

Abstract
In Ghana, majority of cancer studies have focused on only two main teaching hospitals. However, there is the need to study the disease burden from other parts of the country. This study was designed to review cancer cases recorded in major hospitals in the Volta Region of Ghana, with the aim of determining the incidence of cancers and cancer-related mortalities, and contribute to cancer data in the country. In-patient diagnosis data from 2012 to 2014 were collected from 21 hospitals in the Volta Region of Ghana. The data were entered and structured in Microsoft Excel and analyzed with IBM SPSS Statistics 20 and GraphPad Prism 6. Cervical, breast, liver, soft tissue, and prostate cancer were identified as the commonly diagnosed cancers in the Region. Socioeconomic factors such as poor educational background and occupation were associated with incidence of cancer in the study area. The incidence of cancer was determined to be approximately 9, 11, and 6 morbidities per 100,000 people in the years 2012, 2013, and 2014, respectively, with liver cancer being the leading cause of deaths. Public awareness and screening efforts are thus needed to fight against cancer in the Volta Region, and Ghana as a whole. In addition, this study is an original report of cancers in the Volta Region of Ghana and underscores the need to report ethnic/population-specific frequencies to effectively evaluate the burden of cancer in the country.
Impact statement
Region-specific cancer reports are essential in knowing the common cancers in specific populations. This study reports all cancer types recorded in the major hospitals in the Volta Region of Ghana, a population that is sparsely captured in the national cancer registries. The study identified the common cancers as well as the death rates in the Volta Region, hence contributing to the national effort to report cancer data. Although not comprising all the elements of a cancer registry, our data will augment the effort of the two national cancer registries in Ghana to provide the national cancer reports.
Keywords: Frequently diagnosed cancers, cancer mortality, prostate cancer, soft tissue cancer, liver cancer, breast cancer and cervical cancer
Introduction
Cancer and its associated ailments remain a leading cause of mortality worldwide and constitute an enormous burden on societies.1 In 2018, a total of 18.1 million new cases and 9.6 million cancer-related deaths were estimated to have occurred worldwide,2 out of which over 1 million (5.8%) of all the new cases and about half-a-million (7.3%) of all the cancer-related deaths were projected to have occurred in Africa.2 Using data acquired by GLOBOCAN in 2018, the World Health Organization (WHO) estimated the incidence of cancer cases in Ghana to be 22,823.3 Demographic changes alone are anticipated to increase the number of new cancer cases per year by 70% between 2012 and 2030 in Africa.4 The rising global burden of cancer has been attributed to several factors including aging, population growth, and the prevalence and distribution of key risk factors for cancer that are associated with socio-economic development.2 For instance, in rapidly growing countries, cancer burden has shifted from being poverty-related to a disease that occurs as a result of changes in lifestyle due to industrialization.5 Other studies have also strongly associated cancer with risk factors such as smoking, overweight, physical inactivity, changing reproductive patterns, some viral infections, and uncontrollable genetic factors among others.6,7 The incidence of cancer and its severity vary across ages and gender, with lung and stomach cancer being leading causes of cancer deaths in male adults, while breast cancer and cervical cancer lead similarly in female adults, in less developed countries.8 However, in developed countries, prostate and breast cancer lead the mortality of gender-specific cancers.6,7
The national program on cancer control and cancer registries in Ghana is inadequate.9 Ghana’s medical report identifies cancer to be among the top 10 causes of death, and the risk of developing the disease has been found to be associated with geographical location and/or the work environment of an individual.10,11 A number of studies conducted in Ghana are mainly from two geographical locations (Kumasi and Accra) and are based on different types of cancers12–14 or the stages of presentation, which is not representative of the Ghanaian population.15,16 Thus far, only one population-based study has been conducted in Ghana,17 and therefore highlights the need for more comprehensive cancer studies focusing on populations in order to provide accurate information on the incidence of cancer in Ghana.
The Volta Region of Ghana shares boundary with Togo, and is mainly made up of the Ewe ethnic group.18,19 According to the Housing and Population Census of Ghana in 2010, the Volta Region had a population of 2,118,252 which comprised 1,019,398 males and 1,098,854 females.20 There are limited number of cancer studies from the Volta Region of Ghana, and the few studies are mostly focused on risk factors and/or social sciences of cancer.21–23 The current study was aimed at evaluating diagnosed data of cancer cases reported to major hospitals in the Volta Region of Ghana to determine the incidence of the disease and provide data to contribute to the national efforts towards control and prevention of cancer.
