

Abstract
Background:
Fragmentation of care, wherein a patient is readmitted to a hospital different from the initial point of care, has been shown to be associated with worse patient outcomes in other medical specialties. However, postpartum fragmentation of care has not been well characterized in obstetrics.
Objective:
To characterize risk for and outcomes associated with fragmentation of postpartum readmissions wherein the readmitting hospital is different than the delivery hospital.
Methods:
The 2010 to 2014 Nationwide Readmissions Database (NRD) was used for this retrospective cohort study. Postpartum readmissions within 60-days of delivery hospitalization discharge for women aged 15–54 years were identified. The primary outcome, fragmentation, was defined as readmission to a different hospital than the delivery hospital. Hospital, demographic, medical, and obstetric factors associated with fragmented readmission were analyzed. Adjusted log-linear models were performed to analyze risk for readmission with adjusted risk ratios (aRR) and 95% confidence intervals (CI) as the measures of effect. The associations between fragmentation and secondary outcomes including (i) length of stay >90th percentile, (ii) hospitalization costs >90th percentile, and (iii) severe maternal morbidity were determined. Whether specific indications for readmission such as hypertensive diseases of pregnancy, wound complications, and other conditions were associated with higher or lower risk for fragmentation was analyzed.
Results:
From 2010–2014, 141,276 60-day postpartum readmissions were identified of which 15% of readmissions (n=21,789) occurred at a hospital different from where the delivery occurred. Evaluating individual readmission indications, fragmentation was less likely for hypertension (11.1%), wound complications (10.7%), and uterine infections (11.0%), and more likely for heart failure (28.6%), thromboembolism (28.4%), and upper respiratory infections (33.9%) (p<0.01 for all). In the adjusted analysis, factors associated with fragmentation included public insurance compared to private insurance (Medicare: aRR 1.68, 95% CI 1.52, 1.86; Medicaid: aRR 1.28, 95% CI 1.24, 1.32). Fragmentation was associated with increased risk for severe maternal morbidity during readmissions in both unadjusted (relative risk 1.84, 95% CI 1.79, 1.89) and adjusted (aRR 1.81, 95% CI 1.76, 1.86) analyses. In adjusted analyses, fragmentation was also associated with increased risk for length of stay >90th percentile (relative risk 1.48, 95% CI 1.42–1.54) and hospitalization costs >90th percentile (aRR 1.74, 95% CI 1.67, 1.81).
Conclusion:
This study of nationwide estimates of postpartum fragmentation found discontinuity of postpartum care was associated for increased risk for severe morbidity, high costs, and long length of stay. Reduction of fragmentation may represent an important goal in overall efforts to improve postpartum care.
INTRODUCTION
Childbirth is the most common indication for hospitalization in the United States with approximately four million births annually and related costs of $19.1 billion.1 Across medical specialties optimizing coordination of care after hospitalization discharge has become an important focus in safety and quality.2,3 Specific to obstetrics, the American College of Obstetrics and Gynecology (ACOG) recently released recommendations to improve and optimize postpartum care after delivery hospitalization discharge.4 Numerous studies in recent years have analyzed risk factors for and overall epidemiology of readmissions in the postpartum setting;5–9 however, little to no evidence exists regarding whether readmission to a different hospital than where the delivery occurred affects outcomes in obstetrics.
Fragmentation of care, wherein a patient is readmitted to a hospital different from the initial point of care, has been shown to be associated with worse patient outcomes in other medical specialties.10–12 Fragmentation after delivery may be of clinical importance in obstetrics; the readmitting hospital may not be privy to key medical information related to the patient’s medical history, prenatal course, and delivery. Absent medical records, the readmitting hospital may have limited information on factors such as hypertensive disease of pregnancy (HDP), intrauterine infection, retained products of conception, and operative complications.
Given that obstetric fragmentation is of possible clinical significance, the purpose of this study was to characterize fragmentation on a population basis. The objectives of this study were: (i) to estimate the prevalence of fragmentation of postpartum care in a nationally representative sample, (ii) to investigate the demographic, clinical, and hospital predictors of fragmentation, and (iii) to determine the impact of fragmentation on risk of severe maternal morbidity, hospital length of stay, and cost.
METHODS
Data Source
Data from the 2010 to 2014 Nationwide Readmissions Database (NRD) were utilized for this study. The NRD is one of the largest all payer databases assembled annually by the Agency for Healthcare Research and Quality’s Healthcare Cost and Utilization Project.13 Hospital admissions for individual patients are tracked on a state level within a given year.13 The data contains weights that allow for the calculation of national readmission estimates for both insured and uninsured patients. As of 2014, 22 states accounting for 51% of US residents and 49% of US hospitalizations were included in the NRD.13 This study was granted IRB exemption by both the Columbia University and University of Southern California Institutional Review Boards as the data is de-identified and publicly available.
Study Population
Readmissions for obstetric and postpartum indications within 60-days of delivery hospitalization discharge for women aged 15–54 years were identified. Delivery hospitalizations were identified utilizing International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9CM) diagnosis codes of 650 and V27.x; these codes capture >95% of all deliveries.14 All delivery hospitalizations including preterm births and stillbirths were included. We identified readmissions for obstetric and postpartum indications based on primary ICD-9CM diagnosis and procedure codes. Admission indications included (i) sepsis, (ii) heart failure, (iii) wound complications, (iv) hemorrhage, (v) breast complications, (vi) urinary tract infection, (vii) uterine infections, (viii) hypertensive disorders, (ix) thrombotic disorders, (x) upper respiratory infection, (xi) dilation and curettage, (xii) hysterectomy, (xiii) transfusion, and (xiv) laparotomy. Prior studies evaluating postpartum readmissions have included psychiatric, gallbladder disease, and appendicitis diagnoses;7 because these indications for admission may not have been related to postpartum care or may have been more likely to be planned to occur at a different hospital than the delivery hospital they were not included in this analysis.
