

INTRODUCTION
It is an honor to address the American Clinical and Climatological Association, and I want to express my thanks to the DuPonts for giving me this opportunity. I would like to introduce you to the field of space medicine. This is a new, but well-established, discipline that is actually advancing fairly quickly. It's also something that doesn't really get a lot of attention, so the chance to share this with you is very special for me.
I always like to remind people that there are typically six people in space at any given time. We've had a continual human presence on the International Space Station (ISS) since October 2000, and that's pretty significant. The standard ISS compliment was three crew members until about 2009, after which we plussed up to six. This is a thriving effort that, of course, did not start with the ISS. Before that, the United States partnered with Russia throughout most of the 1990s on the Mir space station and Shuttle–Mir program. The Mir station was launched in 1988, and from that time until the year 2000, there was also a human presence. With the exception of a short gap between the Mir and ISS programs, humans have been in orbit continually for over three decades. This gives us a rich history to draw on as we characterize the human response to this novel environment.
I also like to emphasize that the station truly is international. This is a picture of the crew currently in residence that was taken on the morning of October 18, 2019 (Figure 1). We see two Russian cosmonauts, Alexander Skvortsov and Oleg Skripochka, American physician astronaut Dr. Andrew Morgan, Italian astronaut Luca Parmitano, and our two celebrated American women Jessica Meir and Christina Koch. The rather formidable space suits they are wearing show they are about to go out the door to do the first two-woman spacewalk. I and many of us on the inside were surprised with all the attention, since we see them as just part of our cadre and their time had come; but we're not lost on what this moment meant and the inspiration that resulted. Of course, these two ladies absolutely rocked it, so we're really proud of them.
Fig. 1.

The Expedition 62 crew aboard the International Space Station the morning of October 18, 2019. From left are Jessica Meir (suited), Alexander Skvortsov, Oleg -Skripochka, Andrew Morgan, Luca Parmitano (front), and Christina Koch (suited). (-Photo courtesy NASA)
Now to the field of space medicine. I will point out that the iconic series Star Trek cemented the prominent role of a medical officer in future space exploration, as well as something much more intriguing. For Dr. McCoy to render medical aid, he had to first determine from what planet his patient hailed, what species they were, and what anatomy and physiology were involved. The very idea that there was an extraterrestrial aspect to medicine was fascinating to me and many others, and as it turns out altered anatomy and physiology are exactly what we see as I will describe below. Aerospace medicine is a board-certified specialty under the auspices of the American Board of Preventive Medicine, with formal civil and military residency training programs. Graduates serve in the military by supporting high-performance aviation operations as well as the corporate world serving commercial airline transport. Human space flight is a subspecialty of aerospace medicine; not surprisingly, we employ several aerospace medical specialists at the National Aeronautics and Space Administration (NASA). A very interesting new twist is the commercial space flight industry, with companies such as Space X, Blue Origin, and Virgin Galactic creating other markets for space medical expertise.
I will emphasize the contemporary understanding of the human in space, but I will also note that we are nearly 60 years into the human spaceflight experience. Since Russian cosmonaut Yuri Gagarin first orbited the Earth in April 1961, over 560 souls have ventured off the planet in various transport spacecraft and space stations, and this has produced a rich legacy of knowledge and practice. Much of this information can be downloaded freely from NASA and other government sites and I encourage all to explore this database.
I will focus on weightlessness, as it is such an incredible driver for the physiologic changes we see in space. However, other unique occupational exposures influence the human space experience as well as the practice of space medicine. These include ionizing radiation, acceleration forces, pressure excursions, noise, and psychological stress. Radiation exposure is actually the greatest limitation to human occupation of space due to cumulative cancer risk, and these others profoundly influence human health and performance. All of these health risks must be interpreted and managed against a backdrop of adaptation to weightlessness or fractional gravity.
LEAVING THE PLANET
When we launch into space, we traverse several boundaries and zones highly relevant to humans and hardware. The ISS orbits at about 240 nautical miles of altitude, which is really not that far away from Earth. But we must accelerate to orbital velocity—roughly 17,500 mph at this altitude—and cross some of these meaningful boundaries. Above 10,000 feet or so, supplemental oxygen is required for high-performance aircraft. (Commercial airliners are pressurized to equivalent altitudes of 6,000–8,000 feet.) Once you reach 34,000 feet, that's as high as you can go breathing 100% oxygen without positive pressure. Ascend a few thousand feet more and you must provide a protective atmosphere, either a space suit or fully pressurized cabin. At roughly 50,000 feet, the ambient pressure is about 87 millimeters of mercury (mmHg), which is equivalent to the combined pressures of carbon dioxide and water vapor in the lungs; as such, oxygen exchange becomes theoretically impossible. Armstrong's line, at roughly 63,000 feet, is very important to us. At that altitude, the ambient pressure is 47 mmHg, which is the vapor pressure of water at body temperature; water will literally boil off the tongue and conjunctival surfaces. So these are the conditions we protect our passengers from with spacecraft and suits; since we are now building new ones for the first time in decades, this understanding is of even greater relevance.
One other limit of significance is the Karman line, at roughly 100 kilometers. The international community has decided that this is the border of space for those who want to fly and become astronauts—you get above the Karman line, you get your astronaut wings, so to speak. Because of this, the suborbital tourist enterprises, such as Virgin Galactic and Blue Origin, will fly people to about 101 kilometers after powered ascent and a brief few minutes of weightlessness. One hundred kilometers seems like a nice round number, but this is not an arbitrary limit. Above this altitude, the atmosphere is so rarefied that aerodynamic services such as wings and rudders are basically ineffective; you are definitively in rocket territory.
This is my crew on the day of my first flight (Figure 2). I was launching on a Russian Soyuz from the Baikonur Cosmodrome in Kazakhstan. In the middle is Russian commander Gennady Padalka, recognized as one of the best fliers in the business and the record holder for most cumulative days in space at 879 days. I'm the flight engineer on the right, and on the left is Charles Simonyi. Charles flew as a spaceflight participant, which is a fancy phrase for tourist and he paid tens of millions of dollars to fly with us. Interestingly, he was flying for a second time, so on this flight, I, as the American professional astronaut, was the rookie. To calibrate the understanding of our “tourist,” Charles is one of the early fathers of Microsoft, with a PhD in computer science, and is a type-rated jet pilot. Of the seven spaceflight participants that have flown to the ISS, six made their fortunes in the tech industry so these guys are already adventurous nerds, rather like us. It was a pleasure to fly with Charles.
Fig. 2.