Materials and methods
The study was conducted in the Volta Region of Ghana, which lies at the eastern belt of the country and spans the three major divisions of the country: Northern, Central, and Southern divisions. In-patient hospital diagnosis data were retrieved from patient’s files in 21 hospitals (Figure 1) after an administrative clearance has been obtained from the Volta Regional Directorate of the Ghana Health Services. The hospitals selected for the study provide primary, secondary, and/or tertiary healthcare services. Hospital diagnosis data were collected and entered into Microsoft Excel. In Ghana, confirmed or suspected cases of cancers are diagnosed in the Surgery, Pathology, and Medical Oncology/Radiotherapy Departments of hospitals, but in this study, the exact modes/methods of cancer diagnoses and stage of cancer were not reported because the information was not available in the hospital diagnoses data that were retrieved from patients’ files. Since there was no unique patient identification system at the study sites, patient address, date of admission, and hospital names were scrutinized during data collection and analysis, in order to avoid the issue of multiple registration by the same patient. The collated data in Microsoft Excel were analyzed with IBM SPSS Statistics 20 and GraphPad Prism 6. Patient demographics, frequency of cancer diagnosis, and cross tabulation analyses were performed using descriptive statistics. Shapiro–Wilk normality test was used to examine whether the data were normally distributed.
Figure 1.

Map showing the distribution of health facilities used in the study in the Volta Region of Ghana.
The analysis of variance (ANOVA) of number of diagnosed cancer cases from 2012 to 2014 was performed using Kruskal–Wallis test, and inter-group multiple comparisons were done using Dunn’s multiple comparisons test. The age-specific mortality rates (ASMR) for each age group and cancer type were calculated by the formula below as previously described.17,24 The population by age data was obtained from the 2010 Population and Housing Census.20
Results
The study sought to evaluate data on diagnosed cancer cases from major hospitals in the Volta Region of Ghana. A total of 567 diagnosed cancer cases were retrieved from the records of 21 hospitals (Table 1), of which 256 (45.1%) were male and 311 (56.9%) were female (Table 2). The Volta Regional Hospital recorded the highest number of diagnosed cancer cases followed by Margret Marquart Catholic Hospital (Table 1).
Table 1.
Study sites and number of diagnosed cancer cases.
| Hospital name | Number of cases | Percent |
|---|---|---|
| Adidome District Hospital | 2 | 0.4 |
| Akatsi District Hospital | 4 | 0.7 |
| Anfoega Catholic Hospital | 11 | 1.9 |
| Battor Catholic Hospital | 3 | 0.5 |
| Comboni Hospital | 20 | 3.5 |
| Ho Municipal Hospital | 9 | 1.6 |
| Hohoe Municipal Hospital | 22 | 3.9 |
| Ihdn Mission Hospital | 9 | 1.6 |
| Jasikan District Hospital | 3 | 0.5 |
| Keta Municipal Hospital | 34 | 6 |
| Ketu South District Hospital | 17 | 3 |
| Krachi Hospital | 19 | 3.4 |
| Margret Marquart Catholic Hospital | 69 | 12.2 |
| Mary Theresa Hospital | 5 | 0.9 |
| Nkwanta District Hospital | 28 | 4.9 |
| Peki Hospital | 8 | 1.4 |
| Sacred Heart (keta) Hospital | 21 | 3.7 |
| Sogakope District Hospital | 16 | 2.8 |
| St Anthony's (Dzodze) Hospital | 66 | 11.6 |
| Volta Regional Hospital | 199 | 35.1 |
| Worawora Hospital | 2 | 0.4 |
| Total | 567 | 100 |
Table 2.
Demographic characteristics of study participants.
