

Key Points
Question
What is the association of a triple pill containing low doses of 3 antihypertensive medications with therapeutic inertia compared with usual care?
Findings
In this secondary analysis of a randomized clinical trial including 700 patients with mild to moderate hypertension, rates of therapeutic inertia were significantly different between those in the triple pill group and those in the usual care group at the week 6 visit (92 of 106 [86.8%] vs 124 of 194 [63.9%]) and the week 12 visit (81 of 90 [90%] vs 116 of 179 [64.8%]). Compared with those in the usual care group, significantly more patients in the triple pill group achieved blood pressure targets (221 of 318 [69.5%] vs 182 of 329 [55.3%]) with significantly fewer unique antihypertensive treatment regimens (23 vs 54 per 100 treated patients).
Meaning
Use of a low-dose triple combination antihypertensive medication improves blood pressure control and simplifies treatment regimen but is associated with increased therapeutic inertia.
This secondary analysis of a randomized clinical trial investigates the association of antihypertensive triple drug fixed-dose combination therapy with therapeutic inertia and prescribing patterns compared with usual care.
Abstract
Importance
Fixed-dose combination (FDC) therapies are being increasingly recommended for initial or early management of patients with hypertension, as they reduce treatment complexity and potentially reduce therapeutic inertia.
Objective
To investigate the association of antihypertensive triple drug FDC therapy with therapeutic inertia and prescribing patterns compared with usual care.
Design, Setting, and Participants
A post hoc analysis of the Triple Pill vs Usual Care Management for Patients With Mild-to-Moderate Hypertension (TRIUMPH) study, a randomized clinical trial of 700 patients with hypertension, was conducted. Patients were enrolled from 11 urban hospital clinics in Sri Lanka from February 2016 to May 2017; follow-up ended in October 2017. Data were analyzed from September to November 2019.
Interventions
Once-daily FDC antihypertensive pill (telmisartan, 20 mg; amlodipine, 2.5 mg; and chlorthalidone, 12.5 mg) or usual care.
Main Outcomes and Measures
Therapeutic inertia, defined as not intensifying therapy in those with blood pressure (BP) above target, was assessed at baseline and during follow-up visits. Prescribing patterns were characterized by BP-lowering drug class and treatment regimen potency. Predictors of therapeutic inertia were assessed with binomial logistic regression.
Results
Of the 700 included patients, 403 (57.6%) were female, and the mean (SD) age was 56 (11) years. Among patients who did not reach the BP target, therapeutic inertia was more common in the triple pill group compared with the usual care group at the week 6 visit (92 of 106 [86.8%] vs 124 of 194 [63.9%]; P < .001) and week 12 visit (81 of 90 [90%] vs 116 of 179 [64.8%]; P < .001). At the end of the study, 221 of 318 patients in the triple pill group (69.5%) and 182 of 329 patients in the usual care group (55.3%) reached BP targets. Among those who received treatment intensification, the increase in estimated regimen potency was greater in the triple pill group compared with the usual care group at baseline (predicted mean [SD] increase in regimen potency: triple pill, 15 [6] mm Hg; usual care, 10 [5] mm Hg; P < .001), whereas there were no significant differences at the week 6 or at week 12 visit. Clinic systolic BP level was the only consistent predictor of treatment intensification during follow-up. During follow-up, there were 23 vs 54 unique treatment regimens per 100 treated patients in the triple pill vs usual care groups, respectively (P < .001).
Conclusions and Relevance
Triple pill FDC therapy was associated with greater rates of therapeutic inertia compared with usual care. Despite this, triple pill FDC therapy substantially simplified prescribing patterns and improved 6-month BP control rates compared with usual care. Further improvements in hypertension control could be achieved by addressing therapeutic inertia among the minority of patients who do not achieve BP control after initial FDC therapy.
Trial Registration
ANZCTR Identifier: ACTRN12612001120864
Introduction
Hypertension is the leading cause of cardiovascular disease and mortality globally and remains a major public health issue.1 The prevalence of hypertension and deaths attributable to hypertension have increased between 1990 and 2015.2 Achieving the guideline-recommended blood pressure (BP) targets usually requires multiple antihypertensive agents,3 which can lead to complex treatment regimens that can be difficult for physicians to optimize and can require frequent monitoring and dose titration, with current guidelines recommending monthly visits until BP is controlled.4,5 Inaccessibility to health care (particularly in areas of low socioeconomic status), poor medication adherence, and failure to intensify treatment despite poor BP control, termed therapeutic inertia, are major barriers to BP control.6,7
A treatment strategy consisting of fixed-dose combination (FDC) pills aims to address these potential barriers by providing easy access to multiple therapies in a single pill,8 increasing medication adherence9,10,11 and potentially reducing therapeutic inertia. There are few randomized trial data on the association of FDCs with therapeutic inertia,12,13,14 and previous studies have either been observational studies or trials that involved mandatory treatment algorithms in the control group. A better understanding of the association of FDCs with therapeutic inertia and prescribing patterns will help to formulate the most effective implementation strategies to adopt when using combination therapies. Therefore, the objective of this post hoc analysis was to investigate the association of antihypertensive triple drug FDC therapy with therapeutic inertia and prescribing patterns in the Triple Pill vs Usual Care Management for Patients With Mild-to-Moderate Hypertension (TRIUMPH) trial compared with usual care.15
Methods
Study Design
The details of the TRIUMPH trial have been reported elsewhere.15,16 In brief, 700 patients with persistent mild to moderate hypertension (systolic BP [SBP] greater than 140 mm Hg and/or diastolic BP [DBP] greater than 90 mm Hg; or SBP greater than 130 mm Hg and/or DBP greater than 80 mm Hg in patients with diabetes or chronic kidney disease) were randomized to a once-daily FDC pill of 3 BP-lowering drugs at half of standard doses (telmisartan, 20 mg; amlodipine, 2.5 mg; and chlorthalidone, 12.5 mg) (n = 349) or usual care (n = 351). Blood pressure was recorded at randomization, week 6, week 12, and 6 months (end of study). In patients randomized to the triple pill group, a higher-dose version of the triple pill (containing standard doses of the BP-lowering drugs: telmisartan, 40 mg; amlodipine, 5 mg; and chlorthalidone, 25 mg) was available for up-titration at the discretion of the treating physician. Other BP-lowering drugs could also be prescribed in combination with either dose of the triple pill regimen. For participants in the usual care group, investigators were asked to follow their local guidelines to achieve BP targets without any restrictions. Blood pressure targets were defined as SBP less than 140 mm Hg and DBP less than 90 mm Hg or as SBP less than 130 mm Hg and DBP less than 80 mm Hg in patients with diabetes or chronic kidney disease. All BP medications, including the FDC triple pill, were available to patients free of cost.
