

Abstract
Background
Staphylococcus aureus is the most common cause of acute hematogenous osteoarticular infections (AHOAIs) in children. The risk factors for the development of orthopedic complications (OC) after AHOAI are poorly understood. We sought to describe clinical and microbiologic variables present on the index admission that may predict OC in S. aureus AHOAI.
Methods
Staphylococcus aureus AHOAI cases were identified from 2011–2017 at Texas Children’s Hospital and reviewed for the development of OC. OC included chronic osteomyelitis, growth arrest, avascular necrosis, chronic dislocation, and pathologic fracture. All S. aureus isolates were characterized by pulsed-field gel electrophoresis and agr group.
Results
A total of 286 cases were examined of which 27 patients (9.4%) developed OC. Patients who developed OC more often had infection with an agr group III organism (P = .04), bacteremia (P = .04), delayed source control (P < .001), ≥2 surgical procedures (P < .001), intensive care unit admission (P = .09), and fever >4 days after admission (P = .008). There was no association with OC and patient age, methicillin resistance, or choice/route of antibiotics. In multivariable analyses of OC, infection with agr group III S. aureus, prolonged fever, and delayed source control remained statistically significant.
Conclusions
OC develop following S. aureus AHOAI in 9.4% of cases. Although the development of OC is likely multifactorial, agr group III organisms, prolonged fever, and delayed source control are independently associated with OC. Moreover, early aggressive surgical source control may be beneficial in children with S. aureus AHOAI.
Keywords: osteomyelitis, chronic osteomyelitis, source control, pediatric, agr III
Among children with Staphylococcus aureus acute hematogenous osteoarticular infections, orthopedic complications develop in 9.4%. The development of complications was associated with delayed source control, prolonged fever on the index admission, and infection with agr III strains.
Acute hematogenous osteoarticular infections (AHOAIs), which can be considered to include both osteomyelitis and septic arthritis, are among the most common indications for pediatric infectious diseases referral and have the potential to cause substantial morbidity. While a variety of pathogens can cause AHOAI, overwhelmingly the most frequently isolated organism is Staphylococcus aureus [1, 2]. Moreover, AHOAIs are the most common manifestation of invasive S. aureus infection in children [3].
Although most children treated for these infections have a good prognosis, a subset of patients will experience substantial long-term morbidity including chronic infection, pathologic fracture, angular deformity, and growth arrest. Chronic osteomyelitis has been reported to develop following <1%–9% of cases of acute osteomyelitis [2, 4, 5]. Pathologic fractures have been reported in approximately 5% of S. aureus osteomyelitis and are associated with the USA300.0114 pulsotype [6]. The development of sequelae in AHOAI has historically been believed to be related, at least in part, to inadequate or inappropriate treatment of acute infection [7, 8]. Early studies suggested that durations of therapy for acute osteomyelitis of <21 days were associated with an increased risk of development of chronic osteomyelitis [4]. Additionally, surgical drainage of bone abscesses when present is generally regarded as necessary and/or ideal. By contrast, studies conducted in Finland would suggest that a shortened duration of therapy coupled with fairly minimal surgical intervention can achieve good outcomes in children with osteomyelitis [9, 10]. There are, however, very little data examining this topic in a North American population. Moreover, very few studies address the impact of patient-level variables, medical and/or surgical treatment, or bacterial strain contributions on the likelihood of complications following AHOAI.
We sought to examine the outcomes of S. aureus AHOAI in children. Our goals were to better define the incidence of orthopedic sequelae and to correlate clinical and microbiologic data on the index admission with the likelihood of developing sequelae at last follow-up. We hypothesized that delayed or inadequate source control, inappropriate empiric therapy, and infection with virulent strain types would be associated with negative outcomes.
METHODS
Isolates and patients were identified from the database of the S. aureus surveillance study at Texas Children’s Hospital (TCH). Briefly, all S. aureus isolates identified by the clinical microbiology laboratory in the course of care are subcultured and stored in horse blood at –80°C in the Dr. Edward O Mason, Jr. Infectious Diseases Research Laboratory [11]. The database was searched for cases of S. aureus acute hematogenous osteomyelitis or septic arthritis from 1 January 2011 through 31 December 2017. Only cases of culture-confirmed S. aureus AHOAI with an associated viable S. aureus isolate were included in this study. Diagnosis of AHOAI was defined by the constellation of physical examination, radiology, and microbiological findings as previously described [1, 11, 12]. Patients with open or penetrating trauma, orthopedic hardware in place, or osteomyelitis secondary to a contiguous focus or a surgical procedure (such as sternal osteomyelitis after cardiac surgery) were excluded. Radiology reports were reviewed for this study; however, the images were not critically rereviewed. TCH has institutional clinical pathways to guide providers in the empiric management of AHOAI in children that recommend clindamycin for those with mild to moderate disease or vancomycin for those with moderate to severe disease, history of a clindamycin-resistant organism, or receipt of clindamycin in the recent past. In addition, both the Orthopedics and Infectious Diseases services are routinely consulted in cases of suspected AHOAI. Beyond these, however, all treatment decisions are individualized and at the discretion of the physician of record, including decisions regarding surgical intervention, final antibiotic choice, and decision to transition to oral antibiotics. Medical records were reviewed from admission until 30 August 2018 for outcomes of interest. The details of follow-up, microbiology/molecular biology techniques used [13–15], and the analytical plan are provided in the Supplementary Methods. The Baylor College of Medicine Institutional Review Board approved this study.
