

Abstract
Gender inequality in science, medicine, and dentistry remains a central concern for the biomedical research workforce today. Although progress in areas of inclusivity and gender diversity was reported, growth has been slow. Women still face multiple challenges in reaching higher ranks and leadership positions while maintaining holistic success in these fields. Within dental research and academia, we might observe trends toward a more balanced pipeline. However, women continue to face barriers in seeking leadership roles and achieving economic equity and scholarship recognition. In an effort to evaluate the status of women in dental research and academia, the authors examined the role of the International Association for Dental Research (IADR), a global research organization, which has improved awareness on gender inequality. The goal of this article is to review five crucial issues of gender inequality in oral health research and academics—workforce pipeline, economic inequality, workplace harassment, gender bias in scholarly productivity, and work-life balance—and to discuss proactive steps that the IADR has taken to promote gender equality. Providing networking and training opportunities through effective mentoring and coaching for women researchers, the IADR has developed a robust pipeline of women leaders while promoting gender equality for women in dental academia through a culture shift. As knowledge gaps remained on the levels of conscious and unconscious bias and sexist culture affecting women advancement in academics, as well as the intersectionality of gender with race, gender identity, ability status, sexual orientation, and cultural backgrounds, the IADR has recognized that further research is warranted.
Keywords: gender equality, empowerment, economic inequality, work-life balance, workplace harassment, gender bias
Introduction
Throughout centuries and against all the odds, women have overcome professional and societal barriers to advance science. As early as the 19th century, women in male-dominated medicine and dentistry frequently aligned with feminist and suffrage movements breaking barriers and stereotypes in the work environment and demanding equality (Moore 2018). Following World War II, the United Nations (UN) Commission on the Status of Women (CSW) aimed to globally promote women’s rights as human rights. In 1952, the CSW drafted resolution 640 (VII) to recognize and protect the political rights of women, which was then adopted by the UN. In parallel, the CSW worked with the International Labor Organization for the first convention on the principle of equal pay for equal work (International Labour Office 1951). It was not until 1967 that the Convention on the Elimination of All Forms of Discrimination against Women was adopted by the UN General Assembly and ratified by nearly all UN member states, except the United States, Iran, Somalia, Sudan, Palau, Tonga, and Niue (UN 1979). In the United States, during the second wave of feminism, women fought for equality in education, pay, and career advancement while winning legislative recognition with Title IX of the Education Act Amendment (1972), the Equal Opportunity Act (1972), and the Equal Pay Act (1963).
The European Union (EU) implemented a directive for the approximation of member state laws on the principles of equal pay for men and women almost 50 years ago. Given the persistent variability in legal frameworks in the member states, the EU amended this directive to clarify on the principles for equal opportunities and treatment of men and women in matters of employment and occupation (European Commission 2015a; European Parliament 2006). In addition, the European Institute for Gender Equality, in its pursuit of gender equality, provided support for research designed to inform key policy makers and stakeholders about gender inequality (European Institute for Gender Equality 2018). With increasing women participation in the scientific workforce, additional discriminatory challenges appeared requiring further protections (McDonald 2011). Among these protections, the US Equal Opportunity Act specifically included sexual harassment as a violation of Title VII of the Civil Rights Act and offered legal protection to women victims. In the United Kingdom, Ireland, and Australia, the Athena Swan initiative has supported gender equality for women in science and has recognized the good practices of higher education institutions (Ovseiko et al. 2017). Gender equity is named goal 5 out of the 17 Sustainable Development Goals for 2030 (UN 2018). Despite these successful societal interventions, professions with a history of persistent male dominance continue to face challenges.
In this article, we aim to present initiatives of the International Association for Dental Research (IADR) in 5 crucial areas that affect gender equality in all aspects of craniofacial, oral, and dental science.
The Pipeline in Oral Health Research: Is It Still Leaking?
Since the US initiative on equality in science (Women in Science and Technology Equal Opportunity Act of 1979–1980) and the corresponding EU initiative (European Commission 1999), there have been efforts to feed the science pipeline with programs designed to increase women participation in the science, technology, engineering, and math (STEM) fields. Consequently, the most recent report of the Council for Graduate Studies (Okahana 2018) showed that women earn the majority of graduate certificates (64.0%), master’s degrees (57.3%), and doctoral degrees awarded by US institutions (53.0%; Okahana 2018). However, explicit and implicit bias is shown to affect their career advancement and result in low representation in senior ranks (National Research Council 2007).
Specifically, in oral sciences, survey research (between 1994 and 2015) revealed that 54% of the PhD graduates were women, who more frequently pursued postgraduate studies as compared with men (Herzog et al. 2018). Interestingly, among PhD graduates approximately only 35% entered US academics while 11% were employed in industry or government agencies. However, these career choices are not static. Academia has traditionally served as a source for C-suite executives in the oral care industry. Despite the numerous hurdles that obstruct entry into the biotechnology and pharmaceutical industries, the number of women in leadership roles is steadily increasing in this sector. This is likely due to an increasing number of women pursuing STEM and business education opportunities in the health care space. While it is estimated that about 7% to 9% of chief executive officer roles are filled by women in biotechnology, only 4.2% of CEO positions (chief executive officer) are led by female CEOs in the Fortune 500 (“These Are the Women” 2017). These data appear to be counterintuitive, as a significant number of positions in the health care industry are held by women. Over 76% of hospital employees and employees in doctors’ offices and 88% of home health care workers are women (US Bureau of Labor Statistics 2019). Despite this representation in the industry, key decision makers are typically men. Health care, unlike other industries, does not have a “women in health care” problem but a “women in health care leadership” problem (Stone et al. 2018). As women continue to break through the industrial glass ceiling and create networks fostering diversity in leadership positions, their presence is recognized as a critical force to propel translational science and innovation in oral care.
