

Abstract
Background:
Population-based surveys document disparities in substance use among sexual minorities compared to heterosexuals, but few studies examine changes over time. This study compared changes in harmful drinking (including alcohol use disorders and high-intensity drinking), tobacco use, marijuana use, and simultaneous marijuana and alcohol co-use between heterosexual and sexual minority adults over a 15-year period.
Methods:
Gender-stratified logistic regression analyses using 4 waves of cross-sectional data from the National Alcohol Survey (2000, 2005, 2010, and 2015) were conducted to test overall trends over time and differences by sexual identity, as well as the interaction between survey year and sexual identity.
Results:
Among women, significant effects for sexual identity were present in all models, reflecting greater odds of use among sexual minorities across waves. Among men, significant effects for sexual identity were found for high-intensity drinking (reflecting less use among sexual minorities) as well as marijuana use and marijuana and alcohol co-use (reflecting more use among sexual minorities). For women and men, tobacco use generally decreased and both marijuana use and simultaneous marijuana and alcohol co-use increased during the study period. Although trends were largely driven by heterosexual respondents, only one instance of an interactive effect was found; reports of harmful drinking were generally stable over time among heterosexual women, but higher and more variable over time among sexual minority women.
Conclusions:
Findings highlight that differences in patterns of substance use by sexual identity persist and underscore the need for screening, prevention and intervention, particularly for sexual minority women.
Keywords: Hazardous drinking, tobacco use, marijuana use, sexual minorities
Background
Cross-sectional, population-based research in the U.S. has documented greater risk for hazardous drinking, tobacco use, and drug use among sexual minority adults compared to heterosexuals.1–3 Specifically, sexual minority women and men appear to more likely to exceed recommended weekly drinking limits (>14 drinks per week for men and >7 drinks per week for women) than their heterosexual counterparts.4,5 Harmful use of alcohol, including heavy episodic or “binge” drinking (typically 4 or more drinks on an occasion for women and 5 or more on an occasion for men) as well as alcohol-related consequences and dependence symptoms, are particularly pronounced and consistent among sexual minority women compared to heterosexual women,1,2,6 with differences in harmful use of alcohol by sexual identity less consistent among men.7,8 Tobacco use is generally higher among sexual minority adults compared to heterosexuals, again with more consistent and pronounced risk among sexual minority women compared to heterosexual women.5,9–12 Marijuana use among lesbian and bisexual women appears to be two to five time greater than that of heterosexual women.1,12 The odds of past-year marijuana use among gay men appears to be approximately four times that of heterosexual men,1,12 with somewhat elevated but not significantly higher use among bisexual men compared to heterosexual men.
Studies of trends over time (also studied as period effects) can illuminate changes in health behaviors that may potentially be influenced by changes in policy and attitudes about sexual identity.13 Attitudes and policies surrounding alcohol,14–19 tobacco,20,21 and marijuana22–24 use have also changed dramatically over time. Namely, there have been important shifts in women’s attitudes about drinking,25 as well as increases in heavy drinking in some cohorts of women.26,27 For example, between 2000 and 2010, women reported less concern about negative health impacts of drinking and less salience of religious prohibition of drinking, and there was a decline in the proportion of women who were abstainers and an increase in the proportion of high-risk drinkers over the same period.25 Although national population-based studies provide important insights about the impacts of changing social norms and policies related to substance use,14–16,23,24 possible differences in trends by sexual identity are rarely explored.
Only a few studies have examined time as a factor that may impact sexual minority health behaviors in comparison to heterosexuals. Several recent studies have examined trends over time in alcohol, marijuana, and tobacco use among sexual minority youth.28–34 These studies generally suggest that disparities in substance use between sexual minority and heterosexual youth have persisted from 1998 to 2015. To our knowledge, only one study has examined disparities in substance use over time among sexual minority adults. Using data from the National Study of Family Growth in the U.S.,35 this study focused on sexual minority women aged 15–44 and found evidence of increasing disparities in drug use among lesbian and bisexual women compared to heterosexual women over time, but no evidence of differential trends in binge drinking. That is, disparities between bisexual and lesbian women compared to heterosexual women with respect to binge drinking remained unchanged from 2002 to 2015. Additional research using population-based data, with multiple measures of substance use, are needed to better understand changes over time in health disparities among sexual minority women and men compared to heterosexuals.
The current study addresses gaps in the literature to date. First, we explicitly include time as a variable in relation to substance use among sexual minorities compared to heterosexuals. Second, we conduct gender-stratified analyses. This is significant, as the one study to date examining trends over time by sexual identity35 did not include sexual minority men. Stratified analyses by sex is important given evidence that patterns and correlates of substance use differ between sexual minority men and women in comparison to their heterosexual counterparts.1,36–39 Finally, the current study includes substance use measures that are under-investigated in disparities research to date. For example, research on simultaneous use of marijuana and alcohol suggest associations with increased frequency and quantity of alcohol use, as well as greater risk for alcohol dependence, drunk driving, social consequences, and harm to self.40,41 However, general population studies of adults to date have not examined possible differences in these outcomes by sexual identity, and how possible differences might vary over time. Thus, the current study uses data from 2000 to 2015 to address a gap in the literature by examining tobacco use, alcohol use disorder, high-intensity drinking, marijuana use, and simultaneous marijuana and alcohol co-use in gender-stratified multivariable models. We test independent effects of both time and sexual identity (e.g., bisexual/gay/lesbian compared to heterosexual identification), as well as differential effects of time by sexual identity.
Methods
Data Sources
This study used data pooled across four waves of the National Alcohol Survey (NAS) undertaken in 2000 (N = 7,612, cooperation rate [CR] = 58%), 2005 (N = 6,919, CR = 56%), 2010 (N = 7,969, CR = 52%), and 2015 (N = 7,071, CR = 44%). The NAS is a cross-sectional population-based survey of randomly selected US adults (age 18 and over) that has been conducted approximately every 5 years since 1979. Data collection has included random digit dialed (RDD) telephone surveys since 2000, and mobile phones have been included (along with landlines) since 2010. Questions about sexual orientation were added to the NAS beginning in 2000. Blacks/African Americans and Hispanics/Latinos were oversampled in all survey years, and respondents were weighted in each survey to reflect the U.S. adult population at the time of data collection, taking into account age, gender, race/ethnicity, and geographic area. Because questions about sexual orientation were asked toward the end of the survey, our analyses used weights to adjust for the sampling design and non-response, including accounting for partially-completed interviews missing sexual identity. Sexual identity could be categorized for 25,510 of the 29,571 respondents (86%) across the four survey periods.
Measures
Alcohol use disorder (AUD 2+).
Past year alcohol use disorder was based on criteria in the 5th edition of the American Psychiatric Association’s Diagnostic and Statistical Manual (DSM5).42 Items query 11 symptom domains (failure to fulfill role obligations; drinking despite social or interpersonal problems; drinking when physically hazardous; tolerance; withdrawal; using more than or for longer than intended; persistent desire to cut down/control use; giving up important activities; spending a lot of time getting alcohol, using or recovering from use; drinking despite physical or psychological problems; and craving). With these symptoms, varying levels of severity can be defined. Our measure of alcohol use disorder is based on endorsing symptoms in 2 or more domains, which corresponds to at least mild severity and is also inclusive of moderate and severe alcohol use disorder.42
High-intensity drinking (HID 8+).
The NAS surveys assessed drinking quantity (e.g., “During the last 12 months, what is the largest number of drinks you had on any single day?”) and frequency of drinking various amounts (e.g., every day or nearly every day, 3–4 times a week, 1–2 times a week, 1–3 times a month, less than once a month, once in those 12 months, and never in those 12 months) to facilitate the calculation of a Graduated Frequency (GF) measure of consumption in the past year.43,44 Based on prior research suggesting an association between alcohol-related problems and consuming larger amounts of alcohol per day,15 these items were used to create an indicator of any instance of consuming 8 or more drinks on a single day in the past year.
Tobacco use.
Respondents were asked to report how often they had smoked cigarettes or used any other kind of tobacco in the last twelve months. Beginning in 2005, this question was proceeded by a question that asked whether respondents had ever smoked cigarettes or used any other kind of tobacco products in a regular basis in their lifetime, with only those identifying as regular lifetime users being asked about past-year use. Tobacco use of any frequency in the past year was coded as past-year tobacco use; those who reported never using tobacco in the past year as well as those who were not asked this question because they were non-regular lifetime users were coded as non-users.
Marijuana use.
In the 2000 and 2005 surveys, past-year marijuana use was assessed with a question asking respondents, “How often have you used marijuana, hash, THC, or grass during the past twelve months?” In 2010 and 2015, the question was updated slightly to reflect more contemporary terminology (i.e., “How often have you used marijuana, hash, pot, THC, or ‘weed’ during the last twelve months?”). Use at any frequency was classified as use of marijuana in the past year.
