

Abstract
This study examined the associations between personality traits and psychological and behavioural responses to the coronavirus disease 2019 (COVID‐19) pandemic. Personality was assessed in January/February 2020 when the public was not aware of the spread of coronavirus in the USA. Participants were reassessed in late March 2020 with four sets of questions about the pandemic: concerns, precautions, preparatory behaviours, and duration estimates. The sample consisted of N = 2066 participants (mean age = 51.42; range = 18–98; 48.5% women). Regression models were used to analyse the data with age, gender, education, race, and ethnicity as covariates. Consistent with the preregistered hypotheses, higher neuroticism was related to more concerns and longer duration estimates related to COVID‐19, higher extraversion was related to shorter duration estimates, and higher conscientiousness was associated with more precautions. In contrast to the preregistered hypotheses, higher neuroticism was associated with fewer precautions and unrelated to preparatory behaviours. Age moderated several trait–response associations, suggesting that some of the responses were associated more strongly in older adults, a group at risk for complications of COVID‐19. For example, older adults high in conscientiousness prepared more. The present findings provide insights into how personality predicts concerns and behaviours related to the COVID‐19 pandemic. © 2020 European Association of Personality Psychology
Keywords: COVID‐19, personality traits, behavioural responses, neuroticism, conscientiousness
Introduction
In early 2020, the world has faced a pandemic of respiratory disease spreading from person to person caused by a novel coronavirus. This novel coronavirus is called severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) and is responsible for coronavirus disease 2019 (COVID‐19), which poses a serious public health risk. The outbreak was first revealed in late December 2019 in the city of Wuhan, China (Nishiura et al., 2020). Since then, the virus has spread rapidly around the world. The World Health Organization declared the COVID‐19 outbreak a global pandemic on 11 March 2020 (Cucinotta & Vanelli, 2020).
Individual differences in general patterns of thoughts, feelings, and behaviours (i.e. personality) may contribute to how people respond and behave during a pandemic. The present study examined whether individual differences in personality traits (assessed before there was public knowledge of the spread of SARS‐CoV‐2 in the USA) predict pandemic‐related psychological and behavioural responses in late March 2020 when Americans were asked by the White House to follow the ‘15 days to slow the spread’ coronavirus guidelines (The White House, 2020). Personality traits may shape such responses through beliefs and attitudes (McCrae & Costa, 2006) associated with the traits. Such processes may have implications for health services (Emilsson, Gustafsson, Öhnström, & Marteinsdottir, 2020). For instance, taking precautions is a crucial behaviour to slow the spread of the virus, but there are individual differences in how strictly people follow such recommendations. People also differ in their level of concern, preparedness, and expectations for emergencies. Given the relevance of personality for health‐related behaviours and beliefs, these traits may contribute to responses to a pandemic, which in turn points to the relevance of personality for public health officials. The present study thus tested whether personality traits are associated with concerns, precautions, preparatory behaviours, and duration estimates of the pandemic. Knowing how personality plays out in the COVID‐19 pandemic can help to predict behaviour during future infectious disease outbreaks and provide guidance for public health services to develop personality‐tailored advice.
Of the personality traits defined by the five‐factor model (FFM; McCrae & John, 1992), conscientiousness and neuroticism emerge as the most relevant predictors of health behaviours (Aschwanden et al., 2019; Emilsson et al., 2020; Ferguson, Muñoz, Winegard, & Winegard, 2012; Mõttus, Realo, Allik, Esko, & Metspalu, 2012; Sutin et al., 2016; Terracciano & Costa, 2004; Wilson & Dishman, 2015). Individuals higher in conscientiousness, for example, tend to exercise more (Sutin et al., 2016; Wilson & Dishman, 2015), smoke less (Hakulinen et al., 2015; Terracciano & Costa, 2004), adhere better to medication (Molloy, O'Carroll, & Ferguson, 2014), and are more likely to obtain preventive cancer screenings (Aschwanden et al., 2019). Neuroticism, in contrast, has been associated with both health‐risk and health‐promoting behaviours. On the one hand, individuals higher in neuroticism tend to be physically inactive (Sutin et al., 2016; Wilson & Dishman, 2015), smoke more (Hakulinen et al., 2015; Terracciano & Costa, 2004), drink more alcohol (Malouff, Thorsteinsson, Rooke, & Schutte, 2007), use drugs (Terracciano, Löckenhoff, Crum, Bienvenu, & Costa, 2008), eat less fruits and vegetables (Gale et al., 2017), and are more likely to engage in sexual risk‐taking behaviour (Hoyle, Fejfar, & Miller, 2000; Mõttus et al., 2012). On the other hand, higher neuroticism has been linked to greater use of health care services (Cuijpers et al., 2010), higher odds of some preventive screenings (Aschwanden et al., 2019), and—in combination with high conscientiousness—to less smoking after the onset of a disease (Weston & Jackson, 2015). This inconsistency may be explained by mediators and/or moderators of the association between neuroticism and health behaviours: People high in neuroticism may engage in certain health‐risk behaviours (e.g. drinking alcohol) to seek emotional relief (Mõttus et al., 2012), but they may also adopt health‐promoting behaviours (e.g. using health care service) because of an anxiety‐provoked vigilance (Friedman, 2000; Weiss & Deary, 2019), such that individuals with higher neuroticism can be described as the ‘worried well’ (Slavin et al., 2010). In the context of a pandemic that induces fear, we expect the latter to be of relevance.
Few studies have examined the association between the FFM personality traits and health behaviours during a pandemic, although the number of studies focused on COVID‐19 is increasing. For example, a prepublished German experience sampling study (N = 1609) showed that individuals high in neuroticism experienced more negative affect in their daily lives during the pandemic (Kroencke, Geukes, Utesch, Kuper, & Back, 2020). Of note, the effects of neuroticism on negative affect were stronger than those of sociodemographic variables and personally experienced health threats. In a prepublished US study (N = 2231), openness and conscientiousness moderated the relationship between pandemic severity (i.e. respondents' location: city and state) and negative affect, such that pandemic severity did not influence the well‐being of those who were open to new experiences and conscientious (Zhang et al., 2020). In another prepublished US study (N = 1182), lower neuroticism and higher openness were reported as beneficial for showing reasonable behaviours (e.g. social distancing, enhanced sanitation) and the avoidance of unreasonable behaviours (e.g. hoarding, spreading misinformation) (Stadler et al., 2020). In a Brazilian sample (N = 715), individuals low in extraversion and high in conscientiousness were more likely to think it is necessary to avoid approaching people as much as possible until the coronavirus situation is controlled (i.e. social distancing), and individuals high in conscientiousness were also more likely to think that handwashing/using hand sanitizer is necessary (Carvalho, Pianowski, & Gonçalves, 2020). A prepublished US report (N = 502) showed that lower extraversion as well as higher neuroticism, agreeableness, and conscientiousness were associated with more social distancing and hygiene behaviours (Blagov, 2020). Higher openness has also been correlated with more hygiene behaviours in Blagov's study, while in another prepublished US study (N = 501), lower neuroticism and higher extraversion, agreeableness, openness, and conscientiousness were related to greater adherence to formal COVID‐19 guidelines (Bogg & Milad, 2020). A prepublished study from Qatar (N = 405) demonstrated that both higher neuroticism and conscientiousness were associated with more social distancing (Abdelrahman, 2020). A further prepublished US study (N = 1019) revealed that higher extraversion was associated with more social distancing and cleaning/disinfecting, higher conscientiousness was related to more handwashing, and both higher conscientiousness and openness were associated with less use of face masks (Shook, Sevi, Lee, Fitzgerald, & Oosterhoff, 2020). Although these studies provide some evidence for significant cross‐sectional associations, their results might be skewed by the impact of the pandemic on personality (Sutin et al., 2020). The present work addresses this limitation by predicting a broad range of pandemic‐related responses from personality traits that were assessed before the outbreak in a US sample that is about four times larger than those in most previous studies (N = 2066).
The present study
We investigated whether the FFM personality traits are associated with four sets of psychological and behavioural responses to the COVID‐19 pandemic: (a) concerns related to the pandemic (e.g. contracting the coronavirus), (b) precautions taken to avoid catching the coronavirus (e.g. washing hands), (c) preparatory behaviours related to the pandemic (e.g. stocking up on food), and (d) duration estimates of the consequences of the pandemic (e.g. time until society goes back to normal).
We preregistered seven hypotheses (https://osf.io/kbej9): (1) higher neuroticism would be associated with more concerns, (2) higher neuroticism and (3) higher conscientiousness would be associated with more precautions to avoid catching the coronavirus, (4) higher neuroticism and (5) higher conscientiousness would be associated with more pandemic‐related preparatory behaviours, and that (6) higher neuroticism would predict more pessimistic duration estimates of pandemic‐related issues, whereas (7) higher extraversion would predict more optimistic duration estimates. Directional hypotheses were not made for the remaining traits.
Methods
A description of the measures applied in this project as well as the data and analytical codes necessary to reproduce reported results can be retrieved from https://osf.io/tkbf5/. The preregistration of the hypotheses and statistical analyses can be retrieved from https://osf.io/kbej9. Material and procedures were reviewed and approved by the Institutional Review Board of Florida State University.
Sample
Participants were recruited through Dynata (https://www.dynata.com/) to complete an online study on the psychological correlates of well‐being and health. Dynata samples through their proprietary participant panels and compensates participants for completing research and/or market surveys. Participants had to be 18 years or older and living in the USA. The sampling was stratified to be 50% men/women, by age groups, and 20% African American. Dynata contacted participants and directed them to a Qualtrics survey, which 4662 participants consented and initiated between 31 January 2020 and 10 February 2020 (baseline pretest assessment). Between 18 and 29 March 2020, we conducted another survey that included items on psychological and behavioural responses related to the COVID‐19 pandemic (post‐test assessment). Of the baseline sample, n = 2565 consented and completed the post‐test (55.02% response rate). Thereof, n = 499 were excluded due to evidence of careless responding (e.g. demographics did not match across assessments), straightlining (i.e. giving the same answers across questionnaires), missing data on personality (>20% of personality items)/all outcome variables, or because they tested positive for SARS‐CoV‐2 as this study focused on non‐infected individuals. The final sample consisted of 2066 participants (mean age = 51.42 years; age range = 18–98; 48.5% women; 68.0% White; 11.1% Hispanic) for the present analyses. Descriptive statistics for included participants are provided in Table 1.
Table 1.