| Variable | Category | Number of cases | Percent (%) |
|---|---|---|---|
| Gender | Male | 256 | 45.1 |
| Female | 311 | 54.9 | |
| Total | 567 | 100.0 | |
| Educational background | No formal education | 269 | 47.4 |
| Primary School | 38 | 6.7 | |
| Junior High School | 173 | 30.5 | |
| Senior High School | 36 | 6.3 | |
| Tertiary | 44 | 7.8 | |
| Technical/vocational school | 7 | 1.2 | |
| Total | 567 | 100.0 | |
| Occupation | Farmer | 139 | 24.5 |
| Trader | 130 | 22.9 | |
| Student | 66 | 11.6 | |
| Retired | 62 | 10.9 | |
| Unemployed | 45 | 7.9 | |
| Tradesman | 31 | 5.5 | |
| Civil servant | 23 | 4.1 | |
| Business person | 3 | 0.5 | |
| Unskilled labor | 5 | 0.9 | |
| Others | 63 | 11.1 | |
| Total | 567 | 100.0 |
Demographic characterization of patients showed that majority of cancer patients do not have formal education, and a number of the patients had up to Junior High School level of education. A large proportion of the cancer patients were either farmers or traders (Table 2). The mean age of the patients was determined to be 44.5 ± 15.5 years, and a general increase in the number of diagnosed cases was observed with age, with majority of the diagnosis made in individuals who are greater than 70 years (Table 3).
Table 3.
Frequency of diagnosed cancer cases and age range of patients.
|
Age range (n) |
|||||||||
|---|---|---|---|---|---|---|---|---|---|
| ≤9 | 10–19 | 20–29 | 30–39 | 40–49 | 50–59 | 60–69 | ≥70 | Total | |
| Soft tissue | 5 | 11 | 18 | 12 | 14 | 13 | 12 | 6 | 91 |
| Oropharynx | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 3 |
| Nervous system | 2 | 0 | 2 | 2 | 1 | 1 | 0 | 0 | 8 |
| Abdomen | 1 | 3 | 6 | 3 | 1 | 4 | 4 | 3 | 25 |
| Ovary | 0 | 1 | 3 | 2 | 7 | 2 | 1 | 1 | 17 |
| Parotid gland | 5 | 1 | 0 | 3 | 1 | 0 | 1 | 1 | 12 |
| Prostate | 0 | 0 | 0 | 0 | 4 | 8 | 21 | 63 | 96 |
| Thyroid gland | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 2 |
| Bladder | 0 | 1 | 0 | 0 | 0 | 2 | 4 | 11 | 18 |
| Bone and articular cartilage | 1 | 4 | 2 | 0 | 1 | 1 | 1 | 2 | 12 |
| Breast | 1 | 3 | 2 | 8 | 13 | 14 | 11 | 7 | 59 |
| Bronchus or lung | 0 | 1 | 1 | 2 | 0 | 1 | 2 | 2 | 9 |
| Cervix | 0 | 0 | 1 | 9 | 11 | 12 | 10 | 14 | 57 |
| Colon | 0 | 0 | 1 | 0 | 0 | 2 | 1 | 4 | 8 |
| Liver | 1 | 2 | 12 | 14 | 10 | 11 | 6 | 14 | 70 |
| Skin | 0 | 0 | 0 | 1 | 1 | 2 | 1 | 0 | 5 |
| Retina | 2 | 1 | 1 | 2 | 0 | 0 | 1 | 0 | 7 |
| Stomach | 0 | 1 | 0 | 2 | 1 | 0 | 2 | 2 | 8 |
| Tonsil | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 |
| Brain | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 |
| Kidney | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 |
| Non-follicular lymphoma | 2 | 2 | 1 | 3 | 1 | 0 | 0 | 0 | 9 |
| Scrotum | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| Leukemia | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 3 |
| Unspecified | 2 | 1 | 2 | 4 | 6 | 7 | 4 | 18 | 44 |
| Total | 22 | 33 | 54 | 69 | 75 | 82 | 84 | 148 | 567 |
At least 26 different types of cancer cases were diagnosed in the Volta Region and majority of the cases were prostrate (16.9%), soft tissue (16.0%), liver (12.3%), breast (10.4%), and cervical (10.1%) cancers (Figure 2). For the purpose of this study, cancers that were 10% or more of the total number of diagnosed cases were considered as frequently diagnosed cancers. A number of the diagnosed cancer cases (44) did not indicate the type of cancer, and this cuts across all the age groups (Table 3).
Figure 2.

The different types of cancers diagnosed in the Volta Region.
The highest number of cancer cases was recorded in 2013 (234 cancer cases) (Figure 3). Prostate cancer was the most commonly diagnosed cancer over the three-year period, with yearly significant differences from 2012 to 2014 (Figure 3). There was a significant increase in the number of prostate cancer cases from 2012 to 2013 with a P-value of 0.032, but no significant difference in the number of diagnosed cervical and breast cancer cases from 2012 to 2014. The number of diagnosed liver and soft tissue cancer cases, on the other hand, decreased significantly from 2013 to 2014 with P-values of 0.045 and 0.019, respectively (Figure 3).