The recent report Gender in the Global Research Landscape examined gender diversity in the United States, Europe, and Asia-Pacific region and determined the factors shaping the disparities in STEM (Allagnat et al. 2017). When narrowing the analysis to dental research, the report showed that within the last 20 years the involvement of women in dental research increased at a varied rate in different countries, ranging from ~26% in Japan to 55% in Brazil (Allagnat et al. 2017). In the United States, the report showed that women scientists steadily represent 35% of dental researchers, similar to the reported frequency of National Institutes of Health (NIH) R01-type research awards to women dentist-scientists (D’Souza et al. 2017). Notable change happened in Portugal, where systematic public policy efforts on gender equity resulted in a 38% increase of women in dental research (Allagnat et al. 2017). For the purpose of this article, these data on women participation in dental research (2010–2015; Allagnat et al. 2017) were examined in relation to the Global Gender Gap Index (GGGI) per country as calculated by World Economic Forum–based average indicators of equality on 4 critical pillars: economic participation and opportunity, educational attainment, health and survival, and political empowerment (Schwab et al. 2016). Once the final scores were calculated, they ranged between 1, which signified parity, and 0, which signified inequality (Schwab et al. 2016). Although the GGGI report recognized successful initiatives, which closed approximately 96% of the health and educational gap, the economic and political disparity remains problematic (Schwab et al. 2016). Specifically, the GGGI report highlighted that only 59% and 23% of the economic and political gender gaps have been closed, respectively, with just 5 countries showing >30% women participation in economic leadership roles (Iceland, Norway, France, Latvia, and Finland; Schwab et al. 2016). On the other end of the scale, the Middle East and North African countries present wide gender gaps in both economic participation and educational attainment, leading to several societal, cultural, and economic barriers for women (Schwab et al. 2016). We conducted an exploratory analysis with a nonparametric statistical approach (Spearman testing) that recognizes the lack of normality in the variable distribution while assessing the correlation between women participation in dental research (percentage variables as reported by Allagnat et al. 2017) and the GGGI. Figure 1 presents the negative but not statistically significant correlation (r = −0.10, P = 0.38) between the GGGI and the representation of women in dental research in the selected countries, highlighting the paradox in this relationship with women in countries with gender parity showing lower dental research representation. This analysis is in agreement with recent evidence of the paradoxical relationship of small gender gaps and large STEM gender participation gaps (Stoet and Geary 2018). These data emphasized that federal- and state-level policies are necessary but not enough. To close the gender gaps, more substantial culture shifts would need to occur.
Figure 1.
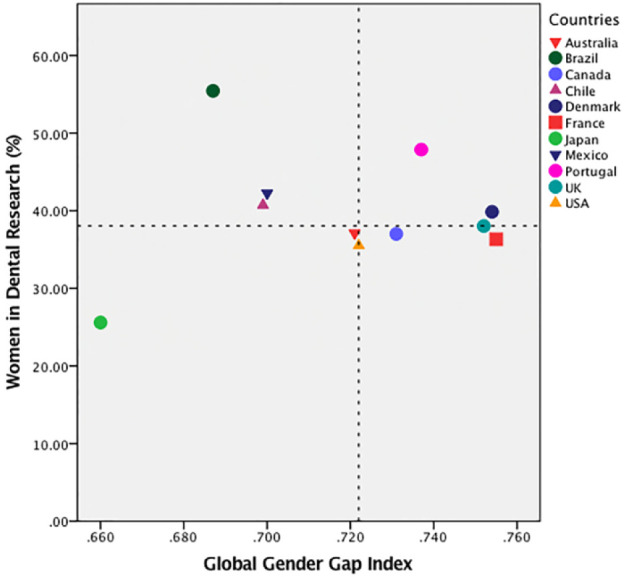
Women participation in dental research based on Gender in the Global Research Landscape (Allagnat et al. 2017) in relation to the Global Gender Gap Index (GGGI) per country. The interrupted lines represent the median values in the x- and y-axes. The upper-right quadrant represents countries with a high GGGI and more women in dental research as compared with the lower-left quadrant, which represents countries with a low GGGI and fewer women in dental research.
Role of the IADR
The IADR has witnessed a significant expansion in membership globally with the growth of several programs and initiatives central to the IADR’s mission and of high impact in the dental and broader biomedical research communities. The IADR membership is divided into 5 regions. In 2015, North America had the largest share of members (36%), followed by Asia/Pacific (26%), Pan European (18%), Latin America (14%), and Africa/Middle East (7%). The overall women representation in these regions increased from 2005 to 2015 (Fig. 2A).
Figure 2.

Women representation in the IADR over the years. (A) Women representation stratified by IADR region. Number of women and men: (B) IADR members and (C) IADR presidents (1920 to 2020). Presidents are elected in a 1-year term. IADR, International Association for Dental Research.
The Latin American region has contributed 14% of IADR members, with women representing 62% of those members. Africa/Middle East has contributed impressively to women representation (49%) relative to the total number of IADR members. The Asia/Pacific region has made significant progress with women representation increasing from 25% to 35% from 2005 to 2015. Women representation from the Pan European region has increased from 33% to 43% within the last decade and from North America from 32% to 39% (Fig. 2A). In addition, the overall gender stratification of the IADR has changed between 2005 and 2015, with women representation increasing by about 10% and the gap between men and women members decreasing (57.5% vs. 42.5%; Fig. 2B). Specific comparisons among professional organizations in dentistry are presented in this issue (Li et al. 2019).