Within the NRD patients have a unique identifier that allows tracking across multiple hospitalizations within a given state within a calendar year. Only admissions from January through October were included as the NRD is assembled annually and cannot be linked across years; delivery hospitalizations during November and December were not included because readmissions for the subsequent 60 days cannot be fully ascertained. Readmissions were categorized as either occurring at the same hospital as the delivery hospitalization discharge or as fragmented and occurring at a different hospital. For patients with >1 readmission, only the first readmission within 60 days of discharge was included in the analysis.
Outcomes
The primary outcome for this analysis was readmission fragmentation. Both unadjusted and adjusted analyses with demographic, hospital, and obstetric and medical factors with fragmentation as the outcome were performed. In addition to the primary outcome, we performed several secondary outcome analyses. First, we evaluated whether readmissions for specific indications were more or less likely to be fragmented. Individual indications for postpartum readmissions were determined using a previously described algorithm based on ICD-9-CM procedure and diagnosis codes excluding diagnoses for appendicitis, gallbladder disease, and psychiatric indications.7 For each indication for readmission, this analysis determined the proportion of readmissions that were fragmented.
Second, this analysis assessed risk for severe maternal morbidity during readmissions and whether fragmentation was associated with increased risk for this outcome. Severe maternal morbidity (SMM) was based on criteria from the Centers for Disease Control and Prevention (CDC). The CDC composite includes ICD-9-CM codes for 18 conditions including eclampsia, stroke, renal failure, hysterectomy, thromboembolism, heart failure, and blood transfusion.15 Readmissions with and without fragmentation were compared with the CDC’s severe maternal morbidity criteria as the outcome. For the SMM analysis, patients with SMM during their delivery admission were excluded to avoid misclassification.
Third, we evaluated risk for high readmission costs and prolonged length of stay and determined whether fragmentation was associated with increased risk for these outcomes. High readmission cost was defined as cost >90th percentile (≥$11,594.72). Prolonged readmission length of stay (pRLOS) was defined as length of readmission stay >90th percentile (≥5 days).
Fourth, we performed a set of ancillary analyses. As the first ancillary analysis we evaluated maternal mortality risk comparing fragmented versus non-fragmented readmissions. Second, because fragmentation may to some degree be a proxy for regionalization of care, we analyzed the proportion of readmitted women who were transferred during their delivery hospitalization to determine to what degree outgoing transfers on a hospital-level may be associated with readmission fragmentation. Third, because postpartum hemorrhage and preeclampsia may be highly predictive of SMM we performed a sensitivity analysis excluding these factors as SMM predictors.
Patient, Hospital, and Clinical Factors
Demographic, hospital, and clinical factors from the delivery hospitalization were included in the analysis. Patient factors including payer status (Medicare, Medicaid, private insurance, self-pay, no charge, and other), median income quartile by ZIP code, and patient age (categorized as 15–19, 20–24, 25–29, 30–34, 35–39, 40–54 years old). Hospital factors included hospital bed size (small, medium, large) and teaching status (metropolitan teaching, non-teaching, and non-metropolitan). Clinical factors from the delivery hospitalization were identified using ICD-9-CM codes and included: cesarean delivery, pregestational diabetes, gestational diabetes, postpartum hemorrhage, systemic lupus erythematosus, multiple gestation, asthma, chronic kidney disease, hypertensive diseases of pregnancy, and chronic hypertension.
Statistical Analysis
Demographic analyses were conducted to describe the differences in the baseline characteristics stratified by fragmentation (same-hospital readmission versus fragmented readmission) status. For our primary analysis, we determined the association between the aforementioned patient, hospital, and clinical factors and risk for fragmentation. Univariable log-linear regression models with a Poisson distribution were fit with unadjusted risk ratios (RR) and 95% confidence intervals (CI) as the measures of association. Adjusted multivariable log-linear regression models including all the demographic, hospital, and obstetric and medical factors were performed with fragmented readmission as the primary outcome and adjusted risk ratios (aRR) with 95% CIs as the measure of association. Because transfer to other facilities could affect readmission outcomes, a sensitivity analysis was performed restricted to only patients with routine discharges; routine discharge excludes transfers to other hospitals and skilled nursing facilities. Adjusted log linear regression models including the same demographic, hospital, and clinical factors as the primary analysis along with fragmented readmission added as a risk factor were additionally performed for the three following secondary outcomes: (i) severe maternal morbidity, (ii) high readmission costs >90th percentile, and (iii) and prolonged lengths of stay >90th percentile. Costs were calculated utilizing NRD provided cost-to-charge ratios and adjusted for the cost of inflation to represent 2016 dollars using the Consumer Price Index.16 Because specific indication for readmission could be associated with cost, length of stay, and risk for severe morbidity, sensitivity analyses were performed repeating the adjusted models with indication for admission as a risk factor. All analyses were performed with SAS 9.4 (SAS Institute, Cary, NC).
RESULTS
From 2010–2014, 141,276 60-day postpartum readmissions were identified. 15.4% of readmissions (n=21,789) involved fragmented care where the readmission hospital was different than the delivery hospital (Table 1). Fragmented readmissions had longer mean length of stay (3.5 versus 2.9 days, p<0.01) and higher total mean readmission costs ($8,499 versus $5,764, p<0.01) compared to same-hospital readmissions (Table 2). Fragmented readmissions had higher rates of SMM (32.4% vs. 17.5%, p<0.01), prolonged length of stay (13.4% vs. 8.9%, p<0.01), and high readmission costs (14.9% vs. 8.4%, p<0.01).
Table 1.