Descriptive statistics for included participants by age category
| All participants | Younger adults | Middle‐aged adults | Older adults | |
| N | 2066 | 549 | 983 | 534 |
| Age range | 18–98 | 18–39 | 40–64 | 65–98 |
| Age mean | 51.42 (16.55) | 29.68 (6.83) | 52.58 (7.12) | 71.63 (4.67) |
| Female | 48.50% | 59.74% | 50.05% | 34.08% |
| Race: White | 68.01% | 46.63% | 70.91% | 84.64% |
| Race: African American | 15.00% | 24.77% | 13.02% | 8.61% |
| Race: Other | 16.99% | 28.60% | 16.07% | 6.74% |
| Ethnicity: Hispanic | 11.08% | 20.58% | 9.36% | 4.49% |
| Education | 3.18 (1.50) | 2.84 (1.55) | 3.21 (1.48) | 3.48 (1.41) |
| Income | 2.99 (1.74) | 2.53 (1.74) | 3.09 (1.77) | 3.28 (1.59) |
| Personality Traits | ||||
| Neuroticism | 2.60 (0.80) | 2.95 (0.71) | 2.59 (0.81) | 2.26 (0.69) |
| Extraversion | 3.12 (0.65) | 3.03 (0.61) | 3.14 (0.68) | 3.20 (0.61) |
| Openness | 3.47 (0.63) | 3.39 (0.60) | 3.47 (0.65) | 3.53 (0.63) |
| Agreeableness | 3.72 (0.64) | 3.46 (0.60) | 3.73 (0.62) | 3.95 (0.60) |
| Conscientiousness | 3.88 (0.70) | 3.52 (0.71) | 3.97 (0.68) | 4.10 (0.59) |
| Outcomes | ||||
| Concern | 2.88 (0.89) | 3.12 (0.96) | 2.88 (0.89) | 2.64 (0.72) |
| Precaution (PC) | 4.15 (1.38) | 4.17 (1.53) | 4.20 (1.34) | 4.03 (1.28) |
| PC: Difficulty | 2.03 (0.70) | 2.01 (0.72) | 2.02 (0.70) | 2.07 (0.69) |
| PC: Effectiveness | 3.82 (1.10) | 3.71 (1.16) | 3.87 (1.06) | 3.84 (1.10) |
| PC: Normativity | 3.29 (0.72) | 3.46 (0.85) | 3.25 (0.71) | 3.19 (0.53) |
| Preparation | 1.99 (1.51) | 2.49 (1.58) | 1.89 (1.49) | 1.66 (1.34) |
| Duration estimates | 6.81 (2.55) | 6.45 (2.60) | 6.84 (2.56) | 7.12 (2.41) |
Note. Values represent a count, range, per cent, or mean (standard deviation). Education was assessed on a scale from 0 (less than high school) to 6 (PhD or equivalent). Income was measured on a scale from 0 (less than $20 000) to 5 ($100 000 or more).
Measures
Personality at pretest
The 60‐item Big Five Inventory‐2 was used to measure personality traits (Soto & John, 2017). It measures the five broad traits and three more circumscribed facets within each trait. Participants rated items that finished the sentence stem ‘I am someone who …’ on a scale from 1 (strongly disagree) to 5 (strongly agree). Twelve items were used to measure each trait: neuroticism (e.g. is moody, has up and down mood swings), extraversion (e.g. is outgoing, sociable), openness (e.g. is curious about many different things), agreeableness (e.g. is compassionate, has a soft heart), and conscientiousness (e.g. is dependable, steady). Items were reverse scored when necessary and the mean taken across items for each trait, with higher scores indicating higher levels of the trait. In addition to the five traits, three facets for each trait were scored: anxiety, depression, and emotional volatility for neuroticism; sociability, assertiveness, and energy level for extraversion; intellectual curiosity, aesthetic sensitivity, and creative imagination for openness; compassion, respectfulness, and trust for agreeableness; and organization, productiveness, and responsibility for conscientiousness. Reliabilities ranged from α = .60 (intellectual curiosity) to α = .89 (neuroticism) and from Ω = .44 (assertiveness) to Ω = .72 (depression) (see Table S2 for all reliability estimates).
Psychological and behavioural responses at post‐test
Four psychological and behavioural outcomes related to the COVID‐19 pandemic were used as outcomes: concerns, precautions, preparatory behaviours, and duration estimates. To assess concerns, 13 items were used. Participants were asked how concerned they were about ‘contracting the coronavirus’; ‘becoming severely ill or dying from the disease caused by the coronavirus’; ‘someone in your family will become severely ill or die from the disease caused by the coronavirus’; ‘losing your job or changes in your employment because of the spread of the coronavirus’; ‘losses in your assets, business or retirement investment plans because of the spread of the coronavirus’; ‘the effects of the coronavirus on your relationship with your partner’; ‘the effects of the coronavirus on your relationships with your friends or family members’; ‘the effects of the coronavirus on your plans for travel, vacations, or attendance at large events’; ‘the effects of the coronavirus on your education or the education of someone close to you (e.g. your children)’; ‘the disruption in daily activities caused by the coronavirus will make you lonely’; ‘people in your community losing their jobs because of the coronavirus’; ‘people in your community not having money for food because of the coronavirus’; and ‘the effects of the coronavirus on the United States economy’. The items were rated on a 5‐point Likert‐type scale ranging from 1 (not at all concerned) to 5 (extremely concerned). The mean was taken across items, with higher scores reflecting more concerns. The reliability estimates were α = .88 and Ω = .64.
To measure precautions, participants were asked which of the following precautions they took to avoid catching the coronavirus: ‘wash hands often’; ‘use hand sanitizer’; ‘avoid touching your eyes, nose, and mouth’; ‘put distance between yourself and other people (social distancing)’; ‘wear a face mask’; ‘clean and disinfect surfaces’; ‘cough and sneeze into your elbow’; and ‘stay at home if you are sick’. For the present analysis, we only included the first six items as they primarily represent a precaution against contracting the virus (versus primarily avoid spreading the potential virus to others). The items were adapted from the recommendations on sickness prevention released by the Centers for Disease Control and Prevention (https://www.cdc.gov/coronavirus/2019-ncov/prepare/prevention.html) and previous work on preventive behaviours to avoid catching influenza (Srivastav et al., 2018). Note that the Centers for Disease Control and Prevention recommended wearing cloth face coverings in public settings on 3 April 2020 (https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/cloth-face-cover.html), after our data collection. Items were scored as 1 (yes) or 0 (no) and summed. A higher score indicates more precautions taken. The reliability estimates were α = .62 and Ω = .60. In addition, we asked participants (a) how difficult it is for them to engage in each precaution (difficulty), (b) how effective they think each precaution is (effectiveness), and (c) how many other people engage in each precaution (normativity). These items were answered on a 5‐point Likert‐type scale ranging from 1 (extremely easy) to 5 (extremely difficult) for difficulty; 1 (extremely ineffective) to 5 (extremely effective) for effectiveness; and 1 (no one) to 5 (everyone) for normativity. The mean was taken across items, with higher scores reflecting higher perceived difficulty, effectiveness, and normativity. The reliability estimates were α = .75/Ω = .55 for difficulty, α = .93/Ω = .83 for effectiveness, and α = .89/Ω = .77 for normativity.
For preparatory behaviours, participants indicated whether they engaged in five behaviours during the past month: ‘I bought face masks’; ‘I stocked up on hand sanitizer’; ‘I stocked up on toilet paper’; ‘I stocked up on food and/or drinks’; and ‘I changed my travel plans because of the coronavirus’. Items were scored as 1 (yes) or 0 (no) and summed up. A higher score indicates more preparatory behaviours. The reliability estimates were α = .65 and Ω = .54.
To measure duration estimates, participants provided five estimates related to consequences of the pandemic. Participants were asked how long they think it will last until ‘the outbreak is controlled’; ‘the social quarantine ends’; ‘society goes back to normal’; ‘the participant recovers from financial losses’; and ‘the United States recovers from financial losses’. The items were rated on a 13‐point Likert‐type scale ranging from 0 (less than a month) to 12 (more than 12 months). The mean was taken across items, with higher scores reflecting longer duration estimates. Longer duration estimates were interpreted as more pessimistic responses. The reliability estimates were α = .81 and Ω = .59.
Covariates
Covariates included in all analyses were self‐reported age in years, gender (0 = male, 1 = female), education (on a scale from 0 = less than high school to 6 = PhD or equivalent), race (two dummy‐coded variables were 1 = White and 1 = African American compared with 0 = other), and ethnicity (1 = Hispanic, 0 = not Hispanic). In a secondary model, self‐reported income (on a scale from 0 = less than $20 000 to 5 = $100 000 or more) was added as an additional covariate. We used data from pretest for all covariates except for income, for which information was available at post‐test only.
Statistical analyses
The present analyses were preregistered at https://osf.io/kbej9. Multiple regression analyses were used to predict the psychological and behavioural responses from personality traits. The sum of precautions and preparatory behaviours and the average of concern and duration estimates were used as outcomes. The preregistered Model 1 included age, gender, education, race, and ethnicity as covariates. Income was added as an additional covariate in Model 2 in supplementary analyses (preregistered). For each personality trait and outcome, a separate model was conducted (preregistered). In a follow‐up model (preregistered), all five traits were added simultaneously. In additional analyses (not preregistered), we aimed to gain a more fine‐grained picture of precautions by examining whether personality traits predicted the perceived difficulty, effectiveness, and normativity of these behaviours. All continuous variables were z scored and interpreted in standard deviation (SD) units.
In a series of exploratory analyses (preregistered), we tested whether age moderated the association between personality and behavioural responses because older adults are at higher risk for severe complications of COVID‐19 (Centers for Disease Control and Prevention, 2020a). We also considered the possible interaction between personality traits (e.g. interaction between neuroticism and conscientiousness) because it has been hypothesized that a combination of high neuroticism and high conscientiousness could be associated with better health outcomes, although results are mixed (Turiano et al., 2018; Turiano, Mroczek, Moynihan, & Chapman, 2013; Weston & Jackson, 2015). To create the interaction terms, the standardized values were multiplied by each other. Significant interactions were probed using simple slopes at theoretically meaningful values (Aiken & West, 2011).
In supplementary analyses (preregistered), we analysed the set of outcomes based on their individual items as there might be differences in the predictive power of personality traits and the various behavioural responses. For concerns, a factor analysis was run to identify potential clusters. The clusters were then used for further analysis. Binary logistic regression analyses were used to analyse the association between personality traits and the individual outcomes with yes/no responses.
Finally, we examined whether the facets of personality traits were associated with the aggregated main outcomes (not preregistered), because facets can have more predictive power than the overarching trait (Paunonen, Haddock, Forsterling, & Keinonen, 2003) or facets from the same trait can have associations that go in opposite directions (Sutin et al., 2011). All analyses were conducted in r (R Core Team, 2020) and rstudio (RStudio Team, 2020). Significance was set to p values < .05.