There has been enormous change in the gender composition in the IADR leadership in the 98 years since its inception. For the first 60 years of the IADR, there had been no women presidents. In contrary to the “misteria” (irrational fear that advancing women mean catastrophic lack of opportunity for men; Choo et al. 2018) that characterizes other organizations, the IADR has taken alternative routes. Since 1980, a dramatic increase in women presidents was observed (Shaddox and Letra 2019), with about a third (28%) of the IADR presidents being women (Fig. 2C). Recently, 4 consecutive presidents were women (2010 to 2014), and currently, the president, president-elect, and vice president are women. Throughout the last 30 years, gender diversity in IADR leadership has shaped the organization’s priorities, with equal opportunity programs that provide avenues for mentoring and increasing women’s visibility in research, academia, and leadership. With its annual career development workshops, experts assist the members with skill building, resilience training, and career advice.
The IADR and its regional divisions play a vital role in developing a pipeline of researchers by engaging dental students in research and leadership. The National Student Research Group (NSRG), which is part of the American division (American Association for Dental Research [AADR]), fosters an environment to encourage students early on to engage in research and to provide a platform for women students to develop leadership skills. Since the inception of the NSRG in 1982, 17 women (47%) have served as NSRG presidents (AADR 2018).
An important IADR initiative on gender equality was the development of the Women in Science Network (WISN). The WISN has been empowering women IADR members with the goal to change the culture in dental research and achieve gender parity in the research workforce. WISN membership has more than quadrupled since its conception, maintaining a high membership of women trainees (Fig. 3). In an effort to actively support women researchers, the IADR WISN recently established 2 awards recognizing women mentors/role models (IADR WISN 2015b) and young women scientists (AADR Anne Haffajee Fellowship; AADR 2014). Since its inception, the WISN has promoted initiatives in the areas of economic equality, harassment, scholarly bias, work-life policies, and women’s rights. Furthermore, the WISN has been regularly conducting symposia on current gender inequalities as well as other forums to bring together women role models from diverse dental research fields to share their academic journeys and career pathways to encourage and motivate younger women faculty and researchers toward navigating their own paths to success (IADR WISN 2015a, 2016a, 2017b).
Figure 3.
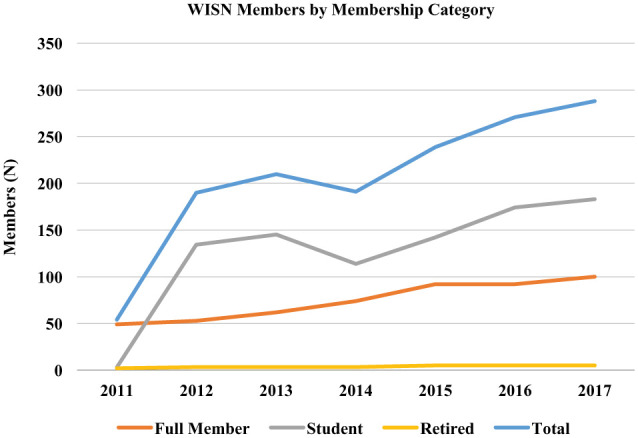
Number of WISN members stratified by membership category. WISN, Women in Science Network.
Economic Inequality
There is convincing evidence that gender-based salary inequities exist globally and constitute a universal threat in society. Indeed, the Global Gender Gap Report found that true economic parity has not been achieved anywhere in the world (Schwab et al. 2016). While it is encouraging that countries such as Slovenia, Norway, and Sweden are approaching parity, Bahrain, United Arab Emirates, and Saudi Arabia present a >50% income gap between genders. In the United States, women are paid on average 80% of men earnings with variability among ethnic groups. African American, Native American, and Hispanic women have lower median annual earnings as compared with White non-Hispanic and Asian women (American Association of University Women 2018). In the EU, the average wage gap among member states is 16.4%, although the pension gap is even wider (39%; American Association of University Women 2018). The income gap strikingly varies among member states, ranging from 6% in Slovenia to 31% in the United Kingdom (European Commission 2015b). Factors affecting this economic inequality include social stereotypes and expectations, which systematically promote women’s role as caregivers and lead to parenting inequality, unaffordable childcare, and a hostile work environment, which frequently discriminates women. As a result, women are largely responsible for all unpaid domestic work, including caregiving and household, which was found to be disproportionally shared by women in the health professions as well (Jolly et al. 2014). The persistent pay gap and the limited representation of women in leadership created an environment of inequality, an issue that the scientific community has been relatively complacent about. Economic inequality has been linked to a workplace power imbalance, which, when combined with unconscious and conscious biases and microaggressions, leads to sexual and other forms of harassment (Lennard 2017).
Role of the IADR
A persistent earnings gap is evident between men and women in academia (more pronounced in higher ranks) (Ioannidou et al. 2014) as well as in the private sector (IADR WISN 2016b, 2017a; Jagsi, Biga, et al. 2016; Nguyen Le et al. 2017).