Figure 3.

Annual distribution of frequently diagnosed cancers from 2012 to 2014.
Based on the population of the Volta Region as published in the 2010 Population and Housing Census, the incidence of cancer was estimated at 9.02/100,000 in 2012, 11.05/100,000 in 2013, and 6.70/100,000 in 2014; 8.04/100,000 in 2012, 11.48/100,000 in 2013, and 5.59/100,000 in 2014 for males, and 9.92/100,000 in 2012, 10.65/100,000 in 2013, and 7.74/100,000 in 2014 for females. The age-specific mortality rates (ASMR) of the various cancer types are summarized in Table 4 and suggest that prostate and liver cancers are the highest contributing cancers to mortality of all ages. Cancer mortality generally increased with age, and a rapid increase is observed from 40 years (Figure 4).
Table 4.
The age-specific mortality rates of the various cancer types.
| Type of cancer | All ages | 10–19 | 20–29 | 30–39 | 40–49 | 50–59 | 60–69 | ≥70 |
|---|---|---|---|---|---|---|---|---|
| Soft tissue | 0.05 | – | – | – | – | – | – | 0.96 |
| Oropharynx | 0.05 | – | – | – | 0.53 | – | – | – |
| Nervous system | 0.05 | – | – | – | 0.53 | – | – | – |
| Abdomen | 0.09 | – | 0.30 | – | – | – | – | 0.96 |
| Ovary | 0.05 | – | – | – | 0.53 | – | – | – |
| Parotid gland | 0.05 | – | – | – | – | – | 1.21 | – |
| Prostate | 0.57 | – | – | – | – | – | 2.42 | 9.63 |
| Thyroid gland | 0.05 | – | – | – | 0.53 | – | – | – |
| Bladder | 0.05 | – | – | – | – | 0.75 | – | – |
| Breast | 0.38 | – | – | 0.41 | – | 2.25 | 3.63 | 0.96 |
| Bronchus or lung | 0.05 | 0.21 | – | – | – | – | – | – |
| Cervix | 0.14 | – | – | – | – | 0.75 | 1.21 | 0.96 |
| Colon | 0.05 | – | – | – | – | 0.75 | – | – |
| Liver | 0.80 | – | 0.60 | 0.83 | 0.53 | 3.75 | 3.63 | 3.85 |
| Retina | 0.05 | – | – | 0.41 | – | – | – | – |
| Stomach | 0.09 | – | – | – | – | – | 1.21 | 0.96 |
| Leukemia | 0.09 | – | – | 0.41 | – | 0.75 | – | – |
| Unspecified | 0.38 | – | – | 0.41 | 1.06 | – | – | 4.82 |
Note: ASMR was calculated based on the number of death and the respective population size.
Figure 4.
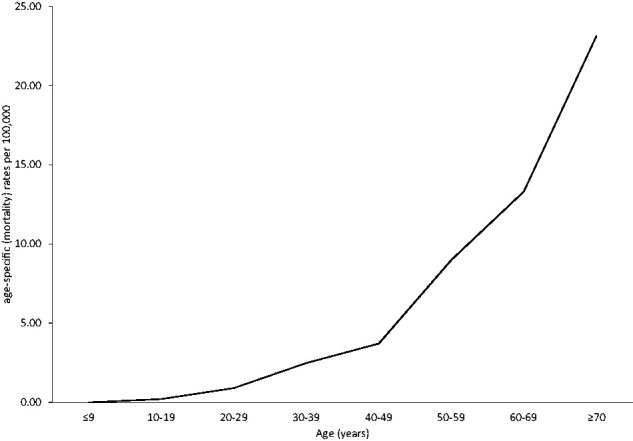
Age-specific mortality rates of all types of cancers.
Discussion
There have been strategies to reduce the incidence of cancers in Ghana25–27; however, the disease remains a threat to the health of the Ghanaian populace. Our current study was designed to examine the various types of cancers reported to hospitals in the Volta Region of Ghana with the aim of contributing to the cancer data in the country. The average age of patients diagnosed with cancer in the Volta Region of Ghana is relatively lower than those in other Regions in the country. This observation was made from the mean age of 44.5 years determined from this study and compared to the mean ages of 52.3 and 51.6 years that have been previously reported for Greater Accra8 and Ashanti Regions,17 respectively. The mean age of patients diagnosed with cancer globally is between 40 and 50 years, with lower ages reported in developing countries compared to developed countries.28 Although the mean age for all cancer from our current report is within the global range and corresponds to that of developing countries, the previous studies from Ghana8,17 reported higher mean ages compared to the global mean.
