

Abstract
Objective:
Leadership is an important factor in creating a safe and healthy work environment. Little is known about its influence in small organizations. This study assessed the relationship between leadership, climate, and employee behavior in organizations with <500 employees.
Methods:
We examined organizational factors and worker perceptions of leadership and safety/health behaviors in an analysis of 1,271 employees in 53 Colorado small organizations. Cross-sectional relationships were assessed using multivariable linear regression models.
Results:
Perceived leadership commitment to safety was associated with safety climate (β = 0.67) and safety behaviors among employees (β = 0.45). Perceived leadership commitment to worksite wellness was associated with health climate (β = 0.66) and health behaviors (β = 0.42).
Conclusions:
Leadership plays an important role in creating a positive work environment around safety and health.
Keywords: Total Worker Health, occupational safety and health, health promotion, health protection, safety climate, health climate, worksite wellness
Introduction:
Leadership contributes significantly to an organization’s safety and health climates and to employee safety and health behaviors. The study of these relationships has increased over the last few decades, but it has lagged in small organizations (1, 2). Most of the small organization literature has focused on either safety or health and wellness. Understanding the work environment as a whole is important when implementing more holistic Total Worker Health® (TWH) interventions to improve workplace safety, health, and well-being (3, 4). Furthermore, most of this literature has not examined factors such as organization size, from micro to larger. It is important to evaluate the relationship between leadership and climate and behavior amongst small organizations because they engage in fewer safety, health, and well-being activities than larger organizations and their employees experience high rates of work-injury and higher rates of poor health (3, 4). Studies of large organizations have identified the importance of leadership in establishing safety climate and health climate (5). The purpose of this study was to understand the relationship between leadership and safety and health climates and behavior in small organizations (< 500 employees as defined by the National Small Business Administration) and to determine whether these relationships differed by definition of small organization.
As the research around workplace safety evolved and safety climate emerged as a field of study in its own right, leadership proved to be an important driver of safety climate and employee behavior (6). According to reviews of organizational climate, culture, and leadership research, leadership is a well-established antecedent of safety climate and behavior (1, 7–12). For example, a meta-analysis found that transformational leadership positively impacted safety climate, safety compliance, and participatory safety behaviors (8). A qualitative study among 14 owners and 21 workers in the dry-cleaning industry indicated that owners said complying with regulations and economic concerns were more important than workplace health and safety. When asked about their employers’ concern for health and safety, employees expressed doubt that their managers prioritized workplace health and safety through examples of how their managers stressed the importance of making a profit and returning clothes to customers (13). This shows how perceptive employees can be when it comes to how their leadership values employee health and safety. Another study demonstrated that a leadership intervention resulted in improved safety climate, safety compliance, and participatory safety behaviors (11). However, research indicates that leadership is more associated with participatory behaviors than compliance behaviors (14). In this study, we defined participatory safety behaviors as individual, voluntary actions like attending a safety meeting or other safety activities whereas compliance behaviors are mandated actions that are necessary to keep the workplace and workers safe, such as wearing personal protective equipment (15). We hypothesized that employees who perceived higher levels of leadership commitment to safety would also perceive a better safety climate and would report higher levels participatory safety behaviors.
Hypothesis 1: Employees working in small organizations who perceive higher levels of leadership commitment to safety will have higher scores on safety climate and participatory safety behavior.
While the health climate literature is sparser than safety climate literature, it is emerging as a field of interest. Health climate is a distinct climate from safety climate, although they may be correlated with one another (5, 16). Health climate is associated with supervisor support (5), indicating that health climate could follow the same pattern established in the safety climate literature, where leadership impacts safety climate and safety behaviors (15, 17, 18). For example, one study found that a better workplace health climate was correlated with healthy days, which is a measure of overall health used by the Centers for Disease Control and Prevention (CDC) (16). Additionally, better leadership has been associated with better self-reported physical health and health outcomes, specifically, fewer instances of self-reported musculoskeletal symptoms (19). Inversely, poor leadership has been associated with poor health outcomes, such as musculoskeletal pain (19) and poor self-rated health (20). In addition, leadership support for health promotion activities increases participation in workplace health promotion programs (21, 22). Another study found that leadership which was hands on, accessible, supportive, inclusive, and democratic was most successful in creating a work environment that was supportive of health promotion (23). Thus, we hypothesized that employees who perceive higher levels of leadership commitment to worksite wellness, would also perceive a better health climate and report higher levels of participatory health behaviors.
Hypothesis 2: Employees working in small organizations who perceive higher levels of leadership commitment to worksite wellness will have higher scores on health climate and participatory health behaviors.
