

Supplemental Digital Content is available in the text.
Keywords: pandemics, reperfusion, restaurants, stroke, viruses
Background and Purpose:
Anecdotal evidence suggests that the coronavirus disease 2019 (COVID-19) pandemic mitigation efforts may inadvertently discourage patients from seeking treatment for stroke with resultant increased morbidity and mortality. Analysis of regional data, while hospital capacities for acute stroke care remained fully available, offers an opportunity to assess this. We report regional Stroke Team acute activations and reperfusion treatments during COVID-19 mitigation activities.
Methods:
Using case log data prospectively collected by a Stroke Team exclusively serving ≈2 million inhabitants and 30 healthcare facilities, we retrospectively reviewed volumes of consultations and reperfusion treatments for acute ischemic stroke. We compared volumes before and after announcements of COVID-19 mitigation measures and the prior calendar year.
Results:
Compared with the 10 weeks prior, stroke consultations declined by 39% (95% CI, 32%–46%) in the 5 weeks after announcement of statewide school and restaurant closures in Ohio, Kentucky, and Indiana. Results compared with the prior year and time trend analyses were consistent. Reperfusion treatments also appeared to decline by 31% (95% CI, 3%–51%), and specifically thrombolysis by 33% (95% CI, 4%–55%), but this finding had less precision.
Conclusions:
Upon the announcement of measures to mitigate COVID-19, regional acute stroke consultations declined significantly. Reperfusion treatment rates, particularly thrombolysis, also appeared to decline qualitatively, and this finding requires further study. Urgent public education is necessary to mitigate a possible crisis of avoiding essential emergency care due to COVID-19.
Coronavirus disease 2019 (COVID-19) has become a global pandemic. While people increasingly seek hospitalization for COVID-19, several hospitals have anecdotally reported fewer patients being treated for other serious conditions, most notably myocardial infarction and stroke.1 This is unexpected, as early reports suggest stroke risk to be greater with COVID-19 due to resultant cardiomyopathy, arrhythmias, hypercoagulability, and shared vascular risk factors.2–4 Acute stroke treatments are highly time-sensitive and impactful (numbers needed to treat, 3–8, to prevent disability).5
We reviewed regional data to test the hypothesis that, in association with COVID-19 mitigation efforts, Stroke Team consultations and reperfusion treatments of intravenous thrombolysis and thrombectomy declined.
Methods
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Stroke Team Database
The University of Cincinnati Stroke Team consists of multidisciplinary stroke specialists who provide 24/7 consultation and direct treatment via telemedicine or in person to all 30 acute care facilities in 23 counties in Southwest Ohio, Northern Kentucky, and Eastern Indiana, capturing ≈2 million inhabitants (Figure I in the Data Supplement). Per a regional protocol, the Stroke Team is activated to discuss potential treatment of all patients with ongoing stroke symptoms and last known well within 24 hours presenting in the emergency department or in the hospital. All activations are prospectively documented by physicians in an internal, secure database for quality assessment.
Study Design
We reviewed Stroke Team activations from December 30, 2019, through April 12, 2020. Ohio announced upcoming closure of all schools and restaurants in an effort to contain COVID-19 on March 126 and Kentucky on March 13, 2020.7 Three time periods were assessed: (1) 2020 pre–COVID-19 mitigation (weeks 1–10, 2020), (2) 2020 post–COVID-19 mitigation announcements (weeks 11–15, 2020), and (3) 2019 mid-March to mid-April (weeks 11–15) as a reference. Data were totaled each week, starting Monday. We secondarily reviewed reperfusion treatments during the same periods. We also explored thrombolysis versus thrombectomy rates and median National Institutes of Health Stroke Scale at presentation among reperfusion-treated patients. The study activity did not constitute human subjects research that required Institutional Review Board oversight. There was no intervention or interaction with a living individual for research purposes, and no identifiable private information was obtained, used, studied, analyzed, or generated for this study.
Statistical Methods
Weekly rates for each period were computed by summing the total events and dividing by the total weeks. These rates were compared by the Poisson test as the primary analysis and presented as the percentage change and 95% CIs using the central method. National Institutes of Health Stroke Scale between time windows of interest were compared using the Wilcoxon rank-sum test. Trends over time were visualized graphically. As a secondary analysis, segmented regression analysis was used to account for time trends. The 2019 activation and treatment trends served as a reference. Based on increased stroke activations and treatments noted visually in week 10, and concern that this unduly influenced results, we performed a sensitivity analysis removing week 10 data and recomputed rates and comparisons using the same approach. SAS 9.4 and R 3.5.2 were used.
Results
From December 30, 2019, to April 12, 2020, the Stroke Team received 1689 stroke activations and treated 117 patients with thrombolysis alone, 43 patients with both thrombolysis and thrombectomy, and 27 patients with thrombectomy alone.
