

Abstract
The proliferation of misinformation on social media platforms is faster than the spread of Corona Virus Diseases (COVID-19) and it can generate hefty deleterious consequences on health amid a disaster like COVID-19. Drawing upon research on the stimulus-response theory (hypodermic needle theory) and the resilience theory, this study tested a conceptual framework considering general misinformation belief, conspiracy belief, and religious misinformation belief as the stimulus; and credibility evaluations as resilience strategy; and their effects on COVID-19 individual responses. Using a self-administered online survey during the COVID-19 pandemic, the study obtained 483 useable responses and after test, finds that all-inclusive, the propagation of misinformation on social media undermines the COVID-19 individual responses. Particularly, credibility evaluation of misinformation strongly predicts the COVID-19 individual responses with positive influences and religious misinformation beliefs as well as conspiracy beliefs and general misinformation beliefs come next and influence negatively. The findings and general recommendations will help the public, in general, to be cautious about misinformation, and the respective authority of a country, in particular, for initiating proper safety measures about disastrous misinformation to protect the public health from being exploited.
Keywords: Coronavirus, Misinformation, Credibility evaluation, Social media, COVID-19 individual response
1. Introduction
Though the year “2020”, due to the COVID-19 pandemic, is called “super year” for environmental sustainability [20], the year is posing a massive global health threat as well as extreme socioeconomic damage. Its global impact on lives and livelihoods is beyond measure as the fight against the COVID-19 is continuing [50]. The public across the world has recognized the severe damaging magnitudes of COVID 19 due to the fast communication and publication [73]. However, the world's first social media pandemic COVID-19 [31], a massive disaster in the 21st century, is not immune to the proliferation of misinformation [58]. Director-General of the World Health Organization (WHO) declared that the COVID-19 epidemic is going through an ‘infodemic’ (shorthand for information epidemic) of misinformation [77]. On March 28, in line with WHO, Antonio Guterres, the Secretary-General of United Nation, tweet that “Our common enemy is COVID19, but our enemy is also an ‘infodemic’ of misinformation” on his personal Twitter account [71]. Besides, researchers also noted that the medical misinformation content pertaining to the COVID-19 pandemic is being proliferated at a frightening rate on social media [27,42]. By referring WHO, Shaw et al. [62] mentioned that there will be a tsunami of information on social media. Further, Brennen et al. [12] orated that misinformation pertaining to the global health crisis COVID-19 pandemic generates a severe risk to public health.
The internet has become the greatest source of health information worldwide due to the use of a huge number of mobile devices and easy and low-cost connectivity with the internet across the world. Barua et al. [5] stated that internet technologies are becoming inexpensive and easy to access. Statista [66] reported that the global mobile population surpasses 4 billion unique users, according to April 2019 data, and as of February 2019, there was global 48% of web page views through mobile devices, and, Asia and Africa leading the pack. Li et al. [44] noted that over 70% of adults use internet services for searching healthcare-related information. Wang et al. [85] reported that 93.5% of the general public in China used the internet as the primary health care information conduit during the initial stage of COVID-19 pandemic. Li et al. [44] reported that approximately 23%–26% of YouTube videos were misleading, i.e. involved in disseminating misinformation regarding COVID-19. On the other hand, another popular social networking site, Facebook, reported that during the March and April of 2020 the body placed warning labels on approximately 90 million pieces of content because they are allied to the Covid-19 misinformation like false cures, anti-vaccination propaganda and conspiracy theories [7]. BBC also reported that the human cost of misinformation could be huge since it undermines the public health messaging [7]. Researchers [36,38,45,63] noted that it can intensify racism, fear, and stigma and produce unconstructive and threatening behavior. Because of fear, the public shows an unusual pattern of shopping behavior in purchasing personal protective equipment [1]. Chou et al. [13] opined that health misinformation on social media can induce people to use toxic substances. Zandifar & Badrfam [88] suggested that misinformation along with other players regarding COVID-19 can contribute to stress and mental morbidity. Rajkumar [56] and Xiao and Torok [86] suggested that amid an infectious disease pandemic, inaccurate or misinformation or exaggerated information can generate health anxiety. In addition, the misinformation effect is also associated with buying and taking drugs without a medical consultant's prescription [16]. Misinformation in different media including social media, therefore, can have a death-and-life threatening effect amid a pandemic. For instance, a resident of Phoenix in the USA, hearing on the news that the chloroquine can cure COVID-19, died after consuming chloroquine which was commonly used at aquariums to clean fish tanks [84].
This misinformation about COVID-19 is generating in many forms, such as conspiracy theories which convey the virus being produced in a laboratory for use as a biological weapon [53]; religious fundamentalist who spread misinformation in the way that praying to the almighty will help not to be affected by COVID-19. The religions can play dual roles amid pandemic as constructive and detrimental [21]. Researchers noted that developing a theory for the pathways of the effects of misinformation on public health would greatly help to understand the mitigation of adverse consequences of misinformation [68]. Further, in search of solution about misinformation regarding COVID-19 pandemic on social media conduit, Dr. Mike Ryan, Executive Director of WHO's Health Emergencies Programme said that ‘we need a vaccine against misinformation,’ [78], and he also urges social science researchers to come forward in this regard. Consequently, this study developed a conceptual framework to empirically examine the effects of misinformation on COVID-19 individual responses and how to resilience it conjoining the stimulus-response theory (hypodermic needle theory) and the resilience theory. As the stimulus, this study has considered general misinformation belief, conspiracy belief, and religious misinformation belief; and as resilience strategy, credibility evaluations. The authors hope that the findings of this study and applicable recommendations will work as good ground to mitigate the disaster of misinformation.
The remainder of this paper is organized as follows. The next section presents the literature review relevant to misinformation, COVID-19, individual responses. Section 3 offers the conceptual framework and proposes the relevant research hypotheses based on the literature. Section 4 and 5 delineates the research method followed to conduct the research and data analysis along with results respectively. Section 6 demarcates the discussion and recommendations for policy development. Finally, limitations and anticipated research paths are placed in the last section of the paper.
2. The literature on misinformation, COVID-19 and individual responses
2.1. Misinformation definition
“Misinformation” is defined in several ways [61,64,76]. Misinformation, according to Scheufele and Krause [61], is incorrect information, the probable outcome of an accident. On the other hand, Wardle and Derakhshan [76] noted that false information which is being shared unconsciously (not knowing that the information is whether correct or not) and without any purpose to make harm to anyone is called misinformation; on the other side, disinformation is false information and shared consciously to make harm intentionally [76]. Additionally, the previous authors also defined mal-information; which is authentic private information shared with the public to cause harm by creating hate speech and harassment. Further, in a more specific manner, Chou et al. [13] defined health misinformation as “health-related claims of fact that is currently false due to a lack of scientific evidence”. For this study purposes, however, the authors considered “misinformation” as a “mother-term” of both (mis and dis) –(i) inaccurate information shared unconsciously by believing that the information is true, and –(ii) inaccurate information shared consciously. Hence, in its place, considering the study of Krause et al. [43], we conceived that the misinformation is false information that can be challenged with the best-available evidence pertaining to the COVID-19. Therefore, the current study considered ‘misinformation’ as ‘umbrella term’ of general misinformation belief, conspiracy belief, and religious misinformation belief.
