

Abstract
The stressful experiences that many asylum seekers and refugees (AS&R) are exposed to during forced migration, and during resettlement in host countries, can have a profound impact on their mental health. Comparatively less research attention has been allocated to exploring other indices of quality of life (QoL) in AS&R populations. This review aimed to (i) synthesize the predictors and correlates of QoL of AS&R populations in high-income countries, and (ii) to identify the methodological strengths and weaknesses of this body of research.
Fourteen databases were systematically searched (Medline, PsychINFO, CINAHL, Cochrane Library, Health Technology Assessment, National Health Service Economic Evaluation, Educational Resource Index and Abstracts, BiblioMap, Scopus, Social Sciences Citation Index, Evidence Aid, DARE, Web of Science and PubMed). Eligibility criteria included: adults seeking asylum or refuge in a high-income country, primary quantitative data, the use of a measure based on the WHO’s definition of QoL, published in a peer-reviewed journal. A narrative synthesis approach was used, and the quality was assessed using the AXIS tool for cross-sectional studies and the CASP tool for longitudinal studies.
Of the 13.656 papers identified, 23 met the eligibility criteria. A wide range of factors were found to have significant associations with QoL. Both positive and negative correlates of QoL were largely dominated by social (e.g. social networks) and mental health factors (e.g. depression). Although all of the cross-sectional studies met over half of the quality criteria, only 12 met 75% or more of these criteria. For the longitudinal studies, for all but one study lacked statistical precision and the results cannot be applied to the local population.
Key findings across the various forms of QoL (overall, physical, psychological, social and environmental) were that having established social networks and social integration were associated with higher QoL, whereas having mental disorders (i.e. PTSD or depression) was strongly associated with reduced QoL. More research is needed into physical and environmental predictors and correlates of QoL. The findings of the review can be used to inform policies and interventions aimed at supporting AS&R and promoting the integration and wellbeing of these populations.
Keywords: Quality of life, Asylum seekers, Refugees, Migration
Introduction
The number of forcibly displaced persons in 2018 exceeded 70.8 million worldwide [1]. Within this displaced group, the estimated number of people awaiting a decision on their application for asylum was 3.5 million, and an estimated 25.9 million individuals were recognized as refugees [1]. High income countries on average host 2.7 refugees per 1000 of population [1]. The stressful experiences that many asylum seekers and refugees (AS&R) are exposed to during forced migration, and during resettlement in host countries, can have a profound impact on their mental health (MH) including high rates of depression, anxiety and posttraumatic stress disorder [2]. However, comparatively less research attention has been allocated to exploring other indices of MH such as quality of life (QoL) in AS&R populations.
Quality of life
QoL has been implicated in MH status. It is defined as an ‘Individuals’ perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns’ ([3], p.1). As such, QoL is a broad ranging and multidimensional concept which includes an individual’s subjective evaluation of their physical health, psychological state, level of independence, social relationships, personal beliefs and their relationship to their environment [4].
Whilst there is growing consensus over the multidimensionality of QoL, little research has focused on understanding the specific predictors and correlates thereof. This is specifically the case with regards to AS&R populations, despite the existing evidence base for their high risk of developing mental disorders. The WHO estimates the prevalence of mental disorders, including depression, anxiety, post-traumatic stress disorder (PTSD), bipolar disorder and schizophrenia, in conflict-affected settings to be 22.1% at any time point in the populations assessed [5]. Evidence has shown that for AS&R the effects of war-related events may persist for years and have been associated with lower QoL even when hostilities have ended [6, 7]. Akinyemi et al. [6] noted that QoL, together with occupational status, were the biggest threats to the mental health of refugee populations and called for attention to the overall QoL in order to support their long-term mental health. Similarly, Matanov et al. [7], found that traumatic war events were directly associated with lower QoL in war-affected communities in the Balkan countries, and experiencing more migration-related stressors was linked to lower QoL in refugee populations who had resettled in Western Europe. Simultaneously, the lack of studies evaluating the efficacy of interventions for increasing QoL in AS&R populations [8, 9] has been noted. Improving understanding about predictors and correlates of QoL in AS&R populations will be important for guiding the foci of these interventions, and more broadly informing policies in high-income countries to support the local settlement, integration and long-term mental health of AS&Rs.
The current paper is the first to systematically review evidence relating to predictors and correlates of QoL of AS&Rs living in high-income countries. The specific aims of the review were to: 1) understand what factors are associated with QoL in AS&R populations; 2) identify the methodological strengths and weaknesses of the research investigating QoL.
Methods
Literature search
Fourteen databases were systematically searched. A search strategy tailored to the aims of the review was applied to each database using the Kings College London library guide [10]. See appendix A for the list of databases which were searched and the full search strategy. Reference chaining was also carried out and five experts in the field of mental health of refugee populations were independently consulted to ensure the final list of included papers was exhaustive.
Eligibility
All quantitative peer-reviewed publications in English, Spanish or Dutch (languages spoken by the authors of this review) which used measures based on the four WHOQOL domains [4], explored predictors and correlates of the QoL of adult AS&R populations residing in a high-income country (as classified by the World Bank1) at the time that the search was conducted were included. The exclusion of grey literature was used as a form of minimal quality assurance. Longitudinal evaluations of interventions were also excluded if a cross-sectional analysis between QoL and other variables were not performed at baseline. The search of databases was conducted up to the 5th of May 2020, and any studies that met inclusion criteria were included in the current review. Furthermore, additional papers identified through expert consultation were included.
CB and RA independently screened the titles and abstracts for inclusion. Articles rated as possible candidates by either CB or RA were added to a preliminary list. Working independently and in duplicate, both reviewers inspected the full texts of the preliminary list for inclusion. A consensus meeting was subsequently held between CB and RA and remaining discrepancies were resolved through discussion with the research team.
Data extraction and quality appraisal
For each included study, CB extracted information on the publication year, country of publication, settings, populations, study design, assessment measures and key findings, which was peer-reviewed by RW. Once the data was extracted, CB rated the quality of each individual study and RA peer reviewed the quality appraisal for a quarter of the studies.
Data synthesis and analysis
A narrative synthesis approach was used to analyze the data. The WHOQOL Group developed a conceptual framework for QoL that incorporates four domains [4]: physical, psychological, social relationships and environment. To support efforts to synthesize the research findings of the studies included in the current review, these four domains were used to group predictors and correlates of QoL investigated in the studies. Two authors (CB and RW) independently mapped the various correlates investigated in the studies onto these four domains, discrepancies were resolved through discussion.
Consideration was given to conducting a meta-analysis. Five studies reported significant relationship between QoL and the correlates in terms of a correlation coefficient (an r statistic) and the statistical significance of this coefficient. Meta-analysis of correlation coefficients is methodologically complex due to the bounded nature of these statistics (i.e. that they can only take values between: − 1 and + 1) and furthermore, correlation coefficients were not reported with a measure of precision such as a confidence interval which would be required for meta-analysis [11, 12]. Similarly, five studies also reported the relationship between QoL and the variables in terms of t-statistics and corresponding p-values. Such statistics do not have an associated measure of precision and therefore cannot be combined within meta-analysis.
The only amenable statistical measure for meta-analysis to represent the relationship between QoL and the predictors were regression (beta) coefficients with accompanying confidence intervals. These were reported in 52% of studies. These act as continuous data and theoretically, synthesis of such data may be possible within a ‘prognostic review’ framework [13]. However, across the studies, the predictors included within regression models to examine the effects of these predictors on QoL varied widely. Therefore, due to anticipated very large heterogeneity originating from the wide range of predictors included within regression models (see Additional file 1), meta-analysis of these beta-coefficients was deemed to be potentially misleading and therefore inappropriate.
Instead, further consideration of the direction, strength and consistency of the correlates of overall QoL has been undertaken for the studies included in this review which reported correlational analysis. Cohen’s [14] conventions were used to interpret the effect sizes; positive large correlation (> 0.50 to + 1.00), positive moderate correlation (0.30 to 0.50) and positive small correlation (< 0.30). Negative large correlation (<− 0.50 to − 1.00), negative moderate correlation (− 0.30 to 0.50) and negative small correlation (> − 0.30). Positive correlations indicate a relationship between two variables in which both variables move in the same direction (i.e. if mental health increases, QoL increases), whereas negative correlations indicate a relationship whereby both variables move in opposite directions (i.e. if depression decreases, QoL increases). Figure 2 provides a representation thereof.
Fig. 2.
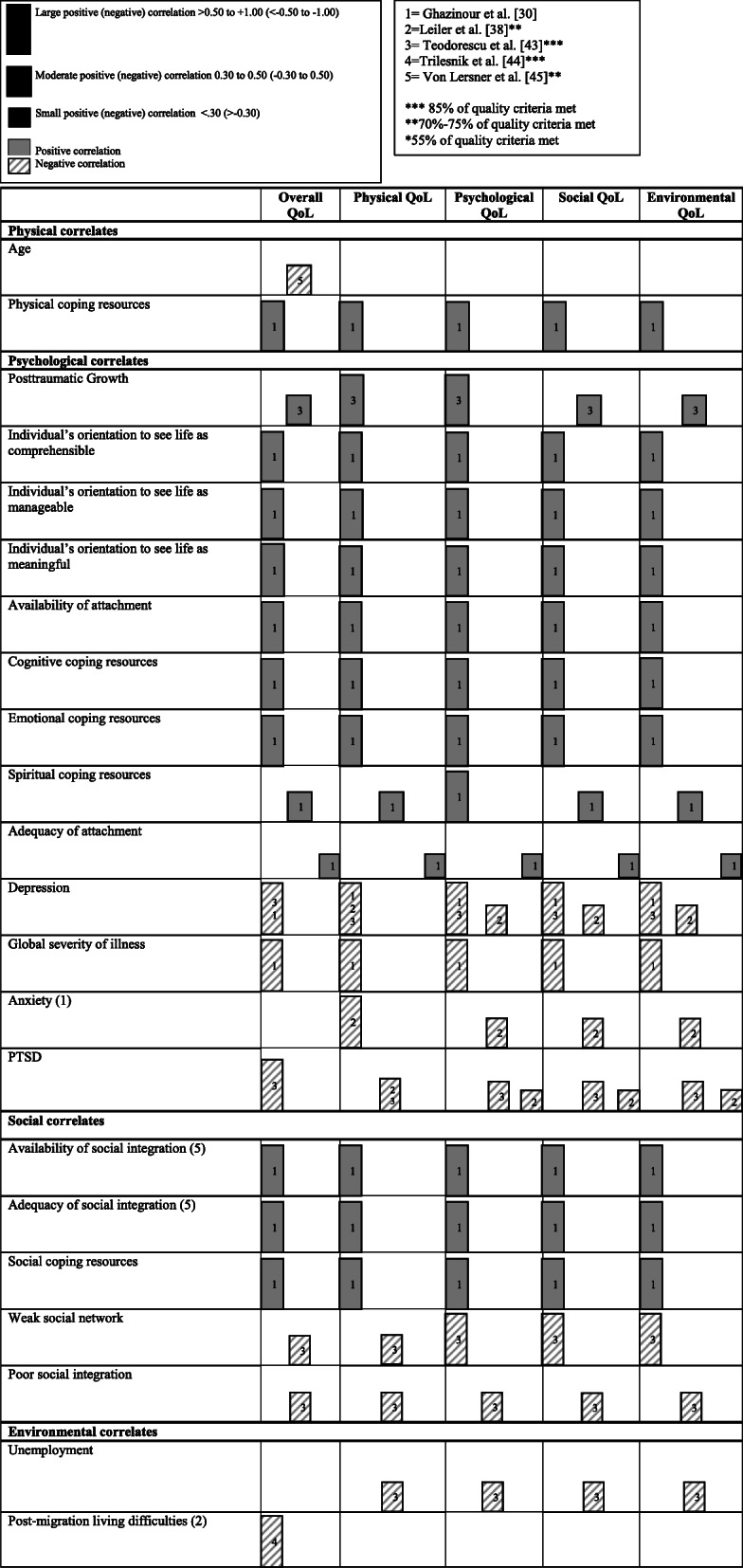
A harvest plot indicating the positive and negative correlations of overall QoL and the four QoL domains. All findings are from cross-sectional studies
The quality of the cross-sectional studies was assessed using the Appraisal tool for Cross-Sectional Studies (AXIS tool) [15]. Longitudinal studies were assessed using the Critical Appraisal Skills Programme [16]. The quality of the studies was independently rated by CB. Additionally, RA rated a quarter of the cross-sectional studies (N = 5) and longitudinal studies (N = 2) in order to ensure a quality check was carried out. There was high agreement regarding quality assessment; items that were rated differently were resolved through discussion.
