

Abstract
Radiotheranostics, injectable radiopharmaceuticals with antitumour effects, have seen rapid development over the past decade. Although some formulations are already approved for human use, more radiopharmaceuticals will enter clinical practice in the next 5 years, potentially introducing new therapeutic choices for patients. Despite these advances, several challenges remain, including logistics, supply chain, regulatory issues, and education and training. By highlighting active developments in the field, this Review aims to alert practitioners to the value of radiotheranostics and to outline a roadmap for future development. Multidisciplinary approaches in clinical trial design and therapeutic administration will become essential to the continued progress of this evolving therapeutic approach.
Introduction
Theranostics is an emerging and expanding medical field based on therapeutic interventions after imaging to verify the presence of a biological target. Although the combination of imaging and therapy dates back 70 years,1 the field has progressed rapidly over the past decade. In 2018 alone more than 1000 publications were published on the topic according to a PubMed search for theranostic or theragnostic. Increased interest has been driven by advances in diverse fields, including radioisotope-based therapeutics (radiotheranostics); bioimage-guided radiotherapy delivery;2,3 optical imaging, laser ablations, and surgery (optotheranostics);4,5 nanotherapeutics;6 interventional oncology;7 and basic sciences.
Radiotheranostics is perhaps the most clinically advanced application of theranostics, with many developments and emerging opportunities. A key aspect of radiotheranostics is that the selection of patients for radiotargeted treatments is based on imaging of the same target area; therefore, imaging and therapeutic intervention are closely linked. The concept of radiotheranostics has been around for more than 70 years, prime examples include using different forms of radioactive iodine to diagnose (eg, 124I) and treat (eg, 131I) thyroid cancers.8,9 With radioactive iodine, metastatic thyroid cancer was transformed from a disease with poor outcome to a disease with about 85% overall survival.10 Nowadays, radiotheranostics is at a point of change, and is moving into the mainstream of cancer therapeutics. The main goals of radiotheranostic indications have been to stabilise end-stage disease that is refractive to other treatments and to improve quality of life in these patient populations. Early clinical trials have improved outcomes for patients with otherwise untreatable prostate and thyroid cancers,11 as well as neuroendocrine tumours. Future objectives include treating early-stage cancer through targeted intervention and reducing the side-effects of systemic radiotherapy. Several radiopharmaceuticals that aim to meet these objectives are in development for cancer treatment (table 1). Radiotheranostics are also being explored for non-cancer applications, such as 90Y-silicate joint injections (radiation synovectomy) for severe arthritis.12 A number of new radioisotopes are expected to further improve the therapeutic window and efficacy (mainly for cancer), and image-guided interventional strategies are poised to deliver therapeutics locally with high precision. US Food and Drug Administration (FDA) approval of 177Lu-dotatate (Lutathera, Adacap [Novartis]) in neuroendocrine tumours, and the potential of a soon to be approved theranostic (177Lu-PSMA-617, Adacap [Novartis]) for patients with prostate cancer, is likely to shift radiotheranostics into the mainstream of cancer care. Market analysts predict considerable revenue growth (figure 1) and pharmaceutical companies are now investing in radiotheranostics.13–15
Table 1:
Summary of radiotheranostics for cancer treatment
| Ligand | Therapeutic isotope | Imaging isotope | Target | Manufacturer | Disease | Clinical trial phase or approval date | |
|---|---|---|---|---|---|---|---|
| Iodine | None | 131I | 124I, 131I | NaI symporter | Curium, GE Healthcare | Thyroid cancer | NA |
| Dotatate (Lutathera) | Peptide | 177Lu | 68Ga, 111In | SS2R | Adacap (Novartis) | Neuroendocrine tumours | Approved, 2018 |
| Satoreotide tetraxetan | Peptide | 177Lu | 68Ga | SS2R | Ipsen | Neuroendocrine tumours, small-cell lung cancer, and breast cancer | Phase 1 and 2 |
| PSMA-617 | Small molecule | 177Lu | 68Ga, 18F | PSMA | Adacap (Novartis) | Castration-resistant prostate cancer | Phase 3 |
| Lexidronam (Quadramet) | None | 153Sm | 99Tc, 18NaF | New bone formation | Lantheus | Bone metastases | Approved, 1997 |
| Radium223 (Xofigo) | None | 223Ra | 99Tc, 18NaF | Calcimimetic | Bayer | Prostate cancer and bone metastases | Approved, 2013 |
| Strontium89 (Metastron) | None | 89Sr | 18NaF | New bone formation | GE Healthcare | Bone pain | Approved, 1993 |
| Ibritumomab tiuxetan (Zevalin) | Antibody | 90Y | None | CD20 | Spectrum Pharmaceuticals | Relapsed or refractory low-grade, follicular, or transformed B-cell non-Hodgkin lymphoma | Approved, 2002 |
| Tositumomab (Bexxar) | Antibody | 131I | 124I, 131I | CD20 | GlaxoSmithKline | Low-grade, transformed low-grade, or follicular large-cell lymphoma | Approved, 2003; withdrawn, 2014 |
| Iobenguane (Azedra) | Antibody | 131I | 123I, 124I | Norepinephrine transporter | Progenics | Pheochromocytoma and Paraganglioma | Approved, 2018 |
| Apamistamab (Iomab-B) | Antibody | 131I | None | CD45 | Actinium Pharmaceuticals | Bone marrow ablation | Phase 3 |
| Lilotomab satetraxetan (Betalutin) | Antibody | 177Lu | None | CD37 | Nordic Nanovector | Indolent non-Hodgkin lymphoma, follicular lymphoma, diffuse large B-cell lymphoma | Phase 1 and 2 |
| Omburtamab | Antibody | 131I | None | CD276 | Ymabs Therapeutics | Neuroblastoma, CNS metastases, and small-round-cell tumour | Phase 2 and 3 |
| 3BP-227 | Small molecule | 177Lu | 177Lu | NTSR1 | Ipsen | Pancreatic ductal adenocarcinoma, colorectal cancer, and gastric cancer | Phase 1 |
| FAPI | Small molecule | 90Y, 231Bi, or 212Pb | 68Ga, 18F | FAP | Sofie Biosciences | Pancreatic ductal adenocarcinoma, colorectal cancer, and head and neck cancer | Compassionate use (Germany) |
| Pentixather | Peptide | 177Lu or 90Y | 68GA | CXCR-4 | Pentixapharm | Multiple myeloma and lymphoma | Compassionate use |
| Glass microspheres | None | 90Y | None | Tumour vessels (angiogenesis) | BTG (Boston Scientific) | Hepatocellular carcinoma | Approved, 2000 |
| Resin microspheres | None | 90Y | None | Tumour vessels (angiogenesis) | Sirtex | Hepatocellular carcinoma and liver metastases | Approved, 1998 |
| Microspheres | None | 166Ho | 166Ho | Tumour vessels (angiogenesis) | Terumo | Hepatocellular carcinoma and liver metastases | Phase 2 |
The list shows common radiotheranostics, but is not comprehensive. The availability and development of radiotheranostics varies between countries. NA=not applicable. SSR2=somatostatin receptor type 2. PSMA=prostate-specific membrane antigen. NTRS1=neurotensin receptor type 1. FAPI=fibroblast-activated protein inhibitor. FAP=prolyl endopeptidase FAP. CXCR-4=C-X-C chemokine receptor type 4.
Figure 1: Revenue growth of the radiotheranostics field.