Definitions
Orthopedic complications included chronic osteomyelitis, pathologic fracture, growth arrest/limb length discrepancy, avascular necrosis, and/or chronic dislocation. To the best of our knowledge, no universally accepted definition for chronic osteomyelitis developing after AHOAI in children exists in the literature, with some authors relying on radiographic findings [5] and others using clinical diagnosis [2] or considering sequelae to include the need for additional surgical or medical therapies [9]. For this study, chronic osteomyelitis was considered to be the presence of any of the following after ≥4 weeks of effective antimicrobial therapy: the presence of a sequestrum or permeative lucencies in bone visible on plain radiographs [5, 8]; new or worsening pain, erythema, drainage, swelling, or loss of function [2]; or readmission for the treatment of AHOAI. The breadth of the criteria was intended to include both radiographic and clinical considerations. The time to initiation of effective antimicrobial therapy and time to surgical interventions were described in terms of hospital days from the time of admission. The extremes of certain continuous variables of interest were defined based on the >75th percentile for the study group; delayed source control was considered surgical intervention after hospital day 3; prolonged fever was regarded as >4 calendar days following hospital admission with a body temperature >100.4°F.
RESULTS
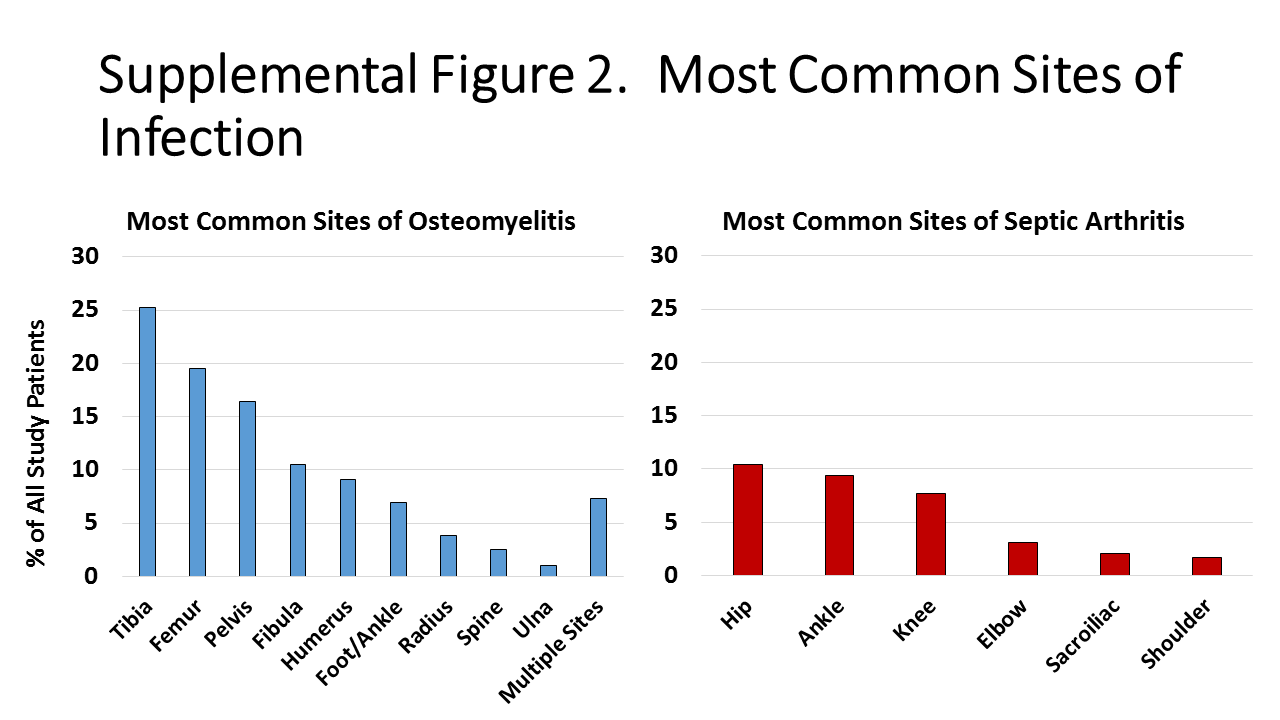
A total of 286 patients with corresponding viable S. aureus isolates met inclusion criteria (Supplementary Figure 1). The median age of patients was 8.4 years (interquartile range [IQR], 4.4–11.7 years; Table 1). A total of 160 patients (55.9%) had isolated osteomyelitis, while 96 (33.6%) had osteomyelitis with concomitant septic arthritis and 30 (10.5%) had isolated septic arthritis. In addition, 134 patients had a subperiosteal/intraosseous abscess (46.8%) and 207 (72.3%) underwent at least 1 surgical procedure; 155 cases were associated with bacteremia (54.2%) and 48 patients had ≥2 days of bacteremia (16.7%). Seventy-nine cases (27.6%) were caused by methicillin-resistant S. aureus (MRSA); cases caused by MRSA and methicillin-susceptible S. aureus (MSSA) are compared in Supplementary Table 1. The majority of infections involved the lower extremities or pelvis (Supplementary Figure 2).