Simultaneous marijuana and alcohol co-use.
Respondents who reported using marijuana in the past year and who also used alcohol in the past year were asked how often they had used alcohol and marijuana at the same time. Those who reported using the two substances together at any frequency were coded as yes to past-year simultaneous marijuana and alcohol co-use.
Survey year.
Survey year was a categorical variable identifying whether respondents participated in the 2000, 2005, 2010, or 2015 wave of the NAS, using 2000 as the reference year when examining changes over time.
Sexual identity.
Sexual identity was queried in the NAS with an item that asked respondents, “Which of the following statements best describes your sexual orientation?” In years 2000, 2005, and 2010, respondents were read three response options: heterosexual (straight), bisexual, or homosexual (gay or lesbian). Due to the smaller number of individuals in the lesbian/gay and bisexual categories in each wave, categories were further collapsed to indicate individuals who would be considered sexual minorities in order to increase stability of estimates in multivariate analyses. To ensure that doing so did not mask any potential differences between those identifying as bisexual and those identifying as gay/lesbian, we tested differences in the prevalence of use of various substance within each year using a 3-category sexual identity variable (heterosexual, bisexual, and lesbian/gay). In 22 out of 24 analyses (4 years by 6 substances) conducted separately for women and for men, there were no differences found between bisexual and lesbian/gay respondents. In 2015, possible responses were expanded to include five options: only heterosexual (straight), mostly heterosexual, bisexual, mostly gay or lesbian, and only gay or lesbian. Respondents in 2015 could also select “Something else.” Respondents who identified as “Mostly gay/lesbian” as well as respondents who identified as “Mostly heterosexual” and “Something else” were coded as sexual minorities. This classification is consistent with research suggesting greater risk of hazardous drinking among individuals who identify as mostly heterosexual45–47 or something else48 compared to those who identify as completely heterosexual.
Sex and other demographic covariates.
Analyses were gender-stratified based on a question asking respondents, “Are you male or female?” Analyses included a cohort variable where respondents were grouped into birth cohort categories based on generations defined by the Pew Research Center (2018): born 1945 or earlier (Silent and Greatest generations), born in 1946 to 1964 (Baby Boomer generation), and born in 1965 or later (Generation X, Millennial, and Post-Millennial generations). Although national polling suggests that Millennials and Post-Millennials have more liberal attitudes toward social and political issues, including same-sex marriage,49 due to their relatively small numbers in this dataset, they were combined with the Generation X cohort. Post-hoc sensitivity analyses showed no differences when a three- versus a four-category cohort variable was used. Other covariates included age (18–29, 30–49, and 50 years old and up); ethnicity and race (non-Hispanic White, non-Hispanic Black/African American, Hispanic/Latino, or other race/ethnicity, which included Asian, American Indian/Alaska Native, Pacific Islander, and those self-identifying as something else); education (high school degree or less versus some college education or higher); and relationship status (being married or living with someone as a couple versus unpartnered, which included separated, divorced, widowed, and never married).
Analyses
All analyses were conducted in Stata (version 15) using sample weights and variance estimation techniques that adjusted for the complex design features of the survey. We first conducted multivariable, gender-stratified logistic regression analyses to test the effects of time (survey wave) and sexual identity controlling for age, cohort, and other demographic characteristics. Model coefficients are displayed as odds ratios, with 3-degree-of-freedom contrasts used to test the overall effect of time.
We then ran models including an interaction between survey wave and sexual identity to examine the differential effects of time for groups defined by sexual identity. In these interaction models, contrasts tested the joint effects of the interaction as well as the simple effects of time, separately by sexual identity (using a 3-degree-of-freedom test of time for heterosexual respondents and another for sexual minority respondents). In addition to presenting model coefficients, we also graphically display predictive margins and tested average marginal effects between groups within years and between a given year and the prior year within groups.
Results
Sample Characteristics
Table 1 depicts characteristics of the pooled NAS survey data by gender and sexual identity. Unweighted cell sizes are presented; however, prevalence estimates are weighted and tests of differences by sexual identity are corrected for the survey design. Among women, the number of sexual minority respondents in each survey ranged from 85 to 263, with the greatest number in the 2015 survey. Survey wave, age, cohort, and partner status varied by sexual identity. Among men, the number of sexual minority respondents in each survey ranged from 81 to 219, with the greatest number in the 2015 survey. All covariates included in the analyses varied by sexual identity.
Table 1:
Sample Characteristics by Gender and Sexual Identity (N=25,510)
| Women | Men | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Heterosexual (n=13,870) | Sexual Minority (n=525) | Heterosexual (n=10,694) | Sexual Minority (n=491) | |||||||
| n | % | n | % | n | % | n | % | |||
| Survey Year | *** | |||||||||
| 2000 | 3,794 | 28.6 | 86 | 15.5 | 3,284 | 28.7 | 84 | 13.4 | ||
| 2005 | 3,379 | 26.0 | 85 | 16.6 | 3,033 | 26.2 | 81 | 15.5 | ||
| 2010 | 3,734 | 25.2 | 91 | 17.6 | 2,320 | 25.5 | 107 | 22.9 | ||
| 2015 | 2,963 | 20.2 | 263 | 50.2 | 1,987 | 19.5 | 219 | 48.2 | ||
| Age | *** | ** | ||||||||
| 18–29 | 1,953 | 20.4 | 154 | 41.1 | 1,995 | 22.5 | 102 | 31.8 | ||
| 30–49 | 4,805 | 38.1 | 186 | 37.1 | 4,022 | 40.1 | 182 | 37.8 | ||
| 50+ | 6,800 | 41.5 | 179 | 21.8 | 4,497 | 37.3 | 205 | 30.5 | ||
| Cohort | *** | *** | ||||||||
| <=1945 | 3,648 | 21.8 | 72 | 7.0 | 2,250 | 18.2 | 67 | 9.9 | ||
| 1946–1964 | 5,280 | 36.1 | 157 | 23.7 | 4,160 | 36.2 | 208 | 31.9 | ||
| 1965+ | 4,636 | 42.1 | 290 | 69.3 | 4,107 | 45.6 | 214 | 58.2 | ||
| Race/Ethnicity | * | |||||||||
| White/Caucasian | 7,908 | 71.1 | 264 | 65.5 | 6,547 | 70.6 | 279 | 64.0 | ||
| Black/African American | 2,906 | 11.7 | 125 | 12.9 | 1,617 | 10.3 | 91 | 16.2 | ||
| Hispanic | 2,540 | 11.4 | 105 | 12.2 | 1,942 | 12.7 | 95 | 12.0 | ||
| Other | 516 | 5.7 | 31 | 9.4 | 518 | 6.4 | 26 | 7.8 | ||
| Education | ** | |||||||||
| High School or Less | 5,675 | 40.5 | 220 | 38.1 | 4,190 | 41.2 | 148 | 31.6 | ||
| Some College or More | 8,140 | 59.5 | 304 | 61.9 | 6,383 | 58.8 | 342 | 68.4 | ||
| Partner Status | *** | *** | ||||||||
| Unpartnered | 6,681 | 39.3 | 319 | 55.8 | 3,754 | 32.1 | 330 | 60.1 | ||
| Partnered | 7,146 | 60.8 | 206 | 44.2 | 6,844 | 67.9 | 160 | 39.9 | ||
Notes. Sexual minority status could only be generated for 25,510 of the 29,571 participants across the four survey periods. Valid percentages are presented; missing data was minimal for most demographic characteristics. Unweighted cell sizes are presented, but prevalence estimates are weighted. Pearson chi-squared statistics are corrected for the survey design with the second-order Rao and Scott correction and converted into an F statistic.
p<0.05;
p<0.01;
p<0.001.
Effects of Time and Sexual Identity for Women and Men
Table 2 presents findings from adjusted gender-stratified models testing main effects of survey year and sexual identity. Among women, sexual minority status was associated with increased odds of using each of the substances examined. Significant effects for time were found for tobacco use, marijuana use, and simultaneous marijuana and alcohol co-use. For tobacco, this was reflected in decreased odds of use in each wave compared to 2000; for marijuana use and simultaneous marijuana and alcohol co-use, these were reflected in increased odds of use in later years (2010 and 2015) compared to 2000. Among men, sexual minority status was associated with decreased odds of high intensity drinking but increased odds of marijuana use and simultaneous marijuana and alcohol co-use. For men, there also was a decline in tobacco use, but marijuana use and simultaneous marijuana and alcohol co-use significantly increased beginning in 2005 compared to 2000.