Results
The main findings are shown in Table 2. Table 3 displays the interactions between age and personality traits, with significant interactions being decomposed and described in the table notes. Table S1 contains the zero‐order correlations between outcomes and both personality traits (Part A) and sociodemographic variables (Part B). The supporting information further includes the descriptive statistics and intercorrelations for personality (Table S2) and outcomes (Table S3) as well as the results for Model 2 (Table S4) and the model with all five personality traits (Table S5). The results for personality predicting difficulty, effectiveness, and normativity of precautions are displayed in Table S6. The interactions between personality traits are shown in Table S7, whereof only the interaction between neuroticism and conscientiousness is discussed because this motivated our exploratory analyses. The information on the factor analysis is presented in supporting information S8; Table S8a displays the item–factor loadings. The results for the facets are illustrated in Figure 1 and summarized in supporting information S9. The data, the analytical codes, and the supplemental results can be retrieved from https://osf.io/tkbf5/.
Table 2.
Associations of personality traits with psychological and behavioural responses to coronavirus disease 2019
| Outcomes | Trait predictors | ||||
| Neuroticism | Extraversion | Openness | Agreeableness | Conscientiousness | |
| Concerns | .14 [0.09, 0.18], <.001 | .05 [0.01, 0.10], .014 | .03 [−0.01, 0.08], .123 | −.04 [−0.09, 0.00], .061 | −.07 [−0.11, −0.02], .004 |
| Health | .17 [0.12, 0.22], <.001 | −.04 [−0.08, 0.01], .099 | .02 [−0.03, 0.06], .446 | −.03 [−0.08, 0.02], .193 | −.10 [−0.14, −0.05], <.001 |
| Contracting | .14 [0.09, 0.18], <.001 | −.02 [−0.06, 0.03], .497 | .00 [−0.04, 0.05], .929 | −.04 [−0.08, 0.01], .141 | −.08 [−0.13, −0.03], <.001 |
| Illness (self) | .18 [0.13, 0.23], <.001 | −.03 [−0.08, 0.01], .159 | .01 [−0.04, 0.05], .693 | −.05 [−0.09, −0.00], .043 | −.11 [−0.16, −0.06], <.001 |
| Illness (family) | .14 [0.10, 0.19], <.001 | −.05 [−0.10, −0.01], .018 | .04 [−0.01, 0.08], .118 | −.00 [−0.05, 0.04], .945 | −.07 [−0.11, −0.02], .004 |
| Personal finances | .05 [0.01, 0.10], .022 | .10 [0.05, 0.14], <.001 | .01 [−0.04, 0.05], .749 | −.08 [−0.13, −0.04], <.001 | −.04 [−0.08, 0.01], .107 |
| Job | .06 [0.01, 0.10], .012 | .06 [0.02, 0.10], .004 | .00 [−0.04, 0.04], .852 | −.05 [−0.09, −0.01], .026 | −.06 [−0.10, −0.02], .005 |
| Assets | .06 [0.01, 0.10], .018 | .05 [0.00, 0.09], .033 | −.01 [−0.06, 0.03], .610 | −.07 [−0.12, −0.03], .002 | .01 [−0.04, 0.05], .746 |
| Travel | −.03 [−0.07, 0.02], .290 | .11 [0.07, 0.15], <.001 | .03 [−0.02, 0.07], .254 | −.05 [−0.10, −0.01], .020 | .02 [−0.03, 0.06], .492 |
| Education | .07 [0.02, 0.11], .003 | .07 [0.02, 0.11], .002 | .00 [−0.04, 0.04], .929 | −.06 [−0.11, −0.02], .007 | −.07 [−0.12, −0.03], .001 |
| Relationships | .18 [0.13, 0.22], <.001 | .05 [0.01, 0.09], .016 | −.05 [−0.09, −0.00], .033 | −.12 [−0.16, −0.08], <.001 | −.14 [−0.19, −0.10], <.001 |
| Partner | .14 [0.09, 0.18], <.001 | .05 [0.01, 0.09], .027 | −.07 [−0.11, −0.02], .002 | −.13 [−0.18, −0.09], <.001 | −.14 [−0.18, −0.09], <.001 |
| Friends/family | .17 [0.12, 0.21], <.001 | .01 [−0.03, 0.05], .683 | −.05 [−0.09, −0.00], .035 | −.11 [−0.15, −0.06], <.001 | −.16 [−0.21, −0.12], <.001 |
| Loneliness | .15 [0.10, 0.20], <.001 | .07 [0.03, 0.11], .002 | −.01 [−0.05, 0.04], .781 | −.07 [−0.12, −0.02], .003 | −.06 [−0.11, −0.02], .006 |
| Community | .04 [−0.01, 0.09], .091 | .05 [0.00, 0.09], .030 | .15 [0.10, 0.19], <.001 | .12 [0.07, 0.17], <.001 | .07 [0.02, 0.11], .004 |
| Job (other) | .04 [−0.01, 0.09], .105 | .04 [0.00, 0.09], .049 | .11 [0.07, 0.16], <.001 | .09 [0.04, 0.14], <.001 | .02 [−0.02, 0.07], .362 |
| Money (other) | .05 [0.00, 0.10], .045 | .03 [−0.01, 0.08], .168 | .15 [0.11, 0.19], <.001 | .13 [0.09, 0.18], <.001 | .02 [−0.02, 0.07], .307 |
| US economy | .02 [−0.03, 0.06], .501 | .05 [0.01, 0.09], .022 | .11 [0.07, 0.16], <.001 | .09 [0.04, 0.13], <.001 | .14 [0.10, 0.19], <.001 |
| Precautions | −.07 [−0.12, −0.03], .002 | .13 [0.08, 0.17], <.001 | .11 [0.07, 0.16], <.001 | .13 [0.09, 0.18], <.001 | .15 [0.10, 0.19], <.001 |
| Wash hands | −.17 [−0.42, 0.07], .159 | .37 [0.14, 0.60], .001 | .24 [0.01, 0.47], .043 | .31 [0.08, 0.55], .009 | .56 [0.33, 0.81], <.001 |
| Hand sanitizer | −.13 [−0.24, −0.03], .013 | .28 [0.18, 0.38], <.001 | .07 [−0.03, 0.17], .164 | .14 [0.04, 0.25], .008 | .11 [0.01, 0.22], .031 |
| Avoid touching | −.13 [−0.24, −0.03], .015 | .18 [0.08,0 .28], <.001 | .19 [0.09, 0.29], <.001 | .21 [0.11, 0.32], <.001 | .27 [0.17, 0.38], <.001 |
| Physical distance | −.12 [−0.25, 0.02], .085 | −.00 [−0.13, 0.12], .959 | .34 [0.21, 0.47], <.001 | .30 [0.17, 0.44], <.001 | .36 [0.22, 0.49], <.001 |
| Face mask | .01 [−0.12, 0.14], .889 | .15 [0.03, 0.27], .012 | .06 [−0.06, 0.18], .355 | −.06 [−0.19, 0.07], .362 | −.10 [−0.23, 0.02], .107 |
| Clean | −.17 [−0.28, −0.06], .003 | .29 [0.18, 0.39], <.001 | .27 [0.17, 0.37], <.001 | .38 [0.27, 0.49], <.001 | .39 [0.28, 0.50], <.001 |
| Preparations | −.04 [−0.08, 0.01], .129 | .14 [0.10, 0.18], <.001 | .03 [−0.01, 0.07], .192 | .00 [−0.04, 0.05], .885 | −.01 [−0.06, 0.03], .574 |
| Face masks | .00 [−0.12, 0.13], .968 | .19 [0.07, 0.31], .002 | −.01 [−0.13, 0.11], .858 | −.09 [−0.21, 0.04], .177 | −.20 [−0.32, −0.08], .001 |
| Hand sanitizer | −.03 [−0.14, 0.07], .519 | .22 [0.12, 0.32], <.001 | .02 [−0.08, 0.11], .747 | −.03 [−0.13, 0.07], .577 | −.11 [−0.21, −0.01], .035 |
| Toilet paper | .06 [−0.04, 0.16], .212 | .16 [0.07, 0.26], <.001 | .00 [−0.09, 0.10], .994 | −.01 [−0.11, 0.09], .875 | −.02 [−0.11, 0.08], .765 |
| Food | −.05 [−0.15, 0.04], .283 | .14 [0.04, 0.23], .004 | .13 [0.03, 0.22], .008 | .08 [−0.01, 0.18], .086 | .09 [−0.01, 0.19], .069 |
| Cancel travel | −.21 [−0.30, −0.11], <.001 | .32 [0.22, 0.41], <.001 | .05 [−0.04, 0.14], .269 | .02 [−0.08, 0.11], .725 | .07 [−0.02, 0.17], .131 |
| Duration estimates | .06 [0.02, 0.11], .009 | −.05 [−0.09, −0.00], .030 | .04 [−0.00, 0.08], .077 | .01 [−0.04, 0.06], .642 | −.06 [−0.10, −0.01], .015 |
| Outbreak | .06 [0.02, 0.11], .009 | −.06 [−0.10, −0.01], .011 | .03 [−0.01, 0.08], .128 | −.01 [−0.05, 0.04], .801 | −.10 [−0.15, −0.06], <.001 |
| Quarantine | .05 [0.01, 0.10], .025 | −.02 [−0.06, 0.02], .351 | .01 [−0.04, 0.05], .781 | −.02 [−0.07, 0.03], .398 | −.14 [−0.19, −0.09], <.001 |
| Society | .05 [0.00, 0.10], .045 | −.06 [−0.10, −0.01], .010 | .08 [0.04, 0.13], <.001 | .02 [−0.03, 0.06], .527 | −.03 [−0.08, 0.01], .146 |
| Economics (Self) | .04 [−0.00, 0.09], .059 | −.01 [−0.05, 0.04], .761 | −.01 [−0.05, 0.04], .787 | .01 [−0.04, 0.05], .755 | −.00 [−0.05, 0.04], .858 |
| US economy | .03 [−0.02, 0.08], .207 | −.05 [−0.09, −0.01], .028 | .03 [−0.01, 0.08], .130 | .04 [−0.00, 0.09], .072 | .04 [−0.00, 0.09], .065 |
Note. Values represent standardized regression coefficients [95% confidence interval], p value. Models control for demographic covariates. Bolded values are statistically significant α = .05. Results are shown for the aggregated main outcomes (concerns, precautions, preparations, and duration estimates), the four subscales of concerns (health, personal finances, relationships, and community), and the individual items of each outcome.
