a pivotal role in curbing high rates of mortality and morbidity in HFpEF [8].
The identified prognostic factors in patients with HFpEF are as follows:
Cystatin C (high serum level confers worse prognosis)
B-type natriuretic peptide
NT-proBNP
Diabetes
Compared to patients with HFrEF, patients with HFpEF show lower levels of both B-type natriuretic peptide and NT-proBNP. However, in both cases, they are an important prognostic factor [123, 124]. Factors such as reduced LV compliance and remodeling of right ventricle (RV) also have prognostic significance, adversely affecting the prognosis [125]. Other factors that worsen prognosis are the coexistence of ischemic heart disease, diabetes mellitus, and chronic renal failure [22, 126].
Summary
Heart failure with preserved ejection fraction (HFpEF) is defined by a left ventricular ejection fraction ≥ 50% in the presence of clinical signs and/or symptoms of heart failure, diastolic dysfunction, or structural abnormality of the left ventricle (LV). However, the system of classifying HF according to LVEF has been recently challenged. Symptoms classically associated with HF include dyspnea, paroxysmal nocturnal dyspnea, orthopnea, and fatigue. Natriuretic peptides are elevated.
The most common underlying causes of the disease are coronary artery disease, valvular heart disease, and hypertension, while the most common comorbidities in this population include obesity, diabetes, atrial fibrillation, metabolic syndrome, chronic obstructive pulmonary disease, sleep-disordered breathing, renal dysfunction, and anemia. Amyloidosis, specifically ATTR amyloidosis, is also an increasingly common cause of HFpEF and must be excluded in patients suspected of HF. While the pathophysiology of HFpEF is still being uncovered, the role of systemic low-grade inflammation and microvascular damage related to endothelial dysfunction, oxidative stress, and myocardial remodeling and fibrosis seem to be important components. As the percentage of HFpEF grows, relative to all cases of HF, it is a diagnosis, which clinicians need to be cognizant of.
Due to the fact that several pathophysiological processes may lead to dyspnea, the differential diagnosis is necessary to exclude the non-cardiac etiologies. Not all cases of HFpEF will present acutely. To screen for subclinical heart failure risk, the H2FPEF score and the HFpEF nomogram may be utilized. As there may be other diseases that mimic or share clinical characteristics, diagnostic algorithms are useful in making the diagnosis of HFpEF. The existence of different phenotypes of HFpEF becomes important when deciding which diagnostic strategies to employ.
Currently there is no proven pharmacotherapy specifically for HFpEF. Current pharmacotherapy includes angiotensin-converting enzyme inhibitors/aldosterone receptor blockers (ACE-inhibitors/ARBs), calcium channel blockers (CCBs), and beta-blockers. These medications are being used among HFpEF patients because of the high cardiovascular risk and concomitant diseases seen in this population. Treatment with spironolactone, however, seems to be promising. Finally, exercise therapy is being studied for its possible role in the treatment of these patients.
Due to a lack of evidence-based treatment strategies for HFpEF, the mortality and morbidity associated with the disease have remained high. The 5-year survival rate among patients with HFpEF is 35–40% after hospitalization. Further studies, especially with the use of machine learning, are warranted to investigate other underlying processes that lead to HFpEF as well as targeted pharmacotherapy for patients with HFpEF.
Compliance with Ethical Standards
Conflict of Interest
The authors declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Footnotes
This article is part of the Topical Collection on Heart Failure
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Daria M. Adamczak, Email: daria.m.adamczak@gmail.com, Email: daria.adamczak@skpp.edu.pl
Mary-Tiffany Oduah, Email: dobezemd@gmail.com.
Thomas Kiebalo, Email: thomas.kiebalo@gmail.com.
Sonia Nartowicz, Email: sonianartowicz@gmail.com.
Marcin Bęben, Email: marcin398@gmail.com.
Mateusz Pochylski, Email: pochylskimateusz@gmail.com.
Aleksandra Ciepłucha, Email: ola.cieplucha@gmail.com.
Adrian Gwizdała, Email: adrian.gwizdala@gmail.com.
Maciej Lesiak, Email: maciej.lesiak@skpp.edu.pl.
Ewa Straburzyńska-Migaj, Email: ewa.straburzynska-migaj@skpp.edu.pl.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
- 1.Savarese G, Lund LH. Global public health burden of heart failure. Card Fail Rev. 2017;3:7–11. doi: 10.15420/cfr.2016:25:2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ziaeian B, Fonarow GC. Epidemiology and aetiology of heart failure. Nat Rev Cardiol. 2016;13:368–378. doi: 10.1038/nrcardio.2016.25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P, ESC Scientific Document Group 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37:2129–2200. doi: 10.1093/eurheartj/ehw128. [DOI] [PubMed] [Google Scholar]