Table 2:
Models Testing the Effects of Time and Sexual Minority Status on Substance Use Stratified by Gender
| Tobacco | DSM5 AUD 2+ | High Intensity Drinking (8+) | Marijuana | Marijuana & Alcohol Co-Use | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR [95% CI] | p | OR [95% CI] | p | OR [95% CI] | p | OR [95% CI] | p | OR [95% CI] | p | |
| Women | ||||||||||
| Sexual Minority | 2.72 [2.04, 3.62] | 0.000 | 2.32 [1.50, 3.59] | 0.000 | 1.94 [1.27, 2.97] | 0.002 | 3.52 [2.50, 4.96] | 0.000 | 2.70 [1.73, 4.21] | 0.000 |
| Survey Year | ||||||||||
| 2000 (Ref) | ||||||||||
| 2005 | 0.80 [0.69, 0.92] | 0.002 | 1.00 [0.76, 1.32] | 0.987 | 0.79 [0.59, 1.06] | 0.114 | 0.75 [0.55, 1.03] | 0.072 | 0.78 [0.52, 1.19] | 0.250 |
| 2010 | 0.65 [0.55, 0.76] | 0.000 | 1.46 [1.05, 2.02] | 0.024 | 1.11 [0.82, 1.51] | 0.499 | 1.20 [0.91, 1.60] | 0.195 | 1.29 [0.90, 1.86] | 0.167 |
| 2015 | 0.55 [0.45, 0.66] | 0.000 | 1.14 [0.81, 3.59] | 0.455 | 0.80 [0.56, 1.14] | 0.219 | 1.57 [1.16, 2.12] | 0.003 | 1.41 [0.94, 2.11] | 0.093 |
| Joint Test of Time Effect | F (3, 26626)=16.67 | <0.001 | F (3, 26219)=2.03 | 0.107 | F (3, 26633)=1.90 | 0.127 | F (3, 26651)=6.90 | 0.001 | F (3, 6651)=2.96 | 0.031 |
| Men | ||||||||||
| Sexual Minority | 1.14 [0.85, 1.52] | 0.384 | 2.32 [0.68, 1.49] | 0.988 | 0.68 [0.47, 0.98] | 0.040 | 1.80 [1.26, 2.56] | 0.001 | 1.72 [1.15, 2.59] | 0.009 |
| Survey Year | ||||||||||
| 2000 (Ref) | ||||||||||
| 2005 | 0.72 [0.63, 0.82] | 0.000 | 1.01 [0.82, 1.26] | 0.958 | 0.89 [0.75, 1.05] | 0.154 | 1.07 [0.86, 1.33] | 0.548 | 0.87 [0.66, 1.14] | 0.322 |
| 2010 | 0.56 [0.48, 0.66] | 0.000 | 1.09 [0.83, 1.43] | 0.545 | 0.85 [0.70, 1.04] | 0.106 | 1.38 [1.09, 1.74] | 0.007 | 1.37 [1.03, 1.83] | 0.031 |
| 2015 | 0.57 [0.48, 0.69] | 0.000 | 0.89 [0.68, 1.16] | 0.378 | 0.86 [0.68, 1.07] | 0.180 | 1.74 [1.35, 2.24] | 0.000 | 1.55 [1.13, 2.13] | 0.007 |
| Joint Test of Time Effect | F (3, 26770)=22.56 | <0.001 | F (3, 27308)=0.53 | 0.658 | F (3, 27796)=1.23 | 0.299 | F (3, 27787)=7.19 | 0.001 | F (3, 27784)=5.08 | 0.002 |
Notes. Estimates are weighted and all models adjust for age, cohort, race/ethnicity, education, and partner status.
Differential Effects of Time by Sexual Identity among Women and Men
Women.
Tables 3a and 3b present findings from gender-stratified multivariable models testing interactive effects of survey year and sexual identity on substance use. Contrasts were specified to examine the overall effect of time separately for heterosexual and sexual minorities, as well as the effect of the interaction. Predicted probabilities and tests of average marginal effects are presented in Table 4. Among women, average marginal effects of sexual minority status were significant in at least one year for each substance studied; when these differences were present (see Table 4 and Figure 1), the predicted probability of use was always higher among sexual minority women than among heterosexual women.
Table 3a:
Models Testing the Differential Effects of Time by Sexual Minority Status - Women
| Tobacco | DSM5 AUD 2+ | High Intensity Drinking (8+) | Marijuana | Marijuana & Alcohol Co-Use | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR [95% CI] | p | OR [95% CI] | p | OR [95% CI] | p | OR [95% CI] | p | OR [95% CI] | p | |
| Survey Year | ||||||||||
| 2000 (Ref) | ||||||||||
| 2005 | 0.79 [0.69, 0.92] | 0.002 | 1.04 [0.78, 1.38] | 0.792 | 0.83 [0.61, 1.12] | 0.233 | 0.81 [0.59, 1.12] | 0.213 | 0.84 [0.55, 1.30] | 0.437 |
| 2010 | 0.64 [0.54, 0.75] | 0.000 | 1.44 [1.01, 2.03] | 0.039 | 1.11 [0.81, 1.52] | 0.528 | 1.21 [0.90, 1.63] | 0.211 | 1.33 [0.90, 1.95] | 0.147 |
| 2015 | 0.56 [0.46, 0.68] | 0.000 | 1.36 [0.95, 1.94] | 0.090 | 0.87 [0.60, 1.27] | 0.469 | 1.66 [1.20, 2.28] | 0.002 | 1.62 [1.06, 2.46] | 0.025 |
| Sexual Minority Status | 2.46 [1.44, 4.20] | 0.001 | 4.42 [2.31, 8.46] | 0.000 | 2.85 [1.34, 6.04] | 0.006 | 5.13 [2.82, 9.32] | 0.000 | 4.79 [2.17, 10.58] | 0.000 |
| Survey Year*Sexual Minority Status | ||||||||||
| 2000 (Ref) | ||||||||||
| 2005 | 1.26 [0.53, 2.97] | 0.593 | 0.61 [0.18, 2.03] | 0.420 | 0.42 [0.12, 1.47] | 0.175 | 0.33 [0.11, 1.02] | 0.055 | 0.46 [0.12, 1.82] | 0.271 |
| 2010 | 1.67 [0.74, 3.79] | 0.220 | 1.35 [0.43, 4.19] | 0.608 | 1.06 [0.34, 3.33] | 0.917 | 0.97 [0.36, 2.59] | 0.954 | 0.78 [0.23, 2.67] | 0.696 |
| 2015 | 0.92 [0.45, 1.85] | 0.805 | 0.29 [0.11, 0.73] | 0.009 | 0.52 [0.18, 1.46] | 0.214 | 0.62 [0.28, 1.37] | 0.240 | 0.41 [0.15, 1.16] | 0.094 |
| Survey Year*Sexual Minority Effect | F (3, 26626)=0.87 | 0.455 | F (3, 26219)=3.19 | 0.023 | F (3, 26633)=1.13 | 0.334 | F (3, 26651)=1.51 | 0.210 | F (3, 26651)=1.11 | 0.344 |
| Time Effect-Heterosexuals | F (3, 26626)=15.64 | <0.001 | F (3, 26219)=2.02 | 0.109 | F (3, 26633)=1.08 | 0.357 | F (3, 26651)=5.87 | 0.001 | F (3, 26651)=3.23 | 0.021 |
| Time Effect-Sexual Minorities | F (3, 26626)=1.99 | 0.113 | F (3, 26219)=3.13 | 0.024 | F (3, 26633)=2.04 | 0.107 | F (3, 26651)=2.52 | 0.056 | F (3, 26651)=0.89 | 0.445 |
Notes. Estimates are weighted and all models adjust for age, cohort, race/ethnicity, education, and partner status.