Table 3.
Exploratory model: Moderation by age
| Age by trait interaction | Psychological and behavioural outcomes | |||
| Concerns | Precautions | Preparations | Duration estimates | |
| Age × neuroticism | .03 [−0.02, 0.07], .280 | −.01 [−0.05, 0.04], .825 | −.02 [−0.07, 0.02], .322 | −.02 [−0.07, 0.02], .340 |
| Age × extraversion | −.04 [−0.08, 0.01], .123 | −.01 [−0.05, 0.03], .648 | −.02 [−0.07, 0.02], .314 | −.02 [−0.06, 0.03], .466 |
| Age × openness | .05 [0.01, 0.10], .017 | .00 [−0.04, 0.04], .986 | .06 [0.02, 0.11], .006 | .08 [0.04, 0.13], <.001 |
| Age × agreeableness | .03 [−0.01, 0.07], .163 | −.00 [−0.05, 0.04], .827 | .07 [0.03, 0.12], .001 | .08 [0.04, 0.13], <.001 |
| Age × conscientiousness | .02 [−0.02, 0.06], .373 | .00 [−0.04, 0.04], .998 | .07 [0.03, 0.11], .002 | .07 [0.02, 0.11], .004 |
Note. Values represent standardized regression coefficients [95% confidence interval], p value. Models control for demographic covariates. Bolded values are statistically significant α = .05. Seven significant interactions were found: first, higher openness was associated significantly with greater concerns among older adults (β = .10 [0.03, 0.16], p = .005), but not middle‐aged adults (β = .04 [−0.01, 0.08], p = .108) or younger adults (β = −.04 [−0.11, 0.03], p = .300). Second, higher openness was associated significantly with more preparations among older adults (β = .10 [0.03, 0.17], p = .003), but not middle‐aged adults (β = .03 [−0.01, 0.07], p = .168) or younger adults (β = −.06 [−0.13, 0.02], p = .139). Third, higher agreeableness was significantly associated with more preparations among older adults (β = .09 [0.02, 0.16], p = .010), but less preparations among younger adults (β = −.09 [−0.17, −0.02], p = .014), while the association was not significant for middle‐aged adults (β = .01 [−0.04, 0.05], p = .702). Fourth, higher conscientiousness was significantly associated with more preparations among older adults (β = .08 [0.01, 0.16], p = .033), but less preparations among younger adults (β = −.09 [−0.16, −0.03], p = .007), while the association was not significant for middle‐aged adults (β = .002 [−0.04, 0.05], p = .940). Fifth, higher openness was associated significantly with longer duration estimates among older adults (β = .14 [0.07, 0.21], p < .001), but not middle‐aged adults (β = .04 [−0.002, 0.09], p = .062) or younger adults (β = −.07 [−0.15, 0.00], p = .056). Sixth, higher agreeableness was associated significantly with longer duration estimates among older adults (β = .11 [0.04, 0.18], p = .020), but shorter duration estimates among younger adults (β = −.10 [−0.17, −0.02], p = .010), whereas the association was not significant for middle‐aged adults (β = .02 [−0.03, 0.06], p = .474). Lastly, higher conscientiousness was associated significantly with shorter duration estimates among younger adults (β = −.14 [−0.21, −0.07], p < .001) and middle‐aged adults (β = −.04 [−0.09, 0.00], p = .070), whereas the association was not significant for older adults (β = .03 [−0.04, 0.11], p = .394).
Figure 1.
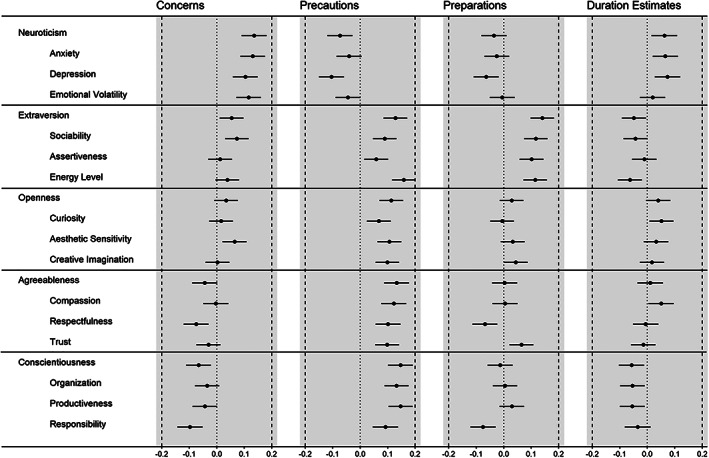
Associations of personality traits and facets with the four outcomes. Standardized regression coefficients (controlled for demographic covariates) are shown. The findings are summarized in supporting information S9.
Concerns
Zero‐order correlations indicated that individuals who scored higher in neuroticism and extraversion, lower in agreeableness and conscientiousness, those with higher education and income, as well as women, African Americans, Hispanics, and people who identified their race as ‘other’ reported greater concerns (Table S1). Older and White respondents reported fewer concerns.
When controlling for sociodemographic covariates, the associations for personality traits remained similar, except for agreeableness that became non‐significant (Table 2): higher neuroticism (Hypothesis 1), higher extraversion, and lower conscientiousness (neither hypothesized) at pretest were associated significantly with greater concerns related to the pandemic at post‐test. When controlling for income, these associations were unchanged, except that extraversion became non‐significant (Table S4). The pattern of associations was the same as in Model 1 when all five personality traits were entered simultaneously (Table S5). These associations did not vary by age, except for openness (Table 3). The interaction between neuroticism and conscientiousness was not significant (Table S7). At the facet level, anxiety was the strongest facet‐level correlate for neuroticism, sociability was the strongest facet‐level correlate for extraversion, and responsibility was the strongest facet‐level correlate for conscientiousness. In general, the association for all facets went in the direction of the domain, but not all were statistically significant (supporting information S9).
When looking at the subscales of concerns (Table 2), higher neuroticism and lower conscientiousness were associated with more health‐related concerns. Higher neuroticism and extraversion as well as lower agreeableness were linked to more concerns about personal finances. All personality traits were associated with concerns about relationships, although not in the same direction. Specifically, higher neuroticism and extraversion were associated with greater concerns over relationships, whereas the other three traits had a negative association. All traits except neuroticism were associated with greater concerns about the economic impact of the virus in their community and the USA.
Precautions
Individuals who scored higher in extraversion, openness, agreeableness, and conscientiousness, as well as women, African Americans, Hispanics, and people who identified their race as ‘other’ reported taking more precautions (Table S1). Older and White respondents reported taking fewer precautions.
In the primary analyses, the associations between personality traits and precautions were unchanged, except for neuroticism that emerged as a significant predictor (Table 2): lower neuroticism (opposite of hypothesized direction; Hypothesis 2) and higher conscientiousness (Hypothesis 3), extraversion, openness, and agreeableness (not hypothesized) were associated significantly with taking more precautions to avoid contracting COVID‐19. These associations were unchanged controlling for income (Table S4). When all five personality traits were entered simultaneously, these associations were unchanged, except that neuroticism became non‐significant (Table S5). These associations did not vary significantly by age (Table 3). Moreover, the findings for perceptions of difficulty, effectiveness, and normativity mirrored the pattern of associations for actually engaging in precautions: People who engaged in fewer precautions also perceived more difficulties to do so, and they believed that these precautions would be rather ineffective and taken by fewer other people (Table S6). There was a significant negative interaction between neuroticism and conscientiousness for precautions (β = −.05 [−0.09, −0.01], p = .011) (Table S7). The association between higher conscientiousness and more precautions was significantly stronger among participants lower in neuroticism (−1 SD; β = .21 [0.14, 0.28], p < .001), compared with those higher in neuroticism (+1 SD; β = .10 [0.04, 0.16], p < .001), but the associations remained significant in both cases. The non‐significant association between neuroticism and precautions was significantly different for participants lower in conscientiousness (−1 SD; β = .05 [−0.02, 0.12], p = .144), compared with those higher in conscientiousness (+1 SD; β = −.05 [−0.11, 0.01], p = .082), but the associations remained non‐significant in both cases. The following facets emerged as the strongest facet‐level correlate for their traits: depression (neuroticism), energy level (extraversion), aesthetic sensitivity (openness), compassion (agreeableness), and productiveness (conscientiousness). In general, the association for all facets went in the direction of the domain, but not all were statistically significant (supporting information S9).
Of note, the item‐level analyses revealed that neuroticism was associated significantly with 50% of the precautions: Lower neuroticism was associated with using hand sanitizer, avoiding touching the face, and cleaning/disinfecting surfaces. Higher conscientiousness was associated with higher engagement in all precautions except for wearing a face mask. The strength of associations is illustrated in Figure 2. The other traits were related positively to at least four of six precautions (see Table 2 for details).
Figure 2.
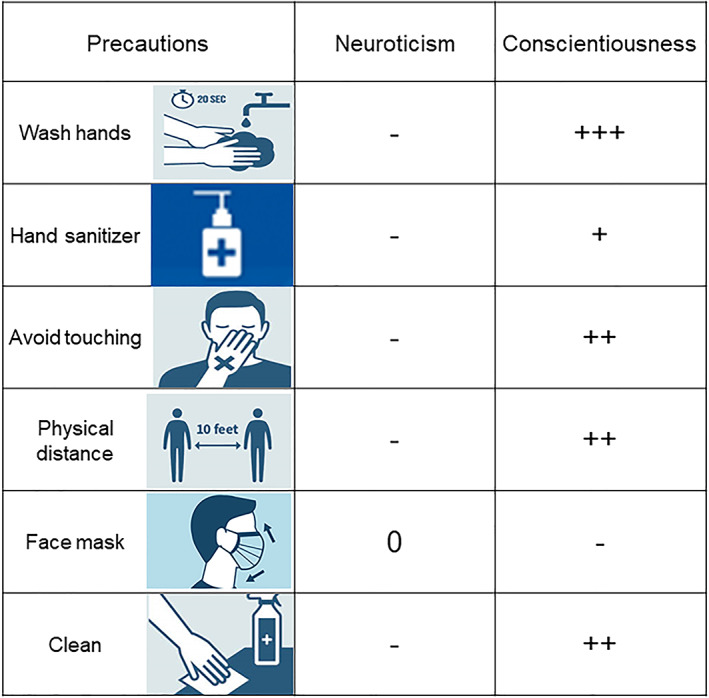
This figure illustrates the direction and strength of association of the two hypothesized traits (i.e. neuroticism and conscientiousness) with each precaution. A zero (0) refers to a standardized regression coefficient (β) around zero. The minus (−) refers to a small negative effect (β < −.10). The plus (+) refers to a positive association, whereas the strength of association is illustrated as + = small (β < .10); ++ = moderate (β < .30); and +++ = large (β > .50). Images were retrieved from online resources (Atlanta ISD, 2020; Centers for Disease Control and Prevention, 2020c; Shenandoah University, 2020). [Colour figure can be viewed at wileyonlinelibrary.com]
Preparatory behaviours
Individuals who scored higher in extraversion and lower in agreeableness and conscientiousness, as well as women, African Americans, Hispanics, and people who identified their race as ‘other’ reported more preparations (Table S1). Older and White respondents reported fewer preparations.