- 4.Luchi RJ, Snow E, Luchi JM, Nelson CL, Pircher FJ. Left ventricular function in hospitalized geriatric patients. J Am Geriatr Soc. 1982;30:700–705. doi: 10.1111/j.1532-5415.1982.tb01983.x. [DOI] [PubMed] [Google Scholar]
- 5.Webb J, Fovargue L, Tøndel K, Porter B, Sieniewicz B, Gould J, Rinaldi CA, Ismail T, Chiribiri A, Carr-White G. The emerging role of cardiac magnetic resonance imaging in the evaluation of patients with HFpEF. Current Heart Failure Reports. 2018;15:1–9. doi: 10.1007/s11897-018-0372-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Singh A, Mehta Y. Heart failure with preserved ejection fraction (HFpEF): implications for the anesthesiologists. J Anaesthesiol Clin Pharmacol. 2018;34:161–165. doi: 10.4103/joacp.JOACP_352_16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Triposkiadis F, Butler J, Abboud FM, Armstrong PW, Adamopoulos S, Atherton JJ, et al. The continuous heart failure spectrum: moving beyond an ejection fraction classification. Eur Heart J. 2019;40:2155–2163. doi: 10.1093/eurheartj/ehz158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–259. doi: 10.1056/NEJMoa052256. [DOI] [PubMed] [Google Scholar]
- 9.Abebe TB, Gebreyohannes EA, Tefera YG, Abegaz TM. Patients with HFpEF and HFrEF have different clinical characteristics but similar prognosis: a retrospective cohort study. BMC Cardiovasc Disord. 2016;16. 10.1186/s12872-016-0418-9. [DOI] [PMC free article] [PubMed]
- 10.Borlaug BA, Paulus WJ. Heart failure with preserved ejection fraction: pathophysiology, diagnosis, and treatment. Eur Heart J. 2011;32:670–679. doi: 10.1093/eurheartj/ehq426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Edelmann F. Facts and numbers on epidemiology and pharmacological treatment of heart failure with preserved ejection fraction. ESC Heart Fail. 2015;2:41–45. doi: 10.1002/ehf2.12037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Dunlay SM, Roger VL, Redfield MM. Epidemiology of heart failure with preserved ejection fraction. Nat Rev Cardiol. 2017;14:591–602. doi: 10.1038/nrcardio.2017.65. [DOI] [PubMed] [Google Scholar]
- 13.Duca F, Zotter-Tufaro C, Kammerlander AA, Aschauer S, Binder C, Mascherbauer J, Bonderman D. Gender-related differences in heart failure with preserved ejection fraction. Sci Rep. 2018;8:1080. doi: 10.1038/s41598-018-19507-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Silverman MG, Patel B, Blankstein R, Lima JAC, Blumenthal RS, Nasir K, Blaha MJ. Impact of race, ethnicity, and multimodality biomarkers on the incidence of new-onset heart failure with preserved ejection fraction (from the Multi-Ethnic Study of Atherosclerosis) Am J Cardiol. 2016;117:1474–1481. doi: 10.1016/j.amjcard.2016.02.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Meta-analysis Global Group in Chronic Heart Failure (MAGGIC) The survival of patients with heart failure with preserved or reduced left ventricular ejection fraction: an individual patient data meta-analysis. Eur Heart J. 2012;33:1750–1757. doi: 10.1093/eurheartj/ehr254. [DOI] [PubMed] [Google Scholar]
- 16.Lee DS, Gona P, Vasan RS, Larson MG, Benjamin EJ, Wang TJ, Tu JV, Levy D. Relation of disease pathogenesis and risk factors to heart failure with preserved or reduced ejection fraction: insights from the Framingham Heart Study of the National Heart, Lung, and Blood Institute. Circulation. 2009;119:3070–3077. doi: 10.1161/CIRCULATIONAHA.108.815944. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ho KK, Anderson KM, Kannel WB, Grossman W, Levy D. Survival after the onset of congestive heart failure in Framingham Heart Study subjects. Circulation. 1993;88:107–115. doi: 10.1161/01.CIR.88.1.107. [DOI] [PubMed] [Google Scholar]
- 18.Rech M, Barandiarán Aizpurua A, van Empel V, van Bilsen M, Schroen B. Pathophysiological understanding of HFpEF: microRNAs as part of the puzzle. Cardiovasc Res. 2018;114:782–793. doi: 10.1093/cvr/cvy049. [DOI] [PubMed] [Google Scholar]
- 19.Reddy YNV, Carter RE, Obokata M, Redfield MM, Borlaug BA. A simple, evidence-based approach to help guide diagnosis of heart failure with preserved ejection fraction. Circulation. 2018;138:861–870. doi: 10.1161/CIRCULATIONAHA.118.034646. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Mayet J, Hughes A. Cardiac and vascular pathophysiology in hypertension. Heart. 2003;89:1104–1109. doi: 10.1136/heart.89.9.1104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Unger ED, Dubin RF, Deo R, Daruwalla V, Friedman JL, Medina C, Beussink L, Freed BH, Shah SJ. Association of chronic kidney disease with abnormal cardiac mechanics and adverse outcomes in patients with heart failure and preserved ejection fraction: CKD and cardiac mechanics in HFpEF. Eur J Heart Fail. 2016;18:103–112. doi: 10.1002/ejhf.445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kristensen SL, Mogensen UM, Jhund PS, Petrie MC, Preiss D, Win S, Køber L, McKelvie RS, Zile MR, Anand IS, Komajda M, Gottdiener JS, Carson PE, McMurray JJV. Clinical and echocardiographic characteristics and cardiovascular outcomes according to diabetes status in patients with heart failure and preserved ejection fraction: a report from the I-Preserve Trial (Irbesartan in Heart Failure With Preserved Ejection Fraction) Circulation. 2017;135:724–735. doi: 10.1161/CIRCULATIONAHA.116.024593. [DOI] [PubMed] [Google Scholar]