Therapeutic inertia was defined as failure to intensify treatment despite not reaching the BP target. Treatment intensification included prescription of any new BP-lowering drug, switching from one drug to another, or increasing the dosage of existing BP-lowering drug(s). Treatment intensification occurring within 2 days before the visit date and up to 2 days prior to the following visit date was used for the present analysis. We estimated regimen potency by calculating the predicted SBP reduction for each patient’s treatment regimen according to the model reported by Law et al.17 We assumed a baseline SBP of 154 mm Hg to calculate the predicted SBP reductions, which is the mean pretreatment BP used by Law et al17 in the development of the model and also the mean baseline BP of the patients enrolled in the TRIUMPH trial.15 We also reported the number of unique clinical pathways in the triple pill group compared with the usual care group, according to achievement of target BP (yes/no) at each follow-up visit and subsequent treatment intensification (intensified/not intensified) at randomization, week 6, and week 12.
Statistical Analysis
Descriptive statistics are presented as counts and percentages for categorical variables, while means and standard deviations are reported for continuous variables. Characteristics of patients were compared using Pearson χ2 test or Fisher exact test for categorical variables and independent-samples t test or Mann-Whitney test for continuous variables. Variables with a P value less than .20 on univariate analysis were entered into binomial logistic regression models to identify the predictors of treatment intensification. Separate models were developed for the triple pill and usual care groups both separately and combined and at the 3 time points (randomization and week 6 and 12 visits). Covariates were either added or removed in a stepwise manner for each model (P less than .05 to enter, P greater than .10 to remove). Odds ratios and 95% CIs were obtained from the final logistic regression models. Finally, a further model was developed (using the same process as outlined above but in which the triple pill and usual care groups were combined) to identify the baseline predictors of achieving BP targets at 6 months. Sunburst plots were generated to illustrate the medication prescribing patterns of patients at randomization, week 6, week 12, and 6 months.
All statistical significance tests were conducted using a 2-sided type I error rate of 5%. All analyses were performed in SPSS version 23.0 (IBM Corporation), and sunburst plots were generated using the package sunburstR in R version 4.0.1 (The R Foundation).
Results
Patient Population
Characteristics of participants in the TRIUMPH trial have been described in detail previously.15 In summary, there were 700 participants included, and all patients were included in the present analysis. The mean (SD) age of the population was 56 (11) years, 403 (57.6%) were women, and 220 (31.4%) had diabetes. The mean (SD) baseline SBP was 154 (11) mm Hg and the mean (SD) DBP was 90 (10) mm Hg in both groups, and 287 participants (41.0%) were taking BP-lowering treatment at baseline prior to randomization.
Association of Triple Pill Therapy With Therapeutic Inertia
Table 1 shows the proportion of patients achieving BP targets and receiving treatment intensification by follow-up visit and treatment group. At baseline, more patients randomized to triple pill therapy compared with usual care received treatment intensification (342 of 348 [98.3%] vs 255 of 351 [72.6%]; P < .001), reflecting the requirements of the trial protocol. Among patients who received treatment intensification at randomization, more patients in the triple pill group compared with the usual care group reached the BP target at the end of the study (218 of 314 [69.4%] vs 135 of 237 [57.0%]; P = .003). During the week 6 and week 12 visits, there were a greater number of patients who achieved BP targets in the triple pill group compared with the usual care group (week 6: triple pill, 223 of 329 [67.8%]; usual care, 150 of 344 [43.6%]; P < .001; week 12: triple pill, 239 of 329 [72.6%]; usual care, 161 of 340 [47.4%]; P < .001). However, among patients who did not reach BP targets, there were more episodes of therapeutic inertia in the triple pill group compared with the usual care group at the week 6 visit (92 of 106 [86.8%] vs 124 of 194 [63.9%]; P < .001) and week 12 visit (81 of 90 [90%] vs 116 of 179 [64.8%]; P < .001).