The WISN conducted salary negotiation workshops at IADR meetings in 2016 and 2017, in collaboration with the American Association of University Women. The Work Smart Workshop was adapted for the dental and craniofacial research community with trained facilitators for effective salary negotiation (IADR WISN 2016b, 2017a). The workshops improved the participants’ understanding on topics such as the pay gap, ways to benchmark a salary, target salary estimation, strategies for a raise or promotion request, negotiation of a start-up and benefits package, persuasive responses during negotiations, and role-play on salary negotiation. A total of 50 individuals (including men and women) participated in both workshops and represented several countries, including the United States, United Kingdom, Russia, Canada, China, Malaysia, and the Netherlands. Seventy-nine percent of the participants were employed as faculty, and 17% were students. About 46% of the participants belonged to ethnic minority groups (Fig. 4). Following the workshop experience, 91% of the participants felt “extremely likely to implement ideas and concepts they learned in the workshop,” and 70% felt that the workshop attendance had a high impact in their ability to negotiate salary. These pilot results revealed the positive feedback on the workshop initiative, which provides a framework for generating new hypotheses for implementation research in the field.
Figure 4.

Demographic characteristics of WISN salary negotiation workshop participants (2016 and 2017). “Work Smart: Salary Negotiation and Promotion in Dental Academia” was presented at the 2016 AADR/CADR General Session, Los Angeles, CA. “Salary Negotiations and Promotion in Dental Academia” was presented at the 2017 IADR/AADR/CADR General Session, San Francisco, CA. AADR, American Association for Dental Research; CADR, Canadian Association for Dental Research; IADR, International Association for Dental Research; WISN, Women in Science Network.
Workplace Harassment
Leaks in the pipeline have been attributed to several factors, including academic climate hostility and incivility (National Research Council 2007). Sexual harassment has been implicated in the creation of a hostile academic environment. The US Equal Employment Opportunity Commission (1980) defined sexual harassment as not only unwelcome sexual advances but also offensive remarks about a person’s sex, which are “used either explicitly or implicitly [as] a term or condition of employment.” Following the legal case at Cornell University (Nemo 1975), sexual harassment was legally recognized and linked to Title VII of the Civil Rights Act as a result of the grassroots feminist movement (McDonald 2011).
In the biomedical sciences, 52% of women faculty, as compared with 5% of men, reported harassment in their careers (Jagsi, Griffith, et al. 2016). Moreover, in a recent US NIH K-award recipient survey, almost 66% of women reported some type of gender bias in their professional advancement, while 30% of them experienced sexual harassment (Jagsi, Griffith, et al. 2016). In dental institutions, 30% of the women dental faculty, as opposed to 9.3% of men, expressed that the work environment was less supportive to women than men. In dental academics, one-third of women faculty, as compared with 3.4% of men, were sexually harassed by a superior or colleague (Nesbitt et al. 2003).
Following the National Science Foundation and NIH recommendations on workplace harassment (NIH 2015; National Science Foundation 2018), scientific organizations and publishers have revised harassment prevention practices with the goal to create a safe, civil, and productive scientific environment, advocating for a “no tolerance” policy (American Association for the Advancement of Science 2015; Bates et al. 2018). Notably, women have overcome major personal and institutional barriers to break their silence with the #MeToo campaign in various industries, including medicine and dentistry (Jagsi 2018).
Role of the IADR
The IADR has been proactive in following these recommendations and developing policies with a theme of nondiscrimination and promotion of diversity and inclusivity.
The IADR has taken the following significant actions on this issue: 1) In close collaboration with the WISN, the IADR and the AADR have established a new professional behavioral policy (IADR 2017), which defines norms and expectations for acceptable behavior at annual meetings. The policy states that the “IADR is committed to providing a friendly, safe and welcoming environment for all, regardless of gender, sexual orientation, ability, ethnicity, socioeconomic status or religion.” 2) The IADR has supported symposia on sexual harassment prevalence, practices, and policies in oral health institutions at its annual meetings (IADR WISN 2018b). 3) The AADR Board of Directors has approved the use of the Sexual Experience Questionnaire, developed by the US Department of Defense (Fitzgerald et al. 1999) and used in other organizations, to assess sexual harassment experiences at its annual meetings.
Gender Bias in Scholarly Productivity
Throughout the centuries, peer review has followed a slow evolutionary process sustaining a traditional, unstandardized, and voluntary model characterized by a significant lack of diversity and deep resistance to practice and policy change. For this model to adhere to the current scientific environment and needs, concrete steps, such as structural organizational changes, peer review mentoring programs, as well as measurable expectations, may warrant gender parity in scholarly publishing (Lariviere et al. 2013; West et al. 2013; Helmer et al. 2017). Consistent evidence has shown that men publish more than women in Europe, the United States, and other countries (Aiston and Jung 2015). Furthermore, the number of women dental scholars in the dental sciences remains limited (Ceci and Williams 2011; Casadevall and Handelsman 2014). In fact, women dental scholars have been found to be significantly underrepresented in the editorial boards of dental journals as well as in the position of editor in chief (Ioannidou and Rosania 2015). Furthermore, evidence has also revealed a consistent underrepresentation of women as speakers in scientific meetings (Schroeder et al. 2013; Casadevall and Handelsman 2014), where “manels” are frequently occurring (i.e., panels of speakers populated entirely by men; Choo et al. 2018).
Role of the IADR
In 2015, the WISN established an award to recognize the distinguished scholarly productivity of a woman researcher in the dental field for her first or senior author role on a peer-reviewed manuscript. At an organizational level, the IADR has acknowledged the importance of gender parity in scientific publishing. A symposium in the 2018 General Session discussed gender-based scholarly productivity and journal policies with the editors in chief of 4 highly ranked oral health journals (Journal of Dental Research, JDR Clinical and Translational Research, Dental Materials, and Clinical Oral Implant Research; IADR WISN 2018a). The goal of the symposium was to assess women participation on editorial and review boards, as well as to compare gender practices and policies among journals. Furthermore, the IADR’s 2 official journals, the Journal of Dental Research and JDR Clinical and Translational Research, have made a proactive effort to increase the participation of women in the editorial board. Specifically, JDR Clinical and Translational Research has women in both the editor in chief and associate editor positions. The IADR has made systematic efforts not to “ova-look” women researchers (i.e., when women are bypassed for an opportunity even though they are eminently qualified; Choo et al. 2018) and to address equal representation of women as presenters at annual sessions. Data on women speakers at IADR annual sessions are presented in the article in this thematic issue by Tiwari and colleagues (2019).