- 23.Lindman BR, Dávila-Román VG, Mann DL, McNulty S, Semigran MJ, Lewis GD, et al. Cardiovascular phenotype in HFpEF patients with or without diabetes. J Am Coll Cardiol. 2014;64:541–549. doi: 10.1016/j.jacc.2014.05.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, et al. ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure): developed in collaboration with the American College of Chest Physicians and the International Society for Heart and Lung Transplantation: endorsed by the Heart Rhythm Society. Circulation. 2005;112:e154–e235. doi: 10.1161/CIRCULATIONAHA.105.167586. [DOI] [PubMed] [Google Scholar]
- 25.Redfield MM, Jacobsen SJ, Burnett JC, Mahoney DW, Bailey KR, Rodeheffer RJ. Burden of systolic and diastolic ventricular dysfunction in the community: appreciating the scope of the heart failure epidemic. JAMA. 2003;289:194–202. doi: 10.1001/jama.289.2.194. [DOI] [PubMed] [Google Scholar]
- 26.Zafrir B, Lund LH, Laroche C, Ruschitzka F, Crespo-Leiro MG, Coats AJS, Anker SD, Filippatos G, Seferovic PM, Maggioni AP, de Mora Martin M, Polonski L, Silva-Cardoso J, Amir O, ESC-HFA HF Long-Term Registry Investigators Prognostic implications of atrial fibrillation in heart failure with reduced, mid-range, and preserved ejection fraction: a report from 14 964 patients in the European Society of Cardiology Heart Failure Long-Term Registry. Eur Heart J. 2018;39:4277–4284. doi: 10.1093/eurheartj/ehy626. [DOI] [PubMed] [Google Scholar]
- 27.Mentz RJ, Kelly JP, von Lueder TG, Voors AA, Lam CSP, Cowie MR, Kjeldsen K, Jankowska EA, Atar D, Butler J, Fiuzat M, Zannad F, Pitt B, O’Connor CM. Noncardiac comorbidities in heart failure with reduced versus preserved ejection fraction. J Am Coll Cardiol. 2014;64:2281–2293. doi: 10.1016/j.jacc.2014.08.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Andersen MJ, Borlaug BA. Heart failure with preserved ejection fraction: current understandings and challenges. Curr Cardiol Rep. 2014;16. 10.1007/s11886-014-0501-8. [DOI] [PubMed]
- 29.Gottdiener JS. Outcome of congestive heart failure in elderly persons: influence of left ventricular systolic function: the Cardiovascular Health Study. Ann Intern Med. 2002;137:631. doi: 10.7326/0003-4819-137-8-200210150-00006. [DOI] [PubMed] [Google Scholar]
- 30.van Empel V, Brunner-La Rocca H-P. Inflammation in HFpEF: key or circumstantial? Int J Cardiol. 2015;189:259–263. doi: 10.1016/j.ijcard.2015.04.110. [DOI] [PubMed] [Google Scholar]
- 31.Su M-YM, Lin L-Y, Tseng Y-HE, Chang C-C, Wu C-K, Lin J-L, et al. CMR-verified diffuse myocardial fibrosis is associated with diastolic dysfunction in HFpEF. JACC Cardiovasc Imaging. 2014;7:991–997. doi: 10.1016/j.jcmg.2014.04.022. [DOI] [PubMed] [Google Scholar]
- 32.Maruhashi T, Soga J, Fujimura N, Idei N, Mikami S, Iwamoto Y, Iwamoto A, Kajikawa M, Matsumoto T, Oda N, Kishimoto S, Matsui S, Hashimoto H, Aibara Y, Yusoff FBM, Hidaka T, Kihara Y, Chayama K, Noma K, Nakashima A, Goto C, Tomiyama H, Takase B, Kohro T, Suzuki T, Ishizu T, Ueda S, Yamazaki T, Furumoto T, Kario K, Inoue T, Koba S, Watanabe K, Takemoto Y, Hano T, Sata M, Ishibashi Y, Node K, Maemura K, Ohya Y, Furukawa T, Ito H, Ikeda H, Yamashina A, Higashi Y. Endothelial function is impaired in patients receiving antihypertensive drug treatment regardless of blood pressure level: FMD-J study (Flow-Mediated Dilation Japan) Hypertension. 2017;70:790–797. doi: 10.1161/HYPERTENSIONAHA.117.09612. [DOI] [PubMed] [Google Scholar]
- 33.Nair N, Gupta S, Collier IX, Gongora E, Vijayaraghavan K. Can microRNAs emerge as biomarkers in distinguishing HFpEF versus HFrEF? Int J Cardiol. 2014;175:395–399. doi: 10.1016/j.ijcard.2014.06.027. [DOI] [PubMed] [Google Scholar]
- 34.Curl CL, Danes VR, Bell JR, Raaijmakers AJA, Ip WTK, Chandramouli C, et al. Cardiomyocyte functional etiology in heart failure with preserved ejection fraction is distinctive—a new preclinical model. J Am Heart Assoc. 2018;7. 10.1161/JAHA.117.007451. [DOI] [PMC free article] [PubMed]
- 35.Paulus WJ. H 2 FPEF score: at last, a properly validated diagnostic algorithm for heart failure with preserved ejection fraction. Circulation. 2018;138:871–873. doi: 10.1161/CIRCULATIONAHA.118.035711. [DOI] [PubMed] [Google Scholar]
- 36.Sharma K, Kass DA. Heart failure with preserved ejection fraction: mechanisms, clinical features, and therapies. Circ Res. 2014;115:79–96. doi: 10.1161/CIRCRESAHA.115.302922. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Zakeri R, Cowie MR. Heart failure with preserved ejection fraction: controversies, challenges and future directions. Heart. 2018;104:377–384. doi: 10.1136/heartjnl-2016-310790. [DOI] [PubMed] [Google Scholar]