Demographics and outcomes of women with 60 day postpartum readmissions
| Readmission hospital | Same hospital as delivery | Different hospital than delivery | P value | ||
|---|---|---|---|---|---|
| N | % | N | % | ||
| Severe maternal morbidity (readmission) | 19,636 | 17.5% | 6,465 | 32.4% | <0.01 |
| Prolonged length of stay | 10,671 | 8.9% | 2,930 | 13.4% | <0.01 |
| High readmission costs | 10,069 | 8.4% | 3,248 | 14.9% | <0.01 |
| Maternal age in years | |||||
| 15–19 years old | 10,519 | 8.8% | 2,034 | 9.3% | <0.01 |
| 20–24 years old | 25,935 | 21.7% | 5,631 | 25.8% | |
| 25–29 years old | 31,235 | 26.1% | 5,760 | 26.4% | |
| 30–34 years old | 29,338 | 24.6% | 4,872 | 22.4% | |
| 35–39 years old | 16,968 | 14.2% | 2,664 | 12.2% | |
| 40–54 years old | 5,492 | 4.6% | 828 | 3.8% | |
| Payer | |||||
| Medicare | 1,433 | 1.2% | 398 | 1.8% | <0.01 |
| Medicaid | 58,616 | 49.1% | 12,325 | 56.6% | |
| Private insurance | 53,992 | 45.2% | 8,096 | 37.2% | |
| Self-pay | 1,501 | 1.3% | 284 | 1.3% | |
| No charge | 64 | 0.1% | 18 | 0.1% | |
| Other | 3,473 | 2.9% | 595 | 2.7% | |
| Missing | 409 | 0.3% | 71 | 0.3% | |
| Median ZIP code income quartile | |||||
| Lowest income quartile | 39,124 | 32.7% | 7,516 | 34.5% | <0.01 |
| 2nd lowest quartile | 29,097 | 24.4% | 5,548 | 25.5% | |
| 2nd highest quartile | 27,802 | 23.3% | 4,779 | 21.9% | |
| Highest income quartile | 22,218 | 18.6% | 3,712 | 17.0% | |
| Delivery postpartum hemorrhage | 6,635 | 5.6% | 1,261 | 5.8% | 0.47 |
| Cesarean delivery | 62,186 | 52.0% | 10,559 | 48.5% | <0.01 |
| Pregestational diabetes | 2,954 | 2.5% | 564 | 2.6% | 0.37 |
| Gestational diabetes | 10,199 | 8.5% | 1,755 | 8.1% | <0.01 |
| Systemic lupus erythematosus | 455 | 0.4% | 129 | 0.6% | 0.01 |
| Multiple gestation | 4,909 | 4.1% | 739 | 3.4% | <0.01 |
| Asthma | 7,213 | 6.0% | 1,276 | 5.9% | 0.58 |
| Chronic kidney disease | 887 | 0.7% | 243 | 1.1% | <0.01 |
| Hypertensive diseases of pregnancy | 25,519 | 21.4% | 3,873 | 17.8% | <0.01 |
| Chronic hypertension | 5,596 | 4.7% | 885 | 4.1% | <0.01 |
| Hospital bed size | |||||
| Small | 11,096 | 9.3% | 2,646 | 12.2% | <0.01 |
| Medium | 30,206 | 25.3% | 5,825 | 26.7% | |
| Large | 78,186 | 65.4% | 13,316 | 61.1% | |
| Hospital teaching status | |||||
| Metropolitan non-teaching | 38,869 | 32.5% | 7,879 | 36.2% | <0.01 |
| Metropolitan teaching | 68,496 | 57.3% | 11,682 | 53.6% | |
| Non-metropolitan | 12,123 | 10.2% | 2,227 | 10.2% | |
Hypertensive disease of pregnancy include gestational hypertension and preeclampsia diagnoses.
Table 2.
Readmission costs and length of stay
| Readmission | Same hospital as delivery | Different hospital than delivery | ||
|---|---|---|---|---|
| Mean | 95% CI | Mean | 95% CI | |
| Readmission length of stay, days | 2.91 | 2.88, 2.94 | 3.46 | 3.36, 3.55 |
| Readmission total costs | $5,764 | $5,760, $5,858 | $8,499 | $8,130, $8,868 |
| Median | IQR | Median | IQR | |
| Readmission length of stay, days | 1.81 | 1.08–2.96 | 1.96 | 1.11–3.52 |
| Readmission total costs | $3,981 | $2,431-$6,574 | $5,096.95 | $3,277.45-$8,444 |
CI, confidence interval. IQR, interquartile range
In unadjusted analyses, younger age compared to women 25–29 years old (20–24 years old: RR 1.15, 95% CI 1.10, 1.19), public insurance compared to private insurance (Medicare: RR 1.67, 95% CI 1.51, 1.84; Medicaid: RR 1.33, 95% CI 1.30, 1.37), and lower ZIP code income quartiles compared to the top quartile (lowest quartile: RR 1.13, 95% CI 1.08, 1.17; second lowest quartile: RR 1.12, 95% CI 1.07, 1.17) were associated with higher risk of fragmented readmission compared to their reference groups. In comparison, women 30 and older were at lower risk for fragmented readmission compared to women 25–29 (Table 3). Medical and obstetric risk factors associated with increased risk for fragmentation included systemic lupus erythematosus and chronic kidney disease. Factors associated with decreased fragmentation included cesarean delivery, multiple gestation, hypertensive diseases of pregnancy, and chronic hypertension (Table 3). Patients delivering at larger hospitals, teaching, and non-metropolitan hospitals were also at significantly decreased risk for fragmentation (Table 3).
Table 3.