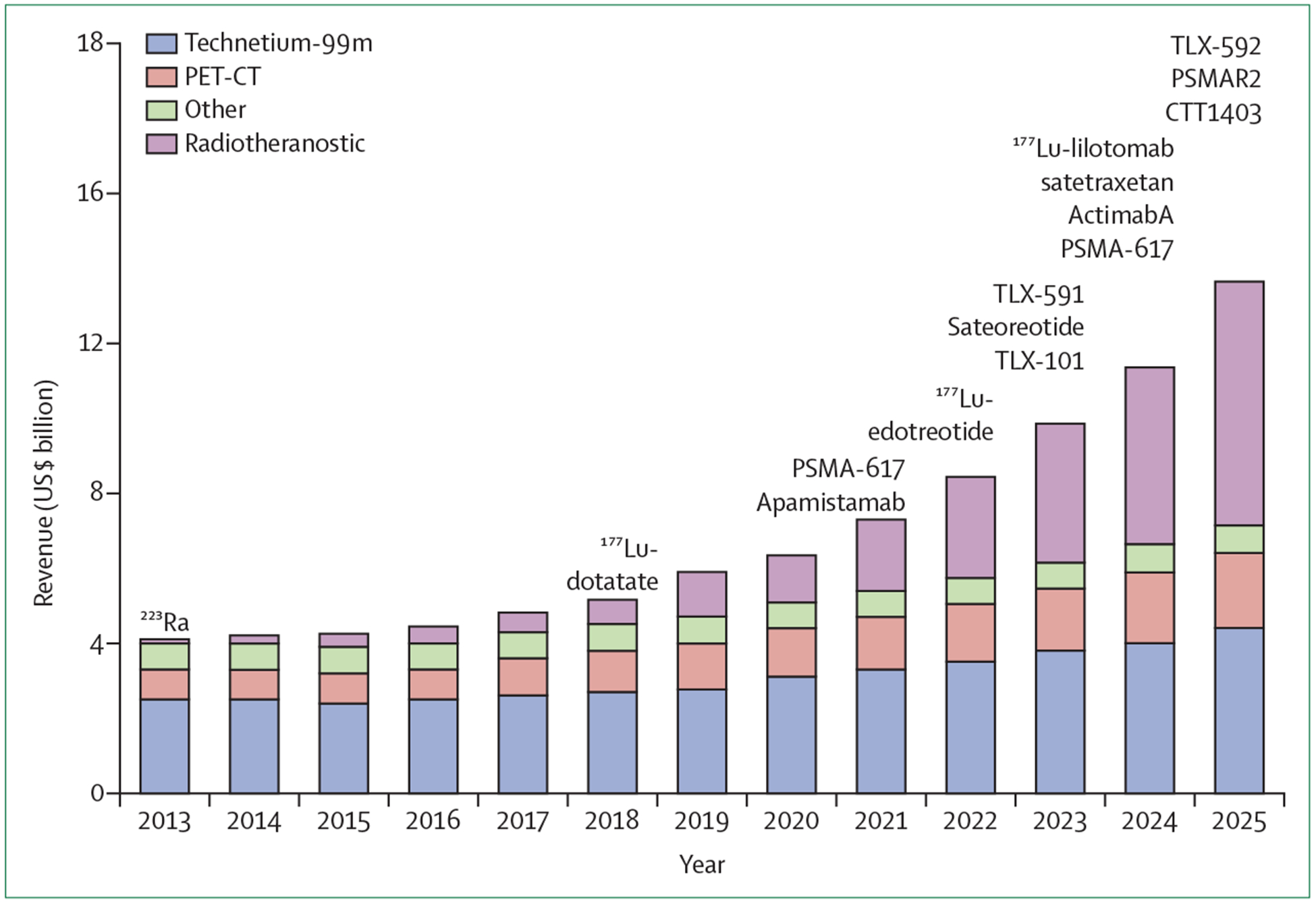
Adapted with permission from Paul-Emmanuel Goethals and Richard Zimmermann (Nuclear Medicine MEDraysintell Report & Directory, July 2019). New radiotheranostics that are not yet approved, but whose approval is expected in the future are indicated after 2020. PSMA=prostate-specific membrane antigen.
Despite the promising possibilities, the field also faces obstacles. This Review discusses key questions from the viewpoint of translational leaders in radiotheranostics and the broader membership of the International Society of Strategic Studies in Radiology. We seek to alert practitioners to the value of radiotheranostics and to outline a roadmap for future development.
Background
The status of clinical radiotheranostics trials
The ligand-linker-radioisotope design is the general structure used in radiotheranostics (figure 2).16 The targeting ligand serves as an anchor and acts to locally enrich the therapeutic radioisotope in or near the cancer. The targeting ligand is commonly a peptide (eg, octreotide acetate targeting somatostatin receptor type 2 [SS2R]), small molecule (eg, fibroblast-activated protein inhibitor [FAPI]), or antibody (eg, against CD20, CD37, or CA 19–9). These radiopharmaceuticals have different macrocyclic chelates (DOTA [1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic acid] and others) that trap α (223Ra or 225Ac) and β emitters (177Lu, 90Y, or 166Ho).16 Similar chemical constructs are used concomitantly for diagnostic PET, single-photon-emission (SPECT)-CT, and MRI, and largely rely on γ or positron emitters (90mTc, 68Ga, 18F, or 64Cu). Planar and SPECT-CT scans can also be obtained with the γ component of 177Lu and 131I. These chemical designs are for systemic administration, although exceptions to this structure include nanoparticle and microparticle therapeutics (eg, 90Y or 66Ho microspheres) that are usually given intra-arterially by image-guided intervention (figure 2). Other exceptions to the generic design include radioactive forms of free iodine that accumulate in thyroid cancer cells through the sodium iodide transporter (eg, 124I for imaging and 131I for therapy) and certain radiometals (eg, 223Ra). Other reviews discuss the use of iodine in more detail and thus will not be covered here.17
Figure 2: Overview of different radiotheranostic constructs.
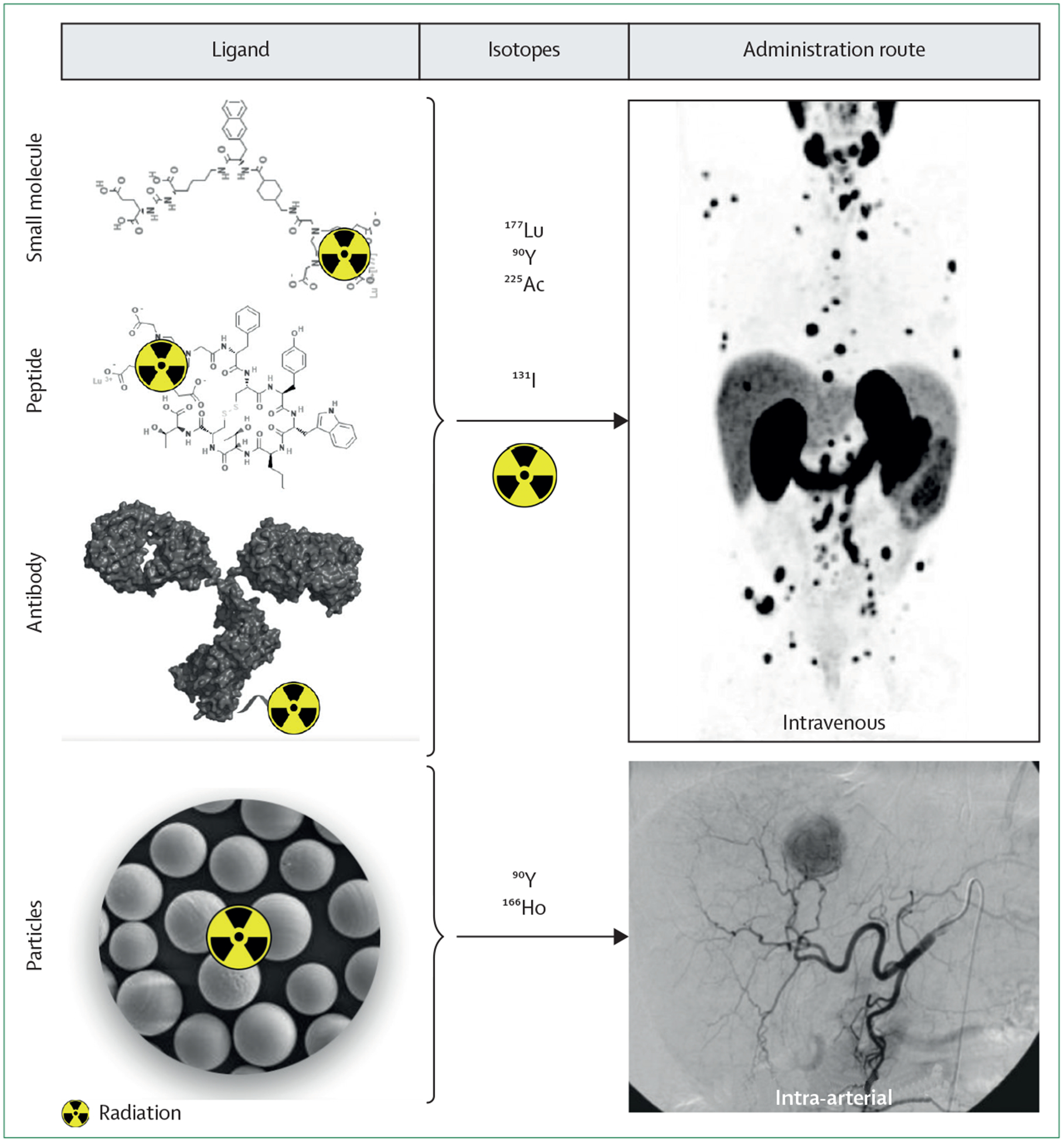
Theranostic radiopharmaceuticals are commonly designed to carry α or β emitters to cancers, which is achieved by attaching targeting ligands (small molecules, peptides, or antibodies) to chelators that complex radioisotopes for systemic delivery. Alternatively, radioiodine is attached directly to targeting ligands. Another application is to deliver micron-sized embolic particles containing 90Y to cancers using catheter based intra-arterial delivery.
