

Several analyses using mathematical models have made predictions for the number of cases and fatalities due to COVID-19 in India1. Though the recommended public health interventions centred on social distancing based on these predictions, are sensible, the assumptions underlying these may not be accurate. The standard epidemiologic modelling methods [such as the susceptible-exposed-infectious-recovered (SEIR) model] assume transmission at the community level. However, the number of cases reported till recently in India was identified through screening just two populations: travellers from countries where community transmission was already ongoing, and the contacts of COVID-19-positive individuals. In such a situation, the magnitude and the time to community seeding depends on numerous, unknown variables such as the infectivity of asymptomatic individuals with infection, the efficacy of contact tracing and the time to quarantine of successfully traced individuals2. One estimate accounting for some of these variables suggested a time to epidemic initiation of about 45 days3.
Not accounting for this delay in the initiation of community transmission in SEIR models may induce a sense of complacency, and result in premature withdrawal of public health interventions. The standard approach to infectious disease modelling is to calibrate the rate of community seeding to reproduce the death rates due to the disease4. However, for such models to be reliable, active surveillance for severe acute respiratory illness (SARI) should be operational, with all patients undergoing testing for COVID-19, with prompt notification of deaths. The sentinel surveillance system for SARI in place at the moment5, will need to be transformed into an active surveillance system for the duration of the outbreak.
While efforts are on to scale up testing for COVID-19, given the resource constraints, it is unreasonable to expect population-level testing rates such as those seen in countries like South Korea. The most practical approach is to test symptomatic patients presenting to hospitals, and aggressive testing to identify and contain local chains of transmission. However, these data will not be representative of infection in the population as a whole, and cannot inform disease modelling. Random sampling in the community to determine the prevalence of infection over multiple points in time may perhaps be the ideal way to track the course of the epidemic. However, given the large population of India and its heterogeneity, obtaining representative prevalence data may be impractical, and will be very resource and time intensive. Given these logistic challenges, reliable data on deaths due to COVID-19 over time, can be used to obtain useful insights into the trajectory of the epidemic, and the effect of public health interventions.
Time to number of deaths as a measure of the effect of public health interventions: The pattern of cumulative deaths early in the epidemic in different countries provides insights into the success of any suppression or containment measures adopted. The Figure shows the time taken in days, for the number of deaths to increase to 10, from the day the first death was recorded in five indicative countries, contrasted with the time to occurrence of at least 100 deaths. Though the outbreak of infection was rapid in South Korea (time taken to the first 10 deaths was five days), the institution of successful measures to suppress the epidemic resulted in a marked prolongation of the time to the occurrence of at least 100 deaths (24 days)6. This is in contrast to the countries where the epidemic remains uncontrolled (time from 10 to 100 deaths, 5-14 days). The number of deaths in India in the weeks following the initiation of the lockdown will provide an indication of the success of the measures adopted. The data on deaths may be expected to lag behind the infection by about three weeks.
Figure.
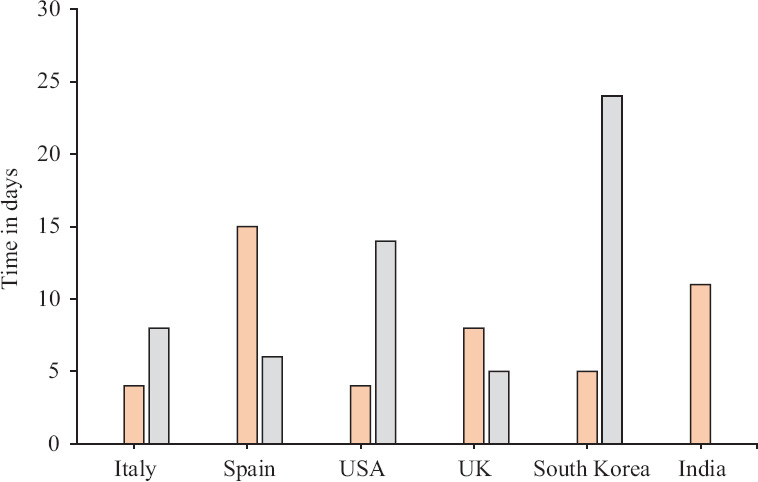
Time to 100 deaths due to COVID-19. The orange bars indicate the time from the first recorded death to 10 deaths. The grey bars show the time taken for the cumulative number of deaths to at least 100 in each of these countries. Source: Ref. 6.
In conclusion, the existing systems for the surveillance and testing of SARI in the country should be intensified, with provisions for the prompt notification of deaths due to COVID-19. In the absence of reliable information on the incidence and prevalence of infection in the population, the cumulative death rate will provide the only credible indicator of the effect of public health interventions on the trajectory of the epidemic.
Footnotes
Conflicts of Interest: None.
References
- 1.COV-IND-19 Study Group. Predictions and role of interventions for COVID-19 outbreak in India. [accessed on March 27, 2020]. Available from: https://mediumcom/@covind_19/predictions-and-role-of-interventions-for-covid-19-outbreak-in-india-52903e2544e6 .
- 2.Kucharski AJ, Russell TW, Diamond C, Liu Y, Edmunds J, Funk S, et al. Early dynamics of transmission and control of COVID-19: A mathematical modelling study. Lancet Infect Dis. 2020 doi: 10.1016/S1473-3099(20)30144-4. pii: S1473-3099(20)30144-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mandal S, Bhatnagar T, Arinaminpathy N, Agarwal A, Chowdhury A, Murhekar M, et al. Prudent public health intervention strategies to control the coronavirus disease 2019 transmission in India: A mathematical model-based approach. Indian J Med Res. 2020 doi: 10.4103/ijmr.IJMR_504_20. doi: 104103/ijmrIJMR_504_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ferguson NM, Laydon D, Nedjati-Gilani G, Imai N, Ainslie K, Baguelin M, et al. Impact of non-pharmaceutical interventions (NPIs) to reduce COVID-19 mortality and healthcare demand. [accessed on March 20, 2020]. Available from: https://wwwimperialacuk/media/imperial-college/medicine/sph/ide/gida-fellowships/Imperial-College-COVID19-NPI-modelling-16-03-2020pdf .
- 5.Indian Council of Medical Research. ICMR initiated sentinel surveillance to detect community transmission of COVID-19. [accessed on March 31, 2020]. Available from: https://icmrnicin/sites/default/files/press_realease_files/PressRelease_ICMR_19March2020pdf .
- 6.World Health Organization. Coronavirus disease (COVID-2019) situation reports. [accessed on March 4, 2020]. Available from: https://wwwwhoint/emergencies/diseases/novel-coronavirus-2019/situation-reports .