

Abstract
The coronavirus disease 2019 pandemic has affected nearly 70% of children and teenagers around the world due to school closure policies. School closure is implemented widely in order to prevent viral transmission and its impact on the broader community, based on preliminary recommendations and evidence from influenza. However, there is debate with regard to the effectiveness of school closures. Growing evidence suggests that a child's SARS‐CoV‐2 infection is often mild or asymptomatic and that children may not be major SARS‐CoV‐2 transmitters; thus, it is questionable if school closures prevent transmission significantly. This question is important as a majority of children in low‐ and middle‐income countries depend on free school meals; unexpected long‐term school closure may adversely impact nutrition and educational outcomes. Food insecurity is expected to be higher during the pandemic. In this viewpoint, we argue for a more thorough exploration of potential adverse impacts of school closures in low‐ and middle‐income countries and recommend actions to ensure that the health and learning needs of vulnerable populations are met in this time of crisis.
As of 21 May 2020, in response to the novel coronavirus disease 2019 (COVID‐19) pandemic, 153 countries have implemented national school closures as part of social distancing policies to curb transmission, although many have recently reopened schools. The United Nations Educational, Scientific and Cultural Organization estimated that school closures have affected 1.2 billion learners including children and teenagers – approximately 68%of students around the world. 1 School closures are based on a preliminary recommendation derived from influenza and hand‐foot‐and‐mouth disease that suggest transmission disruption by limiting contact between students affords broader community protection. 2 , 3 However, the effectiveness of this measure is as yet uncertain. This raises three key questions: (i) Are children the major spreaders of SARS‐CoV‐2? (ii) How many children could get SARS‐CoV‐2? and (iii) What are the negative impacts of school closure policies on the young?
As in other low‐ and middle‐income countries (LMIC), on 18 March 2020, Thailand announced its closure of local and international schools, universities and children care facilities to impede the spread of SARS‐CoV‐2. This closure was in fact, just 1–2 weeks before schools would have been closed under normal circumstances; therefore, it only slightly impacted educational, life‐style or nutritional aspects of most children and learners. This has affected 15 million learners – mostly enrolled at pre‐primary, primary and secondary levels of education. 1
Based on past experience, children are perfect vectors for transmission of some respiratory viral infections such as influenza, measles and hand‐foot‐and‐mouth disease, 4 capable of spreading rapidly among young children in the crowded environments of daycare centres and nurseries. 3 , 5 A number of studies modelling influenza or hand‐foot‐and‐mouth disease demonstrate that ‘reactive school closures’ in response to a viral pathogen can reduce the rate of infection by a quarter and peak infection rates by half among susceptible individuals. 6 , 7 , 8 However, the benefits of school closure in the COVID‐19 outbreak are unproven; it is suggested that hygiene and environmental precautions such as hand washing, public education on hand sanitising, wearing masks, eating cooked food, and using clean serving spoons are more effective than school closure and play a fundamental role in reducing the number of cases and effectively controlling disease outbreaks. 9 , 10
In the case of COVID‐19 in Thailand and most countries, federal authorities have practiced ‘proactive school closures’, by closing schools prior to confirming infection transmission on school campuses. This strategy is not just about keeping the children safe, but rather, to keep the whole community safe. School closures result in a marked reduction of contacts associated with schooling. 11 , 12 Some studies confirm that transmission of influenza was reduced during school closures, especially among school‐age children. 8 , 13 Nevertheless, during the H1N1 influenza pandemic, many students in western countries continued to mix with others during school closures in spite of social distancing policies. 11 , 14 , 15 Without clear scientific guidance about the risks of triggering waves of COVID‐19 spread in schools, it is uncertain whether the policy of school closure is effective and necessary for the COVID‐19 pandemic for students and communities. 