Table 1. Patients Receiving Treatment Intensification in the Triple Pill and Usual Care Groups.
| Treatment characteristic | No./total No. (%) | P value | |
|---|---|---|---|
| Triple pill | Usual care | ||
| Randomization visit | |||
| Not at BP target at visit | 348/349 (100)a | 351/351 (100) | >.99 |
| Treatment inertiab | 6/348 (1.7) | 96/351 (27.4) | <.001 |
| Week 6 visit | |||
| Not at BP target at visit | 106/329 (32.2) | 194/344 (56.4) | <.001 |
| Treatment inertiab | 92/106 (86.8) | 124/194 (63.9) | <.001 |
| Week 12 visit | |||
| Not reaching BP target | 90/329 (27.4) | 179/340 (52.6) | <.001 |
| Treatment inertiab | 81/90 (90) | 116/179 (64.8) | <.001 |
| Month 6 visit | |||
| Not reaching BP target | 97/318 (30.5) | 147/329 (44.7) | <.001 |
Abbreviation: BP, blood pressure.
One patient who reached target was still included in the study.
Denominator is the number of patients not reaching the BP target at the visit and excludes dropouts.
Association of Triple Pill Therapy With Treatment Regimen Potency
At baseline, the estimated mean potency of the treatment regimens was similar between the 2 treatment groups (Table 2). Among patients who received treatment intensification at randomization, regimen potency was greater in the triple pill group (mean [SD] predicted SBP reduction: 14.9 [6.3] mm Hg) compared with patients in the usual care group (mean [SD] predicted SBP reduction: 9.6 [5.1] mm Hg), with a mean difference of 5.3 mm Hg (95% CI, 4.4-6.2; P < .001). At subsequent follow-up visits, the mean increase in potency among those in whom treatment was intensified was less than at baseline and was similar between the 2 treatment groups. These predicted differences were smaller than the observed BP differences between the 2 treatment groups in the trial (mean difference: week 6, 10.5 mm Hg; week 12, 11.6 mm Hg; 6 months, 8.9 mm Hg).
Table 2. Estimated Potency of Prescribed Blood Pressure–Lowering Drug Regimens by Group and Follow-up Visita.
| Estimated potency | Triple pill | Usual care | Mean difference (95% CI), mm Hg | P value | ||
|---|---|---|---|---|---|---|
| No. | Predicted SBP reduction, mean (SD), mm Hg | No. | Predicted SBP reduction, mean (SD), mm Hg | |||
| Randomization visit | ||||||
| Estimated mean regimen potency | 349 | 4.0 (5.2) | 351 | 4.3 (5.4) | −0.3 (−1.1 to 0.5) | .44 |
| Mean change in potency among those who received treatment intensificationb | 335 | 14.9 (6.3) | 252 | 9.6 (5.1) | 5.3 (4.4 to 6.2) | <.001 |
| Week 6 visit | ||||||
| Estimated mean regimen potency | 339 | 18.6 (3.8) | 347 | 11.2 (4.7) | 7.5 (6.8 to 8.1) | <.001 |
| Mean change in potency among those who received treatment intensificationb | 14 | 5.5 (5.8) | 70 | 5.2 (4.5) | 0.2 (−2.5 to 3.0) | .86 |
| Week 12 visit | ||||||
| Estimated mean regimen potency | 337 | 18.7 (4.2) | 345 | 12.4 (5.3) | 6.3 (5.6 to 7.1) | <.001 |
| Mean change in potency among those who received treatment intensificationb | 8 | 2.1 (4.6) | 63 | 4.1 (5.5) | −2.0 (−5.9 to 1.8) | .30 |
| Month 6 visit | ||||||
| Estimated mean regimen potency | 334 | 18.5 (4.8) | 341 | 13.1 (5.7) | 5.3 (4.5 to 6.1) | <.001 |
Abbreviation: SBP, systolic blood pressure.
Estimated treatment regimen potencies were calculated using methods from Law et al17 among patients who did not reach the blood pressure target and received intensification of blood pressure–lowering drug therapy. Data are provided on estimated regimen potency for patients who attended the visit and for those who received treatment intensification at the visit. Untreated patients were given an estimated potency of 0 mm Hg.
Change in regimen potency defined as the difference in predicted SBP reduction from the next visit and the current visit.
Association of Triple Pill Therapy With Drug Regimens
During follow-up, there was a large reduction in the number of unique BP-lowering drug regimens in the triple pill group compared with the usual care group (Figure 1). In the triple pill group, the most commonly prescribed treatment regimen at 6 months was triple pill with no additional therapy, used by 282 of 334 patients (84.4%), with an additional 15 other unique drug regimens prescribed to others. In contrast, in the usual care group, the most commonly prescribed treatment regimen at 6 months was monotherapy with an angiotensin receptor blocker, used by 157 of 341 patients in the usual care group (46.0%). There were an additional 19 unique drug regimens prescribed to the remaining patients in the usual care group. Across 6 months of follow-up, the number of unique drug and dose regimens per 100 persons treated was 23 in the triple pill group and 54 in the usual care group (P < .001). Only 10 of 349 patients in the triple pill group (2.9%) received the full-dose triple pill during the 6-month follow-up.