- 38.Huis in ’t Veld AE, de Man FS, van Rossum AC, Handoko ML. How to diagnose heart failure with preserved ejection fraction: the value of invasive stress testing. Neth Hear J. 2016;24:244–251. doi: 10.1007/s12471-016-0811-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Shah SJ. 20th Annual Feigenbaum Lecture: echocardiography for precision medicine-digital biopsy to deconstruct biology. J Am Soc Echocardiogr. 2019;32:1379–1395.e2. doi: 10.1016/j.echo.2019.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Shah SJ, Aistrup GL, Gupta DK, O’Toole MJ, Nahhas AF, Schuster D, et al. Ultrastructural and cellular basis for the development of abnormal myocardial mechanics during the transition from hypertension to heart failure. Am J Physiol Heart Circ Physiol. 2014;306:H88–100. doi: 10.1152/ajpheart.00642.2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Thomas L, Marwick TH, Popescu BA, Donal E, Badano LP. Left atrial structure and function, and left ventricular diastolic dysfunction. J Am Coll Cardiol. 2019;73:1961–1977. doi: 10.1016/j.jacc.2019.01.059. [DOI] [PubMed] [Google Scholar]
- 42.Oh JK, Hatle L, Tajik AJ, Little WC. Diastolic heart failure can be diagnosed by comprehensive two-dimensional and Doppler echocardiography. J Am Coll Cardiol. 2006;47:500–506. doi: 10.1016/j.jacc.2005.09.032. [DOI] [PubMed] [Google Scholar]
- 43.Shah SJ, Kitzman DW, Borlaug BA, van Heerebeek L, Zile MR, Kass DA, et al. Phenotype-specific treatment of heart failure with preserved ejection fraction: a multiorgan roadmap. Circulation. 2016;134:73–90. doi: 10.1161/CIRCULATIONAHA.116.021884. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Shah SJ, Katz DH, Deo RC. Phenotypic spectrum of heart failure with preserved ejection fraction. Heart Fail Clin. 2014;10:407–418. doi: 10.1016/j.hfc.2014.04.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Lewis GA, Schelbert EB, Williams SG, Cunnington C, Ahmed F, McDonagh TA, et al. Biological phenotypes of heart failure with preserved ejection fraction. J Am Coll Cardiol. 2017;70:2186–2200. doi: 10.1016/j.jacc.2017.09.006. [DOI] [PubMed] [Google Scholar]
- 46.Cohen JB, Schrauben SJ, Zhao L, Basso MD, Cvijic ME, Li Z, et al. Clinical phenogroups in heart failure with preserved ejection fraction. JACC: Heart Failure. 2020;8:172–184. doi: 10.1016/j.jchf.2019.09.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Samson R, Jaiswal A, Ennezat PV, Cassidy M, Le Jemtel TH. Clinical phenotypes in heart failure with preserved ejection fraction. J Am Heart Assoc. 2016;5. 10.1161/JAHA.115.002477. [DOI] [PMC free article] [PubMed]
- 48.Shah SJ, Katz DH, Selvaraj S, Burke MA, Yancy CW, Gheorghiade M, Bonow RO, Huang CC, Deo RC. Phenomapping for novel classification of heart failure with preserved ejection fraction. Circulation. 2015;131:269–279. doi: 10.1161/CIRCULATIONAHA.114.010637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Wachter R, Edelmann F. Diagnosis of heart failure with preserved ejection fraction. Heart Fail Clin. 2014;10:399–406. doi: 10.1016/j.hfc.2014.04.010. [DOI] [PubMed] [Google Scholar]
- 50.Paulus WJ, Tschöpe C, Sanderson JE, Rusconi C, Flachskampf FA, Rademakers FE, Marino P, Smiseth OA, de Keulenaer G, Leite-Moreira AF, Borbély A, Édes I, Handoko ML, Heymans S, Pezzali N, Pieske B, Dickstein K, Fraser AG, Brutsaert DL. How to diagnose diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society of Cardiology. Eur Heart J. 2007;28:2539–2550. doi: 10.1093/eurheartj/ehm037. [DOI] [PubMed] [Google Scholar]
- 51.Paulus WJ, Tschöpe C. A novel paradigm for heart failure with preserved ejection fraction. J Am Coll Cardiol. 2013;62:263–271. doi: 10.1016/j.jacc.2013.02.092. [DOI] [PubMed] [Google Scholar]
- 52.Gevaert AB, Boen JRA, Segers VF, Van Craenenbroeck EM. Heart failure with preserved ejection fraction: a review of cardiac and noncardiac pathophysiology. Front Physiol. 2019;10. 10.3389/fphys.2019.00638. [DOI] [PMC free article] [PubMed]
- 53.Jia G, Hill MA, Sowers JR. Diabetic cardiomyopathy: an update of mechanisms contributing to this clinical entity. Circ Res. 2018;122:624–638. doi: 10.1161/CIRCRESAHA.117.311586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Parasuraman SK, Loudon BL, Lowery C, Cameron D, Singh S, Schwarz K, et al. Diastolic ventricular interaction in heart failure with preserved ejection fraction. J Am Heart Assoc. 2019;8. 10.1161/JAHA.118.010114. [DOI] [PMC free article] [PubMed]
- 55.Tadic M, Cuspidi C, Frydas A, Grassi G. The role of arterial hypertension in development heart failure with preserved ejection fraction: just a risk factor or something more? Heart Fail Rev. 2018;23:631–639. doi: 10.1007/s10741-018-9698-8. [DOI] [PubMed] [Google Scholar]
- 56.Tam MC, Lee R, Cascino TM, Konerman MC, Hummel SL. Current perspectives on systemic hypertension in heart failure with preserved ejection fraction. Curr Hypertens Rep. 2017;19:12. doi: 10.1007/s11906-017-0709-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Lyle MA, Brozovich FV. HFpEF, a disease of the vasculature: a closer look at the other half. Mayo Clin Proc. 2018;93:1305–1314. doi: 10.1016/j.mayocp.2018.05.001. [DOI] [PubMed] [Google Scholar]