Unadjusted and adjusted analysis for readmission to a different hospital than the delivery hospital among women readmitted 60 days postpartum
| Unadjusted model | Adjusted model | |||
|---|---|---|---|---|
| RR | 95% CI | aRR | 95% CI | |
| Maternal age | ||||
| 15–19 years old | 1.04 | 0.99, 1.09 | 0.98 | 0.93, 1.03 |
| 20–24 years old | 1.15 | 1.10, 1.19 | 1.09 | 1.05, 1.14 |
| 25–29 years old | Reference | Reference | ||
| 30–34 years old | 0.91 | 0.88, 0.95 | 0.96 | 0.92, 1.00 |
| 35–39 years old | 0.87 | 0.83, 0.91 | 0.93 | 0.89, 0.98 |
| 40–54 years old | 0.84 | 0.78, 0.91 | 0.92 | 0.85, 0.99 |
| Payer | ||||
| Medicare | 1.67 | 1.51, 1.84 | 1.68 | 1.52, 1.86 |
| Medicaid | 1.33 | 1.30, 1.37 | 1.28 | 1.24, 1.32 |
| Private insurance | Reference | Reference | ||
| Self-pay | 1.22 | 1.08, 1.37 | 1.19 | 1.06, 1.34 |
| No charge | 1.72 | 1.09, 2.72 | 1.57 | 0.99, 2.47 |
| Other | 1.12 | 1.03, 1.22 | 1.07 | 0.98, 1.16 |
| Median ZIP code income quartile | ||||
| Lowest income quartile | 1.13 | 1.08, 1.17 | 1.01 | 0.96, 1.05 |
| 2nd lowest quartile | 1.12 | 1.07, 1.17 | 1.01 | 0.97, 1.06 |
| 2nd highest quartile | 1.02 | 0.98, 1.07 | 0.96 | 0.92, 1.00 |
| Highest income quartile | Reference | Reference | ||
| Delivery postpartum hemorrhage | 1.04 | 0.98, 1.1 | 1.05 | 0.99, 1.11 |
| Cesarean delivery | 0.89 | 0.86, 0.91 | 0.90 | 0.87, 0.92 |
| Pregestational diabetes | 1.04 | 0.95, 1.13 | 1.11 | 1.02, 1.21 |
| Gestational diabetes | 0.95 | 0.90, 1.00 | 1.01 | 0.97, 1.07 |
| Systemic lupus erythematosus | 1.44 | 1.21, 1.71 | 1.40 | 1.18, 1.67 |
| Multiple gestation | 0.84 | 0.78, 0.91 | 0.95 | 0.88, 1.02 |
| Asthma | 0.97 | 0.92, 1.03 | 0.98 | 0.92, 1.04 |
| Chronic kidney disease | 1.40 | 1.23, 1.59 | 1.39 | 1.23, 1.59 |
| Hypertensive diseases of pregnancy | 0.82 | 0.79, 0.84 | 0.84 | 0.81, 0.87 |
| Chronic hypertension | 0.84 | 0.79, 0.90 | 0.87 | 0.81, 0.93 |
| Hospital bed size | ||||
| Small | Reference | Reference | ||
| Medium | 0.84 | 0.80, 0.88 | 0.84 | 0.80, 0.88 |
| Large | 0.76 | 0.72, 0.79 | 0.75 | 0.72, 0.79 |
| Hospital teaching status | ||||
| Metropolitan non-teaching | Reference | Reference | ||
| Metropolitan teaching | 0.86 | 0.84, 0.89 | 0.86 | 0.84, 0.89 |
| Non-metropolitan | 0.92 | 0.88, 0.97 | 0.88 | 0.84, 0.92 |
RR, risk ratio. aRR, adjusted risk ratio. CI, confidence interval. Estimates for medical and obstetric conditions are with absence of the condition as the reference. All variables in the table were included in the adjusted analysis.
Upon adjustment, many of these factors retained significance. Maternal age >30 years remained associated with lower risks of readmission compared to maternal age 25 to 29 years. Medicare and Medicaid insurance were also associated with increased risk for readmission in adjusted analyses compared to commercial insurance (Table 3). Clinical factors including delivery cesarean delivery, hypertensive diseases of pregnancy, and chronic hypertension remained associated with lower risks of fragmentation. In comparison, systematic lupus erythematosus and chronic kidney disease which were associated with increased risks of fragmentation (Table 3). Patients delivering at large and medium hospitals were at lower risk of fragmentation compared to smaller hospitals. Similarly, patients seen at metropolitan teaching hospitals (aRR 0.86, 95% CI 0.84, 0.89) and non-metropolitan (aRR 0.88, 95% CI 0.84, 0.92) hospitals were at lower risks of fragmented readmissions compared to metropolitan non-teaching centers. The sensitivity analysis restricted to routine discharge demonstrated similar findings (Supplemental Table 1).
Evaluating individual readmission indications, fragmentation was less likely for hypertension (11.2% of readmissions), wound complications (11.0% of readmissions), and uterine infections (11.1% of readmissions), and more likely for hemorrhage (16.2% of readmissions), transfusion (20.9% of readmissions), thrombotic disorders (28.4% of readmissions) and upper respiratory infections (34.5% readmissions) (p<0.05 for all) (Figure 1, Supplemental Table 2). In the analyses evaluating severe maternal morbidity during readmission, fragmentation was associated with increased risk in both unadjusted (RR 1.84, 95% CI 1.79, 1.89) and adjusted analyses (aRR 1.81, 95% CI 1.76, 1.86) (Table 4). Risk for severe morbidity associated with fragmentation was attenuated but still present in the adjusted model additionally including indication for admission (aRR 1.25, 95% CI 1.21, 1.28). In adjusted analyses for both prolonged length of stay (>90%ile, ≥5 days) and high readmission hospitalization costs (90%ile, ≥$11,594.72), fragmented readmission was associated with increased risk (aRR 1.48, 95% CI 1.42, 1.54; aRR 1.74 95% CI 1.67, 1.81, respectively) (Table 5). In sensitivity analyses additionally adjusting for indication for admission, increased risks for prolonged length of stay (aRR 1.11, 95% CI 1.06, 1.16) and high readmission costs (aRR 1.24, 95% 1.19, 1.29) associated with fragmentation were attenuated but still present.