As per the Table, stroke activations per week declined by 39% (95% CI, 32%–46%) in the month after announcement of measures to mitigate COVID-19. Stroke reperfusion treatments also appeared to decline by 31% (95% CI, 3%–51%) in the 5 weeks after statewide closure announcements, although confidence limits were wide. Thrombolysis rates appeared to decline by 33% (95% CI, 4%–55%) while the numerical 20% decline in thrombectomy rates did not show significance (95% CI, −37% to 55%). Stroke severity among treated patients appeared to be lower post-COVID mitigation (weekly median National Institutes of Health Stroke Scale score, 16 versus 8; P=0.04), but comparable to 2019 (weekly median National Institutes of Health Stroke Scale score, 8 versus 7; P=0.49).
Table.
Acute Stroke Characteristics Pre- and Post–COVID-19 Mitigation Efforts

Stroke Team activation rates for the first 15 weeks of 2019 and 2020 from the first week of January to the second week in April are shown in Figure 1. A nonsignificant increasing trend in activations was observed in 2019 (P=0.07) and in 2020 before the COVID-19 restrictions (P=0.10). Accounting for time trends, stroke calls per week in 2020 declined by 42% ([95% CI, 28%–52%]; P<0.01) after COVID containment announcements. This reduction is similar to that observed without accounting for time trends (Table). Compared with 2019, we observed a significant decline in stroke activations when accounting for trends in 2020 (36% decline [95% CI, 24%–47%]).
Figure 1.

Trends in total regional Stroke Team calls in the first 15 wk of 2019 and 2020. The dashed lines are the predicted regression lines of the trend in number of stroke calls in 2019 and in 2020 from the segmented regression analysis.
The total number of stroke reperfusion treatments for weeks 1 to 15 of 2019 and 2020 are shown in Figure 2 and by reperfusion therapy type in Figure II in the Data Supplement. Trends were flat in 2019, with an increasing trend in 2020 before week 11 (6% increase [95% CI, 1%–11%]). Immediately following the announcements of closures in week 11, stroke reperfusion treatments per week appeared to decline by 62% ([95% CI, 35%–78%]; P<0.01) with, and 31% without, accounting for time trends. Compared with 2019, treatments per week post–COVID-19 trended toward a decline (36% [95% CI, 3%–60%]; P=0.07).
Figure 2.
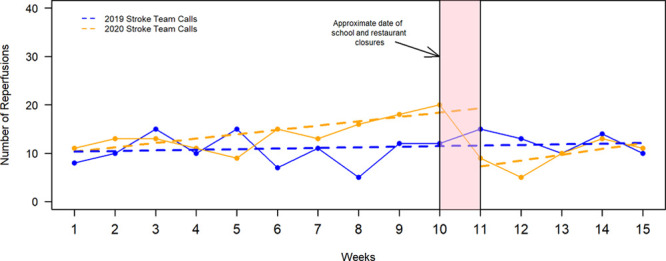
Trends in total regional reperfusions in the first 15 wk of 2019 and 2020. The dashed lines are the predicted regression lines of the trend in number of reperfusions in 2019 and in 2020 from the segmented regression analysis.
We noted increased stroke activations and treatments visually in week 10 that may have biased results. However, a sensitivity analysis removing week 10 data still showed a decline in stroke activations (P<0.01) and a trend (P=0.06) toward a decline in reperfusion treatments and more specifically thrombolysis treatments (Table I in the Data Supplement).
Discussion
In our Tri-State region, following the announcement of COVID-19 preventive efforts, we witnessed 39% reduction in stroke consultations. We also observed a 31% reduction in reperfusion treatment, primarily related to reduced thrombolysis rates, but with less confidence.
During this time period, bed utilization and COVID hospitalized data suggest that the Tri-State healthcare systems were not overwhelmed (Table II in the Data Supplement); for example, the average bed utilization in the most populated county of Hamilton was 62.4%.8–10 Similarly, Hamilton County dispatch centers reported the weekly mean (SD) number of 9-1-1 runs was 2263 (SD, 170) for weeks 11 to 15 of 2020, 2538 (SD, 54) for weeks 11 to 15 of 2019, and 2507 (SD, 115) for weeks 1 to 10 of 2020 (Holly Lampton, unpublished data, 2020).
Our findings raise public health concerns. It is unlikely that stroke incidence declined. Thus, the concerning interpretation of our findings is that stroke patients are not seeking emergent care, presenting beyond 24 hours more frequently, or not seeking acute care at all. Even severe strokes may be receiving less or delayed reperfusion treatments. With ongoing encouragement of stay-at-home orders due to COVID-19,11 the observed declines may persist or worsen.
The main limitations of this report include data from a relatively short duration and single region. However, our singular team has served this region for over 30 years and has anecdotally never observed such a reduction in calls and treatments. Other anecdotal reports suggest this experience is not unique to our region or limited to stroke.1
Conclusions
After the announcement of measures to mitigate COVID-19, acute stroke evaluation calls and treatment rates declined significantly in our region. Urgent public education is necessary to mitigate a potential crisis of avoiding time-sensitive and highly impactful emergency treatment during the COVID-19 era. Locally, we are initiating outreach and education to ensure patients continue to seek appropriate emergent treatment.
Acknowledgments
We thank the University of Cincinnati Stroke Team and Tri-State hospitals and their clinical teams.