Results
The search identified 13.655 articles of which 23 met the inclusion criteria. Article selection is summarized in the PRISMA diagram presented in Fig. 1.
Fig. 1.

PRISMA flow diagram of article selection
Study characteristics
A total of twenty-three studies met the inclusion criteria. Seventeen studies were conducted in Europe, two in Australia, two in Israel, one in the USA and one in Japan. Four studies used the same dataset, therefore there were two repeat samples. Sample sizes ranged from 22 to 663 (Mdn = 119, IQR = 222), with a total sample of 3817 across studies including 2138 males, 1516 females, and 163 not specified. Studies that used the same dataset were only counted once. Eleven of the studies recruited individuals from a medical setting, and the rest were recruited from support agencies, reception facilities (N = 5), community events (N = 4) or other (N = 3). Seventeen studies reported cross-sectional data and six were longitudinal studies including one case control design. All studies used the WHOQOL-100, WHOQOL-BREF or the EUROHIS-QOL measures (see Table 1).
Table 1.
Summary table of the selected articles including study site, country of origin, sample size, type of migrant, study design, assessment tool and findings
| Study | Country in which the Study was Conducted | Migrant Country of Origin | N | Type of Migrant | Study Design | Recruitment Site | Self-Rating Scale for QoL | Other validated Assessment Measures | Summary of Significant Associations with QoL | Non-significant Associations with QoL (p > .005) |
|---|---|---|---|---|---|---|---|---|---|---|
| Carlsson et al. 2010a [17] | Denmark | Iraq, Iran, Afghanistan | 45 | Refugees | Longitudinal | Rehabilitation and research center for torture victims | WHOQOL-Bref (WHOQOL Group, 1998) | HTQ, HSCL-25, HDS |
● WHOQOL Environment Time (Baseline vs. 9-month follow-up)(p = .029) ● WHOQOL Environment Time (Baseline vs. 23-month follow-up)(p = .017) |
• No significant difference between baseline and 9 month, or 23 month follow-up for WHOQOL Physical, mental or social. |
| Carlsson, Mortensen & Kastrupa [18] | Denmark | Iraq, Iran, Afghanistan | 55 | Refugees | Longitudinal | Rehabilitation and research center for torture victims | WHOQOL-Bref (WHOQOL Group, 1998) [4] | HTQ, HSCL-25, HDS |
● Changes in mental health ○ Evaluation of improved mental health (vs. those evaluating no improvement) during treatment had higher health-related quality of life in the ‘mental’ domain (t = 2.46, p = .017) ● Those with the lowest baseline QoL showed the largest increase in QoL. |
• No significant changes over time for the WHOQOL domains. • The Spearman rank correlations between years from exposure to torture and baseline scores were nonsignificant for all QoL domains • The Spearman rank correlation between total number of treatment sessions and difference scores was low and nonsignificant for all QoL domains • Expressing expectations to improve during treatment was not associated with changes in QoL domains |
| Carlsson, Mortensen & Kastrup [19] | Denmark | Iraq, Iran, Afghanistan, other (not specified) | 63 | Refugees | Cross-Sectional | Rehabilitation and research center for torture victims | WHOQOL-Bref [4] | HSCL-25, HDS, HTQ |
● Overall variance accounted for by the regression model was not reported ● WHOQOL Physical ○ Occupation (β = 0.23, p < .05) ○ Social relations (β = 0.33, p < .01) ○ Pain (β = − 0.42, p < .01) ● WHOQOL psychological ○ Social relations (β = 0.31, p < .05) ● WHOQOL Social ○ Social relations (β = 0.39, p < .01) ● WHOQOL Environment ○ Social relations (β = 0.40, p < .01) ▫ Pain (β = − 0.35, p < .05) |
o Number of years since last exposure to torture was not associated with QoL o Age and proficiency in Danish were not significant associated with QoL Regression (Model 2) • Education, torture, or having been on the run were not significantly associated with any of the QoL domains • Occupation was not significantly associated with mental, social or environmental QoL • Pain was not significantly associated with mental or social QoL |
| Carlsson, Olsen, Mortensen & Kastrup* [20] | Denmark | Iran, Iraq, Lebanon | 139 | Refugees | Longitudinal | Rehabilitation and research center for torture victims | WHOQOL-Bref [4] | HTQ, HSCL-25 |
● Overall variance accounted for by the regression model was not reported ● WHOQOL Physical ○ Pain upper extremities (β = 0.20, p < .05) ○ Employment (β = 0.49, p < .001) ▫ Headache (β = − 0.31, p < .001) ● WHOQOL Mental ○ Social relations (β = 0.21, p < .05) ○ Employment (β = 0.40, p < .001) ● WHOQOL Social ○ Social relations (β = 0.40, p < .001) ○ Employment (β = 0.27, p < .01) ▫ Headache (β = − 0.20, p < .05) ● WHOQOL Environment ○ Social relations (β = 0.24, p < .01) ○ Employment (β = 0.36, p < .001) ▫ Headache (β = − 0.19, p < .05) |
Regression (Model 2) • Education, marked mood shifts, and years in Denmark were not associated with any of the QoL domains • Pain in upper extremities was not associated with mental, social or environmental QoL • Headache was not associated with mental QoL • Social relations was not associated with physical QoL |
| Correa-Velez, Green, Murray [21] | Australia | Africa, South Asia, Middle East, West Asia, South East Asia | 104 | Refugees | Cross-Sectional | Agency involved in refugee resettlement | WHOQOL-Bref | HTQ, PMLD, SASCAT |
● Regressing WHOQOL Physical domain on predictor variables was significant (r2 = .30, p < .001) ○ Region of birth (Africa) (β = 0.32, 95% CI = [5.44, 19.83], p = .001) ○ Education (2y/3y) (β = 0.32, 95% CI = [3.80, 16.94], p = .002) ○ Community can be trusted (β = 0.20, 95% CI = [.79, 12.49], p = .027) ● Regressing WHOQOL Psychological domain on predictor variables was significant (r2 = .19, p = .008) ○ Community can be trusted (β = 0.20, 95% CI = [.33, 13.02], p = .039) ▫ Number of people no support (β = − 0.24, 95% CI = [− 5.80, −.57], p = .018) |
• Age, Children (1 or more), English skills and trauma types were non-significant predictors of the physical domain • Age, region of birth (Africa), children (1 or more), education (2y/3y), English skills, and trauma types were non-significant predictors of the psychological domain • The hierarchical logistic regression predicting overall QOL found no significant associations |
| Correa-Velez, Barnett, Gifford & Sackey* [22] | Australia | Sudan, Burma (Myanmar), Iraq, Burundi, the Democratic Republic of Congo, Rwanda, Liberia, Afghanistan, Congo-Brazzaville, Iran, Tanzania, Uganda | 233 | Refugees | Cross-Sectional | Community | WHOQOL-Bref [4] | HSCL-25, HTQ, Items to assess use of Health Services & Medication |
● WHOQOL Environment ▫ Living in regional areas (OR = 0.4, 95% CI = [0.2, 0.9], p < .05) |
• Area of settlement did not predict significant poorer QoL in the physical, mental or social domain |
| Georgiadeu et al. [23] | Germany | Syrian | 119 | Refugees | Cross-sectional | Registry | WHOQOL-Bref | ETI, PHQ-9, GAD-7, SOC-13, F-SozU, |
● WHOQOL Psychological Married with partner in Germany scored higher than married without partner in Germany, t(117) = 2.91, p = .004 ● WHOQOL Social Married with partner in Germany scored higher than married without partner in Germany, U = -3.02, p = .002 ● WHOQOL Environment Married with partner in Germany scored higher than married without partner in Germany, t(117) = 2.27, p = .025. ● WHOQOL Overall Married with partner in Germany scored higher than married without partner in Germany, t(117) = 2.78, p = .006. ● Regressing overall QoL on predictor variables was significant (r2 = .66) ○ Sense of coherence (β = 0.15, 95% CI = [− 0.00, 0.33], p = .049) ○ Social support (β = 0.25, 95% CI = [0.15, 0.46], p < .001) ▫ Depression (β = − 0.44, 95% CI = [− 1.52, − 0.61], p < .001) ● Regressing WHOQOL psychological domain on predictor variables was significant (r2 = .61) ○ Gender (β = 0.15, 95% CI = [0.32, 11.04], p = .038) ○ Residence of partner (β = 0.17, 95% CI = [1.39, 13.95], p = .017) ○ Sense of coherence (β = 0.22, 95% CI = [0.07, 0.47], p = .008) ○ Social support (β = 0.17, 95% CI = [0.04, 0.41], p = .016) ▫ Depression (β = − 0.40, 95% CI = [− 1.66, − 0.56], p < .001) |
• No significant differences in WHOQOL Physical (married with partner vs. married without partner) • Sex, age, residence of partner, residence of minor child, anxiety, number of traumatic events, trauma inventory, and satisfaction with marriage were non-significant predictors of overall QoL • Age accommodation, residence of minor child, anxiety, number of traumatic events, trauma inventory, and satisfaction with marriage were non-significant predictors of WHOQOL psychological. |
| Ghazinour, Richter & Eisemann [24] | Sweden | Iran | 100 | Refugees | Cross-Sectional | Half were recruited as outpatients at a psychiatric clinic and half were recruited as interested volunteers. | WHOQOL-100 [18] | CRI, ISSI, BDI, SCL-90 |
● Gender: Males reported lower overall QoL (t = − 2.99, p = .004) than females ● Males reported lower levels of Independence (Psychological domain), (t = − 2.00, p = .049) than females ● Males reported lower social QoL than females (t = − 2.40, p = .018) ● Males reported lower environmental QoL (t = − 2.06, p = .043) ● Males reported lower spirituality (psychological domain) (t = − 2.82, p = .006) ● Having a BDI score below the mean and having been in the army showed the highest significant overall QoL F(19,70) = 60.06, p < .001 ● Sense of coherence, coping resources, and social support had various significant relationships with QoL (see paper for details) |