Table 1.
General Characteristics and Associations of Orthopedic Complications and Patient Demographics and Disease Course
| Characteristic | All Patients (n = 286) |
Patients With Orthopedic Complications (n = 27) |
Patients Without Orthopedic Complications (n = 259) |
P Value |
|---|---|---|---|---|
| Median age, y (interquartile range)a | 8.4 (4.5–11.7) | 8.6 (6.2–12.2) | 8.3 (4.4–11.7) | .53 |
| Race | … | … | … | .94 |
| White | 207 (72.3) | 21 (77.8) | 186 (71.8) | … |
| Black | 59 (20.6) | 5 (18.5) | 54 (20.8) | … |
| Asian | 10 (3.5) | 1 (3.7) | 9 (3.5) | … |
| Native American | 1 (0.3) | 0 | 1 (0.4) | … |
| Pacific Islander | 1 (0.3) | 0 | 1 (0.4) | … |
| Hispanic Ethnicity | 99 (34.6) | 10 (37) | 89 (34.4) | .83 |
| Private insurance | 138 (48.3) | 11 (40.7) | 127 (49.1) | .4 |
| Manifestation of acute hematogenous osteoarticular infection | … | … | … | .56 |
| Isolated osteomyelitis | 160 (55.9) | 13 (48.1) | 147 (56.8) | … |
| Isolated septic arthritis | 30 (10.5) | 4 (14.8) | 26 (10.1) | … |
| Osteomyelitis and concomitant septic arthritis | 96 (33.6) | 10 (37) | 86 (33.2) | … |
| Multifocal infection | 21 (7.3) | 2 (7.4) | 19 (7.3) | 1 |
| Duration of symptoms on presentation, days | 5 (3–7) | 5 (3.5–7) | 4 (3–7) | .22 |
| Intraosseous/subperiosteal abscess | 134 (46.9) | 17 (62.9) | 117 (45.1) | .1 |
| Maximum abscess diameter, cmb | 3.7 (2–5.2) | 4.3 (2.1–7.5) | 3.7 (1.9–5) | .45 |
| Positive blood culture | 155 (54.2) | 20 (74.1) | 135 (52.1) | .04 |
| Duration of bacteremia, days | 1 (1–2) | 1 (1–2) | 1 (1–2) | .1 |
| Duration of fever after admission, days | 2.5 (1–4) | 3 (0–10) | 2 (0–4) | .04 |
| Fever >4 days after admission | 71 (24.8) | 13 (48.1) | 58 (22.4) | .008 |
| Initial C-reactive protein, mg/dL | 7.6 (3.8–18.3) | 16.1 (4.5–23) | 7.2 (3.8–17.3) | .32 |
| Intensive care unit admissions | 31 (10.8) | 6 (22.2) | 25 (9.6) | .09 |
aAll continuous variables expressed as medians with interquartile ranges.
bAmong 77 patients with abscess diameter documented.
Medical Therapy
All patients received intravenous antimicrobials initially. The most commonly used agents for empiric therapy were vancomycin monotherapy (37.8%), clindamycin monotherapy (36.7%), and vancomycin with nafcillin (17.4%). The most commonly used antimicrobials for definitive therapy included cephalexin (33.6%), cefazolin (23.8%), and clindamycin (23.1%); 43.7% of patients (125/286) were discharged on oral antibiotics. The rate of oral prescribing at discharge increased substantially during the study period from 14.3% in 2011 to 80.5% in 2017 (P = .004). Five patients received all therapy by the intravenous route as inpatients. Ten patients discharged on outpatient parenteral antimicrobial therapy (10/156, 6.4%) were transitioned to oral antibiotics outside of the hospital; 5 patients discharged on oral antibiotics (5/125, 4%) were readmitted and received a second period of intravenous therapy.