2.2. COVID-19 and individual responses
The Novel Coronavirus 2019 first appeared in Wuhan, China at the end of the year 2019, now spread almost all the corners of the globe and cause to death of 369,274 lives globally so far as on May 31, 2020 [41]. The virus exactly responsible for COVID-19 is known as “severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)”. On March 11, 2020, by observing the rapid escalation and severity of COVID-19, WHO declared COVID-19 as pandemic [79]. The impact of COVID-19 is unprecedented and, indeed, the world is not going back to its regular life very soon.
In today's modern media ecosystem, social media is considered as a noteworthy passage for information [52]. Most of the public shows their responses based on the information received via social media, and misinformation on social media can generate disastrous responses from the individual public. Unfortunately, social media does not always share correct information. Brennen et al. [12] pronounced that misinformation related to the pandemic produces deleterious effects on public health and action. Further, numerous researchers orated that social media is liable for proliferating misinformation about health or COVID-19 [27,59]. This is a matter of great sorrow in this unprecedented global crisis moment, because, albeit some countries reported the use of medicines with no proper confirmation [62], still there is no vaccine for the COVID-19 as of May 31, 2020; and preventive measures are considered as the best weapons to fight against COVID-19.
Individual responses, however, regarding the COVID-19 is influenced by the information they received through different media. As mentioned before, the person who died in the USA after consuming chloroquine could be said that he was largely influenced by the message that chloroquine can cure COVID-19. Like this, a huge amount of misinformation is floating in the air. Consequently, public responses in an unfavorable way and incur detrimental consequences. Further, as individual responses, people may not follow the guidelines provided by recognized national and international health organizations because of their ignorance, especially in the developing and under-developed countries for many reasons. For instance, an Imam of a mosque in Dhaka city (Capital of Bangladesh) was encouraging believers to visit mosques by pronouncing that ‘we enter into a mosque by cleaning ourselves, so there is no possibility that coronavirus will attack us’ [6]. The public might, therefore, be abstained from wearing a face mask, washing hands with a regular interval, maintaining social distance and isolation, and can even join in a crowd like participation in prayer.
3. Conceptual framework and hypotheses development
Based on the extensive literature review and understanding of the publics' behaviors and responses regarding the COVID-19 outbreak, the current study proposed the following conceptual framework to assess the effects of misinformation on individual responses. The conceptual framework has developed combining the stimulus-response theory (hypodermic needle theory) and the resilience theory. Based on the stimulus-response theory, this study has considered general misinformation belief, conspiracy belief, and religious misinformation belief as the stimulus; and credibility evaluations as a resilience strategy (See Fig. 1 ). The following section presents a brief description of both of the theories.
Fig. 1.
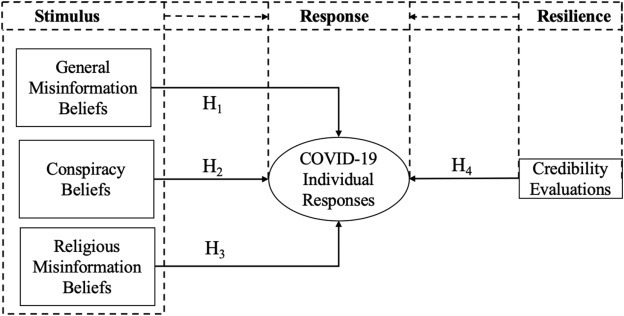
Conceptual Framework.
3.1. Stimulus-response theory and resilience theory
Stimulus-response theory -also known as “hypodermic needle theory,” a dominant theory in communication research [8], is cogitated as one of the first general thoughts explaining media effects [23]. The stimulus-response theory was developed at the very beginning of the twentieth century by combining the then available psychological and sociological theories [17]. The theory, however, expounds that reception of a specific stimulus can be physiologically coupled with the creation of a particular reaction or response [70]. De Fleur [18] empirically explored that the increase of stimulus intensity generates a greater level of response regarding dropping leaflets on a community to convey information. Treisman [70] also documented that any stimulus can be interconnected to any response by any concurrent state of affairs. For this study purpose, therefore, the authors considered ‘misinformation’ as stimuli that can generate favorable or unfavorable responses regarding COVID-19. On the other hand, according to Lowery & DeFleur [46], stimulus-response theory indicates that people lead distinct and isolated lives with limited social control each other because they are from distinct origins and their norms, values, and beliefs are not shared as a unifying set. Further, BBC [7] reported that conspiracies and bad information undermine public health messaging and cause potential harm. Consequently, this study proposed misinformation in three different forms as general misinformation belief, conspiracy belief, and religious misinformation belief because different people have different and distinct beliefs and ways of responding.
The resilience theory is also incorporated in this study with the stimulus-response theory because when people receive (mis)information sometimes they incline to justify or evaluate the (mis)information as resilience. Resilience, however, has been defined from different perspectives and in different ways. The American Psychological Association [2] defines resilience as “the process of adapting well in the face of adversity, trauma, tragedy, threats or significant sources of stress — such as family and relationship problems, serious health problems, or workplace and financial stressors”. From the applied science view, resilience is defined as the “positive or typical developmental adaptations despite exposure to clear threat or adversity” [87]. The functioning definition of resilience is the knack to overcome adversity and be able to be successful even with the presence of high risk [26]. As noted in the introductory part of this study, misinformation pertaining to the COVID-19 and COVID-19 itself has considered as adversity and significant sources of stress and anxiety because it is directly coupled with the serious health problem. Greene et al. [30], however, noted that resilience can appear across the life course with individuals and is concomitant to life stress and people's unique coping ability. Southwick et al. [65] noted that different factors such as biological, psychological, social, and cultural factors interact with each other as the determinants of resilience to distinguish how one reacts to stressful experiences. From the social science perspective, resilience is described as an explanation for diverse outcomes of individuals, families, groups, services, and communities, when exposed to unfavorable incidents [35,47]. Walker et al. [74] documented that resilience can occur in two levels- individual-level resilience and organizational resilience. Polk [55] noted that resilience from the situational point of view as the situational pattern identify those facets encompassing a joining between an individual and a stressful situation. It includes an individual's problem-solving ability, the capability to evaluate situations and responses, and the aptitude to take action in response to a situation Polk [55]. Credibility evaluation of (mis)information, therefore, has considered as resilience strategy from the viewpoints of psychological factors from individual-level and people's unique coping capability to evaluate situations, and a conscious effort to move forward in an insightful way to recover from misinformation stress and respond favorably regarding COVID-19.