The crew of Soyuz TMA-14 on launch morning at the Baikonur Cosmodrome in Kazakhstan, wearing Russian Sokol launch and entry suits. From left are Charles Simonyi, Gennady Padalka, and Michael Barratt. Less obvious are the crew-assigned space flight surgeons behind each crewmember, from left Drs. Richard Jennings, Vadim Shevchenko, and Edward Powers. Flight surgeons are among the last to see the crew before they depart and the first to see them on return. (Photo courtesy NASA)
Just as we launch over the ocean, Russia launches over the vast Kazakh steppe to avoid dropping spent stages onto populated areas. (
Soyuz Launch.
) As the engines build enough thrust to equal the mass of the rocket stack, ingeniously simple cantilever supports fall away and up we go. It's actually a very gentle ascent; we almost can't tell we have left the pad until we see our clock start counting up. There is the noise of course, a very deep crackling roar, characteristic of rocket engines. As we build speed, acceleration or g-forces will start to make us feel a bit heavier. Again, we have to attain 17,500 mph, orbital velocity, and that's what these rockets do. Yuri Gagarin launched from this same pad in 1961, and it was an incredible honor to launch from there (Figure 3). Why is Russia still using it? Because it works; it's simple and elegant in its engineering. My second flight was aboard the Space Shuttle, quite a bit different form the Soyuz. I was very lucky to fly one of the last missions of the Shuttle program, on the good ship Discovery. You can see here (Figure 4) that it was quite a bit more massive than the Soyuz, with a lot of engine thrust offset from the center of mass. All of this was connected by struts and hard points so there was a lot of vibration. (
Space Shuttle Launch.
) After two minutes, the two side solid rocket boosters burned out and separated, and it's amazing how much smoother the ride got at that point as we continued uphill with very well-mannered liquid engines.
Fig. 3.

Liftoff of the Soyuz TMA-14 spacecraft on its way to the International Space Station. (Photo courtesy NASA)
Fig. 4.

Liftoff of the Space Shuttle Discovery on February 24, 2011, for the STS-133 mission. Discovery carried six crewmembers and the last U.S. permanent module to join with the other elements and complete the assembly of the International Space Station. (Photo courtesy NASA)
Looking at the acceleration profiles of the Soyuz and the Shuttle, you see different g loads over time. The Soyuz shows a sharp spike—we get up to almost 4½ g before first stage separation and then we get up to a little bit more than that for the second stage. As you can see in -Figure 5, there are three spikes, all related to staging as engines burned out after consuming the fuel in that stage. The peak g loads were lower in the Shuttle, but if you integrate the area beneath these two curves the resultant velocity is the same—our 17,500 mph sustaining orbital velocity. Another interesting aspect is shown as you look at the right side of the curve; there is nothing gradual about the transition from high-g to zero-g. We go from weighing three or four times our body weight to zero instantly. This simple looking flat vertical line on the curve represents one of the most amazing moments of a crew member's life. At that time, we're pressed hard into our seat and all of a sudden it's quiet; the roar of the engine stops and instantly we're floating forward, we see things that we thought were tied down start to fly in front of us, and we feel a rush of fluid shift toward our chest and toward our head as if we were just hung upside down. It's a busy moment as the crew ensures that the spacecraft has survived the ascent phase, which is pretty rough on hardware, so we're looking for any leaks in the cabin atmosphere and fuel tanks. We are ensuring that our ship is healthy enough to remain in space, and oh by the way, we see the Earth from space for the first time which is just overwhelming. Along with this, we sense that all of our body's neurosensory inputs are immediately and radically altered, with various consequences. It is an amazing moment, the one I wish we could share with everyone.
Fig. 5.

Ascent acceleration (g) profiles for the U.S. Space Shuttle and Russian Soyuz spacecraft. (Source: Barratt, Space Physiology and Medicine; Ernsting's Aviation and Space Medicine, 4th Edition, 2016.)
This is the ISS (Figure 6), the most popular destination in low Earth orbit, taken from Discovery on the STS-133 mission. Coincidently, large Japanese and European cargo vehicles were already docked there, along with two Soyuz crew vehicles and a smaller Russian cargo vehicle. Adding the volume of Discovery when we docked, we became the biggest pressurized volume in history. Many think we must be crowded and bump into each other, but the station really is quite large. And although we are considered a remote environment, we are only 240 nautical miles above the surface of the Earth. But remember we're traveling at 17,500 miles an hour. It takes tremendous energy to build that velocity and to shed that velocity to slow down to come home. What makes us remote is more of a velocity barrier than a distance barrier. The cabin atmosphere is at sea-level pressure, which is 14.7 psi, 80% nitrogen, 20% oxygen. This keeps it as earth-like as possible so that weightlessness is really the big variable in a science. Food is highly preserved, in such forms as freeze-dried, ready-to-eat military rations, and some canned food. But variety is great because it's very international now, which is quite pleasant.
Fig. 6.

The International Space Station, taken from the flight deck of the Space Shuttle Discovery on the STS-133 mission. (Photo courtesy NASA)
As you probably imagine, the views of Earth are pretty stunning. This is my friend Samantha Cristoforetti in the most popular place on the space station, the cupola (Figure 7). It resembles a big bay window that hangs down towards the Earth and I say “down” because it all depends on our preferred reference frame when we go in there. If we are looking down so to speak, it's like looking through a glass bottom boat, and we use a set of coordinates that are based on that being down. Or we may want the opposite experience, so we flip upside down with our head toward the glass; now we're looking up at the Earth as if through a cathedral dome. Whenever we have spare minutes, we are looking out the window. Here are two contrasting views of Earth as we see it from space (Figure 8); crystal blue oceans and coral atolls on the left and western Africa on the right with sand dune patterns shifting over time. The ISS is a powerful platform for Earth observation, partly because we're not that high above the Earth and partly because we have a lot of smart observers up there with cameras that can take advantage of chance events. On June 12, 2009, my crewmates and I were looking to photograph Tokyo, which was unfortunately clouded over. But Gennady noticed a smoke trail as we tracked northeast, so we happened to have three big cameras with three big lenses at the ready when we flew right over this (Figure 9). The Saryachev Peak in the Kuril Islands had just exploded in a violent volcanic blast that took place under a crater lake at the top of the cone. The white cloud visible in the photograph is that lake and some snowpack, which had turned to a cloud of steam in the blast. Also visible is a pyroclastic flow. We were the first to see and report this, which was a magnificent chance observation that provided valuable geological imagery.
Fig. 7.

European Space Agency astronaut Samantha Cristoforetti photographs targets on the surface of the Earth from the station's cupola. (Photo courtesy NASA)
Fig. 8.

Different geographic regions show striking color characteristics viewed from space. (Photos courtesy NASA)
Fig. 9.