Leadership is thought to be an important driver of climate and behavior, regardless of the size of an organization. Cunningham et al. urges researchers to understand the state of workplace health and safety by different definitions of small organization (2). For example, the environment of a micro-sized organization with fewer than 10 employees may be different than that of a larger small organization with, say, 400 employees. An example of this could be the adoption of formal human resources practices. The management literature has demonstrated that the adoption of formal human resource management practices increase as organizations grow (24). Another study found that the size of an organization is negatively associated with organizational commitment, where employees of smaller organizations demonstrated higher levels of commitment (25). Based on the management literature, it would make sense that health and safety attitudes and practices would also differ by size of organization. A few studies have begun to address this issue. A qualitative study of small business owners suggests that small employers often leave the management of health and safety programs up to their employees (26). One study found that larger organizations, defined as having 20 or more employees, had higher scores for management commitment to safety, social support, and safety motivation compared to smaller organizations (27). Thus, while there is some evidence to suggest that the quality of leadership, climate, and behaviors may differ by size of organization (27), our null hypothesis is that the relationship between leadership and climate and behavior does not differ by size of small organization.
Hypothesis 3: The associations seen in Hypotheses 1 and 2 will not differ by gradation of organization size.
Methods:
From April 2017 through December 2018, we recruited 53 Colorado organizations to participate in a longitudinal study called the Small + Safe + Well (SSWell) Study. Details of the study design and theoretical framework have been previously described (3). In brief, organizations participate in a TWH intervention consisting of Health Links™ (4) and a TWH leadership training program, which consists of a six hour in-person training and virtual follow-up for three months after the training (3). To test our hypotheses, we utilized cross-sectional demographic data from the Health Links Healthy Workplace Assessment (4) and cross-sectional data from the Employee Health and Safety Culture Survey completed by employees in participating businesses. This study was approved by the Colorado Multiple Institutional Review Board (COMIRB).
Study Population:
Workplaces
Fifty-three organizations were recruited to participate in the SSWell study from April 2017 through December 2018. In order to be eligible to participate, businesses had to be located within the state of Colorado and employ fewer than 500 employees. Organizations were excluded if they had enrolled in Health Links prior to March 2017. We recruited organizations using multiple outreach methods, including email marketing, regional events, and through channel partners including chambers of commerce, workers’ compensation insurers, local public health agencies, health and wellness coalitions, and trade associations.
Employees
Employees were recruited from the 53 organizations participating in the SSWell Study to complete an Employee Health and Safety Culture Survey. The study coordinator generated a unique survey link and sent it to our main contact at each organization, who then forwarded the link to their employees. The online survey was available for two weeks and the study coordinator sent a reminder email to the main contact half-way through that period. A Spanish language version of the survey was made available to all organizations. One organization requested a paper survey, and those data were later entered manually. Employees who completed the survey had the option to enter their email address into a raffle to win one of fifteen $100 gift cards. Email addresses were collected on a separate database. No identifying information was collected in the Employee Health and Safety Culture Survey, and the employer was blinded to the individual level responses and to whether employees completed the survey at all. All survey data were managed using REDCap data capture tools hosted at the University of Colorado Anschutz Medical Campus. A total of 4,244 employees from the 53 businesses were eligible to participate in the study. We had a total of 1,271 survey responses (response rate = 30%). Survey response rates differed by size of organization, where smaller organizations had higher response rates and larger organizations had lower response rates. Micro organizations had a response rate of 74%, small organizations had a response rate of 53%, medium organizations had a response rate of 40%, and large organizations had a response rate of 17%. The overall response rate of Presidents or CEOs was 34%. 38% of Presidents or CEOs of micro organizations responded, 36% of small organizations responded, 22% of medium organizations responded and 50% of Presidents or CEOs of large organizations responded to the survey.
Measures:
Organizational Level Measures
One representative from participating organizations completed the Health Links Healthy Workplace Assessment (3). The representative who completed the assessment ranged from Human Resource Managers to Safety Coordinators to the Owner. From this assessment, we collected organizational demographic information including industry, geographic region (urban vs. rural), and organization size. Organization size was categorized into four categories: micro (less than 10 employees), small (11 – 50 employees), medium (51–200 employees), and large (201 – 499 employees).
Employee Level Measures
The Employee Health and Safety Culture Survey contained 108 items that asked about employees’ demographics as well as their perspectives on several constructs addressing organizational environment in general as well as workplace health and safety. For this study, we focused on three constructs of the safety-specific environment and three constructs of the health-specific environment. All scales were adopted from previously evaluated studies except for the leadership commitment to safety and worksite wellness questions, which were developed by the researchers to complement part of the Health Links Healthy Workplace Assessment (4). All items in the survey were rated on a five-point Likert scale from strongly disagree to strongly agree. A confirmatory factor analysis indicated that the six indicators are empirically distinct, supporting our conceptual distinctions among the measures (see Table 1, Supplemental Digital Content 1 for more detail).
Table 1.