Overall Orthopedic Complications
Orthopedic complications developed in 27 patients (9.4%) of which the most common were chronic osteomyelitis (14/27, 51.8%) and pathologic fracture (8/27, 29.6%) followed by growth arrest (4, 14.8%) and avascular necrosis (2, 7.5%). One patient experienced both growth arrest and a pathologic fracture. Notably, 3 patients who received an initial diagnosis of isolated septic arthritis were later diagnosed with chronic osteomyelitis in bones adjacent to the affected joint. Further clinical details regarding patients who developed chronic osteomyelitis and pathologic fracture are provided in Supplementary Tables 2 and 3. Orthopedic complications were diagnosed at a median of 67.5 days (IQR, 46–100 days) following the index admission; 12 patients (44.4%) were still receiving antibiotics at the time complications were diagnosed. Among those patients not receiving antibiotics at the time a complication was diagnosed, the median duration of antibiotics prior to discontinuation was 42 days (IQR, 35–42) and complications developed at a median of 21 days (IQR, 4–54) following discontinuation. Complications were associated with hospital readmissions in 18 (66.7%) patients and additional surgeries in 13 (48.1%). For 18 patients, the diagnosis of complications prompted prolongation of antibiotic therapy for a median of 305.5 days (IQR, 242–360).
There was no association with patient age, site of disease, the presence of bone abscesses, or duration of symptoms on presentation and the likelihood of developing orthopedic complications (Table 1). Patients who developed orthopedic complications were more likely to have positive blood cultures (74.1% vs 52.1%, P = .04), fever >4 days after admission (48.1% vs 22.4%, P = .008), and intensive care unit (ICU) admission (22.2% vs 9.6%, P = .09).
Patients who developed orthopedic complications were compared with those who did not in term of microbiologic characteristics of the infecting S. aureus (Table 2). There was no association with methicillin resistance, the USA300 pulsotype, or the presence of genes encoding Panton-Valentine leucocidin (PVL) and orthopedic complications. Patients who developed orthopedic complications were more likely to have infection with an agr III S. aureus (22.2% vs 8.8%, P = .04).
Table 2.
Associations With Orthopedic Complications and Microbiologic and Molecular Characteristics of Staphylococcus aureus
| Microbiologic Characteristics | All Patients (n = 286) |
Patients With Orthopedic Complications (n = 27) |
Patients Without Orthopedic Complications (n = 259) |
P Value |
|---|---|---|---|---|
| Methicillin-resistant Staphylococcus aureus | 79 (27.6) | 8 (29.6) | 71 (27.4) | .8 |
| Clindamycin resistance | 32 (11.2) | 5 (18.5) | 27 (10.4) | .2 |
| Vancomycin minimum inhibitory concentration ≥1.5 μg/mL | 166 (58) | 14 (51.8) | 152 (58.6) | .54 |
| Panton-Valentine leucocidin positive | 115 (40.2) | 14 (51.8) | 101 (38.9) | .21 |
| USA300 pulsotype | 126 (44.1) | 13 (48.1) | 113 (43.6) | .69 |
| agr I | 198 (69.2) | 18 (66.7) | 180 (69.4) | .8 |
| agr II | 35 (12.2) | 2 (7.4) | 33 (12.7) | .55 |
| agr III | 29 (10.1) | 6 (22.2) | 23 (8.8) | .04 |
| agr IV | 11 (3.8) | 1 (3.7) | 10 (3.8) | 1 |
| agr nontypeable | 13 (4.5) | 0 | 13 (5) | .6 |
Medical and surgical treatments were compared in patients with and without orthopedic complications (Table 3). There was no association with antibiotic choices, time to initiation of effective antimicrobials, or the use of oral antibiotics at discharge and the development of orthopedic complications. Patients who developed complications, however, were more likely to have required >1 surgical procedure (48.1% vs 9.3%, P < .001) and to have experienced delayed source control (25.9% vs 6.5%, P < .001). The following were included in a multivariable logistic regression model for orthopedic complications: agr III organism, positive blood culture, ICU admission, duration of fever >4 days after hospital admission, >1 surgical procedure, and delayed source control. Of these variables, only infection with an agr III organism, duration of fever >4 days after admission, and delayed source control remained significantly associated with orthopedic complications (Table 4). When these analyses were repeated with the exclusion of cases of isolated septic arthritis, similar results were achieved (Supplementary Table 4).
Table 3.
