

Abstract
As the COVID‐19 pandemic continues to claim lives across the globe, insufficient data exists regarding the optimal treatment. It is well known that patients 55 years of age or older and patients with certain chronic diseases are at higher risk of severe illness, including acute respiratory distress syndrome and death. A potentially fatal pulmonary complication of sickle cell disease, acute chest syndrome, can be precipitated by acute infections, including respiratory viruses. We report the case of a patient with sickle cell disease (HbSC) who developed COVID‐19 pneumonia and acute chest syndrome who was treated with emergent red blood cell exchange in order to avoid endotracheal intubation.
Keywords: acute chest syndrome, HbSC, SARS‐CoV‐2
1. INTRODUCTION
At the time of this writing the COVID‐19 pandemic, caused by the novel coronavirus SARS‐CoV‐2, has spread across the globe to every continent except Antarctica, involving 195 countries. According to the World Health Organization, at least 2.3 million people have been infected worldwide, and the death toll is 162 956 as of April 21, 2020. 1 Infections vary considerably, from asymptomatic carriers to fatal cases complicated by acute respiratory distress syndrome (ARDS), septic shock, thromboses, and cytokine release syndrome. The most common findings in symptomatic patients are fever, dry cough, and shortness of breath. 2 Older patients (55 years of age and older) and those with certain chronic diseases, including cardiovascular and pulmonary diseases, and diabetes mellitus, are at high risk for severe disease, and sickle cell disease is no exception. As the COVID‐19 pandemic continues to unfold, there is limited information on the severity of COVID‐19 on sickle cell patients or how these patients should be treated. Acute chest syndrome (ACS) is often precipitated by respiratory infection, and description of the clinical overlap between COVID‐19 pneumonia and ACS has been described. 3 , 4 The standard of care for treating sickle cell patients who meet clinical criteria for ACS is transfusion therapy, which we feel should be considered regardless of COVID‐19 status. At the time of this writing, two case reports are published online describing red blood cell exchange to treat acute chest syndrome in the setting of COVID‐19. 5 , 6 To the best of our knowledge, this is the first report of a COVID‐19 positive sickle cell patient with HbSC phenotype with ACS treated with red blood cell exchange (RBCX).
2. CASE REPORT
A 27‐year‐old male with sickle cell disease (HbSC phenotype) was transferred to our institution's COVID‐19 intensive care unit (ICU) from an outside hospital due to worsening hypoxemic respiratory failure. Eleven days prior, he presented to the outside facility complaining of vaso‐occlusive crisis pain, fever, chills, cough, and shortness of breath. He had a history of frequent admissions for pain, had been on hydroxyurea previously but had last filled this prescription more than 4 months earlier and had not been seen in our outpatient sickle cell clinic for more than 1 year. He had regularly been filling his maintenance pain medication, oxycodone‐acetaminophen every 6 hours as needed. Physical examination revealed temperature of 39.2°C, and his oxygen saturation was reportedly adequate. COVID‐19 testing was performed on the day of admission to the outside hospital and was positive per transfer report. Based on hospital records, he was initially started on ceftriaxone and doxycycline, but this was changed to piperacillin and tazobactam on hospital day 3. Treatment for COVID‐19 started on hospital day 3 and included 5 days of hydroxychloroquine and azithromycin. He received intravenous methylprednisone 40 mg twice daily during this time and also had a single dose of tocilizumab administered. On hospital day 11, his oxygen requirement increased significantly, requiring non‐rebreather mask, and a chest X‐ray showed worsening bilateral infiltrates. Transfer to our institution was requested for a higher level of care and potential RBCX, and the COVID ICU team notified the Transfusion Medicine on call physician of the possible need for emergent exchange for acute chest syndrome prior to the patient's arrival. Upon admission to our COVID‐19 ICU, his temperature was 37.2°C, blood pressure of 124/77 mmHg, pulse rate of 82 beats per minute, respiration rate 24 breaths per minute, and oxygen saturation of 95% on 10 L/min via nasal cannula. Due to institutional procedures surrounding COVID‐19, patients needing more than 6 L/min of oxygen via nasal cannula are considered for endotracheal intubation and mechanical ventilation to reduce risk of aerosolizing viral particles. Therefore, he was rapidly weaned from 10 to 6 L/min via nasal cannula with adequate saturation that remained greater than 95%, but was still at high risk for intubation should his respiratory status decline further. His admission labs were remarkable for a white blood count of 44 700/μL (absolute neutrophil count of 33 100/μL, absolute lymphocyte count of 2200/μL), hemoglobin of 10.4 g/dL, and LDH of 732 U/L. Fraction of HbS + HbC was 94% (Table 1). Portable chest X‐ray on admission revealed extensive interstitial and alveolar infiltrates throughout both lungs consistent with COVID‐19 pneumonia (Figure 1). Procalcitonin level was <0.25 ng/mL, so he was no longer considered to have an active bacterial infection and antibacterials were held on admission to our hospital. Pain control was continued with intravenous hydromorphone administered by a patient controlled analgesia (PCA) pump. Supportive care was maintained as the primary COVID‐19 specific therapy, given the treatment that he had previously completed as well as the hospital guidelines at the time, therapies such as remdesivir or convalescent plasma were not readily available or encouraged based on the current evidence at the time of admission. Blood bank technical staff contacted the transferring facility's blood bank to confirm whether he had known antibodies. He was group O Rh negative with no known antibodies, which was confirmed by our blood bank laboratory. He had not been transfused at the outside hospital. In the meantime, a 15.5 Fr triple lumen dialysis catheter was placed in his right common femoral vein.