• Gender: no significant differences found for physical health or psychological health • No significant correlation was found between spirituality (psychological domain) and adequacy of attachment (social support scale) |
| Hengst, Smid & Labanb [25] | Netherlands | Iraq | 294 | Asylum Seekers | Cross-Sectional | Central Organ of Asylum (COA) | WHOQOL-Bref [4] | HTQ, PMLP, WHO-CIDI, BDQ |
● Mediation model of psychopathology, disability and quality of life χ2(12) = 10.52, p = .570 ▫ Unnatural loss of a child (β = −.05, 95% CI = [−.44, −.03], p < .05) ▫ N° of lost family members (β = −.04, 95% CI = [−.01, .00], p < .05) ▫ Other traumatic events (β = −.13, 95% CI = [−.06, −.02], p < .05) ▫ Long asylum procedure (β = −.18, 95% CI = [−.66, −.13], p < .05) ▫ Psychopathology (β = −.33, 95% CI = [−.42, −.20], p < .05) |
• Age, female sex, education level and postmigration stressors were not significantly associated with QoL • Unnatural loss of family, unnatural loss of friends, witnessing the loss of family or friend, number of lost children, and number of lost friends were not significantly associated with QoL |
| Huijts, Kleijn, van Emmerik, Noordhof, and Smith [26] | Netherlands | 38 different countries in the Middle East, former Yugoslavia, or other regions of which 50 were Asian, 35 African, and 4 South American. | 335 | Refugees | Cross-Sectional | Foundation Centrum ‘45, a specialist institute for diagnosis and treatment of posttraumatic stress. | WHOQOL-Bref [4] | COPE-EASY-32, HTQ |
● Regressing overall QoL on predictor variables was significant (r2 = .42, p < .05) ○ Social Support Seeking (β = 0.12, 95% CI = [.03, .21], p < .05) ○ Emotion-Focused Coping (β = 0.13, 95% CI = [.04, .23], p < .01) ○ Self-reported PTSD (β = − 0.61, 95% CI = [−.68, −.54], p < .001) ● Post-hoc analyses revealed that emotion-focused coping and social support seeking differed per country of origin, and per gender. |
Subgroup analysis of regression o Males: emotion-focused coping, was not significantly related to QoL o Females: social support seeking was not significantly related to QoL Multigroup analyses • No significant differences found regarding length of stay in the Netherlands. |
| Jesuthasan et al.* [27] | Germany | Afghanistan, Syria, Iraq, Somalia, Iran, Eritrea | 663 |
Refugees + European Reference Sample |
Cross-Sectional | Shared reception facilities | EUROHIS-QOL questionnaire [24] | HTQ, HSCL-25, ICSEY |
● Female refugees rated their overall QoL significantly lower than the EU reference simple, t(5508) = 16.9, p < .0001 ● Residence and mission in a war zone, and being sick without any access to health care significantly affected all four domains of QoL ● Near death experience affected physical and psychological domains. ● Aggression from family members affected the physical and social domain ● Forced isolation affected the physical, psychological, and environmental domains. ● Within Group (Refugees) Predictors: Regressing overall reduced QoL on socio-demographic and traumatic predictor variables (Overall variance accounted for by the regression model was not reported) A) Reduced QoL ● Age > 30 (OR = 1.6, 95% CI = [1.2–2.3], p = .004) ● Near-Death Experience (OR = 1.7, 95% CI = [1.2, 2.4], p = .001) ● Mission/Residence in War Zone (OR = 0.7, 95% CI = [0.5–1.0], p = .04) ● Attack by Family Member (OR = 2, 95% CI = [1.3, 3.1], p = .001) |
• Having had sexual contacts as a minor did not signfiicantly correlate with overall QoL • No significant association was found between near death experience and the social and environmental domains • No significant association was found between aggression from family members and the psychological and environmental domains • No signiciant association was found between forced isolation and the social domain. |
| Kinzie et al. [28] | USA | Ethiopia, Somalia, Iran and Afghanistan | 22 | Refugees | Longitudinal | Refugee psychiatric clinic | WHOQOL-BREF | HTQ, SDS, CES-D |
● WHOQOL Physical ○ Time (baseline vs. 1-year follow-up) (p < .001) ● WHOQOL Psychological ○ Time (baseline vs. 1-year follow-up) (p < .001) ● WHOQOL Environment ○ Time (baseline vs. 1-year follow-up) (p = .004) |
None reported |
| Laban, Gernaat, Komproe & de Jongb [29] | Netherlands | Iraq | 294 |
Asylum Seekers Group 1: living in the Netherlands < 6 months Group 2: living in the Netherlands for at least 2 years. |
Cross-Sectional | Agency for the reception of asylum seekers | WHOQOL-Bref [4] | PMLP, WHO-CIDI, Physical Health Rating |
● Overall QoL group 1 vs. group 2 (p < .0005, Z(294) = − 5.29) with group 2 scoring lower than group 1 ● Perceived QoL General Health group 1 vs. group 2 (p = .017, Z(294) = − 2.39) with group 2 scoring lower than group 1. |
None reported |
| Laban, Komproe, Gernaat & de Jongb [30] | Netherlands | Iraq | 294 |
Asylum Seekers Group 1: living in the Netherlands < 6 months Group 2: living in the Netherlands for at least 2 years. |
Cross-Sectional | Agency for the reception of asylum seekers | WHOQOL-Bref [4] | HTQ, PMLP, WHO-CIDI |
● Overall QoL was significantly lower in group 2 Z(294) = − 5.29, p = .0005 ● WHOQOL physical was significantly lower in group 2, t(292) = 3.21, p = .001 ● WHOQOL psychological was significantly lower in group 2, t(292) = 2.33, p = .020 ● WHOQOL environment was significantly lower in group 2, t(292) = 5.26, p = .001 ● Regressing overall QoL on predictor variables was significant (r2 = 0.13, p < .001) ▫ Long Asylum Procedure (β = − 0.17, p < .01) ▫ Adverse life events after arrival in the Netherlands (β = − 0.13, p < .05) ▫ WHOQOL Physical (r2 = .31, p < .01) ▫ Adverse life events after arrival (β = − 0.15, p < .05) ▫ Depression (β = − 0.19, p < .01) ▫ Somatoform disorders (β = − 0.12, p < .05) ▫ One or more psychiatric disorders (β = − 0.19, p < .05) ▫ Older age (β = − 0.14, p < .01) ▫ Socio-economic living conditions (β = − 0.20, p < .01) ● WHOQOL Psychological (r2 = .18, p < .01) ▫ Self-reported PTSD (β = − 0.17, p < .05) ▫ Somatoform disorders (β = − 0.15, p < .01) ▫ Socio-economic living conditions (β = − 0.14, p < .05) ▫ Anxiety (β = − 0.17, p < .05) ● WHOQOL Social (r2 = .12, p < .01) ● WHOQOL Environmental (r2 = .15, p < .01) ○ Socio-religious aspects (β = 0.12, p < .05) ▫ Self-rated PTSD (β = − 0.14, p < .05) ▫ Socio-economic living conditions (β = − 0.27, p < .01) |
• WHOQOL social was not significantly different between group 1 and group 2. Regression • Psychopathology and socio-economic living conditions were not associated with overall QoL • Anxiety disorders, PTSD, long asylum procedure, adverse life events after arrival, and family issues were not associated with physical QoL • Having one or more psychiatric disorders, depressive disorders, a long asylum procedure, adverse events after arrival and family issues were not associated with psychological QoL • Psychopathology, adverse events after arrival, family issues and socioeconomic living conditions were not associated with social QoL • One or more psychiatric disorders, depressive disorders, anxiety disorders, somatoform disorders, long asylum procedure, adverse events after arrival, and family issues were not associated with environmental QoL |
| Lee et al. [31] | Japan | North Korea | 81 | Refugees (resettled in Japan vs. resettled in South Korea) | Cross -sectional | Support center | WHOQOL-Bref | BDI |
● Resettled in Japan vs. Resettled in South Korea ● Overall QOL (p < .05), Korea scoring higher ● WHOQOL Physical (p < .05), Korea scoring higher ● WHOQOL Mental (p < .01), Korea scoring higher ● WHOQOL social (p < .05), Korea scoring higher ● WHOQOL environment (p < .001), Korea scoring higher |
None reported |
| Leiler et al. [32] | Sweden | Afghanistan, Syria, Iraq, Iran, Eritrea, Somalia | 510 | AS&R | Cross-sectional | Housing facilities | WHOQOL-BREF | PHQ-9, GAD-7, PC-PTSD |
● WHOQOL Physical ▫ Depression (r = − 0.58, p < .001) ▫ Anxiety (r = − 0.52, p < .001) ▫ PTSD (r = − 0.36, p < .001) ● WHOQOL Psychological ▫ Depression (r = − 0.38, p < .001) ▫ Anxiety (r = − 0.32, p < .001) ▫ PTSD (r = − 0.21, p < .001) ● WHOQOL Social ▫ Depression (r = − 0.37, p < .001) ▫ Anxiety (r = − 0.37, p < .001) ▫ PTSD (r = − 0.27, p < .001) ● WHOQOL Environment ▫ Depression (r = − 0.34, p < .001) ▫ Anxiety (r = − 0.33, p < .001) ▫ PTSD (r = − 0.23, p < .001) |
No significant differences found between asylum seekers and refugees neither in the domain scores nor in overall QoL score. |
| Löfvander, Rosenblad, Wiklund, Bennström & Leppert [33] | Sweden | Somalia, Iraq, Syria | 66 pairs of refugees and matched Swedish born | Refugees | Longitudinal Case-Control | Asylum and integration healthcare center | WHOQOL-Bref [4] | GHQ-12, GAF |
● Between Groups (Men) ○ Psychological (Baseline; p = .020) ○ Social Relations (Baseline; p = .002, 6 Months p < .001, 12 Months p = .001) ● Between Groups (Women) ○ Social Relations (6 Months; p = .030) ● Between Groups (Mixed) ○ Psychological (Baseline; p = .004, 6 Months; p = .025, 12 Months; p = .041) ○ Social (Baseline; p = .002, 6 Months; p < .001, 12 Months; p = .001) |