Supported by the early successes of using radioiodine therapy for thyroid conditions, subsequent attempts were made to treat haematological malignancies, because these cancers typically respond well to radiotherapy. With CD20 as a target, 131I-tositumomab (Bexxar) and 90Y-ibritumomab tiuxetan (Zevalin) have been studied for the treatment of B-cell lymphomas,18,19 and both were subsequently US FDA approved for relapsed or refractory non-Hodgkin lymphoma (table 1). In 2014, 90Y-ibritumomab tiuxetan was used for consolidation therapy after frontline chemotherapy. However, despite promising clinical results, neither approved product was financially successful and did not find wide clinical traction because of complicated logistics, the absence of a trained workforce, reimbursement concerns, and, in particular, competing non-radioactive therapies, all of which impeded widespread clinical use. Lessons from these early products are still relevant nowadays and highlight the need for more interdisciplinary strategies.20
In solid tumours, the first prospective randomised phase 3 trial with therapeutic radioactive radioisotopes that showed a benefit to survival was the ALSYMPCA study (223Ra).21 223Ra was given to male patients with bone metastases from castration-resistant prostate cancer with no visceral metastases. The mechanism of action of 223Ra, which is an α emitter, is through its incorporation into areas of new bone formation. Analysis of 921 patients showed significantly improved survival for patients who received six doses of 50 Bq 223Ra isotope in addition to standard-of-care therapy compared with standard-of-care alone (median overall survival of 14.9 months vs 11.3 months, hazard ratio 0.70 [95%CI 0.58–0.83]). Patients treated with 223Ra had a low frequency of myelosuppression depite radioactive treatment and fewer adverse events than the control group, leading to its FDA approval in 2013 (table 1). 223Ra radiotreatment is recommended by the European Society for Molecular Oncology (2015)22 and the National Comprehensive Cancer Network (2016)23 and was also supported by most panellists in a 2018 consensus meeting.24
One radiotheranostic application targeted cancers that overexpressed SSR2.25 Such malignancies include neuroendocrine tumours, and, to a lesser degree, small-cell lung cancer. The therapeutic part of this approach is 177Lu-dotatate, with 68Ga-dotatate as the diagnostic counterpart. Examples of scans of patients who responded or did not respond to this regimen are in figure 3. A randomised controlled trial published in 2017 evaluated the efficacy and safety of 177Lu-dotatate in patients with advanced midgut neuroendocrine tumours and showed longer progression-free survival and a significantly higher response than participants treated with high-dose octreotide acetate.26 Clinically significant myelosuppression occurred in fewer than 10% of patients. 177Lu-dotatate received US FDA and European Medicines Agency (EMA) approval in 2018 (table 1). Results from the same trial published in 2018 showed that clinically relevant symptoms such as diarrhoea, fatigue, and pain developed over a significantly longer time period in patients on 177Lu-dotatate than high-dose octreotide acetate.27 Furthermore, patients had a longer sustained function in health-related quality-of-life categories, including those pertaining to basic and advanced daily-living activities. Administration of 177Lu-dotatate is done in four systemic doses, and should always be coupled with intravenous infusion of amino acids for nephroprotection. However, based on compassionate use data, renal radionephropathy was rarely observed, even after 6–8 cycles of treatment.28,29 Alternative strategies to 177Lu-dotatate include octreotide acetate derivatives linked to cytotoxins (eg, maitansine conjugate, PEN-221), which can be given for more than four doses. Finally, efforts to design SS2R antagonists, rather than agonists, are in development.
Figure 3: Examples of patients with well-differentiated neuroendocrine tumours undergoing 177Lu-dotatate treatment.
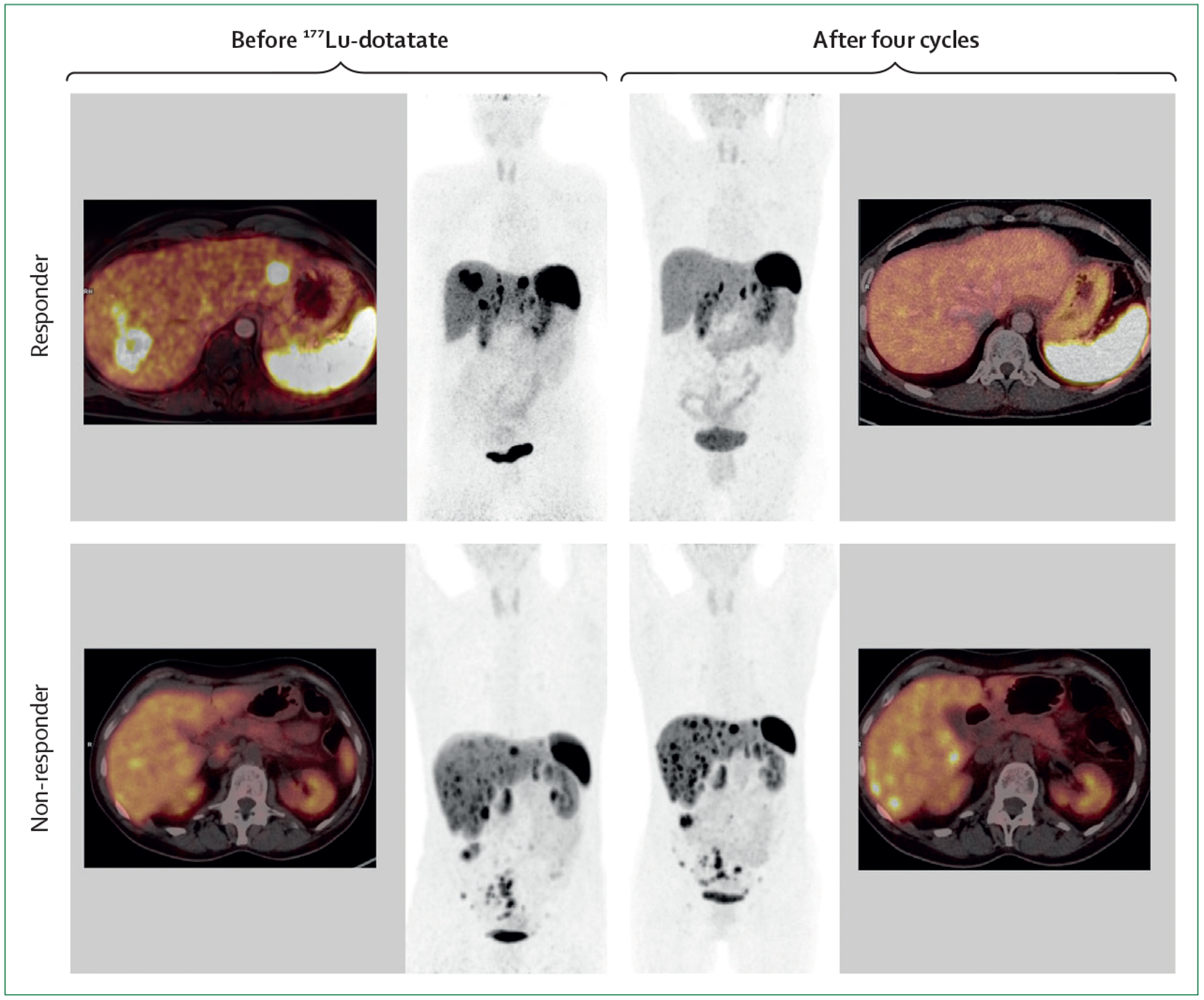
After four cycles of 177Lu-dotatate therapy a corresponding 68Ga-dotatate PET/CT scan reveals remission in a responder and progression in a non-responder (10 months between images). Responder: patient with a pancreatic neuroendocrine tumour (Ki67 of20%) showing disease progression. Non-responder: patient with a well differentiated ileal neuroendocrine tumour (Ki67 of 1%) presenting with liver metastases and peritoneal carcinomatosis. Progressive disease is still seen after four cycles of 177Lu-dotatate.
Another advanced radiotheranostic indication is the targeting of prostate-specific membrane antigen (PSMA) in prostate cancer. PSMA is expressed in 85–95% of patients with late-stage prostate cancer, and of those, 40–60% respond to 177Lu-PSMA-617 (a small molecule drug containing 177Lu and targeting PSMA), as evidenced by a decrease in prostate-specific antigen (PSA) of greater than 50%.11,30 For the 5–15% of patients who are PSMA-negative, as determined by imaging, PSMA-directed treatment is of no benefit. Most patients given 177Lu-PSMA-617 can be treated as outpatients, and side-effects are relatively uncommon but not absent. In one recent single-arm study,11 30 patients with metastatic castration-resistant prostate cancer who had progressed after conventional standard-of-care treatments were given 177Lu-PSMA-617; these patients had a high PSA response, few toxic effects, and effective pain reduction. These data led to the initiation of an ongoing randomised phase 3 trial (VISION; NCT03511664) for metastatic castration-resistant prostate cancer in thirdline postnovel androgen therapy and post-taxane therapy. Radiographic progression-free survival and overall survival will serve as primary endpoints; trial recruitment finished in the second half of 2019.
A meta-analysis31 published in 2018 included 455 patients in Europe and Australia, where 177Lu-PSMA-617 has been most widely applied as part of compassionate use programmes. In this analysis, PSA declined in two-thirds of patients, with a more than 50% reduction seen in a third of patients following the first cycle of 177Lu-PSMA-617. These encouraging data triggered the initiation of multiple prospective PSMA-directed multicentre trials, including both single arm (NCT03042312) and randomised controlled study designs (NCT03392428).