Figure 1. Number of Unique Antihypertensive Regimens by Treatment Group and Follow-up Visit.
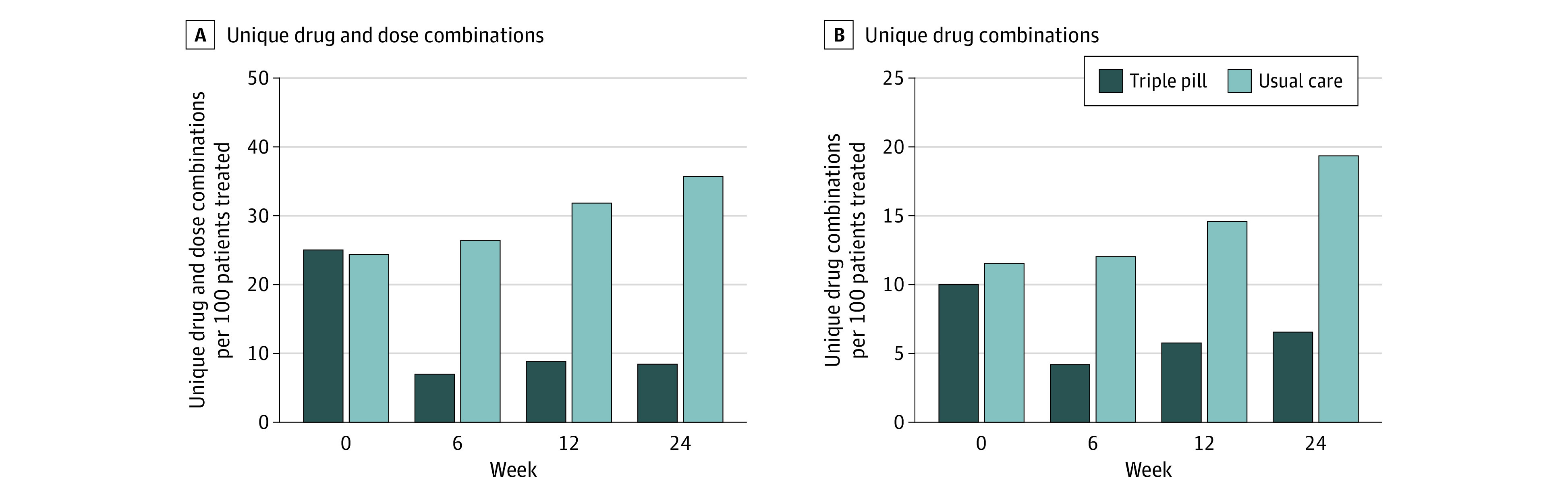
During the 6-month study period, there were 23 unique drug and dose regimens (12 unique drug regimens) per 100 persons treated in the triple gill group and 54 unique drug and dose regimens (25 unique drug regimens) per 100 persons treated in the usual care group. The number of patients treated with any blood pressure–lowering drug was similar between groups (randomization: triple pill, 140 of 349 [40.1%]; usual care, 147 of 351 [41.9%]; week 6: triple pill, 331 of 339 [97.6%]; usual care, 341 of 347 [98.3%]; week 12: triple pill, 328 of 337 [97.3%]; usual care, 342 of 345 [99.1%]; 6 months: triple pill, 321 of 334 [96.1%]; usual care, 336 of 341 [98.5%]).
eFigure 1 in the Supplement shows the prescribing patterns of BP-lowering drugs in triple pill and usual care groups. Compared with usual care, patients in the triple pill group received far fewer changes in treatment regimen and were taking more classes of BP-lowering drugs from week 6 onwards (after initiation of the triple pill). Figure 2 shows the frequency distribution of patients by SBP level at each visit. A greater proportion of patients in the triple pill group had BP levels more than 10 mm Hg below the BP target compared with usual care groups at week 6 (197 of 329 [59.9%] vs 109 of 344 [31.7%]; P < .001) and week 12 (215 of 329 [65.3%] vs 116 of 340 [34.1%]; P < .001). Similarly, fewer patients in the triple pill group were more than 10 mm Hg above the BP target compared with usual care at week 6 (36 of 329 [10.9%] vs 85 of 344 [24.7%]; P < .001) and week 12 (15 of 329 [4.6%] vs 71 of 340 [20.9%]; P < .001).
Figure 2. Distribution of Patients by Systolic Blood Pressure (SBP) and Rate of Treatment Intensification.