- 58.Heinzel FR, Hohendanner F, Jin G, Sedej S, Edelmann F. Myocardial hypertrophy and its role in heart failure with preserved ejection fraction. J Appl Physiol. 2015;119:1233–1242. doi: 10.1152/japplphysiol.00374.2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Nadruz W, Shah AM, Solomon SD. Diastolic dysfunction and hypertension. Med Clin N Am. 2017;101:7–17. doi: 10.1016/j.mcna.2016.08.013. [DOI] [PubMed] [Google Scholar]
- 60.Kjeldsen SE, von Lueder TG, Smiseth OA, Wachtell K, Mistry N, Westheim AS, Hopper I, Julius S, Pitt B, Reid CM, Devereux RB, Zannad F. Medical therapies for heart failure with preserved ejection fraction. Hypertension. 2020;75:23–32. doi: 10.1161/HYPERTENSIONAHA.119.14057. [DOI] [PubMed] [Google Scholar]
- 61.Davis BR, Kostis JB, Simpson LM, Black HR, Cushman WC, Einhorn PT, et al. Heart failure with preserved and reduced left ventricular ejection fraction in the antihypertensive and lipid-lowering treatment to prevent heart attack trial. Circulation. 2008;118:2259–2267. doi: 10.1161/CIRCULATIONAHA.107.762229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Jin C-N, Liu M, Sun J-P, Fang F, Wen Y-N, Yu C-M, et al. The prevalence and prognosis of resistant hypertension in patients with heart failure. PLoS One. 2014;9:e114958. doi: 10.1371/journal.pone.0114958. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Manolis AS, Manolis AA, Manolis TA, Melita H. Cardiac amyloidosis: an underdiagnosed/underappreciated disease. European Journal of Internal Medicine. 2019;67:1–13. doi: 10.1016/j.ejim.2019.07.022. [DOI] [PubMed] [Google Scholar]
- 64.Kapoor M, Rossor AM, Laura M, Reilly MM. Clinical presentation, diagnosis and treatment of TTR amyloidosis. J Neuromuscul Dis. 2019;6:189–199. doi: 10.3233/JND-180371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Siddiqi OK, Ruberg FL. Cardiac amyloidosis: an update on pathophysiology, diagnosis, and treatment. Trends in Cardiovascular Medicine. 2018;28:10–21. doi: 10.1016/j.tcm.2017.07.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Alkhawam H, Patel D, Nguyen J, Easaw SM, Al-Sadawi M, Syed U, et al. Cardiac amyloidosis: pathogenesis, clinical context, diagnosis and management options. Acta Cardiol. 2017;72:380–389. doi: 10.1080/00015385.2017.1335034. [DOI] [PubMed] [Google Scholar]
- 67.Shin SC, Robinson-Papp J. Amyloid neuropathies. Mount Sinai Journal of Medicine: A Journal of Translational and Personalized Medicine. 2012;79:733–748. doi: 10.1002/msj.21352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Rapezzi C, Merlini G, Quarta CC, Riva L, Longhi S, Leone O, Salvi F, Ciliberti P, Pastorelli F, Biagini E, Coccolo F, Cooke RMT, Bacchi-Reggiani L, Sangiorgi D, Ferlini A, Cavo M, Zamagni E, Fonte ML, Palladini G, Salinaro F, Musca F, Obici L, Branzi A, Perlini S. Systemic cardiac amyloidoses: disease profiles and clinical courses of the 3 main types. Circulation. 2009;120:1203–1212. doi: 10.1161/CIRCULATIONAHA.108.843334. [DOI] [PubMed] [Google Scholar]
- 69.Ando Y, Coelho T, Berk JL, Cruz MW, Ericzon B-G, Ikeda S, et al. Guideline of transthyretin-related hereditary amyloidosis for clinicians. Orphanet Journal of Rare Diseases. 2013;8:31. doi: 10.1186/1750-1172-8-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Yanagisawa A, Ueda M, Sueyoshi T, Okada T, Fujimoto T, Ogi Y, Kitagawa K, Tasaki M, Misumi Y, Oshima T, Jono H, Obayashi K, Hirakawa K, Uchida H, Westermark P, Ando Y, Mizuta H. Amyloid deposits derived from transthyretin in the ligamentum flavum as related to lumbar spinal canal stenosis. Mod Pathol. 2015;28:201–207. doi: 10.1038/modpathol.2014.102. [DOI] [PubMed] [Google Scholar]
- 71.Westermark P, Westermark GT, Suhr OB, Berg S. Transthyretin-derived amyloidosis: probably a common cause of lumbar spinal stenosis. Ups J Med Sci. 2014;119:223–228. doi: 10.3109/03009734.2014.895786. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Geller HI, Singh A, Alexander KM, Mirto TM, Falk RH. Association between ruptured distal biceps tendon and wild-type transthyretin cardiac amyloidosis. JAMA. 2017;318:962–963. doi: 10.1001/jama.2017.9236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Milandri A, Farioli A, Gagliardi C, Longhi S, Salvi F, Curti S, Foffi S, Caponetti AG, Lorenzini M, Ferlini A, Rimessi P, Mattioli S, Violante FS, Rapezzi C. Carpal tunnel syndrome in cardiac amyloidosis: implications for early diagnosis and prognostic role across the spectrum of aetiologies. Eur J Heart Fail. 2020;22:507–515. doi: 10.1002/ejhf.1742. [DOI] [PubMed] [Google Scholar]
- 74.Sperry BW, Reyes BA, Ikram A, Donnelly JP, Phelan D, Jaber WA, Shapiro D, Evans PJ, Maschke S, Kilpatrick SE, Tan CD, Rodriguez ER, Monteiro C, Tang WHW, Kelly JW, Seitz WH, Jr, Hanna M. Tenosynovial and cardiac amyloidosis in patients undergoing carpal tunnel release. J Am Coll Cardiol. 2018;72:2040–2050. doi: 10.1016/j.jacc.2018.07.092. [DOI] [PubMed] [Google Scholar]
- 75.Genova A, Dix O, Saefan A, Thakur M, Hassan A. Carpal tunnel syndrome: a review of literature. Cureus. 2020. 10.7759/cureus.7333. [DOI] [PMC free article] [PubMed]
- 76.Sekijima Y, Uchiyama S, Tojo K, Sano K, Shimizu Y, Imaeda T, Hoshii Y, Kato H, Ikeda SI. High prevalence of wild-type transthyretin deposition in patients with idiopathic carpal tunnel syndrome: a common cause of carpal tunnel syndrome in the elderly. Hum Pathol. 2011;42:1785–1791. doi: 10.1016/j.humpath.2011.03.004. [DOI] [PubMed] [Google Scholar]