Higher incidence of cancer among females compared to males is reported in our study and consistent with previously published data in Ghana.8,17 In contrast to our result, the GLOBOCAN data in 20182 and 201929 estimated a higher global incidence in males compared to females. However, studies among Ethiopians,30 Asian Americans, Native Hawaiians, Pacific Islanders,31 and African Americans32 presented an estimate of more females living with cancer compared to males which is similar to our data.
The decrease in the number of cancer cases with increasing level of education, and the observed highest number of diagnosed cancer cases in farmers and traders suggest that socioeconomic factors influence the prevalence of cancer. Farmers and traders are among the less educated in Ghana, and the findings are consistent with a study from the Ashanti Region of Ghana that reported the largest number of diagnosed cancer cases among traders.17 Socioeconomic factors such as level of education and occupation have also been shown to influence the prevalence of cancers in other parts of the world.33,34
Prostate and cervical cancers were the most diagnosed cancers in the Volta Region from 2012 to 2014. This conclusion stems from the number of cases diagnosed from the Region over the three-year period. A global report showed that lung, breast, prostate, and cervical cancer are the most frequently diagnosed cancers2; however, there are geographic variability across the world’s regions. In Ghana, a recent study identified prostate cancer as the most common cancer among men.2 Cancer awareness and increased screening for prostate cancer by hospitals in Ghana to facilitate early detection and treatment,9 may account for the high number of reported cases. Even though cervical cancer has been reported as the most common cancer among women in the Greater Accra and Ashanti Regions of Ghana,35 other studies, also from the Greater Accra and Ashanti Regions, have identified breast cancer as the most frequent cancer diagnosed among Ghanaian women.14,17 There are therefore varied reports as to whether breast or cervical cancer is the most prevalent cancer in Ghanaian women. It has, however, been established that breast cancer is the most common female cancer globally followed by cervical cancer.36,37
There have been intensive public awareness and educational programs on breast cancer prevention in Ghana since 2007. The breast cancer awareness was championed by organizations such as Mammocare Ghana and the Cancer Society of Ghana.13 The public knowledge and governmental attention given to breast cancer, possibly accounted for the decline of breast cancer cases compared to cervical cancer cases in our report. In addition, the 2011 national strategy for cancer control in Ghana adopted and implemented routine screening for HPV and HPV-induced cervical cancer in all major hospitals.9 This possibly contributed to the increased number of cervical cancer cases recorded in our study from 2012 to 2014.
Another frequently diagnosed cancer in the Volta Region over the period under consideration in this study was soft tissue cancer, which is a heterogenous group of different types of sarcoma. A review of cancer-related autopsies at a major referral hospital in Ghana, and a study that assessed the incidence of cancers in the Ashanti Region of Ghana, both estimated soft tissue cancer to have a prevalence of 1.7% of all cancer cases.17,38 Our study however showed a significantly higher prevalence (16%) of diagnosed soft tissue cancer cases among cancer patients in the Volta Region of Ghana. Although inherited genetic syndromes, and chemical and radiation exposures have generally been shown to be risk factors of soft tissue cancers, the cause of soft tissue cancers in the Volta Region of Ghana is unclear. Apart from soft tissue cancer, liver cancer is also one of the frequently diagnosed cancers in the Volta Region and accounted for 12% of all the diagnosed cancer cases in this study. The percentage was however lower compared to previous studies in Ghana (21%) and Benin (23%).39 In Nigeria, another West African country, liver cancer was found to be the least (1.4%) diagnosed cancer among other cancers,40 with a prevalence that falls significantly below the global value.2
