

Abstract
Peritoneal lymphomatosis is an extremely rare presentation of lymphoma. Due to its relative low frequency, it receives much less attention than peritoneal carcinomatosis. The challenge is to differentiate between lymphomatosis and carcinomatosis, as well as peritoneal tuberculosis or other pathologic entities within the peritoneal cavity based essentially on radiologic features.
18F-FDG PET/CT is the main imaging modality for staging and monitoring response to treatment in lymphoma. Peritoneal lymphomatosis is most often associated to aggressive histological subtypes of high-grade lymphoma which are reputed high FDG uptake.
We report two cases of Burkitt’s lymphoma and diffuse large B cell lymphoma (DLBCL), with intense FDG uptake involving the entire peritoneum and decreased FDG activity of the rest of the body including brain and kidneys, giving it an appearance of “peritoneal super scan”, follow up FDG PET/CT showed the disappearance of the peritoneal lymphomatosis and the reappearance of cerebral and urinary activity synonym of complete metabolic response.
Key Words: Burkitt’s lymphoma DLBCL lymphoma, FDG PET-CT, Peritoneal lymphomatosis, Peritoneal super scan
Introduction
Peritoneal lymphomatosis is rare as compared to peritoneal carcinomatosis, which is one of the commonly encountered findings in oncologic imaging. Among the lymphoma subtypes; peritoneal lymphomatosis is associated with aggressive histological subtypes of high-grade lymphoma, such as small-cell, large-cell, lymphoblastic Burkitt-like, and diffuse large B cell lymphomas (1). This extensive peritoneal involvement is exceptional in lymphoma disease as the omentum does not contain lymphoid tissue (2). The authors report two cases of peritoneal lymphomatosis with an unsual but characteristic aspect on FDG PET/CT.
Cases report
Case 1
A 16-year-old male presented to the medicine department with a complaint of progressive abdominal distension, dyspnea, and chest pain, for the last two months. Abdominal ultrasonography revealed markedly thickened omentum and subsequent CT studies clearly delineated the thickening of the omentum, intestines, and peritoneal lining.
The patient underwent PET/CT (General Electric Discovery ST) one hour after injection of 240 MBq (6.4 mCi) 18F-FDG. The PET/CT demonstrated bilateral pleural effusion and high abundance peritoneal effusion that is associated with lymphadenopathy above and under the diaphragm, and reduced FDG activity of the rest of the body that includes brain and kidneys. Moreover, the biopsy from a right axillary lymphadenopathy confirmed the diagnosis of DLBCL (Figure 1).
Figure 1.

A 16-year-old man, with diffuse large B-cell lymphoma. PET/CT scan on initial staging shows multiple areas of increased FDG uptake in the peritoneum (SUVmax=3.7), in the bilateral pleural effusion (SUVmax=2.6), with lymphadenopathy above and under the diaphragm on the maximum intensity projection (MIP) image (a). As well as on coronal (b) and on sagittal (c) PET/CT images
Follow-up F-18 FDG PET/CT scan was taken after three cycles of R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, prednisolone), and showed a lack of abnormal uptake, which indicated complete metabolic remission (Figure 2).
Figure 2.

Complete metabolic remission on FDG-PET/CT after 3 courses of R-CHOP
Case 2
A 30-year-old man was admitted to the gastroenterology department because of progressive abdominal distention for one month. Abdominal ultrasonography revealed omental and peritoneal thickening. Omental biopsy was performed under ultrasonography guidance and the histopathologic examination objectified a high-grade Burkitt’s lymphoma. Therefore, the patient was referred to the nuclear medicine department for staging with 18F-FDG PET/CT, and the scan was performed 60 minutes after intravenous injection of 275 MBq (7.43 mCi) of 18F-FDG. Images showed increased FDG uptake in the thickenning of the omentum and peritoneal lining, consistently with an extensive lymphomatous involvement, associated with lymphadenopathy above and under the diaphragm, and involvements of bones (Figure 3).
Figure 3.