4 , 10 A thorough systematic review of 16 studies of previous coronavirus outbreaks, including the 2003 SARS virus in China, Hong Kong and Singapore suggests that school closures play insignificant roles in transmission control and others' school activities. For example, temperature screening did not contribute to effective case detection especially in asymptomatic individuals during incubation period. 4 , 9 , 10 As of May, only 5.8% out of a total of 3037 confirmed COVID‐19 cases in Thailand occurred in individuals fewer than 20 years of age. Recent studies show that a child's SARS‐CoV‐2 infection is often mild or asymptomatic 16 , 17 with low prevalence of infection, 2–6.7%. 18 , 19 , 20 In Iceland, researchers found that at‐risk populations or in contact with infected persons, no child under 10 years of age had a positive test, as compared with 0.8% of those 10 years of age or older. 18 A retrospective observational study in China, Singapore, Japan, Iran and South Korea of recorded SARS‐CoV‐2 household transmission clusters demonstrated that children were identified as the index case in only 3 (9.7%) out of 31 households. 10 Evidence supports that most children infected with SARS‐CoV‐2 have a known household contact whose symptoms precede that of the child, 10 , 19 indicating children are less likely to be the primary source of household SARS‐CoV‐2 infection. School outbreaks are rare to date. A school cluster of COVID‐19 reported in New Zealand, for instance showed that it was caused by infected school staff who transmitted to others. 20 To date, about 23% of schools world‐wide have reopened locally, regionally or nationally, according to United Nations Educational, Scientific and Cultural Organization 1 following a gradual decline in the rate of new infections with no reports about potential spread of COVID‐19 in school settings.
However, schools that are closed for a long period of time could inevitably have detrimental educational, social and health ramifications for children who live under vulnerable circumstances, such as children in marginal communities or in poverty who are faced with malnutrition and interruption of their education. Considering experiences from Thailand, we discuss two major threads and suggest opportunities during COVID‐19 school closures and how these may affect children at‐risk in LMIC settings such as Thailand (see Table 1 for key recommended actions).
Table 1.
Recommended approaches to addressing food and learning insecurity in school children at‐risk or in low‐ and middle‐income countries during the Covid‐19 Pandemic 21 , 22 , 23
| Measures | |
|---|---|
| Personal hygiene |
|
| Detection and isolation |
|
| Public decontamination |
|
| Health‐care resources |
|
| Children health |
|
| Social distancing |
|
| Stop non‐essential classes |
|
| Minimise school closure |
|
| Fruit and vegetable community gardening |
|
| Education |
|
UHT, ultra‐high temperature.
First, 300 000–500 000 Thai children, most of whom reside in rural areas, suffer from malnutrition, compared to 250 million malnourished school children world‐wide. According to the World Health Organization data from 2016, 10.5% of children under 5 years of age were stunted with 60% of these children living in households with insecure income, with an additional 28–30% of children aged 5–19 years classified as underweight. 24 , 25 In contrast, the prevalence of obesity increases. Rundle et al. postulate that COVID‐19 school closures may exacerbate the epidemic of childhood obesity in high‐income households because they are likely to purchase ultra‐processed, calorie‐dense foods. 26 , 27 However, in LMIC and in Thailand specifically, stunting and wasting as indicators of long‐term inadequate nutrition are especially prevalent in low‐income households. We argue that these populations are much more prone to malnutrition due to school closures. The national school breakfast and lunch programmes serve nearly 6.3 million children daily (60% of all students in Thailand) at pre‐primary and primary school levels, providing essential nutrition for growing children. Many children rely on these free meals for healthy nutrition. When schools close, nutrition is compromised. It is estimated that school feeding programmes provide up to 30–50% of a child's daily nutritional requirements through meals healthier than those prepared at home at the same price. The true cost for household food preparation is plausibly much higher when considering time spent purchasing, preparing foods, and higher retail food prices. From our experience, many children consume only two meals a day and one meal at school is considered high value for children's growth and development. In Thailand, schools have tentatively been scheduled to reopen on 1 July, which would result in an extra 43 days of school closure than expected. This would result in almost 270 million missed meals nationwide; for a child who misses school meals this may lead to a 1–2 kg weight loss over these 43 days – close to 5–10% of a child's total body weight. In addition, school closures can bring added financial pressures and risk of child undernutrition for poorer families given the now larger costs of childcare. 28