The eruption of Saryachev Peak. (Photo courtesy NASA)
WEIGHTLESSNESS
Weightlessness or the absence of gravity is one of the dominant forces that affect our everyday life. Without its influence, there's no sedimentation, the weight-driven separation of particulates in a fluid column. There's no buoyancy, so no separation of fluids whether liquids or gases. Much of what mixes gases in this room are differential weight-induced buoyancies, CO2 being heavier than oxygen for instance. In orbit, there is no buoyancy driven convection. If there's any convection to be had, it must be artificially induced. Consider a candle flame, which normally has a very orderly circuit bringing in fuel and oxygen at the bottom, with resulting combustion products flowing upward as they warm. As these products are taken away, the fuel and oxygen are always replenished. If you strike a match in weightlessness and hold it in a non-ventilated area, it will go out. A little bit of induced convection goes a long way, and it can really flare with an artificial airflow. We study combustion quite a bit because we can control all the factors that influence burning. Diffusion remains intact, however. Normally, diffusion is pretty weak as a gas mixer on Earth, but it is a dominant force in a spacecraft.
The ISS is a very well-equipped laboratory (Figure 10). We do a lot of biomedical experiments, fluid physics, combustion, earth observation, plant growth, and all sorts of experiments. We can draw blood; spin it down a centrifuge; and freeze plasma, serum, urine samples, and animal tissues for later return to Earth. We now have a pretty active rodent research program onboard and several other biological experiments. We can also do metabolic gas analysis. One factor that is part and parcel to weightlessness is glove boxes, which we use to avoid liberation of liquid particulates of anything that we don't want to breathe or otherwise encounter in the atmosphere. Much of our work is done in glove boxes; if anything is particularly hazardous, it requires progressively increased levels of containment. This includes tissue fixatives, such as we use in animal research work and various other chemical reagents.
Fig. 10.
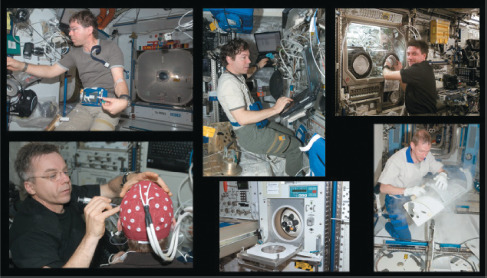
Research laboratory capabilities of the International Space Station. (Photos courtesy NASA)
Many people thought phlebotomy would be very difficult to do in microgravity, but almost any medical procedure that can be done on the ground can be done in space. We take a lot of blood samples for nutrition and metabolism experiments, so every crew member would typically be sampled once a month. A physician crewmember by default becomes the onboard medical officer and ends up doing this for his or her crew, just like I ended up taking blood on most of my crewmates and myself. Mainly we have to learn “zero g-stuff management;” anything we set down is going to float away so we make the best use of Velcro and sticky tape. All of these medical procedures are actually quite doable.
EFFECTS OF WEIGHTLESSNESS ON THE HUMAN
Weightlessness is by far the dominant condition that affects the human in space. That includes most of our medical risks and most of the changes that affect our performance. Interestingly, we have found over the years that these are not necessarily sinister but adaptive; they actually optimize human performance in spaceflight. Once humans have gone through a predictable set of adaptations, they start to perform quite well up there. However, they pay for it when they want to go home as some of these adaptations become maladaptive upon return to Earth and its gravity field. Periods of adaptation accompany “g-state transitions,” and performance may be compromised during these adaptive periods. For context, I am showing my colleague Alvin Drew zipping himself into a sleeping bag (Figure 11). It looks like he's standing up, but there is no up or down. We have this orientation for photos and video for viewers on the ground so they don't get disoriented.
Fig. 11.

NASA astronaut Alvin Drew secures his sleeping bag before turning in for the night. (Photo courtesy NASA)
It is somewhat arbitrary but convenient to divide the process of adaptation to weightlessness into three main phases, and each of those phases can be fairly conveniently divided into three main system responses. In the first phase, with changes evident within seconds to minutes, we see anthropometry, fluid shift, and neurosensory manifestations.
Here we see the neutral body posture (Figure 12), which is realized immediately upon arrival into weightlessness. We can see this once we are free of restraints. If we purposely make ourselves very rigid and then suddenly relax, we will snap into this position in two or three seconds with a couple of dampening motions. It's basically the sum of the contractive forces of the larger limb and trunk muscles. This is the new body posture that must be accommodated when designing a workstation, sleeping station, medical restraint, or other body interface. If we try to restrain the body in a recumbent position on a flat surface, it's actually uncomfortable. Figure 13 shows me working with the metabolic gas analyzer. I've got my toes under a rail and I can reach everything that I need to reach and that is the new natural posture I want. Along with this neutral body posture comes some anthropometry changes. Abdominal girth decreases and thoracic diameter increases. Consider that abdominal viscera are normally suspended from the diaphragm on mesenteric tissue; remove gravity and the diaphragm floats upwards. With abdominal viscera moving toward the head, the waist gets thinner. The chest actually increases in volume, mostly along an antero-postero dimension, causing it to circularize. We also see spinal lengthening of typically 3 to 6% in seated height. How much of this involves straightening of thoracic curvature and how much stems from intervertebral disc changes is still under study. But it's relevant since much of our flight gear is highly customized. The space suit or custom seat liner we fit into preflight may be a tight fit with a 6% spinal growth, so we have to allow for that.
Fig. 12.

The neutral body posture of weightlessness.
Fig. 13.

With my feet loosely tucked beneath a restraint rail, the rest of me naturally assumes the neutral body posture. (Photo courtesy NASA)
We use the moniker “fluid shift” for the global changes that result from abolishing the hydrostatic gradient along tissues and blood column, as well as the compressive force on vasculature from the weight of body tissues. This causes much of the blood in the lower extremities to shift toward the thorax and head. Almost immediately after the ascent engines cut off, we feel like we're hanging upside down, with a strong sense of facial congestion. Here are pictures of my Russian cosmonaut colleague Yuri Onufrienko before launch and in flight (Figure 14 ). You can see a bit of puffiness in the head, which is worse at the beginning of flight. This improves somewhat over several days, but everybody feels this stuffiness to some degree. It's not a pleasant feeling for the first few days. Some of this actually starts on the launch pad, because we're lying down with our feet up for two to three hours before launch and shifting a lot of fluid to our thorax. Figure 15 shows vascular pressure responses related to fluid shifts in weightlessness. Upon standing on Earth, a significant hydrostatic gradient increases venous pressure and capacitance volume below the waist. When recumbent, that gradient is now antero-posterior and a lot shorter, and venous pressures evens out along the body. However this does not mimic spaceflight changes. With the increase in thoracic diameter, thoracic pressure decreases and further drives cephalad migration of lower extremity fluid. Cardiac chambers dilate significantly and remain that way as a new space flight norm.
Fig. 14.

Cosmonaut Yuri Onufrienko before (14A) and during (14B) spaceflight. (-Photos courtesy NASA)
Fig. 15.

