

Abstract
Background:
Psychological stress was an important mental health problem among the general population and warrant research to inform strategies for effective prevention. iMBIs provide a possibility to offer easily accessible, efficacious, convenient, and low-cost interventions on a wide scale. However, the efficacy of iMBIs in the general population remains unclear. The aim of this meta-analysis is to evaluate the effects of iMBIs for stress reduction in the general population.
Methods:
A systematic search in PubMed, Embase, Web of Science, Medline, Cochrane Library, CNKI, and Wanfang Data databases was performed up to April 10, 2019. The overall effect sizes of the iMBIs on stress, depression, anxiety, and mindfulness were recorded by the metric of Hedges’ g with 95% confidence interval (CI), Z-value, and P value.
Results:
Sixteen eligible studies were included in the meta-analysis. The overall results indicated that iMBIs had small to moderate effects on stress (Hedges’ g = −0.393) and mindfulness (Hedges’ g = −0.316) compared with the control group. Results from subgroup analyses revealed that the type of sample and delivery mode had a greater impact on heterogeneity across the studies. Meta-regression found that the overall effect might be moderated by guidance for iMBIs.
Conclusion:
The present meta-analysis suggested that iMBIs had small to moderate effects in reducing stress and improving mindfulness of the general population in comparison with the control group. Future research is needed to explore how iMBIs are remolded to improve adherence and suit specific individuals.
Keywords: Internet mindfulness-based interventions, meta-analysis, mindfulness, stress
1. Introduction
Psychological stress is a continuous feeling of worry about your work or personal life, which prevents you from relaxing. Excessive and chronic amounts of stress, however, may lead to serious health consequences. Current studies indicated that psychological stress was independently associated with the increased risk of stroke,[1] coronary heart diseases[2] and mental illnesses such as depression[3] and anxiety.[3]
Psychological stress has become increasingly common among the general population, especially in students[4] and staff.[5] Therefore, kinds of interventions were designed to help people manage and control stress. Among them, mindfulness-based interventions worked well. A meta-analysis concluded that mindfulness-based stress reduction (MBSR) was effective for reducing stress levels in healthy people.[6]
Mindfulness is the psychological process of focusing attention on experiences occurring in the present moment, which can improve well-being and mental health. Therefore, mindfulness training was introduced in the stress management program by researchers. As mentioned above, MBSR was proposed by Jon Kabat-Zinn, which combined mindfulness meditation, body awareness, and yoga to assist people in mindfulness.[7] Similar interventions were also designed for mentally and physically ill patients, including mindfulness-based cognitive therapy (MBCT)[8] and acceptance and commitment therapy (ACT).[9] The current mindfulness interventions involve various forms, with differences in delivery methods and the number of sessions.
Although the effect of mindfulness in increasing mental health has been proved, face to face delivery restricts its application among the general population. Mental health care is difficult to reach the general population. With the development of Internet technology, Internet-based interventions may solve the problem. A survey was conducted to examine the mindfulness meditation delivery format preferences of adult English speakers. It was concluded that the Internet was a top priority for most participants.[10] Internet mindfulness-based interventions (iMBIs) have unique advantages in reaching the general population. The merits of iMBIs can be listed as follows:
-
(1)
standardized and even more efficient,
-
(2)
not only convenient access to mindfulness resources, but also the ability to control when and where people access the intervention, and
-
(3)
low cost.
A meta-analysis has proved that online mindfulness interventions play an important role in increasing mental health, especially stress.[11] However, the studies involving patients with mental and physical illnesses were also included in the previous meta-analysis. The purpose of this article is to combine the results of studies which investigate the effect of iMBIs only in the general population.
2. Materials and methods
This study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.[12]
2.1. Literature search
Two independent researchers conducted a systematic literature search in databases including PubMed, Embase, Web of Science, Medline, Cochrane Library, CNKI, and Wanfang Data to search for relevant studies form the first available year to 11 Jan 2019 to identify the studies of iMBIs for the general population on stress. The terms were used both in abbreviations and full text as follows: “mindful” or “mindfulness,” “online,” “e-health,” “Internet,” “web” or “app,” “general population,” “students” or “employee,” and “stress”. The last search was performed on 10 April 2019. In addition, we checked the reference lists of related reviews and retrieved articles for additional potentially eligible studies, as well.