Demographic Characteristics of Employees Participating in the SSWell Study. N = 1,271.
| Characteristic | n (%) | Mean (SD) |
|---|---|---|
| Age | 41.3 (13.1) | |
| Gender | ||
| Female | 842 (66.2%) | |
| Male | 419 (33.0%) | |
| Race | ||
| White | 1,184 (93.2%) | |
| Black/African American | 34 (2.7%) | |
| Asian | 30 (2.4%) | |
| Native American/Alaskan Native | 21 (1.7%) | |
| Native Hawaiian/Pacific Islander | 7 (0.6%) | |
| Ethnicity | ||
| Hispanic/Latino/Spanish | 123 (9.7%) | |
| Education | ||
| Did not complete high school | 8 (0.6%) | |
| High school diploma or GED | 110 (8.7%) | |
| Some college or 2-year degree | 288 (22.7%) | |
| 4-year college degree | 462 (36.3%) | |
| Graduate or professional degree | 247 (19.4%) | |
| Job Level | ||
| Non-management | 768 (60.4%) | |
| Management | 500 (39.3%) | |
| Job Tenure (y, SD) | 5.3 (6.7) | |
| Salaried | 661 (52.0%) | |
| Full-time worker | 1,090 (85.8%) | |
| Hours worked per week (h, SD) | 39.4 (12.4) | |
| Shift work | 181 (14.2%) | |
| Contract work | 48 (3.8%) |
Demographics.
We collected information on employee demographics including age, gender, ethnicity, and race, and questions specific to their work, such as job tenure, job level, and type of work (salaried vs. hourly, contract work, shift work, etc.) from the employee survey.
Safety-specific environment.
We asked employees to rate their leadership’s commitment to safety via five items assessing communication, role modeling, positive feedback, resource allocation, and accountability. This construct represents health-protecting leadership, but we used the term “safety” because it is a commonly understood term among the survey respondents. One example item from this construct is “Leaders are role models for prioritizing safety.” Employees were also asked to rate their company’s safety climate via six items measuring organizational commitment to safety (28). An example item from this construct is “My organization listens carefully to our ideas about improving safety” (28). The final safety-specific indicator of the work environment was an employee’s participation in safety programs. Participatory safety behaviors consisted of three items that assessed proactive participation in the safety program (15). An example item from this construct is “I promote the safety program within the organization” (15).
Health-specific environment.
We asked employees to rate their leadership’s commitment to worksite wellness via five items assessing communication, role modeling, positive feedback, resource allocation, and accountability. Leadership commitment to worksite wellness represents health promoting leadership, but we used the term “worksite wellness” because it is commonly understood among employees. One example item from this construct is “Leaders are role models for prioritizing worksite wellness.” Employees were also asked to rate their company’s health climate via four items measuring organizational commitment to health (16). An example item from this construct is “My organization is committed to employee health and well-being” (16). The final health-specific indicator of the work environment was an employee’s participation in health promotion programs. Participatory health behaviors consisted of three items that assessed proactive participation in the worksite wellness program (15). An example item from this construct is “I promote the worksite wellness program within the organization” (15).
Statistical Analysis:
We calculated Cronbach’s alpha and correlation between each of the Employee Health and Safety Culture Survey items for each of the unique constructs to assess their reliability as well as their convergent and discriminant validity. We then generated descriptive statistics for the demographic, safety-specific, and health-specific indicators.
To test hypotheses 1 and 2, we used linear mixed model regression analyses with a random effect for organization. A compound symmetry covariance matrix was used for the random effect. We chose this strategy to account for the nested nature of the data, in that we had multiple employees from each organization in this dataset. We first performed unadjusted univariate regressions between leadership commitment to safety and safety climate and participatory safety behaviors. We then adjusted the models for industry, region, size of organization, age, gender, job level, and job tenure. In addition, we performed unadjusted regressions between leadership commitment to health and health climate and participatory health behaviors, followed by adjusted regressions controlling for industry, region, size of organization, age, gender, job level, and job tenure.
To test Hypothesis 3, the multivariable models described above were re-run to include an interaction term between size of organization and leadership commitment to safety and health. We used an F-test to determine if the interaction term meaningfully contributed to the model, defined as a p-value < 0.05. When the interaction term meaningfully contributed to the model, we used estimate statements to determine which size category was driving the association. In these instances, the large size was the referent group. All analyses were conducted using SAS version 9.4 (Cary, NC).
Results:
Demographic characteristics
More than half of the participating organizations were in the services industry (N = 28, 53%), 13% (N = 7) were in public administration, 11% (N = 6) were in healthcare and social assistance, 8% (N = 4) were in retail, 6% (N = 3) were in construction, 6% (N = 3) in manufacturing, and 4% (N = 2) in transportation. Most were located in an urban area (N = 39, 74%). Micro businesses made up 15% of this sample (representing 36 employees), with 40% small businesses (representing 248 employees), 34% medium businesses (representing 664 employees), and 11% large businesses (representing 323 employees).