-Vascular -pressure gradients in response to postural change and -weightlessness.
Source: Barratt, Space Physiology and Medicine; Ernsting's Aviation and Space -Medicine, 5th Edition.
Much of our insight began with a rather bold experiment—the first central line in space. Figure 16 shows two physicians that flew in 1991 on the Space Shuttle Columbia on a dedicated life sciences mission. This is Drew Gaffney, a cardiologist, and Jim Bagian, an internist, flight surgeon, and Air Force para-rescue jumper. Launching with a right heart catheter introduced via an antecubital vein attached to a pressure transducer under the space suit, we obtained immediate central venous pressure data. At that time, we expected to see the central volume shift and central venous pressure (CVP) increase. However, CVP actually decreased. Shown in Figure 17 is a representative pressure tracing from a subsequent and confirmatory experiment. The reference posture for the baseline in the suit room was a seated position. You can see lots of vibration affecting the pressure signal in parallel to the now familiar launch acceleration profile below. With engine cut off, we expected CVP to resemble a recumbent value, but in fact, the baseline was actually lower than the seated value. So CVP decreased in spite of this significant fluid shift to the chest. It is very counterintuitive, and we thought these results were anomalous, so we did this three more times and the results were always the same.
Fig. 16.

Physician astro-nauts James Bagian (left) and Andrew Gaffney (right) during the STS-40 mission on the Space Shuttle, the first dedicated space life sciences mission. (Photo courtesy NASA)
Fig. 17.

Central -venous pres-sure during ascent and arrival into weightlessness. (Source: Foldager, et al. J Appl Physiol 1996;81:408–12.)
We didn't adequately factor the thoracic pressure decrease into our understanding at the time. One of our test venues is parabolic flight, which involves maneuvers that afford about 25-second periods of weightlessness. Using human subjects instrumented with central lines and esophageal manometers confirmed that thoracic pressure decreases quite readily and quickly. Interestingly, there is an observable increase in transmural pressure across the heart because surrounding pressure in the thorax decreases even more. This discovery was somewhat surprising and arguably revolutionized our understanding of cardiovascular regulation in space.
Other interesting aspects of fluid shifting in weightlessness involve a cardio-renal response, what we used to call the Gauer Henry response, and diminished plasma volume. With a sensed volume overload terrestrially, we expect an atrial stretch receptor response and elevated renal perfusion with a resulting diuresis. We indeed see cardiac chambers dilate; stroke volume increases about 27%, and cardiac output increases 29% within seconds of arriving in weightlessness. We have demonstrated this on parabolic flight as well. Mean arterial pressure doesn't change, and the only way that can happen is from a compensatory increase in vascular compliance, which is indeed what happens. However, we do not see a resulting diuresis. This is countered by the observation of a 12 to 15% reduction in plasma volume. Isotopically labeled water studies have confirmed that total body water doesn't change. To make a very long story short, about 10 to 15% of circulating plasma volume extravasates into the interstitial tissue and eventually into the intracellular space along with its sodium. This begins immediately but requires several days to complete. We will address the resulting hemo-concentration in the subacute phase.
The third of three affected systems in the acute phase is the neurosensory response. All of the inputs that determine sense of position and guide locomotion are radically altered in weightlessness. The otoliths of the neuro-vestibular system are relieved of their gravitational load and will only move with induced motion. Vision is a very powerful input advising a stable vertical reference, but in weightlessness “up” is arbitrary and what you choose to make it. With joints and bone/muscle interfaces unloaded, proprioceptive inputs are significantly diminished, as are tactile inputs from the soles of the feet. With radical alteration of these inputs that are centrally integrated to determine position sense and guide locomotion, the initial response is often sensory conflict.
We have our own version of sea sickness. Space adaptation syndrome is a blanket term of which space motion sickness is a part. This may occur fairly rapidly, even after just a few minutes following main engine cutoff, and it can occur suddenly and with little warning. Along with frank emesis, we see decreased appetite, fatigue, and lethargy. The incidence on early Shuttle flights was noted to be 60 to 70% for first-time flyers. This can be very incapacitating for the first several hours for some, but most are able to continue working through the symptoms. Interestingly, as we progressed in the Shuttle program, the incidence decreased to about half of what it was before. Much of this was likely thanks to cognitive strategies, avoiding provocative motions, as well as strategic use of medications prophylactically, and early treatment. Use of intramuscular promethazine is extremely effective (upwards of 95%) and is used often during these first few flight hours.
These acute effects occurring in the first several minutes to hours give way to subacute effects that are more or less bounded to the first 7 to10 days. The main processes involve adaptive changes in fluid regulation, blood volume and composition, and neurosensory adaptation. As mentioned above, there is a loss of 12 to 15% of circulating plasma volume, which leads to a relative state of hemo-concentration. Apparently, this is not well tolerated, and the body responds by quickly ridding itself of what it considers an excess number of red blood cells (RBC) in a process called neocytolysis. Facilitated by a significant decrease in erythropoietin, newly minted nucleated erythrocytes are selectively destroyed until a normal concentration appropriate to the new plasma volume is attained. This phenomenon was first seen in space flight and elucidated by Bobby Alford's team. Chromium tagged red blood cell studies were performed both in the late Apollo and early Shuttle programs. Along with the RBC dropout, there are measurable increases in circulating iron and bilirubin, reflective of the lytic process in action. We have since recognized this phenomenon in a couple of terrestrial scenarios, and I refer you to an outstanding review by Rizzo and colleagues noted in the selected references. It's a great example of something we found because we fly in space because we took the force of gravity away and let the body show us things that were otherwise prevented or masked by gravity.
Although central blood volume does increase and atrial stretch receptors are intact, in weightlessness the cardio-renal response is uncoupled for reasons not entirely understood. In spite of this central volume shift, the glomerular filtration rate does not change. Mechanistically, there appears to be an increase in vascular permeability allowing oncotic proteins (mostly albumin) to flow out, with plasma water following. This creates a new norm, which is about 15% less circulating plasma volume.
An interesting concern to us is nephrolithiasis. We frequently see a reduced fluid intake and urine volume, and for whatever reason thirst seems to be somewhat attenuated. When coupled with increased bone resorption in weightlessness and the subsequent urinary spilling of calcium and phosphate, at the least the theoretical risk increases. In practice, one case occurred inflight over 30 years ago on the Russian Salyut station. However, we have seen a definite increased incidence in renal stones in the postflight period following spaceflight. Therefore, we perform renal stone risk profiles on all crewmembers, perform targeted ultrasound surveillance, and encourage oral hydration while on board.
Following the acute shock of neurosensory conflict, neurosensory adaptation continues in a more pleasant way. Figure 18 is a picture of me and my crewmates on my first day on the ISS. I had spent two days on the tiny Russian Soyuz doing a rendezvous flight; then all of a sudden we docked and were in a large volume, which from a neuro--vestibular standpoint is fairly challenging because we no longer had walls everywhere to keep us in position. Here I am holding on to a handrail as hard as I can and onto my friend Kowichi Wakata, and I have both feet under foot rails because of a perception of falling in every direction. It takes several weeks for a first-time flyer to fully adapt to a 3--dimensional position and locomotion sense. Contrast that image with one a few months into flight; Figure 19 shows the spaceflight posture and me floating comfortably in the middle of a module, holding onto one handrail. It's just remarkable how we transform into 3-dimensional creatures. One little illustrative twist: normally on the ground we're used to walking with our legs and carrying things with our arms, but walking has no meaning up there. We pull ourselves along with handrails and kickoff sometimes and fly like Superman. Figure 20 shows me holding three 20-pound food containers which I can carry comfortably between my legs, fly them 60 feet, and drop in a desired position.
Fig. 18.

