

Abstract
Background:
Considering the role of Vitamin D in cardiovascular disease (CVD) and the relationship between coronary artery calcification (CAC) and CVD, we aimed to investigate the association between the serum level of Vitamin D and CAC.
Materials and Methods:
This was a cross-sectional study on 67 consecutive patients who were referred for performing computed tomography angiography. We used Spearman correlation to evaluate the relationship between Vitamin D and CAC and then linear regressions to control for demographics and vascular risk factors.
Results:
There was no association between CAC and Vitamin D levels (Spearman coefficient = −0.03, P = 0.805). After controlling for age, sex, hypertension, hyperlipidemia, diabetes mellitus, and smoking, there was still no association between Vitamin D and CAC score (estimate = 0.001, S. E. = 0.020, P = 0.942).
Conclusion:
We did not find the association between the serum level of Vitamin D and coronary artery calcification.
Keywords: Atherosclerosis, computed tomography angiography, coronary artery diseases, vascular calcification, Vitamin D
INTRODUCTION
Nowadays, cardiovascular disease (CVD) is considered one of the most common and important noncommunicable diseases.[1] Several studies have shown that there is a strong association between Vitamin D deficiency and an increased risk of CVD.[2,3]
Coronary artery calcification (CAC) is considered as a risk factor in addition to traditional risk factors such as diabetes mellitus (DM), hypertension (HTN), smoking, and hypercholesterolemia that will improve the prediction of CVD risk categorization. Computed tomography angiography (CTA) can measure the calcium score of coronary arteries which is an established marker of CAC and atherosclerosis.[4]
Most of the studies which evaluate the relationship between Vitamin D and CAC were published based on the United States population.[5] In addition, the results regarding this issue are still inconclusive. The aim of the present study is to gain more insight on the association between the serum level of Vitamin D and CAC in the Iranian population.
MATERIALS AND METHODS
In our cross sectional study, cardiologists referred 67 consecutive patients based on the indications of cardiac CTA between April 2016 and October 2018. The indication of cardiac CTA was according to the American Heart Association guideline.[6]
Vitamin D measurement
Based on Vitamin D levels, we classified patients into three groups: Vitamin D sufficient (Vitamin D ≥20 ng/mL), insuficient (12–20 ng/mL), or deicient (<12 ng/mL).[7]
Coronary artery calcification assessment
CAC was assessed by CTA. The coronary artery calcium score (CACS) was calculated by the Agastone scoring method (Smart Score software). The CACS equal to zero was assumed as the absence of CAC and CACS greater than zero as the presence of CAC. In this study, we examined the association of Vitamin D with the presence of CAC and with its severity.
Assessment of other variables
Age, gender, past medical history of HTN, hyperlipidemia, DM, and smoking were obtained using the questionnaire administrated by a trained nurse.
Statistical analysis
We used t-test and Mann–Whitney for bivariate comparison of quantitative variables, and Chi-square for the comparison of categorical variables between patients with and without CAC. Then, we used logistic regression to examine the association between Vitamin D levels and CAC and linear regressions to examine the association between Vitamin D levels and CACS. The models were controlled for the demographics. The analyses were performed using the Statistical Package for Social Sciences software (SPSS, version 22).
RESULTS
The characteristics of the recruited patients are shown in Table 1 . They were on average 57 years and 60% were men. Patients with and without CAC were not different in HTN, smoking, creatinine, and C-reactive protein levels. However, patients with CAC were older and reported hypercholesterolemia and DM more compared to patients without CAC [Table 1].
Table 1.
Baseline clinical characteristics of patients according to coronary artery calcification status
| Characteristics | Total (n=67), n (%) | Without CAC (n=30), n (%) | With CAC (n=37), n (%) | P |
|---|---|---|---|---|
| Age (year) | 56.6±10.9 | 53.2±12.1 | 59.0±9.4 | 0.036 |
| Sex | ||||
| Female | 27 (40) | 11 (37) | 16 (43) | 0.625 |
| Male | 40 (60) | 19 (63) | 21 (57) | |
| Hyperlipidemia | 35 (52) | 12 (60) | 23 (62) | 0.048 |
| Hypertension | 30 (45) | 11 (37) | 19 (51) | 0.325 |
| Smoking | 10 (15) | 3 (10) | 7 (19) | 0.304 |
| Diabetes | 16 (24) | 4 (13) | 12 (32) | 0.045 |
| Creatinine (mg/dl) | 1.0±0.1 | 1.0±0.2 | 1.0±0.1 | 0.373 |
CAC=Coronary artery calcification
Vitamin D level and coronary artery calcifications
Vitamin D level was not different between patients with (median = 31.5 ng/ml and interquartile range [IQR] = 24.4 ng/ml) and without (median = 31.1 ng/ml and IQR = 30.2 ng/ml) CAC (P = 0.779). In a logistic regression model, Vitamin D level was not related to the odds of CAC (odds ratio = 1.00 (95% confidence interval: 0.97–1.03; P = 0.995).