3.2. General misinformation beliefs
When misinformation like “Coronavirus is not heat-resistant and will be killed in a temperature of 26-27 degrees” or “the virus does not settle in the air but on the ground, so it is not transmitted through the air” was proliferated, many public from countries with high temperature thought that they are not going to be affected by a coronavirus [80]. As a result, WHO, with evidence, made it clear that COVID-19 can be transmitted in all places, including the places with hot and humid climate [80]. In Bangladesh, when it was spread that “eating Centella asiatica (Asiatic penny-wort in India or “Thankuni” in Bangladesh) will prevent coronavirus infection, the price was raised five times higher than the regular price and surprisingly and ridiculously publics were hunting after it in the kitchen garden. Further, Fakhruddin et al. [24] suggested that unreliable information or misinformation resulting in mistrust in public, which ultimately adversely affects individual decisions associated with health [54,67]. In light of this, the first hypothesis is:
Hypothesis 1
General misinformation beliefs about COVID-19 have a negative impact on COVID-19 individual responses.
3.3. Conspiracy beliefs
Some conspiracies have been spread about COVID-19 just after its appearance to the world. For example, the international level conspiracy is ‘the virus being a biological weapon, created either by the US (to destroy Chinese) or China (to destroy Americans)’. But there are national and local level conspiracies too, which can have direct impacts on the behavior of the general public. Government and government-owned organizations can conceal true information from the public to not to lose their present political position and given chair. For example, the current Health Minister of Bangladesh said that “I don't think that COVID-19 is a dangerous disease” [22]. The reason behind that kind of statement of a high official in Bangladesh is might be to keep the economy alive. It also might be happening that those kinds of statements lead the public to respond poorly against COVID-19. Thus, the study offers the next hypothesis as follows:
Hypothesis 2
Conspiracy beliefs about COVID-19 have a negative impact on COVID-19 individual responses.
3.4. Religious misinformation beliefs
In any disaster, epidemic, or pandemic, religions play a substantial role in influencing people's behaviors. Religious groups in different countries promoting that their faith in religions will save them from COVID-19 [69]. Albeit religions have been providing contentment and a sense of security throughout the history of human civilization, they can simultaneously play both productive and counterproductive roles at the time of pandemics [21]. In Bangladesh, a country with a majority of Muslims (more than 90%), the biggest role is played by the Imam or Mulla or Maulana (Islamic Priest). In the country, as mentioned before, an Imam of a mosque in Dhaka city was advising to visit mosque [6] which might generate unfavorable COVID-19 responses. Marcos Feliciano, a conservative Pentecostal preacher in Brazil, mark a day as anti-COVID “Day of Abstinence”, affirming that fasting would yield a miracle to heal [69]. However, researchers documented that religious fundamentalists are inclined to trust in false information [10]. With this, we proposed the last hypothesis as follows:
Hypothesis 3
Religious Misinformation Beliefs about COVID-19 have a negative impact on COVID-19 individual responses.
3.5. Credibility evaluations
Information shared through social media is questionable in terms of credibility. The public's response to information is influenced by the credibility of the information. Consequently, credibility evaluation is an important determinant of public behaviors. Information credibility is comparatively well comprehended in the case of traditional media, but social media pose challenges in evaluating the source credibility since social media consumers themselves are publishers [75] i.e., they publish user-generated content most of the time. Thus, the source of information is imperative in the credibility evaluation of information [51]. Consequently, we can summarize that when users of social networks engaged themselves in credibility evaluation of information, they respond to a message more responsibly. Therefore, we posited as following:
Hypothesis 4
Users' credibility evaluation of information about COVID-19 has a positive impact on COVID-19 individual responses.
4. Research methods
A structured questionnaire was used to determine the individual responses toward COVID-19 as the effects of misinformation on social media. Since the structural equation modeling (SEM) has been used widely in survey-based research [19] and to test the research hypotheses, the current study also employed SEM.
4.1. Measurements
Belief in misinformation scale about COVID-19 was measured with a three-item scale previously used by Bode & Vraga [9] for the Zika virus, faintly modified based on their ideas for the current study purpose. For credibility evaluations, four statements from Meyer [49] were adopted and one statement “I do double-check the information about COVID-19 received through social media” was self-developed (Cronbach's ∞ = 0.890). Conspiracy belief was measured by using five items from Brotherton et al. [11]. Three items were developed for measuring religious misinformation belief (Cronbach's ∞ = 0.783). Finally, five items for COVID-19 individual responses (Cronbach's ∞ = 0.893) were developed following the guidelines and recommendations specified by WHO [81], and Center for Diseases Control (CDC) [14]. All the items were measured on a 5-point Likert scale ranged from “1 =strongly agree,” through “3 = no opinion,” to “5 = strongly disagree,” but the scale of credibility was coded reversely.
4.2. Participants and data collections
During the lockdown period amid pandemic in almost every corner in the world, including Bangladesh, data collection using online media is best suitable, so did the current research. E-mail and social media networks were used for collecting data from Bangladeshi respondents, and 483 individuals responded to the survey. The demographic summary of the respondents is indicated in Table 1 .
Table 1.
Psychometric properties of the respondents.
| Variables and dimensions | Frequency | Percentage | Variables and dimensions | Frequency | Percentage |
|---|---|---|---|---|---|
| Gender | Religions | ||||
| Female | 204 | 42.20 | Islam | 375 | 77.60 |
| Male | 279 | 57.80 | Hinduism | 79 | 16.40 |
| Age | Buddhism | 18 | 3.70 | ||
| 18–30 | 104 | 21.50 | Christianity | 8 | 1.70 |
| 31–40 | 261 | 54.00 | Non-believers | 3 | 0.60 |
| 41–50 | 95 | 19.70 | Education | ||
| 50–60 | 23 | 4.80 | Highschool | 90 | 18.60 |
| Experience in Using Social Media | Honors | 214 | 44.30 | ||
| Less than 5 years | 112 | 23.20 | Masters | 170 | 35.20 |
| 6–10 years | 291 | 60.20 | PhD | 9 | 1.90 |
| >10 years | 80 | 16.60 | Others | 0 | 0.00 |
5. Data analysis and results
The current study is an attempt to predict the key target construct and test new hypotheses. Accordingly, Partial Least Square (PLS) was selected to evaluate the model because it offers the required features. As a variance-based structural equation modeling (SEM) technique, PLS path modeling is extensively applied in business and social sciences, and its talent to model composites and factors made it a formidable statistical tool [34]. The definition of the PLS path model involved two sets of linear equations: the measurement model and the structural model [34]. The measurement model stipulates the interactions between a construct and its observed indicators, on the other hand, the structural model stipulates the interactions between the constructs [34]. Consequently, PLS has been considered as the “most fully developed and general system” ([48], p. 240). PLS demands fewer requirements compared to that of covariance structure analyses [29]. Hence, considering the advantages offered by PLS, the paper employed SmartPLS 3.0 as PLS-SEM technical software [57].