TABLE 1.
Vital signs and laboratory data on admission, following RBCX, and at discharge
| Labs/vitals | Initial admission (4/18/20) | Post‐RBC exchange (4/19/20) | Discharge (5/1/20) |
|---|---|---|---|
| Temperature | 37.2°C | 36.8°C | 36.7°C |
| Blood pressure | 124/77 | 120/68 | 110/68 |
| Pulse rate | 82 | 86 | 93 |
| Oxygen saturation | 95% on 10 L/min via nasal cannula | 98% on 2 L/min via nasal cannula | 95% on 2 L/min via nasal cannula |
| Respiratory rate | 24/min | 20/min | 18/min |
| WBC count | 44 700/μL | 20 300/μL | 23 600/μL |
| Hemoglobin | 10.4 g/dL | 10.3 g/dL | 11.5 g/dL |
| Hematocrit | 31.6% | 31.3% | 34.9% |
| Platelet count | 1 338 000/μL | 504 000/μL | 371 000/μL |
| LDH | 732 U/L | N/A | 341 U/L |
| Fraction of HbS + HbC | 94% | 34% | N/A |
FIGURE 1.
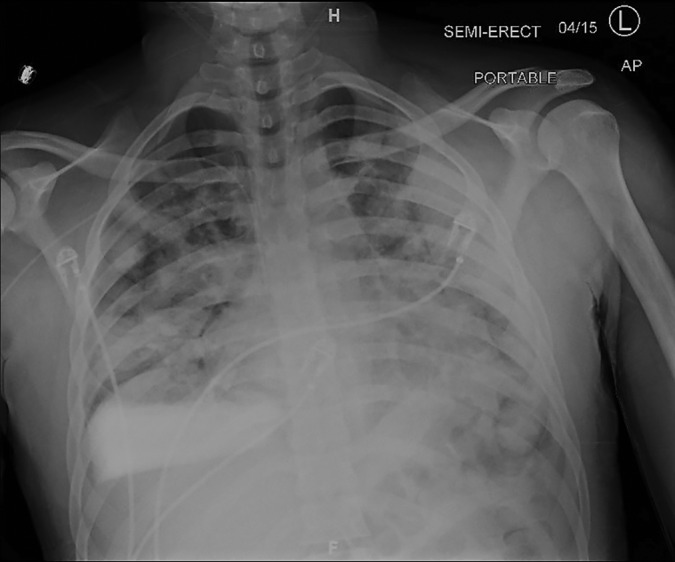
Admission chest X‐ray showing interstitial and alveolar infiltrates throughout both lungs
Due to the patient's high risk for decompensation and intubation, the blood bank requirement for C, E, and K antigen‐negative RBCs was waived to expedite RBCX, which was accomplished using the SPECTRA OPTIA Apheresis System (TerumoBCT, Lakewood, Colorado), using Fraction of Cells Remaining (FCR) 30%, end hematocrit 30%, and goal HbS + HbC fractionation <30%. Based on height of 170 cm and weight of 65 kg, the total blood volume was 4.5 L, and 2857 mL of the patient's native RBCs were removed and replaced with 2441 mL of HbS‐negative donor RBCs (eight units) with an average unit hematocrit of 60%. ACD‐A was used for anticoagulation with AC ratio of 13, and calcium gluconate 2 g was added to normal saline 250 mL for calcium replacement. According to institution guidelines for COVID‐19, the apheresis nurse donned an N95 respirator and surgical mask, disposable gown and gloves, goggles, and head and shoe covers. The paper apheresis worksheet was protected by a clear plastic cover. The patient was in a private room to allow as much distance as possible between providers and patient. After the exchange, the apheresis machine was immediately decontaminated using institution‐approved disposable bleach wipes.
Immediately after the red blood cell exchange, the hematocrit was 31.3%, and the HbS + HbC fractionation was decreased to 34%. Within 2 hours of completing the procedure, his respiratory status improved and his oxygen saturation was 98% on 2 L/min via nasal cannula. With his improvement, he was transferred from the ICU to the COVID‐19 medical floor where he remained afebrile and breathing room air at rest, while needing 2 L/min via nasal cannula on exertion. He was discharged home on hospital day 12 with home oxygen for ambulation as well as with prescriptions for his maintenance pain medications and to restart hydroxyurea. Despite waiving the requirement for C, E, and K‐negative RBCs for the exchange, he exhibited no evidence of transfusion‐related hemolysis; his Hb remained stable throughout his hospital course, and his LDH gradually declined.