2.2. Inclusion and exclusion criteria
To be included in the meta-analysis:
-
(1)
experimental groups must involve MBIs such as MBSR, MBCT, and ACT either with or without guidance,
-
(2)
MBIs should be administrated through the website, a computer, smartphone application, or virtual classrooms,
-
(3)
control groups involved an inactive or active condition,
-
(4)
participants should not have any clinically diagnosed mental or physical disease,
-
(5)
validated outcome measurements must be used for examination of the effectiveness of iMBIs for general population on stress, and
-
(6)
the studies were conducted using a randomized controlled design.
The exclusion criteria were:
-
(1)
the intervention did not involve mindfulness training or combined mindfulness-based training with other psychoeducational therapy such as cognitive behavioral therapy,
-
(2)
sufficient information for the calculation of effect size was not provided in the study, and
-
(3)
articles concluded duplicate or overlapping studies.
This procedure was performed by two researchers and if the disagreement appeared, the third researcher was consulted.
2.3. Data extraction and quality assessment
Full text of eligible articles was independently reviewed by 2 researchers and data extraction was independently conducted at the same time, as well. All disagreement was discussed with the third researcher to reach consensus. Data extracted were as follows:
-
(1)
participants’ characteristics (e.g., type of sample, age, gender distribution);
-
(2)
the intervention characteristics (e.g., type of MBIs, guidance, delivery mode, number of sessions, duration in weeks);
-
(3)
the study characteristics (e.g., number of participants per group, control condition, follow-up timing); and
-
(4)
outcome measurements for stress, depression, anxiety and mindfulness.
In addition, 2 researchers independently assessed the quality of all eligible articles according to the Jadad scale[13] and the Cochrane risk of bias tool.[14] A total score of the Jadad scale ranged from 0 to 7, and the article with a total score of 4 to 7 was considered as high quality.[13] The Cochrane risk of bias tool covered the following items: random sequence generation, allocation concealment, performance and detection bias, incomplete outcome data, selective reporting, and other bias.[14]
2.4. Calculation of effect sizes
The primary analysis was to examine the overall effect size of iMBIs for the general population on stress and mindfulness. To correct the small sample bias, the metric of Hedges’ g was used to record the overall effect size.[15] In within-group analyses, the measures of pre- and post-intervention were not independent, so the correlation between them should be taken into account. Since it was often not available in the articles, recommended by Rosenthal,[16] 0.7 as a conservative estimate for it was used in the meta-analysis when calculating the overall effect. The reported information such as Cohen d, means of pre- and post-treatment and standard deviations for both the experiment and control groups, was converted into Hedges’ g by comprehensive meta-analysis software version 3 (CMA 3.0).[17] If one study contained two experiment groups of different iMBIs and one control group, we calculated the overall effect size of those 2 experiment groups in comparison with the control group respectively. On the other hand, if 1 study contained 2 control groups of different intervention and 1 experiment group, we used the inactive control group such as waitlist for calculation of the overall effect size. Subgroup analyses of the stress studies were performed on the basis of the type of sample (i.e., students, staff, or mixed students and staff) and delivery mode (i.e., application, website, or others). We also conducted a meta-regression using the mixed effects model to explore whether the overall effect of iMBIs for the general population on stress and mindfulness varied across the studies based on the following:
-
(1)
publish year,
-
(2)
type of MBIs (i.e., MBSR, ACT, mindfulness meditation or others),
-
(3)
treatment duration, and
-
(4)
guidance.
Subgroup analyses and meta-regression were conducted to determine whether the variables had contributed to heterogeneity in the meta-analysis. An effect size from 0.00 to 0.32 represented a small effect size, 0.33 to 0.55 represented a moderate effect size and 0.56 to 1.20 represented a large effect size according to Lipsey and Wilson.[18]
2.5. Statistical analysis
Due to the variation (e.g., type of MBIs, delivery mode) across the studies, we assumed the true effect size may not remain stable. Therefore, the overall effect was synthesized on the basis of a random effect model. We pooled the reported data into comprehensive meta-analysis software version 3 to synthesize the effect size of iMBIs for the general population on stress, depression, anxiety and mindfulness using the metric of Hedges’ g with 95% confidence interval (CI), Z-value, and P value and generated a forest plot for the effect size of iMBIs for the general population on stress and mindfulness. The overall heterogeneity between articles was assessed by the I2 and chi-square statistic (Q). The significant Q-Statistic (P ≤ .05) informed the researcher of the presence of significant heterogeneity within the studies. The I2 indicated the percentage of heterogeneity across the primary studies with 25%, 50%, and 75% as low, moderate and high heterogeneity, respectively.[19,20] We also performed sensitivity analyses by excluding every eligible study sequentially to explore potential sources of heterogeneity.