It is unclear how long school closures will last. If applied to the COVID‐19 situations in Hong Kong, Taiwan, and Singapore, ‘the hammer and the dance’ theory proposed by Tomas Pueyo 29 would suggest that social distancing orders such as work from home (WFH) and school closures risk disease flare ups if eased too quickly. However, each country has different measures depending upon how the COVID‐19 situation evolves after the reopening of schools. The World Health Organization recommends that the transition from lockdown be ‘evidence‐based’ and implemented gradually to prevent the risk of new outbreaks. 21 Therefore, even though children are less likely to spread SARS‐CoV‐2, redesigning classrooms on hygiene policies and new physical distancing rules more intensively will help schools open sooner and at a reduced risk of disease spreading and school re‐closure (Table 1). On 18 March, Thailand's decree for school closures also came with restrictions that resulted in closure of the restaurant and bar industries as well as other common sports and entertainment business sectors, restricted movement between provinces, and subsequently placed a curfew on its citizenry that began on 3 April. These aggressive restrictions have resulted in curbing the rate of daily new infection from 30% to an average 0–1.9% in the 4 weeks prior to 26 May. 30 Figure 1 proposes essential additions to the current health‐care surveillance and nutrition delivery systems during COVID‐19 to mitigate the burden of malnutrition in high‐risk children that can be managed at primary health‐care centres or schools. 22 Weight measurement is used to minimise direct or invasive contact when conducting child assessments in screening for malnutrition. Administering vaccines are also recommended, as preliminary data shows that once there is 14‐day home quarantine for suspected individuals, children in the same household tend not to get scheduled vaccinations due to a concern of social distancing and disease awareness at clinics. Vaccination is the only service that is to be performed under direct medical supervision in line with COVID‐19 emergency guidelines.
Fig 1.
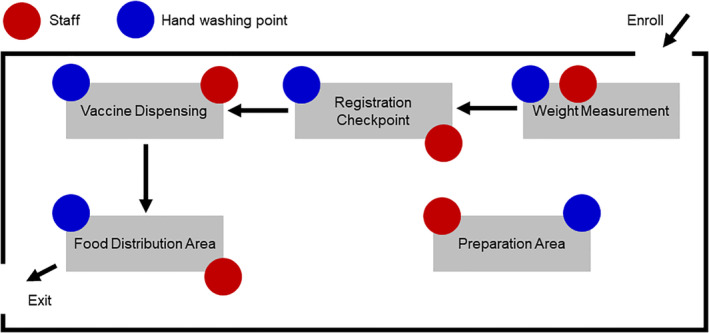
Health‐care service delivery flow (modified from a guideline from the World Food Programme). 22 The circuit demonstrates a one‐way path for flow of health‐care services within a facility and includes a weight station, registration point, essential vaccine delivery point and food distribution point provided by essential medical personnel, caretakers and volunteers.
Sufficient and good‐quality nutrition is critical for continued development, health, and survival of current and succeeding generations. Ultra‐high temperature milk is generally provided to children in most areas because of convenience, long shelf‐lives, and no need for refrigeration. It was previously determined that an additional three eggs per week at school is enough to stabilise normal serum protein levels. 31 However, our recent work demonstrates that up to 10 whole eggs a week can enhance children's weight and height by 30–60% as compared with students with a conventional school lunch programme in 1 year (K Mayurasakorn, unpubl. data, 2020). Therefore, we recommend that eggs and milk be provided as essential raw protein sources. According to a letter by Mr Anan Suwannarat (Permanent Secretary of the Minister of Agriculture and Cooperatives, Thailand) on 13 April 2020, the Milk and Food Board for Children and Youth of Thailand announced its distribution of ultra‐high temperature milk to students from 18 May to 30 June 2020, typically schools open under normal circumstances. On 30 April 2020, the childcare from Ministry of Interior, Thailand were tasked with providing food and nutrition service to and nutrition in their areas in preparing meals and delivering to household in accordance with COVID‐19 precautions (written communication, 30 April 2020). Food insecurity also has an impact upon all members of the household. It is associated with mental illness, poor physical health and reduced school participation in children. The United Nations Children's Fund's ‘guidance for COVID‐19 prevention and control in schools’ proposes that teachers canvass their students for any effects from COVID‐19, and coordinate with social service agencies and local organisations to identify and help children in distress. 23 Additionally, a symptomatic child should be in school unless school is suspected.