Table 3b:
Models Testing the Differential Effects of Time by Sexual Identity - Men
| Tobacco | DSM5 AUD 2+ | High Intensity Drinking (8+) | Marijuana | Marijuana & Alcohol Co-Use | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR [95% CI] | p | OR [95% CI] | p | OR [95% CI] | p | OR [95% CI] | p | OR [95% CI] | p | |
| Survey Year | ||||||||||
| 2000 (Ref) | ||||||||||
| 2005 | 0.71 [0.62, 0.81] | 0.000 | 1.01 [0.83, 1.24] | 0.887 | 0.89 [0.75, 1.05] | 0.165 | 1.06 [0.85, 1.33] | 0.612 | 0.84 [0.66, 1.14] | 0.230 |
| 2010 | 0.57 [0.48, 0.67] | 0.000 | 1.10 [0.83, 1.45] | 0.503 | 0.86 [0.70, 1.05] | 0.147 | 1.42 [1.12, 1.81] | 0.004 | 1.43 [1.03, 1.83] | 0.016 |
| 2015 | 0.58 [0.48, 0.70] | 0.000 | 0.93 [0.70, 1.22] | 0.606 | 0.87 [0.69, 1.09] | 0.245 | 1.78 [1.37, 2.32] | 0.000 | 1.59 [1.19, 2.22] | 0.006 |
| Sexual Minority Status | 1.21 [0.70, 2.10] | 0.491 | 1.76 [0.95, 3.24] | 0.071 | 0.98 [0.52, 1.83] | 0.950 | 2.62 [1.43, 4.79] | 0.002 | 2.35 [1.23, 3.04] | 0.027 |
| Survey Year*Sexual Minority Status | ||||||||||
| 2000 (Ref) | ||||||||||
| 2005 | 1.48 [0.68, 3.24] | 0.327 | 0.67 [0.25, 1.78] | 0.421 | 0.86 [0.32, 2.35] | 0.775 | 1.08 [0.42, 2.76] | 0.879 | 1.60 [0.52, 4.96] | 0.415 |
| 2010 | 0.87 [0.38, 1.98] | 0.739 | 0.67 [0.18, 2.53] | 0.551 | 0.56 [0.19, 1.63] | 0.287 | 0.47 [0.17, 1.28] | 0.139 | 0.41 [0.12, 1.39] | 0.153 |
| 2015 | 0.80 [0.38, 1.66] | 0.541 | 0.42 [0.18, 1.00] | 0.050 | 0.63 [0.27, 1.48] | 0.288 | 0.64 [0.29, 1.44] | 0.283 | 0.68 [0.26, 1.80] | 0.442 |
| Survey Year*Sexual Minority Effect | F (3, 27770)=0.97, | 0.408 | F (3, 27308)=1.28 | 0.278 | F (3, 27796)=0.57 | 0.632 | F (3, 27787)=1.15 | 0.329 | F (3, 27784)=1.67 | 0.172 |
| Time Effect-Heterosexuals | F (3, 27770)=21.40 | <0.001 | F (3, 27308)=0.33 | 0.802 | F (3, 27796)=1.03 | 0.377 | F (3, 27787)=7.64 | <0.001 | F (3, 27784)=6.04 | <0.001 |
| Time Effect-Sexual Minorities | F (3, 27770)=2.68 | 0.045 | F (3, 27308)=1.70 | 0.165 | F (3, 27796)=0.94 | 0.421 | F (3, 27787)=0.48 | 0.699 | F (3, 27784)=0.61 | 0.607 |
Notes. Estimates are weighted and all models adjust for age, cohort, race/ethnicity, education, and partner status.
Table 4.
Predicted Probability of Substance Use by Year and Sexual Identity Stratified by Gender
| Women | Men | |||||
|---|---|---|---|---|---|---|
| Heterosexual | Sexual Minority | Heterosexual | Sexual Minority | |||
| Est [95%CI] | Est [95%CI] | Est [95%CI] | Est [95%CI] | |||
| Tobacco | ||||||
| 2000 | 0.27 [0.25, 0.29] | 0.46 [0.34, 0.59] | b | 0.39 [0.37, 0.41] | 0.43 [0.31, 0.56] | |
| 2005 | 0.23 [0.21, 0.25] a | 0.46 [0.31, 0.62] | b | 0.31 [0.29, 0.33] a | 0.44 [0.31, 0.57] | |
| 2010 | 0.19 [0.18, 0.21] | 0.48 [0.34, 0.62] | b | 0.27 [0.24,0.29] | 0.28 [0.16, 0.40] | |
| 2015 | 0.18 [0.15, 0.20] | 0.32 [0.23, 0.40] | b | 0.27 [0.24, 0.30] | 0.27 [0.18, 0.35] | |
| DSM5 AUD 2+ | ||||||
| 2000 | 0.05 [0.04, 0.06] | 0.16 [0.09, 0.24] | b | 0.11 [0.10, 0.12] | 0.17 [0.09, 0.24] | |
| 2005 | 0.05 [0.04, 0.06] | 0.11 [0.02, 0.21] | 0.11 [0.10, 0.12] | 0.13 [0.05, 0.20] | ||
| 2010 | 0.07 [0.05, 0.08] a | 0.25 [0.11, 0.40] | b | 0.12 [0.09, 0.14] | 0.13 [0.01, 0.26] | |
| 2015 | 0.06 [0.05, 0.08] | 0.08 [0.04, 0.12]a | 0.10 [0.08, 0.12] | 0.08 [0.04, 0.12] | ||
| HID 8+ | ||||||
| 2000 | 0.06 [0.05, 0.07] | 0.14 [0.06, 0.21] | b | 0.20 [0.18, 0.21] | 0.20 [0.11, 0.28] | |
| 2005 | 0.05 [0.04, 0.06] | 0.06 [0.01, 0.11] | 0.18 [0.17, 0.20] | 0.16 [0.07, 0.25] | ||
| 2010 | 0.06 [0.05, 0.08] a | 0.15 [0.06, 0.25]a | 0.18 [0.16, 0.20] | 0.11 [0.03, 0.19] | ||
| 2015 | 0.05 [0.04, 0.07] | 0.07 [0.03, 0.11] | 0.18 [0.15, 0.20] | 0.12 [0.07, 0.18] | ||
| Marijuana | ||||||
| 2000 | 0.06 [0.05, 0.07] | 0.22 [0.14, 0.31] | b | 0.09 [0.08, 0.10] | 0.19 [0.11, 0.28] | b |
| 2005 | 0.05 [0.04, 0.06] | 0.08 [0.02, 0.14]a | 0.09 [0.08, 0.11] | 0.21 [0.11, 0.32] | b | |
| 2010 | 0.07 [0.06, 0.09] a | 0.25 [0.13, 0.36]a | b | 0.12 [0.10, 0.14] a | 0.14 [0.05, 0.23] | |
| 2015 | 0.09 [0.07, 0.11] | 0.23 [0.16, 0.30] | b | 0.14 [0.12, 0.17] | 0.21 [0.14, 0.29] | |
| Marijuana & Alcohol Co-use | ||||||
| 2000 | 0.03 [0.03, 0.04] | 0.13 [0.05, 0.20] | b | 0.06 [0.05, 0.07] | 0.12 [0.05, 0.19] | |
| 2005 | 0.03 [0.02, 0.04] | 0.06 [0.00, 0.11] | 0.05 [0.04, 0.06] | 0.15 [0.05, 0.24] | b | |
| 2010 | 0.04 [0.03, 0.05] a | 0.13 [0.04, 0.22] | 0.08 [0.06, 0.09]a | 0.07 [0.01, 0.14] | ||
| 2015 | 0.05 [0.04, 0.07] | 0.09 [0.05, 0.14] | 0.08 [0.07, 0.10] | 0.13 [0.07, 0.18] | ||
Notes. Predictive margins are from weighted models testing the interaction between survey year and sexual identity that adjust for age, cohort, race/ethnicity, education, and partner status.
Significant (p<0.05) average marginal effect compared to prior year within sexual identity;
Significant (p<0.05) average marginal effect of sexual minority status (versus heterosexual status) within survey year.
Figure 1.