Two-thirds of the survey respondents were female (N = 842, 66%) and the average age was 41 years (SD = 13). This sample was highly educated, as the majority of respondents (N = 997, 78%) had achieved at least some college or a 2-year degree or higher. More than half reported being in a non-management role (N = 768, 60%), were full time workers (N = 1,090, 86%), and the average job tenure was 5 years (SD = 7) (Table 1). Demographic characteristics stratified by size of organization can be seen in Table 2, Supplemental Digital Content 2.
Table 2.
Means, standard deviations, reliabilities, and correlations of employee level indicators of safety and health at work. N = 1,271
| Mean | SD | Perceived leadership commitment to safety | Safety climate | Participatory safety behaviors | Perceived leadership commitment to worksite wellness | Health climate | Participatory health behaviors | |
|---|---|---|---|---|---|---|---|---|
| Perceived leadership commitment to safety | 3.68 | 0.84 | 0.92 | 0.77 | 0.49 | 0.69 | 0.61 | 0.38 |
| Safety climate | 3.83 | 0.79 | 0.92 | 0.46 | 0.56 | 0.63 | 0.35 | |
| Participatory safety behaviors | 3.81 | 0.77 | 0.88 | 0.37 | 0.40 | 0.50 | ||
| Perceived leadership commitment to worksite wellness | 3.49 | 0.91 | 0.94 | 0.76 | 0.44 | |||
| Health climate | 3.88 | 0.82 | 0.89 | 0.44 | ||||
| Participatory health behaviors | 3.54 | 0.88 | 0.93 |
p < 0.0001 for all
Cronbach’s Alpha along the diagonal
Descriptive Statistics and Bivariate Relationships
Table 2 summarizes the relationship between safety-specific indicators and health-specific indicators. Perceived leadership commitment to safety had the lowest mean score (mean = 3.68, SD = 0.84) among the safety-specific indicators. Safety climate had a mean of 3.83 (SD = 0.79) and participatory safety behaviors had a mean of 3.81 (SD = 0.77). As with the safety indicators, perceived leadership commitment to worksite wellness had the lowest mean score among the health-specific indicators (mean = 3.49, SD = 0.91). The mean score for health climate was 3.88 (SD = 0.82) and participatory health behaviors had a mean of 3.54 (SD = 0.88).
Perceived leadership commitment to safety was positively correlated with safety climate (r = 0.77) and with participatory safety behaviors (r = 0.51). Perceived leadership commitment to worksite wellness was positively correlated with health climate (r = 0.76) and participatory health behaviors (r = 0.44). The safety-focused and health-focused constructs were also positively correlated, albeit weakly in some cases. For example, participatory health behaviors had a somewhat weak correlation with leadership commitment to safety (r = 0.38) and safety climate (r = 0.35).
Linear Regression Results
Safety-Specific Indicators.
In both the unadjusted (not shown) and adjusted linear regression models, perceived leadership commitment to safety was significantly associated with safety climate and employee participatory safety behaviors (p < 0.001 for all), supporting Hypothesis 1. In the adjusted model, for each one-point increase in perceived leadership commitment to safety, safety climate was 0.67 points higher (95% CI: 0.63–0.71) and safety behaviors were 0.38 points higher (95% CI: 0.34–0.42) on a scale of 1 to 5. (Table 3).
Table 3.
Adjusted Linear Mixed Model Regression Results. N = 1,271
| Model 1: Safety Climate | Model 3: Health Climate | ||||||
|---|---|---|---|---|---|---|---|
| β Estimate | 95% CI | p-value | β Estimate | 95% CI | p-value | ||
| Leadership commitment to safety | 0.67 | (0.63, 0.71) | <0.001 | Leadership commitment to worksite wellness | 0.66 | (0.63, 0.70) | <0.001 |
| Model 2: Participatory Safety Behaviors | Model 4: Participatory Health Behaviors | ||||||
| β Estimate | 95% CI | p-value | β Estimate | 95% CI | p-value | ||
| Leadership commitment to safety | 0.45 | (0.41, 0.50) | <0.001 | Leadership commitment to worksite wellness | 0.42 | (0.37, 0.47) | <0.001 |
All models were adjusted for industry, region, business size, age, gender, job level, and job tenure
Health-Specific Indicators.
As with perceived leadership commitment to safety, in both the unadjusted (not shown) and adjusted linear regression models, perceived leadership commitment to worksite wellness was significantly associated with health climate and employee participatory health behaviors (p < 0.001 for all), supporting Hypothesis 2. In the adjusted model, for each one-point increase in perceived leadership commitment to worksite wellness, health climate was 0.66 points higher (95% CI: 0.63–0.70), and health behaviors were 0.42 points higher (0.37–0.47) on a scale of 1 to 5 (Table 3).
Effect of Organization Size
Safety-Specific Indicators.