First day aboard the International Space Station after a two-day rendezvous flight aboard the relatively tiny Soyuz spacecraft and holding on tight! (Photo courtesy NASA)
Fig. 19.

Floating comfortably in the middle of a module a few months in with minimal restraint. (Photo courtesy NASA)
Fig. 20.

An interesting reversal of what limbs are used for—locomotion versus carrying loads. (Photo courtesy NASA)
Long-term effects on the cardiovascular and musculoskeletal systems actually begin immediately but require weeks to months to manifest. Along with the effects of weightlessness, these are also dependent on the equilibrium resulting from diet and exercise -countermeasures—areas where we can have some influence. We mentioned earlier that cardiac output and stroke volume increase fairly immediately by 27 or 28%, and our early Shuttle flights suggested that these values may return to a preflight norm within the time period of a Shuttle flight, typically 10 days or two weeks. However, when we finally did definitive studies during six-month ISS missions, we saw these pressure values continue to decrease, compared with preflight seated posture. Systolic, diastolic, and mean arterial pressures decreased by 8, 9, and 10 -millimeters of mercury, and stroke volume and cardiac output continued to increase. Along with this, systemic vascular resistance showed a compensatory decrease. Somewhat paradoxically, sympathetic tone remains normal or even slightly high. We can stress the cardiovascular system with an orthostatic challenge in space using lower body negative pressure, which emulates standing, and a totally normal sympathetic response results.
An additional landmark investigation was the Integrated Cardio-vascular Study, a very comprehensive inflight effort involving 13 subjects. This has helped put to rest some concerns about cardiac deconditioning in long duration weightlessness. There had been worry about cardiac atrophy in spite of countermeasures, but this was not seen. Early inflight ultrasound studies also hinted at a cardiomyopathic structural change, but what we were interpreting, or misinterpreting, is the more spherical shape of the heart in weightlessness, due to the unloaded diaphragm and pericardium. It returns fairly quickly to its more familiar ellipsoid shape upon return. We have also worried about malignant dysrhythmias, and at least one crew member, a Russian cosmonaut, was returned to Earth early because of a new onset supraventricular tachycardia that had not been seen on the ground. But this may have been completely incidental to the flight experience and not due to any arrhythmogenic effect of weightlessness. In any case, with fairly extensive monitoring, we have not seen anything worrisome.
We do inflight fitness assessments more or less monthly. Aerobic capacity typically decreases during the first assessment by 10 to 12%, and with subsequent assessments you tend to creep up toward normal as the months go by. Some crewmembers actually get back to their preflight norm while in flight. The first value obtained following landing again shows a decline. We usually wait until return day 4 or 5 before performing a max test, mainly to avoid injury. It's important to note the significant readaptation processes in play in the immediate post-landing period. As such, performance assessments during this time do not necessarily reflect how well a crewmember completed their inflight countermeasure exercises. However, it does suggest that not too much should be expected of people when they're freshly landed from a cardiovascular standpoint.
Now a little more about musculoskeletal atrophy. Figure 21 shows my friend Bill Shepherd who commanded the first ISS mission. He was a U.S. Navy SEAL—a very strong guy. This photo was taken four months into flight. From the waist down, you can see unduly skinny legs; trust me, before he launched, his legs were commensurate with his arms. A loss of postural muscle mass follows the fluid shift from lower extremities. We measure calf circumference to assess volume and by default muscle mass, mainly to help guide countermeasures. We refer to the resulting disuse atrophy of the lower extremities as “bird legs” or “chicken legs.”
Fig. 21.

NASA astronaut Bill Shepherd four months into the first crewed flight aboard the International Space Station. (Photo courtesy NASA)
Relatively new in our countermeasures inventory is a resistive exercise device that affords heavy axial loads (up to 600 pounds) for exercises like squats, deadlifts, and heel raises. Toward the end of my mission, I was doing nearly 550 lb. heel raises; while that may sound impressive, it is quite peculiar to our weightless environment. Doing heel raises here on the ground involves lifting me and whatever is on the bar, but in space body weight counts for nothing. It also means that the force distribution is very different from what we're used to on the ground. In space, all that force now comes across the shoulder and is transmitted down the spinal column and to the feet rather than just being distributed throughout the body. Great care must be taken to maintain spinal alignment during these loaded exercises. However, this machine has really revolutionized our ability to maintain postural bone and muscle in space. Aside from the resistive device, we also have two bicycles and two treadmills for the six crewmembers aboard. All crewmembers are scheduled for two and a half hours of daily exercise, spread between the resistive aerobic devices. All of these devices are vibration isolated so they don't impart these big mechanical loads to the stack that may cause structural fatigue.
Figure 22 shows a histogram of bone mineral density loss as assessed by pre- and postflight DXA scans, again with the zero line representing preflight baseline. The dominant loss is in the postural bones that endure the brunt of weight bearing during terrestrial standing and locomotion. These sites represent our main areas of interest in tracking bone loss and recovery: lumbar spine, pelvis, femoral neck, greater trochanter, and calcaneus. We have seen a progressive decrease in bone density loss due to improved countermeasures across crews aboard the Mir station, the ISS before, and the ISS after the use of heavy resistive exercise. We're going in the right direction with heavier loads and exercises that target these areas of loss. Surprisingly, we do not lose and may actually gain bone in the wrist, and we usually see a 1 or 2% increase in skull density.
Fig. 22.