Figure 1. Risk for fragmentation by readmission diagnosis.
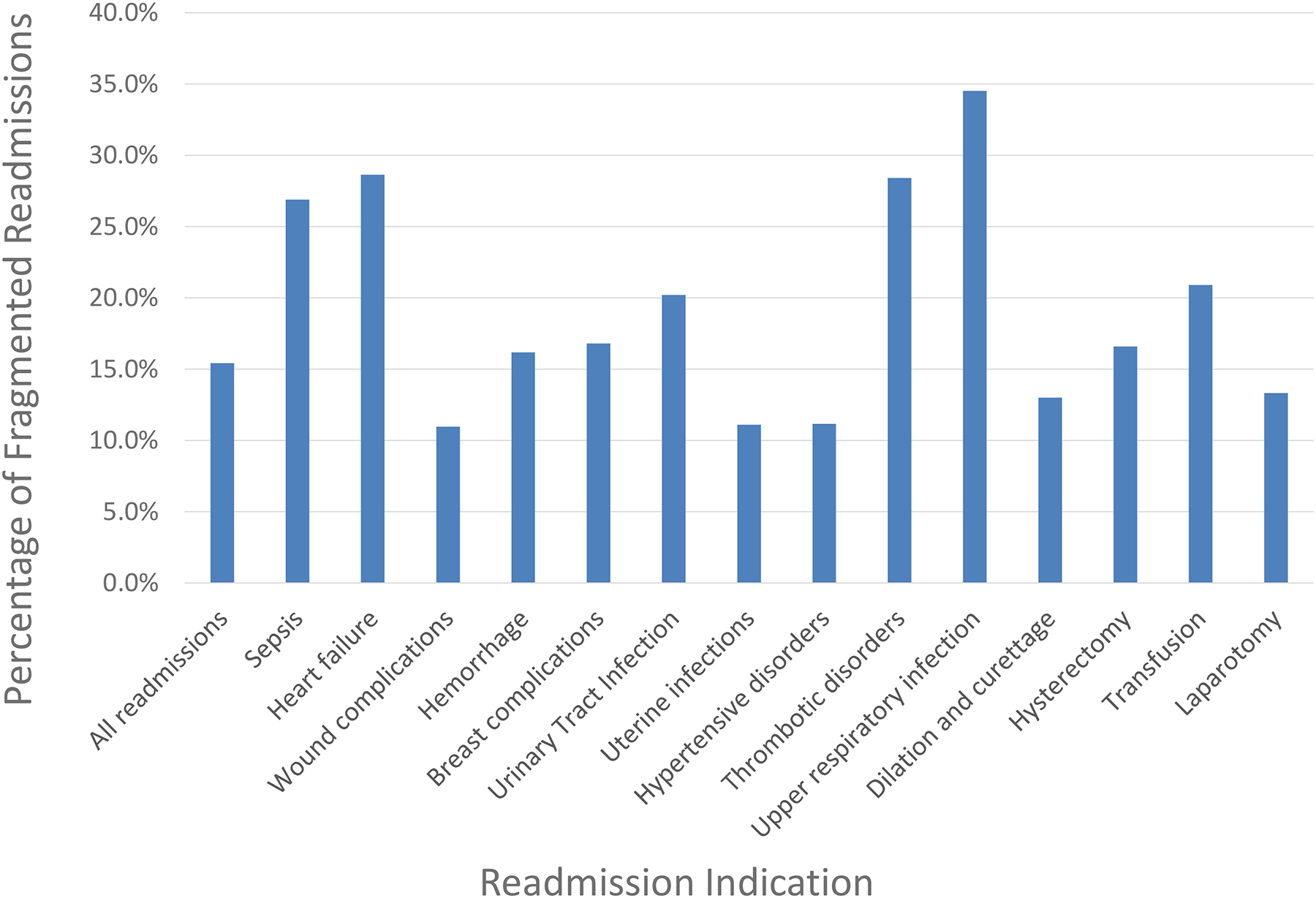
The figure demonstrates the proportion of readmissions that were fragmented (i.e. occurring at a hospital different than the discharge hospital) by the primary indication for readmission.
Table 4.
Unadjusted and adjusted analysis for severe maternal morbidity during postpartum readmission
| Unadjusted model | Adjusted model | |||
|---|---|---|---|---|
| RR | 95% CI | aRR | 95% CI | |
| Readmission to hospital other than delivery hospital | 1.84 | 1.79, 1.89 | 1.81 | 1.76, 1.86 |
| Maternal age | ||||
| 15–19 years old | 1.02 | 0.97, 1.07 | 0.96 | 0.92, 1.01 |
| 20–24 years old | 1.03 | 0.99, 1.06 | 0.97 | 0.94, 1.01 |
| 25–29 years old | Reference | Reference | ||
| 30–34 years old | 0.98 | 0.94, 1.01 | 1.02 | 0.99, 1.06 |
| 35–39 years old | 0.93 | 0.89, 0.97 | 1.00 | 0.96, 1.04 |
| 40–54 years old | 0.99 | 0.93, 1.06 | 1.08 | 1.01, 1.15 |
| Payer | ||||
| Medicare | 1.22 | 1.09, 1.35 | 1.14 | 1.02, 1.27 |
| Medicaid | 1.17 | 1.14, 1.20 | 1.11 | 1.08, 1.14 |
| Private insurance | Reference | Reference | ||
| Self-pay | 1.21 | 1.09, 1.34 | 1.15 | 1.04, 1.28 |
| No charge | 1.35 | 0.85, 2.16 | 1.21 | 0.76, 1.94 |
| Other | 1.01 | 0.93, 1.09 | 0.98 | 0.90, 1.06 |
| Median ZIP code income quartile | ||||
| Lowest income quartile | 1.21 | 1.17, 1.25 | 1.15 | 1.11, 1.20 |
| 2nd lowest quartile | 1.12 | 1.08, 1.17 | 1.08 | 1.04, 1.13 |
| 2nd highest quartile | 1.08 | 1.04, 1.12 | 1.06 | 1.02, 1.11 |
| Highest income quartile | Reference | Reference | ||
| Delivery postpartum hemorrhage | 1.46 | 1.38, 1.54 | 1.48 | 1.40, 1.56 |
| Cesarean delivery | 0.97 | 0.95, 0.99 | 0.99 | 0.96, 1.01 |
| Pregestational diabetes | 1.07 | 0.99, 1.15 | 1.14 | 1.06, 1.23 |
| Gestational diabetes | 1.01 | 0.97, 1.06 | 1.04 | 1.00, 1.09 |
| Systemic lupus erythematosus | 1.13 | 0.93, 1.36 | 1.13 | 0.93, 1.36 |
| Multiple gestation | 1.22 | 1.15, 1.29 | 1.30 | 1.22, 1.38 |
| Asthma | 0.99 | 0.94, 1.04 | 1.01 | 0.96, 1.07 |
| Chronic kidney disease | 1.43 | 1.25, 1.62 | 1.45 | 1.27, 1.65 |
| Hypertensive diseases of pregnancy | 0.85 | 0.83, 0.88 | 0.87 | 0.84, 0.89 |
| Chronic hypertension | 0.70 | 0.65, 0.75 | 0.68 | 0.64, 0.73 |
| Hospital bed size | ||||
| Small | Reference | Reference | ||
| Medium | 1.00 | 0.96, 1.05 | 1.03 | 0.98, 1.08 |
| Large | 0.97 | 0.93, 1.01 | 0.99 | 0.95, 1.03 |
| Hospital teaching status | ||||
| Metropolitan non-teaching | Reference | Reference | ||
| Metropolitan teaching | 0.89 | 0.87, 0.91 | 0.90 | 0.87, 0.92 |
| Non-metropolitan | 1.10 | 1.05, 1.14 | 1.07 | 1.02, 1.11 |
RR, risk ratio. aRR, adjusted risk ratio. CI, confidence interval. Estimates for medical and obstetric conditions are with absence of the condition as the reference. For the fragmentation variable, hospital where delivery occurred is the reference. All variables in the table were included in the adjusted analysis.