- 77.Maurer MS, Elliott P, Comenzo R, Semigran M, Rapezzi C. Addressing common questions encountered in the diagnosis and management of cardiac amyloidosis. Circulation. 2017;135:1357–1377. doi: 10.1161/CIRCULATIONAHA.116.024438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Di Giovanni B, Gustafson D, Delgado DH. Amyloid transthyretin cardiac amyloidosis: diagnosis and management. Expert Rev Cardiovasc Ther. 2019;17:673–681. doi: 10.1080/14779072.2019.1662723. [DOI] [PubMed] [Google Scholar]
- 79.Gopal DM, Ruberg FL, Siddiqi OK. Impact of genetic testing in transthyretin (ATTR) cardiac amyloidosis. Current Heart Failure Reports. 2019;16:180–188. doi: 10.1007/s11897-019-00436-z. [DOI] [PubMed] [Google Scholar]
- 80.Martinez-Naharro A, Treibel TA, Abdel-Gadir A, Bulluck H, Zumbo G, Knight DS, et al. Magnetic resonance in transthyretin cardiac amyloidosis. J Am Coll Cardiol. 2017;70:466–477. doi: 10.1016/j.jacc.2017.05.053. [DOI] [PubMed] [Google Scholar]
- 81.Ruberg FL, Grogan M, Hanna M, Kelly JW, Maurer MS. Transthyretin amyloid cardiomyopathy. J Am Coll Cardiol. 2019;73:2872–2891. doi: 10.1016/j.jacc.2019.04.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Cappelli F, Baldasseroni S, Bergesio F, Perlini S, Salinaro F, Padeletti L, Attanà P, Paoletti Perini A, Moggi Pignone A, Grifoni E, Fabbri A, Marchionni N, Gensini GF, Perfetto F. Echocardiographic and biohumoral characteristics in patients with AL and TTR amyloidosis at diagnosis: AL and TTR amyloidosis characteristic. Clin Cardiol. 2015;38:69–75. doi: 10.1002/clc.22353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Maurer MS, Bokhari S, Damy T, Dorbala S, Drachman BM, Fontana M, Grogan M, Kristen AV, Lousada I, Nativi-Nicolau J, Cristina Quarta C, Rapezzi C, Ruberg FL, Witteles R, Merlini G. Expert consensus recommendations for the suspicion and diagnosis of transthyretin cardiac amyloidosis. Circ Heart Fail. 2019;12:e006075. doi: 10.1161/CIRCHEARTFAILURE.119.006075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Gillmore JD, Maurer MS, Falk RH, Merlini G, Damy T, Dispenzieri A, Wechalekar AD, Berk JL, Quarta CC, Grogan M, Lachmann HJ, Bokhari S, Castano A, Dorbala S, Johnson GB, Glaudemans AWJM, Rezk T, Fontana M, Palladini G, Milani P, Guidalotti PL, Flatman K, Lane T, Vonberg FW, Whelan CJ, Moon JC, Ruberg FL, Miller EJ, Hutt DF, Hazenberg BP, Rapezzi C, Hawkins PN. Nonbiopsy diagnosis of cardiac transthyretin amyloidosis. Circulation. 2016;133:2404–2412. doi: 10.1161/CIRCULATIONAHA.116.021612. [DOI] [PubMed] [Google Scholar]
- 85.Treglia G, Glaudemans AWJM, Bertagna F, Hazenberg BPC, Erba PA, Giubbini R, Ceriani L, Prior JO, Giovanella L, Slart RHJA. Diagnostic accuracy of bone scintigraphy in the assessment of cardiac transthyretin-related amyloidosis: a bivariate meta-analysis. Eur J Nucl Med Mol Imaging. 2018;45:1945–1955. doi: 10.1007/s00259-018-4013-4. [DOI] [PubMed] [Google Scholar]
- 86.Perugini E, Guidalotti PL, Salvi F, Cooke RMT, Pettinato C, Riva L, Leone O, Farsad M, Ciliberti P, Bacchi-Reggiani L, Fallani F, Branzi A, Rapezzi C. Noninvasive etiologic diagnosis of cardiac amyloidosis using 99m Tc-3,3-diphosphono-1,2-propanodicarboxylic acid scintigraphy. J Am Coll Cardiol. 2005;46:1076–1084. doi: 10.1016/j.jacc.2005.05.073. [DOI] [PubMed] [Google Scholar]
- 87.Ilieșiu AM, Hodorogea AS. Treatment of heart failure with preserved ejection fraction. Adv Exp Med Biol. 2018;1067:67–87. doi: 10.1007/5584_2018_149. [DOI] [PubMed] [Google Scholar]
- 88.Yamamoto K. Pharmacological treatment of heart failure with preserved ejection fraction. Yonago Acta Med. 2017;60:71–76. doi: 10.33160/yam.2017.06.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Kanwar M, Walter C, Clarke M, Patarroyo-Aponte M. Targeting heart failure with preserved ejection fraction: current status and future prospects. Vasc Health Risk Manag. 2016;12:129–141. doi: 10.2147/VHRM.S83662. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Cleland JGF, Tendera M, Adamus J, Freemantle N, Polonski L, Taylor J, et al. The perindopril in elderly people with chronic heart failure (PEP-CHF) study. Eur Heart J. 2006;27:2338–2345. doi: 10.1093/eurheartj/ehl250. [DOI] [PubMed] [Google Scholar]
- 91.Massie BM, Carson PE, McMurray JJ, Komajda M, McKelvie R, Zile MR, et al. Irbesartan in patients with heart failure and preserved ejection fraction. N Engl J Med. 2008;359:2456–2467. doi: 10.1056/NEJMoa0805450. [DOI] [PubMed] [Google Scholar]
- 92.Yusuf S, Pfeffer MA, Swedberg K, Granger CB, Held P, McMurray JJV, et al. Effects of candesartan in patients with chronic heart failure and preserved left-ventricular ejection fraction: the CHARM-Preserved Trial. Lancet. 2003;362:777–781. doi: 10.1016/S0140-6736(03)14285-7. [DOI] [PubMed] [Google Scholar]
- 93.Flather MD, Shibata MC, Coats AJS, Van Veldhuisen DJ, Parkhomenko A, Borbola J, et al. Randomized trial to determine the effect of nebivolol on mortality and cardiovascular hospital admission in elderly patients with heart failure (SENIORS) Eur Heart J. 2005;26:215–225. doi: 10.1093/eurheartj/ehi115. [DOI] [PubMed] [Google Scholar]