Between groups (men) • No significant differences for physical QoL or environmental QoL at any timepoint. • No significant differences at 6-months or 12-months for psychological QoL. Between groups (women) • No significant differences for physical, psychological or environmental QoL at any timepoint. • No significant differences at baseline or at 12 months for social QoL Between groups (mixed) • No significant differences for physical or environmental QoL at any timepoint |
| Regev & Slonim-Nevo [34] | Israel | Sudan | 300 | AS&R | Cross-sectional | Community | WHOQOL-Bref | HTQ, PCL-C, BSI, MSPSS |
● Overall model for WHOQOL was significant (r2 = 0.07, p < .001) ○ Social support (β = 0.32, p < .001) ○ Other’s traumatic events (β = 0.27, p < .001) ▫ Gender (β = − 0.32, p < .001) ▫ Self-traumatic events (β = − 0.20, p < .001) |
● Length of stay was not a significant predictor of QoL |
| Slonim-Nevo [35] | Israel | Sudan | 340 | AS&R | Cross-sectional | Community | WHOQOL-Bref | HTQ, Language proficiency in Hebrew, PMLD, perceived discrimination, PCL-C, BSI, AIS, CSQ, FAD, MSPSS |
● Overall model for WHOQOL Physical was significant (r2 = 0.32, p < .001) ○ Legal status (β = 0.14, p < .01) ▫ PTSD (β = − 0.40, p < .001) ▫ Perceived discrimination (β = − 0.30, p < .001) ● Overall model for WHOQOL Psychological was significant (r2 = 0.31, p < .001) ▫ PTSD status (β = − 0.29, p < .001) ▫ Perceived discrimination (β = − 0.38, p < .001) ● Overall model for WHOQOL Social was significant (r2 = 0.12, p < .001) ▫ PTSD (β = − 0.27, p < .001) ▫ Perceived discrimination (β = − 0.15, p < .05) ● Overall model for WHOQOL Environment was significant (r2 = 0.25, p < .001) ▫ Perceived discrimination (β = − 0.24, p < .001) ▫ Post-migration living difficulties (β = − 0.38, p < .001) |
● WHOQOL Physical ○ Gender ○ Post-migration living difficulties ● WHOQOL psychological ○ Gender ○ Legal status ○ Post-migration living difficulties ● WHOQOL Social ○ Gender ○ Legal status ○ Post-migration living difficulties ● WHOQOL Environment ○ Gender ○ Legal status ○ PTSD diagnosis |
| Stammel et al. [36] | Germany | Iran, Chechnya, Turkey, Syria, Kosovo, Afghanistan, Iraq, Other countries of the russian Federation, Armenia, Kenya, Angola, Chile, Lebanon | 76 | AS&R | Longitudinal | Center for torture victims | EUROHIS-QOL | MINI, PDS, HSCL-25, SCL-90-R | ● Multilevel analysis revealed QoL increased significantly after an average of 14 months of treatment (Pseudo R2 = .14, β = 0.42, 95% CI [0.29, 0.55], p < .001). | ● Not specified |
| Teodorescu, Siqveland, Heir, Hauff, Wentzel-Larsen & Lien [37] | Norway | Eastern Europe, Africa, Middle East, Far East, Latin America | 55 | Refugees | Cross-Sectional | Hospital outpatient department | WHOQOL-Bref [4] | LEC, CAPS, SCID-PTSD, MINI, IES-R, HSCL-25, PTGI-SF |
● Bivariate correlations ● WHOQOL Physical ○ Posttraumatic growth (rs = .51, p < ..001) ▫ Weak social network (rs = −.35, p < .01) ▫ Poor social integration (rs = −.32, p < .05) ▫ Unemployment (rs = −.34, p < .05) ▫ Posttraumatic stress (rs = −.45, p < .01) ▫ Depression (rs = −.59, p < .001) ● WHOQOL Psychological ○ Posttraumatic growth (rs = .58, p < ..001) ○ Physical QoL (rs = .73, p < .001) ▫ Weak social network (rs = −.53, p < .001) ▫ Poor social integration (rs = −.37, p < .01) ▫ Unemployment (rs = −.31, p < .05) ▫ Posttraumatic stress (rs = −.53, p < .001) ▫ Depression (rs = −.58, p < .001) ● WHOQOL social ○ Posttraumatic growth (rs = .41, p < .01) ○ Physical QoL (rs = .46, p < .001) ○ Psychological QoL (rs = .54, p < .001) ▫ Weak social network (rs = −.61, p < .001) ▫ Poor social integration (rs = −.48, p < .001) ▫ Unemployment (rs = −.37, p < .01) ▫ Posttraumatic stress (rs = −.45, p < .01) ▫ Depression (rs = −.54, p < .001) ● WHOQOL environment ○ Posttraumatic growth (rs = .49, p < .001) ○ Physical QoL (rs = .48, p < .001) ○ Psychological QoL (rs = .53, p < .001) ○ Social QoL (rs = .62, p < .001) ▫ Weak social network (rs = −.56, p < .001) ▫ Poor social integration (rs = −.40, p < .01) ▫ Unemployment (rs = −.38, p < .01) ▫ Posttraumatic stress (rs = −.38, p < .01) ▫ Depression (rs = −.51, p < .001) ● Overall QoL ○ Posttraumatic growth (rs = .47, p < .001) ○ Physical QoL (rs = .62, p < .001) ○ Psychological QoL (rs = .71, p < .001) ○ Social QoL (rs = .39, p < .01 ○ Environmental QoL (rs = .48, p < .001) ▫ Weak social network (rs = −.39, p < .01) ▫ Poor social Integration (rs = −.38, p < .01) ▫ Posttraumatic stress (rs = −.65, p < .001) ▫ Depression (rs = −.70, p < .001) ● Regression ● WHOQOL Physical (ΔR2 = 0.49, F (4,46) = 13.15, p < .001) ○ Posttraumatic growth (β = 0.37, 95% CI = [.04, 16.22], p < .01) ● WHOQOL Psychological (ΔR2 = 0.56, F (4,46) = 17.97, p < .001) ○ Posttraumatic growth (β = 0.39, 95% CI = [9.18, 16.37], p < .001) ▫ Depression (β = − 0.31, 95% CI = [9.18, 16.37], p < .05) ● WHOQOL Social (ΔR2 = 0.34, F (4,46) = 7.51, p < .001) ▫ Depression (β = − 0.43, 95% CI = [11.21, 21.41], p < .05) ● WHOQOL Environmental (ΔR2 = 0.38, F (4,46) = 8.79, p < .001) ○ Posttraumatic growth (β = 0.33, 95% CI = [11.28, 18.86], p < .01) ▫ Depression (β = − 0.33, 95% CI = [11.28, 18.86], p < .05) ▫ Gender (β = − 0.26, 95% CI = [11.28, 18.86], p < .05) ▫ Unemployment (β = − 0.25, 95% CI = [11.28, 18.86], p < .05) |
Correlations ● Non-significant correlations reported between age and physical, psychological, social, environmental and overall QoL. ● Non-significant correlations reported between gender and physical, psychological, social, environmental and overall QoL. ● Non-significant correlation reported between overall QoL and unemployment Regression model ● Posttraumatic stress symptoms did not significantly predict any of the four domains of QoL ● Gender did not significantly predict physical, psychological or social QoL. ● Depressive symptoms did not significantly predict physical QoL ● Posttraumatic growth did not significantly predict social QoL ● Unemployment did not significantly predict physical, psychological or social QoL |
| Trilesnik et al. [38] | Germany | Not specified | 133 | Refugees | Cross-sectional | Psychosocial counseling centers | WHOQOL-BREF | WEMWBS, HSCL-25, HTQ, SCL-90, PMLDC, | ● Post-migration living difficulties and overall WHOQOL (r = −.54, p < .001) | ● No significant difference between post-treatment and pre-treatment levels of well-being. |
| Von Lersner et al. [39] | Germany | Bosnia, Serbia, Kosovo, Iraq, Turkey | 100 |
Refugees (Stayers vs.returnees) |
Cross-sectional | Refugee centres, language schools and doctors’ offices. | EUROHIS-QOL | PDS, MINI, |
● Stayers ○ Healthy participants vs. those with mental disorder(s) (t (37.4) = 5.65, p < .01) with healthy participants having higher QoL ▫ Age and QoL (r = −.39, p < .05) |
● No significant difference in returnees between mentally healthy participants and participants with at least one mental disorder on QoL |
a, bSame dataset has been used although they addressed different research questions. *Discrepancy exists between how the study used the measure and what the purpose of the measure was intended to be. AIS Anger idioms scale. BDI Beck Depression Inventory. BDQ Brief Disability Questionnaire. BSI Brief Symptom Inventory. CAPS Clinician Administered PTSD Scale. CES-D Self reported depression scale. CIDI World Health Organization Composite International Diagnostic Interview. CRI Coping Resources Inventory. CSQ Culture shock questionnaire. ETI Essen Trauma Inventory. FAD Family assessment device. GAD-7 General anxiety disorder. GAF General Activity Functioning Assessment Scale. GHQ-12 General Health Questionnaire. HDS Hamilton Depression Scale. HSCL-25 Hopkins Symptoms Checklist. HTQ Harvard Trauma Questionnaire. ICSEY International Comparative Study of Ethno-Cultural Youth Questionnaire. IES-R Impact of Event Scale-Revised. ISSI Interview Schedule of Social Interaction. LEC Life Events Checklist. MINI International Neuropsychiatric Interview 5.0.0. MSPSS Multidimensional scale of perceived social support. NA Not Assessed. PC-PTSD Primary care PTSD screen. PCL-C PTSD checklist civilian version. PDS Post traumatic Stress Diagnostic Scale. PHQ-9 Patient health questionnaire. PMLP Post Migration Living Problems. PTGI-SF Posttraumatic Growth Inventory Short Form. SASCAT Short version of the adapted social capital assessment tool. SCID-PTSD Structural Clinical Interview for DSM-IV-TR PTSD Module. SCL-90 Symptom Checklist. SDS Sheehan Disability Scale. SOC-13 Sense of Coherence Scale. F-SozU Social support questionnaire. WEMWBS Warwick Edinburgh Mental Well- Being Scale. WHOQOL-BREF World Health Organization Quality of Life-Bref. QLQ Quality of Life Questionnaire
●Main findings relevant to SWB and/or QoL
⎕Negative Predictor
○Positive Predictor
The WHOQOL-100 is the QoL questionnaire developed by the WHO [40]. It consists of 100 items, and each item is measured from on a 1 to 5 Likert scale. The internal consistency of the Danish version was high (Cronbach’s α = 0.97), with a test-retest reliability of 0.70 [41]. Furthermore, it has been validated in refugee populations [42].