Table 5.
Adjusted analyses for prolonged length of stay and high readmission costs
| Prolonged length of stay | High costs | |||
|---|---|---|---|---|
| aRR | 95% CI | aRR | 95% CI | |
| Readmission to hospital other than delivery hospital | 1.48 | 1.42, 1.54 | 1.74 | 1.67, 1.81 |
| Maternal age | ||||
| 15–19 years old | 1.08 | 1.01, 1.15 | 0.89 | 0.83, 0.95 |
| 20–24 years old | 1.03 | 0.98, 1.08 | 0.94 | 0.89, 0.99 |
| 25–29 years old | Reference | Reference | ||
| 30–34 years old | 0.98 | 0.93, 1.02 | 1.04 | 0.99, 1.09 |
| 35–39 years old | 1.00 | 0.94, 1.06 | 1.08 | 1.02, 1.14 |
| 40–54 years old | 0.92 | 0.84, 1.01 | 1.19 | 1.10, 1.30 |
| Payer | ||||
| Medicare | 1.82 | 1.62, 2.05 | 1.74 | 1.54, 1.95 |
| Medicaid | 1.44 | 1.38, 1.50 | 1.25 | 1.20, 1.30 |
| Private insurance | Reference | Reference | ||
| Self-pay | 1.57 | 1.37, 1.80 | 1.26 | 1.09, 1.47 |
| No charge | 1.12 | 0.53, 2.38 | 1.06 | 0.50, 2.23 |
| Other | 1.17 | 1.05, 1.31 | 1.01 | 0.91, 1.13 |
| Median ZIP code income quartile | ||||
| Lowest income quartile | 1.28 | 1.21, 1.35 | 0.97 | 0.92, 1.02 |
| 2nd lowest quartile | 1.11 | 1.04, 1.17 | 0.94 | 0.89, 0.99 |
| 2nd highest quartile | 1.10 | 1.04, 1.16 | 0.93 | 0.88, 0.98 |
| Highest income quartile | Reference | Reference | ||
| Delivery postpartum hemorrhage | 1.10 | 1.02, 1.18 | 1.44 | 1.34, 1.53 |
| Cesarean delivery | 1.74 | 1.68, 1.80 | 1.39 | 1.34, 1.44 |
| Pregestational diabetes | 1.42 | 1.30, 1.55 | 1.44 | 1.32, 1.58 |
| Gestational diabetes | 1.11 | 1.05, 1.18 | 1.04 | 0.98, 1.10 |
| Systemic lupus erythematosus | 1.47 | 1.19, 1.81 | 1.63 | 1.34, 1.99 |
| Multiple gestation | 1.03 | 0.95, 1.12 | 1.10 | 1.02, 1.20 |
| Asthma | 1.07 | 1.00, 1.15 | 1.10 | 1.03, 1.18 |
| Chronic kidney disease | 1.34 | 1.15, 1.56 | 1.38 | 1.19, 1.61 |
| Hypertensive diseases of pregnancy | 0.84 | 0.81, 0.88 | 0.86 | 0.82, 0.90 |
| Chronic hypertension | 1.01 | 0.94, 1.10 | 0.87 | 0.80, 0.95 |
| Hospital bed size | ||||
| Small | Reference | Reference | ||
| Medium | 1.05 | 0.98, 1.13 | 0.82 | 0.77, 0.87 |
| Large | 1.21 | 1.14, 1.29 | 0.89 | 0.84, 0.94 |
| Hospital teaching status | ||||
| Metropolitan non-teaching | Reference | Reference | ||
| Metropolitan teaching | 1.02 | 0.98, 1.06 | 0.94 | 0.90, 0.97 |
| Non-metropolitan | 0.81 | 0.76, 0.86 | 1.02 | 0.96, 1.08 |
aRR, adjusted risk ratio. CI, confidence interval. Estimates for medical and obstetric conditions are with absence of the condition as the reference. For the fragmentation variable, hospital where delivery occurred is the reference. High readmission costs were defined as >90th percentile or ≥$13,720.27. Prolonged lengths of stay were defined as >90th percentile or ≥6 days. All variables in the table were included in the adjusted analysis.