In a sensitivity analysis, we examined Vitamin D as a categorical variable following the recent clinical guideline.[7] CAC was not different in the Vitamin D categories (Chi-square = 1.72, P = 0.423).
Vitamin D levels and coronary artery calcium scores
The association between Vitamin D level and CACS was weak and insignificant (Spearman correlation coefficient = 0.03; P = 0.805). After excluding patients with CACS = 0, there was still no association between Vitamin D levels and CACS (Spearman correlation coefficient = −0.01, P = 0.975) [Figure 1].
Figure 1.
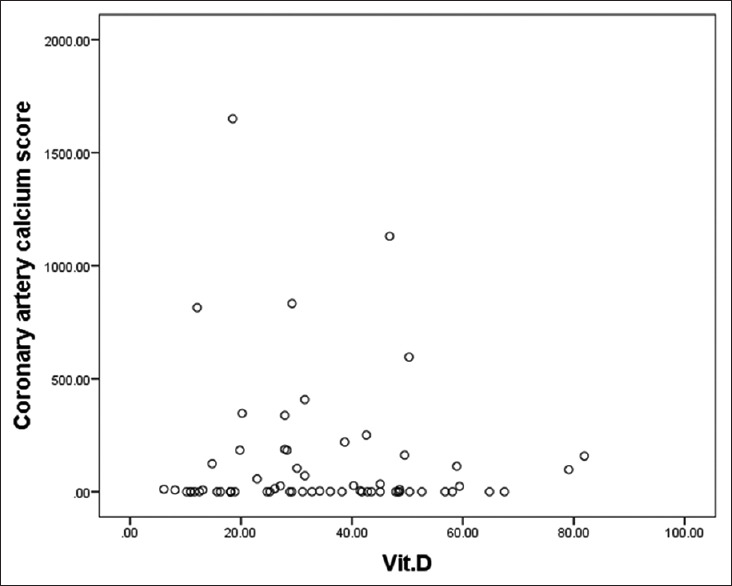
Spearman correlation between Vitamin D and coronary artery calcium score
As clinical and demographic characteristics of patients might have resulted in insignificant association between serum Vitamin D levels and CACS, we leveraged linear regressions to examine the simultaneous association of covariates with the CACS in the presence of Vitamin D. As CACS did not have a normal distribution, we transformed the CACS by a natural logarithmic function and used this transformation values as the outcome of the succeeding regression models. Then, we examined the association between Vitamin D with CACS in linear regression models controlled for the demographics and clinical characteristics. The addition of terms for vascular risk factors did not change the conclusion that Vitamin D was not related to CACS [Table 2].
Table 2.
The association between the serum levels of Vitamin D and coronary artery calcification score*
| Association of Vitamin D with CAC score | ||
|---|---|---|
| Estimate (SE) | P | |
| Model 1 | 0.007 (0.018) | 0.704 |
| Model 2 | −0.005 (0.019) | 0.807 |
| Model 3 | 0.001 (0.020) | 0.942 |
*All the models are linear regressions with the Vitamin D as the predictor and CAC score as the outcome, Model 1 was not controlled for any other covariate, Model 2 was controlled for age and sex, Model 3 was controlled for age, sex, hypertension, diabetes mellitus, smoking, and hyperlipidemia. SE=Standard error, CAC=Coronary artery calcification
In a sensitivity analysis, we examined the association of the CACS with the categories of Vitamin D. Medians of CACS were not different in different categories of Vitamin D (< 12: median = 0.0, IQR = 8.5; 12–20: median = 0.0, IQR = 169.0; ≥20: Median = 7.0, IQR = 159; Kruskal-Wallis Chi-square = 2.272, P = 0.321).
DISCUSSION
According to the study of Framingham,[8] we can predict the 10-year risk of CAD, though the prediction does not have high accuracy, and better CAD prediction models are needed. Recently, some studies showed interest in the relationship between the serum Vitamin D level and CAC because the CAC considered a strong marker for CAD.[5,9] However, studies investigating the association between serum level of Vitamin D and CAC had mixed and very contrasting results.[5,10,11,12]
Leveraging data from near to 70 adults, we found that Vitamin D was not associated with CAC. Controlling for demographics and vascular risk factors did not change this conclusion.
In our opinion, the main reason that can explain contrasting results about the association between Vitamin D level and CAC is that many studies did not adjust their results with the confounding variables. All of the traditional cardiovascular risk factors in the Framingham study[8] such as smoking, DM, HTN, hyperlipidemia, age, and sex can interfere with the association of Vitamin D level and CAC. For instance, Lee et al.'s study[11] was based on middle-aged men, whereas the study of Lim[12] was a cohort limited to elderly people. Therefore, all of the possible cardiovascular confounding variables must be considered in future investigations.