Bone mineral density changes in International Space Station astronauts. (Source: Principles of Clinical Medicine for Space Flight, Springer, 2019.)
In the past 10 years or so, a constellation of neuro-ophthalmic findings has become a central focus of our attention. It involves rather critical neuroanatomy that might affect performance during a mission or long-term health outcomes. Although the changes that we see seem formidable, the only actual symptom that rises to the clinical horizon is a hyperopic vision shift that is likely due to the globe flattening. We see striatal folds in the choroid of the retina in a certain number of people, as well as optic disc edema. A few people have experienced cotton wool spots and an increase in optic nerve sheath diameter, which make up the major findings in what we now call Spaceflight Associated Neuro-Ocular Syndrome. The optic disc edema suggests there may be an increased intracranial pressure (ICP) phenomenon going on, which presents a dilemma. How do you clinically approach those who are totally asymptomatic other than their hyperopic vision shift? Correlating the level of ICP that might correspond to these findings terrestrially causes us to worry.
The MRI imagery in Figure 23 shows some of the classic -findings—globe flattening, optic nerve sheath distension, and a curious -laterality—which seem to be weighted toward the right side. It also shows a gender preference, with the greater expression in males. After characterizing this in long duration ISS crew, we looked back at our Space Shuttle records and discovered that in over 500 flight experiences 23% of the crew noticed a subjective change in their visual acuity and 11% had a documented degradation. These were short flights that lasted a couple weeks or less. We had thought this was at least partially due to age-related presbyopia, but now we know better. By looking retrospectively at 3T MRI images from a smattering of long and short duration flyers, we saw some of these subtle changes. Although the expression varies, the incidence of this syndrome is likely 100%, which is probably reflecting a phase of adapting to the zero gravity environment that we didn't recognize until recently. It is at the same time very exciting but also very disturbing. We typically see postflight resolution of optic disc edema in those that manifest it, but other changes such as globe flattening, optic nerve sheath distension, and the hyperopic vision shift may be permanent. There is now an intensive focus on possible associated long-term health outcomes.
Fig. 23.

Postflight 3T MRI imagery showing classic neuro-ophthalmic findings associated with prolonged stays in weightlessness. Arrows on the right close-up image show the posterior globe flattening (small arrows) and central protuberance of the optic disc (large arrow). (Source: Evidence Report Risk of Spaceflight Associated Neuro-ocular Syndrome. NASA Human Research Program. Approved for Public Release: November 30, 2017.)
Space flight involves several potential contributing factors that may lead to these findings. First and foremost is the cephalad fluid shift. CO2 is known to be a very strong cerebral vasodilator, and our CO2 level on the ISS is more than 10 times the atmospheric level from crewmember respiration. Removing CO2 from the cabin atmosphere and scrubbing down to a normal level using chemical absorbent beds is very energy intensive. The findings seem to show greater expression in males, and there may be some metabolic and fluid regulatory components as well. Some have related this to the arrival of heavy resistive exercise inflight, since we started observing this in earnest about the time the resistive exercise device arrived. However, looking back, we found a study that showed half of the 16 cosmonauts on the Mir station had some degree of postflight disc edema. We have also seen classic findings in at least one Skylab astronaut from the 1970s. So this is not new, nor is it due to resistive exercise or confined to Americans.
Figure 24 shows a lower-body negative pressure device, which the Russians use as a countermeasure on orbit in the days prior to landing to get used to gravity pulling down fluids from the central circulation. Again it reintroduces a hydrostatic challenge. As shown in Figure 25, we also used it as part of the Fluid Shift experiment. This is astronaut Scott Kelly during his nearly yearlong mission. This device allows us to assess the effects of fluid shifts against the expression of neuro--ophthalmic findings.
Fig. 24.

Russian “Chibis” lower body negative pressure device. (Photo courtesy NASA)
Fig. 25.

NASA astronaut Scott Kelly in the lower body negative pressure device taking part in the Fluid Shift experiment, which assessed pulse, blood pressure, and ultrasound imagery of cerebral venous vasculature in response to simulated orthostatic challenge. (Photo courtesy NASA)
The bar graph in Figure 26 shows the distribution of neuro-ophthalmic findings for long duration astronauts on the ISS. As of 2017, of 64 tested, 10 had optic disc edema denoted as Frisen Grade 1 or higher. The other findings I mentioned earlier are distributed here, and it's noteworthy that they do not necessarily coincide in the same subjects. While we have seen a few individuals with moderate ICP elevations postflight, we really have no idea what the ICP is in space. Along with pre- and postflight MRI and other studies, we now perform periodic inflight ophthalmic ultrasound, higher resolution fundus imagery, and optical coherence tomography (OCT), which at least gives us insight into some of the end organ effects over time. We are aggressively pursuing measuring ICP inflight as we work to determine long-term implications of this entity.
Fig. 26.

Distribution of neuro-ophthalmic findings in long duration crewmembers. USOS = US On-orbit Segment. SANS = spaceflight associated neuro-ocular syndrome. (Source: Evidence Report: Risk of Spaceflight Associated Neuro-ocular Syndrome. NASA Human Research Program. Approved for Public Release: November 30, 2017.)
Most of the adaptive changes associated with weightlessness are not problematic, unless you want to come home. Earlier, I showed a video of two vehicles in their launch phase. Here is what landing looks like in each of these. (
Space Shuttle Landing.
) Following atmospheric entry, the Space Shuttle flew and landed like a cargo plane, affording a gentle landing that made up for the rough Shuttle launch. The crewmembers were seated upright as in an aircraft, which introduced an early vertical load on the hydrostatic column.
Compare this with landing in the Soyuz (https://www.youtube.com/watch?v=eyHknE6nJsA). Here you see a single parachute. During atmospheric entry, that speed of 17,500 miles an hour has now been traded for vertical velocity. Before this point, we can see how hot it is on the outside as we use atmospheric friction to slow down. Our outer window melts before our eyes, and sparks are flying as our heat shield ablates. It takes about seven minutes to more or less fall straight down and back toward the Kazakh Steppe. Many dynamic events occur during this time such as parachute deploy, heat shield jettison, and reorientation of the seats for landing impact. This is all done using pyro cartridges, so there is lots of noise, fire, and sudden motion. About a meter above the ground, landing engines fire in a pulse fashion to cushion the impact. In reality, it feels like two successive significant impacts. Compared to the Space Shuttle, the Soyuz offers a gentle launch but we pay for it on landing. Nevertheless, the Soyuz is an elegant vehicle—it is by far the safest human carrier in history, and it will be a long time before its record is beaten.
Figure 27 illustrates the landing acceleration profiles of the two vehicles. The Soyuz on the left shows large spikes up to 4½ g; the Shuttle is gentler by comparison. A significant difference is the orientation in which you take those g-loads. Crewmembers are recumbent in the Soyuz so that these loads are all through the chest, in what we call the body “X” axis. Although the loads are lower in the Shuttle, they are imparted more directly along the vertical hydrostatic blood column in the body “Z” axis, introducing an early orthostatic challenge. In the early Shuttle days, we actually had people briefly lose consciousness at 1½ g during the turn to final approach. Adaptation to weightlessness renders the human exquisitely sensitive to orthostatic intolerance. As we have seen, vascular volume and red blood cell mass are decreased, baroreceptors are deconditioned, and vascular compliance is high. This warrants protective countermeasures. Along with this cardiovascular challenge is the neuro-vestibular deconditioning. Everything that makes us humans optimal for living and moving freely in three dimensions now bites us as signals governing position sense and locomotion must again be reinterpreted. This is manifested as Entry Adaptation Syndrome, which includes difficulty in walking and handling postural challenges, as well as entry motion sickness with nausea and emesis reminiscent of arrival into weightlessness. This may be compounded with generalized weakness, depending on how well inflight exercise countermeasures were followed.
Fig. 27.

