

Description
A previously healthy 58-year-old man presented to an emergency department with a 3-day history of intermittent drenching sweats with rigours, diarrhoea, fatigue and decreased oral intake. These symptoms began a week after the patient returned from a summer vacation to a rural community in Central Oregon. On examination, temperature was 37.3°C, heart rate was 74 beats per minute and blood pressure was 88/56 mm Hg. The patient appeared diaphoretic. Laboratory evaluation was notable for a peripheral platelet count of 26 K/cu mm, white blood cell count of 6.38 K/cu mm, serum creatinine of 2.11 mg/dL, aspartate aminotransferase of 101 U/L and alanine aminotransferase of 102 U/L. A peripheral blood smear revealed the presence of multiple corkscrew-shaped organisms (figure 1).
Figure 1.
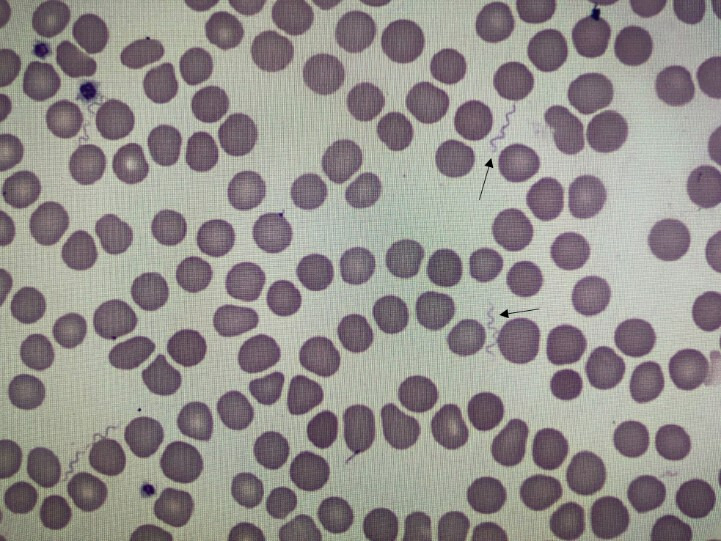
A peripheral blood smear demonstrating the presence of multiple corkscrew organisms (arrows), pathognomonic for Borrelia infection.
The constellation of symptoms and pattern of laboratory findings was consistent with tick-borne relapsing fever (TBRF), however the patient never noticed or removed a tick during his vacation.1 The patient was started on oral doxycycline 100 mg two times per day for a planned 10-day course. Within 2 hours of the first dose of doxycycline, the patient became delirious, tachycardic and diaphoretic, with a fever of 40.2°C, consistent with a Jarisch-Herxheimer reaction, an inflammatory response to antibiotic treatment of a spirochaetal infection. The pathogenesis is hypothesised to be due to lipoproteins that are released with lysis of spirochaetes and the ensuing cytokine stimulation.2 The patient subsequently improved with supportive therapies and antipyretics. Two-tiered serologic testing via immunoassay and IgM western blot later returned positive for Borrelia hermsii, confirming the diagnosis of TBRF. Other spirochaetal infections were considered, including Treponema pallidum and Leptospira. However, those organisms are too small to be visualised by light microscopy. The presence of corkscrew-shaped organisms on peripheral blood smear is pathognomonic for Borrelia infection and can confirm the diagnosis before the return of serologic testing.3
TBRF in the Northwestern region of North America is most commonly due to B. hermsii, a spirochaete transmitted from the rodent-associated Ornithodoros hermsi tick through a painless bite, often occurring at night when it is known to feed.4 TBRF typically presents after a week-long incubation period with a pattern of undulating fevers for 3 days, followed by a week without symptoms.5 B. hermsii is a corkscrew-shaped bacteria, approximately 3 to 25 μm in length, easily visualised with light microscopy.5 Exposure to B. hermsii peaks in July and August when travellers come in contact with the O. hermsi tick while vacationing to summer cabins or rural vacation homes in endemic regions.4
Learning points.
Consider tick-borne relapsing fever in the differential diagnosis for patients who present with an undulating febrile illness, compatible travel history and characteristic laboratory pattern.
When corkscrew-shaped organisms are visible, light microscopy is a useful aid in differentiating tick-borne relapsing fever from other spirochaetal infections.
The Jarisch-Herxheimer reaction is characterised by the onset of fever, rigours and hypotension 1 to 4 hours after starting antibiotic therapy in patients with a spirochaetal infection.
Acknowledgments
The authors would like to thank Peter Sullivan for providing the information that the presence of corkscrew-shaped organisms on peripheral blood smear is pathognomonic for Borrelia infection, as other spirochaetes are too small to be visualised.
Footnotes
Contributors: ESA, MO, MA and AMM were each involved in the care of the patient and contributed equally to writing the manuscript. MO annotated the figure.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Patient consent for publication: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Dworkin MS, Schwan TG, Anderson DE, et al. Tick-Borne relapsing fever. Infect Dis Clin North Am 2008;22:449–68. 10.1016/j.idc.2008.03.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Butler T. The Jarisch–Herxheimer reaction after antibiotic treatment of spirochetal infections: a review of recent cases and our understanding of pathogenesis. Am J Trop Med Hyg 2017;96:46–52. 10.4269/ajtmh.16-0434 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Malison MD. Relapsing fever. JAMA 1979;241:2819–20. 10.1001/jama.1979.03290520043026 [DOI] [PubMed] [Google Scholar]
- 4.Dworkin MS, Shoemaker PC, Fritz CL, et al. The epidemiology of tick-borne relapsing fever in the United States. Am J Trop Med Hyg 2002;66:753–8. 10.4269/ajtmh.2002.66.753 [DOI] [PubMed] [Google Scholar]
- 5.Centers for Disease Control and Prevention Relapsing Fever [Internet]. CDC, 2015. Available: https://www.cdc.gov/relapsing-fever/index.html [Accessed 17 Sep 2019].