5.1. Measurement model validation
The core purpose of the measurement model is to evaluate and authenticate that the indicators and scale items employed for every construct are both reliable and valid [60]. Cronbach's alpha (CA) is used to test the reliability of the scale items. Table 2 shows that the lowest Cronbach's alpha is 0.932 which suggests a good level of reliability, whereas the threshold level is 0.70 [32]. Composite reliability is considered to produce the better result of the reliability of the scale than Cronbach's alpha. For better estimates of the reliability of the scale, additionally, composite reliability of the items was tested and found higher than the threshold value 0.7 recommended by Fornell and Larcker [25]. Moreover, it is noted that the indicators' standard loadings of more than 0.7 are considered the measurement model fitness [33]. Table 2 articulates that the loadings ranged from 0.887 to 0.963 are greater than the threshold level. For assessing the indicators, further, the average variance extracted (AVE) was analyzed. The AVE more than 0.5 conveys that at least 50% of the total variance of all items can be explained by the construct [25]. Thus, AVE ranged from 0.825 to 0.891 enunciates that convergent validity requirements were covered.
Table 2.
Measures' convergent validity and reliability.
| Construct | Indicators | Standard loadings | Cronbach's alpha (CA) | Composite reliability | Average Variance Extraction (AVE) |
|---|---|---|---|---|---|
| CB | CB1 | 0.811 | 0.894 | 0.922 | 0.703 |
| CB2 | 0.827 | ||||
| CB3 | 0.858 | ||||
| CB4 | 0.848 | ||||
| CB5 | 0.846 | ||||
| CE | CE1 | 0.822 | 0.890 | 0.919 | 0.694 |
| CE2 | 0.807 | ||||
| CE3 | 0.849 | ||||
| CE4 | 0.843 | ||||
| CE5 | 0.845 | ||||
| C19IR | IR1 | 0.820 | 0.895 | 0.923 | 0.705 |
| IR2 | 0.834 | ||||
| IR3 | 0.843 | ||||
| IR4 | 0.844 | ||||
| IR5 | 0.857 | ||||
| GMB | GMB1 | 0.784 | 0.769 | 0.867 | 0.685 |
| GMB2 | 0.843 | ||||
| GMB3 | 0.853 | ||||
| RMB | RMB1 | 0.754 | 0.783 | 0.875 | 0.700 |
| RMB2 | 0.878 | ||||
| RMB3 | 0.872 |
Note: CB = Conspiracy Beliefs; CE = Credibility Evaluations; C19IR = COVID-19 Individual Responses; GMB = General Misinformation Beliefs about COVID-19; RMB = Religious Misinformation Beliefs about COVID-19.
The discriminant validity of the data was ensured as shown in Table 3 by calculating the square root of the AVE which are larger than the corresponding correlation. Indicator cross-loadings were also checked and found all indicators were loaded to their corresponding constructs. Table 3, shows that the correlations of the independent variables did not outstrip the critical level of 0.90 and the correlations among the variables were less than the threshold level 0.70 [32]. All-inclusive, no unfavorable issues were found to question the measurement model convergent validity and discriminant validity.
Table 3.
Shared variance (SV) and average variance extracted (AVE).
| SV/AVE | C19IR | CB | CE | MB | RMB |
|---|---|---|---|---|---|
| C19IR | 0.840 | ||||
| CB | −0.482 | 0.838 | |||
| CE | 0.578 | −0.281 | 0.833 | ||
| MB | −0.460 | 0.299 | −0.323 | 0.828 | |
| RMB | −0.527 | 0.383 | −0.360 | 0.377 | 0.837 |
5.2. Structural model evaluation
The bootstrapping technique (resampling = 5000, minimum) was implemented to evaluate the statistical significance of the path coefficients [33]. In this step, this study examines the proposed relationship between exogenous and endogenous variables by path coefficient (β) and t-statistics at a significance level of 0.05 (p < .05). As shown in Table 4 , all postulated hypotheses for this study are confirmed. The results show that the relationships between GMB and C19IR (t = 4.13, β = −0.18, p < .001), hypothesis H1; CB and C19IR (t = 5.47, β = −0.23, p < .001), hypothesis H2; RMB and C19IR (t = 5.57, β = −0.24, p < .001), hypothesis H3; and CE and C19IR (t = 8.46, β = 0.37, p < .001), hypothesis H4; were uncovered significant. The testing results of the structural model are also shown in Fig. 2 .
Table 4.
Testing the hypotheses in the structural model.
| Hypothesis | Relationship | Direction | Std Beta | Std error | t-value | P-values | Decision |
|---|---|---|---|---|---|---|---|
| H1 | GMB - > C19IR | Negative | −0.18 | 0.04 | 4.13 | 0.00 | Supported |
| H2 | CB - > C19IR | Negative | −0.23 | 0.04 | 5.47 | 0.00 | Supported |
| H3 | RMB - > C19IR | Negative | −0.24 | 0.04 | 5.57 | 0.00 | Supported |
| H4 | CE - > C19IR | Positive | 0.37 | 0.04 | 8.46 | 0.00 | Supported |
t-value ≥1.96, and p ≤ .05.
Fig. 2.
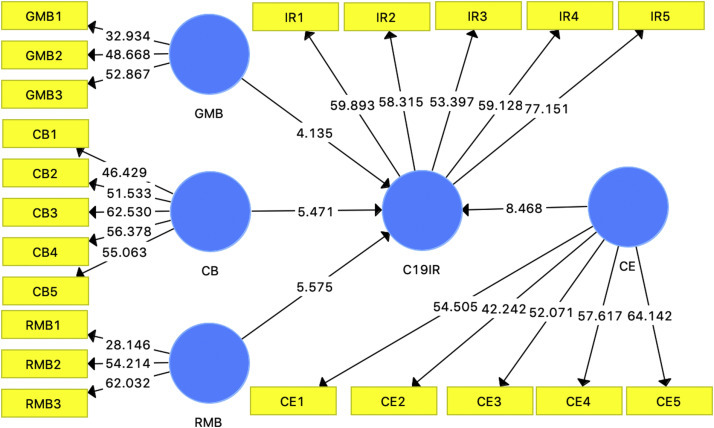
Empirical results.
5.3. R2 and predictive relevance (Q2)
Fig. 2 shows the portion of variance explained in the COVID19 individual responses with R2. Hair et al., (2011) advocated that R2 values of 0.25, 0.50, or 0.75 for dependent constructs in the global structural model can be treated as weak, moderate, or strong, respectively. This study finds a moderate value of R2 (0.534), i.e. the proposed conceptual model envisages an adequate portion of the variance in the COVID19 individual responses.
Further, besides R2, Stone-Geisser's Q2 is also a good measure for depicting the predictive relevance of a model. The predictive relevance (Q2) for COVID19 individual responses is 0.371, which is much larger than zero. Therefore, the resulting value of Q2 indicates that the exogenous variables have good predictive relevance for the endogenous variables in the model.