Mortality of cancer patients in the Volta Region increased with age. This observation was obtained from the ages at which the incidence of death due to cancers was diagnosed in the Region and reported in this study. The above trend was consistent with several studies and may be explained by the positive correlation between cancer mortality and age-specific rate of all cancers. Liver cancer had the highest mortality in this study. The high mortality caused by liver cancer may be due to hepatic infections and lifestyle risk factors such as smoking, diet, and radiation exposure, which are associated with the disease. The global mortality of liver cancer was estimated at 8.2%2 and global statistics suggest that majority of liver cancer deaths can be accounted for by hepatitis B virus (HBV) (33%), alcohol (30%), and hepatitis C virus (HCV) (21%).41 The prevention and protection against hepatitis viruses and alcoholic hepatitis would thus be important in the reduction of liver cancer mortality rate.42 A five-year retrospective study on hepatic viruses conducted at the Volta Regional Hospital recorded a prevalence of 6.94% and 1.84% for HBV and HCV, respectively.43 A hepatitis B sero-prevalence study conducted among blood donors at the same regional hospital recorded an overall prevalence of 7.5%, which suggests that the Region is an intermediate to high endemic region for HBV infection.44 Although smoking is not a major public health problem in Ghana, the risk factor has been associated with the development of liver and kidney cancers in the country.17 Other reports from Ghana also identified breast, cervical, liver, and prostate cancers as the leading causes of cancer mortality.8,17,25 HPV is the major cause of cervical cancer in Ghana, and the cancer accounts for about 8% of all cancer deaths in the country.38 Globally, lung, colorectal, stomach, liver, and breast cancers result in the highest estimated deaths.2,45
Our study could not effectively control for inter-hospital multiple registrations of patients since there is no single patient identification code across the various hospitals used. Thus, the study considered the patient’s home address and date of admission to control for the inter-hospital multiple registrations. The study did not also report on the mode or method of cancer diagnosis, the stage of cancer, and/or the method of treatment, since the information was not available in the hospital diagnosis data that were retrieved from the patients’ files. Other useful general indicators of cancer such as topography and morphology were also missing from the data.
Conclusion
Prostate, soft tissue, liver, breast, and cervical cancers are the commonly diagnosed cancers in the Volta Region of Ghana from 2012 to 2014, with liver cancer being the leading cause of mortality. There was a modest effort by other researchers in Ghana to determine the incidence of the disease in the country; however, most of these studies were conducted in the Greater Accra and Ashanti Regions. This study therefore gives an alternative perspective of the incidence of cancers in Ghana and emphasizes the need for a national effort to effectively estimate the incidence and mortality of cancer in the country. We propose the set-up of PBCRs in all Regional capitals to collect data on cancers to aid in policy and decision making to curb the burden of cancers in Ghana.
Authors’ contributions
Conceptualization, OQ, and SMA; methodology, OQ, SMA, SL, RA, and DNKQ; analysis and interpretation of data, OQ, SMA, SL, RA, and DNKQ; Manuscript draft SMA; Critical review and editing, OQ, SMA, SL, RA, and DNKQ; All the authors read and approved the final version of the manuscript.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge the support of the West African Centre for Cell Biology of Infectious Diseases (WACCBIP) for this study. Samuel Mawuli Adadey is supported by WACCBIP DELTAS PhD fellowship; Sylvester Languon, Richmond Ayee, and Darius NK Quansah are supported by WACCBIP ACE Masters fellowship.
ORCID iD
Osbourne Quaye https://orcid.org/0000-0002-0621-876X
References
- 1.Fitzmaurice C, Allen C, Barber RM, Barregard L, Bhutta ZA, Brenner H, Dicker DJ, Chimed-Orchir O, Dandona R, Dandona L. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: a systematic analysis for the global burden of disease study. JAMA Oncol 2017; 3:524–48 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018; 68:394–424 [DOI] [PubMed] [Google Scholar]
- 3.WHO. The global cancer observatory . [WHO fact sheet]. Geneva: WHO, 2019 [Google Scholar]