For the first ancillary analysis, maternal mortality was more common during fragmented compared to non-fragmented readmissions (RR 3.27, 95% 2.34, 4.55). Overall there were 94 deaths among non-fragmented readmissions versus 58 among fragmented readmissions (7.9 versus 28.8 versus per 10,000 readmissions, p<0.01). For the second ancillary analysis evaluating transfers, 310 of the 141,276 postpartum readmissions had an antecedent transfer during their delivery hospitalization; this small sample precluded further analysis. When risk for antecedent transfer was analyzed by indication for readmission, no indication had a higher than 0.5% likelihood of delivery hospitalization transfer. For the third ancillary analysis, evaluating the model for severe morbidity excluding postpartum hemorrhage and hypertensive diseases of pregnancy at delivery, results were similar to the primary analysis (Supplemental Table 3).
DISCUSSION
Main Findings
In this nationally representative sample, fragmentation of care occurred in more than 15% of postpartum readmissions. Fragmented care was associated with significantly higher risk of severe maternal morbidity, prolonged length of stay, and higher costs compared to non-fragmented readmissions. Of all factors associated with fragmentation, public compared to private insurance was associated with the largest effect in increased risk; this finding supports that socioeconomic status and payer may be associated with fragmentation. When analyses were additionally adjusted for indication for readmission, risks for morbidity, prolonged length of stay, and high costs associated with fragmentation were attenuated but still present.
Implications
Since the adoption of the 2012 Hospital Readmissions Reduction Program (HRRP), readmission risk identification and reduction has emerged as a health services priority.11,17 The incentives for reducing readmissions are improved patient care and decreased provider expenses, as hospitals incur financial penalties for exceeding average readmission rates.11 It is unclear to what degree postpartum readmissions are preventable and controversial to what degree they represent poor quality care. Individual postpartum readmissions may result from (i) appropriate care of and surveillance for high-acuity patients, (ii) suboptimal care during delivery and after discharge, or (iii) both. Although there are no current obstetric readmission penalties in place, similar policy approaches to HRRP may ultimately cover obstetric readmission rates as a specialty. Given the number of obstetrics hospitalizations, postpartum readmissions nationwide may represent a focus for decreasing costs and length of stay. Fragmentation, which is associated with increased risk for severe morbidity and may involve providers caring for patients with suboptimal documentation and medical records, may represent a target for postpartum care quality improvement.
While further research is indicated to determine to what degree fragmentation is planned and appropriate versus being due to suboptimal outpatient management, our study noted that public insurance was a significant risk factor for readmission at a different hospital than the delivery hospital. Public insurance has been demonstrated to be a significant risk factor for postpartum readmission in a number of clinical scenarios5,8,9 and these findings support that patients with Medicaid and Medicare are a particularly high risk group for whom educational interventions or increased postpartum surveillance could be targeted.
Strengths and Limitations
In interpreting the findings of this study there are important limitations to consider. First, it is possible that fragmentation occurred in some cases for appropriate indications. It is possible that in the setting of specific complications patients were directed by providers to present at hospitals other than where they delivered. To some degree, fragmentation as measured in this analysis could be a proxy for regionalization of care wherein patients with higher acuity are appropriately referred to hospitals greater resources. This study cannot make determinations as to whether fragmented readmissions were due to providers making recommendations for patients to be evaluated at hospitals other than where they delivered, whether patients made that decision independently, or whether fragmented readmissions were the result of a third party such as diversion by emergency rescue or referrals from urgent care centers. That fragmentation was less likely among wound infections and more likely in the setting of heart failure supports the possibility that readmission fragmentation differentials may be due in part to planned care and the availability of hospital services. In particular, the differential in maternal death may be due to regionalization. While the NRD has limitations that preclude more granular analysis of the role of regionalized care, further studies using hospital system informatics data or individual State Inpatient Databases linked to detailed hospital-level data sources such as the American Hospital Association Annual Survey could provide additional insights. Second, it is likewise possible that increased risk for severe morbidity associated with fragmentation is a cause rather than an effect of fragmented readmission. Women who develop a serious postpartum complication as an outpatient may be more likely to present emergently to another hospital and less likely to present to the hospital where they delivered independent of the outpatient care they received. The degree to which optimization of postpartum care can reduce the risk for fragmentation is outside the scope of this analysis. We lack data on postpartum readmission acuity, distance to delivery hospital, and type of transportation, all factors that could account for fragmentation to some degree. Third, we did not evaluate factors related to the readmitting hospital associated with outcomes as that was beyond the scope of this analysis; analyzing these factors may be an important component of subsequent analyses. Fourth, the CDC severe maternal morbidity composite was designed primarily for delivery hospitalizations and was used because there is no specific metric for postpartum complications. Fifth, because of limitations in translating ICD-9-CM to ICD-10-CM billing data we did not use data beyond 2014. Sixth, informatics analyses that include communication and electronic medical information in the setting of fragmentation may add additional insight. Seventh, we specifically evaluated transfers that occurred during the antecedent delivery hospitalization prior to readmissions; we did not evaluate all transfers during delivery hospitalizations because maternal and neonatal files are not linked and we could not determine whether transfer was secondary to neonatal or maternal regionalization. Eighth, maternal race and ethnicity are not available in this dataset precluding analysis of these factors. Other limitations of this study include those inherent to the use of administrative data, including the possibility for misclassification and under-ascertainment of diagnosis codes. Additionally, as the NRD only tracks readmissions within the same state, interstate readmissions are not captured. The strengths of this study include a large nationally representative database specifically designed to track hospital readmissions, allowing for generalizability of results and sufficient numbers to make meaningful statistical comparisons even for relatively uncommon outcomes. Unadjusted and adjusted analyses yielded similar results, increasing validity. Finally, sensitivity analyses including indication for admission demonstrated attenuated, but still significant, increased risk.