The publication bias was evaluated by a funnel plot, a classic fail-safe N test, and Duval and Tweedle's trim and fill method. A funnel plot showed the asymmetric distribution indicating the potential publication bias.[14] A fail-safe N test estimated the number of unpublished studies needed to lower the effect size below significance.[21,22] Duval and Tweedle's trim and fill method was used to calculate an adjusted effect size by accounting for the impact of these estimated missing studies on overall effect size.[23]
2.6. Ethical approval
This meta-analysis does not require ethical approval or patient consent because the data used in the meta-analysis were extracted from previously published studies which had declared ethical approvals and no original clinical raw data was utilized. This meta-analysis was performed in accordance with PRISMA guidelines.
3. Results
As shown in Figure 1, 347 records were identified through database searching. After removing duplicates, 176 records were screened at the base of the abstract. And 124 of 176 records were excluded due to no relevance. Full text of remained articles was obtained for further assessment. Afterward, 36 articles were removed due to various reasons. Therefore, a total of 16 articles were included in this meta-analysis.
Figure 1.

Flow diagram of literature selection for meta-analysis.
3.1. Characteristics of included studies and quality appraisal
The major characteristics of 16 included studies are presented in Table 1.[24–39] Seven studies were carried out in the USA, four in the UK, and 1 each in Hong Kong, Canada, Austria, Sweden, and Finland. The sample size of the above studies ranged from 13 to 184. Females constituted the majority of participants in all studies but one. All participants were adults, with a mean age varying from 25.3 to 44.3 years old. Most studies were conducted in staff (n = 6), while 5 in students, 3 in mixed staff and students. And 2 studies did not mention the occupation of the included population. There were a variety of iMBIs designed in these studies. Mindfulness meditation was adapted in five studies when ACT was applied in four studies, MBSR in three studies and surviving and thriving during stress in one study.
Table 1.
Characteristics of studies included in the analysis.

The iMBIs also differ in duration, frequency, and delivery mode. The duration ranged from 2 weeks to 12 weeks. The delivery mode included website (n = 9), application (n = 4), virtual learning facility (n = 2) and online virtual classroom (n = 1). An online math training was conducted as a control group in one study, with the waitlist in 13 studies and mental health education in one study. Ten studies reported follow-up data, with follow-up time ranged from 3 weeks to 1 year. Outcome measures of stress in comparison were reported in 14 studies, with depression in 8 studies, anxiety in 7 studies and mindfulness in 10 studies. In addition, a total of the quality appraisal scores of each eligible article shown in Table 1 ranged from 3 to 7. Twelve of all included studies were of moderate qualities, two of low qualities and one of the high qualities.
3.2. Effects on stress and mindfulness
The overall effect size of 17 comparisons on stress was g = −0.393 (95% CI = −0.511, −0.275, Z = −6.533, P < .001), indicating that moderate effect of iMBIs in reducing stress among the general population (Fig. 2). The heterogeneity across the articles was low to moderate with Q = 24.23 (df = 16, P = .001) and I2 = 33.99%. As shown in Figure 3, the overall effect size of iMBIs on mindfulness (13 comparisons) was calculated at g = −0.316, (95% CI = −419, −0.212, Z = −5.985, P < .001). The assessment of the heterogeneity showed the low heterogeneity with studies (Q = 6.573, P < .001, I2 = 0%).
Figure 2.

Primary analysis of stress. CI = confidence interval.
Figure 3.
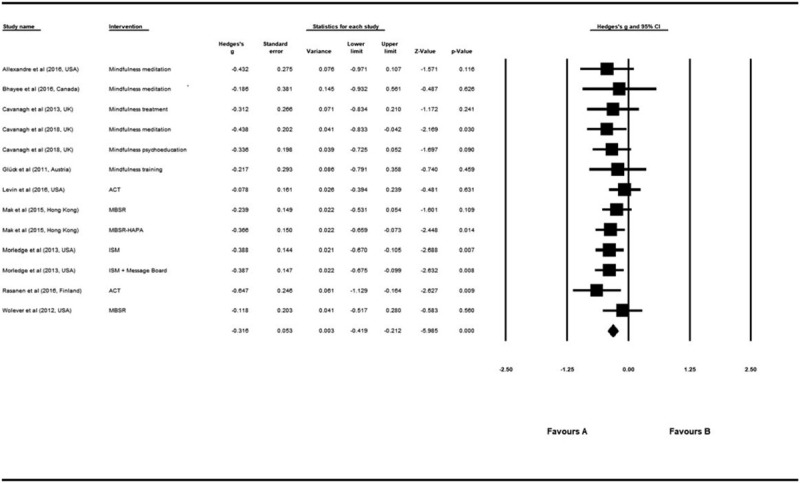
Primary analysis of mindfulness. CI = confidence interval.