Associations of Orthopedic Complications and Treatment Variables
| Clinical Characteristics | All Patients (n = 286) |
Patients With Orthopedic Complications (n = 27) |
Patients Without Orthopedic Complications (n = 259) |
P Value |
|---|---|---|---|---|
| Empiric therapy | ||||
| Clindamycin monotherapy | 105 (36.7) | 6 (22.2) | 99 (38.2) | .14 |
| Vancomycin monotherapy | 108 (37.8) | 10 (37) | 98 (37.8) | 1 |
| Vancomycin + Nafcillin | 50 (17.5) | 8 (29.6) | 42 (16.2) | .11 |
| Ineffective empiric therapya | 12 (4.2) | 2 (7.4) | 10 (3.9) | .31 |
| Time from admission to initiation of effective antibiotics, daysb | 1 (0–1) | 1 (0–1) | 1 (0–1) | .49 |
| Definitive therapy | ||||
| First-generation cephalosporin | 165 (57.7) | 17 (62.9) | 148 (57.1) | .68 |
| Clindamycin | 67 (23.4) | 4 (14.8) | 63 (24.3) | .31 |
| Vancomycin | 23 (8) | 3 (11.1) | 20 (7.7) | .47 |
| Oral antibiotics at discharge | 125 (43.7) | 8 (29.6) | 117 (45.1) | .15 |
| Duration of total antibiotic therapy, daysc | 42 (29–55) | 42 (33–64) | 41 (29–55) | .36 |
| Surgical procedure performed | 206 (72.1) | 23 (85.1) | 183 (70.7) | .12 |
| Corticotomy and/or incision/drainage of subperiosteal abscessd | 154 (53.8) | 19 (70.4) | 135 (52.1) | .11 |
| Bone biopsyd | 53 (18.5) | 7 (25.9) | 46 (17.8) | .3 |
| Arthrocentesis and/or arthrotomyd | 127 (44.4) | 14 (51.9) | 113 (43.6) | .42 |
| Drainage/debridement of adjacent soft tissued | 40 (13.9) | 6 (22.2) | 34 (13.1) | .24 |
| External drain placedd | 160 (55.9) | 19 (70.4) | 141 (54.4) | .15 |
| More than 1 surgical procedure | 37 (12.9) | 13 (48.1) | 24 (9.3) | <.001 |
| Time from admission to first surgical procedure, days | 1 (0–2) | 1.5 (1–2) | 1 (0–2) | .22 |
| Delayed source control | 28 (9.8) | 7 (25.9) | 21 (6.5) | <.001 |
| Duration of total follow-up, dayse | 85.5 (34.5–280.5) | 67.5 (46–100) | 95 (34–337) | .37 |
aAll cases of ineffective empiric therapy were the result of clindamycin being prescribed empirically in patients who were ultimately found to be infected with a clindamycin-resistant S. aureus.
bAll continuous variables expressed as medians with interquartile ranges.
cFor each patient who developed a complication and had therapy extended because of the complication, duration of therapy was regarded as the time the patient received antibiotics until diagnosis with an orthopedic complication.
dNot mutually exclusive categories.
eFor patients who developed complications, the date of diagnosis with complications was regarded as the date of follow-up; details on follow-up outcomes of patients who developed complications are provided in the Supplementary Materials.
Table 4.
Multivariable Analyses of Associations With Orthopedic Complications
| Clinical/Microbiologic Characteristics | Adjusted P Value | Odds Ratio | 95% Confidence Interval |
|---|---|---|---|
| Bacteremia | .1 | 2.4 | 0.85–6.8 |
| Intensive care unit admission | .36 | 1.78 | 0.52–6.12 |
| agr III Staphylococcus aureus | .007 | 5.05 | 1.56–16.31 |
| Prolonged fever | .04 | 1.9 | 1.79–5.51 |
| More than 1 surgical procedure | .66 | 0.9 | 0.29–2.75 |
| Delayed source control | .002 | 5.91 | 1.95–17.88 |
No significant collinearity was noted among variables.
Chronic Osteomyelitis and Pathologic Fracture
Chronic osteomyelitis and pathologic fractures were examined separately (Supplementary Tables 5 and 6). Chronic osteomyelitis was associated with agr group III infection (27.2% vs 8.9%, P = .08), the presence of bone abscess (100% vs 50.2%, P = .001), prolonged fever (54.5% vs 23.3%, P = .03), ICU admission (36.4% vs 10.2%, P = .03), multiple surgical procedures (54.5% vs 10.2%, P = .001), and delayed source control (45.4% vs 8.6%, P = .002). Fewer patients with chronic osteomyelitis were infected with an isolate with a vancomycin minimum inhibitory concentration (MIC) ≥1.5 µg/mL (27.2% vs 58.3%, P = .06). In multivariable analyses, agr III infection (P = .04; odds ratio [OR], 2.5; 95% confidence interval [CI], 1.71–24.8) and delayed source control (P = .006; OR, 8.26; 95% CI, 1.85–36.9) remained significantly associated with chronic osteomyelitis.