6. Discussion and recommendations for policy development
The result of the study articulates that misinformation as the stimulus undermines the COVID-19 individual responses. On the other hand, as findings suggest, the credibility evaluation of information as resilience strategy has strong positive influences on the COVID-19 individual responses, hence, first of all, the respective authority should encourage the social media users to evaluate the credibility of information before they take any decision on a matter related to health issue based on the information they received through social media. As the social ecology of resilience, the public has the sources like WHO, UN, CDC, and other national and local organizations to evaluate the (mis)information about COVID-19. Rosenberg et al. [58] noted that misinformation on social media has found to be more popular and is highly prevalent. For its popularity, it's quite difficult to stop the spreading on the social media conduit. Moreover, advancement in technological development made it easier to spread. Though some social media platform authorities have taken measures to try to limit the proliferation of disastrous misinformation regarding COVID-19 by removing fact-checked false and potentially harmful information [58], it is still difficult to stop. Hence, WHO noted that the proliferation of misinformation is viral in such a way that it is practically impossible to stop, and the body is fighting against “infodemic” [77]. Further, Chatterjee et al. [15] noted that since there is no vaccine and confirmed treatment, the possible best approach to counteract and slow down the spread of COVID-19 is knowing the true and accurate information about its causes and how it spreads. Also, Li et al. [44] contended that the dissemination of factual information would contribute to the successful management of the current century's greatest public health disaster. In a situation like that, it would be more appropriate to inspire the public to evaluate the credibility of the information. This would make modest improvements in taking decisions based on information and misinformation. Pennycook et al. [53] also suggested that, in the case of COVID-19, improvements in misinformation sharing can have a meaningful consequence. Situational motivation can increase public involvement in cross-checking the information with respective organizations like WHO, CDC, etc. which eventually might influence the public's responses. However, in response to misinformation on social media conduit, WHO, associating with the Government of the United Kingdom, has been started a campaign to counter misinformation about COVID-19 [82]. The “Stop The Spread” campaign of WHO is trying to raise the awareness of COVID-19 misinformation, as well as the joint campaign is targeted to encourage the public to evaluate the credibility of the information by double-checking it with trusted sources like WHO and other regional and national health agencies. Further, Geldsetzer [28] also suggested that information campaigns by public health authorities and the media as well as communication of health care workers can play a pivotal role in creating awareness about COVID-19.
This is surely praiseworthy initiative by the WHO since our empirical results show that the credibility evaluation certainly helps people to positively respond to COVID-19. This kind of initiative is much more important and emergency in developing countries like Bangladesh where people easily spread disastrous misinformation and take decisions based on that about diagnostic and treatment of pandemic. As we mentioned earlier, some publics in Bangladesh were spread that “eating Centella asiatica will prevent coronavirus infection, then the price was raised five times higher than the regular price and surprisingly and ludicrously publics were hunting after it in the kitchen garden. Many countries in the world are no exception, hence, it is urgent to deploy some kind of motivational campaign to make consciousness among mass people.
Further, international and national respective organizations like WHO, UN, or other can motivate the public to use the health apps amid disaster developed by those organizations. If there are no such kinds of apps, than those national organizations can develop community-based apps especially for managing COVID-19 pandemic or other disasters, and can influence the public to use them and cross-check or evaluate the credibility of the information they receive. Izumi et al. [40] also suggested that community-based disaster risk reduction innovative approaches and tools, as innovation and technology development in disaster risk management, would assist to reduce the risk magnitudes. This study, since there is a huge number of mobile devices and internet user across the world, therefore, strongly suggests the development and deployment of community-based health apps both in local and international languages.
Another important finding of the study, the strong negative impact of religious misinformation belief on COVID-19 individual responses, suggests that the religious faith leaders have a strong influence on their respective religion's believers. They can come forward and play a spirited role in spreading true information. The government should take the initiative for directing the religious faith leaders so that the faith leaders provide true information to the peoples and make awareness among them amid the pandemic like COVID-19 as well as at other times for the safety of the society. However, UNICEF has come forward to play an urgent role in Bangladesh in association with the Islamic Foundation Bangladesh (IFB) – a government organization. UNICEF in Bangladesh noted that the Imams or Moulanas as “expert communicator” agreed to spread the health-related news before or after the ‘namaz’ (praying) time on their megaphone and will help to debunk the misinformation about diagnostic and treatment of the disease ([72]a). The same role can be played by both local and international bodies in different regions around the globe since many countries reported that faith leaders are playing a role in influencing the public [69].
According to the study's empirical result, conspiracy beliefs play a negative role in influencing the publics' responses too. Conspiracies of government and by many organizations are not new to a pandemic. Many conspiracy theories were also spread relating Zika virus, Ebola, or even AIDS. Many reasons might be associated with conspiracy theories. Protecting their chair or to keep moving the economy in a country, whatever the reason is, the government and responsible authority should behave conscientiously. Otherwise, it can create a massacre in the health system of a country as we have been observed in the case for the USA.
Social media also can play a significant role in stopping the spread of misinformation. Although Brennen et al. [12] reported that social media conduit like Facebook, Twitter, and YouTube have started to pull out the information that fact-checked false and goes against community standard as well as COVID-19, the government should warn social media to be more professional and uncompromising regarding undue sharing of disastrous misinformation in a situation like pandemic as well as all the time. In addition to that, social media can work for creating awareness among users regarding the negative impact of sharing information without evidence, specifically when it is related to health issues like a pandemic or any sensitive issues like religion and politics.
Ishiwatari et al. [37] suggested that local organizations and communities can also play a pivotal role in managing disasters like COVID-19 pandemic but they should be supported with fundamental scientific knowledge and information regarding the disaster risk. Consequently, the government of a country and international organizations like WHO, UN, UNICEF individually and jointly can organize some scientific-educational learning facilities for local organizations, spoke persons of the government like health minister or others, and community representatives. With the insignificant worldwide cooperation at the initial stages, the world, however, was unprepared for this pandemic disaster [50]. Realizing the necessity, local, regional, and international organizations have started working together. For instance, WHO arranged several online training programs for both healthcare providers and general people with the intention to -(i) support national readiness and preparedness for COVID-19; (ii) help countries to increase their capacity to respond to COVID-19; (iii) increase international coordination for response and preparedness; (iv) streamline the process of coordinating resources and assessing country preparedness level WHO [83]. As regional cooperation, as government organization of India, Indian Technical and Economic Cooperation Programme (ITEC) also arranged online training on COVID-19 for the health professional of the SAARC (The South Asian Association for Regional Cooperation) countries [39]. Recently, the government of Bangladesh has launched an online learning program about COVID-19 to educate healthcare providers. However, this kind of program should arrange also for community leaders, government spokespersons because they are too involved in the dissemination of the information.
7. Conclusions, limitations and anticipated research paths
This study contributes to the research of both communication and public health by proposing and evaluating a conceptual framework developed incorporating the stimulus-response theory (hypodermic needle theory) and the resilience theory. The study considered general misinformation belief, conspiracy belief, and religious misinformation belief as the stimulus; and credibility evaluations as a resilience strategy; and tested their effects on COVID-19 individual responses. As resilience strategy, credibility evaluation of misinformation has found as a significant predictor of COVID-19 individual responses, accordingly, some suggestion was placed to encourage the public to be resilient. This study, however, is not out of some unavoidable limitations.