We observed no effect of business size on the hypothesized relationships. Figure 1a shows that regardless of size across the range of small businesses, there is a positive association between perceived leadership commitment to safety and safety climate. Figure 1b shows that regardless of size, there is a positive association between perceived leadership commitment to safety and participatory safety behaviors. An F-test indicated that there was a statistically significant effect of business size as a moderator of the relationship between perceived leadership commitment to safety and participatory safety behaviors (see Table 3, Supplemental Digital Content 3). Specifically, amongst organizations with 11–50 employees, perceived leadership commitment to safety had greater impact on safety climate compared to larger organizations (201–499 employees). However, upon observation of Figure 1b, the practical difference in this relationship by size of organization is negligible.
Figure 1:
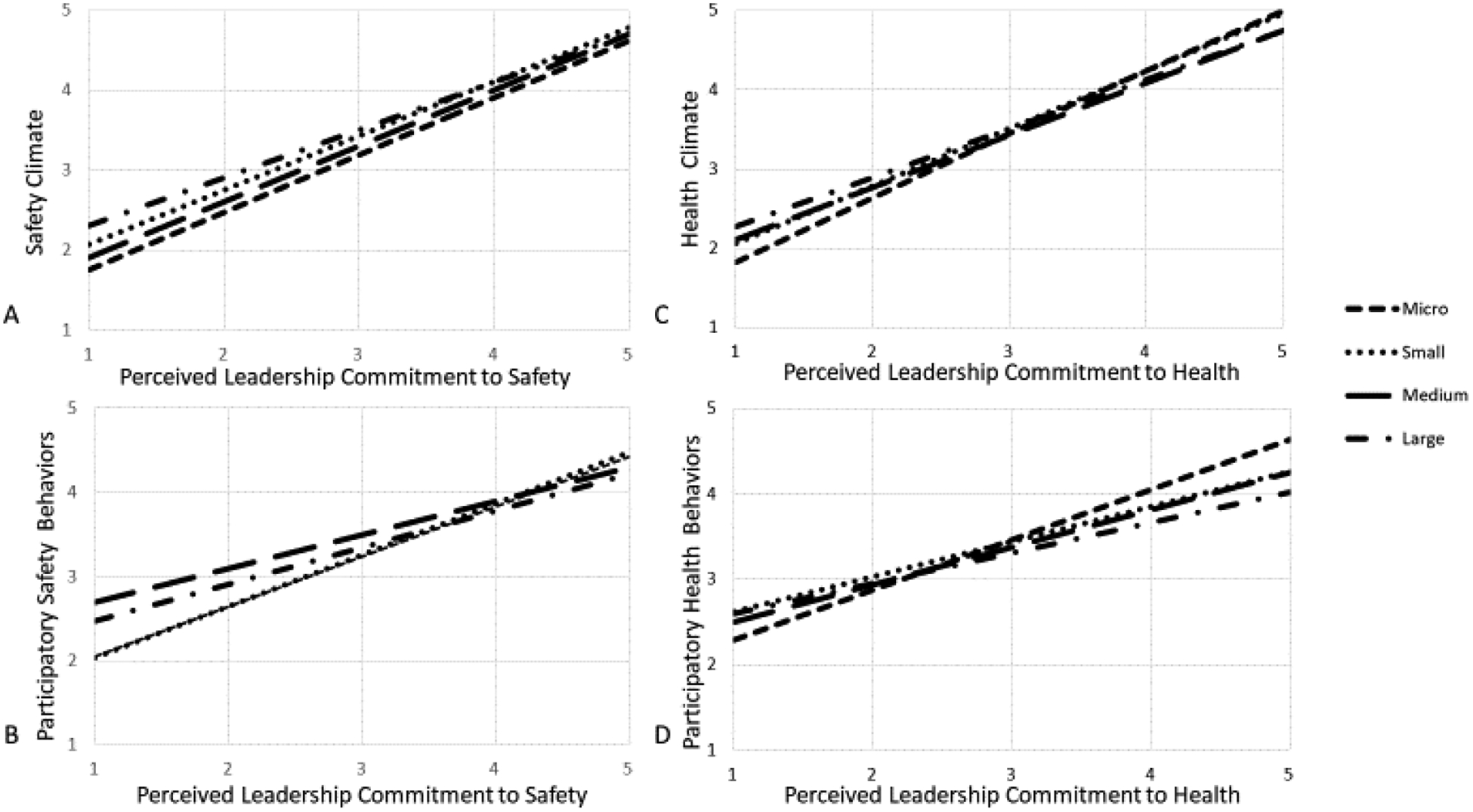
The relationship between safety specific and health specific constructs by size of small organization.
All scales are a 1 to 5 Likert scale where 1 = worst and 5 = best.
Note: Some of the lines may be hidden behind other lines due to overlapping trajectories.
Health-Specific Indicators.