Second, unexpected school closures have forced schools to provide online learning lessons. Providing education during the COVID‐19 outbreak poses a challenge to all countries who wish to reduce inequality. Evidence indicates that time outside of school is a source of educational inequalities among families across a wide range of socio‐economic status. 28 Youth from financially insecure households experience a greater degree of impediments to learning than their wealthier counterparts during a school break. 32 The full extent of the COVID‐19 crisis in causing disruption for child care, education, and financial insecurity due to parental unemployment, is still unknown. However, should parents continue with their ongoing commitments and responsibilities, the school closures and child care restrictions may leave children unattended at home, thereby curtailing children's learning capacity during school closure. 33 One observational study shows that all students regardless of income status lost an equal amount of 1.8 months of progress in mathematical skills and 4 months of spelling skill, while students of low socio‐economic status experienced the largest learning deficit when it came to reading comprehensiveness. 32 In addition, children facing social hardships have been shown to suffer greater societal disconnection. This separation, starvation, and passive sedentary behaviour experienced during the COVID‐19 crisis may contribute to acute and subacute poorer health outcomes, including the mental health and wellbeing of the children. 28 Although the use of online learning is a key difference compared to regular, scheduled school closures, extended school closures may still lead to widening the learning, health, and nutrition gaps between youth from lower‐income and higher‐income households. Perhaps worse than educational impediment, an end to the pandemic is yet to be imagined, which will lead to grievous economic depression. This can exacerbate existing poverty and its association with children's nutrition and learning outcomes. In Thailand, the Ministry of Education is aware of the situation and hopes to use the distance learning television model developed during the reign of His Majesty King Bhumibol (King Rama IX), who established bridging the knowledge gap for underprivileged children and youth in rural areas. 34 Still, teachers should also consider how to modify their learning tools for students without digital access such as assigning students to review lessons and do homework, contacting students via telephone or home visit while adhering to physical distancing restrictions. 23
Based on the current data indicating that children are less likely to be main vectors of SAR‐CoV‐2, the benefits of school reopening and continuing education far outweigh the risks. This is an unprecedented time in our lives when we must ensure the health and education of the next generation to prevent deepening inequalities, which will affect the health and learning potential among vulnerable households. We must do this through the use of real‐time strategies that circumvent COVID‐19 at every step, and share lessons learned with the global community to improve our support of our children, which in turn, supports us all.
Acknowledgements
The authors would like to express their thanks to Dr Saipin Chotivichien and Ms Pornwipa Daoduong, Bureau of Nutrition, Department of Health, Ministry of Public Health, Thailand for their expert opinion and guidance.
Conflict of interest: None declared.
References
- 1. United Nations Educational, Scientific and Cultural Organization . COVID‐19 Educational Disruption and Response. 2020. Available from: https://en.unesco.org/covid19/educationresponse [accessed 26 May 2020].