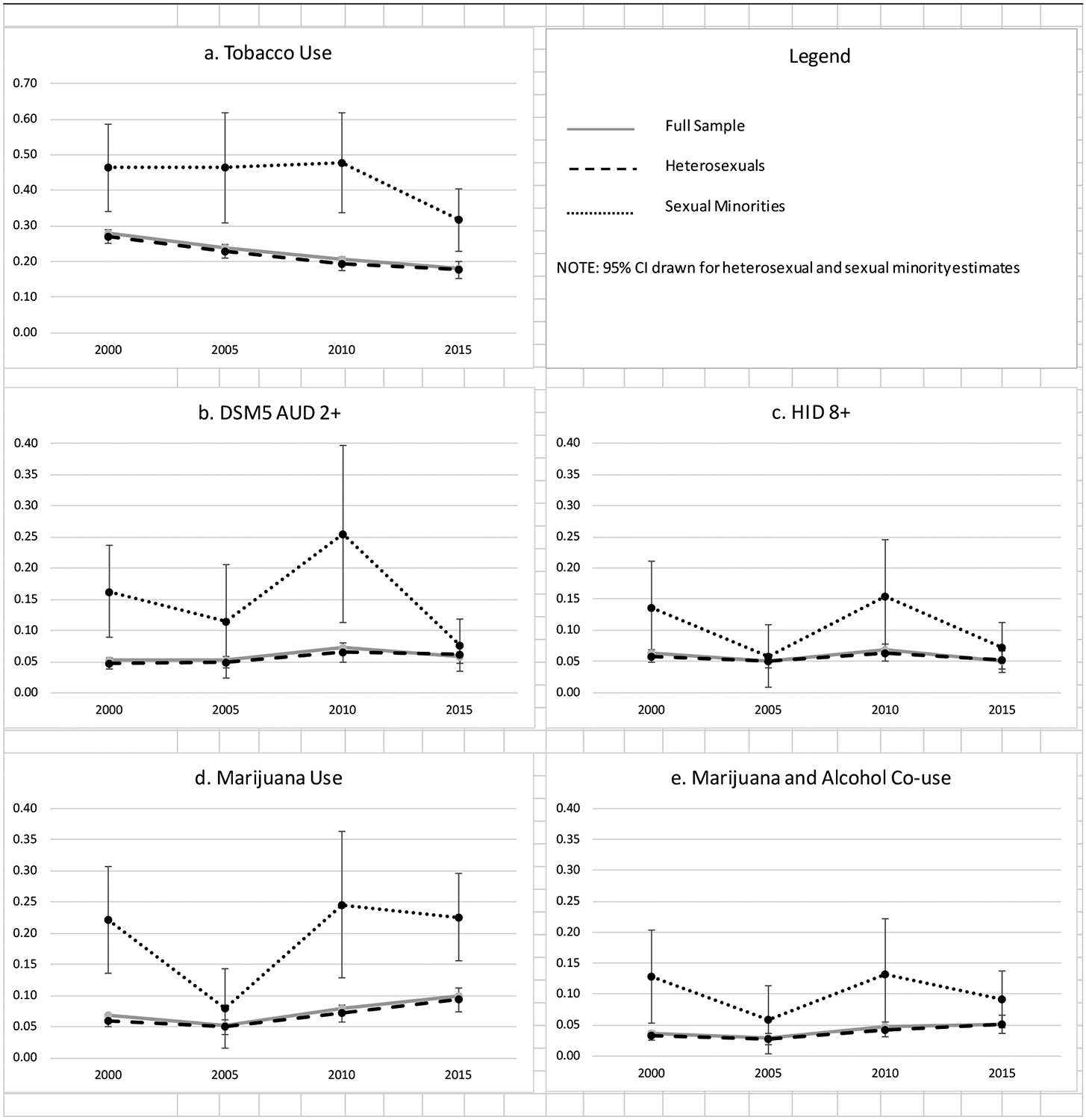
Predicted Probability of Substance Use-Women
Trends in decreased tobacco use were generally driven by heterosexual women, as the joint contrast of the simple effect of time was significant for heterosexual women but not for sexual minority women. As presented in Table 3a and displayed in Figure 1a, tobacco use started declining for heterosexual women between 2000 and 2005 (Prtobacco 0.27 vs 0.23, p=0.001). Trends in increased odds of marijuana as well as marijuana and alcohol co-use also seemed to be driven by heterosexual women, with rates being significantly lower in 2005 compared to 2010 (Prmarijuana 0.05 vs 0.07, p=0.002; Prco-use 0.03 vs 0.04, p=0.010, respectively). Marijuana use among sexual minority women did significantly drop between 2000 and 2005 (Prmarijuana 0.22 vs 0.08, p=0.009) and rebound between 2005 and 2010 (Prmarijuana 0.08 vs 0.25, p=0.008), but the contrast of the simple effect of time for sexual minority women was only marginally significant. Despite lack of significant time trends for tobacco and marijuana use among sexual minority women, there was no evidence of an interaction between survey year and sexual identity for either outcome. Rather, there was a significant interaction of time and sexual identity only with respect to AUD. In this case (see Figure 1b), although the predicted probability of AUD was generally stable among heterosexual women, it fluctuated widely across years among sexual minority women.
Men.
Among men, tests of average marginal effects within year by sexual identity revealed significant differences between heterosexual and sexual minority men for marijuana use in 2000 and 2005 (Prmarijuana 0.09 vs 0.19, p=0.015; Prmarijuana 0.09 vs 0.21, p=0.031, respectively) and for simultaneous marijuana and alcohol co-use in 2005 (Prco-use 0.05 vs 0.15, p=0.039). Although sexual minority status was associated with decreased odds of high intensity drinking among men overall, tests of average marginal effects between heterosexual and sexual minorities revealed no significant difference within survey years.
Similar to findings for women, trends in decreased tobacco use and increased marijuana use and simultaneous marijuana and alcohol co-use were largely driven by changes among heterosexuals; joint contrasts for simple effects of time for each of these outcomes were significant for heterosexuals but not for sexual minorities. Among heterosexuals, tobacco use started decreasing between 2000 and 2005 (Prtobacco 0.39 vs 0.31, p<0.001). Marijuana use began increasing in 2005 to 2010 (Prmarijuana 0.09 vs 0.12, p=0.002), as did simultaneous marijuana and alcohol co-use (Prco-use 0.05 vs 0.08, p<0.001). Despite observed trends among men being largely driven by heterosexuals, there was no evidence of an interaction between survey year and sexual identity for any outcome.
Discussion
Gender-stratified analyses of NAS data from 2000–2015 highlighted that, among women, sexual minority status was associated with increased odds for all outcomes examined, while among men, sexual minority status was associated with decreased odds of high intensity drinking but increased use of marijuana and simultaneous marijuana and alcohol co-use. Elevated risk for substance use among sexual minorities, particularly among sexual minority women, is a common finding in the epidemiologic literature.1,2,6 The analyses also highlighted important trends from 2000–2015. Overall, for both men and women, tobacco use decreased and marijuana use and simultaneous marijuana and alcohol co-use increased over time, but these trends were largely driven by changes among heterosexuals, without similar changes among sexual minority respondents.
During this time period, attitudes and policies towards substance use, particularly pertaining to tobacco and marijuana use have shifted, and these have been invoked to explain observed differences in rates of use over time. Although several recent studies have examined changes over time in alcohol, marijuana, and tobacco use among sexual minority youth, only one study, to our knowledge, has examined disparities in substance use over time among sexual minority adults.35 Our findings differ somewhat from that study, as we did not see evidence that disparities by sexual identity among women were increasing over time; however, we included a larger age range of respondents, which somewhat limits comparison of the two studies. In addition, our findings focused on marijuana use while the other study aggregated recreational use of marijuana and other drugs (e.g., cocaine, crystal meth, or injection of non-prescribed drugs). Replication with additional datasets would be informative.
Stigma, discrimination and resultant sexual minority stress are frequently invoked to explain differences in substance use between heterosexuals and sexual minorities.50 According to minority stress theory, the cumulative impact of stress associated with experiences of discrimination, expectations of rejection, managing identity disclosure, and self-stigmatization contributes to increased risk for health problems.50–52 Recent U.S. research has confirmed that indicators of minority stress are associated with harmful use of alcohol, drug use, and tobacco use among sexual minorities.36,37,53–57 For example, substance use is greater among sexual minorities who experience discrimination36,37 and who live in states or communities that are more hostile for sexual minorities (such as low approval of same-sex marriage).58 Research in other countries similarly suggests that minority stress contributes to disparities in risk for alcohol, tobacco and drug problems by sexual identity.59–61
Despite advances in enactment of, and support for, key policies such as the right of same-sex couples to marry during the study period,62,63 our data generally suggest that disparities in substance use by sexual identity have persisted over time. It is possible that more time is needed for positive social change to be reflected in lower levels of minority stress and substance use. A recent study using repeated cross-sectional survey data in Sweden (a country with a longer history of policies that are inclusive and supportive of sexual minorities) found that changes in structural stigma (laws, policies and social attitudes concerning sexual minorities) was associated with a reduction, and eventual elimination, of disparities in psychological distress between sexual minorities and heterosexuals.64 It is equally plausible that structural and interpersonal experiences of stigma continue to undermine the health and well-being of sexual minorities in the U.S. For example, there are an increasing number of states in the U.S that have enacted laws permitting denial of services to sexual minorities for reasons associated with religious beliefs, such as refusing to participate in issuing marriage licenses or to permit same-sex couples to adopt children.65 A recent study revealed that living in states that enacted laws permitting denial of services based on sexual identity was associated with increases in mental distress among sexual minorities (but not heterosexuals) compared to individuals living in states without such laws.66 Additional research, using new datasets, is warranted to monitor trends over time and explore mechanisms that illuminate how changes in structural stigma may impact sexual minority health.
In addition to policies and societal attitudes, there appear to be several factors that contribute to persistent disparities in risk for sexual minority women compared to heterosexual women, such as individual-level minority stress, disproportionate experiences of victimization, and more exposure to drinking contexts and permissive drinking norms.60 For example, recent research investigating pathways to harmful alcohol use among sexual minority women suggest that multiple factors may contribute to risk of harmful drinking, including sexual minority discrimination, stigma consciousness, proximal minority stress (i.e., self-stigmatization and identity concealment), rumination (i.e., fixating on negative feelings), social isolation, psychological distress, and drinking to cope with negative affect.67,68 In addition, sexual minority women appear to be disproportionately impacted by factors that increase risk for harmful use of alcohol among women, including childhood and adult victimization.69,70 Furthermore, patronage of bars and participation in other drinking contexts can be a source of support and community, but may also be associated with heavier drinking for some sexual minority women.71,72 Future research is needed to better understand how to reduce risk and enhance protective factors that may be particularly salient for sexual minority women.