In terms of limitations and anticipated research paths, this study can be extended by fulfilling some gaps that were not possible to follow by this study. Future studies are encouraged to include a large number of samples (because the current study considered only 483 sample) from multiple countries since the COVID-19 is a global issue. In addition, there might be cultural differences in belief, for instance, in the case of religious misinformation belief. Hence, the authors suggest testing the proposed and examined model in different contexts and cultures. Further, the study reports a strong relationship between predictor variables and endogenous constructs. In that case, it can be better to include mediating or moderating variables like involvement recognition, situational motivation, in the model in order to produce more generalized deeper insights since by referring Baron and Kenny [3], Barua et al. [4] noted that in the presence of the strong relationship between exogenous and criterion construct, the introduction of mediating variables is better to explore deeper understandings.
Declaration of Competing Interest
None.
Footnotes
Supplementary data to this article can be found online at https://doi.org/10.1016/j.pdisas.2020.100119.
Appendix A. Supplementary data
: The questionnaire is available upon request.
References
- 1.Addo P.C., Jiaming F., Kulbo N.B., Liangqiang L. COVID-19: fear appeal favoring purchase behavior towards personal protective equipment. Serv Ind J. 2020;40(7–8):471–490. doi: 10.1080/02642069.2020.1751823. [DOI] [Google Scholar]
- 2.American Psychological Association . American Psychological Association; Washington, DC: 2012. Building your resilience.https://www.apa.org/topics/resilience Accessed on July 13, 2020: from. [Google Scholar]
- 3.Baron R.M., Kenny D.A. The moderator–mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–1182. doi: 10.1037/0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- 4.Barua Z., Aimin W., Hongyi X. A perceived reliability-based customer satisfaction model in self-service technology. Serv Ind J. 2018;38(7–8):446–466. doi: 10.1080/02642069.2017.1400533. [DOI] [Google Scholar]
- 5.Barua Z., Aimin W., Akter S. International conference on innovation and management held in Malaysia. 2016, November. The influence of antecedents of perceived risk on satisfaction and behavioral intention toward self-service technologies: an empirical study. [Google Scholar]
- 6.BBC-Bangla Corona Virus: What will happen praying in mosque in Bangladesh? 2020. https://www.bbc.com/bengali/news-51960526 Accessed on April 25, 2020.
- 7.BBC Social media firms fail to act on Covid-19 fake news. 2020. https://www.bbc.com/news/technology-52903680 Accessed on July 12, 2020, at.
- 8.Bineham J.L. A historical account of the hypodermic model in mass communication. Commun Monogr. 1988;55(3):230–246. doi: 10.1080/03637758809376169. [DOI] [Google Scholar]
- 9.Bode L., Vraga E.K. See something, say something: correction of global health misinformation on social media. Health Commun. 2018;33(9):1131–1140. doi: 10.1080/10410236.2017.1331312. [DOI] [PubMed] [Google Scholar]
- 10.Bronstein M.V., Pennycook G., Bear A., Rand D.G., Cannon T.D. Belief in fake news is associated with delusionality, dogmatism, religious fundamentalism, and reduced analytic thinking. J Appl Res Memory Cogn. 2019;8(1):108–117. doi: 10.1016/j.jarmac.2018.09.005. 2018. [DOI] [Google Scholar]
- 11.Brotherton R., French C.C., Pickering A. Measuring belief in conspiracy theories: the generic conspiracist beliefs scale. Front Psychol. 2013;4:1–15. doi: 10.3389/fpsyg.2013.00279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Brennen J.S., Simon F., Howard P.N., Nielsen R.K. Types, sources, and claims of COVID-19 misinformation. Reuters Inst. 2020;7 [Google Scholar]
- 13.Chou W.Y.S., Oh A., Klein W.M. Addressing health-related misinformation on social media. Jama. 2018;320(23):2417–2418. doi: 10.1001/jama.2018.16865. [DOI] [PubMed] [Google Scholar]
- 14.CDC Coronavirus disease 2019 (COVID-19): protect yourself. 2020. https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/prevention.html Accessed: April 10, 2020 at.
- 15.Chatterjee R., Bajwa S., Dwivedi D., Kanji R., Ahammed M., Shaw R. COVID-19 risk assessment tool: dual application of risk communication and risk governance. Prog Disaster Sci. 2020;100109 doi: 10.1016/j.pdisas.2020.100109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Cuan-Baltazar J.Y., Muñoz-Perez M.J., Robledo-Vega C., Pérez-Zepeda M.F., Soto-Vega E. Misinformation of COVID-19 on the internet: infodemiology study. JMIR Public Health Surveill. 2020;6(2) doi: 10.2196/18444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.DeFleur M.L., Ball-Rokeach S.J. 4th ed. Longman; New York: 1982. Theories of mass communication. [Google Scholar]
- 18.De Fleur M.L. A mass communication model of stimulus response relationships: an experiment in leaflet message diffusion. Sociometry. 1956;19(1):12–25. doi: 10.2307/2786100. [DOI] [Google Scholar]
- 19.Dijkstra T.K., Henseler J. Consistent and asymptotically normal PLS estimators for linear structural equations. Comput Stat Data Anal. 2015;81:10. doi: 10.1016/j.csda.2014.07.008. [DOI] [Google Scholar]
- 20.Djalante R., Shaw R., DeWit A. Building resilience against biological hazards and pandemics: COVID-19 and its implications for the Sendai framework. Prog Disaster Sci. 2020:100080. doi: 10.1016/j.pdisas.2020.100080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Djalante R., Lassa J., Setiamarga D., Mahfud C., Sudjatma A., Indrawan M. 2020. Review and analysis of current responses to COVID-19 in Indonesia: Period of January to March 2020. Progress in disaster science; p. 100091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ei Somoy 365 Online News portal. 2020. https://eisomoy365.com/3193/?fbclid=IwAR2gJ17vLP9Ii3p_o-WI2cT6MLyf471-ELSFdFZWYcLreOi6cyP1JDWZ-zo Accessed May 15 at.