3.3. Subgroup analyses
Exploratory subgroup analyses of the stress studies were conducted based on the delivery mode (i.e., application, website, or others) and the type of sample (i.e., students, staff, or both students and staff). As presented in Figure 4, the results showed that the effect size of 3 delivery mode groups remained in moderate range, and the effect size of the application group (g = −0.417, 95% CI = −0.800, −0.035, Z = −2.137, P = .033) and the others group (g = −0.459, 95% CI = −0.652, −0.265, Z = −4.639, P < .001) were both higher than the website group (g = −0.360, 95% CI = −0.527, −0.194, Z = −4.252, P < .001). The level of heterogeneity was in low range across the application group (Q = 1.277, P = .259, I2 = 21.66%) and the others group (Q = 4.236, P = .375, I2 = 5.579%), and in a moderate range across the website group (Q = 17.963, P = .036, I2 = 49.90%). In the subgroup analysis of different sample types, the effect size of the staff group (g = −0.541, 95% CI = −0.803, −0.279, Z = −4.043, P < .001) was much higher than other two groups (Fig. 5). But the higher heterogeneity was observed across the staff group (Q = 6.436, P = .169, I2 = 37.85%) than two other groups.
Figure 4.

Subgroup analysis of delivery mode on stress. CI = confidence interval.
Figure 5.

Subgroup analysis of sample type on stress. CI = confidence interval.
3.4. Meta-regression analyses
Using the meta-regression, the results indicated that the overall effect size was moderated by guidance for iMBIs on stress (slope: 0.11, Z = 2.70, P = .007) and mindfulness (slope: 0.10, Z = 0.96, P = .337). In addition, we found no evidence that publication date, MBIs type, and treatment duration had a positive significant influence on the overall effect size of iMBIs on stress and mindfulness.
3.5. Publication bias and sensitivity analyses
As shown in Figures 6 and 7, the Begg funnel plot was basically symmetric for stress and mindfulness. Similarly, the calculation of the Duval and Tweedie's trim and fill showed that there were no missing articles required to make the Begg funnel plot symmetric for both stress and mindfulness. Meantime, a fail-safe N test results showed that the estimated number of unpublished studies for stress (273) and mindfulness (103) were both higher than the recommended minimum of 95 and 75 (5 k + 10, where k is the number of studies in the meta-analysis), respectively.[16] Furthermore, the corresponding Hedges’ g was not significantly altered during the procedure of sensitivity analyses.
Figure 6.

Publication bias in stress studies.
Figure 7.

Publication bias in mindfulness studies.
3.6. Effects on depression, anxiety
Based on 9 comparisons, a small to moderate effect of iMBIs on the reduction of depression was found with g = −0.339 (95% CI = −0.491, −0.188, Z = −4.387, P < .001). The moderate heterogeneity was observed across the studies Q = 11.89 (df = 8, P = .156) and I2 = 32.75%. For anxiety, the combined effect size of 8 comparisons was g = −0.200 (95% CI = −0.324, −0.075, Z = −3.139, P = .002), suggesting a small effect on anxiety. The level of the heterogeneity was in small range with Q = 4.865 (df = 7, P = .676) and I2 = 0%.
4. Discussion
The main purpose of this meta-analysis is to estimate the overall effect size of iMBIs on the stress of the general population in comparison with control conditions. In the previous meta-analysis,[11] researchers also included studies involving the population with somatic illness or psychological illness, which were excluded in this meta-analysis. When all studies were included, the primary results showed significant, small to moderate effect sizes for stress (g = −0.393) and mindfulness (g = −0.375), providing further evidence for potential use on iMBIs as a low cost, alternative to face-to-face interventions for the general population.