- 94.Pitt B, Pfeffer MA, Assmann SF, Boineau R, Anand IS, Claggett B, et al. Spironolactone for heart failure with preserved ejection fraction. N Engl J Med. 2014;370:1383–1392. doi: 10.1056/NEJMoa1313731. [DOI] [PubMed] [Google Scholar]
- 95.Solomon SD, McMurray JJV, Anand IS, Ge J, Lam CSP, Maggioni AP, et al. Angiotensin–neprilysin inhibition in heart failure with preserved ejection fraction. N Engl J Med. 2019;381:1609–1620. doi: 10.1056/NEJMoa1908655. [DOI] [PubMed] [Google Scholar]
- 96.Borlaug BA, Anstrom KJ, Lewis GD, Shah SJ, Levine JA, Koepp GA, Givertz MM, Felker GM, LeWinter MM, Mann DL, Margulies KB, Smith AL, Tang WHW, Whellan DJ, Chen HH, Davila-Roman VG, McNulty S, Desvigne-Nickens P, Hernandez AF, Braunwald E, Redfield MM, for the National Heart, Lung, and Blood Institute Heart Failure Clinical Research Network Effect of inorganic nitrite vs placebo on exercise capacity among patients with heart failure with preserved ejection fraction: the INDIE-HFpEF randomized clinical trial. JAMA. 2018;320:1764–1773. doi: 10.1001/jama.2018.14852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Nochioka K, Sakata Y, Miyata S, Miura M, Takada T, Tadaki S, et al. Prognostic impact of statin use in patients with heart failure and preserved ejection fraction:—a report from the CHART-2 study—. Circ J. 2015;79:574–582. doi: 10.1253/circj.CJ-14-0865. [DOI] [PubMed] [Google Scholar]
- 98.Tschöpe C, Van Linthout S, Kherad B. Heart failure with preserved ejection fraction and future pharmacological strategies: a glance in the crystal ball. Curr Cardiol Rep. 2017;19:70. doi: 10.1007/s11886-017-0874-6. [DOI] [PubMed] [Google Scholar]
- 99.Kapelios CJ, Murrow JR, Nührenberg TG, Montoro Lopez MN. Effect of mineralocorticoid receptor antagonists on cardiac function in patients with heart failure and preserved ejection fraction: a systematic review and meta-analysis of randomized controlled trials. Heart Fail Rev. 2019;24:367–377. doi: 10.1007/s10741-018-9758-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Lamb YN, Deeks ED. Tafamidis: a review in transthyretin amyloidosis with polyneuropathy. Drugs. 2019;79:863–874. doi: 10.1007/s40265-019-01129-6. [DOI] [PubMed] [Google Scholar]
- 101.Maurer MS, Schwartz JH, Gundapaneni B, Elliott PM, Merlini G, Waddington-Cruz M, Kristen AV, Grogan M, Witteles R, Damy T, Drachman BM, Shah SJ, Hanna M, Judge DP, Barsdorf AI, Huber P, Patterson TA, Riley S, Schumacher J, Stewart M, Sultan MB, Rapezzi C, ATTR-ACT Study Investigators Tafamidis treatment for patients with transthyretin amyloid cardiomyopathy. N Engl J Med. 2018;379:1007–1016. doi: 10.1056/NEJMoa1805689. [DOI] [PubMed] [Google Scholar]
- 102.Fleg JL, Cooper LS, Borlaug BA, Haykowsky MJ, Kraus WE, Levine BD, et al. Exercise training as therapy for heart failure: current status and future directions. Circ Heart Fail. 2015;8:209–220. doi: 10.1161/CIRCHEARTFAILURE.113.001420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Pandey A, Kitzman DW, Brubaker P, Haykowsky MJ, Morgan T, Becton JT, Berry JD. Response to endurance exercise training in older adults with heart failure with preserved or reduced ejection fraction. J Am Geriatr Soc. 2017;65:1698–1704. doi: 10.1111/jgs.14867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Kosowski M, Kübler P, Kołodziej A, Krakowiak B, Kustrzycka-Kratochwil D, Sławin J, et al. InterAtrial Shunt Device (IASD®) implantation—a novel treatment method for heart failure with preserved ejection fraction. Kardiol Pol. 2017:736–41. 10.5603/KP.a2017.0096. [DOI] [PubMed]
- 105.Kaye DM, Petrie MC, McKenzie S, Hasenfuβ G, Malek F, Post M, Doughty RN, Trochu JN, Gustafsson F, Lang I, Kolodziej A, Westenfeld R, Penicka M, Rosenberg M, Hausleiter J, Raake P, Jondeau G, Bergmann MW, Spelman T, Aytug H, Ponikowski P, Hayward C, on behalf of the REDUCE LAP-HF study investigators Impact of an interatrial shunt device on survival and heart failure hospitalization in patients with preserved ejection fraction. ESC Heart Fail. 2019;6:62–69. doi: 10.1002/ehf2.12350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Tsao CW, Lyass A, Enserro D, Larson MG, Ho JE, Kizer JR, et al. Temporal trends in the incidence of and mortality associated with heart failure with preserved and reduced ejection fraction. JACC Heart Fail. 2018;6:678–685. doi: 10.1016/j.jchf.2018.03.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Kalogirou F, Forsyth F, Kyriakou M, Mantle R, Deaton C. Heart failure disease management: a systematic review of effectiveness in heart failure with preserved ejection fraction. ESC Heart Fail. 2020;7:195–213. doi: 10.1002/ehf2.12559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Shah SJ, Cogswell R, Ryan JJ, Sharma K. How to develop and implement a specialized heart failure with preserved ejection fraction clinical program. Curr Cardiol Rep. 2016;18:122. doi: 10.1007/s11886-016-0802-1. [DOI] [PubMed] [Google Scholar]