- 23.Esser F. Stimulus–response model. Int Encycl Commun. 2008 doi: 10.1002/9781405186407.wbiecs103. [DOI] [Google Scholar]
- 24.Fakhruddin B., Blanchard K., Ragupathy D. Are we there yet? The transition from response to recovery for the COVID-19 pandemic. Prog Disaster Sci. 2020;100102 doi: 10.1016/j.pdisas.2020.100102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Fornell C.G., Larcker D.F. Evaluating structural equation models with unobservable variables and measurement error. J Mark Res. 1981;18(1):39–50. doi: 10.1177/002224378101800104. [DOI] [Google Scholar]
- 26.Fraser M.W., Galinsky M.J., Richman J.M. Risk, protection, and resilience: toward a conceptual framework for social work practice. Soc Work Res. 1999;23(3):131–143. doi: 10.1093/swr/23.3.131. [DOI] [Google Scholar]
- 27.Frenkel S., Alba D., Zhong R. The New York Times; 2020. Surge of virus misinformation stumps facebook and twitter.https://www.nytimes.com/2020/03/08/technology/coronavirus-misinformation-socialmedia.html March 8. Available from: [Google Scholar]
- 28.Geldsetzer P. Use of rapid online surveys to assess People's perceptions during infectious disease outbreaks: a cross-sectional survey on COVID-19. J Med Internet Res. 2020;22(4) doi: 10.2196/18790. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Götz O., Liehr-Gobbers K., Krafft M. Springer; Berlin, Heidelberg: 2010. Evaluation of structural equation models using the partial least squares (PLS) approach. Handbook of partial least squares (pp. 691–711) [DOI] [Google Scholar]
- 30.Greene R.R., Galambos C., Lee Y. Resilience theory: theoretical and professional conceptualizations. J Hum Behav Soc Environ. 2004;8(4):75–91. doi: 10.1300/J137v08n04_05. [DOI] [Google Scholar]
- 31.Guynn J. Welcome to the first social media pandemic. Here are 8 ways you can stop the spread of coronavirus misinformation. USA Today; March 19, 2020. https://www.usatoday.com/story/tech/2020/03/19/coronavirus-covid-19-misinformation-social-mediafacebook-youtube-instagram/2870277001/ Available at.
- 32.Hair J.F., Anderson R.E., Babin B.J., Black W.C. Pearson; Upper Saddle River, NJ: 2010. Multivariate data analysis: A global perspective. [Google Scholar]
- 33.Hair J.F., Ringle C.M., Sarstedt M. PLS-SEM: indeed a silver bullet. J Mark Theory Pract. 2011;19(2):139–152. doi: 10.2753/MTP1069-6679190202. [DOI] [Google Scholar]
- 34.Henseler J., Hubona G., Ray P.A. Using PLS path modeling in new technology research: updated guidelines. Ind Manag Data Syst. 2016 doi: 10.1108/IMDS-09-2015-0382. [DOI] [Google Scholar]
- 35.Herrman H., Stewart D.E., Diaz-Granados N., Berger E.L., Jackson B., Yuen T. What is resilience? Can J Psychiatr. 2011;56(5):258–265. doi: 10.1177/070674371105600504. (Doi:10.1177%2F070674371105600504) [DOI] [PubMed] [Google Scholar]
- 36.Hopman J., Allegranzi B., Mehtar S. Managing COVID-19 in low-and middle-income countries. Jama. 2020;323(16):1549–1550. doi: 10.1001/jama.2020.4169. [DOI] [PubMed] [Google Scholar]
- 37.Ishiwatari M., Koike T., Hiroki K., Toda T., Katsube T. Managing disasters amid COVID-19 pandemic: approaches of response to flood disasters. Prog Disaster Sci. 2020;100096 doi: 10.1016/j.pdisas.2020.100096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Ippolito G., Hui D.S., Ntoumi F., Maeurer M., Zumla A. Toning down the 2019-nCoV media hype—and restoring hope. Lancet Respir Med. 2020;8(3):230–231. doi: 10.1016/S2213-2600(20)30070-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.ITEC Covid-19 pandemic: prevention and management guidelines for health care professional. 2020. https://www.itecgoi.in/applicant_getCountry_e-ITEC.php?salt3=c564542d7f2020-2021&salt=e36ddecf9e3440&salt2=ccd6f778f026 Access on July 10, 2020 at.
- 40.Izumi T., Shaw R., Djalante R., Ishiwatari M., Komino T. Disaster risk reduction and innovations. Prog Disaster Sci. 2019;2:100033. doi: 10.1016/j.pdisas.2019.100033. [DOI] [Google Scholar]
- 41.JHU Coronavirus resource center. 2020. https://coronavirus.jhu.edu Accessed on May 31, 2020 at.
- 42.Kouzy R., Abi Jaoude J., Kraitem A., El Alam M.B., Karam B., Adib E. Coronavirus goes viral: quantifying the COVID-19 misinformation epidemic on twitter. Cureus. 2020;12(3) doi: 10.7759/cureus.7255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Krause N.M., Freiling I., Beets B., Brossard D. Fact-checking as risk communication: the multi- layered risk of misinformation in times of COVID-19. J Risk Res. 2020:1–8. doi: 10.1080/13669877.2020.1756385. [DOI] [Google Scholar]
- 44.Li H.O.Y., Bailey A., Huynh D., Chan J. YouTube as a source of information on COVID-19: a pandemic of misinformation? BMJ Glob Health. 2020;5(5) doi: 10.1136/bmjgh-2020-002604. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Logie C.H., Turan J.M. How do we balance tensions between COVID-19 public health responses and stigma mitigation? Learning from HIV research. AIDS Behav. 2020:1–4. doi: 10.1007/s10461-020-02856-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Lowery S.A., DeFleur M.L. 3rd ed. Longman; White Plains, NY: 1995. Milestones of mass communication research: Media effects. [Google Scholar]
- 47.Masten A.S. Ordinary magic: resilience processes in development. Am Psychol. 2001;56(3):227. doi: 10.1037//0003-066x.56.3.227. [DOI] [PubMed] [Google Scholar]
- 48.McDonald R.P. Path analysis with composite variables. Multivar Behav Res. 1996;31(2):239–270. doi: 10.1207/s15327906mbr3102_5. [DOI] [PubMed] [Google Scholar]
- 49.Meyer P. Defining and measuring credibility of newspapers: developing an index. Journal Q. 1988;65(3):567–574. doi: 10.1177/107769908806500301. [DOI] [Google Scholar]
- 50.Mukherjee M., Chatterjee R., Khanna B.K., Dhillon P.P.S., Kumar A., Bajwa S. Ecosystem-centric business continuity planning (eco-centric BCP): a post COVID19 new normal. Prog Disaster Sci. 2020;100117 doi: 10.1016/j.pdisas.2020.100117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Nyhan B., Reifler J. Media Policy Initiative Research Paper, New America Foundation; 2012. Misinformation and fact-checking: Research findings from social science. [Google Scholar]
- 52.Ortiz-Ospina E. The rise of social media. 2020. https://ourworldindata.org/rise-of-social-media Available from:
- 53.Pennycook G., McPhetres J., Zhang Y., Rand D. 2020. Fighting COVID-19 misinformation on social media: Experimental evidence for a scalable accuracy nudge intervention. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Poland G.A., Spier R. Fear, misinformation, and innumerates: how the Wakefield paper, the press, and advocacy groups damaged the public health. Vaccine. 2010;28(12):2361–2362. doi: 10.1016/j.vaccine.2010.02.052. [DOI] [PubMed] [Google Scholar]
- 55.Polk L.V. Toward a middle-range theory of resilience. Adv Nurs Sci. 1997;19(3):1–13. doi: 10.1097/00012272-199703000-00002. [DOI] [PubMed] [Google Scholar]
- 56.Rajkumar R.P. COVID-19 and mental health: a review of the existing literature. Asian J Psychiatr. 2020;102066 doi: 10.1016/j.ajp.2020.102066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Ringle C.M., Wende S., Becker J.-M. SmartPLS GmbH; Boenningstedt: 2015. SmartPLS 3.http://www.smartpls.com [Google Scholar]
- 58.Rosenberg H., Syed S., Rezaie S. The twitter pandemic: the critical role of twitter in the dissemination of medical information and misinformation during the COVID-19 pandemic. Can J Emerg Med. 2020:1–7. doi: 10.1017/cem.2020.361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Russonello G. The New York Times; 2020, March 13. Afraid of coronavirus? That might say something about your politics.https://www.nytimes.com/2020/03/13/us/politics/coronavirus-trump-polling.html Available from: [Google Scholar]
- 60.Sagib G.K., Zapan B. Bangladeshi mobile banking service quality and customer satisfaction and loyalty. Manag Market. 2014;9(3) [Google Scholar]
- 61.Scheufele D.A., Krause N.M. Science audiences, misinformation, and fake news. Proc Natl Acad Sci. 2019;116(16):7662–7669. doi: 10.1073/pnas.1805871115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Shaw R., Kim Y.K., Hua J. Governance, technology and citizen behavior in pandemic: lessons from COVID-19 in East Asia. Prog Disaster Sci. 2020;100090 doi: 10.1016/j.pdisas.2020.100090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Smith G.D., Ng F., Li W.H.C. COVID-19: emerging compassion, courage and resilience in the face of misinformation and adversity. J Clin Nurs. 2020;29(9–10):1425. doi: 10.1111/jocn.15231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Southwell B.G., Thorson E., Sheble L., editors. Misinformation and mass audiences. University of Texas Press; Austin, TX: 2018. [Google Scholar]
- 65.Southwick S.M., Bonanno G.A., Masten A.S., Panter-Brick C., Yehuda R. Resilience definitions, theory, and challenges: interdisciplinary perspectives. Eur J Psychotraumatol. 2014;5(1):25338. doi: 10.3402/ejpt.v5.25338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Statista Mobile internet usage worldwide - statistics & facts. 2019. https://www.statista.com/topics/779/mobile-internet/ Accessed July 12, 2020, from.