Work-Life Balance
Working people need a balance between work and life. National surveys have confirmed that after compensation, this balance is the most important workplace attribute. In fact, individuals who feel that they have a better work-life balance tend to work 21% harder than those who do not (Strong et al. 2013; Krueger et al. 2017). In academia, a recent work-life balance survey that included 2,379 higher education staff from 56 countries revealed that, in comparison with professional staff and their male counterparts, women academics felt more strongly that their work had a negative impact on their mental health. They also felt that having children held them back in their career development and that they bear substantially more of the child care load. In agreement with the above, a recent and extensive survey of almost 1,000 US physician mothers emphasized that the paternal discrimination in their US academic institutions affected their medical training and practice (Halley et al. 2018).
With the gradual evolution of family models worldwide, the traditional family structure has been replaced by contemporary models, with both spouses working outside the home and at least 1 parent working long hours at atypical times (Organisation for Economic Co-operation and Development 2016). While many higher education and research institutes make systematic efforts to accommodate dual-career couples or single-parent families, only a third of the dental institutes have adapted to the new reality (Dannels et al. 2009). As women entered the workforce in high numbers, social stereotypes and expectations have remained strong, influencing domestic responsibilities and compromising work-life balance (Parker and Rohal 2015).
Optional delayed tenure clock for childbirth or adoption is offered in only 46% of the dental schools, and only 41% of schools provide options for child care in close proximity (Dannels et al. 2009). Even when available, such programs remain largely underutilized. Hence, there is an urgent need to actively promote a culture that allows and encourages their utilization.
Role of the IADR
The IADR as an international organization recognizes the policy disparities among countries. First, parental leave is a critical policy for working parents provided by 96% of 186 countries around the world. While the United States is the only high-income country that does not mandate paid parental leave (Earle et al. 2011), all EU member countries provide at least 14 weeks of paid parental leave (Organisation for Economic Co-operation and Development 2016). Public policy improvements have extended parental leave in the form of paternity leave in 81 countries. The IADR as a global organization with more than 10,000 members recognizes the discrepancies in policy and culture between continents and countries, when engaging in the discussion about changes in parental policy. IADR leaders frequently hold leadership positions in dental institutions worldwide and are in a position to apply these successful strategies to support women researchers in their own institutions. The IADR offers work-life support through its annual career development workshop to men and women researchers (Drake and Ioannidou 2018). Through this workshop, the IADR has recognized the different mentoring needs between genders, adopting its programs accordingly.
Knowledge Gaps: Future Research Directions
Although the IADR has made systematic efforts and implemented policies to support women, gender inequality is still present in dental and craniofacial research institutions. As recently reported, academic and research institutions have been slow to adapt to the social demand of gender equity (“Feminism Is for Everybody” 2019). The IADR has joined 53 other organizations in a new initiative focusing on advancing women’s full participation and advancement in STEMM (science, technology, engineering, mathematics, and medicine). In this consortium, member associations will support inclusion, promote no-tolerance policies on sexual harassment, and facilitate institutional transformation similarly to Athena Swan programs. Research could facilitate this change with gender-related questions and appropriate methodologies. Research should examine conscious and unconscious bias and sexist culture that affects women’s advancement in academics. Moving forward, appropriate implementation strategies should be tested with the goal to support diversity and inclusivity. Furthermore, research would need to assess the levels of sexual harassment in dental institutions and address concerns of accountability and culture shift as recommended (Bates et al. 2018).
Following initiatives by the NIH and National Science Foundation, the traditional gender binary construct simplistically describing the “man” or “woman” is not considered inclusive enough in biomedical research. The recent Institute of Medicine (2011) report The Health of Lesbian, Gay, Bisexual and Transgender People: Building a Foundation for Better Understanding provided population estimates, with 1.3% to 4.5% of women and 2.3% to 6.8% of men identifying as homosexuals. Although medical organizations such as the American Medical Association and American Association of Medical Colleges have been offering resources on policies and practices related to gender identity and sexual orientation, dental organizations lag behind. IADR researchers from different disciplines are in a position to identify gaps in knowledge related to gender-nonconforming people and/or people with different sexual orientations. Many of the themes examined in this article become more relevant when gender identity intersects with race and/or with sexual orientation.
Conclusion
This article has reviewed data on the status of women in dental research. It has showed that although there has been legislative progress supporting and securing women’s role in dental research, gender inequality is still evident in a complex political, economic, and social context. Science historians and policy scholars have reported that the systematic efforts to enhance diversity with mandated programs or quotas might not be enough to resolve gender inequality (Schiebinger 1999; Dobbin and Kalev 2017). In an effort toward “no tolerance,” it is not enough for institutions to develop policies alone. These policies need to be put into practice and outcomes assessed in a timely manner to gauge the transformative potential on institutional environments and cultures. More importantly, researchers could be actively engaged in this shift, addressing social stereotypes and cultural expectations. The next generation of dental researchers will have to be educated on gender diversity and equality. The IADR plays an indispensable role in this direction by spreading awareness of challenges faced by women researchers, creating opportunities for career advancement, and fostering transparent conversations for cultural change. As the leading global dental research organization, the IADR is setting a higher bar for questioning social stereotypes and cultural expectations and offering equal opportunities to women researchers to “aspire, achieve, participate in and contribute to” (Ginsburg 1996) dental and craniofacial research.