The associations between agreeableness and conscientiousness and preparatory behaviours were not apparent when controlling for the sociodemographic covariates (Table 2). Only higher extraversion (not hypothesized) was associated with engaging in more preparations. The other traits, including neuroticism (Hypothesis 4) and conscientiousness (Hypothesis 5), were unrelated to preparatory behaviours. These associations were unchanged controlling for income (Table S4). When all five personality traits were entered simultaneously, these associations were unchanged, except for conscientiousness: When controlling for the other personality traits, higher conscientiousness was significantly associated with fewer preparations (Table S5). These associations varied significantly by age for openness, agreeableness, and conscientiousness, but not for neuroticism or extraversion (Table 3). The interaction between neuroticism and conscientiousness was not significant (Table S7). At the facet level, sociability was the strongest facet‐level correlate for extraversion. Of note, two facets of agreeableness went in opposite directions, which may have obscured the association at the trait level: lower respectfulness and higher trust were associated significantly with more preparations. Specific facets of neuroticism (depression), openness (creative imagination), and conscientiousness (responsibility) were statistically significant while there was no significant association at the trait level (supporting information S9).
The item‐level analyses (Table 2) indicated that higher neuroticism was associated with fewer changes of travel plans, whereas higher conscientiousness was associated with less stockpiling of face masks and hand sanitizer. Higher extraversion was associated positively with all five preparatory behaviours, whereas agreeableness was unrelated to all of them. Higher openness was related to more stockpiling of food.
Duration estimates
Individuals who scored higher in openness and agreeableness, those who were older and with higher income as well as education, reported longer duration estimates, whereas Hispanics and people who identified their race as ‘other’ reported shorter duration estimates (Table S1).
A reverse pattern was found when controlling for sociodemographic covariates (Table 2): whereas openness and agreeableness became non‐significant, higher neuroticism (Hypothesis 6) and both lower extraversion (Hypothesis 7) and conscientiousness (not hypothesized) were associated significantly with longer duration estimates. These associations were unchanged controlling for income (Table S4). When all five personality traits were entered simultaneously (Table S5), conscientiousness remained significant, openness became significant, but neuroticism and extraversion became non‐significant. The associations varied by age for openness, agreeableness, and conscientiousness but not for neuroticism or extraversion (Table 3). The interaction between neuroticism and conscientiousness was not significant (Table S7). At the facet level, both anxiety and depression were the strongest facet‐level correlates for neuroticism, energy level was the strongest facet‐level correlate for extraversion, and both organization and productiveness were the strongest facet‐level correlates for conscientiousness. In general, the association for most facets went in the direction of the domain, but not all were statistically significant (supporting information S9).
The item‐level analyses (Table 2) showed that higher neuroticism was related to more pessimistic (i.e. longer) duration estimates regarding the outbreak, quarantine, and until society goes back to normal. Higher extraversion was linked to more optimistic (i.e. shorter) duration estimates concerning the outbreak and until society goes back to normal and the US economy recovers. Higher conscientiousness was associated with more optimistic duration estimates of the outbreak and quarantine. Higher openness was linked to more pessimistic duration estimates until society goes back to normal. Agreeableness was unrelated to all items.
Discussion
This study examined whether personality traits and facets are associated with psychological and behavioural responses to the COVID‐19 pandemic. Four of the seven preregistered hypotheses were supported: higher neuroticism was associated with more concerns, higher conscientiousness was associated with more precautions, and higher neuroticism and extraversion were related to more pessimistic and optimistic duration estimates, respectively. In contrast to our hypotheses, higher neuroticism was associated with fewer precautions and was unrelated to preparatory behaviours. In exploratory analyses, there was evidence that the association between the traits and some of the responses was associated more strongly for older adults, a group at high risk for complications of COVID‐19.
Neuroticism
Neuroticism reflects the tendency to experience irritability, anger, sadness, anxiety, worry, and hostility (Costa & McCrae, 1992). It is thus unsurprising that individuals high in this trait reported more concerns and were pessimistic about the duration estimates related to the COVID‐19 pandemic. Previous research showed that people higher in neuroticism experience more chronic negative affect, have especially intense reactions to negative events, and rely more on emotion‐focused than problem‐focused coping strategies (Bolger & Schilling, 1991; Carver & Connor‐Smith, 2010; Gross, Sutton, & Ketelaar, 1998; Luhmann & Eid, 2009). Moreover, a recent COVID‐19 study has also reported that people high in neuroticism experienced more negative affect in their daily lives during the pandemic (Kroencke et al., 2020).
In contrast to our expectation, higher neuroticism was related to fewer precautions. Additional analyses revealed that this effect was mainly driven by the facet of depression. In other COVID‐19 studies, higher neuroticism has been linked to more physical distancing and hygiene behaviours (Abdelrahman, 2020; Blagov, 2020) but also to less guideline adherence that included similar items as our precautions (e.g. washing hands or avoid touching the face) (Bogg & Milad, 2020). Across current and previous COVID‐19 findings, the weighted average association (determined by the r‐to‐z approach) is r = −.15, representing a small negative effect. Instead of the expected anxiety‐provoked vigilance (Friedman, 2000; Weiss & Deary, 2019), people high in neuroticism reported fewer precautions, which is consistent with high neuroticism leading to undesirable coping behaviours (Cooper, Agocha, & Sheldon, 2000). Notably, this association was not moderated by age or conscientiousness, although there was some trend indicating that high neuroticism and low conscientiousness is an unfavourable combination when it comes to the adoption of health behaviours, as reported in previous research (Terracciano & Costa, 2004). There was no support, however, for a beneficial combination of high neuroticism and high conscientiousness in this study.
We did not find evidence for an association between neuroticism and preparatory behaviours. At the facet level, however, higher depression was associated significantly with fewer preparations (Figure 1). This again supports the idea of undesirable coping behaviours (Cooper et al., 2000) and further demonstrates the value of facet‐level analyses to gain a deeper understanding of which component of the broad traits is most relevant for specific outcomes (Paunonen et al., 2003).
Conscientiousness
In line with our hypothesis, individuals high in conscientiousness took more precautions to avoid catching the coronavirus. This finding is consistent with the general literature on health behaviours (Bogg & Roberts, 2004; Molloy et al., 2014; Nolan, McCrory, & Moore, 2019) and recent COVID‐19 studies (Abdelrahman, 2020; Blagov, 2020; Bogg & Milad, 2020; Carvalho et al., 2020; Shook et al., 2020). The weighted average association is r = .19, indicating a small‐to‐moderate effect. As being organized, dutiful, and responsible are key attributes of conscientiousness, individuals with high scores on this trait may be more likely to follow recommendations on precautions. The one exception among precautions was wearing a face mask, which was not associated with conscientiousness. Another study reported that higher conscientiousness was even negatively associated with wearing a face mask (Shook et al., 2020). It should be noted that at the time of Shook et al.'s and our survey, wearing a face mask in public settings was not recommended by the CDC, which means that conscientious individuals adhered to rules by not endorsing this precaution.
On the other hand, conscientiousness was not associated significantly with preparatory behaviours. At the facet level, however, higher responsibility was related to fewer preparations. These individuals may stockpile less because they feel interpersonally responsible and care about their community (i.e. they do not want to take resources from others). This association is consistent with our finding that individuals high in conscientiousness reported more concerns about the community (Table 2).
Extraversion
As expected, higher extraversion was related to more optimistic (i.e. shorter) pandemic‐related duration estimates, and this effect was mainly driven by the facet of energy level. Individuals high in extraversion tend to experience positive affect, have greater global self‐efficacy, and make more positive evaluations of their lives (Soto, 2015) and health (Sutin & Terracciano, 2016). This positive view may be mirrored in duration estimates, such that these individuals are more hopeful and optimistic that the pandemic and the recovery from its consequences will be sooner rather than later. It should be noted that higher extraversion was linked to greater concerns too, which contradicts the aforementioned line of argumentation. However, concerns over the pandemic should not be equated to pessimism; to some extent, they might be a rational response. Further research is required to clarify potential underlying mechanisms of different responses. Moreover, higher extraversion was associated with more preparatory behaviours, and age did not moderate this association. Future investigations could test other possible mediators or moderators such as a need to feel prepared, hedonic consumption, or emotion regulation consumption. Hedonic consumption and emotion regulation consumption involve emotional aspects of consumers' interactions with products (Alba & Williams, 2013; Kemp & Kopp, 2011), for example, purchasing a product for the purposes of pleasure or of alleviating, repairing, and managing an emotion. Previous work found a positive association between extraversion and this kind of consumption (Matzler, Würtele, & Renzl, 2006). The stockpiling of face masks, hand sanitizer, toilet paper, and food could be a strategy of emotion regulation: individuals high in extraversion may have bought more of these items to make them feel ‘safe and prepared’ in times of a new and dangerous threat. These individuals also reported more precautions, with the interesting exception of physical (social) distancing. As being sociable and active individuals, they might particularly struggle to follow the recommendation on social distancing (Carvalho et al., 2020).
Is personality more predictive of coronavirus disease 2019 responses in older adults?
About 25.9% of our sample was aged 65 years or older and potentially at higher risk for complications of COVID‐19. Due to this vulnerability, one might expect that they would report greater concerns and engage in more precautions and preparations, but our zero‐order correlations showed the opposite pattern: Older age was related to fewer concerns, precautions, and preparations. However, our exploratory analyses revealed seven significant age interactions that suggest that personality is more predictive of certain responses among older adults. Among the 65–96 year olds, higher openness was associated with greater concerns, and both higher openness and agreeableness were related to more preparations and longer duration estimates. Higher conscientiousness was also associated significantly with more preparatory behaviours among older adults while it was non‐significant for middle‐aged adults high in conscientiousness, and younger adults high in conscientiousness even engaged in fewer preparations. Older adults high in conscientiousness may have stockpiled because they may feel more threatened by COVID‐19 because they are a high‐risk group and thus may be trying to reduce their store visits. On the other hand, younger adults high in conscientiousness may not have stockpiled because they may feel less threatened or for rational reasons such as there were inconsistencies in official guidelines and expert opinion on face masks at the time of data collection (Centers for Disease Control and Prevention, 2020b; Chan & Yuen, 2020; World Health Organization, 2020). Higher conscientiousness was further associated with shorter duration estimates among younger and middle‐aged adults, but not older adults. This pattern has implications for public health messaging. If all older adults took COVID‐19 seriously, individual differences in personality should not matter (i.e. there would be no variability to predict). Yet, our findings indicate that they do matter and could be considered in the development of personality‐tailored communication to older adults (i.e. at‐risk groups).