The majority of healthy individuals who have difficulty in stress management won’t seek help from a psychological therapist until their problems have become severe. There are a lot of reasons for this phenomenon, such as geographic distances, concerns of confidentiality, disgrace and potential impact on career, cost and time constraints. Compared with face-to-face interventions, iMBIs could overcome such obstacles to reach those who are unwilling to receive face-to-face interventions[10] or do not have access to psychotherapy. Given the enormous stress at study and work, iMBIs can be a highly convenient way for the reduction of stress among the general population.
As mentioned above, subgroup analyses were performed to investigate differences between the effectiveness of iMBIs in reducing the stress of staff and students. The result suggested iMBIs were more effective in stress reduction of staff than students. This finding can be explained by the possibility that staff with higher levels of stress at baseline experienced a larger reduction in stress level. This is consistent with a previous study, which found that participants with higher levels of distress were likely to benefit from application-based mindfulness intervention more than those with a lower level of distress.[30] However, the findings also put forward the question of whether iMBIs should be remolded to suit specific individuals. A review has reported that mindfulness training with a focus on self-compassion is particularly effective in reducing stress and enhancing professional skills among health care workers who are vulnerable to stress overload and compassion fatigue due to an emotionally exhausting environment.[40] Further researches should be carried out to solve the problem.
Similarly, the subgroup analysis was conducted to inquire into differences among application, website and other deliveries. It showed that iMBI which had the largest effect size was other deliveries (main including the virtual classroom) and the next was application. It is noticeable, however, that only two included studies reported the effect of application-based MBIs on stress.[30,35] Due to the small size of the sample and high heterogeneity across the studies, the findings should be interpreted with caution.
Indeed, with the increasing population of mobile phone use, smartphone apps have the potential to offer a wide range of content that is both interactive and dynamic, which were also high capability-price ratio, flexible, and easily accessible. More than 90% of owners reported having their phones charged, turned on, and constantly within arm's reach.[41] These features make the application particularly suitable for the delivery of MBIs.[42] For example, in a study on iMBIs, many participants reported that they found it difficult to fit mindfulness into their busy lifestyles.[43] Application, however, offers the chance to associate the mindfulness with diaries, alarm clocks, and other functions to improve the adherence. It offers a possible explanation for the result of the subgroup analysis.
Otherwise, results must be explained with caution when taking the heterogeneity across the included studies into consideration. The differences among the studies having potential influences on heterogeneity were as follows:
-
(1)
sample type,
-
(2)
publish year,
-
(3)
type of iMBIs,
-
(4)
the duration of intervention,
-
(5)
with or without guidance, and
-
(6)
delivery mode.
Sensitivity analyses, subgroup analyses, and meta-regression were carried out in order to investigate the sources of heterogeneity. First, sensitivity analyses suggested that the effect size was not significantly altered when excluding each included study sequentially. Next, according to the subgroup analyses mentioned above, the type of sample and delivery mode contributed to the heterogeneity. Besides, meta-regression was conducted to determine the possible confounding factors. The results indicated that guidance had a great influence on heterogeneity, which notably higher effect sizes were observed for iMBIs with guidance than without guidance. The result is in accordance with the previous review.[11] It is a possible explanation that therapist guidance improves the adherence of participants. Low levels of adherence and high rates of drop-out (without completing the whole program) are common issues with iMBIs and were found in many included studies. However, it should be noted that the involvement of a therapist is costly and automated support could also achieve the same effect.[44]
Another interesting finding is that participants mainly consisted of females in 13 of 16 included studies. It has been proved that girls were more depressed than boys and girls used more emotion-focused and ruminative coping than did boys.[45] Given that the purpose of mindfulness is to reduce ruminative coping, it is reasonable to hypothesize that females benefit more than males. The assumption was proved in a previous study. Rojiani declared that women showed greater decreases in negative affect and greater increases on scales measuring mindfulness and self-compassion after mindfulness training and that the effectiveness of MBIs may be maximized by gender-specific modifications.[46] Therefore, further research should aim to explore how iMBIs are applied in male samples.
Despite the effect of mindfulness on stress reduction has been proved in the present meta-analysis, we still know little about the underlying mechanism. A recent study reported mindfulness could reduce stress via positive reappraisal, through which stressful events are transformed to beneficial, meaningful, and positive events (e.g., thinking that one can learn something from troubles).[47] Due to the insufficient data on emotion regulation, we hope that future studies could focus on this respect.