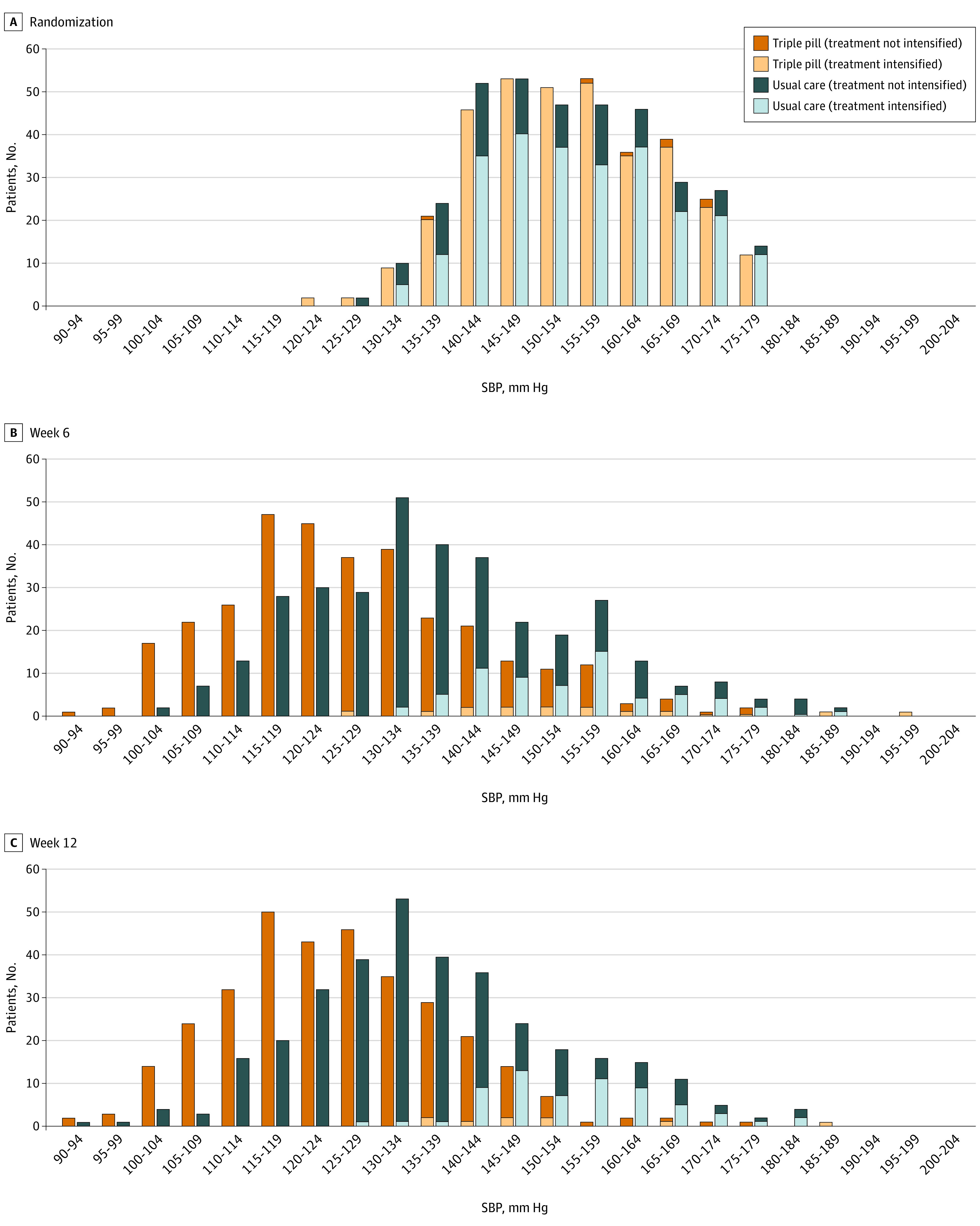
Orange shading indicates patients in the triple pill group and blue shading indicates patients in the usual care group. Lighter shading indicates the patients who underwent treatment intensification during the visit.
Association of Triple Pill Therapy With BP Control and Clinical Pathways
At the end of the study, 221 of 318 patients in the triple pill group (69.5%) and 182 of 329 patients in the usual care group (55.3%) reached BP targets. There was an even greater treatment effect for the proportion of patients reaching an SBP less than 130 mm Hg and a DBP less than 80 mm Hg (triple pill, 181 of 318 [56.9%]; usual care, 103 of 329 [31.3%]; relative risk 1.59; 95% CI, 1.38-1.85; P < .001).
There was a large reduction in the number of clinical pathways for the triple pill group compared with the usual care group, as assessed by the patient journey at each visit (BP target achieved [yes/no] and therapy intensified [yes/no]) (eFigure 2 in the Supplement). There were 23 unique clinical pathways per 100 treated patients in the triple pill group compared with 54 per 100 treated patients in the usual care group. As shown in eTable 1 in the Supplement, the most common clinical pathway for both groups was intensification of therapy at baseline, followed by sustained achievement in BP target at each subsequent follow-up visit (146 of 311 [46.9%] in the triple pill group and 47 of 326 [14.4%] in the usual care group). The 10 most frequent clinical pathways accounted for 289 of 311 patients in the triple pill group (92.9%) compared with 169 of 326 patients in the usual care group (51.8%) (eFigure 2 and eTable 1 in the Supplement).
Predictors of Treatment Intensification at Each Visit and BP Control at 6 Months
eTable 2 in the Supplement shows the predictors of treatment intensification at randomization, week 6, and week 12. A higher SBP significantly increased the chance of treatment intensification for the triple pill group at week 12 and the usual care group at randomization, week 6, and week 12. The mean (SD) SBP levels among those who did not reach BP targets were lower in the triple pill group compared with the usual care group at 6 weeks (145 [17] mm Hg vs 149 [15] mm Hg; P < .001) and at 12 weeks (142 [12] mm Hg vs 148 [14] mm Hg; P < 001). This explained, in part, the lower rates of treatment intensification in the triple pill group compared with the usual care group at weeks 6 and 12. Randomization to the triple pill group was not a significant independent predictor of treatment intensification at weeks 6 or 12, although the numbers intensified were low.