- 4.Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer 2015; 136:E359–E86 [DOI] [PubMed] [Google Scholar]
- 5.Fidler MM, Bray F, Soerjomataram I. The global cancer burden and human development: a review. Scand J Public Health 2018; 46:27–36 [DOI] [PubMed] [Google Scholar]
- 6.Torre LA, Bray F, Siegel RL, Ferlay J, Lortet‐Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin 2015; 65:87–108 [DOI] [PubMed] [Google Scholar]
- 7.Boyle P, Ferlay J. Cancer incidence and mortality in Europe, 2004. Ann Oncol 2005; 16:481–8 [DOI] [PubMed] [Google Scholar]
- 8.Calys-Tagoe BN, Yarney J, Kenu E, Amanhyia NA, Enchill E, Obeng I. Profile of cancer patients’ seen at korle Bu teaching hospital in Ghana (a cancer registry review). BMC Res Notes 2014; 7:577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ministry_of_Health. National strategy for cancer control in Ghana 2012–2016, Accra, Ghana. Ghana: Ministry of Health, 2011 [Google Scholar]
- 10.Aikins Ad G. Ghana’s neglected chronic disease epidemic: a developmental challenge. Ghana Med J 2007; 41:154–9 [PMC free article] [PubMed] [Google Scholar]
- 11.Armah FA, Gyeabour EK. Health risks to children and adults residing in riverine environments where surficial sediments contain metals generated by active gold mining in Ghana. Toxicol Res 2013; 29:69–79 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kitcher E, Yarney J, Gyasi R, Cheyuo C. Laryngeal cancer at the korle Bu teaching hospital Accra Ghana. Ghana Med J 2006; 40:45–9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Clegg-Lamptey J, Hodasi W. A study of breast cancer in korle Bu teaching hospital: assessing the impact of health education. Ghana Med J 2007; 41:72–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Mensah AC, Yarney J, Nokoe SK, Opoku S, Clegg-Lamptey J. Survival outcomes of breast cancer in Ghana: an analysis of clinicopathological features. Open Access Library J 2016; 3:1–11 [Google Scholar]
- 15.Gyasi R, Tettey Y. Childhood deaths from malignant neoplasms in Accra. Ghana Med J 2007; 41:78–81 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Yamoah K, Beecham K, Hegarty SE, Hyslop T, Showalter T, Yarney J. Early results of prostate cancer radiation therapy: an analysis with emphasis on research strategies to improve treatment delivery and outcomes. BMC Cancer 2013; 13:23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Laryea DO, Awuah B, Amoako YA, Osei-Bonsu E, Dogbe J, Larsen-Reindorf R, Ansong D, Yeboah-Awudzi K, Oppong JK, Konney TO. Cancer incidence in Ghana, 2012: evidence from a population-based cancer registry. BMC Cancer 2014; 14:362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Vermeer DE. Geophagy among the ewe of Ghana. Ethnology 1971; 10:56–72 [Google Scholar]
- 19.Nugent P. ‘A few lesser peoples’: the Central Togo minorities and their Ewe neighbours Ethnicity in Ghana. Berlin: Springer, 2000, pp. 162–82
- 20.Ghana_Statistical_Service . 2010 population and housing census. Accra, Ghana: Ghana Statistical Service, 2013 [Google Scholar]
- 21.Dadzi R, Adam A. Assessment of knowledge and practice of breast self-examination among reproductive age women in akatsi South district of Volta region of Ghana. PLoS One 2019; 14:e0226925. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Binka C, Nyarko SH, Awusabo-Asare K, Doku DT. Barriers to the uptake of cervical cancer screening and treatment among rural women in Ghana. Biomed Res Int 2019; 2019:6320938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kortei NK, Koryo-Dabrah A, Akonor PT, Manaphraim NYB, Ayim-Akonor M, Boadi NO, Essuman EK, Tettey C. Potential health risk assessment of toxic metals contamination in clay eaten as pica (geophagia) among pregnant women of Ho in the Volta region of Ghana. BMC Pregnancy Childbirth 2020; 20:7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Statistics_Canada. Age-standardized rates. [Special Interest]. Ottawa, Canada: Statistics Canada, 2017 [Google Scholar]
- 25.Nartey Y, Hill P, Amo-Antwi K, Asmah R, Nyarko K, Yarney J, Damale N, Cox B. Recommendations for cervical cancer prevention and control in Ghana: public education and human papillomavirus vaccination. Ghana Med J 2018; 52:94–102 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Zelle SG, Nyarko KM, Bosu WK, Aikins M, Niëns LM, Lauer JA, Sepulveda CR, Hontelez JA, Baltussen R. Costs, effects and cost‐effectiveness of breast cancer control in Ghana. Trop Med Int Health 2012; 17:1031–43 [DOI] [PubMed] [Google Scholar]