We observed no effect of organization size on the relationship between perceived leadership commitment to worksite wellness and health climate (Figure 1c and Table 3, Supplemental Digital Content 3), nor did we observe an effect of organization size on the relationship between perceived leadership commitment to worksite wellness and participatory health behaviors (Figure 1d and Table 3, Supplemental Digital Content 3).
Discussion:
In this study, employee perceptions of leadership commitment to both safety and worksite wellness proved to be key components in identifying the work climate as being supportive of safety and health. Leadership commitment was also associated with proactive participation in safety and worksite wellness initiatives amongst employees. Specifically, we observed that those with higher perceived leadership commitment to safety reported a better safety climate and reported higher levels of participatory safety behaviors. Similarly, we saw that employees who reported higher levels of perceived leadership commitment to worksite wellness also reported a better health climate and higher levels of participation in worksite wellness activities. None of these associations differed meaningfully by the size of the organization. These findings suggest that small businesses of any size can benefit from leadership that displays commitment to safety and health.
Our findings that perceived leadership commitment to safety was associated with safety climate and participatory safety behaviors are consistent with the previous literature (1, 6, 7, 9, 10, 15, 17, 18, 29). These findings stress the importance of having leadership that values safety and makes it known to their employees. As a further contribution to this literature, we also observed the importance of leadership on health climate and health behaviors in small organizations. When employees feel that their leadership cares about their personal health, they are more likely perceive a positive health climate and actively participate in worksite wellness programs. This is consistent with previous studies that demonstrated the impact of leadership on participation in workplace health promotion programs (21, 22). This illustrates that leaders can play an instrumental role in creating a work environment that encourages employees to make healthy decisions. In order to truly assess the impact of leadership on safety and health climates and participatory safety and health behaviors, these associations should be assessed prospectively. Few studies have done this. One study that prospectively focused on safety found that one of the most important predictors of future injury was management commitment to safety (30).
This study allowed us to observe multiple facets of TWH policies and strategies and their associations across the entire workplace environment. Although we and other researchers have found that safety and health measures are conceptually distinct (5), we find that they are still somewhat correlated with one another. This indicates the importance of leadership in creating an environment that is supportive of employee health, safety and well-being and supports the implementation of a coordinated TWH approach to workplace safety and health (31, 32). Future research should test these relationships using a prospective design. Researchers should also begin to consider how leadership commitment to safety and to worksite wellness can be integrated to influence TWH outcomes (33).
We contribute to the TWH small organization literature by demonstrating that these relationships remain significant regardless of how small organization is defined. Numerous studies demonstrate a lack of research in TWH amongst small organizations and for those conducted, TWH in practice is usually less comprehensive in small organizations compared to large ones. (2, 34–37). Indeed, our own research with small organizations shows that organizations with more employees tend to have more TWH policies and programs (4). However, our present study demonstrates that the relationship between leadership and climate, and between leadership and proactive employee behaviors hold regardless of size of small organization. It suggests that interventions to improve leadership practices that support employees’ total health, safety, and well-being can be applied regardless of small organization size.
Future intervention research
There is limited intervention research on the relationship between leadership and TWH outcomes. Leadership support, like being visible and open to interactions with staff, is critical to the success of safety, health and well-being initiatives (38). One qualitative study demonstrated that small organization senior leaders value health, safety, and well-being at work because of its perceived benefits to meeting their business objectives. On the other hand, they rarely spoke about their leadership role in TWH from the perspective of the benefit to employees or benefit for improving their own behaviors (39). This suggests a need for TWH leadership interventions that help small organization leaders understand their role and their employee’s perspective in creating a healthy and safe work environment.
Strengths and limitations:
This study has several strengths. First, unlike some previous TWH-organization assessments that have primarily focused on organization policies and practices, we focused on the workers’ perspective (33) which, according to Punnett et al., is a critical component of the TWH framework (40). We studied a large and varied sample, consisting of 1,271 employees from 53 small organizations across a range of industries, improving generalizability. More studies that examine a range of industries and organization types in other regions are warranted to more firmly establish the generalizability these observations. Importantly, we used validated scales to measure the organizational, safety, and health environments. Finally, our study was designed to test components of a specific theoretical framework (3, 41). By using the TWH framework to learn about multiple facets of the organization, we are addressing calls to understand the organization as a whole by assessing multiple climates in conjunction with one another, as Schneider suggests in his review of organizational climate and culture (1).
This study has several limitations. First, the data were self-reported, which could bias the results as survey respondents might answer surveys in a way that makes them or their organization look as favorable as possible (42). Second, the organizations participating in the SSWell study may be more highly motivated to improve the health, safety, and well-being of their employees, so the results may not be generalizable to all small organizations. Third, it is a cross-sectional study, so assumptions of causality cannot be determined.