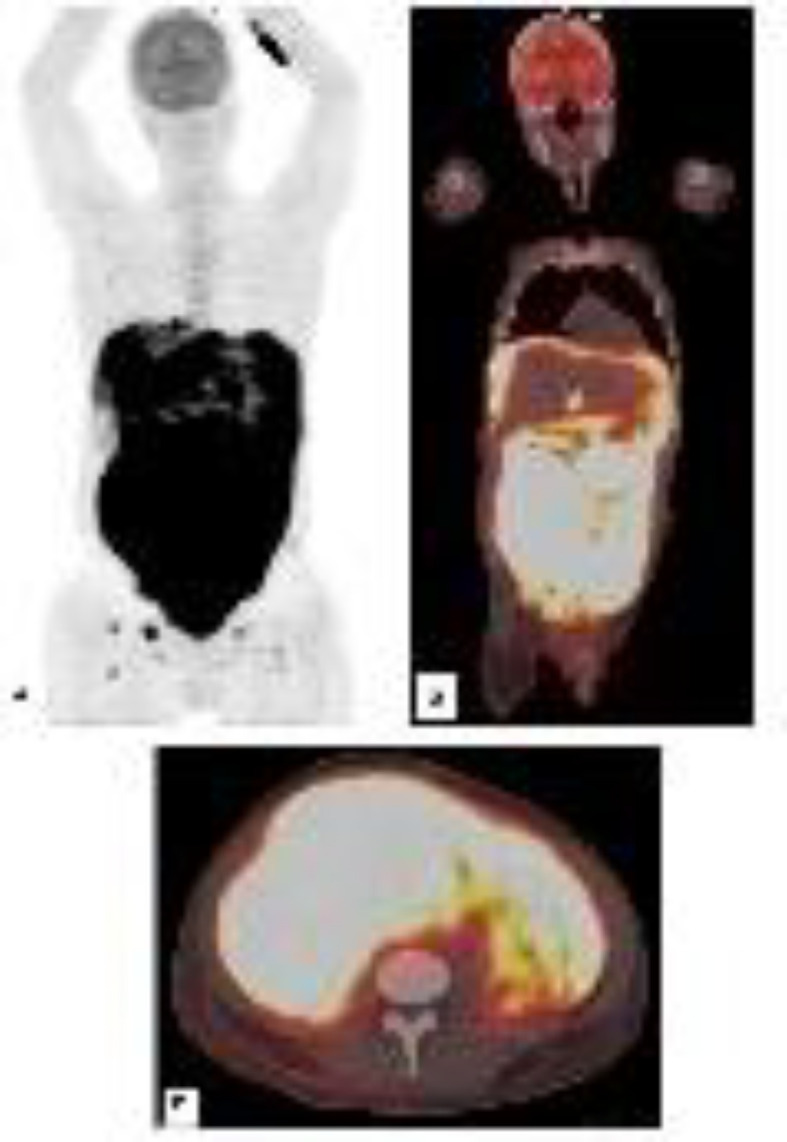
A 30-year-old man, with high grade Burkitt’s lymphoma. The pretreatment PET MIP image shows extensive and diffuse increased FDG uptakes in the peritoneum (SUVmax=11), with lymphadenopathy above and under the diaphragm, and involvements of bones (Ischium (SUVmax=7.8); Right Femur (SUVmax=5.1)). We notice the reduced FDG uptake in the brain (SUVmax=3.6). Coronal (b) and transverse (c) PET/CT images more clearly show FDG uptakes in peritoneum and omentum
The re-evaluation after 4 cycles of Dose-adjusted EPOCH-R (etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin, and rituximab) objectified the disappearance of all hypermetabolic disorders with the reappearance reappearance of cerebral and urinary activity synonym of complete metabolic response (Figure 4).
Figure 4.

Complete metabolic remission on FDG-PET/CT after 4 cycles of Dose-adjusted EPOCH-R, with an aspect of bone marrow activation after chemotherapy
Discussion
Diffuse peritoneal and omental seeding are well-known forms of dissemination of metastatic carcinoma which are usually spreading from ovarian, colorectal, gastric, or breast cancer (3). The presentation of lymphoma as peritoneal lymphomatosis is rare, but it needs to be thought of, since the treatments and prognosis are very different from peritoneal carcinomatosis (4). The route of this dissemination is not clear enough, because the omentum does not contain lymphoid tissue; the possible pathways are transverse mesocolon, gastrocolic ligament, and visceral peritoneal surfaces (2).
Although anatomical imaging is effective in detection of peritoneal involvement, differentiation of lymphomatosis from carcinomatosis, tuberculosis or mesothelioma, cannot be made easily with anatomical imaging only. Ascites, omental caking and diffusing peritoneal thickening were reported to be the most common presentations (5). On FDG PET/CT peritoneal involvement is more extensive. On this scan, the characteristic uptake pattern with active lymphadenopathy and multiple active lesions in the peritoneum (6).
18F-FDG PET/CT imaging provides invaluable information in staging; follow-up; and determination of therapy efficacy in patients with lymphomas. FDG uptake has been reported in peritoneal lymphomatosis in DLBCL and in Burkitt’s lymphoma as well (2). On our patients, PET/CT showed an extraordinary peritoneal avidity for FDG. The Ann Arbor classification does not mention peritoneal involvement. However, the St. Jude staging system classifies these patients as having stage III disease (6).
Peritoneal lymphomatosis can lead to an abdominal compartment syndrome and multiple organ failure with associated adverse hemodynamic effects involving the bowel, kidneys, and the respiratory tract. The proposed mechanism includes reduced venous return caused by the increased intra-abdominal pressure followed by a compromise in renal perfusion leading to oliguria. Therefore, this abdominal compartment is a significant cause of morbidity (7).