Findings from this study underscore the importance of screening, brief interventions and referral to treatment (when warranted) to identify and support clients in need, which may be particularly salient for sexual minority women. Further, substance use prevention and intervention strategies appropriate for sexual and gender minority individuals also are needed to reduce disparities. These may include interventions tailored specifically for LGBT communities,7,73 initiatives to ensure that behavioral health interventions address the role of stigma as a risk factor,74 and support of LGBT-affirming institutional and societal policies75 Given research suggesting that substance use and psychological distress are influenced by socio-political context,58,76–80 future studies also should examine these factors in relation to substance use outcomes among sexual minorities.
This study has a number of strengths; notably, data are from a probability-based US sample in which responses to questions about use of various substances by sexual identity can be analyzed over a 15-year period across four waves. However, important limitations should be noted. Although the NAS oversampled Blacks/African Americans and Hispanics/Latinos, it did not oversample other racial/ethnic minority groups. Future research to examine current and historical disparities among (and within) Asian American, Pacific Islander, American Indian and Alaska Native sexual minority adults would be informative. Data were collected via self-report and may be subject to social desirability bias. Potential under-reporting of sexual minority identity and use of various substances may have reduced our ability to examine differences by sexual identity among these generally low-prevalence characteristics and behaviors. Although we tested differences among a 3-category sexual identity variable before we collapsed bisexual and lesbian/gay identities into a dichotomous indicator of identity in our multivariable models, the current study may have missed possible differences between groups (e.g., differences between bisexual and lesbian women or between bisexual and gay men) simply because we did not have a large enough subsample to detect potential differences. In addition, because the identity option of “something else” was asked in only one year, were we not able to examine possible differences over time with this group. This is a notable limitation in the context of recent research suggesting differential health risks for individuals who select “something else” or “not sure” in response to sexual identity questions.37,48
An important limitation of research on sexual minorities using population-based data are relatively small numbers of sexual minority respondents.81,82 Smaller numbers of sexual minorities may have also contributed to wider confidence intervals and unstable point estimates in multivariable models predicting lower prevalence behaviors. Consequently, some of the variation between years in the current study may be an artifact of small sample size rather than an indication of significant differences in health behaviors or exposure to stigma. Comparisons from year-to-year among sexual minority respondents should be interpreted with caution.
Also, although many of the questions and response options were identical across years, some changes occurred with respect to response options for sexual identity and tobacco use. Sensitivity analyses investigating potential effects of these changes did not suggest that they meaningfully altered the nature of findings. Further, changing policies regarding availability and use of various substances (namely marijuana) could have exaggerated observed trends in states where such policies have been enacted. Finally, our analyses examined any use of various substances or engagement in different levels of substance using behaviors (e.g., high-intensity drinking and AUD, as well as simultaneous marijuana and alcohol co-use), but we did not examine use frequency or other aspects of substance use which may differ among heterosexuals and sexual minorities, such as quantity of drug use or drug-related consequences and other indicators of more serious drug abuse. These factors would be important to investigate in future studies.
Conclusion
Despite social and political changes in the U.S. regarding sexual minorities, sexual-orientation-related disparities in substance use remain, with disparities most pronounced among sexual minority women. Future research should continue to monitor disparities in tobacco, alcohol, and drug use among sexual minorities. Research on individual-, interpersonal-, and policy-level interventions designed to reduce minority stress and substance use by sexual minority adults is also imperative.
Figure 2.
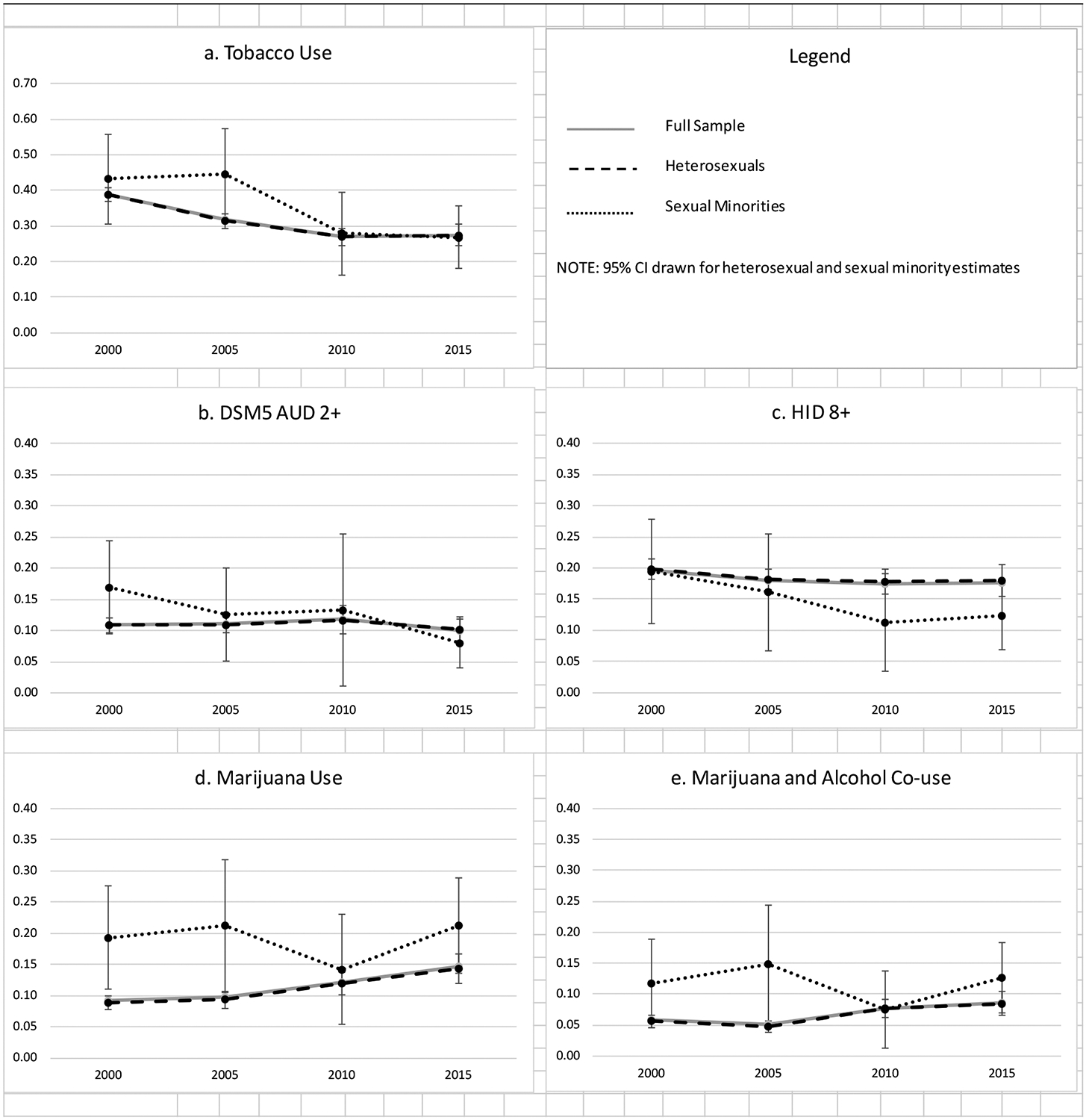
Predicted Probability of Substance Use-Men
Funding:
Research reported in this publication was supported by the National Institute on Drug Abuse of the National Institutes of Health under Grant number R01DA036606 (Trocki and Drabble PI) and the National Institute on Alcohol Abuse and Alcoholism under Grant number P50AA005595 (Greenfield PI). The funding organization had no role in the design or conduct of the study; collection, management, analysis, or interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
References
- 1.McCabe SE, Hughes TL, Bostwick WB, West BT, Boyd CJ. Sexual orientation, substance use behaviors and substance dependence in the United States. Addiction. 2009;104(8):1333–1345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Drabble L, Midanik LT, Trocki KF. Reports of alcohol consumption and alcohol-related problems among homosexual, bisexual and heterosexual respondents: Results from the 2000 National Alcohol Survey. Journal of Studies on Alcohol. 2005;66:111–120. [DOI] [PubMed] [Google Scholar]
- 3.Blosnich JR, Farmer GW, Lee JG, Silenzio VM, Bowen DJ. Health inequalities among sexual minority adults: evidence from ten US states, 2010. American journal of preventive medicine. 2014;46(4):337–349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gonzales G, Przedworski J, Henning-Smith C. Comparison of health and health risk factors between lesbian, gay, and bisexual adults and heterosexual adults in the United States: results from the National Health Interview Survey. JAMA internal medicine. 2016;176(9):1344–1351. [DOI] [PubMed] [Google Scholar]
- 5.Caceres BA, Makarem N, Hickey KT, Hughes TL. Cardiovascular disease disparities in sexual minority adults: An examination of the Behavioral Risk Factor Surveillance System (2014–2016). American Journal of Health Promotion. 2018:0890117118810246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Operario D, Gamarel KE, Grin BM, et al. Sexual minority health disparities in adult men and women in the United States: National Health and Nutrition Examination Survey, 2001–2010. American Journal of Public Health. 2015;105(10):e27–e34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Green KE, Feinstein BA. Substance use in lesbian, gay, and bisexual populations: An update on empirical research and implications for treatment. Psychology of Addictive Behaviors. 2012;26(2):265–278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hughes T. Alcohol use and alcohol-related problems among sexual minority women. Alcoholism Treatment Quarterly. 2011;29(4):403–435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.McCabe SE, Matthews AK, Lee JG, Veliz P, Hughes TL, Boyd CJ. Tobacco u and sexual orientation in a national cross-sectional study: Age, race/ethnicity, and sexual identity–attraction differences. American journal of preventive medicine. 2018;54(6):736–745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lee JG, Griffin GK, Melvin CL. Tobacco use among sexual minorities, USA, 1987–2007: A Systematic Review. Tobacco control. 2009;18:275–282. [DOI] [PubMed] [Google Scholar]
- 11.Johnson SE, Holder-Hayes E, Tessman GK, King BA, Alexander T, Zhao X. Tobacco product use among sexual minority adults: Findings from the 2012– 2013 national adult tobacco survey. American journal of preventive medicine. 2016;50(4):e91–e100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Trocki KF, Drabble LA, Midanik LT. Tobacco, marijuana use and sensation-seeking: Comparisons across gay, lesbian, bisexual, and heterosexual groups. Psychology of Addictive Behaviors. 2009;23(4):620–631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Meyer IH. Does an improved social environment for sexual and gender minorities have implications for a new minority stress research agenda? Psychology of sexualities review. 2016;7(1):81–90. [PMC free article] [PubMed] [Google Scholar]