In univariable analyses, pathologic fractures were associated with infection with PVL-positive organisms (75% vs 39.2%, P = .06), larger median bone abscess diameters (8.8 cm vs 3.5 cm, P = .06), bacteremia (75% vs 53.6%, P = .03), fever >4 days (62.5% vs 23.8%, P = .03), and multiple surgical procedures (62.5% vs 11.5%, P = .001). None of these variables maintained statistical significance in multivariable analyses. The risk of pathologic fracture increased substantially among patients with ≥3 debridement procedures (Supplementary Figure 3; P = .002); however, the risk of fracture in patients with 1–2 surgeries (1.3% and 2.2%, respectively) was similar to the risk for those who did not undergo surgery (1.3%, P = .8)
Patients Managed Without Surgical Intervention
Seventy-nine patients (27.6%) were managed with medical therapy alone. Compared to those who underwent both surgical and medical management, patients managed with medical therapy alone had fewer bone abscesses (25.3% vs 55.1%, P < .001), smaller abscesses (2.8 cm [IQR, 1.1–4.7 cm] vs 3.8 cm [IQR, 2–6 cm], P = .2), were less often admitted to the ICU (5.1% vs 13%, P = .06), and had lower admission C-reactive protein (CRP, median, 5.9 vs 9.2 mg/dL, P = .03). Additionally, patients managed with medical therapy alone were less likely to have infection with MRSA (15.2% vs 31.3%, P < .001) or a USA300 pulsotype (30.3% vs 48.7%, P = .001). Four patients (5.1%) who did not undergo surgery developed orthopedic complications by last follow-up; all 4 of these patients had either fever lasting >4 days during their index admission or infection with an agr III organism.
Other Musculoskeletal Complaints
At the time of final follow-up, an additional 11 patients (3.8%) had chronic musculoskeletal complaints that did not meet our predefined criteria for orthopedic complications. These symptoms included morning stiffness (n = 2), pain/swelling in a joint or extremity with exertion (n = 5), intermittent pain (n = 1), or joint pain/swelling with a change in weather (n = 2). A larger proportion of these patients had delayed source control compared to those who did not have any musculoskeletal complaints at follow-up (3/11, 27.3% vs 19/249, 7.6%; P = .056). An additional patient was diagnosed with osteosarcoma in the same bone that had previously been infected; this patient had a culture from bone that grew S. aureus, completed antimicrobial therapy, and was later diagnosed with malignancy.
DISCUSSION
While the vast majority of children with AHOAIs have good outcomes, a significant number of patients experience long-term morbidity. We report that 9.4% of patients experience sequelae after culture-proven S. aureus AHOAI, with 5% developing chronic osteomyelitis, consistent with previous studies [4].
Tremendous variability exists across centers with regard to the management of AHOAI [1, 2, 9, 16]. Our data revealed an independent association with delayed source control and long-term orthopedic sequelae. This finding points to the benefits of combined medical and surgical management of AHOAI over medical management alone. However, 27.6% of our patients were managed without surgical intervention, the majority of which experienced no sequelae. Our data support the need to identify which patients require source control early in their presentation so that intervention can occur promptly to improve outcomes. The potential benefits of early source control, however, must be weighed carefully against the risks of surgery/anesthesia.
Additionally, we found an association with infection with agr group III S. aureus and sequelae, specifically chronic osteomyelitis; the reasons for this finding are unclear. agr is a complex regulatory system that controls a number of growth and virulence factors in S. aureus [17, 18]. Notably, recent studies suggest that agr dysfunction and polymorphisms within this complex may promote chronic infection in a rat osteomyelitis model [19]. We previously reported an association with agr IV, elevated vancomycin MICs, and disease severity at time of presentation in MSSA AHOAI [11]. While these variables may contribute to acute disease, our current findings do not support a role for elevated vancomycin MIC or agr IV in the development of post-discharge complications. Studies from the mid-2000s suggested that MRSA (particularly PVL-positive, USA300 MRSA) was associated with a more severe infection phenotype in AHOAI than that caused by MSSA [2, 20–22]. However, recently there has been a relative decline in community-associated MRSA (CA-MRSA) strains contributing to invasive S. aureus infection in many centers [23]. While the mechanisms linking agr III strains with negative outcomes are unclear, it may represent the emergence of new virulent strain types in the post–CA-MRSA era.
Given that chronic osteomyelitis was the most common complication seen, the risk factors for chronic osteomyelitis largely mirrored those for orthopedic complications as a whole. While the number of patients who developed pathologic fracture was quite small, by contrast, we did not observe an association with fracture and agr III infection or timing of surgical intervention. We did, however, find a strong association in univariable analyses between the need for ≥2 surgical procedures and the development of pathologic fractures that was most evident in patients undergoing ≥3 procedures. This association is notable and deserves further investigation; however, it does not prove causation. While it is certainly conceivable that repeated surgical debridements in bone may weaken the cortex predisposing to fracture, it is also possible that these patients experience a greater severity of infection (necessitating multiple surgical procedures) and that the degree of illness itself predisposes to fracture. This second hypothesis is supported by the association with pathologic fractures and larger bone abscesses compared to those patients who did not experience fracture. Importantly, the risk of fracture in patients who underwent 1–2 procedures was not increased compared to those who did not undergo any surgical intervention. Previous investigations noted an association with USA300.0114 pulsotype and pathologic fracture [6]. We did not observe an association with the USA300 pulsotype and fracture; however, this may again be a product of the shifting molecular epidemiology of invasive staphylococcal disease, as well as the small number of cases.