The WHOQOL-BREF is the abbreviated version of the WHOQOL-100 [4] and contains 26 questions. The internal consistency of the WHOQOL-BREF was high (Cronbach’s α = 0.86), and demonstrated discriminant and construct validity (i.e. [43]). It has also been validated in refugee populations [44]. Lastly, the EUROHIS-QOL [45] is an 8-item index which is based on the WHOQOL-100 and WHOQOL-BREF. Each item is measured using the 1 to 5 Likert scale. It has demonstrated high internal consistency (Cronbach’s α = 0.80), and satisfactory convergent and discriminant validity [45].
Quality of cross-sectional studies
None of the seventeen cross-sectional studies met all 20 quality criteria of the AXIS tool, and although all of the cross-sectional studies met over half of the quality criteria, only 12 met 75% or more of these criteria. The study with the highest quality rating met nineteen of the quality criteria [22] and the study with the lowest quality rating met eleven of the quality criteria [24]. The quality assessment of each cross-sectional study can be found in Table 2.
Table 2.
Quality assessment of the included cross- sectional studies using the AXIS tool

1 = Carlsson et al. [19], 2 = Lee et al. [31], 3 = Correa-Velez et al. [22], 4 = Correa-Velez et al. [21], 5 = Georgiadou [23], 6 = Ghazinour et al. [24], 7 = Hengst et al. [25], 8 = Huijts et al. [26], 9 = Jesuthasan et al. [27], 10 = Laban et al. [29], 11 = Laban et al. [30], 12 = Leiler et al. [32], 13 = Regev et al. [34], 14 = Slonim-Nevo et al. [35], 15 = Teodorescu et al. [37], 16 = Trilesnik et al. [38], 17 = Von Lersner et al. [39]
 Quality met
Quality met
Quality not met
Unclear
Many methodological weaknesses were noted. Firstly, sample size justification (i.e. power calculation) was only reported by one study [38]. Five studies were unclear regarding sample selection, and one study was unclear regarding taking the sample frame from an appropriate population base [24]. Secondly, there were significant concerns regarding response bias as eight studies did not make a clear attempt to quantify the level of non-responders. Thirdly, five studies were unclear on standards used for determining statistical significance and/or precision estimates in their results section. This was due to insufficient detail regarding data management, significance levels, effect sizes and/or confidence intervals. Lastly, eight studies did not clearly report sources of funding and/or conflicts of interest. Five studies were not clear on whether ethical approval or consent had been obtained.
Quality of longitudinal studies
Table 3 provides details about the quality of the longitudinal studies. Five studies clearly defined their primary outcome, one did not [28]. Five also used validated measures, one did not [18]. All of the studies identified confounding factors, however two did not take them into account in the analysis, and two studies were unclear. Overall, a range of follow-up periods were used; 6-months, 7-months, 9-months, 12-months, 14-months, 23-months and 10-years.
Table 3.
Quality Assessment of the Included Longitudinal Studies using the CASP Tool
| CASP Tool | Carlsson et al. Baseline vs. 9-month follow-up [18] |
Carlsson, Olsen, Mortensen & Kastrup 10-year follow-up [20] |
Carlsson et al. Baseline vs 9 month vs. 23 month follow-up [17] |
Kinzie et al. Baseline vs- 12 month follow-up [28] | Löfvander et al. Baseline, 6- and 12-month follow-up [33] |
Stammel et al. Baselinve vs. 7 months vs. 14 months [36] |
|---|---|---|---|---|---|---|
| Did the study address a clearly focused issue? | Yes | Yes | Yes | No | Yes | Yes |
| Was the cohort recruited in an acceptable way? | No | Yes | Yes | Yes | Yes | Yes |
| Was the exposure accurately measured to minimise bias? | Cannot tell – no control group | Cannot tell – no control group | Yes | Cannot tell – no control group | Yes | Cannot tell – no control group |
| Was the outcome accurately measured to minimise bias? | Yes | Yes | Yes | Yes | Yes | Yes |
| Have the authors identified all important confounding factors? | Yes | Yes | No | Yes | Yes | Yes |
| Have they taken account of the confounding factors in the design and/or analysis? | No | No | Cannot tell | Cannot tell | Yes | Yes |
| Was the follow up of subjects complete enough? | Yes | Yes | Yes | Yes | Cannot tell | Cannot tell |
| What are the results of this study? | After a mean of 8 months of multidisciplinary treatment, mental symptoms and health-related quality of life did not change | The level of emotional distress was high at follow-up. Social relations and unemployment at follow-up were important predictors of mental health symptoms and low health-related quality of life. | Reduction in trauma /depression (baseline > 23 month) means. Minimal differences due to low effect sizes. Intervention not effective. | There were significant changes between means on the WHOQOL physical, mental and environmental domains after 1 year. | New immigrants did not have inferior physical or psychological health, quality-of-life, well-being or social functioning compared with their age- and sex-matched Swedish born pairs during a 1-year follow-up. | Quality of life increased significantly after an average of 14 months of treatment. |
| How precise are the results? | Cannot tell | Cannot tell | Cannot tell | Cannot tell | Cannot tell | Good |
| Do you believe the results? | Cannot tell | Cannot tell | Yes | No, more information is required | Cannot tell | Yes |
| Can the results be applied to the local population? | No | No | No | No | No | No |
| Do the results of this study fit with other available evidence? | Yes | Yes | Cannot tell | Cannot tell | No | No |
| What are the implications of this study for practice? |
When planning health-related and social interventions an increased focus is needed on the present exile situation, e.g., social relations, occupation and resources available in the present situation. |
Post migratory factors, such as social relations and occupation, are important for mental health and health-related quality of life. For the clinician dealing with severely traumatized refugees, it is important to be aware of a possible chronic condition. | Long-term follow-ups should be included in randomized trials focusing on the effects of different treatment approaches, including the appropriate length of treatment. | The results can have implications for the treatment of torture survivors. | General screening in unselected settings of refugees and new immigrants seems to be of little value. Clinical consultations in selected cases are to be preferred, adopting a holistic practical approach in patient and family-focused care. | It provides evidence for the efficacy of multidisciplinary treatment, more research needed. |
The two biggest limitations were that all studies lacked statistical precision (e.g. failing to state the confidence intervals or effect size), and the results cannot be applied to the local population as studies were conducted on very specific samples. There was a shortage of detail regarding follow-up assessments – three studies did not provide enough information on non-responders [18, 20, 33]. All but one [36] study did not clearly report effect sizes, variance accounted for by regression models, and/or the confidence intervals for the results. The quality assessment of each individual longitudinal study can be found in Table 3.
Overall quality of life (oQoL)
All WHOQOL-BREF domains positively correlated with each other [37]. There was evidence of differences in oQoL according to the time that had passed since arriving in the host country – Two studies, using the same sample, found that asylum seekers who had recently resettled (< 6 months) rated their oQoL higher than those who had lived in the host country for at least 2 years [29, 30]. Simultaneously, Stammel et al. found that refugees’ oQoL increased after 14 months of multidisciplinary treatment.
In terms of physical correlates, significant gender differences were found - males reported lower oQoL than females [24], and Regev et al. [34] found gender to be a significant negative predictor of oQoL, however the coding of variables was not reported. When compared to a non-refugee EU sample, a female refugee sample rated their oQoL significantly lower [27]. Being older (> 30 years) predicted lower oQoL [27], and was a negative correlate of oQoL [39].
Psychological associations with lower oQoL included, self-rated PTSD [26], posttraumatic stress [37], depression [23, 24, 37] and having one or more mental disorders, including depression, anxiety, PTSD and somatoform disorders [25]. Furthermore, experiencing the following adverse events was negatively associated with oQoL; near-death experiences [27], self-traumatic events [34], forced isolation [27], adverse events post-resettlement [30], and other traumatic experiences [25, 34].
When compared to individuals with a mental disorder, healthy individuals reported higher oQoL [39]. Sense of coherence was positively associated with oQoL [23, 24], with males reporting a significantly lower sense of coherence than females [24]. Exposure to other people’s traumatic events [34] and posttraumatic growth [37] were positive predictors of oQoL; and coping strategies [24, 26], availability and adequacy of attachment [24] correlated with increased oQoL. According to one study, coping strategies only led to an increase in oQoL for females [26]. Exposure to other people’s traumas was interpreted by the authors as potentially providing validation for people’s own experiences [34].
Weak social networks and poor social integration were social correlates of low oQoL [37]. Specific events that predicted lower oQoL included the unnatural loss of a child [25], attacks by family members2 [27], and number of lost family members [25].
Positive social predictors of oQoL focused on having social support [23, 26, 34]. Additionally, social integration [24] and having a spouse in the host country [23, 27], were associated with higher oQoL. One study suggested that social support was only a significant predictor for males [26].
Three of the environmental predictors that were investigated predicted low oQoL; prior mission/residence in a war zone [27], being sick without access to healthcare and long asylum procedures [25, 30]. Post-migration living difficulties negatively correlated with oQoL [38]. Similarly, one study found that North Korean refugees resettled in South Korea vs. those resettled in Japan had higher QoL, which the authors interpreted as being due to difficulties adapting to a new culture [31]. No positive predictors or correlates of eQoL were found.
The consideration of the direction, strength and consistency of the correlational analyses of the correlates of oQoL reported across studies is summarized in Fig. 2. For oQoL, both the strongest positive and negative correlations were found by Ghazinour et al. The strongest positive correlate found was between physical coping resources and psyQoL (r = 0.82, p < .001) and the strongest negative correlation found was between depression and psyQoL (r = − 0.86, p < .001) [24]. However, this study reported the lowest quality of the 23 studies included. The majority of strong positive correlations found for oQoL were mental correlates.
Physical quality of life (pQoL)
Laban et al. [30] found that asylum seekers who had recently resettled (< 6 months) rated their pQoL higher than those who had lived in the host country for at least 2 years [30]. On the other hand, Kinzie et al. [28] reported pQoL improved over time (1 year) for refugees who were undergoing treatment. Older age was a negative predictor of pQoL [30]. Negative Physical correlates of pQoL in AS&R were physical pain [19] and headaches [20]. The only positive Physical predictor found was region of birth, specifically being African was a positive predictor of pQoL [21].