Another US FDA-approved radioactive therapeutic is 131I-iobenguane (MIBG; Azedra), which is aimed at patients with unresectable adrenal tumours, such as pheochromocytoma and paragangliomas.32 The FDA granted this application fast-track, breakthrough therapy, priority review, and orphan drug designation on the basis of a single arm, open-label clinical trial in 68 patients.32 The study met the primary endpoint by confirming that 25% of patients reduced hypertensive medication dose by 50% or more for at least 6 months, with an overall tumour response in 22% of patients. This treatment has been used in similar clinical indications for more than 10 years in many countries outside the USA.
Additional compounds in phase 2 and phase 3 trials in clinical development include the CD37-targeting radio-conjugate 177Lu-DOTA-HH1 (lilotomab satetraxetan) for haematological malignancies and 131I-labelled omurtamab for patients with advanced neuroblastoma.33–35 The companies producing these therapies are in close discussions with the US FDA and aim for approval in the near future. Several other radiotheranostics are also in the latter stages of development (table 1).
Patient acceptance and effect on quality of life
Systemic administration of radiotheranostics are simple procedures and well tolerated by most patients. Compared with chemotherapy or other targeted therapies, the number of reported side-effects is lower and primarily consists of fatigue and nausea. The potential short-term and long-term toxic effects depend on the ligand and the respective radioisotope, but include nephrotoxicity (<10% for 177Lu-dotatate) and myelosuppression (about 25%), and when these side-effects are present, patients might require a reduction in dose.36 Furthermore, long-term data will have to be gathered in larger patient populations.
In many cases, quality-of-life measurements have gained traction as qualified outcome parameters with the US FDA, EMA, and insurers. The NETTER-1 trial27 (177Lu-dotatate), for example, showed significantly improved health-related quality-of-life measurements. This outcome is in line with another single-centre study focusing on SS2R-targeted radiotheranostics in midgut neuroendocrine tumours,37 as well as PSMA-targeted radio ligand therapy in prostate cancer.11,38 Favourable outcomes on quality of life were also reported for numerous other theranostic applications in thyroid cancer39 and bone metastases.40,41 The ongoing VISION study (177Lu-PSMA-617; NCT03511664) also investigates quality-of-life parameters (health-related quality of life; EQ-5D-5L; Functional Assessment of Cancer Therapy-Prostate; Brief Pain Inventory) as secondary outcomes, in addition to safety and tolerability.
Best route of administration: systemic or image-guided?
Most radiotheranostics are given systemically (intravenously) to treat known or potentially disseminated disease to minimise invasiveness. However, in certain instances, the delivery of intravenous radiotheranostics can be challenging to deliver in sufficient doses to target tumour cells, while also trying to minimise off-target toxicity. In some patients with localised disease, these issues might be overcome with catheter-delivered intra-arterial radiotheranostics.42
The selectivity of theranostics in catheter-delivered radioisotopes have used lipiodol tumour affinity or simple tumour hypervascularity. Lipiodol has been labelled with both 131I and 188Rh, and microspheres with 90Y and 166Ho, for treatment.43 90Y resin microspheres (SIR-Spheres) and theraspheres have been approved in several countries for use in primary liver cancers and metastatic disease.44 More recently, there has been interest in combining the superselectivity of catheter-directed therapy with biologically targeted theranostic agents such as dotatate. Initial studies have shown that intra-arterial 90Y or 177Lu-dotatate can be delivered safely and decrease hepatic metastases.45,46 This intra-arterial approach has also been applied in meningiomas, which also express SSR2. For patients with meningioma receiving both intravenous and intra-arterial delivery of 177Lu-dotatate, the intra-arterial option provided higher doses and was more cytotoxic with fewer systemic side-effects.42
Lastly, interventional techniques such as tumour ablation can be coupled with the biologic selectivity of targeted imaging agents to create a theranostic effect. For example, PSMA PET-guided cryoablation and stereotactic radiotherapy of oligometastatic prostate cancer have recently been shown to have a synergistic effect.47,48
Challenges
There are several challenges facing the clinical translation and more widespread use of radiotheranostics (table 2). The overall guiding principle is to provide the best possible care to large segments of cancer patients in a fiscally responsible manner. We categorise the challenges as technical, economic, or biomedical.
Table 2:
Challenges in developing clinical radiotheranostics: reasons and possible solutions
| Solution | |
|---|---|
| Technical or organisational challenges | |
| Absence of interdisciplinary treatment teams | Create multidisciplinary disease teams |
| Small workforce | Revise training programmes; implement e-learning tools |
| Bottlenecks in radioisotope availability | Scale-up through commercial vendors |
| Uneven global availability | Scale-up through commercial vendors |
| Regulatory challenges | .. |
| Economic challenges | |
| High development cost | .. |
| Reimbursement ill-defined | .. |
| Insufficient access to funding with decreased research budgets | .. |
| Competing technologies | Prospective comparative multicentre trials |
| Global differences | Cost-benefit analysis in low and middle-income countries |
| Biomedical challenges | |
| Few available drugs | Explore new nuclides to target ligands and indications |
| Absence of large-scale prospective trials | Multicentre prospective clinical trials; design and conduct clinical trials (expertise, training, and sites) |
| Combination treatments largely unexplored | Prospective clinical trials (based on preclinical evidence) |
Technical challenges
First and foremost is the general shortage of interdisciplinary teams with standardised and efficient protocols. The use of radioactive substances is highly regulated and primarily reserved for diagnostic use in nuclear medicine and radiology. Physicians working with theranostics must bridge interdisciplinary boundaries and form disease-oriented teams, much like existing tumour boards. This approach will probably be necessary to implement adequate processes for selecting the right patients and delivering the most appropriate therapies. Establishment of such teams is already happening in centres worldwide, with a few in the USA and many more in Europe and Australia, but should now be done more widely. Second, is the occasional restricted availability of therapeutic radioisotopes and their sources, because of aging reactors, a lack of investment into new reactors, and production that does not conform with good manufacturing practices. There are also global differences in the availability of different radioisotopes and the hope is that these bottlenecks can be overcome through a coordinated industrial scale-up process.
Economic challenges
Reimbursement and clinical responsibilities coupled with use of alternative therapies often remains poorly defined and varies from country to country. Despite these hurdles, successes in neuroendocrine tumours and prostate cancer have led to investments by the pharmaceutical industry and support from the US FDA.14
Adequate research funding to prove the value of theranostics, largely done through large interdisciplinary teams, will be useful in providing support for well-designed prospective clinical trials.
Biomedical challenges
These challenges include the small number of radiotheranostics on the market, as well as the absence of both large-scale prospective trials and research into combination treatments. Some of these issues are being addressed by developing new targeting ligands, radioisotopes, and applications. Basic, preclinical, and translational research are particularly important to the progress in this field, and will need to be supported appropriately by pharmaceutical companies and regulatory agencies.
Recommendations
We suggest a number of recommendations to address existing challenges (table 2).
Radiotheranostics pipeline
The development pipeline is varied and includes additional indications for existing radiotheranostic agents and new targets, radioisotopes, targeting ligands, and treatment combination therapies. Each of these approaches should be studied in more detail in future clinical trials. In order to more rapidly explore novel agents, developing facilitated procedures (eg, fast track approvals, simplified regulations for clinical studies, and adequate good manufacturing practice redefinition for radio pharmaceuticals) to test new (diagnostic) radiopharmaceuticals that can be given intravenously in minute amounts might be necessary. Although regulations are different between countries, often these guidelines are so stringent that they hinder the exploration of new pharmaceuticals.
New indications
A number of different cancers, other than neuroendocrine tumours, overexpress SS2R (eg, breast, small-cell lung cancer, pheochromocytoma, and meningioma), and PSMA expression is not restricted to prostate cancer (hepatocellular carcinoma, renal cell cancer). 177Lu-dotatate is currently being explored for the treatment of pheochromocytoma, paraganglioma, and meningioma,49,50 177Lu-OPS201 for breast and small-cell lung cancer (NCT03773133), and PSMA-617 for hepatocellular carcinoma.51
As with other new therapeutic approaches, late-stage cancers are often explored first—eg, NETTER-126 focused on secondline treatment, and the ongoing VISION study investigates thirdline treatment in metastatic castration-resistant prostate cancer after novel androgen axis therapy and post-taxane therapy. Future trials should investigate the option to start radiotheranostic therapy earlier. Preliminary data are encouraging for 177Lu-dotatate-like therapeutic concepts in the neoadjuvant setting52 and for 177Lu-PSMA-617 before radical prostatectomy and pelvic lymph node dissections.53
New targets
Ideal targets are selectively overexpressed in a tumour or tumour-associated cell, are absent or expressed at low amounts in physiological tissues, and have an extracellular component.54 New biological targets include the C-X-C chemokine receptor type 4 (CXCR-4)–SDF-1 axis (figure 4)55 and prolyl endopeptidase FAP, which is up-regulated by cancer-associated fibroblasts.56 The FAPI family targets the microenvironment and has been licensed to Sofie Biosciences in 2019. First-inhuman use has already been reported for both targets, and additional prospective trials are anticipated. Additional targets under clinical investigation are the gastrin-releasing peptide receptor (GRP-R) and the integrin αVβ3 or αVβ5 receptors, among others. Haematological malignancies, such as CD38 positive myeloma cells or CD45 positive acute myeloid leukaemia cells, are also attractive targets for radiotheranostics. Such therapies not only offer considerable benefits for clinical outcomes, but also positively affect quality of life, and many more targets are currently being studied.57 Radionuclide therapy often requires only a single infusion visit compared with more frequent infusions for cold-antibody maintenance therapy.20
Figure 4: CXCR-4-directed radiotheranostics in a patient with intramedullary and extramedullary multiple myeloma.