- 2. Jackson C, Vynnycky E, Mangtani P. The relationship between school holidays and transmission of influenza in England and Wales. Am. J. Epidemiol. 2016; 184: 644–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Siriyaporn S, Wongnuch P, Laor P, Inta C, Apidechkul T. Effectiveness of hand foot mouth disease prevention and control measures between high and low epidemic areas, Northern Thailand. J. Health Res. 2018; 32: 217–28. [Google Scholar]
- 4. Isaacs D, Britton P, Howard‐Jones A et al. To what extent do children transmit SARS‐CoV‐2 virus? J. Paediatr. Child Health 2020. (forthcoming). 56(6): 978–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Centers for Disease Control and Prevention . Measles Cases and Outbreaks. Atlanta, GA: CDC; 2020. Available from: https://www.cdc.gov/measles/cases-outbreaks.html [accessed 26 May 2020].
- 6. Chadsuthi S, Wichapeng S. The modelling of hand, foot, and mouth disease in contaminated environments in Bangkok, Thailand. Comput. Math. Methods Med. 2018; 2018: 1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Ferguson NM, Cummings DAT, Fraser C, Cajka JC, Cooley PC, Burke DS. Strategies for mitigating an influenza pandemic. Nature 2006; 442: 448–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Cauchemez S, Valleron AJ, Boëlle PY, Flahault A, Ferguson NM. Estimating the impact of school closure on influenza transmission from sentinel data. Nature 2008; 452: 750–4. [DOI] [PubMed] [Google Scholar]
- 9. Viner RM, Russell SJ, Croker H et al. School closure and management practices during coronavirus outbreaks including COVID‐19: A rapid systematic review. Lancet Child Adolesc. Health 2020; 4: 397–404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Zhu Y, Bloxham CJ, Hulme KD et al. Children are unlikely to have been the primary source of household SARS‐CoV‐2 infections. medRxiv 2020. 10.1101/2020.03.26.20044826. [DOI] [Google Scholar]
- 11. Brooks SK, Smith LE, Webster RK et al. The impact of unplanned school closure on children's social contact: Rapid evidence review. Euro Surveill. 2020; 25: 1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Munasinghe L, Asai Y, Nishiura H. Quantifying heterogeneous contact patterns in Japan: A social contact survey. Theor. Biol. Med. Model 2019; 16: 6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Wheeler CC, Erhart LM, Jehn ML. Effect of school closure on the incidence of influenza among school‐age children in Arizona. Public Health Rep. 2010; 125: 851–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Eames KT, Tilston NL, Edmunds WJ. The impact of school holidays on the social mixing patterns of school children. Epidemics 2011; 3: 103–8. [DOI] [PubMed] [Google Scholar]
- 15. Hens N, Ayele GM, Goeyvaerts N et al. Estimating the impact of school closure on social mixing behaviour and the transmission of close contact infections in eight European countries. BMC Infect. Dis. 2009; 9: 187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Dong Y, Mo X, Hu Y et al. Epidemiology of COVID‐19 among children in China. Pediatrics 2020; 145: 1–10. [DOI] [PubMed] [Google Scholar]
- 17. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID‐19) outbreak in China: Summary of a report of 72 314 cases from the Chinese center for disease control and prevention. JAMA 2020; 323: 1239–42. [DOI] [PubMed] [Google Scholar]
- 18. Gudbjartsson DF, Helgason A, Jonsson H et al. Spread of SARS‐CoV‐2 in the Icelandic population. N. Engl. J. Med. 2020; 382: 2302–15. 10.1056/NEJMoa2006100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Zimmermann P, Curtis N. Coronavirus infections in children including COVID‐19: An overview of the epidemiology, clinical features, diagnosis, treatment and prevention options in children. Pediatr. Infect. Dis. J. 2020; 39: 355–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. NZ Ministry of Health . COVID‐19 – Significant clusters: NZ Ministry of Health. Wellington: The New Zealand Ministry of Health; 2020. Available from: https://www.health.govt.nz/our‐work/diseases‐and‐conditions/covid‐19‐novel‐coronavirus/covid‐19‐current‐situation/covid‐19‐current‐cases/covid‐19‐significant‐clusters [accessed 26 May 2020].