Negative Psychological predictors of pQoL included diagnoses of depression [30], somatoform disorders [30], PTSD [35], having one or more mental disorders [30], and adverse life events post-migration [30]. Negative correlates of pQoL found were similar; depression [24, 32, 37], anxiety [32] and PTSD [32, 37]. Contrarily, coping strategies [24], availability and adequacy of attachment [24], were correlated with increased pQoL [37]. Posttraumatic growth was a positive predictor of pQoL [37].
One study reported on negative social predictors of pQoL and found that perceived discrimination [35] negatively predicted pQoL. Weak social networks [37] and poor social integration [37] were negatively correlated with pQoL. Positive social predictors were having social relations [19, 20] and feeling that most people in the community can be trusted [21]. Additionally, social integration was positively correlated with pQoL [24].
Living conditions post-resettlement, specifically socio-economic conditions [30] was a significant negative environmental predictor of pQoL. Unemployment was significantly negatively correlated with pQoL but was not a significant predictor [37]. Being employed [19, 20] and having completed either secondary or tertiary education [21] were significant environmental predictors of increased pQoL [19, 20]. Additionally, legal status increased pQoL, with refugees reporting higher pQoL than asylum seekers [35]. Lastly, place of resettlement was significant, as one study found that North Korean refugees resettled in South Korea vs. those resettled in Japan had higher QoL, which the authors interpreted as being due to difficulties adapting to a new culture [31].
Psychological quality of life (psyQoL)
Differing results were found for asylum seekers and refugees on psyQoL over time. Laban et al. [30] found that asylum seekers who had recently resettled (< 6 months) rated their pQoL higher than those who had lived in the host country for at least 2 years [30], whereas Kinzie et al. [28] reported psyQoL improved over time (1-year) for refugees who were undergoing multidisciplinary treatment [28]. Group comparisons over time between refugees and a non-migrant sample also showed that refugees scored significantly higher on psyQoL outcomes at baseline, 6 months and 12 months [33].
The only physical predictor for psyQoL was gender, with males reporting higher psyQoL overall [23]. Males also reported lower levels of independence and spirituality than females, which belong to the psychological domain [24].
Psychological predictors found to decrease psyQoL were depression [23, 37], anxiety [36,], PTSD [30, 35], and somatoform disorders [30]. Negative correlates for psyQoL found were similar; depression [24, 32, 37], anxiety [32] and PTSD [32, 37].
Psychological correlates for an increased psyQoL were self-evaluations of improved MH during treatment [18] coping strategies [24], and availability and adequacy of attachment [24]. Sense of coherence and posttraumatic growth [37] positively predicted psyQoL [23].
Negative social predictors reported were perceived discrimination [35], and number of key persons who provide no support [21]. Having a weak social network and poor social integration negatively correlated with psyQoL [37]. Findings on positive social predictors relevant to psyQoL highlighted the importance of social support [19, 20, 23], feeling that most people in the community can be trusted [21], and having one’s spouse in the host country [23]. Additionally, social integration [24] positively correlated with psyQoL.
The only significant negative environmental predictor of psyQoL was poor socio-economic living conditions post-resettlement [30]. Unemployment was a negative correlate [37]. Lastly, place of resettlement was significant as one study found that North Korean refugees resettled in South Korea vs. those resettled in Japan had higher QoL [31].
Social quality of life (sQoL)
There were two physical correlates of sQoL - having headaches predicted lower sQoL [20], and Gender. Löfvander et al. [33], noted that whereas the male refugees had higher sQoL compared to Swedish born controls (matched for age and gender) at the three assessment points (baseline, 6 months and 12-month follow-up), female refugees had significantly higher sQoL relative to Swedish born matched controls at baseline assessment only. Another study reported males had lower sQoL than female refugees [24].
Negative psychological correlates of sQoL reported were; depression [24, 32, 37], anxiety [32], PTSD [32], and post-traumatic stress [37]. PTSD [35] and depression [37] were negative predictors of sQoL. Availability and adequacy of attachment [24], and coping strategies [24] were positively correlated with sQoL, and posttraumatic growth positively predicted sQoL [37]. Perceived discrimination [35], was a significant negative social predictor of sQoL. Simultaneously, weak social network [37], and poor social integration [37] were negatively correlated with sQoL. Social integration [24] and being married with a spouse in the host country [23] were positively correlated with sQoL, and social relations [19, 20], positively predicted sQoL.
Employment was the only environmental predictor found to increase sQoL [20], and unemployment was found to decrease sQoL [37] Additionally, one study found that North Korean refugees resettled in South Korea vs. those resettled in Japan had higher QoL, which the authors interpreted as being due to difficulties adapting to a new culture [31].
Environmental quality of life (eQoL)
Three studies revealed the eQoL increased over time for refugees, after 9-months [17], 12-months [28] and 23-month follow-up [17].
Laban et al. [30] found that asylum seekers who had recently resettled (< 6 months) rated their eQoL higher than those who had lived in the host country for at least 2 years [30].
In terms of negative physical predictors of eQoL, studies reported on the presence of pain [19] and headache [20]. Gender was also a predictor of eQoL; however, the authors did not specify how gender was coded [37]. However, Ghazinour et al. [24], found that males reported lower eQoL than females.
The negative psychological predictors of eQoL were self-rated PTSD [30], and depression [37]. Negative correlates found were similar; depression [24, 32], anxiety [32] and PTSD [32] negatively correlated with pQoL. Positive psychological correlates of eQoL were coping strategies [24], availability and adequacy of attachment [24]. Posttraumatic growth was a positive predictor of eQoL [37].
Perceived discrimination [35], was a significant negative predictor of eQOL. Poor social integration and having a weak social network [37] were negatively correlated with eQOL. The significant positive social predictor identified for eQOL was having social relations [19, 20]. Social integration [24] positively correlated with eQoL and having one’s spouse in the host country was associated with higher eQoL, as compared to not having one’s partner in the host country [23].
The negative environmental predictors found comprised socio-economic living conditions post resettlement (including living in regional areas as opposed to central areas) [22, 30], post-migration living difficulties [35], unemployment [37], and socio-religious aspects, such as a lack of contact with people of the same religion [30]. The significant positive environmental predictor of eQoL was being employed [20]. Additionally, place of resettlement was found to be significant in two studies; Correa-Velez et al. [22] found that living in regional areas was a positive predictor of eQoL, and Lee et al. [31] found that North Korean refugees resettled in South Korea vs. those resettled in Japan had higher QoL.
Differences between asylum seekers and refugees
Sixteen of the included studies focused on refugees, three on asylum seekers and four used mixed samples or terminology. Only nine studies (39.1%) gave the specific criteria used to define their sample as either a refugee or asylum-seeking population (i.e. by law). This is important as some studies used mixed terminologies or did not distinguish between the two. Given that asylum seekers and refugees constitute different populations with different needs, this distinction is important. Only two studies specifically compared asylum seekers to refugees [32, 35]. Leiler et al. [32] found no significant differences between them on any of the four QoL domains nor in oQoL. Slonim-Nevo [35] did find that having a legal status positively predicted pQoL. Similarly, long asylum procedures were found to be a negative predictor for oQoL by all three studies that focused exclusively on asylum seekers [25, 29, 30]. However, Laban et al. [30] did not find long asylum procedures to be a significant predictor for pQoL specifically. Furthermore, for asylum seekers, QoL did not appear to improve over time whereas for refugees findings suggest that it does.
Discussion
To date, there has been a paucity of efforts to synthesize evidence relating to predictors and correlates of QoL of AS&Rs. The current review sought to address this gap, so that policy makers and organizations working to support AS&Rs in high-income countries can be guided by an improved understanding about what enhances the lived experience of AS&Rs. Key findings across the various forms of QoL (overall, physical, psychological, social and environmental) were that having established social networks and social integration were associated with higher QoL, whereas having mental disorders (i.e. PTSD or depression) was strongly associated with reduced QoL. Physical predictors and correlates were the least reported.
Psychological predictors and correlates (including the presence of mental disorders) of QoL were the most extensively studied and reported across studies. The predictors and correlates of QoL noted in the current review can be compared with predictors of common mental disorders (CMD) identified in previous reviews. For example, Bogic et al. [46] found that poor post-migration socio-economic status including unemployment, low income, poor host language proficiency and lack of social support were each associated with depression experienced by war-affected refugees. These findings overlap with those found in the current review. However, there were also important points of distinction; the current review showed that having a spouse was positively associated with increased QoL, whereas Bogic et al. [46] did not find any consistent association between marital status and mental disorders. Furthermore, this review showed that positive coping strategies were highly associated with increased QoL, whereas Bogic et al. [46] indicated that these factors had not been assessed in studies exploring mental disorders experienced by war-affected refugees. To ensure that AS&Rs are afforded the opportunity to enjoy full and meaningful lives, it will be important to understand and address not only factors associated with mental disorders, but also those uniquely associated with QoL.
The associations that QoL had with various social factors and environmental factors, point to the value of extensive integration programs that include housing and employment assistance [47]. Unfortunately, however, in many high-income countries, AS&Rs face social exclusion, restricted employment opportunities, and/or below average earnings [48]. The current review highlighted that having weak social networks, and poor social integration were both moderately correlated with lower overall QoL. Those involved in developing migrant integration policies need to be cognizant of the associations that QoL have with various aspects of the socio-ecological context that AS&Rs live in. Most European governments and other OECD countries outside Europe have imposed employment bans or time constraints to asylum seekers entering the labor market [49, 50]. Although asylum policies vary by country, region, and even over time within a country, such policies generally lead to long waiting periods in which asylum seekers find themselves in a legal and social limbo, without the ability to work and integrate. Research has shown that longer waiting times to obtain a refugee status strongly reduces employment integration of refugees (i.e. [51–53]) and can also reduce social integration (i.e. [54, 55]). Therefore, the findings of the current review should be considered by policymakers as being consistent with a need to reduce asylum procedure times, in order to promote socio-economic integration, reduce the risk of marginalization and mental ill-health, and overall increase the QoL of AS&R populations. The discourse must shift from a narrative regarding AS&R as being a burden on society to seeing their support as an investment in the social and economic framework of the host country.
Regarding methodological quality, studies had moderate to good quality overall with more recent publications generally scoring higher on quality assessment. There was a tendency to recruit opportunistic samples through health centers, which may have resulted in a bias towards AS&R who were already seeking care and with greater support systems rather than more marginalized individuals. This limits the generalizability of findings. Evidence of basic design flaws, and the predominance of cross-sectional methodologies were important limitations of the available evidence base. Moving forward more transparency is required regarding sampling procedures and non-responders. Furthermore, authors need to clearly state sources of funding and possible conflicts of interest that may have led to outcome bias.