- 67.Tafuri S., Gallone M.S., Cappelli M.G., Martinelli D., Prato R., Germinario C. Addressing the anti-vaccination movement and the role of HCWs. Vaccine. 2013;32(38):4860–4865. doi: 10.1016/j.vaccine.2013.11.006. [DOI] [PubMed] [Google Scholar]
- 68.Tan A.S., Lee C.J., Chae J. Exposure to health (mis) information: lagged effects on young adults' health behaviors and potential pathways. J Commun. 2015;65(4):674–698. doi: 10.1111/jcom.12163. [DOI] [Google Scholar]
- 69.The Guardian As coronavirus spreads around the world, so too do the quack cures. 2020. https://www.theguardian.com/world/2020/apr/16/as-coronavirus-spreads-around-the-world-so-too-do-the-quack-cures Accessed May 24, 2020.
- 70.Treisman M. Stimulus-response theory and expectancy. Br J Psychol. 1960;51(1):49–60. doi: 10.1111/j.2044-8295.1960.tb00724.x. [DOI] [PubMed] [Google Scholar]
- 71.UN . 2020. Misinformation and cybercrime in COVID-19 crisis. (Accessed on April 20, 2020 at: https://www.un.org/en/un-coronavirus-communications-team/un-tackling-‘infodemic’-misinformation-and-cybercrime-covid-19) [Google Scholar]
- 72.UNICEF Religious leaders play key role in battle against COVID-19. 2020. https://www.unicef.org/bangladesh/en/stories/religious-leaders-play-key-role-battle-against-covid-19 Accessed May 21, 2020.
- 73.Vallejo B.M., Jr., Ong R.A.C. 2020. Policy responses and government science advice for the COVID 19 pandemic in the Philippines: January to April 2020. Progress in disaster science; p. 100115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Walker B., Nilakant V., Baird R. Promoting organisational resilience through sustaining engagement in a disruptive environment: What are the implications for HRM? 2014. http://hdl.handle.net/10092/10571
- 75.Wang Y., McKee M., Torbica A., Stuckler D. Systematic literature review on the spread of health-related misinformation on social media. Soc Sci Med. 2019 doi: 10.1016/j.socscimed.2019.112552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Wardle C., Derakhshan H. Vol. 27. 2017. Information disorder: toward an interdisciplinary framework for research and policy making. Council of Europe report.https://firstdraftnews.org/latest/coe-report/ (Accessed May 20, 2020;) [Google Scholar]
- 77.WHO Novel Coronavirus(2019-nCoV) situation report – 13. 2020. https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200202-sitrep-13-ncov-v3.pdf Accessed on April 18, 2020 at.
- 78.WHO World health organization: coronavirus. 2020. https://www.who.int/docs/default-source/coronaviruse/transcripts/who-audio-emergencies-coronavirus-full-press-conference-13feb2020-final.pdf?sfvrsn=b5435aa2_2 Accessed on April 18, 2020 at.
- 79.WHO WHO timeline - COVID-19. 2020. https://www.who.int/news-room/detail/27-04-2020-who-timeline---covid-19 Accessed on April 20, 2020 at.
- 80.WHO Rumours and facts on COVID-19. 2020. https://www.who.int/docs/default-source/nepal-documents/novel-coronavirus/un-rumour-tracking-english-issue-2.pdf?sfvrsn=bd68b830_2 Accessed on April 22, 2020 at.
- 81.WHO Protecting yourself and others from the spread COVID-19. 2020. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public Accessed: April 10, 2020 at.
- 82.WHO Countering misinformation about COVID-19: A joint campaign with the Government of the United Kingdom. 2020. https://www.who.int/news-room/feature-stories/detail/countering-misinformation-about-covid-19 Accessed May 29, 2020.
- 83.WHO Coronavirus disease (COVID-19) training: Online training. 2020. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/training/online-training Accessed July 10, 2020.
- 84.Waldrop T., Alsup D., McLaughlin E. Fearing coronavirus, Arizona man dies after taking a form of chloroquine used to treat aquariums. 2020. CNN.comhttps://www.cnn.com/2020/03/23/health/arizona-coronavirus-chloroquine-death/index.html March 25, 2020. Accessed 12 July 2020: at.
- 85.Wang C., Pan R., Wan X., Tan Y., Xu L., Ho C.S. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. 2020;17(5):1729. doi: 10.3390/ijerph17051729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Xiao Y., Torok M.E. Taking the right measures to control COVID-19. Lancet Infect Dis. 2020;20(5):523–524. doi: 10.1016/S1473-3099(20)30152-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Yates T.M., Tyrell F.A., Masten A.S. 2015. Resilience theory and the practice of positive psychology from individuals to societies. Positive psychology in practice: Promoting human flourishing in work, health, education, and everyday life; pp. 773–788. [Google Scholar]
- 88.Zandifar A., Badrfam R. Iranian mental health during the COVID-19 epidemic. Asian J Psychiatr. 2020;51 doi: 10.1016/j.ajp.2020.101990. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
: The questionnaire is available upon request.