- 27.Hsing A, Mante S, Mensah J, Kyei M, Yarney J, Vanderpuye V, Beecham K, Tettey Y, Biritwum R, Adjei A. Management of prostate cancer in Accra, Ghana. J West African Coll Surg 2016; 6:31–65 [PMC free article] [PubMed] [Google Scholar]
- 28.Bray F, McCarron P, Parkin DM. The changing global patterns of female breast cancer incidence and mortality. Breast Cancer Res 2004; 6:229–39 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Pilleron S, Sarfati D, Janssen‐Heijnen M, Vignat J, Ferlay J, Bray F, Soerjomataram I. Global cancer incidence in older adults, 2012 and 2035: a population‐based study. Int J Cancer 2019; 144:49–58 [DOI] [PubMed] [Google Scholar]
- 30.Memirie ST, Habtemariam MK, Asefa M, Deressa BT, Abayneh G, Tsegaye B, Abraha MW, Ababi G, Jemal A, Rebbeck TR. Estimates of cancer incidence in Ethiopia in 2015 using population-based registry data. J Glob Oncol 2018; 4:1–11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Torre LA, Sauer AMG, Chen MS, Jr, Kagawa‐Singer M, Jemal A, Siegel RL. Cancer statistics for Asian Americans, native Hawaiians, and pacific islanders, 2016: converging incidence in males and females. CA Cancer J Clin 2016; 66:182–202 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.DeSantis CE, Miller KD, Goding Sauer A, Jemal A, Siegel RL. Cancer statistics for African Americans, 2019. CA A Cancer J Clin 2019; 69:211–33 [DOI] [PubMed] [Google Scholar]
- 33.Balcazar H, Castro FG, Krull JL. Cancer risk reduction in Mexican American women: the role of acculturation, education, and health risk factors. Health Educ Q 1995; 22:61–84 [DOI] [PubMed] [Google Scholar]
- 34.Yan B, Yang L-M, Hao L-P, Yang C, Quan L, Wang L-H, Wu Z, Li X-P, Gao Y-T, Sun Q. Determinants of quality of life for breast cancer patients in Shanghai, China. PLoS One 2016; 11:e0153714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Nartey Y, Hill PC, Amo-Antwi K, Nyarko KM, Yarney J, Cox B. Cervical cancer in the Greater Accra and Ashanti regions of Ghana. J Glob Oncol 2016; 3:782–90 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Adanu RM. Cervical cancer knowledge and screening in Accra, Ghana. J Womens Health Gend Based Med 2002; 11:487–8 [DOI] [PubMed] [Google Scholar]
- 37.Han X, Wang Q, Wang Y, Hu B, Dong X, Zhang H, Wang W. Long non‐coding RNA metastasis‐associated lung adenocarcinoma transcript 1/microRNA‐202‐3p/periostin axis modulates invasion and epithelial–mesenchymal transition in human cervical cancer. J Cell Physiol 2019; 234:14170–80 [DOI] [PubMed] [Google Scholar]
- 38.Wiredu EK, Armah HB. Cancer mortality patterns in Ghana: a 10-year review of autopsies and hospital mortality. BMC Public Health 2006; 6:159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Agyare C, Spiegler V, Asase A, Scholz M, Hempel G, Hensel A. An ethnopharmacological survey of medicinal plants traditionally used for cancer treatment in the Ashanti region, Ghana. J Ethnopharmacol 2018; 212:137–52 [DOI] [PubMed] [Google Scholar]
- 40.Sowunmi A, Alabi A, Fatiregun O, Olatunji T, Okoro US, Etti A. Trend of cancer incidence in an oncology center in Nigeria. West Afr J Radiol 2018; 25:52 [Google Scholar]
- 41.Akinyemiju T, Abera S, Ahmed M, Alam N, Alemayohu MA, Allen C, Al-Raddadi R, Alvis-Guzman N, Amoako Y, Artaman A. The burden of primary liver cancer and underlying etiologies from 1990 to 2015 at the global, regional, and national level: results from the global burden of disease study 2015. JAMA Oncol 2017; 3:1683–91 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Awuku Y, Yeboah-Afihene M. Hepatitis B at-Birth dose vaccine: an urgent call for implementation in Ghana. Vaccines 2018; 6:15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Lokpo SY, Osei-Yeboah J, Norgbe GK, Owiafe PK, Ayroe F, Ussher FA, Dakorah MP, Gameli Deku J, Manaphraim NYB, Akomanin Asiamah E. Viral hepatitis endemicity and trends among an asymptomatic adult population in Ho: a 5-Year retrospective study at the Ho municipal hospital, Ghana. Hepat Res Treat 2017; 2017:6174743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Osei E, Lokpo SY, Agboli E. Sero-prevalence of hepatitis B infection among blood donors in a secondary care hospital, Ghana (2014): a retrospective analysis. BMC Res Notes 2017; 10:391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin 2017; 67:7–30 [DOI] [PubMed] [Google Scholar]