Last but not least, the small to moderate effect size of iMBIs on the reduction of depression (g = −0.339) and anxiety (g = −0.200) should be treated with caution, for a small number of relevant studies were included in the present meta-analysis. It may have something to do with the small effect size that we only included studies on healthy adults. Healthy adults are likely to have lower levels of depression and anxiety at baseline, leading to less room for enhancement compared to patients with somatic illness or psychological illness. Given the increasing incidence rates of depression and anxiety disorders in the general population,[48] the effect of iMBIs deserves expecting.
As the first meta-analysis examining the effects of iMBIs on stress reduction of the general population, it will be important for future researchers to report these possible influence factors (such as the gender and the delivery mode of iMBIs) so that the relationship between these factors and intervention effectiveness can be examined, and perhaps iMBIs are remolded to improve adherence and suit specific individuals.
Several limitations of this meta-analysis were worth noting. First, only published literature in English and Chinese were included in this study. If possible, future studies should search for articles in other languages and gray literature which meet the criterion. And there was a risk of publication bias in this meta-analysis and we failed to conduct more sophisticated assessments. Second, there was limited information provided by several studies and thus we were unable to perform a future investigation on other possible confounding factors that may influence the final effect size of iMBI on stress and mindfulness. Future researchers should pay more attention to possible influence factors (such as the gender of participants, and the age of participants) so that the correlation between those factors and the effectiveness of iMBI on stress and mindfulness among the general population can be evaluated. Moreover, due to insufficient information, we cannot have the capacity to examine how students and staff benefit differently from iMBIs or the effectiveness of different types of iMBIs. Third, confounders may not completely be controlled when conducting the meta-analysis. Thereby, there remained an unclear risk of bias across the included studies. Sensitivity analysis by excluding studies sequentially was performed for the precision of our research. In spite of the limitation aforementioned, we followed a strict protocol through the whole research to mitigate the potential bias and ensure the reliability and objectivity of the meta-analysis.
5. Conclusion
In summary, online mindfulness-based treatment was considered as an innovative and effective approach in terms of the reduction of several psychological symptoms. Our research results showed that there was a moderate effect of iMBI on stress among the general population and a small effect on mindfulness. However, there are still some questions remaining to be solved. In the future, more methodologically rigorous investigations into the potential confounding factors will provide more information to investigate how those factors influence the effect size. More importantly, researchers should pay more attention to explore how to remold iMBIs for the improvement of adherence and suitability for specific individuals.
Author contributions
Conceptualization: JX, YZ, YH; Data curation: JX, YZ; Formal analysis: JX, YZ, YH; Methodology: JX, YZ, YH; Project administration: JX, YZ; Resources: JX, YZ, YH; Software: JX, YZ; Supervision: YH; Writing-original draft: JX, YZ; Writing-review and editing: JX, YZ, YH.
Conceptualization: Yun Zhang, Ying Huang.
Data curation: Yun Zhang, Jiaming Xue.
Formal analysis: Yun Zhang, Jiaming Xue, Ying Huang.
Investigation: Yun Zhang, Jiaming Xue.
Methodology: Yun Zhang, Jiaming Xue, Ying Huang.
Project administration: Ying Huang.
Resources: Yun Zhang, Ying Huang.
Software: Jiaming Xue.
Supervision: Ying Huang.
Validation: Ying Huang.
Visualization: Yun Zhang, Jiaming Xue.
Writing – original draft: Yun Zhang, Jiaming Xue.
Writing – review & editing: Ying Huang.
Footnotes
Abbreviations: ACT = acceptance and commitment therapy, iMBIs = Internet mindfulness-based interventions, MBCT = mindfulness-based cognitive therapy, MBSR = mindfulness-based stress reduction.
How to cite this article: Zhang Y, Xue J, Huang Y. A meta-analysis: Internet mindfulness-based interventions for stress management in the general population. Medicine. 2020;99:28(e20493).
YZ and JX contributed equally to this article.
The authors have no conflicts of interest to disclose.
All data generated or analyzed during this study are included in this published article [and its supplementary information files].