- 21. World Health Organization . COVID‐19 Strategy Update 2020. Geneva: World Health Organization; 2020. Available from: https://www.who.int/publications‐detail/covid‐19‐strategy‐update‐‐‐14‐april‐2020 [accessed 26 May 2020].
- 22. World Food Programme . WFP's Additional Recommendations for the Management of Maternal and Child Malnutrition Prevention and Treatment in the Context of COVID 19. Rome: World Food Programme; 2020. Available from: https://www.unscn.org/uploads/web/file/COVID‐19‐Nutrition‐Program‐Adaptations‐Interim‐Brief‐1.pdf [accessed 26 May 2020].
- 23. United Nations Children's Fund, World Health Organization, International Federation of Red Cross and Red Crescent Societies . The Guidance for COVID‐19 Prevention and Control in Schools: Key Messages and Actions. New York, NY: UNICEF; 2020: 1–13. Available from: https://www.unicef.org/thailand/media/4061/file/Key%20Messages%20and%20Actions%20for%20COVID-19%20Prevention%20and%20Control%20in%20Schools.pdf [accessed 26 May 2020].
- 24.United Nations Children's Fund (UNICEF), World Health Organization, International Bank for Reconstruction and Development/The World Bank. Levels and trends in child malnutrition: Key Findings of the 2020 Edition of the Joint Child Malnutrition Estimates. Geneva: World Health Organization; 2020. Available from: https://www.who.int/publications-detail/jme-2020-edition [accessed 26 May 2020].
- 25. NCD Risk Factor Collaboration . Worldwide trends in body‐mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population‐based measurement studies in 128.9 million children, adolescents, and adults. Lancet 2017; 390: 2627–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Rundle AG, Park Y, Herbstman JB, Kinsey EW, Wang YC. COVID‐19–related school closings and risk of weight gain among children. Obesity 2020; 28: 1008–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. von Hippel PT, Workman J. From kindergarten through second grade, U.S. children's obesity prevalence grows only during summer vacations. Obesity (Silver Spring) 2016; 24: 2296–300. [DOI] [PubMed] [Google Scholar]
- 28. Morgan K, Melendez‐Torres GJ, Bond A et al. Socio‐economic inequalities in adolescent summer holiday experiences, and mental wellbeing on return to school: Analysis of the school health research network/health behaviour in school‐aged children survey in Wales. Int. J. Environ. Res. Public Health 2019; 16: 1107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Pueyo T. Coronavirus: The Hammer and the Dance. San Francisco, CA: A Medium Corporation; 2020. Available from: https://medium.com/@tomaspueyo/coronavirus‐the‐hammer‐and‐the‐dance‐be9337092b56 [accessed 26 May 2020]. [Google Scholar]
- 30. Department of Disease Control . Covid‐19 Infected Situation Reports: Ministry of Public Health, Thailand. Nonthaburi: Ministry of Public Health (Thailand); 2020. Available from: https://covid19.th-stat.com/en [accessed 26 May 2020].
- 31. Mayurasakorn K, Sitphahul P, Hongto PO. Supplement of three eggs a week improves protein malnutrition in Thai children from rural areas. J. Med. Assoc. Thai. 2010; 93: 301–9. [PubMed] [Google Scholar]
- 32. Stewart H, Watson N, Campbell M. The cost of school holidays for children from low income families. Childhood 2018; 25: 516–29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Bygren M, Duvander A‐Z. Parents' workplace situation and fathers' parental leave use. J. Marriage Fam. 2006; 68: 363–72. [Google Scholar]
- 34.United Nations Educational, Scientific and Cultural Organization Bangkok: Asia and Pacific Regional Bureau for Education. Education Minister Nataphol Teepsuwan on COVID‐19 Strategy in Thailand. Bangkok: UNESCO; 2020. Available from: https://bangkok.unesco.org/content/education‐minister‐nataphol‐teepsuwan‐covid‐19‐strategy‐thailand [accessed 26 May 2020].