The appearance of peritoneal lymphomatosis on PET/CT with an intense FDG uptake involving the entire peritoneum and decreased FDG activity of the rest of the body in particular physiological uptake in brain and kidneys, can be called “peritoneal super scan” (8), by analogy to the super bone scan on bone scintigraphy which is characterized by a strikingly high bone to soft tissue, with a uniform symmetrical increase in bone uptake and absent renal visualization. The faint visualization of the brain, renal cortex, and soft tissue might be the result of extraordinarily high uptake of FDG by the peritoneum and the omentum. Low brain uptake of FDG has been reported when using corticosteroids and sedatives; these conditions should be taken into consideration (9).
In addition to peritoneal super scan, some other FDG PET super scans were described; Su et al. presented a case of FDG PET super scan involving skeletons which are similar to the super scan of bone scintigraphy (10). Basu et al. described a “hepatic super scan” by FDG PET in a patient with Hodgkin disease who had unusually elevated hepatic radioactivity, in addition to multiple lymph nodes above and under the diaphragm, the diagnosis was confirmed by liver biopsy which demonstrated diffuse hepatic involvement (11).
These two uncommon cases illustrate the usefulness of FDG PET/CT imaging in detecting lymphomatous involvement in omentum and peritoneum as well as in other sides of the body in assessing its response to treatment. This is important because peritoneal lymphomatosis can be so easily mistaken for carcinomatosis secondary to an occult primary neoplasm. We suggest that the reappearance of the physiological uptake of FDG in brain, kidneys, and the parallel disappearance of the “peritoneal super scan” may be a parameter to predict a complete metabolic response; however, further studies on large series are needed to confirm or refute this hypothesis.
References
- 1.Park EK, Lee SR, Kim YC, Oh SY, Choe JG. Peritoneal Lymphomatosis Imaged by F-18 FDG PET/CT. Nucl Med Mol Imaging. 2010;44:159–160. doi: 10.1007/s13139-010-0018-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Yapar AF, Reyhan M. 18F-FDG uptake in diffuse peritoneal lymphomatosis. Clin Nucl Med. 2012;37:176–177. doi: 10.1097/RLU.0b013e31823ea93e. [DOI] [PubMed] [Google Scholar]
- 3.Cunningham N, Ffrench-Constant S, Planche K, Gillmore R. Peritoneal lymphomatosis: a rare presentation of follicular lymphoma mimicking peritoneal carcinomatosis. Case Reports. 2015;2015:bcr2014207136. doi: 10.1136/bcr-2014-207136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lu SJ, Sinha AK. Peritoneal lymphomatosis shown on positron emission tomography/ computed tomography scanning. Br J Haematol . 2011;153(3):290. doi: 10.1111/j.1365-2141.2011.08608.x. [DOI] [PubMed] [Google Scholar]
- 5.Uslu L, Sen F, Sager S, Halaç M. Extensive peritoneal and pleural lymphomatosis in a patient with Burkitt lymphoma revealed with 18F-FDG PET/CT. Nuklearmedizin. 2013;52:56–57. [PubMed] [Google Scholar]
- 6.Van Rheenen RW, Bongaerts AH, Glaudemans AW. Peritoneal lymphomatosis found on 18F-FDG PET/CT. Eur J Haematol. 2012;89:503–504. doi: 10.1111/j.1600-0609.2012.01823.x. [DOI] [PubMed] [Google Scholar]
- 7.Wong S, Sanchez TR, Swischuk LE, Huang FS. Diffuse peritoneal lymphomatosis: atypical presentation of Burkitt lymphoma. Pediatr Radiol. 2009;39:274–276. doi: 10.1007/s00247-008-1063-y. [DOI] [PubMed] [Google Scholar]
- 8.Roy SG, Parida GK, Tripathy S, Singhal A, Shamim SA, Tripathi M. Peritoneal super scan on 18F-FDG PET-CT in a patient of burkitt's lymphoma. Indian J Nucl Med. 2017;32:155–6. doi: 10.4103/0972-3919.202250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kim DW, Kim CG, Park SA, Jung SA, Yang SH. Metabolic super scan in F-FDG PET/CT imaging. J Korean Med Sci. 2010;25:1256–7. doi: 10.3346/jkms.2010.25.8.1256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Su HY, Liu RS, Liao SQ, Wang SJ. F-18 FDG PET superscan. Clin Nucl Med. 2006;31:28–9. doi: 10.1097/01.rlu.0000191569.37542.3d. [DOI] [PubMed] [Google Scholar]
- 11.Basu S, Nair N. Unusually elevated liver radioactivity on F-18 FDG PET in Hodgkin’s disease: hepatic ‘superscan’. Clin Nucl Med. 2004;29:626–8. doi: 10.1097/00003072-200410000-00005. [DOI] [PubMed] [Google Scholar]