Importantly, we did not observe an association with the use of oral antibiotics at time of discharge and the development of any orthopedic sequelae in S. aureus AHOAI. These data are in agreement with data from previous studies, suggesting that most patients can be transitioned to oral antibiotics with good outcomes [10, 16, 24].
There are limitations to this study that should be acknowledged. Foremost, these findings are from a single center and may not be representative of the US population at large, particularly with regard to the impact of agr group and surgical interventions on outcomes. Notably, the rate of surgical intervention for S. aureus AHOAI at TCH is comparable to that in a study at the University of Tennessee [2] but higher than reported in a multicenter study of all-cause osteomyelitis [24]. Additionally, due to the observational nature of the study, we were unable to assess the impact of antibiotic duration on the likelihood of orthopedic sequelae. The definition of chronic osteomyelitis used for this study was developed by the authors and may have led to misclassification of some patients. However, given that all patients with chronic osteomyelitis had radiographic evidence of disease, the impact of this is likely minor. Given the variable durations of follow-up, the development of certain complications, namely, growth arrest and/or avascular necrosis, may have been underestimated. Furthermore, the adequacy of surgical source control was not fully explored and was beyond the scope of this study. Finally, the restriction of the study to S. aureus AHOAI limits the generalizability of our findings, particularly when considering that most patients with culture-negative AHOAI do quite well [25].
In conclusion, orthopedic sequelae as a collective group complicate 9.4% of S. aureus AHOAIs and are associated with substantial morbidity. While the development of orthopedic sequelae is almost certainly multifactorial in these patients, agr group III organisms, prolonged fever, and delayed source control are independently associated with negative outcomes. Large-scale, prospective studies are needed to better understand the predictors of outcome in this common but serious childhood infection.
Supplementary Data
Supplementary materials are available at Clinical Infectious Diseases online. Consisting of data provided by the authors to benefit the reader, the posted materials are not copyedited and are the sole responsibility of the authors, so questions or comments should be addressed to the corresponding author.
{kind=link}
{kind=link}
{kind=link}
Notes
Acknowledgments. The authors are grateful to the Texas Children’s Hospital clinical microbiology laboratory for their assistance.
Financial support.This work was supported by the National Institute of Allergy and Infectious Diseases (NIAID; K23AI099159) and the Texas Children’s Hospital Pediatric Pilot Research Fund (J. C. M.).
Potential conflicts of interest. S. L. K. is a primary investigator on clinical trials sponsored by Merck and Allergan and has received grant funding from Pfizer not directly related to the work under consideration. J. C. M. and J. G. V. are coinvestigators on these studies. J. C. M. also reports funding from the NIAID. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
References
- 1. McNeil JC, Forbes AR, Vallejo JG, et al. . Role of operative or interventional radiology-guided cultures for osteomyelitis. Pediatrics 2016; 137:e20154616. [DOI] [PubMed] [Google Scholar]
- 2. Arnold SR, Elias D, Buckingham SC, et al. . Changing patterns of acute hematogenous osteomyelitis and septic arthritis: emergence of community-associated methicillin-resistant Staphylococcus aureus. J Pediatr Orthop 2006; 26:703–8. [DOI] [PubMed] [Google Scholar]
- 3. Martínez-Aguilar G, Avalos-Mishaan A, Hulten K, Hammerman W, Mason EO Jr, Kaplan SL. Community-acquired, methicillin-resistant and methicillin-susceptible Staphylococcus aureus musculoskeletal infections in children. Pediatr Infect Dis J 2004; 23:701–6. [DOI] [PubMed] [Google Scholar]
- 4. Dich VQ, Nelson JD, Haltalin KC. Osteomyelitis in infants and children. A review of 163 cases. Am J Dis Child 1975; 129:1273–8. [DOI] [PubMed] [Google Scholar]
- 5. Riise ØR, Kirkhus E, Handeland KS, et al. . Childhood osteomyelitis-incidence and differentiation from other acute onset musculoskeletal features in a population-based study. BMC Pediatr 2008; 8:45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Belthur MV, Birchansky SB, Verdugo AA, et al. . Pathologic fractures in children with acute Staphylococcus aureus osteomyelitis. J Bone Joint Surg Am 2012; 94:34–42. [DOI] [PubMed] [Google Scholar]
- 7. Wald ER. Risk factors for osteomyelitis. Am J Med 1985; 78:206–12. [DOI] [PubMed] [Google Scholar]