- 14.Grant BF, Chou SP, Saha TD, et al. Prevalence of 12-month alcohol use, high-risk drinking, and DSM-IV alcohol use disorder in the United States, 2001–2002 to 2012–2013: results from the National Epidemiologic Survey on Alcohol and Related Conditions. JAMA psychiatry. 2017;74(9):911–923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Greenfield TK, Ye Y, Bond J, et al. Risks of alcohol use disorders related to drinking patterns in the US general population. Journal of studies on alcohol and drugs. 2014;75(2):319–327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Midanik L, Greenfield T. Trends in social consequences and dependence symptoms in the United States: The National Alcohol Surveys, 1984–1995. American Journal of Public Health. 2000;90(1):53–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Zemore SE, Karriker-Jaffe KJ, Mulia N. Temporal trends and changing racial/ethnic disparities in alcohol problems: results from the 2000 to 2010 National Alcohol Surveys. Journal of addiction research & therapy. 2013;4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kerr WC, Mulia N, Zemore SE. US trends in light, moderate, and heavy drinking episodes from 2000 to 2010. Alcoholism: clinical and experimental research. 2014;38(9):2496–2501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Grucza RA, Sher KJ, Kerr WC, et al. Trends in adult alcohol use and binge drinking in the early 21st‐century United States: a meta‐analysis of 6 National Survey Series. Alcoholism: clinical and experimental research. 2018;42(10):1939–1950. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Burns D. How far we have come in the last 50 years in smoking attitudes and actions. Annals of the American Thoracic Society. 2014;11(2):224–226. [DOI] [PubMed] [Google Scholar]
- 21.Cummings KM, Proctor RN. The changing public image of smoking in the United States: 1964–2014. Cancer Epidemiology and Prevention Biomarkers. 2014;23(1):32–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Carliner H, Brown QL, Sarvet AL, Hasin DS. Cannabis use, attitudes, and legal status in the US: a review. Preventive medicine. 2017;104:13–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kerr WC, Lui C, Ye Y. Trends and age, period and cohort effects for marijuana use prevalence in the 1984–2015 US National Alcohol Surveys. Addiction. 2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Schauer GL, Berg CJ, Kegler MC, Donovan DM, Windle M. Assessing the overlap between tobacco and marijuana: Trends in patterns of co-use of tobacco and marijuana in adults from 2003–2012. Addictive behaviors. 2015;49:26–32. [DOI] [PubMed] [Google Scholar]
- 25.Karriker-Jaffe KJ, Greenfield TK, Mulia N, Zemore SE. Ten-year trend in women’s reasons for abstaining or limiting drinking: The 2000 and 2010 United States National Alcohol Surveys. Journal of Women’s Health. 2018;27(5):665–675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kerr WC, Greenfield TK, Ye Y, Bond J, Rehm J. Are the 1976–1985 birth cohorts heavier drinkers? Age‐period‐cohort analyses of the N ational A lcohol S urveys 1979–2010. Addiction. 2013;108(6):1038–1048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Keyes KM, Jager J, Mal‐Sarkar T, Patrick ME, Rutherford C, Hasin D. Is there a recent epidemic of women’s drinking? A critical review of national studies. Alcoholism: clinical and experimental research. 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Watson RJ, Goodenow C, Porta C, Adjei J, Saewyc E. Substance use among sexual minorities: Has it actually gotten better? Substance Use & Misuse. 2018;53(7):1221–1228. [DOI] [PubMed] [Google Scholar]
- 29.Watson RJ, Lewis NM, Fish JN, Goodenow C. Sexual minority youth continue to smoke cigarettes earlier and more often than heterosexuals: Findings from population-based data. Drug & Alcohol Dependence. 2018;184:64–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Homma Y, Saewyc E, Zumbo BD. Is it getting better? An analytical method to test trends in health disparities, with tobacco use among sexual minority vs. heterosexual youth as an example. International journal for equity in health. 2016;15(1):79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Fish JN, Turner B, Phillips G, Russell ST. Cigarette smoking disparities between sexual minority and heterosexual youth. Pediatrics. 2019;143(4):e20181671. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Fish JN, Watson RJ, Porta CM, Russell ST, Saewyc EM. Are alcohol‐related disparities between sexual minority and heterosexual youth decreasing? Addiction. 2017;112(11):1931–1941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Fish JN, Watson RJ, Gahagan J, Porta CM, Beaulieu‐Prévost D, Russell ST. Smoking behaviours among heterosexual and sexual minority youth? Findings from 15 years of provincially representative data. Drug and alcohol review. 2019;38(1):101–110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Fish JN, Baams L. Trends in alcohol-related disparities between heterosexual and sexual minority youth from 2007 to 2015: findings from the Youth Risk Behavior Survey. LGBT health. 2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Paschen-Wolff MM, Kelvin E, Wells BE, Campbell AN, Grosskopf NA, Grov C. Changing trends in substance use and sexual risk disparities among sexual minority women as a function of sexual identity, behavior, and attraction: Findings from the National Survey of Family Growth, 2002–2015. Archives of sexual behavior. 2019:1–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.McCabe SE, Hughes TL, Matthews AK, et al. Sexual orientation discrimination and tobacco use disparities in the United States. Nicotine & Tobacco Research. 2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.McCabe SE, Hughes TL, West BT, Veliz P, Boyd CJ. DSM‐5 Alcohol Use Disorder severity as a function of sexual orientation discrimination: A national study. Alcoholism: Clinical and Experimental Research. 2019. doi: 10.1111/acer.13960. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Mereish EH, Bradford JB. Intersecting identities and substance use problems: Sexual orientation, gender, race, and lifetime substance use problems. Journal of Studies on Alcohol and Drugs. 2014;75(1):179–188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Trocki KF, Drabble LA, Midanik LT. Tobacco, marijuana, and sensation seeking: Comparisons across gay, lesbian, bisexual, and heterosexual groups. Psychology of Addictive Behaviors. 2009;23(4):620–631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Midanik LT, Tam TW, Weisner C. Concurrent and simultaneous drug and alcohol use: Results of the 2000 National Alcohol Survey. Drug and Alcohol Dependence. 2007;90:72–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Subbaraman MS, Kerr WC. Simultaneous versus concurrent use of alcohol and cannabis in the National Alcohol Survey. Alcoholism: Clinical and Experimental Research. 2015;39(5):872–879. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 5th Edition. Arlington, VA: American Psychiatric Association; 2013. [Google Scholar]
- 43.Greenfield TK, Kerr WC, Bond J, Ye Y, Stockwell T. Improving graduated frequencies alcohol measures for monitoring consumption patterns: Results from an Australian national survey and a US diary validity study. Contemporary Drug Problems. 2009;36(3/4):705–733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Greenfield TK. Ways of measuring drinking patterns and the difference they make: Experience with graduated frequency. Journal of Substance Abuse. 2000;12(1–2):33–49. [DOI] [PubMed] [Google Scholar]
- 45.Hughes TL, Wilsnack SC, Kristjanson AF. Substance use and related problems among US women who identify as mostly heterosexual. BMC public health. 2015;15(1):803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Hughes T, Szalacha LA, McNair R. Substance abuse and mental health disparities: Comparisons across sexual identity groups in a national sample of young Australian Women. Social Science & Medicine. 2010;71(4):824–831. [DOI] [PubMed] [Google Scholar]
- 47.Coulter RW, Jun HJ, Calzo JP, et al. Sexual‐orientation differences in alcohol use trajectories and disorders in emerging adulthood: results from a longitudinal cohort study in the United States. Addiction. 2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Eliason MJ, Radix A, McElroy JA, Garbers S, Haynes SG. The “something else” of sexual orientation: Measuring sexual identities of older lesbian and bisexual women using National Health Interview Survey questions. Women’s Health Issues. 2016;26:S71–S80. [DOI] [PubMed] [Google Scholar]
- 49.Pew Research Center. Generation Z Looks a Lot Like Millennials on Key Social and Political Issues. https://www.pewsocialtrends.org/2019/01/17/generation-z-looks-a-lot-like-millennials-on-key-social-and-political-issues/.Published 2019. Accessed.