3. DISCUSSION
At the time of this writing, no definitive treatment exists for COVID‐19, although several clinical trials are ongoing to identify effective pharmacologic and biologic agents against the SARS‐ CoV‐2 virus. Current treatment is supportive care aimed at preventing or mitigating the severe complications of COVID‐19 pneumonia. 7 Patients often suffer precipitous respiratory failure requiring endotracheal intubation and mechanical ventilation, and these patients often remain intubated for 2 to 3 weeks before either recovering or succumbing to the disease. Sickle patients may present with ACS which can have overlapping symptoms with COVID‐19 as detailed previously. Beerkens et al, highlighted a case of ACS caused by COVID‐19, where the patient with a history of HbS/β0‐thalassemia presented initially with left hip pain related to avascular necrosis, but on hospital day 5 spiked a fever, and in spite of antibiotic therapy with ceftriaxone and azithromycin, remained febrile and developed bilateral pulmonary infiltrates by hospital day 10. Additional similarities between our cases included elevated LDH and very high abnormal hemoglobin content on fractionation (88% in Beerkens' case vs 94% in ours). Initially treated with simple transfusion of 1 unit of RBCs, the patient underwent RBCX on hospital day 11 due to decompensation, with oxygenation improvement beginning HOSPITAL DAY 13. In contrast, our patient had notable oxygenation improvement within hours. 5 In another case study, Hussain et al, provide clinical courses of four patients with sickle cell disease: HbSS who received RBCX after intubation, HbS/β + who presented with typical vaso‐occlusive crisis symptoms and was positive for COVID‐19 but did not require supplemental oxygen, HbSS with nausea, vomiting and diarrhea after 1 day, febrile for 1 day then improved, and a HbSC patient who had been symptomatic the week prior with cough and fever, was diagnosed for COVID‐19 elsewhere but left against medical advice, and was discharged after 4 days without developing respiratory symptoms. 6 These cases demonstrate the varied presentations sickle patients may exhibit as well as a spectrum of clinical courses. Our case highlights how early coordination between the ICU service and Transfusion Medicine can mobilize resources to rapidly execute a red blood cell exchange in a patient at risk for mechanical ventilation. RBC transfusion provided either by simple transfusion or RBCX plays an important role in the management of acute chest syndrome in sickle cell disease, and expert panels have made strong recommendations for the use of RBCX rather than simple transfusion in severe ACS. 8 Our patient was treated early with RBCX which may have made a difference in his course of disease. Our patient's oxygen requirement decreased from 6 to 2 L/min via nasal cannula, pre‐ and post‐RBCX, and he did not require intubation.
CONFLICT OF INTEREST
The authors declare they have no conflicts of interest relevant to the article.
Allison D, Campbell‐Lee S, Crane J, et al. Red blood cell exchange to avoid intubating a COVID‐19 positive patient with sickle cell disease? J Clin Apher. 2020;35:378–381. 10.1002/jca.21809
REFERENCES
- 1. Coronavirus Disease 2019 (COVID‐19) Situation Report – 92. World Health Organization. https://www.who.int/docs/default‐source/coronaviruse/situation‐reports/20200421‐sitrep‐92‐covid‐19.pdf?sfvrsn=38e6b06d_4. Accessed April 21, 2020.
- 2. Singhal T. A review of coronavirus disease‐2019 (COVID‐19). Indian J Pediatr. 2020;87(4):281‐286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Li Y, Xia L. Coronavirus disease 2019 (COVID‐19): role of chest CT in diagnosis and management. AJR Am J Roentgenol. 2020;214:1‐7. 10.2214/AJR.20.22954. [DOI] [PubMed] [Google Scholar]
- 4. Paul RN, Castro OL, Aggarwal A, Oneal PA. Acute chest syndrome: sickle cell disease. Eur J Haematol. 2011;87:191‐207. 10.1111/j.1600-0609.2011.01647.x. [DOI] [PubMed] [Google Scholar]
- 5. Beerkens F, John M, Puliafito B, Corbett V, Edwards C, Tremblay D. COVID‐19 pneumonia as a cause of acute chest syndrome in an adult sickle cell patient. Am J Hematol. 2020;95:E154‐E156. 10.1002/ajh.25809. [DOI] [PubMed] [Google Scholar]
- 6. Hussain F, Njoku FU, Saraf SL, Molokie RE, Gordeuk VR, Han J. COVID‐19 infection in patients with sickle cell disease. Br J Haematol. 2020;189:851‐852. 10.1111/bjh.16734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Cunningham AC, Goh HP, Koh D. Treatment of COVID‐19: old tricks for new challenges. Crit Care. 2020;24:91. 10.1186/s13054-020-2818-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Yawn BP, Buchanan GR, Afenyi‐Annan AN, et al. Management of sickle cell disease: summary of the 2014 evidence‐based report by expert panel members. JAMA. 2014;312(10):1033‐1048. [DOI] [PubMed] [Google Scholar]