Conclusions:
Regardless of the size of small organization, our study shows that the perception of leadership is related to workplace safety and health climates and to proactive employee behaviors. This study reinforced the role leaders play in fostering a positive safety climate and encouraging proactive safety behaviors at work. This study adds to the literature by demonstrating the importance of leadership in also fostering a positive health climate and proactive employee participation in worksite wellness programs. Further prospective and intervention research is needed to fully understand the impact of leadership on creating a workplace culture that is supportive of worker health, safety, and well-being.
Supplementary Material
Acknowledgments
This publication was supported by the Cooperative Agreement number, 1 U19 OH 011227, funded by the Centers for Disease Control and Prevention/National Institute for Occupational Safety and Health. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention or the Department of Health and Human Services.
Footnotes
COI: none declared
References
- 1.Schneider B, González-Romá V, Ostroff C, West MA. Organizational climate and culture: Reflections on the history of the constructs in the Journal of Applied Psychology. Journal of Applied Psychology. 2017;102:468–482. [DOI] [PubMed] [Google Scholar]
- 2.Cunningham TR, Sinclair R, Schulte P. Better understanding the small business construct to advance research on delivering workplace health and safety. Small Enterprise Research. 2014;21:148–160. [Google Scholar]
- 3.Schwatka NV, Tenney L, Dally MJ, et al. Small Business Total Worker Health: a Conceptual and Methodological Approach to Facilitating Organizational Change. Occupational Health Science. 2018;2:25–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Tenney L, Fan W, Dally M, et al. Health Links Assessment of Total Worker Health(R) Practices as Indicators of Organizational Behavior in Small Business. J Occup Environ Med. 2019;61:623–634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sawhney G, Sinclair RR, Cox AR, Munc AH, Sliter MT. One Climate or Many: Examining the Structural Distinctiveness of Safety, Health, and Stress Prevention Climate Measures. J Occup Environ Med. 2018;60:1015–1025. [DOI] [PubMed] [Google Scholar]
- 6.Hofmann DA, Burke MJ, Zohar D. 100 years of occupational safety research: From basic protections and work analysis to a multilevel view of workplace safety and risk. The Journal of applied psychology. 2017;102:375–388. [DOI] [PubMed] [Google Scholar]
- 7.Zohar D. Thirty years of safety climate research: Reflections and future directions. Accident Analysis & Prevention. 2010;42:1517–1522. [DOI] [PubMed] [Google Scholar]
- 8.Clarke S. Safety leadership: A meta‐analytic review of transformational and transactional leadership styles as antecedents of safety behaviours. Journal of Occupational and Organizational Psychology. 2013;86:22–49. [Google Scholar]
- 9.Hystad SW, Bartone PT, Eid J. Positive organizational behavior and safety in the offshore oil industry: Exploring the determinants of positive safety climate. The journal of positive psychology. 2014;9:42–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.McCaughey D, Halbesleben JR, Savage GT, Simons T, McGhan GE. Safety leadership: extending workplace safety climate best practices across health care workforces. Advances in health care management. 2013;14:189–217. [DOI] [PubMed] [Google Scholar]
- 11.Clarke S, Taylor I. Reducing workplace accidents through the use of leadership interventions: A quasi-experimental field study. Accid Anal Prev. 2018;121:314–320. [DOI] [PubMed] [Google Scholar]
- 12.Shen Y, Ju C, Koh TY, Rowlinson S, Bridge AJ. The Impact of Transformational Leadership on Safety Climate and Individual Safety Behavior on Construction Sites. Int J Environ Res Public Health. 2017;14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Goldenhar LM, Ruder AM, Ewers LM, Earnest S, Haag WM, Petersen MR. Concerns of a Dry-Cleaning Industry: A Qualitative Investigation of Labor Management. American journal of industrial medicine. 1999;35:112–123. [DOI] [PubMed] [Google Scholar]
- 14.Inness M, Turner N, Barling J, Stride CB. Transformational leadership and employee safety performance: A within-person, between-jobs design. Journal of Occupational Health Psychology. 2010;15:279–290. [DOI] [PubMed] [Google Scholar]
- 15..Griffin MA, Neal A. Perceptions of safety at work: a framework for linking safety climate to safety performance, knowledge, and motivation. Journal of occupational health psychology. 2000;5:347–358. [DOI] [PubMed] [Google Scholar]
- 16.Zweber ZM, Henning RA, Magley VJ. A practical scale for Multi-Faceted Organizational Health Climate Assessment. J Occup Health Psychol. 2016;21:250–259. [DOI] [PubMed] [Google Scholar]
- 17.Neal A, Griffin MA. A study of the lagged relationships among safety climate, safety motivation, safety behavior, and accidents at the individual and group levels. Journal of applied psychology. 2006;91:946–953. [DOI] [PubMed] [Google Scholar]
- 18.Christian MS, Bradley JC, Wallace JC, Burke MJ. Workplace safety: a meta-analysis of the roles of person and situation factors. Journal of Applied Psychology. 2009;94:1103–1127. [DOI] [PubMed] [Google Scholar]