Acceleration or g profiles of the U.S. Space Shuttle and Russian Soyuz spacecraft during atmospheric entry prior to landing.
Of the three dominant problems crewmembers experience upon return from space—generalized weakness, orthostatic intolerance, and neuro-vestibular impairment—the latter seems to have emerged as the dominant issue for contemporary crewmembers returning from the ISS. It's not that neuro-vestibular deconditioning has gotten worse, but rather that we have developed fairly effective countermeasures for the other two. Our current countermeasures program allows us to return crew with levels of fitness and strength as never before. We combat orthostatic intolerance with pre-landing oral fluid loading, strategic positioning of crewmembers relative to the entry g vector, anti-orthostatic leg compression garments, and post-landing volume repletion. At this point, however, we have no effective countermeasures for neuro-vestibular deconditioning.
If you ever happen to encounter a freshly returned spacecraft, please consider the clinical approach. You will typically find people that are pale, diaphoretic, and splinting their head to avoid provocative motion inputs. They will be volume depleted and thirsty. Cold oral fluids are welcome and intravenous repletion is very effective. Heat stress is common due to the inevitably warm cabin and thermal properties of the suit, so cooling by removing the suit, using fans, and taking in cold oral fluids are all very useful. The crew should avoid standing and any rapid movements that may be quite provocative. Allow gentle, passive reintroduction to gravitational loads.
Each body system recovers at a different rate, but in general, functionality returns very rapidly. Figure 28 shows curves depicting some issues discussed above in the immediate postflight period and the rate of recovery. After a six-month flight, it would be hard to tell at a glance who in the room had just returned from space two to three days earlier. However, you can quickly discriminate with a couple of simple tests. The returned flyer will almost certainly fail a Romberg's test, show difficulty cornering while walking, and may still show some orthostatic intolerance in response to a challenge. Because vascular volume is repleted quickly, a slightly low hematocrit may be present until red blood cell mass is restored. Deliberate testing on a posture platform shows balance deficits that typically require two to three weeks to resolve. All of these are used in determining when a crewmember can return to normal activities, such as driving, and to high-performance aviation. There is a mandatory 45-day intensive physical rehab program, but crewmembers are typically returned to duty status at about 30 days.
Fig. 28.