Future research and implications
The current review has highlighted a need for research to further explore factors positively associated with QoL. Mixed-method approaches may be used to allow for a qualitative exploration of context and culture, together with a quantitative prediction. Longitudinal studies aimed at exploring causal relationships that variables (including mental disorders) potentially have with QoL are required. Specifically more research is needed on environmental and physical correlates and predictors of QoL. Clinical trials of interventions conducted with AS&R populations that employ instruments assessing QoL as primary outcomes is required. This is a particularly worthy area of research focus in light of the fact that many people opt not to engage with treatments for mental disorders owing to the stigma that it can bring [56].
Limitations of this review
The exclusion of grey literature may have introduced a publication bias into the findings presented in the current review. However, the peer review process for journal submission was used as a form of minimal quality assurance for the studies included in the review.
Similarly, the exclusion of articles that were not written in a language spoken by the authors (English, Spanish or Dutch) may have introduced a language bias. These decisions were made due to authors’ language proficiency and a lack of time to arrange translating resources. Therefore, publications on other languages should be considered an area for future research.
The samples of the included studies varied significantly with respect to country of origin, time since resettlement, year and country of study publication. However, this reflects the reality that AS&Rs populations tend to be very diverse in terms of their personal circumstances. Furthermore, studies recruiting AS&Rs in low- and middle-income countries were excluded given that this review aimed to support efforts to provide further evidence to guide health and social care policy that could inform the support of AS&R in high-income countries. As the majority of the world’s AS&R live in low- and middle- income countries [1], this limitation highlights the importance of further research concerning the factors influencing AS&Rs’ QoL in low and middle-income settings. The analyses used in the studies included in the current review do not permit causal relationships to be inferred. Finally, there was heterogeneity in the measures of QoL used and this limited efforts to synthesize the findings. Consideration was also given to conducting a meta-analysis but given the large heterogeneity of available data, a meta-analysis was deemed inappropriate.
Conclusion
In summary, this review expands knowledge on the predictors and correlates of QoL in AS&R populations. The findings highlight that there are significant physical, psychological, social and environmental predictors and correlates that affect QoL in AS&Rs. Overall, the majority of strong positive correlations found for oQoL were MH related correlates. Positive MH is a key determinant for good integration [57, 58], and good integration is a determinant of good MH [59]. Efforts to develop and deliver interventions to support AS&Rs need to be aware of QoL as an important outcome and target important determinants thereof.
Supplementary information
Additional file 1. Appendix B Positive and negative predictors of overall QoL and each of the four domains.
Acknowledgements
Not applicable.
Appendix
Database Search Strategy
The databases searched were Medline, PsycINFO, CINAHL, Cochrane Library, Health Technology Assessment, National Health Service Economic Evaluation, Educational Resource Index and Abstracts, BiblioMap, Scopus, Social Sciences Citation Index, Evidence Aid, DARE, Web of Science and PubMed) up to 5th of May, 2020. The Scopus database enabled searching Embase articles not indexed in the previous databases.
Search Strategy.
| Concept | Keywords | Controlled Vocabulary | Example database Psychinfo |
|---|---|---|---|
| • Asylum seekers | Asylum seeker | Asylum Seeker | • Asylum Seekers OR Refugees OR political asylum OR political refugee |
| • Refugees | Refugee | Seekers, Asylum | • asylum N2 seek* OR refuge* OR |
| • Political asylum | Political asylum | Refugee | Seeker*, Asylum OR political N2 asylum OR political N2 refuge* |
| • Political refugees | Political refugees | Stateless people | |
| • Adults | Adults | Political asylum | • Adult* |
| Political refugees | |||
| Adult | |||
| • Quality of Life | Wellbeing | Wellbeing | ·Wellbeing OR Subjective wellbeing OR Psychological wellbeing OR Emotional wellbeing OR Quality of life OR QoL OR Life quality OR Health-related quality of life OR Life satisfaction OR Satisfaction with life |
| • Wellbeing | Subjective wellbeing | Subjective wellbeing | |
| Psychological wellbeing | Psychological wellbeing | ||
| Emotional wellbeing | Emotional wellbeing | ||
| Quality of life | Quality of life | ·Well N2 being OR Subjective N3 well N2 being OR Psychological N3 well N2 being OR Emotional N3 well N2 being OR Quality N3 of N3 life OR QoL OR Life N2 quality OR Health N2 related N5 quality N3 of N3 life | |
| Life quality | QoL | ||
| Life satisfaction | Life quality | ||
| Health-related quality of life | |||
| Life satisfaction | OR Life N3 satisfaction | ||
| Satisfaction with life | |||
| • Predictive Terms | Predictor | Predictor | · predictor OR correlation OR determinant |
| Correlation | Correlation Determinant | ·predict* OR correlat* | |
| Determinant | OR determin* |
Authors’ contributions
The substantive contribution of author CB has been the conception and design of the research, conducting the literature review, carrying out the analysis and interpretation of the findings, writing the paper and doing critical revision. Author RA has contributed by peer-reviewing the methodology and revising the final manuscript. The contribution of author CD has been to support the conception of the review and providing a critical review for its intellectual content. Author SN assisted with the synthesising of the review findings and the revising of the final manuscript. Author RW has supervised the conduct of the work, including taking part in the conception of the review, peer reviewing the methodology, analysis and interpretation, revising of the final manuscript and providing critical revision of the overall review. All authors read and approved the final manuscript.”
Authors’ information
Dr. Ross White is the Research Director on the Doctorate of Clinical Psychology training programme and the Interim Head of Primary Care and Mental Health of the Institute of Population Health at the University of Liverpool.
Professor Christopher Dowrick is a Professor of Primary Medical Care. Additionally, he works as a General Practitioner and is a Professorial Research Fellow with the Department of General Practice in the University of Melbourne, and Chair of the Working Party for Mental Health in the World Organisation of Family Doctors.
Dr. Sarah Nevitt is a research associate in the Department of Biostatistics at the University of Liverpool.
Miss Rebekah Amos is a PhD candidate and demonstrator at the School of Psychology at the University of Liverpool.
Miss Catharina van der Boor is a PhD candidate and demonstrator at the School of Psychology at the University of Liverpool.
Funding
This work was supported by the Economic and Social Research Council [ES/S000976/1].
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
This article does not contain any studies with human participants or animals performed by any of the authors.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Further information on the classification of countries per income can be found at: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519
This terminology was replicated from the study itself, the authors of the study do not specify what is meant specifically with this term.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary information accompanies this paper at 10.1186/s13031-020-00292-y.
References
- 1.United Nations High Commissioner for Refugees. Global Trends Forced Displacement in 2018. 2019. Retrieved April 27, 2020, from https://www.unhcr.org/5d08d7ee7.pdf.
- 2.Turrini G, Purgato M, Ballette F, Nosè M, Ostuzzi G, Barbui C. Common mental disorders in asylum seekers and refugees: umbrella review of prevalence and intervention studies. Int J Ment Heal Syst. 2017;11(1):51. doi: 10.1186/s13033-017-0156-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.World Health Organization . WHOQOL Measuring Quality of Life. Geneva: World Health Organisation; 1997. [Google Scholar]
- 4.WHOQOL Group Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol Med. 1998;28(3):551–558. doi: 10.1017/s0033291798006667. [DOI] [PubMed] [Google Scholar]
- 5.Charlson F, van Ommeren M, Flaxman A, Cornett J, Whiteford H, Saxena S. New WHO prevalence estimates of mental disorders in conflict settings: a systematic review and meta-analysis. Lancet. 2019;394(10194):240–248. doi: 10.1016/S0140-6736(19)30934-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Akinyemi OO, Owoaje ET, Ige OK, Popoola OA. Comparative study of mental health and quality of life in long term refugees and host populations in Oru-Ijebu, Southwest Nigeria. BMC Res Notes. 2012;5(1):394. doi: 10.1186/1756-0500-5-394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Matanov A, Giacco D, Bogic M, Ajdukovic D, Franciskovic T, Galeazzi GM, Kucukalic A, Lecic-Tosevski D, Morina N, Popovski M, Schützwohl M. Subjective quality of life in war-affected populations. BMC Public Health. 2013;13(1):624. doi: 10.1186/1471-2458-13-624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bosqui TJ, Marshoud B. Mechanisms of change for interventions aimed at improving the wellbeing, mental health and resilience of children and adolescents affected by war and armed conflict: a systematic review of reviews. Confl Heal. 2018;12(1):15. doi: 10.1186/s13031-018-0153-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Turrini G, Purgato M, Acarturk C, Anttila M, Au T, Ballette F, Bird M, Carswell K, Churchill R, Cuijpers P, Hall J. Efficacy and acceptability of psychosocial interventions in asylum seekers and refugees: systematic review and meta-analysis. Epidemiol Psychiatr Sci. 2019;28(4):376–388. doi: 10.1017/S2045796019000027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kings College London. Searching for Systematic Reviews: Advanced search Techniques. http://libguides.kcl.ac.uk/systematicreview/advanced.
- 11.Field AP. Meta-analysis of correlation coefficients: a Monte Carlo comparison of fixed-and random-effects methods. Psychol Methods. 2001;6(2):161. doi: 10.1037/1082-989x.6.2.161. [DOI] [PubMed] [Google Scholar]
- 12.Hedges LV, Olkin I. Statistical methods for meta-analysis. Academic press. 2014. [Google Scholar]
- 13.Riley RD, Moons KG, Snell KI, Ensor J, Hooft L, Altman DG, Hayden J, Collins GS, Debray TP. A guide to systematic review and meta-analysis of prognostic factor studies. Bmj. 2019;364:k4597. doi: 10.1136/bmj.k4597. [DOI] [PubMed] [Google Scholar]
- 14.Cohen J. Statistical power analysis for the behavioral sciences: Routledge; 2013.
- 15.Downes MJ, Brennan ML, Williams HC, Dean RS. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS) BMJ Open. 2016;6(12):e011458. doi: 10.1136/bmjopen-2016-011458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Critical Appraisal Skills Programme. CASP (Cohort Study) Checklist. [online] Available at: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Cohort-Study-Checklist_2018.pdf. 2018. [Accessed: 17 Dec 2018].