Sources of Funding
This study was supported by NINDS U24 NS107241.
Disclosures
Dr Khatri: Cerenovus (Investigator Initiated Study grant), Bayer (National Leader), Nervive (NIH Small Business Innovation Research Co-Investigator), Diamedica (Scientific Advisory Board), and Lumosa (consultant). Dr Adeoye is a Founder and Equity Holder at Sense Diagnostics. Dr Grossman: Genentech (speakers bureau) and Biosense Webster (consultant). Dr Kreitzer: Portola (speaker bureau) and Emergency Medicine Cardiac Research and Education Group International Seminars (honorarium). Dr Walsh: Portola Pharmaceuticals (speakers bureau), Novartis (salary support, modest), and Jan Medical, Inc (salary support, modest). Dr Prestigiacomo: International Brain Research Foundation (board member) and Cerenovus (Data Safety Monitoring Board). Dr Flaherty: CSL Behring, Jannsen, and Portola (speakers bureaus); US patents holder (No. 9357970 B2 and 10506936 B2). Dr Broderick: Genentech (TIMELESS [Trial of Thrombolysis in Imaging-Eligible, Late-Window Patients to Assess the Efficacy and Safety of Tenecteplase], salary support). Dr Kircher: Roche (TIMELESS, research funding). The other authors report no conflicts.
Supplementary Material
Nonstandard Abbreviations and Acronyms
- COVID-19
- coronavirus disease 2019
J. Hsiao and E. Sayles are co-first authors.
Drs Adeoye and Khatri are co-senior authors.
For Sources of Funding and Disclosures, see page XXX.
This manuscript was sent to Marc Fisher, Senior Consulting Editor, for review by expert referees, editorial decision, and final disposition.
The Data Supplement is available with this article at https://www.ahajournals.org/doi/suppl/10.1161/STROKEAHA.120.030499.
References
- 1.Sheth K. Hospital Admissions for Strokes Appear to Have Plummeted, a Doctor Says, a Possible Sign People are Afraid to Seek Critical Help. 2020. The Washington Post; https://www.washingtonpost.com/national/health-science/hospital-admissions-for-strokes-appear-to-have-plummeted-a-doctors-says-a-possible-sign-people-are-afraid-to-seek-critical-help/2020/04/08/2048b886-79ac-11ea-b6ff-597f170df8f8_story.html#comments-wrapper. Accessed April 16, 2020 [Google Scholar]
- 2.Driggin E, Madhavan MV, Bikdeli B, Chuich T, Laracy J, Bondi-Zoccai GB, et al. Cardiovascular considerations for patients, health care workers, and health systems during the coronavirus disease 2019 (COVID-19) pandemic. J Am Coll Cardiol. 2020; 20:34637–34644 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Klok FA, Kruip MJHA, van der Meer NJM, Arbous MS, Gommers DAMPJ, Kant KM, Kaptein FHJ, van Paassen J, Stals MAM, Huisman MV, et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb Res. 2020; 191:145–147. doi: 10.1016/j.thromres.2020.04.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wu C, Chen X, Cai Y, Xia J, Zhou X, Xu S, Huang H, Zhang L, Zhou X, Du C, et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern Med. 2020e200994.doi: 10.1001/jamainternmed.2020.0994 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Martinez-Gutierrez JC, Leslie-Mazwi T, Chandra RV, Ong KL, Nogueira RG, Goyal M, Albuquerque FC, Hirsch JA. Number needed to treat: a primer for neurointerventionalists. Interv Neuroradiol. 2019; 25:613–618. doi: 10.1177/1591019919858733 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Office of the Governor State of Ohio Governor Dewine Announces School Closures. 2020. Mike DeWine: Governor of Ohio; https://governor.ohio.gov/wps/portal/gov/governor/media/news-and-media/announces-school-closures. Accessed April 16, 2020 [Google Scholar]
- 7.Office of the Governor State of Kentucky Gov. Beshear Taking Aggressive Action in Response to COVID-19. 2020. Kentucky.gov; https://kentucky.gov/Pages/Activity-stream.aspx?n=GovernorBeshear&prId=88. Accessed April 20, 2020 [Google Scholar]
- 8.Regenstrief Institute. Regenstrief COVID-19 Dashboard. https://www.regenstrief.org/covid-dashboard/. Accessed May 19, 2020
- 9.Ohio Department of Health. State of Ohio: COVID-19 Dashboard. https://coronavirus.ohio.gov/wps/portal/gov/covid-19/dashboards. Accessed May 19, 2020
- 10.Argis.com. Hospital Preparedness Dashboard. https://www.arcgis.com/apps/opsdashboard/index.html#/85054b06472e4208b02285b8557f24cf. Accessed May 19, 2020
- 11.Office of the Governor State of Ohio Ohio Stay At Home Order Extended Through May 1.. 2020. Mike DeWine: Governor of Ohio; https://governor.ohio.gov/wps/portal/gov/governor/media/news-and-media/ohio-stay-at-home-order-extended-through-may-1. Accessed April 16, 2020 [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.