When considering predictors of BP control among all participants in a multivariable model (Table 3), randomization to triple pill was an independent predictor of reaching the BP target at the end of the study (adjusted odds ratio, 1.50; 95% CI, 1.04-2.15). Diabetes, a higher body mass index, a higher SBP at randomization, and increasing episodes of therapeutic inertia were independent predictors of failing to reach the BP target at the end of the study.
Table 3. Multivariate Model for Predictors of Reaching Blood Pressure (BP) Target at 6 Months for All Trial Participants.
| Variable | Adjusted OR (95% CI) | P value |
|---|---|---|
| Coronary artery disease | 0.64 (0.33-1.23) | .18 |
| Chronic kidney disease | 0.34 (0.08-1.57) | .17 |
| Diabetes | 0.52 (0.34-0.80) | .003 |
| Current alcohol drinker | 0.67 (0.40-1.13) | .13 |
| 10-y ASCVD risk (per 10% higher) | 0.90 (0.77-1.07) | .24 |
| BMIa | 0.95 (0.91-0.99) | .01 |
| Systolic BP at baseline (per 10–mm Hg higher) | 0.83 (0.71-0.97) | .02 |
| Taking BP-lowering drug at baseline | 1.12 (0.76-1.64) | .58 |
| Randomization to triple pill | 1.50 (1.04-2.15) | .03 |
| Therapeutic inertia (failure to intensify treatment) | ||
| 1 Time vs 0 times | 0.46 (0.31-0.70) | <.001 |
| 2 Times vs 0 times | 0.32 (0.19-0.54) | <.001 |
| 3 Times vs 0 times | 0.18 (0.06-0.50) | .001 |
Abbreviations: ASCVD, atherosclerotic cardiovascular disease; BMI, body mass index; OR, odds ratio.
Calculated as weight in kilograms divided by height in meters squared.
Discussion
The main findings of this analysis are (1) triple pill FDC therapy was associated with greater rates of therapeutic inertia compared with usual care, in part because SBP was lower in the triple pill group and SBP level was the main predictor of treatment intensification; (2) despite higher rates of therapeutic inertia, triple pill FDC therapy improved BP control with fewer unique treatment regimens and clinical pathways, which reflect the therapy’s ability to simplify treatment; and (3) failure to intensify treatment was strongly associated with failure to reach BP targets at the end of the study. These findings were only possible through the TRIUMPH trial’s unique pragmatic design, which allowed for physicians to adjust antihypertensive therapy at their discretion.
A major benefit of FDCs of antihypertensive drugs is that they provide early and effective treatment by providing a more potent therapy upfront, which allows for earlier achievement of BP targets. This will reduce the number of physician visits, which are currently recommended at monthly intervals until BP targets are achieved.4,5 Fixed-dose combination therapies simplify the management of hypertension through fewer drug combinations and fewer medication changes. In the present study, there was a large reduction in the number of unique clinical pathways for the triple pill group compared with the usual care group. These benefits are likely to be of most impact in low socioeconomic populations, who often experience higher rates of cardiovascular disease and limited access to health care.18 However, the benefits of FDC therapies will reach a threshold if therapeutic inertia persists after initiation of the combination therapy.12
Therapeutic inertia has been previously reported as a major impediment to adequate BP control.19,20,21 In the CardioMonitor survey21 of 21 053 patients with hypertension in Western Europe and the US, there were 11 969 patients with inadequately controlled hypertension, of whom only 15% to 38% received treatment intensification, with rates of 13% to 42% reported in other large studies.19,20,22 These findings are consistent with usual care in the present study, in which treatment intensification occurred in 35.2% to 36.0% of visits at which BP was not controlled; however, a novel finding was that therapeutic inertia rates were even higher in the triple pill group during follow-up, with only 10.0% to 13.2% who did not achieve BP targets receiving treatment intensification in this group. The lower rate of treatment intensification in the triple pill group was partly due to their lower SBP levels, with fewer patients having an SBP more than 10 mm Hg above the BP target. However, it is also likely due in part to the reluctance to up-titrate to the higher-dose triple pill containing double the doses of all 3 drugs. This double-dose version was only used in 10 patients (2.9%).
To our knowledge, there have been few randomized trials reporting the effects of FDCs on therapeutic inertia compared with usual care, especially in the context of initial or early treatment, since control group regimens were protocolized and standardized in most previous trials. In the Simplified Treatment Intervention to Control Hypertension (STITCH) trial,13 the use of a simplified algorithm starting with dual combination therapy provided better BP control than the traditional stepped-care titration at 6 months, but to our knowledge, there have been no reports of the rates of therapeutic inertia by randomized group during follow-up. In the Strategies of Treatment in Hypertension Evaluation (STRATHE) trial, dual combination therapy improved BP control without excess adverse events compared with both sequential monotherapy and a stepped-care regimen.23 Polypills containing a combination of BP-lowering drugs and statins with or without aspirin have been shown to improve adherence and BP control and to reduce low-density lipoprotein cholesterol levels compared with usual care.24,25 In particular, the SPACE collaboration analysis25 of 3140 patients found that 80% to 95% of all patients randomized to a polypill were taking combination therapy (aspirin, statin, and 2 BP-lowering drugs) by 1 month irrespective of the number of drugs at baseline, reflecting the potential of polypills to simplify regimens and provide treatment intensification.