References
- [1].Booth J, Connelly L, Lawrence M, et al. Evidence of perceived psychosocial stress as a risk factor for stroke in adults: a meta-analysis. BMC Neurol 2015;15:233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Li J, Zhang M, Loerbroks A, et al. Work stress and the risk of recurrent coronary heart disease events: a systematic review and meta-analysis. Int J Occup Med Environ Health 2015;28:8–19. [DOI] [PubMed] [Google Scholar]
- [3].Melchior M, Caspi A, Milne BJ, et al. Work stress precipitates depression and anxiety in young, working women and men. Psychol Med 2007;37:1119–29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Beiter R, Nash R, McCrady M, et al. The prevalence and correlates of depression, anxiety, and stress in a sample of college students. J Affect Disord 2015;173:90–6. [DOI] [PubMed] [Google Scholar]
- [5].Goh J, Pfeffer J, Zenios SAJMS. The relationship between workplace stressors and mortality and health costs in the United States. Manage Sci 2015;62:608–28. [Google Scholar]
- [6].Chiesa A, Serretti A. Mindfulness-based stress reduction for stress management in healthy people: a review and meta-analysis. J Altern Complement Med 2009;15:593–600. [DOI] [PubMed] [Google Scholar]
- [7].Kabat-Zinn J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: theoretical considerations and preliminary results. Gen Hosp Psychiatry 1982;4:33–47. [DOI] [PubMed] [Google Scholar]
- [8].Morgan D. Mindfulness-based cognitive therapy for depression: a new approach to preventing relapse. Psychother Res 2003;13:123–5. [DOI] [PubMed] [Google Scholar]
- [9].Hayes SC, Luoma JB, Bond FW, et al. Acceptance and commitment therapy: model, processes and outcomes. Behav Res Ther 2006;44:1–25. [DOI] [PubMed] [Google Scholar]
- [10].Wahbeh H, Svalina MN, Oken BS. Group, One-on-one, or internet? Preferences for mindfulness meditation delivery format and their predictors. Open Med J 2014;1:66–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Spijkerman MP, Pots WT, Bohlmeijer ET. Effectiveness of online mindfulness-based interventions in improving mental health: A review and meta-analysis of randomised controlled trials. Clin Psychol Rev 2016;45:102–14. [DOI] [PubMed] [Google Scholar]
- [12].Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg 2010;8:336–41. [DOI] [PubMed] [Google Scholar]
- [13].Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 1996;17:1–2. [DOI] [PubMed] [Google Scholar]
- [14].Sterne JA, Egger M, Moher D. Addressing reporting biases. Cochrane Handbook for Systematic Reviews of Interventions: Cochrane Book Series. 2008. 297–333. [Google Scholar]
- [15].Hedges LV, Olkin I. Statistical methods for meta-analysis. N Direct Progr Eval 1985;1984:25–42. [Google Scholar]
- [16].Rosenthal RJER. Meta-analytic procedures for social science research sage publications: Beverly hills, 1984, 148 pp. Educ Res 1986;15:18–20. [Google Scholar]
- [17].Borenstein M, Hedges L, Higgins J, et al. Comprehensive Meta-Analysis (Version 3) [Computer Software]. Englewood, NJ: Biostat. Inc; 2014. [Google Scholar]
- [18].Lipsey MW, Wilson DB. The efficacy of psychological, educational, and behavioral treatment. Confirmation from meta-analysis. Am Psychol 1993;48:1181–209. [DOI] [PubMed] [Google Scholar]
- [19].Higgins JP, Thompson SGJ. Quantifying heterogeneity in a meta-analysis. Stat Med 2002;21:1539–58. [DOI] [PubMed] [Google Scholar]
- [20].Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses. BMJ 2003;327:557–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Egger M, Smith GD, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315:629–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Rosenthal RJPb. The file drawer problem and tolerance for null results. Psychol Bull 1979;86:638–41. [Google Scholar]
- [23].Duval S, Tweedie R. Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000;56:455–63. [DOI] [PubMed] [Google Scholar]
- [24].Aikens KA, Astin J, Pelletier KR, et al. Mindfulness goes to work: impact of an online workplace intervention. J Occup Environ Med 2014;56:721–31. [DOI] [PubMed] [Google Scholar]
- [25].Allexandre D, Bernstein AM, Walker E, et al. A web-based mindfulness stress management program in a corporate call center: A randomized clinical trial to evaluate the added benefit of onsite group support. J Occup Environ Med 2016;58:254–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Bhayee S, Tomaszewski P, Lee DH, et al. Attentional and affective consequences of technology supported mindfulness training: a randomised, active control, efficacy trial. BMC Psychol 2016;4:60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Bostock S, Crosswell AD, Prather AA, et al. mindfulness on-the-go: Effects of a mindfulness meditation app on work stress and well-being. J Occup Environ Med 2019;24:127–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Cavanagh K, Strauss C, Cicconi F, et al. A randomised controlled trial of a brief online mindfulness-based intervention. Behav Res Ther 2013;51:573–8. [DOI] [PubMed] [Google Scholar]