- 19.Montano D. Supervisor behaviour and its associations with employees’ health in Europe. International archives of occupational and environmental health. 2016;89:289–298. [DOI] [PubMed] [Google Scholar]
- 20.Schmidt B, Loerbroks A, Herr RM, et al. Associations between supportive leadership and employees self-rated health in an occupational sample. International journal of behavioral medicine. 2014;21:750–756. [DOI] [PubMed] [Google Scholar]
- 21.Lier LM, Breuer C, Dallmeyer S. Organizational-level determinants of participation in workplace health promotion programs: a cross-company study. BMC Public Health. 2019;19:268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kaspin LC, Gorman KM, Miller RM. Systematic review of employer-sponsored wellness strategies and their economic and health-related outcomes. Population health management. 2013;16:14–21. [DOI] [PubMed] [Google Scholar]
- 23.Skarholt K, Blix EH, Sandsund M, Andersen TK. Health promoting leadership practices in four Norwegian industries. Health promotion international. 2016;31:936–945. [DOI] [PubMed] [Google Scholar]
- 24.Kotey B, Slade P. Formal Human resource management practices in small growing firms. Journal of Small Business Management. 2005;43:16–40 [Google Scholar]
- 25.Saridakis G, Torres RM, Johnstone S. Do human resource practices enhance organizational commitment in SMEs with low employee satisfaction? British Journal of Management. 2013; 24:445–458 [Google Scholar]
- 26.Eakin JM. Leaving it up to the workers: sociological perspective on the management of health and safety insmall workplaces. International journal of health services. 1992;22:689–704. [DOI] [PubMed] [Google Scholar]
- 27.Guo BHW, Yiu TW, Gonzalez VA. Does company size matter? Validation of an integrative model of safety behavior across small and large construction companies. Journal of safety research. 2018;64:73–81. [DOI] [PubMed] [Google Scholar]
- 28.Lee J, Huang YH, Robertson MM, Murphy LA, Garabet A, Chang WR. External validity of a generic safety climate scale for lone workers across different industries and companies. Accid Anal Prev. 2014;63:138–145. [DOI] [PubMed] [Google Scholar]
- 29.Neal A, Griffin MA, Hart PM. The impact of organizational climate on safety climate and individual behavior. Safety Science. 2000;34:99–109. [Google Scholar]
- 30.Beus JM, Payne SC, Bergman ME, Arthur W Jr. Safety climate and injuries: an examination of theoretical and empirical relationships. Journal of applied psychology. 2010;95:713–727. [DOI] [PubMed] [Google Scholar]
- 31.Tamers SL, Chosewood LC, Childress A, Hudson H, Nigam J, Chang C-C. Total Worker Health® 2014⁻2018: The Novel Approach to Worker Safety, Health, and Well-Being Evolves. International journal of environmental research and public health. 2019;16:321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Barbeau EM, Goetzel RZ, Lakdawalla D, Reville RT, Seabury SA, Sorensen G. Research compendium; the NIOSH Total Worker Health Program: seminal research papers 2012. 2012.
- 33.Sorensen G, Sparer E, Williams JAR, et al. Measuring Best Practices for Workplace Safety, Health, and Well-Being: The Workplace Integrated Safety and Health Assessment. J Occup Environ Med. 2018;60:430–439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Rohlman DS, Campo S, Hall J, Robinson EL, Kelly KM. What Could Total Worker Health® Look Like in Small Enterprises? Annals of work exposures and health. 2018;62:S34–s41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Merchant JA, Lind DP, Kelly KM, Hall JL. An employee total health management-based survey of Iowa employers. J Occup Environ Med. 2013;55:S73–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Sinclair RC, Cunningham TR. Safety activities in small businesses. Safety science. 2014;64:32–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Sinclair RC, Cunningham TR, Schulte PA. A model for occupational safety and health intervention diffusion to small businesses. American journal of industrial medicine. 2013;56:1442–1451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Kelloway EK, Barling J. Leadership development as an intervention in occupational health psychology. Work & Stress. 2010;24:260–279. [Google Scholar]
- 39.Thompson J, Schwatka N, Tenney L, Newman L. Total Worker Health: A Small Business Leader Perspective. International journal of environmental research and public health. 2018;15:2416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Punnett L, Warren N, Henning R, Nobrega S, Cherniack M, team C-Nr. Participatory ergonomics as a model for integrated programs to prevent chronic disease. Journal of Occupational and Environmental Medicine. 2013;55:S19–S24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Anger WK, Elliot DL, Bodner T, et al. Effectiveness of total worker health interventions. J Occup Health Psychol. 2015;20:226–247. [DOI] [PubMed] [Google Scholar]
- 42.Donaldson SI, Grant-Vallone EJ. Understanding Self-Report Bias in Organizational Behavior Research. Journal of Business and Psychology. 2002;17:245–260. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.