Different reasons for therapeutic inertia have been previously reported. In the Reasons for not Intensifying Antihypertensive Therapy (RIAT) study20 of 35 302 patients, the main reasons for not intensifying antihypertensive treatment when BP remained above target were the assumption that the interval after starting the new drug was too short to attain its full effect, the satisfaction with a clear improvement of BP or with a BP nearing the target, and the acceptance of good self-measurements. Similarly, in the PRESCAP cross-sectional study22 of 12 961 patients, the physicians’ perception of good BP control in uncontrolled patients together with the presence of multiple antihypertensive agents were the 2 variables most strongly associated with therapeutic inertia.
Greater efforts are required to prevent therapeutic inertia, particularly when using FDC therapies. Potential strategies to improve therapeutic inertia may include education, incentives for appropriate treatment intensification, and physician feedback or reminders.13 There may also be a need for more dosage options with the FDC triple pill to allow physicians to intensify therapy without fear of overtreatment and adverse drug effects.
Limitations
The present study has limitations to consider. The trial protocol included only 4 patient visits, which provided only 3 time points (with the first visit being at randomization) for assessing opportunities for treatment intensification. However, a low number of follow-up visits may represent real clinical practice, particularly in low-income settings. By specifying the timing of patient visits, the study did not fully reflect real-world treatment of hypertension. The study was not able to investigate prescriber-related reasons for therapeutic inertia, which may differ in the setting of triple pill use. This will be investigated in a subsequent process evaluation of the TRIUMPH trial.26 Additionally, patients did not have access to home and ambulatory BP monitoring, and therefore, our findings cannot be extrapolated to these devices.
Conclusions
Initiation of triple pill FDC therapy substantially simplified prescribing patterns and improved 6-month BP control rates compared with usual care. However, therapeutic inertia was more common among patients receiving triple pill therapy compared with usual care. Further improvements in hypertension control could be achieved by addressing therapeutic inertia among the minority of patients who do not achieve BP control after initial FDC therapy.
eTable 1. Ten most common clinical pathways among patients in the triple pill and usual care groups.
eTable 2. Multivariate predictors of intensification of BP-lowering drug therapy after not reaching BP target.
eFigure 1. Treatment patterns according to BP-lowering drug class and achievement of BP target.
eFigure 2. Number of unique clinical pathways among patients in the triple pill and usual care groups.
References
- 1.GBD 2016 Risk Factors Collaborators Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1345-1422. doi: 10.1016/S0140-6736(17)32366-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Forouzanfar MH, Liu P, Roth GA, et al. . Global burden of hypertension and systolic blood pressure of at least 110 to 115 mm Hg, 1990-2015. JAMA. 2017;317(2):165-182. doi: 10.1001/jama.2016.19043 [DOI] [PubMed] [Google Scholar]
- 3.Mensah GA, Bakris G. Treatment and control of high blood pressure in adults. Cardiol Clin. 2010;28(4):609-622. doi: 10.1016/j.ccl.2010.08.002 [DOI] [PubMed] [Google Scholar]
- 4.Whelton PK, Carey RM, Aronow WS, et al. . 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71(6):e13-e115. [DOI] [PubMed] [Google Scholar]
- 5.Williams B, Mancia G, Spiering W, et al. ; ESC Scientific Document Group . 2018 ESC/ESH guidelines for the management of arterial hypertension. Eur Heart J. 2018;39(33):3021-3104. doi: 10.1093/eurheartj/ehy339 [DOI] [PubMed] [Google Scholar]
- 6.Cushman WC, Basile J. Achieving blood pressure goals: why aren’t we? J Clin Hypertens (Greenwich). 2006;8(12):865-872. doi: 10.1111/j.1524-6175.2006.05789.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chow CK, Gupta R. Blood pressure control: a challenge to global health systems. Lancet. 2019;394(10199):613-615. doi: 10.1016/S0140-6736(19)31293-0 [DOI] [PubMed] [Google Scholar]
- 8.López-Jaramillo P, González-Gómez S, Zarate-Bernal D, et al. . Polypill: an affordable strategy for cardiovascular disease prevention in low-medium-income countries. Ther Adv Cardiovasc Dis. 2018;12(6):169-174. doi: 10.1177/1753944718764588 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Thom S, Poulter N, Field J, et al. ; UMPIRE Collaborative Group . Effects of a fixed-dose combination strategy on adherence and risk factors in patients with or at high risk of CVD: the UMPIRE randomized clinical trial. JAMA. 2013;310(9):918-929. Published correction appears in JAMA. 2013;310(14):1507. doi: 10.1001/jama.2013.277064 [DOI] [PubMed] [Google Scholar]