- 109.Roh J, Houstis N, Rosenzweig A. Why don’t we have proven treatments for HFpEF? Circ Res. 2017;120:1243–1245. doi: 10.1161/CIRCRESAHA.116.310119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Bhatia RS, Tu JV, Lee DS, Austin PC, Fang J, Haouzi A, et al. Outcome of heart failure with preserved ejection fraction in a population-based study. N Engl J Med. 2006;355:260–269. doi: 10.1056/NEJMoa051530. [DOI] [PubMed] [Google Scholar]
- 111.Edelmann F. Epidemiology and prognosis of heart failure. Herz. 2015;40:176–184. doi: 10.1007/s00059-015-4215-5. [DOI] [PubMed] [Google Scholar]
- 112.Meta-analysis Global Group in Chronic Heart Failure (MAGGIC) The survival of patients with heart failure with preserved or reduced left ventricular ejection fraction: an individual patient data meta-analysis. Eur Heart J. 2012;33:1750–1757. doi: 10.1093/eurheartj/ehr254. [DOI] [PubMed] [Google Scholar]
- 113.Kontogeorgos S, Thunström E, Johansson MC, Fu M. Heart failure with preserved ejection fraction has a better long-term prognosis than heart failure with reduced ejection fraction in old patients in a 5-year follow-up retrospective study. Int J Cardiol. 2017;232:86–92. doi: 10.1016/j.ijcard.2017.01.048. [DOI] [PubMed] [Google Scholar]
- 114.Somaratne JB, Berry C, McMurray JJV, Poppe KK, Doughty RN, Whalley GA. The prognostic significance of heart failure with preserved left ventricular ejection fraction: a literature-based meta-analysis. Eur J Heart Fail. 2009;11:855–862. doi: 10.1093/eurjhf/hfp103. [DOI] [PubMed] [Google Scholar]
- 115.Henning RJ. Diagnosis and treatment of heart failure with preserved left ventricular ejection fraction. World J Cardiol. 2020;12:7–25. doi: 10.4330/wjc.v12.i1.7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Chen S, Tang Y, Zhou X. Cystatin C for predicting all-cause mortality and rehospitalization in patients with heart failure: a meta-analysis. Biosci Rep. 2019;39. 10.1042/BSR20181761. [DOI] [PMC free article] [PubMed]
- 117.Kasahara S, Sakata Y, Nochioka K, Yamauchi T, Onose T, Tsuji K, et al. Comparable prognostic impact of BNP levels among HFpEF, borderline HFpEF and HFrEF: a report from the CHART-2 study. Heart Vessel. 2018;33:997–1007. doi: 10.1007/s00380-018-1150-4. [DOI] [PubMed] [Google Scholar]
- 118.Salah K, Stienen S, Pinto YM, Eurlings LW, Metra M, Bayes-Genis A, Verdiani V, Tijssen JGP, Kok WE. Prognosis and NT-proBNP in heart failure patients with preserved versus reduced ejection fraction. Heart. 2019;105:1182–1189. doi: 10.1136/heartjnl-2018-314173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Sandesara PB, O’Neal WT, Kelli HM, Samman-Tahhan A, Hammadah M, Quyyumi AA, et al. The prognostic significance of diabetes and microvascular complications in patients with heart failure with preserved ejection fraction. Diabetes Care. 2018;41:150–155. doi: 10.2337/dc17-0755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Carrasco-Sánchez FJ, Galisteo-Almeda L, Páez-Rubio I, Martínez-Marcos FJ, Camacho-Vázquez C, Ruiz-Frutos C, et al. Prognostic value of cystatin C on admission in heart failure with preserved ejection fraction. J Card Fail. 2011;17:31–38. doi: 10.1016/j.cardfail.2010.07.248. [DOI] [PubMed] [Google Scholar]
- 121.Tribouilloy C, Rusinaru D, Mahjoub H, Tartiere J-M, Kesri-Tartiere L, Godard S, Peltier M. Prognostic impact of diabetes mellitus in patients with heart failure and preserved ejection fraction: a prospective five-year study. Heart. 2008;94:1450–1455. doi: 10.1136/hrt.2007.128769. [DOI] [PubMed] [Google Scholar]
- 122.Izumiya Y, Hanatani S, Kimura Y, Takashio S, Yamamoto E, Kusaka H, et al. Growth differentiation factor-15 is a useful prognostic marker in patients with heart failure with preserved ejection fraction. Can J Cardiol. 2014;30:338–344. doi: 10.1016/j.cjca.2013.12.010. [DOI] [PubMed] [Google Scholar]
- 123.van Veldhuisen DJ, Linssen GCM, Jaarsma T, van Gilst WH, Hoes AW, Tijssen JGP, et al. B-type natriuretic peptide and prognosis in heart failure patients with preserved and reduced ejection fraction. J Am Coll Cardiol. 2013;61:1498–1506. doi: 10.1016/j.jacc.2012.12.044. [DOI] [PubMed] [Google Scholar]
- 124.Kang S-H, Park JJ, Choi D-J, Yoon C-H, Oh I-Y, Kang S-M, Yoo BS, Jeon ES, Kim JJ, Cho MC, Chae SC, Ryu KH, Oh BH, KorHF Registry Prognostic value of NT-proBNP in heart failure with preserved versus reduced EF. Heart. 2015;101:1881–1888. doi: 10.1136/heartjnl-2015-307782. [DOI] [PubMed] [Google Scholar]
- 125.Burke MA, Katz DH, Beussink L, Selvaraj S, Gupta DK, Fox J, Chakrabarti S, Sauer AJ, Rich JD, Freed BH, Shah SJ. Prognostic importance of pathophysiologic markers in patients with heart failure and preserved ejection fraction. Circ Heart Fail. 2014;7:288–299. doi: 10.1161/CIRCHEARTFAILURE.113.000854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Quirós López R, García Alegría J, Martín Escalante MD, Trujillo Santos J, Villena Ruiz MÁ, Perea ME. Factores pronósticos y supervivencia a largo plazo tras el diagnóstico inicial de insuficiencia cardiaca. Med Clin. 2012;138:602–608. doi: 10.1016/j.medcli.2011.03.031. [DOI] [PubMed] [Google Scholar]