Author Contributions
E. Ioannidou, contributed to conception, design, and data analysis, drafted and critically revised the manuscript; A. Letra, L.M. Shaddox, F. Teles, S. Ajiboye, M. Ryan, C.H. Fox, T. Tiwari, contributed to data analysis, critically revised the manuscript; R.N. D’Souza, contributed to conception and design, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Acknowledgments
We thank the IADR Central Office staff—Denise Streszoff, associate executive director, and Erika T. Duffy, assistant manager membership benefits—for providing valuable information for this manuscript. In addition, the authors are grateful for the assistance in manuscript preparation provided by Dr. Nayanjot Rai, research associate at University of Colorado.
Footnotes
This research received support from Colgate-Palmolive, Procter & Gamble, and Denstply-Sirona.
C.H. Fox and S. Ajiboye are IADR employees. M. Ryan is the vice president and chief dental officer at Colgate-Palmolive Company. The other authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
ORCID iDs: E. Ioannidou  https://orcid.org/0000-0003-1954-5900
https://orcid.org/0000-0003-1954-5900
A. Letra
https://orcid.org/0000-0002-7197-6735
T. Tiwari
https://orcid.org/0000-0001-9334-4440
References
- Aiston S, Jung J. 2015. Women academic and research productivity: an international comparison. Gender and Education. 27(3):205–255. [Google Scholar]
- Allagnat L, Berghmans S, Falk-Krzesinski H, Hanafi S, Harbert R, Hiuggett S, Tobin S. 2017. Gender in the global research landscape. Amsterdam (Netherlands): Elsevier. [Google Scholar]
- American Association for the Advancement of Science. 2015. Annual meeting code of conduct. http://meetings.aaas.org/policies/.
- American Association for Dental Research. 2014. AADR Anne D. Haffajee Fellowship; Alexandria (VA); [accessed 2018 Feb]. http://www.iadr.org/AADR/Awards/Fellowships/Haffajee. [Google Scholar]
- American Association for Dental Research. 2018. AADR National Student Research Group; [accessed 2018 Feb]. http://www.iadr.org/AADR/Students.
- American Association of University Women. 2018. The simple truth about the gender pay gap. Washington (DC): American Association of University Women; https://www.aauw.org/research/the-simple-truth-about-the-gender-pay-gap/. [Google Scholar]
- Bates CK, Jagsi R, Gordon LK, Travis E, Chatterjee A, Gillis M, Means O, Chaudron L, Ganetzky R, Gulati M, et al. 2018. It is time for zero tolerance for sexual harassment in academic medicine. Acad Med. 93(2):163–165. [DOI] [PubMed] [Google Scholar]
- Casadevall A, Handelsman J. 2014. The presence of female conveners correlates with a higher proportion of female speakers at scientific symposia. MBio. 5(1):e00846-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ceci SJ, Williams WM. 2011. Understanding current causes of women’s underrepresentation in science. Proc Natl Acad Sci U S A. 108(8):3157–3162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Choo EK, DeMayo RF. Glaucomflecken. 2018. A lexicon for gender bias in academia and medicine. BMJ. 363:k5218. [Google Scholar]
- Commission on the Status of Women. 1952. Convention on the political rights of women. New York (NY): United Nations. [Google Scholar]
- D’Souza RN, Colombo JS, Embree MC, Myers JM, DeRouen TA. 2017. Our essential and endangered dentist-scientist workforce. J Dent Res Clin Transl Res. 2(1):10–22. [DOI] [PubMed] [Google Scholar]
- Dannels SA, McLaughlin JM, Gleason KA, Dolan TA, McDade SA, Richman RC, Morahan PS. 2009. Dental school deans’ perceptions of the organizational culture and impact of the ELAM program on the culture and advancement of women faculty. J Dent Educ. 73(6):676–688. [PubMed] [Google Scholar]
- Dobbin F, Kalev A. 2017. Training programs and reporting systems won’t end sexual harassment: promoting more women will. Harvard Business Review. https://hbr.org/2017/11/training-programs-and-reporting-systems-wont-end-sexual-harassment-promoting-more-women-will.
- Drake D, Ioannidou E. 2018. Faculty Development Workshop: mentoring mentors and mentees. Presented at: AADR General Session and Exhibition, Fort Lauderdale (FL). [Google Scholar]
- Earle A, Mokomane Z, Heymann J. 2011. International perspectives on work-family policies: lessons from the world’s most competitive economies. Future Child. 21(2):191–210. [DOI] [PubMed] [Google Scholar]
- European Commission. 1999. Women and science: mobilizing women to enrich European research. Brussels (Belgium): European Commission; [accessed 2018 Mar]. https://ec.europa.eu/research/swafs/pdf/pub_gender_equality/g_wo_co_en.pdf. [Google Scholar]
- European Commission. 2015. a. Strategic engagement for gender equility 2016–2019. Luxembourg (Belgium): Publications Office of the European Union; [accessed 2018 Mar]. https://ec.europa.eu/anti-trafficking/sites/antitrafficking/files/strategic_engagement_for_gender_equality_en.pdf. [Google Scholar]
- European Commission. 2015. b. Visions for gender equality. Luxembourg (Belgium): Publications Office of the European Union; [accessed 2018 Jan]. https://ec.europa.eu/info/sites/info/files/150902_vision_report_sep_en.pdf. [Google Scholar]
- European Institute for Gender Equality. 2018. Gender awareness raising. Luxembourg (Belgium): European Union. https://eige.europa.eu/gender-mainstreaming/methods-tools/gender-awareness-raising.