- [29].Cavanagh K, Churchard A, O’Hanlon P, et al. A randomised controlled trial of a brief online mindfulness-based intervention in a non-clinical population: Replication and extension. Mindfulness 2018;9:1191–205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Champion L, Economides M, Chandler C. The efficacy of a brief app-based mindfulness intervention on psychosocial outcomes in healthy adults: A pilot randomised controlled trial. PLoS One 2018;13:e0209482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Eustis EH, Hayes-Skelton SA, Orsillo SM, et al. Surviving and thriving during stress: A randomized clinical trial comparing a brief web-based therapist-assisted acceptance-based behavioral intervention versus waitlist control for college students. Behav Ther 2018;49:889–903. [DOI] [PubMed] [Google Scholar]
- [32].Gluck TM, Maercker A. A randomized controlled pilot study of a brief web-based mindfulness training. BMC Psychiatry 2011;11:175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Levin ME, Pistorello J, Seeley JR, et al. Feasibility of a prototype web-based acceptance and commitment therapy prevention program for college students. J Am Coll Health 2014;62:20–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Levin ME, Hayes SC, Pistorello J, et al. Web-based self-help for preventing mental health problems in universities: comparing acceptance and commitment training to mental health education. J Clin Psychol 2016;72:207–25. [DOI] [PubMed] [Google Scholar]
- [35].Ly KH, Asplund K, Andersson GJII. Stress management for middle managers via an acceptance and commitment-based smartphone application: a randomized controlled trial. Internet Interv 2014;1:95–101. [Google Scholar]
- [36].Mak WW, Chan AT, Cheung EY, et al. Enhancing Web-based mindfulness training for mental health promotion with the health action process approach: randomized controlled trial. J Med Internet Res 2015;17:e8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].Morledge TJ, Allexandre D, Fox E, et al. Feasibility of an online mindfulness program for stress management--a randomized, controlled trial. Ann Behav Med 2013;46:137–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [38].Rasanen P, Lappalainen P, Muotka J, et al. An online guided ACT intervention for enhancing the psychological wellbeing of university students: a randomized controlled clinical trial. Behav Res Ther 2016;78:30–42. [DOI] [PubMed] [Google Scholar]
- [39].Wolever RQ, Bobinet KJ, McCabe K, et al. Effective and viable mind-body stress reduction in the workplace: a randomized controlled trial. J Occup Health Psychol 2012;17:246–58. [DOI] [PubMed] [Google Scholar]
- [40].Raab K. Mindfulness, self-compassion, and empathy among health care professionals: a review of the literature. J Health Care Chaplain 2014;20:95–108. [DOI] [PubMed] [Google Scholar]
- [41].Rainie L, Zickuhr K. Americans’ views on mobile etiquette. Pew Res Center 2015;26:948–58. [Google Scholar]
- [42].Steinhubl SR, Muse ED, Topol EJ. Can mobile health technologies transform health care? JAMA 2013;310:2395–6. [DOI] [PubMed] [Google Scholar]
- [43].Laurie J, Blandford A. Making time for mindfulness. Int J Med Inform 2016;96:38–50. [DOI] [PubMed] [Google Scholar]
- [44].Kelders SM, Bohlmeijer ET, Pots WT, et al. Comparing human and automated support for depression: fractional factorial randomized controlled trial. Behav Res Ther 2015;72:72–80. [DOI] [PubMed] [Google Scholar]
- [45].Li CE, DiGiuseppe R, Froh J. The roles of sex, gender, and coping in adolescent depression. Adolescence 2006;41:409–15. [PubMed] [Google Scholar]
- [46].Rojiani R, Santoyo JF, Rahrig H, et al. Women benefit more than men in response to college-based meditation training. Front Psychol 2017;8:551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [47].Garland EL, Gaylord SA, Fredrickson BL. Positive reappraisal mediates the stress-reductive effects of mindfulness: an upward spiral process. Mindfulness 2011;2:59–67. [Google Scholar]
- [48].World Health Organization. The global burden of disease: 2004 update. 2008. [Google Scholar]