- 17.Carlsson JM, Olsen DR, Kastrup M, Mortensen EL. Late mental health changes in tortured refugees in multidisciplinary treatment. J Nerv Ment Dis. 2010;198(11):824–828. doi: 10.1097/NMD.0b013e3181f97be3. [DOI] [PubMed] [Google Scholar]
- 18.Carlsson JM, Mortensen EL, Kastrup M. A follow-up study of mental health and health-related quality of life in tortured refugees in multidisciplinary treatment. J Nerv Ment Dis. 2005;193(10):651–657. doi: 10.1097/01.nmd.0000180739.79884.10. [DOI] [PubMed] [Google Scholar]
- 19.Carlsson JM, Mortensen EL, Kastrup M. Predictors of mental health and quality of life in male tortured refugees. Nordic J Psychiatr. 2006;60(1):51–57. doi: 10.1080/08039480500504982. [DOI] [PubMed] [Google Scholar]
- 20.Carlsson JM, Olsen DR, Mortensen EL, Kastrup M. Mental health and health-related quality of life: a 10-year follow-up of tortured refugees. J Nerv Ment Dis. 2006;194(10):725–731. doi: 10.1097/01.nmd.0000243079.52138.b7. [DOI] [PubMed] [Google Scholar]
- 21.Correa-Velez I, Green A, Murray K, Schweitzer RD, Vromans L, Lenette C, Brough M. Social context matters: predictors of quality of life among recently arrived refugee women-at-risk living in Australia. Journal of Immigrant & Refugee Studies. 2020. pp. 1–17. [Google Scholar]
- 22.Correa-Velez I, Barnett AG, Gifford SM, Sackey D. Health status and use of health services among recently arrived men with refugee backgrounds: a comparative analysis of urban and regional settlement in south-East Queensland. Aust J Prim Health. 2011;17(1):66–71. doi: 10.1071/PY10051. [DOI] [PubMed] [Google Scholar]
- 23.Georgiadou E, Schmitt GM, Erim Y. Does the separation from marital partners of Syrian refugees with a residence permit in Germany have an impact on their quality of life? J Psychosom Res. 2020;109936. [DOI] [PubMed]
- 24.Ghazinour M, Richter J, Eisemann M. Quality of life among Iranian refugees resettled in Sweden. J Immigr Health. 2004;6(2):71–81. doi: 10.1023/B:JOIH.0000019167.04252.58. [DOI] [PubMed] [Google Scholar]
- 25.Hengst SM, Smid GE, Laban CJ. The effects of traumatic and multiple loss on psychopathology, disability, and quality of life in Iraqi asylum seekers in the Netherlands. J Nerv Ment Dis. 2018;206(1):52–60. doi: 10.1097/NMD.0000000000000750. [DOI] [PubMed] [Google Scholar]
- 26.Huijts I, Kleijn WC, van Emmerik AA, Noordhof A, Smith AJ. Dealing with man-made trauma: the relationship between coping style, posttraumatic stress, and quality of life in resettled, traumatized refugees in the Netherlands. J Trauma Stress. 2012;25(1):71–78. doi: 10.1002/jts.21665. [DOI] [PubMed] [Google Scholar]
- 27.Jesuthasan J, Sönmez E, Abels I, Kurmeyer C, Gutermann J, Kimbel R, Krüger A, Niklewski G, Richter K, Stangier U, Wollny A. Near-death experiences, attacks by family members, and absence of health care in their home countries affect the quality of life of refugee women in Germany: a multi-region, cross-sectional, gender-sensitive study. BMC Med. 2018;16(1):15. doi: 10.1186/s12916-017-1003-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kinzie JD, Kinzie JM, Sedighi B, Woticha A, Mohamed H, Riley C. Prospective one-year treatment outcomes of tortured refugees: a psychiatric approach. Torture. 2012;22(1):1–10. [PubMed] [Google Scholar]
- 29.Laban CJ, Gernaat HB, Komproe IH, De Jong JT. Prevalence and predictors of health service use among Iraqi asylum seekers in the Netherlands. Soc Psychiatry Psychiatr Epidemiol. 2007;42(10):837–844. doi: 10.1007/s00127-007-0240-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Laban CJ, Komproe IH, Gernaat HB, de Jong JT. The impact of a long asylum procedure on quality of life, disability and physical health in Iraqi asylum seekers in the Netherlands. Soc Psychiatry Psychiatr Epidemiol. 2008;43(7):507. doi: 10.1007/s00127-008-0333-1. [DOI] [PubMed] [Google Scholar]
- 31.Lee CH, Min SK, Jeon WT, Kigawa M, Sugawara M. Mental health and quality of life of north Korean defectors living in Japan. Asian J Psychiatr. 2009;2(3):95–99. doi: 10.1016/j.ajp.2009.07.001. [DOI] [PubMed] [Google Scholar]
- 32.Leiler A, Bjärtå A, Ekdahl J, Wasteson E. Mental health and quality of life among asylum seekers and refugees living in refugee housing facilities in Sweden. Soc Psychiatry Psychiatr Epidemiol. 2019;54(5):543–551. doi: 10.1007/s00127-018-1651-6. [DOI] [PubMed] [Google Scholar]
- 33.Löfvander M, Rosenblad A, Wiklund T, Bennström H, Leppert J. A case–control study of self-reported health, quality-of-life and general functioning among recent immigrants and age-and sex-matched Swedish-born controls. Scand J Public Health. 2014;42(8):734–742. doi: 10.1177/1403494814550175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Regev S, Slonim-Nevo V. Sorrow shared is halved? War trauma experienced by others and mental health among Darfuri asylum seekers. Psychiatry Res. 2019;273:475–480. doi: 10.1016/j.psychres.2019.01.049. [DOI] [PubMed] [Google Scholar]
- 35.Slonim-Nevo V, Regev S, Millo Y. The psycho-social conditions of asylum-seekers from Darfur in Israel. Refuge. 2015;31(2):25–38. [Google Scholar]
- 36.Stammel N, Knaevelsrud C, Schock K, Walther LC, Wenk-Ansohn M, Böttche M. Multidisciplinary treatment for traumatized refugees in a naturalistic setting: symptom courses and predictors. Eur J Psychotraumatology. 2017;8(sup2):1377552. doi: 10.1080/20008198.2017.1377552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Teodorescu DS, Siqveland J, Heir T, Hauff E, Wentzel-Larsen T, Lien L. Posttraumatic growth, depressive symptoms, posttraumatic stress symptoms, post-migration stressors and quality of life in multi-traumatized psychiatric outpatients with a refugee background in Norway. Health Qual Life Outcomes. 2012;10(1):84. doi: 10.1186/1477-7525-10-84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Trilesnik B, Eckhoff L, Özkan I, Loos K, Penteker G, Graef-Calliess IT. Implementing a need-adapted stepped-care model for mental health of refugees: pilot data of the state-funded project “refuKey”. Anxiety. 2019;85:75–79. doi: 10.3389/fpsyt.2019.00688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Von Lersner U, Wiens U, Elbert T, Neuner F. Mental health of returnees: refugees in Germany prior to their state-sponsored repatriation. BMC Int Health Hum Rights. 2008;8(1):8. doi: 10.1186/1472-698X-8-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.World Health Organization . Field trial WHOQOL-100 February 1995: the 100 questions with response scales. World Health Organization. 1995. [Google Scholar]
- 41.Bech VNP. The WHO quality of life (WHOQOL) questionnaire: Danish validation study. Nordic J Psychiatr. 2001;55(4):229–235. doi: 10.1080/080394801681019075. [DOI] [PubMed] [Google Scholar]
- 42.De Vries J, Van Heck GL. Quality of life and refugees. Int J Ment Health. 1994;23(3):57–75. [Google Scholar]
- 43.Sreedevi A, Cherkil S, Kuttikattu DS, Kamalamma L, Oldenburg B. Validation of WHOQOL-BREF in Malayalam and determinants of quality of life among people with type 2 diabetes in Kerala, India. Asia Pac J Public Health. 2016;28(1_suppl):62S–69S. doi: 10.1177/1010539515605888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Redko C, Rogers N, Bule L, Siad H, Choh A. Development and validation of the Somali WHOQOL-BREF among refugees living in the USA. Qual Life Res. 2015;24(6):1503–1513. doi: 10.1007/s11136-014-0877-3. [DOI] [PubMed] [Google Scholar]
- 45.Schmidt S, Mühlan H, Power M. The EUROHIS-QOL 8-item index: psychometric results of a cross-cultural field study. Eur J Public Health. 2006;16(4):420–428. doi: 10.1093/eurpub/cki155. [DOI] [PubMed] [Google Scholar]
- 46.Bogic M, Njoku A, Priebe S. Long-term mental health of war-refugees: a systematic literature review. BMC Int Health Hum Rights. 2015;15(1):29. doi: 10.1186/s12914-015-0064-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Valenta M, Bunar N. State assisted integration: refugee integration policies in Scandinavian welfare states: the Swedish and Norwegian experience. J Refug Stud. 2010;23(4):463–483. [Google Scholar]
- 48.Phillimore J, Goodson L. Problem or opportunity? Asylum seekers, refugees, employment and social exclusion in deprived urban areas. Urban Stud. 2006;43(10):1715–1736. [Google Scholar]
- 49.Organisation for Economic Co-operation and Development. Making integration work: refugees and others in need of protection: OECD Publishing; 2016.
- 50.European Council on Refugees and Exiles (ECRE) (2016) ‘The length of asylum procedures in Europe’, October, http://www.ecre.org/wp-content/uploads/2016/10/AIDA-Brief-DurationProcedures.pdf.
- 51.Bloch A. Refugees' opportunities and barriers in employment and training. Leeds: Corporate Document Services; 2002. [Google Scholar]
- 52.Hainmueller J, Hangartner D, Lawrence D. When lives are put on hold: lengthy asylum processes decrease employment among refugees. Sci Adv. 2016;2(8):e1600432. doi: 10.1126/sciadv.1600432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Warfa N, Curtis S, Watters C, Carswell K, Ingleby D, Bhui K. Migration experiences, employment status and psychological distress among Somali immigrants: a mixed-method international study. BMC Public Health. 2012;12(1):749. doi: 10.1186/1471-2458-12-749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Bakker L, Dagevos J, Engbersen G. The importance of resources and security in the socio-economic integration of refugees. A study on the impact of length of stay in asylum accommodation and residence status on socio-economic integration for the four largest refugee groups in the Netherlands. J Int Migr Integr. 2014;15(3):431–448. [Google Scholar]
- 55.Phillimore J. Refugees, acculturation strategies, stress and integration. J Soc Pol. 2011;40(3):575–593. [Google Scholar]
- 56.Corrigan PW, Druss BG, Perlick DA. The impact of mental illness stigma on seeking and participating in mental health care. Psychol Sci Public Interest. 2014;15(2):37–70. doi: 10.1177/1529100614531398. [DOI] [PubMed] [Google Scholar]
- 57.Robila M. Refugees and social integration in Europe. United Nations Department of Economic and Social Affairs (UNDESA) 2018. [Google Scholar]
- 58.Schick M, Zumwald A, Knöpfli B, Nickerson A, Bryant RA, Schnyder U, Müller J, Morina N. Challenging future, challenging past: the relationship of social integration and psychological impairment in traumatized refugees. Eur J Psychotraumatol. 2016;7(1):28057. doi: 10.3402/ejpt.v7.28057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Haasen C, Demiralay C, Reimer J. Acculturation and mental distress among Russian and Iranian migrants in Germany. Eur Psychiatr. 2008;23:10–13. doi: 10.1016/S0924-9338(08)70056-7. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1. Appendix B Positive and negative predictors of overall QoL and each of the four domains.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.