Theoretical and practical implications
The present study makes several noteworthy contributions that may have implications for both theory and public health. First, in general, the zero‐order correlation coefficients between the COVID‐19 responses and personality traits ranged from r = .00 to r = .18 and were comparable with those of sociodemographic variables (r = .00 to r = −.21; Table S1); in some cases, they were even stronger. For example, washing hands was associated more strongly with conscientiousness (r = .12) than age (r = .04) or female gender (r = .07). Besides the comparable effect sizes, personality was more predictive of certain responses in one high‐risk group, older adults. This underlines the importance of personality and indicates that personality should be considered when identifying at‐risk individuals.
Second, we found different associations with specific precautions within traits (Figure 2). This might be useful information for public health messaging for better adherence to specific precautions. These associations were further mirrored by perceptions of difficulty, effectiveness, and normativity of precautions: individuals high in neuroticism and low in conscientiousness, for instance, engaged in fewer precautions, but they also found it more difficult and less effective to do so, and they thought that fewer people would take these precautions. These findings suggest that recommendations for precautions need to be modified to be effective for those high in neuroticism and low in conscientiousness. For instance, people high in neuroticism may try to disassociate from threatening information to minimize the connection between their behaviour and the health outcome (Gunthert, Cohen, & Armeli, 1999; Rothman, Haddock, & Schwarz, 2001). It may be helpful to develop public health messaging that reduces such threat‐to‐health information.
Third, by considering facets of personality, we were able to obtain a deeper understanding of personality in the context of COVID‐19 responses. In the case for preparatory behaviours, specific facets of neuroticism (depression) and conscientiousness (responsibility) had more predictive power than the trait, and the association for agreeableness was masked by two facets (respectfulness and trust) that went in opposite directions. This pattern might be of interest for local authorities that appeal to the public to stop stockpiling (Zytaruk, 2020); their public health messages should particularly focus on these facets. Moreover, these findings confirm existing assumptions and research (Paunonen et al., 2003; Schimmack, Oishi, Furr, & Funder, 2004; Sutin et al., 2011) that an analysis at the facet level can provide a more detailed picture of personality–outcome relations than at the trait level.
Fourth, the findings on concerns could have implications for health care professionals, particularly in terms of identifying individuals who might be at risk for experiencing loneliness. Loneliness has been a frequently discussed public health issue during the coronavirus crisis (American Psychological Association, 2020; Luchetti et al., 2020, manuscript accepted for publication; Miller, 2020). We found that people high in neuroticism and extraversion reported greater concerns that the disruption in daily activities caused by the coronavirus will make them lonely (Table 2). These individuals might benefit most from inclusion in early interventions to promote social connectedness.
Finally, the findings on duration estimates may be of interest for economists who are concerned about financial investment and/or consumer confidence. For instance, individuals higher in extraversion reported shorter duration estimates until the USA recovers from financial losses. These individuals may be more likely to invest in the stock markets (Lai, 2019) and may also have greater consumer confidence, which may both positively contribute to the recovery of the US economy. Furthermore, duration estimates were interrelated with precautions and preparations (Table S3), suggesting that perceptions about the duration affect people's actual engagement in precautions and preparations.
In sum, identifying individuals based on their personality and subsequently delivering personality‐tailored messages may be useful during a pandemic. It might be possible to inexpensively screen large numbers of individuals in the community for high neuroticism scores, for instance, via web‐based questionnaires (Chapman, Hampson, & Clarkin, 2014; Lahey, 2009). The development of innovative approaches that promote personality‐tailored, real‐time, and accurately targeted messaging is now required.
Do these associations generalize to other contexts?
This study shows that personality predicts relevant psychological and behavioural responses in a real‐world crisis. A question that remains to be addressed is how much of the reported associations are specific to the coronavirus crisis or generalize to other contexts. 1 Based on the broader personality and health literature (Bogg & Roberts, 2004; Hampson & Friedman, 2008; Srivastava & Das, 2015; Strickhouser, Zell, & Krizan, 2017), we expect that our findings would generalize to other contexts. The premise of this study and the specific hypotheses were based on both personality theory and the large literature on the health benefits of conscientiousness, the health risks of neuroticism, and the optimistic worldview of extraversion. As such, we believe that the associations found with pandemic‐related reactions and behaviours reflect the processes of the traits. From another perspective, it may be argued that the coronavirus pandemic is a ‘strong situation’ that should mute the effects of personality (Meyer, Dalal, & Hermida, 2010; Mischel & Shoda, 1995, 1998). That is, when situations are strong, individual differences should matter less for predicting outcomes (e.g. if everyone in the population is concerned about the coronavirus, there would not be enough variability for personality to predict concerns). The findings from the present research do not support this argument. Presumably, the coronavirus pandemic is a strong situation given the health, economic, and social tolls on the population. Yet, personality traits continued to predict the outcomes in theoretically meaningful and theoretically expected ways.
Strengths and limitations
In terms of strengths, this study benefits from a large sample covering the adult lifespan, the assessment of all five major dimensions of personality prior to the acute phase of the coronavirus pandemic in the USA, and data on four psychological and behavioural pandemic‐related responses. However, it also has limitations that need to be addressed. First, the attrition across pretest/post‐test suggests selection effects that might limit the generalizability of the findings. Likewise, participants were from the USA, and it remains to be tested whether similar patterns are found in other cultural contexts. Second, potentially important variables were not assessed, such as COVID‐19 knowledge accuracy that could be a motive for behavioural responses. Third, questions regarding the outcomes were broad and self‐reported. Future studies could use more objective methods such as mobile sensing or the electronically activated recorder (Mehl, Pennebaker, Crow, Dabbs, & Price, 2001) to refine the knowledge on the role of personality in pandemic‐related behaviours. Such a design could track ambient sounds of individuals and examine whether they verbalize more worry or how many times the faucet is on, which could be a potential indicator of handwashing.
Conclusion
Overall, the results suggest that neuroticism, extraversion, and conscientiousness are linked to psychological and behavioural responses to the COVID‐19 pandemic. Several associations between personality traits and responses were stronger in older adults who are at higher risk for severe illness from COVID‐19. This study supports theory and research on the relation between personality and health and further contributes to the literature on pandemic‐related health behaviours. Public health officials may wish to take personality traits into account when planning and applying public health messages for precautions, and personality could be incorporated into health risk prediction models (Chapman, Lin, Roy, Benedict, & Lyness, 2019).
Data Accessibility Statement
We embrace the principle of sharing research data and thus provide a description of the measures, the data necessary to reproduce reported results, and the statistical scripts for the analyses reported in this manuscript on the Open Science Framework (OSF). The material can be retrieved from https://osf.io/tkbf5/.
Hypotheses and statistical analyses of this project were preregistered (https://osf.io/kbej9).
Conflict of Interest
The authors declare no potential conflicts of interest concerning the research, the authorship, and publication of this article.
Supporting information
Table S1 Zero‐Order Correlations Between (A) Personality Traits and Outcomes as well as (B) Sociodemographic Variables and Outcomes
Table S2. Personality Traits and Facets: Intercorrelations, Descriptive Statistics, and Reliabilities
Table S3. Outcomes: Intercorrelations and Descriptive Statistics
Table S4. Model 2: Controlling for Income
Table S5. Personality Traits Entered Simultaneously
Table S6. Personality Predicting Difficulty, Effectiveness, and Normativity of Precautions.
Table S7. Exploratory Model: Interaction Between Personality Traits
Table S8. Item‐Factor Loadings of Concern Items
Supporting info item
Acknowledgement
This work was supported by the National Institute on Aging of the National Institutes of Health (grants R21AG057917 and R01AG053297).
The authors would like to thank Dr André Kretzschmar (University of Zurich, Switzerland) for the r script to produce Figure 1.
Aschwanden, D. , Strickhouser, J. E. , Sesker, A. A. , Lee, J. H. , Luchetti, M. , Stephan, Y. , Sutin, A. R. , and Terracciano, A. (2020) Psychological and Behavioural Responses to Coronavirus Disease 2019: The Role of Personality. Eur. J. Pers., 10.1002/per.2281.



This article earned Open Data, Open materials and Preregistered + Analysis Plan badges through Open Practices Disclosure from the Center for Open Science: https://osf.io/tvyxz/wiki. The data are permanently and openly accessible at https://osf.io/tkbf5/. The permanent path to the registration is openly accessible at https://osf.io/kbej9. Author's disclosure form may also be found at the Supporting Information in the online version.
Footnotes
To tackle this issue more empirically, we ran a post hoc analysis with pretest data, correlating mindsets of preventive health with neuroticism and conscientiousness. We asked participants to rate ‘how much prevention affects health’ on a scale from 1 (no effect) to 5 (very strong effect). The association of prevention–health with neuroticism was negative (r = −.157, p < .000) and positive with conscientiousness (r = .212, p < .000). This means that individuals with higher neuroticism and lower conscientiousness tended to think ‘that prevention has a small effect on health’. These individuals also engaged in fewer precautions to avoid contracting the coronavirus.