- 50.Meyer IH. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin. 2003;129(5):674–697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Meyer IH, Frost D. Minority stress and the health of sexual minorities. In: Patterson CJ, D’Augelli AR, eds. Handbook of psychology and sexual orientation. New York: Oxford University Press; 2013:252–266. [Google Scholar]
- 52.Frost DM. The benefits and challenges of health disparities and social stress frameworks for research on sexual and gender minority health. Journal of Social Issues. 2017;73(3):462–476. [Google Scholar]
- 53.McCabe SE, Bostwick WB, Hughes TL, West BT, Boyd CJ. The relationship between discrimination and substance use disorders among lesbian, gay, and bisexual adults in the United States. American Journal of Public Health. 2010;100(10):1946–1952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Blosnich J, Lee JG, Horn K. A systematic review of the aetiology of tobacco disparities for sexual minorities. Tobacco Control. 2013;22(2):66–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Lehavot K, Simoni JM. The impact of minority stress on mental health and substance use among sexual minority women. Journal of Consulting and Clinical Psychology. 2011;79(2):159–170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Livingston NA, Flentje A, Heck NC, Szalda-Petree A, Cochran BN. Ecological momentary assessment of daily discrimination experiences and nicotine, alcohol, and drug use among sexual and gender minority individuals. Journal of consulting and clinical psychology. 2017;85(12):1131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Amadio DM. Internalized heterosexism, alcohol use, and alcohol-related problems among lesbians and gay men. Addictive behaviors. 2006;31(7):1153–1162. [DOI] [PubMed] [Google Scholar]
- 58.Hatzenbuehler ML, Flores AR, Gates GJ. Social attitudes regarding same-sex marriage and LGBT health disparities: Results from a national probability sample. Journal of Social Issues. 2017;73(3):508–528. [Google Scholar]
- 59.Perales F, Todd A. Structural stigma and the health and wellbeing of Australian LGB populations: Exploiting geographic variation in the results of the 2017 same-sex marriage plebiscite. Social Science & Medicine. 2018. [DOI] [PubMed] [Google Scholar]
- 60.Hughes TL, Wilsnack SC, Kantor L. The influence of gender and sexual orientation on alcohol use and alcohol-related problems: Toward a global perspective. Alcohol Research: Current Reviews. 2016;38(1):121–132. [PMC free article] [PubMed] [Google Scholar]
- 61.Lea T, de Wit J, Reynolds R. Minority stress in lesbian, gay, and bisexual young adults in Australia: Associations with psychological distress, suicidality, and substance use. Archives of sexual behavior. 2014;43(8):1571–1578. [DOI] [PubMed] [Google Scholar]
- 62.Pew Research Center. Changing Attitudes on Gay Marriage. http://www.pewforum.org/fact-sheet/changing-attitudes-on-gay-marriage/.Published 2017. AccessedFebruary 24, 2018.
- 63.Lee H-Y, Mutz DC. Changing Attitudes Toward Same-Sex Marriage: A Three-Wave Panel Study. Political Behavior. 2019;41(3):701–722. [Google Scholar]
- 64.Hatzenbuehler ML, Bränström R, Pachankis JE. Societal-level explanations for reductions in sexual orientation mental health disparities: Results from a ten-year, population-based study in Sweden. Stigma and Health. 2018;3(1):16–26. [Google Scholar]
- 65.Human Rights Campaign. Washing DC: Human Rights Campaign and Equality Federation Institute;2019. [Google Scholar]
- 66.Raifman J, Moscoe E, Austin SB, Hatzenbuehler ML, Galea S. Association of state laws permitting denial of services to same-sex couples with mental distress in sexual minority adults: A difference-in-difference-in-differences analysis. JAMA psychiatry. 2018;75(7):671–677. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Lewis RJ, Mason TB, Winstead BA, Gaskins M, Irons LB. Pathways to hazardous drinking among racially and socioeconomically diverse lesbian women: Sexual minority stress, rumination, social isolation, and drinking to cope. Psychology of Women Quarterly. 2016;40(4):564–581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Lewis RJ, Winstead BA, Lau-Barraco C, Mason TB. Social factors linking stigma-related stress with alcohol use among lesbians. Journal of Social Issues. 2017;73(3):545–562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Hughes TL, McCabe SE, Wilsnack SC, West BT, Boyd CJ. Victimization and substance use disorders in a national sample of heterosexual and sexual minority women and men: Sexual identity, victimization and SUDs. Addiction. 2010;105(12):2130–2140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Drabble L, Trocki KF, Hughes TL, Korcha RA, Lown AE. Sexual orientation differences in the relationship between victimization and hazardous drinking among women in the National Alcohol Survey. Psychology of addictive behaviors. 2013;27(3):639–648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Trocki K, Drabble L, Midanik LT. Use of heavier drinking contexts among heterosexuals, homosexuals and bisexuals: Results from a national household probability survey. Journal of Studies on Alcohol. 2005;66:105–110. [DOI] [PubMed] [Google Scholar]
- 72.Parks CA, Hughes TL, Kinnison KE. The relationship between early drinking contexts of women “coming out” as lesbian and current alcohol use. Journal of LGBT Health Research. 2007;3(3):73–90. [DOI] [PubMed] [Google Scholar]
- 73.Lee JG, Matthews AK, McCullen CA, Melvin CL. Promotion of tobacco use cessation for lesbian, gay, bisexual, and transgender people: a systematic review. American journal of preventive medicine. 2014;47(6):823–831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Herek GM. A nuanced view of stigma for understanding and addressing sexual and gender minority health disparities. LGBT Health. 2016;3(6):397–399. [DOI] [PubMed] [Google Scholar]
- 75.Pachankis JE. The scientific pursuit of sexual and gender minority mental health treatments: Toward evidence-based affirmative practice. American Psychologist. 2018;73(9):1207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Hatzenbuehler ML. Social factors as determinants of mental health disparities in LGB populations: Implications for public policy. Social Issues and Policy Review. 2010;4(1):31–62. [Google Scholar]
- 77.Hottes TS, Bogaert L, Rhodes AE, Brennan DJ, Gesink D. Lifetime prevalence of suicide attempts among sexual minority adults by study sampling strategies: A systematic review and meta-analysis. American Journal of Public Health. 2016;106(5):e1–e12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Hatzenbuehler ML, McLaughlin KA, Keyes KM, Hasin DS. The impact of institutional discrimination on psychiatric disorders in lesbian, gay, and bisexual populations: A prospective study. American Journal of Public Health. 2010;100(3):452–459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Riggle ED, Rostosky SS, Horne SG. Does it matter where you live? Nondiscrimination laws and the experiences of LGB residents. Sexuality Research and Social Policy. 2010;7(3):168–175. [Google Scholar]
- 80.Hatzenbuehler ML, Jun H-J, Corliss HL, Austin SB. Structural stigma and sexual orientation disparities in adolescent drug use. Addictive Behaviors. 2015;46:14–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Meyer IH, Wilson PA. Sampling lesbian, gay, and bisexual populations. Journal of Counseling Psychology. 2009;56(1):23–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Drabble LA, Trocki KF, Korcha RA, Klinger JL, Veldhuis CB, Hughes TL. Comparing substance use and mental health outcomes among sexual minority and heterosexual women in probability and non-probability samples. Drug and Alcohol Dependence. 2018;185:285–292. [DOI] [PMC free article] [PubMed] [Google Scholar]