- European Parliament. 2006. Directive 2006/54/EC of the European Parliament and of the Council on the implementation of the principle of equal opportunities and equal treatment of men and women in matters of employment and occupation. Official Journal of the European Union. [Google Scholar]
- Feminism is for everybody. 2019. Lancet. 393(10171):493. [DOI] [PubMed] [Google Scholar]
- Fitzgerald L, Magley V, Drasgow F, Waldo C. 1999. Measuring sexual harassment in the military: the Sexual Harassment Questionnaire. Military Psychology. 11(3):243–263. [Google Scholar]
- Ginsburg R. 1996. US reports: United States v. Virginia, 518 US 515. Docket No. 94–1941. [Google Scholar]
- Halley MC, Rustagi AS, Torres JS, Linos E, Plaut V, Mangurian C, Choo E, Linos E. 2018. Physician mothers’ experience of workplace discrimination: a qualitative analysis. BMJ. 363:k4926. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Helmer M, Schottdorf M, Neef A, Battaglia D. 2017. Gender bias in scholarly peer review. Elife. 6:e21718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Herzog CR, Berzins DW, DenBesten P, Gregory RL, Hargreaves KM, Messer RLW, Mina M, Mooney MP, Paine ML, Phillips C, et al. 2018. Oral sciences PhD program enrollment, graduates, and placement: 1994 to 2016. J Dent Res. 97(5):483–491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- IADR Women in Science Network. 2015. a. Glass ceiling or sticky floor? Barriers for women in academia. http://www.iadr.org/IADR/Meetings/Past-Meetings/Meeting-Page-Archives/IADR-APR-General-Session-Exhibition/2015-Botson/Featured-Presentations-Symposia.
- IADR Women in Science Network. 2015. b. WISN awards. http://www.iadr.org/IADR/Join-Renew/Groups-and-Networks/Women-In-Science/Awards.
- IADR Women in Science Network. 2016. a. Leadership programs for women: developing women academic leaders in dentistry. http://iadr.enoah.com/Portals/32/docs/AADR Annual Meeting/AADR_HOW.pdf.
- IADR Women in Science Network. 2016. b. Work smart: salary negotiation and promotion in dental academia. http://www.iadr.org/Portals/69/docs/Meetings/IAGS/2017/IADR_HOW.pdf?ver=2017–02–06–110222–973.
- IADR Women in Science Network. 2017. a. Salary negotiations and promotion in dental academia. http://www.iadr.org/Portals/69/docs/Meetings/IAGS/2017/IADR_HOW.pdf?ver=2017–02–06–110222–973.
- IADR Women in Science Network. 2017. b. What will it take to close the gender gap in dental academia? http://www.iadr.org/IADR/Meetings/Past-Meetings/Meeting-Page-Archives/IADR-AADR-CADR-General-Session-San-Francisco-Calif-USA/Featured-Presentations-symposia.
- IADR Women in Science Network. 2018. a. Gender bias in scholarly activities: an evidence based approach. https://iadr2018.zerista.com/event/member/489623.
- IADR Women in Science Network. 2018. b. Sexual Harassment in Science: steps to no tolerance. https://iadr2018.zerista.com/event/member/489624.
- Institute of Medicine. 2011. The health of lesbian, gay, bisexual and transgender people: building a foundation for better understanding. Washington (DC): Institute of Medicine. [PubMed] [Google Scholar]
- International Association for Dental Research. 2017. IADR meeting professional conduct policy. Alexandria (VA): IADR; [accessed 2018 Feb]. http://www.iadr.org/IADR/About-Us/Policy-Statements/Meeting-Professional-Conduct-Policy [Google Scholar]
- International Labour Office. 1951. Declaration on fundamental principles and rights at work: equal remuneration convention. Geneva (Switzerland: ): International Labour Office. [Google Scholar]
- Ioannidou E, D’Souza RN, Macdougall MJ. 2014. Gender equity in dental academics: gains and unmet challenges. J Dent Res. 93(1):5–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ioannidou E, Rosania A. 2015. Under-representation of women on dental journal editorial boards. PLoS One. 10(1):e0116630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jagsi R. 2018. Sexual harassment in medicine—#MeToo. N Engl J Med. 378(3):209–211. [DOI] [PubMed] [Google Scholar]
- Jagsi R, Biga C, Poppas A, Rodgers GP, Walsh MN, White PJ, McKendry C, Sasson J, Schulte PJ, Douglas PS. 2016. Work activities and compensation of male and female cardiologists. J Am Coll Cardiol. 67(5):529–541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jagsi R, Griffith KA, Jones R, Perumalswami CR, Ubel P, Stewart A. 2016. Sexual harassment and discrimination experiences of academic medical faculty. JAMA. 315(19):2120–2121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jolly S, Griffith KA, DeCastro R, Stewart A, Ubel P, Jagsi R. 2014. Gender differences in time spent on parenting and domestic responsibilities by high-achieving young physician-researchers. Ann Intern Med. 160(5):344–353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krueger P, White D, Meaney C, Kwong J, Antao V, Kim F. 2017. Predictors of job satisfaction among academic family medicine faculty: findings from a faculty work-life and leadership survey. Can Fam Physician. 63(3):e177–e185. [PMC free article] [PubMed] [Google Scholar]
- Lariviere V, Ni C, Gingras Y, Cronin B, Sugimoto CR. 2013. Bibliometrics: global gender disparities in science. Nature. 504(7479):211–213. [DOI] [PubMed] [Google Scholar]
- Lennard N. 2017. Not just toxic masculity: income inequality also drives sexual abuse in the workplace. The Intercept. https://theintercept.com/2017/12/12/matt-lauer-payout-nbc-sexual-assault-wealth-inequality/.