References
- Abdelrahman, M. (2020). Personality traits, risk perception and protective behaviors during COVID‐19 [Preprint]. PsyArXiv. 10.31234/osf.io/6g7kh [DOI] [PMC free article] [PubMed]
- Aiken, L. S. , & West, S. G. (2011). Multiple regression: Testing and interpreting interactions, SAGE, Thousand Oaks, California, USA: Sage Publications, Inc. [Google Scholar]
- Alba, J. W. , & Williams, E. F. (2013). Pleasure principles: A review of research on hedonic consumption. Journal of Consumer Psychology, 23, 2–18. 10.1016/j.jcps.2012.07.003 [DOI] [Google Scholar]
- American Psychological Association . (2020). COVID‐19 isn't just a danger to older people's physical health. https://www.apa.org/news/apa/2020/03/covid-19-danger-physical-health
- Aschwanden, D. , Gerend, M. A. , Luchetti, M. , Stephan, Y. , Sutin, A. R. , & Terracciano, A. (2019). Personality traits and preventive cancer screenings in the health retirement study. Preventive Medicine, 126, 105763. 10.1016/j.ypmed.2019.105763 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Atlanta ISD . (2020). How to prevent the spread of COVID‐19. https://www.atlisd.net/39810
- Blagov, P. S. (2020). Adaptive and dark personality traits in the COVID‐19 pandemic: Predicting health‐behavior endorsement and the appeal of public‐health messages [Preprint]. PsyArXiv. 10.31234/osf.io/chgkn [DOI] [PMC free article] [PubMed]
- Bogg, T. , & Milad, E. (2020). Slowing the spread of COVID‐19: Demographic, personality, and social cognition predictors of guideline adherence in a representative U.S. sample [Preprint]. PsyArXiv. 10.31234/osf.io/yc2gq [DOI] [PubMed]
- Bogg, T. , & Roberts, B. W. (2004). Conscientiousness and health‐related behaviors: A meta‐analysis of the leading behavioral contributors to mortality. Psychological Bulletin, 130, 887–919. 10.1037/0033-2909.130.6.887 [DOI] [PubMed] [Google Scholar]
- Bolger, N. , & Schilling, E. A. (1991). Personality and the problems of everyday life: The role of neuroticism in exposure and reactivity to daily stressors. Journal of Personality, 59, 355–386. 10.1111/j.1467-6494.1991.tb00253.x [DOI] [PubMed] [Google Scholar]
- Carvalho, L. D. F. , Pianowski, G. , & Gonçalves, A. P. (2020). Personality differences and COVID‐19: are extroversion and conscientiousness personality traits associated with engagement with containment measures?. Trends in psychiatry and psychotherapy, S2237–60892020005005201. 10.1590/2237-6089-2020-0029 [DOI] [PubMed] [Google Scholar]
- Carver, C. S. , & Connor‐Smith, J. (2010). Personality and coping. Annual Review of Psychology, 61, 679–704. 10.1146/annurev.psych.093008.100352 [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention . (2020a). People who are at higher risk for severe illness. https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-at-higher-risk.html
- Centers for Disease Control and Prevention . (2020b). Preventing COVID‐10 from spreading 2020. https://www.cdc.gov/coronavirus/2019-ncov/if-you-are-sick/index.html? CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019‐ncov%2Fhcp%2Fguidance‐prevent‐spread.html
- Centers for Disease Control and Prevention . (2020c). Use of cloth face coverings to help slow the spread of COVID‐19. https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/diy-cloth-face-coverings.html
- Chan, K. H. , & Yuen, K.‐Y. (2020). COVID‐19 epidemic: Disentangling the re‐emerging controversy about medical facemasks from an epidemiological perspective. International journal of epidemiology, dyaa044. 10.1093/ije/dyaa044 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chapman, B. P. , Hampson, S. , & Clarkin, J. (2014). Personality‐informed interventions for healthy aging: Conclusions from a National Institute on Aging work group. Developmental Psychology, 50, 1426–1441. 10.1037/a0034135 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chapman, B. P. , Lin, F. , Roy, S. , Benedict, R. H. B. , & Lyness, J. M. (2019). Health risk prediction models incorporating personality data: Motivation, challenges, and illustration. Personality Disorders: Theory, Research, and Treatment, 10, 46–58. 10.1037/per0000300 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cooper, M. L. , Agocha, V. B. , & Sheldon, M. S. (2000). A motivational perspective on risky behaviors: The role of personality and affect regulatory processes. Journal of Personality, 68, 1059–1088. 10.1111/1467-6494.00126 [DOI] [PubMed] [Google Scholar]
- Costa, P. T. Jr. , & McCrae, R. R. (1992). Revised NEO personality inventory (NEOPI‐R) and NEO five‐factor inventory (NEO‐FFI) manual. Psychological Assessment Resources. https://www.scirp.org/(S(i43dyn45teexjx455qlt3d2q))/reference/ReferencesPapers.aspx?ReferenceID=1025708 [Google Scholar]
- Cucinotta, D. , & Vanelli, M. (2020). WHO declares COVID‐19 a pandemic. Acta Bio‐Medica: Atenei Parmensis, 91, 157–160. 10.23750/abm.v91i1.9397 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cuijpers, P. , Smit, F. , Penninx, B. W. J. H. , de Graaf, R. , ten Have, M. , & Beekman, A. T. F. (2010). Economic costs of neuroticism: A population‐based study. Archives of General Psychiatry, 67, 1086–1093. 10.1001/archgenpsychiatry.2010.130 [DOI] [PubMed] [Google Scholar]
- Emilsson, M. , Gustafsson, P. , Öhnström, G. , & Marteinsdottir, I. (2020). Impact of personality on adherence to and beliefs about ADHD medication, and perceptions of ADHD in adolescents. BMC Psychiatry, 20, 139. 10.1186/s12888-020-02543-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ferguson, C. J. , Muñoz, M. E. , Winegard, B. , & Winegard, B. (2012). The influence of heritability, neuroticism, maternal warmth and media use on disordered eating behaviors: A prospective analysis of twins. Psychiatric Quarterly, 83, 353–360. 10.1007/s11126-012-9205-7 [DOI] [PubMed] [Google Scholar]
- Friedman, H. S. (2000). Long‐term relations of personality and health: Dynamisms, mechanisms, tropisms. Journal of Personality, 68, 1089–1107. 10.1111/1467-6494.00127 [DOI] [PubMed] [Google Scholar]
- Gale, C. R. , Čukić, I. , Batty, G. D. , McIntosh, A. M. , Weiss, A. , & Deary, I. J. (2017). When is higher neuroticism protective against death? Findings from UK Biobank. Psychological Science, 28, 1345–1357. 10.1177/0956797617709813 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gross, J. J. , Sutton, S. K. , & Ketelaar, T. (1998). Relations between affect and personality: Support for the affect‐level and affective‐reactivity views. Personality and Social Psychology Bulletin, 24, 279–288. 10.1177/0146167298243005 [DOI] [Google Scholar]
- Gunthert, K. C. , Cohen, L. H. , & Armeli, S. (1999). The role of neuroticism in daily stress and coping. Journal of Personality and Social Psychology, 77, 1087–1100. 10.1037/0022-3514.77.5.1087 [DOI] [PubMed] [Google Scholar]
- Hakulinen, C. , Hintsanen, M. , Munafò, M. R. , Virtanen, M. , Kivimäki, M. , Batty, G. D. , & Jokela, M. (2015). Personality and smoking: Individual‐participant meta‐analysis of nine cohort studies. Addiction, 110, 1844–1852. 10.1111/add.13079 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hampson, S. E. , & Friedman, H. S. (2008). Personality and health: A lifespan perspective. In John O. P., Robin R. W., & Pervin L. A. (Eds.), Handbook of personality: Theory and research (pp. 770–794). New York, NY, USA: The Guilford Press. [Google Scholar]
- Hoyle, R. H. , Fejfar, M. C. , & Miller, J. D. (2000). Personality and sexual risk taking: A quantitative review. Journal of Personality, 68, 1203–1231. 10.1111/1467-6494.00132 [DOI] [PubMed] [Google Scholar]
- Kemp, E. , & Kopp, S. W. (2011). Emotion regulation consumption: When feeling better is the aim. Journal of Consumer Behaviour, 10, 1–7. 10.1002/cb.341 [DOI] [Google Scholar]
- Kroencke, L. , Geukes, K. , Utesch, T. , Kuper, N. , & Back, M. (2020). Neuroticism and emotional risk during the COVID‐19 pandemic [Preprint]. PsyArXiv. 10.31234/osf.io/8c6nh [DOI] [PMC free article] [PubMed]
- Lahey, B. B. (2009). Public health significance of neuroticism. American Psychologist, 64, 241–256. 10.1037/a0015309 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lai, C.‐P. (2019). Personality traits and stock investment of individuals. Sustainability, 11, 5474. 10.3390/su11195474 [DOI] [Google Scholar]
- Luchetti, M. , Lee, J. H. , Aschwanden, D. , Sesker, A. A. , Strickhouser, J. E. , Terracciano, A. , & Sutin, A. R. (2020). (manuscript submitted for publication). The trajectory of loneliness in response to COVID‐19. The final article will be available, upon publication, via its 10.1037/amp0000690 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luhmann, M. , & Eid, M. (2009). Does it really feel the same? Changes in life satisfaction following repeated life events. Journal of Personality and Social Psychology, 97, 363–381. 10.1037/a0015809 [DOI] [PubMed] [Google Scholar]
- Malouff, J. M. , Thorsteinsson, E. B. , Rooke, S. E. , & Schutte, N. S. (2007). Alcohol involvement and the five‐factor model of personality: A meta‐analysis. Journal of Drug Education, 37, 277–294. 10.2190/DE.37.3.d [DOI] [PubMed] [Google Scholar]
- Matzler, K. , Würtele, A. , & Renzl, B. (2006). Dimensions of price satisfaction: A study in the retail banking industry. International Journal of Bank Marketing, 24, 216–231. 10.1108/02652320610671324 [DOI] [Google Scholar]
- McCrae, R. R. , & Costa, P. T. (2006). Personality in adulthood: A five‐factor theory perspective (2nd ed.). New York, NY, USA: Guilford Press. [Google Scholar]
- McCrae, R. R. , & John, O. P. (1992). An introduction to the five‐factor model and its applications. Journal of Personality, 60, 175–215. 10.1111/j.1467-6494.1992.tb00970.x [DOI] [PubMed] [Google Scholar]
- Mehl, M. R. , Pennebaker, J. W. , Crow, D. M. , Dabbs, J. , & Price, J. H. (2001). The electronically activated recorder (EAR): A device for sampling naturalistic daily activities and conversations. Behavior Research Methods, Instruments, & Computers: A Journal of the Psychonomic Society, Inc, 33, 517–523. 10.3758/BF03195410 [DOI] [PubMed] [Google Scholar]