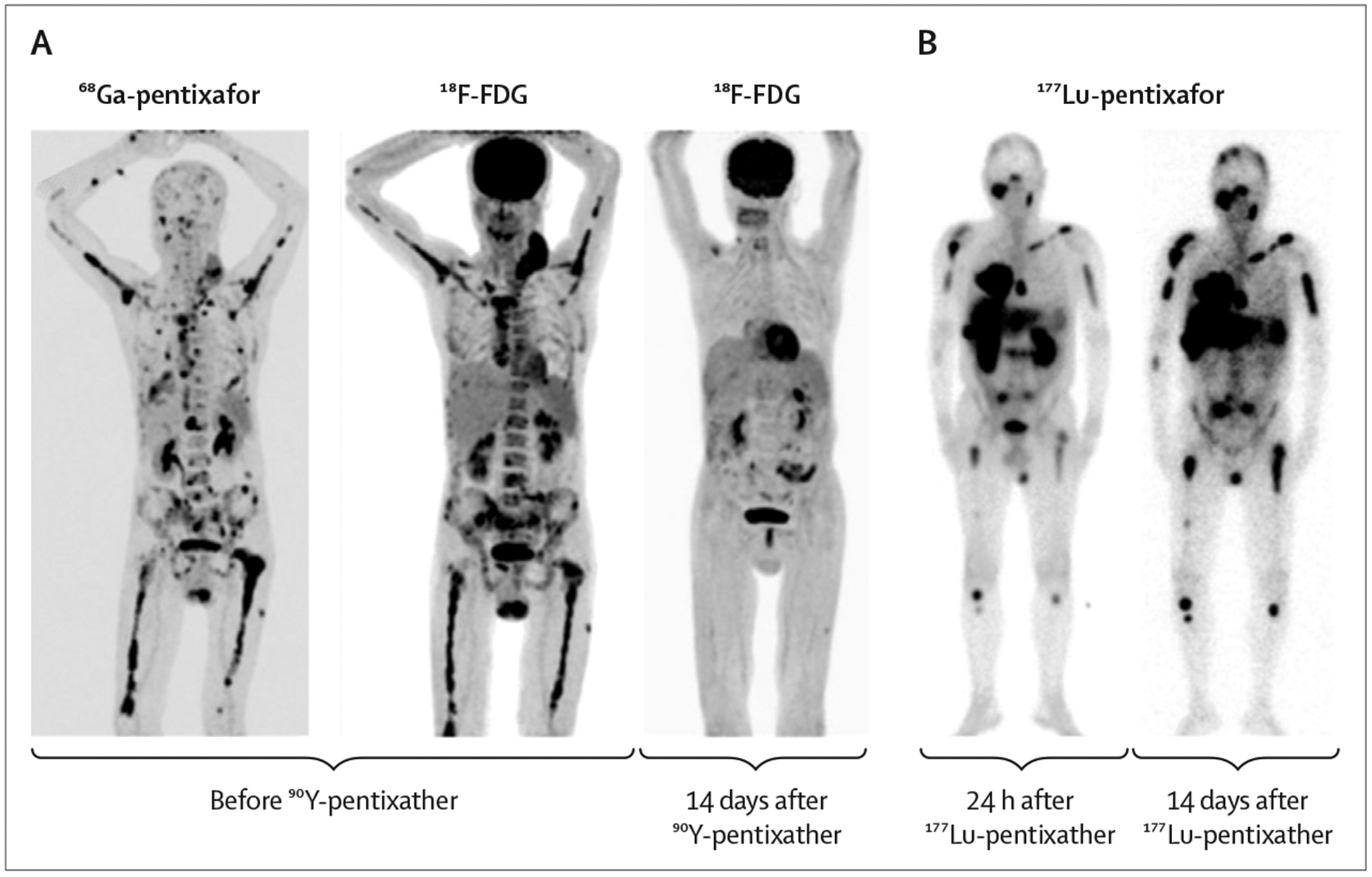
(A) Maximum-intensity projections of 68Ga-pentixafor and 18F-labeled fluoro-2-deoxyglucose (18F-FDG) PET/CT indicate multiple extramedullary and intramedullary 18F-FDG-avid myeloma lesions with high CXCR-4 expression. Corresponding 18F-FDGPET/CT image 14 days after 90Y-pentixather treatment shows complete metabolic response compared with images before therapy. (B) Scintigraphic images of a patient with multiple myeloma at 24 h and 14 days after 15.2 GBq of 177Lu-pentixather. This figure shows how ligand binding to CXCR-4 is retained for 14 days after injection. The imaging does not provide any information on the success or failure of treatment. Visual differences in tumour-to-background ratios at both time points are because of reduced background uptake at the later time point and longer emission times to account for lower particle counts. Adapted and reprinted with permission from Hermann et al (2016).55
New radioisotopes
To further develop theranostics, an option is to expand the range of therapeutic radioisotopes (table 1). Common therapeutic radioisotopes include 177Lu, 90Y, and 131I, which can enact their therapeutic effect via β emission. α-emitting radioisotopes, such as 225Ac, 213Bi, 212Pb, and 211At, are particularly appealing because they convey substantially more energy than β emitters and have a smaller depth of penetration in tissue (about 5 mammalian cell diameters), which increases the damage to tumour cells. Despite encouraging data for 225Ac-PSMA-617 in prostate cancer, clinical translation will probably take longer for β-emitting theranostics because of logistical challenges (eg, production of radionuclides, waste management, and half-life) and the potential for more severe toxic effects.58 The efficacy of different radioisotopes for tumours of varied size will also be important to study in future trials.
New targeting ligands and approaches
Expanding the range of radioactively-labelled ligands beyond the use of peptides is feasible and promising; for example, the expansion of radiotheranostics as antibodies will increase the number of druggable targets. In addition, there are opportunities for development with small molecules, nanobodies, and engineered proteins. As well as developing new targeting ligands, pretargeted radio immunotherapy could also be used to improve efficacy compared with therapies that do not use pretargeting. In this two-step approach, patients first receive non-radioactive tumour-targeting antibodies, and after a delay (24–48 h) to allow for blood clearance and tumour accumulation, patients receive a low-molecular weight radioactive agent with high affinity for the homed anti body. Most pretargeted radioimmunotherapy approaches in a preclinical setting have used antibody–streptavidin conjugates or fusion proteins labelled with 90Y-DOTA biotin.20 Click-chemistry approaches in preclinical studies have been developed for pretargeting in imaging and therapeutic applications.59–62
Combination therapies
The most suitable way to improve clinical acceptance of theranostics, as well as increase clinical effectiveness, is through the identification of optimal combinations of theranostic agents with other synergistic treatments, including chemotherapy, targeted inhibitors, and immuno therapies. Despite the success of 177Lu-dotatate in the NETTER-1 trial,26 only 1% of patients achieved complete response. To cure patients undergoing PSMA-targeted radiotheranostics in a thirdline setting is likely to be impossible. The question is how do we best combine treatments to achieve high success rates?63 Since radiotheranostics stimulate the immune response, they might enhance the efficacy of immunotherapy.64 Combinations of 177Lu-dotatate with nivolumab are being tested for the treatment of small-cell lung cancer (NCT03325816) and 177Lu-PSMA-617 with pembrolizumab in metastatic prostate cancer (NCT03805594). Investigations into combining radiotheranostics with conventional chemotherapy (capecitabine; NCT02736500) or targeted inhibitors for radiosensitising (olaparib; NCT03874884) are ongoing. Preclinical trials and early clinical data suggest that integrating radiotheranostics with external beam radiotherapy is a promising avenue for further translational studies.65
Future clinical trials
As the portfolio of cancer therapeutics widens, the right choice, timing, and combination of interventions will become the main challenge of precision oncology. With respect to radiotheranostics, we envision future trials that can address the stage of disease, dosing, combination treatments, and new indications.
Targeting different stages
New therapeutics are usually first introduced as palliative regimens in advanced metastatic disease. Following phase 1 and 2 evaluations, positive results in prospective randomised trials are vital to clinical approval and reimbursement processes. In the past decade, all radiotheranostic approaches have followed this route to US FDA approval and Centers for Medicare and Medicaid Services reimbursement. However, the ultimate goal is for earlier detection and firstline radiotheranostics (eg, in prostate cancer) to be included into the pathway for approval. This concept will have to be carefully tested in well designed, step-wise, multicentre prospective clinical trials. In prostate cancer, one possible next step is to test curative PSMA theranostics as a firstline therapy. The low-toxicity profile of PSMA theranostics, mainly because of a small molecule that targets PSMA, might allow earlier application of PSMA therapy. Radiosensitivity and favourable dosimetry in localised early disease might therefore provide curative potential in prostate cancer therapy.