Conclusion
In summary, this study of nationwide estimates of postpartum fragmentation found discontinuity of postpartum care was associated for increased risk for severe morbidity, high costs, and long length of stay. Reduction of fragmentation may represent an important goal in overall efforts to improve postpartum care. Given the relatively high likelihood of fragmentation, the potential benefit of improved patient discharge education, obstetric care coordination programs, emergency medical services network communication, telemedicine, and health information exchanges should be investigated.
Supplementary Material
AJOG at a Glance.
A. Why was the study conducted?
To characterize risk for and outcomes associated with fragmentation of postpartum readmissions wherein the readmitting hospital is different than the delivery hospital.
B. What are the key findings?
Discontinuity of postpartum care was associated with increased risk for severe morbidity, high costs, and long length of stay.
C. What does this study add to what is already known?
Reduction of fragmentation may represent an important goal in overall efforts to improve postpartum care.
Funding
Dr. Friedman is supported by a career development award (K08HD082287) from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health.
Dr. Attenello is supported by a career development award (NIH SC CTSI KL2 Clinical and Translational Research Scholar Award).
This research was presented at the 2019 Annual Meeting for the Society for Maternal-Fetal Medicine Annual Pregnancy Meeting in Las Vegas, Nevada.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Condensation
Postpartum fragmentation was associated with increased risk for severe morbidity, high costs, and long length of stay.
Conflict of Interest Dr. D’Alton had a leadership role in ACOG II’s Safe Motherhood Initiative which received unrestricted funding from Merck for Mothers. Dr. Wright has served as a consultant for Tesaro and Clovis Oncology. The other authors report no conflict of interest.
REFERENCES
- 1.Merrill C, Steiner C. Hospitalizations related to childbirth, 2003 In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]. Agency for Healthcare Research and Quality (US); 2006. [PubMed] [Google Scholar]
- 2.The Centers for Medicare and Medicaid Services. Transitional Care Management Services. 2016. https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/Downloads/Transitional-Care-Management-Services-Fact-Sheet-ICN908628.pdf.
- 3.Burton R Health Policy Brief: Care Transitions. Health Affairs. September 13, 2012. https://www-healthaffairs-org.ezproxy.cul.columbia.edu/do/10.1377/hpb20120913.327236/full/. [Google Scholar]
- 4.McKinney J, Keyser L, Clinton S, Pagliano C. ACOG Committee Opinion No. 736: Optimizing Postpartum Care. Obstetrics & Gynecology. 2018;132(3):784–785. [DOI] [PubMed] [Google Scholar]
- 5.Wen T, Wright JD, Goffman D, et al. Postpartum venous thromboembolism readmissions in the United States. American journal of obstetrics and gynecology. 2018;219(4):401. e401–401. e414. [DOI] [PubMed] [Google Scholar]
- 6.Clapp MA, Little SE, Zheng J, Kaimal AJ, Robinson JN. Hospital-level variation in postpartum readmissions. Jama. 2017;317(20):2128–2129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Clapp MA, Little SE, Zheng J, Robinson JN. A multi-state analysis of postpartum readmissions in the United States. Amerian Journal of Obstetrics and Gynecology. 2016;215(1):113. e111–113. e110. [DOI] [PubMed] [Google Scholar]
- 8.Too G, Wen T, Boehme AK, et al. Timing and risk factors of postpartum stroke. Obstetrics and gynecology. 2018;131(1):70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wen T, Wright JD, Goffman D, et al. Hypertensive Postpartum Admissions Among Women Without a History of Hypertension or Preeclampsia. Obstetrics & Gynecology. 2019;133(4):712–719. [DOI] [PubMed] [Google Scholar]
- 10.Zafar SN, Shah AA, Channa H, Raoof M, Wilson L, Wasif N. Comparison of rates and outcomes of readmission to index vs nonindex hospitals after major cancer surgery. JAMA surgery. 2018;153(8):719–727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.McIlvennan CK, Eapen ZJ, Allen LA. Hospital readmissions reduction program. Circulation. 2015;131(20):1796–1803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Zheng C, Habermann EB, Shara NM, et al. Fragmentation of care after surgical discharge: non-index readmission after major cancer surgery. Journal of the American College of Surgeons. 2016;222(5):780–789. e782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.The Agency for Healthcare Research and Quality. Introduction to the HCUP Nationwide Readmissions Database (NRD) 2010–2015. 2017. https://www.hcup-us.ahrq.gov/db/nation/nrd/Introduction_NRD_2010-2015.pdf.
- 14.Kuklina EV, Whiteman MK, Hillis SD, et al. An enhanced method for identifying obstetric deliveries: implications for estimating maternal morbidity. Maternal and child health journal. 2008;12(4):469–477. [DOI] [PubMed] [Google Scholar]
- 15.The Centers fo Disease and Prevention. Severe Maternal Morbidity Indicators and Corresponding ICD Codes during Delivery Hospitalizations. Available at: https://www.cdc.gov/reproductivehealth/maternalinfanthealth/smm/severe-morbidity-ICD.htm. Accessed September 15, 2019.
- 16.The Bureau of Labor Statistics. Consumer Price Index Data from 1913 to 2019. Accessed September 15, 2019 Available at https://www.bls.gov/cpi.
- 17.The Centers for Medicare and Medicaid Services. Hospital Readmissions Reduction Program (HRRP). https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html. Accessed September 15, 2019.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.