Our study has some limitations, including small sample size and lack of information about patients' calcium and parathyroid hormone levels and their drugs use. In addition, its design was a cross-sectional one which precludes causality conclusion. This study has also several strengths. It was the first research investigating an association between Vitamin D level and CAC in Isfahan, Iran attempting adjustment for different confounders. We used standardized methods to obtain patients CACs and Vitamin D levels.
CONCLUSION
In conclusion, we did not find any association between serum vitamin D level and coronary artery calcification. Other mechanisms may be involved in the association between vitamin D level and cardiovascular outcomes.
Financial support and sponsorship
This study was financially supported by the Isfahan University of Medical Sciences.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to thank the Isfahan University of Medical Sciences (Research Project number: 396601) for their financial support.
REFERENCES
- 1.Laslett LJ, Alagona P, Jr, Clark BA, 3rd, Drozda JP, Jr, Saldivar F, Wilson SR, et al. The worldwide environment of cardiovascular disease: Prevalence, diagnosis, therapy, and policy issues: A report from the American college of cardiology. J Am Coll Cardiol. 2012;60:S1–49. doi: 10.1016/j.jacc.2012.11.002. [DOI] [PubMed] [Google Scholar]
- 2.Kunadian V, Ford GA, Bawamia B, Qiu W, Manson JE. Vitamin D deficiency and coronary artery disease: A review of the evidence. Am Heart J. 2014;167:283–91. doi: 10.1016/j.ahj.2013.11.012. [DOI] [PubMed] [Google Scholar]
- 3.Anderson JL, May HT, Horne BD, Bair TL, Hall NL, Carlquist JF, et al. Relation of vitamin D deficiency to cardiovascular risk factors, disease status, and incident events in a general healthcare population. Am J Cardiol. 2010;106:963–8. doi: 10.1016/j.amjcard.2010.05.027. [DOI] [PubMed] [Google Scholar]
- 4.Polonsky TS, McClelland RL, Jorgensen NW, Bild DE, Burke GL, Guerci AD, et al. Coronary artery calcium score and risk classification for coronary heart disease prediction. JAMA. 2010;303:1610–6. doi: 10.1001/jama.2010.461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Malik R, Aneni EC, Roberson L, Ogunmoroti O, Ali SS, Shaharyar S, et al. Measuring coronary artery calcification: Is serum vitamin D relevant? Atherosclerosis. 2014;237:734–8. doi: 10.1016/j.atherosclerosis.2014.10.087. [DOI] [PubMed] [Google Scholar]
- 6.Fihn SD, Blankenship JC. Clinical guidelines. J Thorac Cardiovasc Surg. 2015;149:e5–23. doi: 10.1016/j.jtcvs.2014.11.002. [DOI] [PubMed] [Google Scholar]
- 7.Food and Nutrition Board IoM. DRI Dietary Reference Intakes for Calcium and Vitamin D. Washington, DC: National Academy Press; 2011. [Google Scholar]
- 8.Berry JD, Lloyd-Jones DM, Garside DB, Greenland P. Framingham risk score and prediction of coronary heart disease death in young men. Am Heart J. 2007;154:80–6. doi: 10.1016/j.ahj.2007.03.042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Pletcher MJ, Tice JA, Pignone M, Browner WS. Using the coronary artery calcium score to predict coronary heart disease events: A systematic review and meta-analysis. Arch Intern Med. 2004;164:1285–92. doi: 10.1001/archinte.164.12.1285. [DOI] [PubMed] [Google Scholar]
- 10.Lichtenstein G, Perlman A, Shpitzen S, Durst R, Shaham D, Leitersdorf E, et al. Correlation between coronary artery calcification by non-cardiac CT and Framingham score in young patients. PLoS One. 2018;13:e0195061. doi: 10.1371/journal.pone.0195061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lee S, Ahuja V, Masaki K, Evans RW, Barinas-Mitchell EJ, Ueshima H, et al. A Significant Positive Association of Vitamin D Deficiency with Coronary Artery Calcification among Middle-aged Men: For the ERA JUMP Study. J Am Coll Nutr. 2016;35:614–20. doi: 10.1080/07315724.2015.1118651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lim S, Shin H, Kim MJ, Ahn HY, Kang SM, Yoon JW, et al. Vitamin D inadequacy is associated with significant coronary artery stenosis in a community-based elderly cohort: The Korean Longitudinal Study on Health and Aging. J Clin Endocrinol Metab. 2012;97:169–78. doi: 10.1210/jc.2011-1580. [DOI] [PubMed] [Google Scholar]