Expanding of dose
Most radiotheranostic therapies are restricted to a single administration (for many haematological malignancies) or a low number of administrations (for solid cancers). For example, 177Lu-dotatate is limited to four doses as the tolerability has not yet been shown in prospective studies. Most pharmaceutical companies recommend that radiopharmaceuticals should be given to patients as a universal standard dose; however, pretherapeutic and post-therapeutic imaging can be used for more accurate dose-finding and for individualising the treatment of patients.66,67 Furthermore, because only a few dose escalation studies have been done to date (NCT03773133, NCT02592707, NCT03525392, NCT03490838), future clinical studies are warranted to explore dose escalation and timing. These efforts should similarly encompass more accurate dosimetry predictions based on quantitative imaging studies by PET/CT.
Exploring new indications
Several new indications await investigation in future prospective trials and the treatment of haematological malignancies is a logical next step, given the plethora of targets accessible to antibodies. The stepwise introduction of new indications, and combining theranostics with other regimens such as immunotherapies, requires close partnerships between the pharmaceutical industry and academic institutions. Theranostic applications beyond cancer (ie, for inflammatory disease), might also stimulate industry interest and motivate the necessary funding of clinical trials.
Training the next generation of physicians, physicists, radiochemists, and radiopharmacists
The clinical use of radiotheranostics can be more complex than use of conventional chemotherapy because of logistical challenges and regulatory hurdles. However, these difficulties can all be addressed. For example, considerations include attention to radiation safety during the application of treatment and in waste management, the limited half-life of the therapy (hours or days compared to months for chemotherapy), and the possibility and need for imaging after radiotheranostic administration.68 The safe application of radiotheranostics requires a specialised and well-trained team of physicians, radiopharmacists, medical physicists, and nurses to ensure patient safety.68,69 Clearly defined roles within a team are necessary when it comes to diagnosis, drug preparation, radiation safety, treatment, monitoring, and follow-up. Strategically aligning all training goals is crucial, particularly in view of the field’s expected expansion.
There is an international shortage in the number of trained radiochemists required to produce diagnostic and therapeutic radiopharmaceuticals (State of the Science of Nuclear Medicine, commissioned by the National Research Council of the National Academies).70 Formulating and safely dispensing these drugs requires additional expertise in the field of radiopharmacy. This expertise is particularly important when handling large quantities of therapeutic radioisotopes, such as β-emitting and α-emitting nuclides. Radiopharmacists also need these skills, because practicing pharmacy includes reviewing patient profiles and answering questions related to the drug and its uses. Technologists, medical physicists, and nurses would also require specialised training to care for patients receiving radiotheranostics. Medical physicists must understand both radiation safety and dosimetry. For personalised medicine to be realised in the context of radiotheranostics, board-certified medical physicists who are experts in patient dosimetry and endoradiotherapy dose-planning will be key. These personnel are in short supply and supplemental training with short internships or fellowships that specifically focus on endoradiotherapy would help support professionals in the field. Finally, e-learning approaches, exchange programmes, and medical student teaching should be considered in the future to try and expand the use of radiotheranostics to other countries.
The use of radiotheranostics in the clinical practice will depend on well trained nuclear medicine and radiology physicians who can bridge the divides between radiochemistry and pharmacy, nuclear imaging, clinical investigation, and different fields of clinical oncology. Building these bridges can be achieved by creating a nuclear medicine training programme based on cutting-edge research in tandem with a specialised training curriculum in patient management that emphasises the handling and management of targeted radio isotope therapy side-effects.
The success of theranostics will require attention to the education and training of future generations of specialists. Concepts that have been discussed include additional oncology training and fellowships for nuclear medicine or additional theranostics training for oncologists.71 More specifically, we suggest that following standard residency in radiology or nuclear medicine, imaging physicians should complete a 1–2-year fellowship in molecular imaging and radiotheranostics. This training should follow a minimum of 1 year in a clinical medical or oncology internship. Medical oncology fellowships should dedicate 6–12 months to allow fellows to rotate through different radiotheranostic programmes. For oncologists who currently have little experience in nuclear medicine-based radiotheranostics, this training programme would promote familiarity and confidence in these novel techniques.
For all professions involved, Our communities and societies must ensure high standards are maintained via recertification, board reviews, and recredentialing, depending on the local and national requirements. These recertifications should not be burdensome; rather, they should be used to maintain the highest levels of standards and safety. Furthermore, the multidisciplinary tumour board model is a successful way to bring together all the physicians responsible for managing patients. In this model, the fellowship-trained nuclear medicine physician would work together with the radiologist, medical oncologist, radiation oncologist, surgeon, and others to manage the patient safely and to coordinate management of side-effects.
Summary
Radiotheranostics are cell-killing radiation strategies that combine molecular targeting and optimised radiation dosimetry and are likely to emerge as an important player among cancer treatments (nuclear oncology).72 Although in its infancy, the combined approach of chemotherapy, immune modulation, and radiotheranostics should support precise cancer therapy in both palliative and curative settings. To realise this technique’s potential, interdisciplinary efforts are needed to overcome structural, financial, and educational challenges to forming therapy teams that reflect the methodological, as well as medical, expertise required. Initial clinical success will determine the extent of specialty theranostic centres and the number of trained individual specialists. Fruitful partnerships with industry will be essential to the successful growth of theranostics.
Search strategy and selection criteria.
References for this Review were identified through searches of PubMed with the terms “theranostics”, “theragnostics”, “177Lutetium”, and “Lutathera” between Jan 1, 1990 and Oct 1, 2019. Articles were also identified through searches of the authors’ own files. Only papers published in English were reviewed. The final reference list was generated based on originality and relevance to the broad scope of this Review.
Acknowledgments
We thank all members of the International Society for Strategic Studies in Radiology for their discussion and review of the manuscript. We appreciate the thoughtful additional comments and reviews by Andrew M Scott (Austin Hospital, Melbourne, VIC, Australia), and Paul-Emmanuel Goethals and Richard Zimmermann (MEDraysintell, Louvain-la-Neuve, Belgium).
Funding
SSG, JSL, SBS, MB, HH, and RW received grant support from the National Cancer Institute (NCI). JSL, SBS, and HH are supported by a P30 Cancer Center Support Grant (P30 CA008748) to the Memorial Sloan Kettering Cancer Center, an NCI-designated comprehensive cancer centre. MS acknowledges support of the Deutsche Forschungsgemeinschaft.
Footnotes
Declaration of interests
KH reports personal fees from Bayer, SIRTEX, Adacap, Curium, Endocyte, IPSEN, Siemens Healthineers, GE Healthcare, Amgen, and Novartis; non-financial support from ABX; grants and personal fees from BTG; and stock options (<1% of the company) from Sofie Biosciences, outside the submitted work. MS reports personal fees from GE Healthcare outside the submitted work. JSL reports personal fees from Clarity Pharmaceuticals, Varian Medical Systems, and InVicro; personal fees and other support from pHLIP Technologies; non-financial support from Trace-Ability, Thermo Fisher Scientific, Ground Fluor Pharmaceuticals, AbbVie, and Genentech; other support from Telix Pharmaceuticals, Eli Lilly, Sapience Therapeutics, MabVax Therapeutics, SibTech, ImaginAb, Merck, Bristol-Myers Squibb, Y-mAbs, and Regeneron Pharmaceuticals, outside the submitted work. SBS reports grants from GE Healthcare and Elesta; grants and other support from Johnson & Johnson; personal fees from BTG, XACT Robotics, Endoways, and Adgero; non-financial support from AngioDynamics; personal fees and other support from Aperture Medical; and other support from Immunomedics and Progenics, outside the submitted work. MB attended an advisory board meeting of Merck KGaA (Darmstadt), for which the University of Dresden received a travel grant. He further received funding for his research projects and for educational grants to the University of Dresden by Teutopharma GmbH (2011–2015), IBA (2016), Bayer AG (2016–2018), Merck KGaA (2014–2030), and Medipan GmbH (2014–2018). He is on the supervisory boards of HI-STEM gGmbH for the German Cancer Research Centre (DKFZ, Heidelberg). As a former chair of OncoRay (Dresden) and present CEO and Scientific Chair of the German Cancer Research Center (DKFZ, Heidelberg), he has been responsible for collaborations with a multitude of companies and institutes worldwide; signed contracts for institutes and staff members for research funding and collaborations with industry and academia; and has been responsible for commercial technology transfer activities of institutes, including the DKFZ-PSMA617 related patent portfolio [WO2015055318 (A1), ANTIGEN (PSMA)] and similar IP portfolios. MB confirms that none of the above funding sources were involved in the preparation of this Review. SSG reports personal fees from AbbVie, Ceremark Pharma, Endra, and Great Point (BVP); other support from Akrotome Imaging, Cellsight Technologies, CytomX Therapeutics, Grail, ImaginAb, MagArray, Nodus Therapeutics, Puretech, RefleXion Medical, SiteOne Therapeutics, Spectrum Dynamics, and Vor Biopharma; and personal fees and other from EARLI, Nines, Nusano, and Vave Health, outside the submitted work. HH reports personal fees from Ion Beam Applications, outside the submitted work. RW reports personal fees from Tarveda Pharmaceuticals and ModeRNA; personal fees and non-financial support from Accure Health and Lumicell; and non-financial support from T2Biosystems (Shareholder), outside the submitted work. BJM declares no competing interests.