Recovery curves associated with spaceflight deconditioning of physiologic -systems as they return back toward terrestrial norms following landing.
CONCLUSION
I will conclude by noting that this is a very unique moment in the spaceflight community. There has never been a time when so many human-rated spacecraft are being built. These are not ideations or PowerPoints; these are actual vehicles being tested and flown, and this effort is multinational. Multiple vehicles from India, Russia, China, and the United States are under construction, and some have been test flown. The United States is building the Orion spacecraft to take us beyond low-Earth orbit for the first time since the Apollo program, as well as the Boeing Starliner and the SpaceX Dragon to carry crewmembers to the ISS. With these endeavors, space medicine is getting bigger, not smaller, as we expand beyond the agency level and include commercial industry and multinational partners.
I would like to draw three conclusions: (1) Weightlessness causes a predictable constellation of changes of which we have a serviceable but incomplete understanding. (2) Most of those changes are adaptive and allow for space flight, though some may be maladaptive for Earth return. (3) A fairly well established space medicine literature base is available. Most of the canon is captured in the texts listed in the reference section, but many classic works associated with programs such as Apollo, Skylab, and Shuttle elegantly describe the biomedical findings as they were captured in earlier days.
Footnotes
Potential Conflicts of Interest: None disclosed.
BIBLIOGRAPHY Textbooks and Overviews
- Principles of Clinical Medicine for Space Flight. 2nd. Springer Publishing; 2019. Barratt, Baker, Pool, eds. [Google Scholar]
- Space Physiology and Medicine. 4th. Springer Publishing; 2016. Nicogossian, Williams, Huntoon, Doarn, Polk, and Schneider, Eds. [Google Scholar]
- NASA Human Research Program Evidence Books. Contemporary and well-referenced treatises on space flight associated medical responses from a risk management basis. Available at: https://humanresearchroadmap.nasa.gov/evidence/.
- Johnston RS, Lawrence F, Dietlein MD, Charles A, Berry MD, editors. Biomedical Results of Apollo. Washington, D.C.: Scientific and Technical Information Office, NASA; 1975. [Google Scholar]
- Johnston RS, Dietlein LF, editors. Biomedical Results from Skylab. Washington, D.C.: Scientific and Technical Information Office, NASA; SP-377. [Google Scholar]
- Biomedical Results of the Space Shuttle Program. D. Risin and P.C. Stepaniak, Editors. 2013. NASA/SP-2013-607.
Selected Articles Cardiovascular
- Buckey J, Lane L, Levine B, et al. Orthostatic intolerance after spaceflight. J Appl Physiol. 1996;81((1)):7–18. doi: 10.1152/jappl.1996.81.1.7. [DOI] [PubMed] [Google Scholar]
- Buckey JC, Gaffney FA, Lane LD, et al. Central venous pressure in space. J Appl Physiol. 1996;81:19–25. doi: 10.1152/jappl.1996.81.1.19. [DOI] [PubMed] [Google Scholar]
- Norsk P, Damgaard M, Petersen L, et al. Vasorelaxation in space. Hypertension. 2006;47((1)):69–73. doi: 10.1161/01.HYP.0000194332.98674.57. [DOI] [PubMed] [Google Scholar]
- Foldager N, Andersen TA, Jessen FB, et al. Central venous pressure in humans during microgravity. J Appl Physiol. 1996;81((1)):408–12. doi: 10.1152/jappl.1996.81.1.408. [DOI] [PubMed] [Google Scholar]
- Fritsch-Yelle JM, Charles JB, Jones MM, Beightol LA, Eckberg DL. Spaceflight alters autonomic regulation of arterial pressure in humans. J Appl Physiol. 1994;77((4)):1776–83. doi: 10.1152/jappl.1994.77.4.1776. [DOI] [PubMed] [Google Scholar]
- Wantier M, Estenne M, Verbanck S, Prisk GK, Paiva M. Chest wall mechanics in sustained microgravity. J Appl Physiol. 1998;84((6)):2060–5. doi: 10.1152/jappl.1998.84.6.2060. [DOI] [PubMed] [Google Scholar]
- Verheyden B, Liu J, Beckers F, Aubert AE. Adaptation of heart rate and blood pressure to short and long duration space missions. Res Physiol & Neurobiol. 2009;169S:S13–S16. doi: 10.1016/j.resp.2009.03.008. [DOI] [PubMed] [Google Scholar]
- Meck JV, Waters WW, Ziegler MG, et al. Mechanisms of post-spaceflight orthostatic hypotension: low alpha1-adrenergic receptor responses before flight and central autonomic dysregulation postflight. Am J Physiol Heart Circ Physiol. 2004;286((4)):H1486–95. doi: 10.1152/ajpheart.00740.2003. [DOI] [PubMed] [Google Scholar]
- Baevsky RM, Baranov VM, Funtova II, et al. Autonomic cardiovascular and respiratory control during prolonged spaceflights aboard the International Space Station. J Appl Physiol. 2007;103:156–61. doi: 10.1152/japplphysiol.00137.2007. [DOI] [PubMed] [Google Scholar]
- Hughson RL, Shoemaker JK, Blaber AP, et al. Cardiovascular regulation during long-duration spaceflights to the International Space Station. J Appl Physiol. 2012;112:719–27. doi: 10.1152/japplphysiol.01196.2011. [DOI] [PubMed] [Google Scholar]
- Norsk P, Asmar A, Damgaard M, Christensen NJ. Fluid shifts, vasodilatation and ambulatory blood pressure reduction during long duration spaceflight. J Physiol. 2015;593:573–84. doi: 10.1113/jphysiol.2014.284869. [DOI] [PMC free article] [PubMed] [Google Scholar]
Fluid and Volume Regulation
- Leach CS, Alfrey CP, Suki WN, et al. Regulation of body fluid compartments during short-term spaceflight. J Appl Physiol. 1996;81((1)):105–16. doi: 10.1152/jappl.1996.81.1.105. [DOI] [PubMed] [Google Scholar]
- Norsk P, Drummer C, Rocker L, et al. Renal and endocrine responses in humans to isotonic saline infusion during microgravity. J Appl Physiol. 1995;78((6)):2253–9. doi: 10.1152/jappl.1995.78.6.2253. [DOI] [PubMed] [Google Scholar]
- Drummer C, Norsk P, Heer M. Water and sodium balance in space. Am J Kidney Dis. 2001;38((3)):684–90. doi: 10.1053/ajkd.2001.27765. [DOI] [PubMed] [Google Scholar]
Hematology
- Alfrey CP, Udden MM, Leach-Huntoon C, Driscoll T, Pickett MH. Control of red blood cell mass in spaceflight. J Appl Physiol. 1996;81((1)):98–104. doi: 10.1152/jappl.1996.81.1.98. [DOI] [PubMed] [Google Scholar]
- Rice L, Alfrey CP. Modulation of red cell mass by neocytolysis in space and on Earth. Pflugers Arch. 2000;441((2-3 Suppl)):R91–4. doi: 10.1007/s004240000333. [DOI] [PubMed] [Google Scholar]
- Risso A, Ciana A, Achilli C, Antonutto G, Minetti G. Neocytolysis: none, one or many? A reappraisal and future perspectives. Frontiers in Physiol. 2014;5:54. doi: 10.3389/fphys.2014.00054. Feb. [DOI] [PMC free article] [PubMed] [Google Scholar]
Neuro-Vestibular
- Reschke MF, Bloomberg JJ, Harm DL, Paloski WH, Layne C, McDonald V. Posture, locomotion, spatial orientation, and motion sickness as a function of space flight. Brain Res Brain Res Rev. 1998;28((1-2)):102–17. doi: 10.1016/s0165-0173(98)00031-9. [DOI] [PubMed] [Google Scholar]
- Mulavara AP, Feiveson AH, Fiedler J, et al. Locomotor function after long--duration space flight: effects and motor learning during recovery. Exp Brain Res. 2010;202:649–59. doi: 10.1007/s00221-010-2171-0. [DOI] [PubMed] [Google Scholar]
Musculoskeletal
- Lang T, LeBlanc A, Evans H, Lu Y, Genant H, Yu A. Cortical and trabecular bone mineral loss from the spine and hip in long duration spaceflight. J Bone Miner Res. 2004;19((6)):1006–12. doi: 10.1359/JBMR.040307. [DOI] [PubMed] [Google Scholar]
- Sibonga JD, Evans HJ, Sung HG, et al. Recovery of spaceflight-induced bone loss: bone mineral density after long-duration missions as fitted with an exponential function. Bone. 2007;41((6)):973–8. doi: 10.1016/j.bone.2007.08.022. [DOI] [PubMed] [Google Scholar]
- Smith SM, Heer MA, Shackelford L, et al. Benefits for bone from resistance exercise and nutrition in long-duration spaceflight: evidence from biochemistry and densitometry. J Bone Miner Res. 2012;27((9)):1896–1906. doi: 10.1002/jbmr.1647. [DOI] [PubMed] [Google Scholar]
- Moore AD, Downs ME, Lee SM, et al. Peak exercise oxygen uptake during and following long-duration spaceflight. J Appl Physiol. 1985;117((3)):231–8. doi: 10.1152/japplphysiol.01251.2013. 2014 Aug 1. [DOI] [PubMed] [Google Scholar]
Neuro-Ophthalmic Changes
- Mader, Gibson, Pass, et al. Optic disc edema, globe flattening, choroidal folds, and hyperopic shifts observed in astronauts after long-duration space flight. Ophthalmology. 2011;118:2058–69. doi: 10.1016/j.ophtha.2011.06.021. [DOI] [PubMed] [Google Scholar]
- Stenger MB, et al. Risk of Spaceflight Associated Neuro-ocular Syndrome (SANS). Evidence Report, NASA Human Research Program, Human Health and Countermeasures Element. NASA Johnson Space Center 2017.
- Zhang LF, Hargens AR. Spaceflight-induced intracranial hypertension and visual impairment: pathophysiology and countermeasures. Physiol Rev. 98((1)):59–87. doi: 10.1152/physrev.00017.2016. 2018 Jan 1. [DOI] [PubMed] [Google Scholar]
- Kramer LA, Sargsyan AE, Hasan KM, et al. Orbital and intracranial effects of microgravity: findings at 3T MRI imaging. Radiology. 2012;263((3)):819–27. doi: 10.1148/radiol.12111986. (Epub 2012 Mar 13) [DOI] [PubMed] [Google Scholar]
- Lawley JS, Petersen LG, Howden EJ, et al. Effect of gravity and microgravity on intracranial pressure. J Physiol. 2017;595:2115–27. doi: 10.1113/JP273557. [DOI] [PMC free article] [PubMed] [Google Scholar]
Miscellaneous
- Prisk GK. Microgravity and the lung. J Appl Physiol. 2000;89:385–96. doi: 10.1152/jappl.2000.89.1.385. [DOI] [PubMed] [Google Scholar]
- Iwasaki K, Levine BD, Zhang R, Zuckerman JH, et al. Human cerebral autoregulation before, during and after spaceflight. J Physiol. 2007;579:799–810. doi: 10.1113/jphysiol.2006.119636. [DOI] [PMC free article] [PubMed] [Google Scholar]