- Li J, de Souza R, Efsandiari S, Feine J. 2019. Have women broken the glass ceiling in North American dental leadership? Adv Dent Res. 30(3): 78–84. [DOI] [PubMed] [Google Scholar]
- McDonald P. 2011. Workplace sexual harassment 30 years on: a review of the literature. International Journal of Management Reviews. 14:1–17. [Google Scholar]
- Moore W. 2018. The medical suffragettes. Lancet. 391(10119):422–423. [DOI] [PubMed] [Google Scholar]
- National Institutes of Health. 2015. Civil rights protections in NIH-supported pesearch, programs, conferences and other activities. Rockville (MD): National Institutes of Health. NOT-OD-15-152. [Google Scholar]
- National Research Council. 2007. Beyond bias and barriers: fulfilling the potential of women in academic science and engineering. Washington (DC): National Academy of Science. [PubMed] [Google Scholar]
- National Science Foundation. 2018. Important notice No. 144. Alexandria (VA): National Science Foundation; https://www.nsf.gov/pubs/issuances/in144.pdf. [Google Scholar]
- Nemo E. 1975. August 19 Women start to speak out about sexual harassment at work. The New York Times; [accessed 2018 Jan 15]. https://timesmachine.nytimes.com/timesmachine/1975/08/19/76591747.pdf. [Google Scholar]
- Nesbitt PE, Inglehart MR, Sinkford JC. 2003. Work environment perceptions of full-time dental educators: does gender matter? J Dent Educ. 67(8):916–924. [PubMed] [Google Scholar]
- Nguyen Le TA, Lo Sasso AT, Vujicic M. 2017. Trends in the earnings gender gap among dentists, physicians, and lawyers. J Am Dent Assoc. 148(4):257–262.e2. [DOI] [PubMed] [Google Scholar]
- Okahana H. 2018. Graduate enrollment and degrees: 2004 to 2017. Washington (DC): Council of Graduate Schools; https://cgsnet.org/graduate-enrollment-and-degrees. [Google Scholar]
- Organisation for Economic Co-operation and Development. 2016. Family size and household composition. Paris (France): Social Policy Division. [Google Scholar]
- Ovseiko PV, Chapple A, Edmunds LD, Ziebland S. 2017. Advancing gender equality through the Athena SWAN Charter for Women in Science: an exploratory study of women’s and men’s perceptions. Health Res Policy Syst. 15(1):12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parker KHJ, Rohal M. 2015. Parenting in America. Washington (DC: ): PEW Research Center. [Google Scholar]
- Schiebinger L. 1999. Has feminism changed science? Cambidge (MA): Harvard University Press. [Google Scholar]
- Schroeder J, Dugdale HL, Radersma R, Hinsch M, Buehler DM, Saul J, Porter L, Liker A, De Cauwer I, Johnson PJ, et al. 2013. Fewer invited talks by women in evolutionary biology symposia. J Evol Biol. 26(9):2063–2069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwab K, Samans R, Zahidi S, Leopold TR. 2016. The global gender gap report. Geneva (Switzerland): World Economic Forum. [Google Scholar]
- Shaddox L, Letra A. 2019. Then and now—a look inside the lives of 11 women presidents of the IADR. Adv Dent Res. 30(3):95–118. [DOI] [PubMed] [Google Scholar]
- Stoet G, Geary DC. 2018. The gender-equality paradox in science, technology, engineering, and mathematics education. Psychol Sci. 29(4):581–593. [DOI] [PubMed] [Google Scholar]
- Stone T, Miller B, Southerlan E, Raun A. 2018. Women in healthcare leadership. https://www.oliverwyman.com/our-expertise/insights/2019/jan/women-in-healthcare-leadership.html.
- Strong EA, De Castro R, Sambuco D, Stewart A, Ubel PA, Griffith KA, Jagsi R. 2013. Work-life balance in academic medicine: narratives of physician-researchers and their mentors. J Gen Intern Med. 28(12):1596–1603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- These are the women CEOs leading Fortune 500 companies. 2017. Fortune. http://fortune.com/2017/06/07/fortune-500-women-ceos/.
- Tiwari TR, Randall CL, Cohen L, Holtzmann J, Webster-Cyriaque J, Ajiboye SA, Schou L, Wandera M, Ikeda K, Fidela de Lima Navarro M, et al. 2019. Gender inequalities in the dental workforce: global perspectives. Adv Dent Res. 30(3):60–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- United Nations. 1979. Convention on the elimination of all forms of discrimination against women (CEDAW). New York (NY): United Nations. General Assembly resolution 34/180. [Google Scholar]
- United Nations. 2018. The sustainable development goals report. New York (NY): United Nations. [Google Scholar]
- US Bureau of Labor Statistics. 2019. Labor force statistics from Current Population Survey. Washington (DC): US Bureau of Labor Statistics. [Google Scholar]
- US Equal Employment Opportunity Commission. 1980. Sexual harassment. Washington (DC): US Equal Employment Opportunity Commission. [Google Scholar]
- West JD, Jacquet J, King MM, Correll SJ, Bergstrom CT. 2013. The role of gender in scholarly authorship. PLoS One. 8(7):e66212. [DOI] [PMC free article] [PubMed] [Google Scholar]