References
- 1.Seidlin SM, Marinelli LD, Oshry E. Radioactive iodine therapy; effect on functioning metastases of adenocarcinoma of the thyroid. J Am Med Assoc 1946; 132: 838–47. [DOI] [PubMed] [Google Scholar]
- 2.Bentzen SM. Theragnostic imaging for radiation oncology: dose-painting by numbers. Lancet Oncol 2005; 6: 112–17. [DOI] [PubMed] [Google Scholar]
- 3.Baumann M, Krause M, Overgaard J, et al. Radiation oncology in the era of precision medicine. Nat Rev Cancer 2016; 16: 234–49. [DOI] [PubMed] [Google Scholar]
- 4.Kim H, Beack S, Han S, et al. Multifunctional photonic nanomaterials for diagnostic, therapeutic, and theranostic applications. Adv Mater 2018; 30: 30. [DOI] [PubMed] [Google Scholar]
- 5.Mallidi S, Spring BQ, Hasan T. Optical imaging, photodynamic therapy and optically triggered combination treatments. Cancer J 2015; 21: 194–205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Jokerst JV, Gambhir SS. Molecular imaging with theranostic nanoparticles. Acc Chem Res 2011; 44: 1050–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Li J, Liu F, Gupta S, Li C. Interventional nanotheranostics of pancreatic ductal adenocarcinoma. Theranostics 2016; 6: 1393–402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Fahey FH, Grant FD, Thrall JH. Saul Hertz, MD, and the birth of radionuclide therapy. EJNMMI Phys 2017; 4: 15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hertz B A tribute to Dr. Saul Hertz: the discovery of the medical uses of radioiodine. World J Nucl Med 2019; 18: 8–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Luster M, Clarke SE, Dietlein M, et al. Guidelines for radioiodine therapy of differentiated thyroid cancer. Eur J Nucl Med Mol Imaging 2008; 35: 1941–59. [DOI] [PubMed] [Google Scholar]
- 11.Hofman MS, Violet J, Hicks RJ, et al. [177Lu]-PSMA-617 radionuclide treatment in patients with metastatic castration-resistant prostate cancer (LuPSMA trial): a single-centre, single-arm, phase 2 study. Lancet Oncol 2018; 19: 825–33. [DOI] [PubMed] [Google Scholar]
- 12.Markou P, Chatzopoulos D. Yttrium-90 silicate radiosynovectomy treatment of painful synovitis in knee osteoarthritis. Results after 6 months. Hell J Nucl Med 2009; 12: 33–36. [PubMed] [Google Scholar]
- 13.Dolgin E Radioactive drugs emerge from the shadows to storm the market. Nat Biotechnol 2018; 36: 1125–27. [DOI] [PubMed] [Google Scholar]
- 14.Sherman M, Levine R. Nuclear medicine and Wall Street: an evolving relationship. J Nucl Med 2019; 60 (suppl 2): 20S–24S. [DOI] [PubMed] [Google Scholar]
- 15.Schaffert S, Herrmann K. A conversation between Susanne Schaffert and Ken Herrmann. J Nucl Med 2019; 60: 875–78. [DOI] [PubMed] [Google Scholar]
- 16.Banerjee S, Pillai MR, Knapp FF. Lutetium-177 therapeutic radiopharmaceuticals: linking chemistry, radiochemistry, and practical applications. Chem Rev 2015; 115: 2934–74. [DOI] [PubMed] [Google Scholar]
- 17.Nagarajah J, Janssen M, Hetkamp P, Jentzen W. Iodine symporter targeting with 124I/131I theranostics. J Nucl Med 2017; 58 (suppl 2): 34S–38S. [DOI] [PubMed] [Google Scholar]
- 18.Witzig TE, Gordon LI, Cabanillas F, et al. Randomized controlled trial of yttrium-90-labeled ibritumomab tiuxetan radioimmunotherapy versus rituximab immunotherapy for patients with relapsed or refractory low-grade, follicular, or transformed B-cell non-Hodgkin’s lymphoma. J Clin Oncol 2002; 20: 2453–63. [DOI] [PubMed] [Google Scholar]
- 19.Kaminski MS, Estes J, Zasadny KR, et al. Radioimmunotherapy with iodine (131)I tositumomab for relapsed or refractory B-cell non-Hodgkin lymphoma: updated results and long-term follow-up of the University of Michigan experience. Blood 2000; 96: 1259–66. [PubMed] [Google Scholar]
- 20.Green DJ, Press OW. Whither radioimmunotherapy: to be or not to be? Cancer Res 2017; 77: 2191–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Parker C, Nilsson D, Heinrich SI, et al. Alpha Emitter Radium-223 and survival in metastatic prostate cancer. N Engl J Med 2013; 369: 213–23. [DOI] [PubMed] [Google Scholar]
- 22.Parker C, Gillessen S, Heidenreich A, et al. Cancer of the prostate: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2015; 26 (suppl 5): 69–77. [DOI] [PubMed] [Google Scholar]
- 23.Mohler JL, Armstrong AJ, Bahson RR, et al. Prostate cancer, version 1.2016. J Natl Compr Canc Netw 2016; 14: 19–30. [DOI] [PubMed] [Google Scholar]
- 24.Fanti S, Minozzi S, Antoch G, et al. Consensus on molecular imaging and theranostics in prostate cancer. Lancet Oncol 2018; 19: e696–708. [DOI] [PubMed] [Google Scholar]
- 25.Levine R, Krenning EP. Clinical history of the theranostic radionuclide approach to neuroendocrine tumors and other types of cancer: historical review based on an interview of Eric P. Krenning by Rachel Levine. J Nucl Med 2017; 58 (suppl 2): 3S–9S. [DOI] [PubMed] [Google Scholar]
- 26.Strosberg J, El-Haddad G, Wolin E, et al. Phase 3 trial of 177Lu-dotatate for midgut neuroendocrine tumors. N Engl J Med 2017; 376: 125–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Strosberg J, Wolin E, Chasen B, et al. Health-related quality of life in patients with progressive midgut neuroendocrine tumors treated with 177Lu-dotatate in the phase III NETTER-1 trial. J Clin Oncol 2018; 36: 2578–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rudisile S, Gosewisch A, Wenter V, et al. Salvage PRRT with 177Lu-DOTA-octreotate in extensively pretreated patients with metastatic neuroendocrine tumor (NET): dosimetry, toxicity, efficacy, and survival. BMC Cancer 2019; 19: 788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Mc Ewan A, Wieler M, Makis W, et al. Induction and maintenance regimen with peptide receptor radionuclide therapy (PRRT) Lu-177-DOTA-TATE (Lu-177) in patients with advanced neuroendocrine tumours (NET). Neuroendocrinology 2016; 103: 94–94. [Google Scholar]
- 30.Rahbar K, Boegemann M, Yordanova A, et al. PSMA targeted radioligandtherapy in metastatic castration resistant prostate cancer after chemotherapy, abiraterone and/or enzalutamide. A retrospective analysis of overall survival. Eur J Nucl Med Mol Imaging 2018; 45: 12–19. [DOI] [PubMed] [Google Scholar]
- 31.Kim YJ, Kim YI. Therapeutic responses and survival effects of 177Lu-PSMA-617 radioligand therapy in metastatic castrate-resistant prostate cancer: a meta-analysis. Clin Nucl Med 2018; 43: 728–34. [DOI] [PubMed] [Google Scholar]
- 32.Pryma DA, Chin BB, Noto RB, et al. Efficacy and safety of high-specific-activity 131I-MIBG therapy in patients with advanced pheochromocytoma or paraganglioma. J Nucl Med 2019; 60: 623–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Blakkisrud J, Holtedahl JE, Løndalen A, et al. Biodistribution and dosimetry results from a phase 1 trial of therapy with the antibody-radionuclide conjugate 177Lu-lilotomab satetraxetan. J Nucl Med 2018; 59: 704–10. [DOI] [PubMed] [Google Scholar]
- 34.Pandit-Taskar N, Zanzonico PB, Kramer K, et al. Biodistribution and dosimetry of intraventricularly administered 124I-omburtamab in patients with metastatic leptomeningeal tumors. J Nucl Med 2019; 60: 1794–801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Souweidane MM, Kramer K, Pandit-Taskar N, et al. Convection-enhanced delivery for diffuse intrinsic pontine glioma: a single-centre, dose-escalation, phase 1 trial. Lancet Oncol 2018; 19: 1040–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Bodei L, Kidd M, Paganelli G, et al. Long-term tolerability of PRRT in 807 patients with neuroendocrine tumours: the value and limitations of clinical factors. Eur J Nucl Med Mol Imaging 2015; 42: 5–19. [DOI] [PubMed] [Google Scholar]
- 37.Marinova M, Mücke M, Fischer F, et al. Quality of life in patients with midgut NET following peptide receptor radionuclide therapy. Eur J Nucl Med Mol Imaging 2019; 46: 2252–59. [DOI] [PubMed] [Google Scholar]