- Meyer, R. D. , Dalal, R. S. , & Hermida, R. (2010). A review and synthesis of situational strength in the organizational sciences. Journal of Management, 36, 121–140. 10.1177/0149206309349309 [DOI] [Google Scholar]
- Miller, G . (2020). Social distancing prevents infections, but it can have unintended consequences. https://www.sciencemag.org/news/2020/03/we-are-social-species-how-will-social-distancing-affect-us#
- Mischel, W. , & Shoda, Y. (1995). A cognitive‐affective system theory of personality: Reconceptualizing situations, dispositions, dynamics, and invariance in personality structure. Psychological Review, 102, 246–268. 10.1037/0033-295X.102.2.246 [DOI] [PubMed] [Google Scholar]
- Mischel, W. , & Shoda, Y. (1998). Reconciling processing dynamics and personality dispositions. Annual Review of Psychology, 49, 229–258. 10.1146/annurev.psych.49.1.229 [DOI] [PubMed] [Google Scholar]
- Molloy, G. J. , O'Carroll, R. E. , & Ferguson, E. (2014). Conscientiousness and medication adherence: A meta‐analysis. Annals of Behavioral Medicine, 47, 92–101. 10.1007/s12160-013-9524-4 [DOI] [PubMed] [Google Scholar]
- Mõttus, R. , Realo, A. , Allik, J. , Esko, T. , & Metspalu, A. (2012). History of the diagnosis of a sexually transmitted disease is linked to normal variation in personality traits. The Journal of Sexual Medicine, 9, 2861–2867. 10.1111/j.1743-6109.2012.02891.x [DOI] [PubMed] [Google Scholar]
- Nishiura, H. , Jung, S. , Linton, N. M. , Kinoshita, R. , Yang, Y. , Hayashi, K. , Kobayashi, T. , … Akhmetzhanov, A. R. (2020). The extent of transmission of novel coronavirus in Wuhan, China, 2020. Journal of Clinical Medicine, 9, 330. 10.3390/jcm9020330 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nolan, A. , McCrory, C. , & Moore, P. (2019). Personality and preventive healthcare utilisation: Evidence from the Irish Longitudinal Study on Ageing. Preventive Medicine, 120, 107–112. 10.1016/j.ypmed.2018.12.029 [DOI] [PubMed] [Google Scholar]
- Paunonen, S. V. , Haddock, G. , Forsterling, F. , & Keinonen, M. (2003). Broad versus narrow personality measures and the prediction of behaviour across cultures. European Journal of Personality, 17, 413–433. 10.1002/per.496 [DOI] [Google Scholar]
- R Core Team (2020). R: A language and environment for statistical computing (Version 4.0.0) [Computer software]. Vienna, Austria: R Foundation for Statistical Computing. Retrieved from http://www.R-project.org/ [Google Scholar]
- Rothman, A. J. , Haddock, G. , & Schwarz, N. (2001). “How many partners is too many?” Shaping perceptions of personal vulnerability. Journal of Applied Social Psychology, 31, 2195–2214. 10.1111/j.1559-1816.2001.tb00171.x [DOI] [Google Scholar]
- RStudio Team (2020). RStudio: Integrated Development for R (Version 1.1.456) [Computer software]. Boston, MA: RStudio. Retrieved from http://www.rstudio.com/ [Google Scholar]
- Schimmack, U. , Oishi, S. , Furr, R. M. , & Funder, D. C. (2004). Personality and life satisfaction: A facet‐level analysis. Personality and Social Psychology Bulletin, 30, 1062–1075. 10.1177/0146167204264292 [DOI] [PubMed] [Google Scholar]
- Shenandoah University . (2020). Shenandoah Director Of Graduate Public Health Programs Michelle Gamber, Who Is Engaged In COVID‐19 Research, Makes Some Suggestions For Practicing Good Social Distancing. https://www.su.edu/blog/2020/03/some-social-distancing-resources-from-an-expert/
- Shook, N. , Sevi, B. , Lee, J. , Fitzgerald, H. N. , & Oosterhoff, B. (2020). Who's listening? Predictors of concern about COVID‐19 and preventative health behaviors [preprint]. PsyArXiv. 10.31234/osf.io/c9rfg [DOI]
- Slavin, M. J. , Brodaty, H. , Kochan, N. A. , Crawford, J. D. , Trollor, J. N. , Draper, B. , & Sachdev, P. S. (2010). Prevalence and predictors of “subjective cognitive complaints” in the Sydney Memory and Ageing Study. The American Journal of Geriatric Psychiatry, 18, 701–710. 10.1097/JGP.0b013e3181df49fb [DOI] [PubMed] [Google Scholar]
- Soto, C. J. (2015). Is happiness good for your personality? Concurrent and prospective relations of the big five with subjective well‐being. Journal of Personality, 83, 45–55. 10.1111/jopy.12081 [DOI] [PubMed] [Google Scholar]
- Soto, C. J. , & John, O. P. (2017). The next Big Five Inventory (BFI‐2): Developing and assessing a hierarchical model with 15 facets to enhance bandwidth, fidelity, and predictive power. Journal of Personality and Social Psychology, 113, 117–143. 10.1037/pspp0000096 [DOI] [PubMed] [Google Scholar]
- Srivastav, A. , Santibanez, T. A. , Lu, P.‐J. , Stringer, M. C. , Dever, J. A. , Bostwick, M. , Kurtz, M. S. , … Williams, W. W. (2018). Preventive behaviors adults report using to avoid catching or spreading influenza, United States, 2015‐16 influenza season. PLoS ONE, 13, e0195085. 10.1371/journal.pone.0195085 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Srivastava, K. , & Das, R. (2015). Personality and health: Road to well‐being. Industrial Psychiatry Journal, 24, 1. 10.4103/0972-6748.160905 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stadler, M. , Niepel, C. , Botes, E. , Dörendahl, J. , Krieger, F. , & Greiff, S. (2020). Individual psychological responses to the SARS‐CoV‐2 pandemic: Different clusters and their relation to risk‐reducing behavior [preprint]. PsyArXiv.. 10.31234/osf.io/k8unc [DOI] [Google Scholar]
- Strickhouser, J. E. , Zell, E. , & Krizan, Z. (2017). Does personality predict health and well‐being? A metasynthesis. Health Psychology, 36, 797–810. 10.1037/hea0000475 [DOI] [PubMed] [Google Scholar]
- Sutin, A. R. , Luchetti, M. , Aschwanden, D. , Lee, J. H. , Sesker, A. A. , Strickhouser, J. , Stephan, Y. , & Terracciano, A. (2020). Change in five‐factor model personality traits during the acute phase of the coronavirus pandemic [Preprint]. PsyArXiv. 10.31234/osf.io/ja7b5 [DOI] [PMC free article] [PubMed]
- Sutin, A. R. , Stephan, Y. , Luchetti, M. , Artese, A. , Oshio, A. , & Terracciano, A. (2016). The five‐factor model of personality and physical inactivity: A meta‐analysis of 16 samples. Journal of Research in Personality, 63, 22–28. 10.1016/j.jrp.2016.05.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sutin, A. R. , & Terracciano, A. (2016). Five‐factor model personality traits and the objective and subjective experience of body weight: Personality and body weight. Journal of Personality, 84, 102–112. 10.1111/jopy.12143 [DOI] [PubMed] [Google Scholar]
- Sutin, A. R. , Terracciano, A. , Kitner‐Triolo, M. H. , Uda, M. , Schlessinger, D. , & Zonderman, A. B. (2011). Personality traits prospectively predict verbal fluency in a lifespan sample. Psychology and Aging, 26, 994–999. 10.1037/a0024276 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Terracciano, A. , & Costa, P. T. (2004). Smoking and the five‐factor model of personality. Addiction, 99, 472–481. 10.1111/j.1360-0443.2004.00687.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Terracciano, A. , Löckenhoff, C. E. , Crum, R. M. , Bienvenu, O. J. , & Costa, P. T. (2008). Five‐factor model personality profiles of drug users. BMC Psychiatry, 8. 10.1186/1471-244X-8-22 [DOI] [PMC free article] [PubMed] [Google Scholar]
- The White House . (2020). 15 days to slow the spread. https://www.whitehouse.gov/articles/15-days-slow-spread/
- Turiano, N. A. , Mroczek, D. K. , Moynihan, J. , & Chapman, B. P. (2013). Big 5 personality traits and interleukin‐6: Evidence for “healthy neuroticism” in a US population sample. Brain, Behavior, and Immunity, 28, 83–89. 10.1016/j.bbi.2012.10.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Turiano, N. A. , Weston, S. J. , Čukić, I. , Mueller, S. , Zhaoyang, R. , Zyoneda, T. , Aschwanden, D. , et al. (2018). Is healthy neuroticism associated with mortality? Evidence from a 14‐study coordinated analysis. Innovation in Aging, 2, 785–786. 10.1093/geroni/igy023.2910 [DOI] [Google Scholar]
- Weiss, A. , & Deary, I. J. (2019). A new look at neuroticism. Should we worry so much about worrying? 29, 92–101. 10.1177/0963721419887184 [DOI] [Google Scholar]
- Weston, S. J. , & Jackson, J. J. (2015). Identification of the healthy neurotic: Personality traits predict smoking after disease onset. Journal of Research in Personality, 54, 61–69. 10.1016/j.jrp.2014.04.008 [DOI] [Google Scholar]
- Wilson, K. E. , & Dishman, R. (2015). Personality and physical activity: A systematic review and meta‐analysis. Personality and Individual Differences, 72, 230–242. 10.1016/j.paid.2014.08.023 [DOI] [Google Scholar]
- World Health Organization . (2020). Coronavirus disease (COVID‐19) advice for the public 2020. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public
- Zhang, X. , Wang, Y. , Lyu, H. , Zhang, Y. , Liu, Y. , & Luo, J. (2020). The influence of COVID‐19 on well‐being [Preprint]. PsyArXiv. 10.31234/osf.io/znj7h [DOI]
- Zytaruk, T . (2020). Surrey mayor appeals to people's ‘basic humanity’ to stop stockpiling, re‐selling. https://www.northdeltareporter.com/news/surrey-mayor-appeals-to-peoples-basic-humanity-to-stop-stockpiling-re-selling/
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1 Zero‐Order Correlations Between (A) Personality Traits and Outcomes as well as (B) Sociodemographic Variables and Outcomes
Table S2. Personality Traits and Facets: Intercorrelations, Descriptive Statistics, and Reliabilities
Table S3. Outcomes: Intercorrelations and Descriptive Statistics
Table S4. Model 2: Controlling for Income
Table S5. Personality Traits Entered Simultaneously
Table S6. Personality Predicting Difficulty, Effectiveness, and Normativity of Precautions.
Table S7. Exploratory Model: Interaction Between Personality Traits
Table S8. Item‐Factor Loadings of Concern Items
Supporting info item
Data Availability Statement
We embrace the principle of sharing research data and thus provide a description of the measures, the data necessary to reproduce reported results, and the statistical scripts for the analyses reported in this manuscript on the Open Science Framework (OSF). The material can be retrieved from https://osf.io/tkbf5/.
Hypotheses and statistical analyses of this project were preregistered (https://osf.io/kbej9).