- 8. Krogstad P. Osteomyelitis. In: Cherry JD, Harrison GJ, Kaplan SL, Steinbach WJ, Hotez PJ, eds. Feigin and Cherry’s textbook of pediatric infectious diseases. 8th ed Vol. 1 Philadelphia, PA: Elsevier, 2019:516–29. [Google Scholar]
- 9. Peltola H, Pääkkönen M, Kallio P, Kallio MJ; Osteomyelitis-Septic Arthritis Study Group Short- versus long-term antimicrobial treatment for acute hematogenous osteomyelitis of childhood: prospective, randomized trial on 131 culture-positive cases. Pediatr Infect Dis J 2010; 29:1123–8. [DOI] [PubMed] [Google Scholar]
- 10. Peltola H, Unkila-Kallio L, Kallio MJ. Simplified treatment of acute staphylococcal osteomyelitis of childhood. The Finnish Study Group. Pediatrics 1997; 99:846–50. [DOI] [PubMed] [Google Scholar]
- 11. Kok EY, Vallejo JG, Sommer LM, et al. . Association of vancomycin mic and molecular characteristics with clinical outcomes in methicillin-susceptible Staphylococcus aureus acute hematogenous osteoarticular infections in children. Antimicrob Agents Chemother 2018; 62. doi: 10.1128/AAC.00084-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Williams DJ, Deis JN, Tardy J, Creech CB. Culture-negative osteoarticular infections in the era of community-associated methicillin-resistant Staphylococcus aureus. Pediatr Infect Dis J 2011; 30:523–5. [DOI] [PubMed] [Google Scholar]
- 13. Jarraud S, Mougel C, Thioulouse J, et al. . Relationships between Staphylococcus aureus genetic background, virulence factors, agr groups (alleles), and human disease. Infect Immun 2002; 70:631–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Moore PC, Lindsay JA. Genetic variation among hospital isolates of methicillin-sensitive Staphylococcus aureus: evidence for horizontal transfer of virulence genes. J Clin Microbiol 2001; 39:2760–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Pichon B, Hill R, Laurent F, et al. . Development of a real-time quadruplex PCR assay for simultaneous detection of nuc, Panton-Valentine leucocidin (PVL), mecA and homologue mecALGA251. J Antimicrob Chemother 2012; 67:2338–41. [DOI] [PubMed] [Google Scholar]
- 16. Keren R, Shah SS, Srivastava R, et al. ; Pediatric Research in Inpatient Settings Network Comparative effectiveness of intravenous vs oral antibiotics for postdischarge treatment of acute osteomyelitis in children. JAMA Pediatr 2015; 169:120–8. [DOI] [PubMed] [Google Scholar]
- 17. Novick RP. Autoinduction and signal transduction in the regulation of staphylococcal virulence. Mol Microbiol 2003; 48:1429–49. [DOI] [PubMed] [Google Scholar]
- 18. Que Y-A, Moreillon P. Staphylococcus aureus (including staphylococcal toxic shock). In: Mendell G, Bennett J, Dolin R, eds. Principles and practice of infectious diseases. 7th ed, Vol. 2 Philadelphia, PA: Churchill Livingstone Elsevier, 2010:2543–78. [Google Scholar]
- 19. Suligoy CM, Lattar SM, Noto Llana M, et al. . Mutation of Agr is associated with the adaptation of Staphylococcus aureus to the host during chronic osteomyelitis. Front Cell Infect Microbiol 2018; 8:18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Hawkshead JJ 3rd, Patel NB, Steele RW, Heinrich SD. Comparative severity of pediatric osteomyelitis attributable to methicillin-resistant versus methicillin-sensitive Staphylococcus aureus. J Pediatr Orthop 2009; 29:85–90. [DOI] [PubMed] [Google Scholar]
- 21. Bocchini CE, Hulten KG, Mason EO Jr, Gonzalez BE, Hammerman WA, Kaplan SL. Panton-Valentine leukocidin genes are associated with enhanced inflammatory response and local disease in acute hematogenous Staphylococcus aureus osteomyelitis in children. Pediatrics 2006; 117:433–40. [DOI] [PubMed] [Google Scholar]
- 22. Carrillo-Marquez MA, Hulten KG, Hammerman W, Mason EO, Kaplan SL. USA300 is the predominant genotype causing Staphylococcus aureus septic arthritis in children. Pediatr Infect Dis J 2009; 28:1076–80. [DOI] [PubMed] [Google Scholar]
- 23. Hultén KG, Mason EO, Lamberth LB, Forbes AR, Revell PA, Kaplan SL. Analysis of invasive community-acquired methicillin-susceptible Staphylococcus aureus infections during a period of declining community acquired methicillin-resistant Staphylococcus aureus infections at a large children’s hospital. Pediatr Infect Dis J 2018; 37:235–41. [DOI] [PubMed] [Google Scholar]
- 24. Zaoutis T, Localio AR, Leckerman K, Saddlemire S, Bertoch D, Keren R. Prolonged intravenous therapy versus early transition to oral antimicrobial therapy for acute osteomyelitis in children. Pediatrics 2009; 123:636–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Floyed RL, Steele RW. Culture-negative osteomyelitis. Pediatr Infect Dis J 2003; 22:731–6. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.