- 38.Fendler WP, Reinhardt S, Ilhan H, et al. Preliminary experience with dosimetry, response and patient reported outcome after 177Lu-PSMA-617 therapy for metastatic castration-resistant prostate cancer. Oncotarget 2017; 8: 3581–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Waissi F, Kist JW, Lodewijk L, et al. Fast-track radioiodine ablation therapy after thyroidectomy reduces sick leave in patients with differentiated thyroid cancer (FASTHYNA trial). Clin Nucl Med 2019; 44: 272–75. [DOI] [PubMed] [Google Scholar]
- 40.Nilsson S, Cislo P, Sartor O, et al. Patient-reported quality-of-life analysis of radium-223 dichloride from the phase III ALSYMPCA study. Ann Oncol 2016; 27: 868–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Lange R, Overbeek F, de Klerk JM, et al. Treatment of painful bone metastases in prostate and breast cancer patients with the therapeutic radiopharmaceutical rhenium-188-HEDP. Clinical benefit in a real-world study. Nuklearmedizin 2016; 55: 188–95. [DOI] [PubMed] [Google Scholar]
- 42.Verburg FA, Wiessmann M, Neuloh G, Mottaghy FM, Brockmann MA. Intraindividual comparison of selective intraarterial versus systemic intravenous 68Ga-dotatate PET/CT in patients with inoperable meningioma. Nuklearmedizin 2019; 58: 23–27. [DOI] [PubMed] [Google Scholar]
- 43.Spyridonidis T, Spyridonidis J, Papathanasiou N, Katsanos K. History and development of radioembolization: an old idea with modern applications. Nucl Med Commun 2019; 40: 684–92. [DOI] [PubMed] [Google Scholar]
- 44.Saini A, Wallace A, Alzubaidi S, et al. History and evolution of yttrium-90 radioembolization for hepatocellular carcinoma. J Clin Med 2019; 8: 8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Singh A, Zhang J, Kulkarni H, Baum R. Intra-arterial PRRT of SSTR-expressing tumors in patients with hepatic only versus extrahepatic tumor: efficacy and safety evaluation. J Nucl Med 2019; 60: 625. [Google Scholar]
- 46.Limouris GS, Karfis I, Chatzioannou A, et al. Super-selective hepatic arterial infusions as established technique (‘ARETAIEION’ Protocol) of [177Lu]DOTA-TATE in inoperable neuroendocrine liver metastases of gastro-entero-pancreatic (GEP) tumors. Q J Nucl Med Mol Imaging 2012; 56: 551–58. [PubMed] [Google Scholar]
- 47.Cornelis FH, Durack JC, Morris MJ, Scher HI, Solomon SB. Effective prostate-specific membrane antigen-based 18F-DCFPyL-guided cryoablation of a single positive site in a patient believed to be more metastatic on 11C-choline PET/CT. Clin Nucl Med 2017; 42: e516–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Lohaus F, Zöphel K, Löck S, et al. Can local ablative radiotherapy revert castration-resistant prostate cancer to an earlier stage of disease? Eur Urol 2019; 75: 548–51. [DOI] [PubMed] [Google Scholar]
- 49.Bartolomei M, Bodei L, De Cicco C, et al. Peptide receptor radionuclide therapy with (90)Y-DOTATOC in recurrent meningioma. Eur J Nucl Med Mol Imaging 2009; 36: 1407–16. [DOI] [PubMed] [Google Scholar]
- 50.Mak IYF, Hayes AR, Khoo B, Grossman A. Peptide receptor radionuclide therapy as a novel treatment for metastatic and invasive phaeochromocytoma and paraganglioma. Neuroendocrinology 2019; 109: 287–98. [DOI] [PubMed] [Google Scholar]
- 51.Kesler M, Levine C, Hershkovitz D, et al. 68Ga-PSMA is a novel PET-CT tracer for imaging of hepatocellular carcinoma: a prospective pilot study. J Nucl Med 2018; 60: 185–91. [DOI] [PubMed] [Google Scholar]
- 52.van Vliet EI, van Eijck CH, de Krijger RR, et al. Neoadjuvant treatment of nonfunctioning pancreatic neuroendocrine tumors with [177Lu-DOTA0,Tyr3]octreotate. J Nucl Med 2015; 56: 1647–53. [DOI] [PubMed] [Google Scholar]
- 53.Hofman MS. PSMA targeted therapies. Advanced Prostate Cancer Consensus Conference 2019; Basel, Switzerland; Aug 29–31, 2019. [Google Scholar]
- 54.Cheever MA, Allison JP, Ferris AS, et al. The prioritization of cancer antigens: a national cancer institute pilot project for the acceleration of translational research. Clin Cancer Res 2009; 15: 5323–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Herrmann K, Schottelius M, Lapa C, et al. First-in-human experience of CXCR4-directed endoradiotherapy with 177Lu- and 90Y-labeled pentixather in advanced-stage multiple myeloma with extensive intra- and extramedullary disease. J Nucl Med 2016; 57: 248–51. [DOI] [PubMed] [Google Scholar]
- 56.Lindner T, Loktev A, Altmann A, et al. Development of quinoline-based theranostic ligands for the targeting of fibroblast activation protein. J Nucl Med 2018; 59: 1415–22. [DOI] [PubMed] [Google Scholar]
- 57.Lee ST, Burvenich I, Scott AM. Novel target selection for nuclear medicine studies. Semin Nucl Med 2019; 49: 357–68. [DOI] [PubMed] [Google Scholar]
- 58.Kratochwil C, Bruchertseifer F, Rathke H, et al. Targeted α-therapy of metastatic castration-resistant prostate cancer with 225Ac-PSMA-617: swimmer-plot analysis suggests efficacy regarding duration of tumor control. J Nucl Med 2018; 59: 795–802. [DOI] [PubMed] [Google Scholar]
- 59.Zeglis BM, Sevak KK, Reiner T, et al. A pretargeted PET imaging strategy based on bioorthogonal Diels-Alder click chemistry. J Nucl Med 2013; 54: 1389–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Rossin R, Verkerk PR, van den Bosch SM, et al. In vivo chemistry for pretargeted tumor imaging in live mice. Angew Chem Int Ed Engl 2010; 49: 3375–78. [DOI] [PubMed] [Google Scholar]
- 61.Devaraj NK, Thurber GM, Keliher EJ, Marinelli B, Weissleder R. Reactive polymer enables efficient in vivo bioorthogonal chemistry. Proc Natl Acad Sci USA 2012; 109: 4762–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Poty S, Carter LM, Mandleywala K, et al. Leveraging bioorthogonal click chemistry to improve 225Ac-radioimmunotherapy of pancreatic ductal adenocarcinoma. Clin Cancer Res 2019; 25: 868–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Langbein T, Weber WA, Eiber M. Future of theranostics: an outlook on precision oncology in nuclear medicine. J Nucl Med 2019; 60 (suppl 2): 13S–19S. [DOI] [PubMed] [Google Scholar]
- 64.Sathianathen NJ, Krishna S, Konety BR, Griffith TS. The synergy between ionizing radiation and immunotherapy in the treatment of prostate cancer. Immunotherapy 2017; 9: 1005–18. [DOI] [PubMed] [Google Scholar]
- 65.Dietrich A, Koi L, Zöphel K, et al. Improving external beam radiotherapy by combination with internal irradiation. Br J Radiol 2015; 88: 20150042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Garske-Román U, Sandström M, Fröss Baron K, et al. Prospective observational study of 177Lu-DOTA-octreotate therapy in 200 patients with advanced metastasized neuroendocrine tumours (NETs): feasibility and impact of a dosimetry-guided study protocol on outcome and toxicity. Eur J Nucl Med Mol Imaging 2018; 45: 970–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Eberlein U, Cremonesi M, Lassmann M. Individualized dosimetry for theranostics: necessary, nice to have, or counterproductive? J Nucl Med 2017; 58 (suppl 2): 97S–103S. [DOI] [PubMed] [Google Scholar]
- 68.Yonekura Y, Mattsson S, Flux G, et al. ICRP publication 140: Radiological protection in therapy with radiopharmaceuticals. Ann ICRP 2019; 48: 5–95. [DOI] [PubMed] [Google Scholar]
- 69.Wibmer AG, Hricak H, Ulaner GA, Weber W. Trends in oncologic hybrid imaging. Eur J Hybrid Imaging 2018; 2: 1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Committee on State of the Science of Nuclear Medicine, et al. Advancing nuclear medicine through innovation. Washington, DC: National Academies Press (US); 2007. [PubMed] [Google Scholar]
- 71.Czernin J Toward independent nuclear medicine, molecular imaging, and theranostic programs. J Nucl Med 2019; 60: 1037. [DOI] [PubMed] [Google Scholar]
- 72.Ahmadzadehfar H, Essler M. It is time to move forward into the era of theranostics. EJNMMI Res 2018; 8: 9. [DOI] [PMC free article] [PubMed] [Google Scholar]