- 10.Patel A, Cass A, Peiris D, et al. ; Kanyini Guidelines Adherence with the Polypill (Kanyini GAP) Collaboration . A pragmatic randomized trial of a polypill-based strategy to improve use of indicated preventive treatments in people at high cardiovascular disease risk. Eur J Prev Cardiol. 2015;22(7):920-930. doi: 10.1177/2047487314530382 [DOI] [PubMed] [Google Scholar]
- 11.Selak V, Elley CR, Bullen C, et al. . Effect of fixed dose combination treatment on adherence and risk factor control among patients at high risk of cardiovascular disease: randomised controlled trial in primary care. BMJ. 2014;348:g3318. doi: 10.1136/bmj.g3318 [DOI] [PubMed] [Google Scholar]
- 12.Briasoulis A, Bakris G. Initial single-pill combination therapy for cardiovascular risk factor management: it is not just convenience. J Hypertens. 2013;31(8):1537-1538. doi: 10.1097/HJH.0b013e328361d016 [DOI] [PubMed] [Google Scholar]
- 13.Feldman RD, Zou GY, Vandervoort MK, Wong CJ, Nelson SA, Feagan BG. A simplified approach to the treatment of uncomplicated hypertension: a cluster randomized, controlled trial. Hypertension. 2009;53(4):646-653. [DOI] [PubMed] [Google Scholar]
- 14.Dresser GK, Nelson SA, Mahon JL, et al. . Simplified therapeutic intervention to control hypertension and hypercholesterolemia: a cluster randomized controlled trial (STITCH2). J Hypertens. 2013;31(8):1702-1713. doi: 10.1097/HJH.0b013e3283619d6a [DOI] [PubMed] [Google Scholar]
- 15.Webster R, Salam A, de Silva HA, et al. ; TRIUMPH Study Group . Fixed low-dose triple combination antihypertensive medication vs usual care for blood pressure control in patients with mild to moderate hypertension in Sri Lanka: a randomized clinical trial. JAMA. 2018;320(6):566-579. doi: 10.1001/jama.2018.10359 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Salam A, Webster R, Singh K, et al. . Triple Pill vs Usual Care Management for Patients With Mild-to-Moderate Hypertension (TRIUMPH): study protocol. Am Heart J. 2014;167(2):127-132. doi: 10.1016/j.ahj.2013.10.020 [DOI] [PubMed] [Google Scholar]
- 17.Law MR, Morris JK, Wald NJ. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. BMJ. 2009;338:b1665. doi: 10.1136/bmj.b1665 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Muñoz D, Wang TJ. The polypill revisited: why we still need population-based approaches in the precision medicine era. Circulation. 2019;140(22):1776-1778. doi: 10.1161/CIRCULATIONAHA.119.043491 [DOI] [PubMed] [Google Scholar]
- 19.Okonofua EC, Simpson KN, Jesri A, Rehman SU, Durkalski VL, Egan BM. Therapeutic inertia is an impediment to achieving the Healthy People 2010 blood pressure control goals. Hypertension. 2006;47(3):345-351. [DOI] [PubMed] [Google Scholar]
- 20.Ferrari P; National Coordinators for the Reasons for not Intensifying Antihypertensive Treatment (RIAT) trial12 . Reasons for therapeutic inertia when managing hypertension in clinical practice in non-Western countries. J Hum Hypertens. 2009;23(3):151-159. doi: 10.1038/jhh.2008.117 [DOI] [PubMed] [Google Scholar]
- 21.Wang YR, Alexander GC, Stafford RS. Outpatient hypertension treatment, treatment intensification, and control in Western Europe and the United States. Arch Intern Med. 2007;167(2):141-147. doi: 10.1001/archinte.167.2.141 [DOI] [PubMed] [Google Scholar]
- 22.Alonso Moreno FJ, Llisterri Caro JL, Rodríguez Roca GC, et al. . Medical conduct in primary care as regards blood pressure control. PRESCAP 2010 study. Semergen. 2013;39(1):3-11. Article in Spanish. doi: 10.1016/j.semerg.2012.05.007 [DOI] [PubMed] [Google Scholar]
- 23.Mourad JJ, Waeber B, Zannad F, Laville M, Duru G, Andréjak M; investigators of the STRATHE trial . Comparison of different therapeutic strategies in hypertension: a low-dose combination of perindopril/indapamide versus a sequential monotherapy or a stepped-care approach. J Hypertens. 2004;22(12):2379-2386. doi: 10.1097/00004872-200412000-00021 [DOI] [PubMed] [Google Scholar]
- 24.Muñoz D, Uzoije P, Reynolds C, et al. . Polypill for cardiovascular disease prevention in an underserved population. N Engl J Med. 2019;381(12):1114-1123. doi: 10.1056/NEJMoa1815359 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Webster R, Patel A, Selak V, et al. ; SPACE Collaboration . Effectiveness of fixed dose combination medication (‘polypills’) compared with usual care in patients with cardiovascular disease or at high risk: a prospective, individual patient data meta-analysis of 3140 patients in six countries. Int J Cardiol. 2016;205:147-156. doi: 10.1016/j.ijcard.2015.12.015 [DOI] [PubMed] [Google Scholar]
- 26.Salam A, Webster R, Patel A, et al. . Process evaluation of a randomised controlled trial of a pharmacological strategy to improve hypertension control: protocol for a qualitative study. BMJ Open. 2018;8(8):e022317. doi: 10.1136/bmjopen-2018-022317 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eTable 1. Ten most common clinical pathways among patients in the triple pill and usual care groups.
eTable 2. Multivariate predictors of intensification of BP-lowering drug therapy after not reaching BP target.
eFigure 1. Treatment patterns according to BP-lowering drug class and achievement of BP target.
eFigure 2. Number of unique clinical pathways among patients in the triple pill and usual care groups.