

Abstract
CONTEXT:
Emotional communications play an important role in having a satisfying relationship and a more successful marriage. If marriage does not provide suitable conditions to satisfy couple's needs, not only it does not help to mental health but also results in negative and irreversible effects.
AIMS:
This research was performed with the aim of determining the impact of emotional intelligence training on marital satisfaction, sexual quality of life, and psychological well-being of women.
SETTINGS AND DESIGN:
The present research is an experimental study conducted on 70 women referring to community health centers of Shahid Beheshti University of Medical Sciences in 2019.
SUBJECTS AND METHODS:
The sampling was performed using multistage cluster sampling. Before implementing the training intervention, the research instruments (general questionnaire, Kansas Marital Satisfaction Scale, Iranian version of Sexual Quality of Life-Female questionnaire, and World Health Organization Five Well-Being Index) were provided to the participants in order to complete them. All participants recompleted the instruments immediately and 1 month after the training intervention.
STATISTICAL ANALYSIS USED:
The significance level was considered as P < 0.05.
RESULTS:
The mean scores of marital satisfaction in the control group had no significant difference before, immediately after, and 1 month after the intervention (P = 0.895). However, in the intervention group, over time, the mean scores of marital satisfaction increased (P = 0.001), and the difference between the two groups was significant (P < 0.001). The mean scores of sexual quality of life and psychological well-being had no significant differences before, immediately after, and 1 month after the intervention in the control group. However, in the intervention group, over time, the mean scores of sexual quality of life and psychological well-being firstly increased and then decreased (P < 0.001), and the difference between the two groups was significant (P < 0.001).
CONCLUSIONS:
Training the components of emotional intelligence can be effective on enhancing marital satisfaction, sexual quality of life, and psychological well-being of women.
Keywords: Emotional intelligence, marital satisfaction, psychological well-being, sexual quality of life
Introduction
Marriage can be described as the most important phenomenon in human relationships as it can provide the principal structure for developing familial relationships and development of the next generation.[1] It results in peace, personal and social development, gratification of sexual needs, and psychological needs of individuals, thereby providing individual and public health.[2] In spite of the desired consequences of marriage, unfortunately, many couples have problems in establishing and maintaining proper and effective relationships with each other,[3] such that we are witnessing progressive rate of divorce in different societies.[4] Various studies have indicated that different factors such as marital and sexual dissatisfaction can affect the relationships between couples and may also cause an increased tendency for separation between them.[5] Marital satisfaction is considered as a sense of happiness and satisfaction between couples about different aspects of their marriage.[6] Kaplan and Maddux (2002) stated that marital satisfaction is a personal experience in marriage and can be accessed just by the couples themselves. This concept develops in response to the extent of satisfaction with the marital relationship. They believe that marital satisfaction depends on personal expectations and beliefs.[7] Concerning the importance of the role of family in the society and prevention of devastation of its foundation, awareness of the factors affecting marital satisfaction as the basis for familial integrity seems to be essential.[8] One of the factors that can affect adaptation and satisfaction of spouses with marital life is the quality of life.[9] Quality of life is a complex concept affected by various factors such as physical health, psychological status, level of independence, social relations, personal beliefs, and environmental factors.[10] Furthermore, one of the important dimensions of quality of life is sexual quality of life.[11] Sexual quality of life is one of the key issues in the area of sexual health. Researchers believe that it refers to the sense of sexual attraction, interest and participation in daily activities as well as perception of sexual function, which is tightly interwoven with overall quality of life and the level of satisfying from it.[12,13] Concerning the undeniable role of sexual function in the human life and its relationship with the quality of life as well as psychological well-being, as the sexual quality of individuals' life increases, so does their well-being.[14,15] Psychological well-being is one of the aspects for healthy functioning in individuals.[16] Csiks Zentmihaly has defined well-being as achieving a balance between positive and negative emotions along with satisfaction with life. One of the important variables regarding the psychological well-being is emotional intelligence.[17] Emotional intelligence can be regarded as the ability of appropriately identifying the emotions and affections in others and suitable responses to them, as well as stimulation, awareness, organization, and control of one's emotional responses.[18] Today, emotional intelligence has been emphasized as a factor for improving marital satisfaction between couples. Using emotional intelligence skills, couples will be able to overcome stressful factors in the course of their marital life.[19] The notable point is that emotional intelligence is not something intrinsic or genetic; rather, it can be trained and learned.[20] Training emotional intelligence results in increased awareness of individuals of their emotions as well as acquiring greater skills and abilities in managing their problems and emotions, thereby contributing to more successful adaptation to the environment, needs, pressures, and higher psychological health.[21] According to Silva et al. study, there are significant but mild levels of association between emotional intelligence and sexual function.[22] The results of the study by Guerra-Bustamante et al. suggested that as the capacity of understanding and regulation of emotional intelligence increases, psychological well-being also increases.[23] Siavoshi et al. also found that there was a positive and significant relationship between emotional intelligence and marital satisfaction.[24] Considering the importance of emotional intelligence skills and its role in regulating the emotional states and in turn improving the relationships between couples and their psychological health, this can be employed in investigating and providing supportive and educational interventions by nurses.[19] Not many studies exist that determine the impact of training the components of emotional intelligence on marital and sexual variables, such as marital satisfaction, sexual quality of life, and psychological well-being. In order to fill the gap in the research, we developed this study with the aim of assessing the impact of training emotional intelligence on three components of women marital satisfaction, sexual quality of life, and their psychological well-being
Subjects and Methods
The present research is an experimental study with pre/posttest design as well as intervention and control groups that was performed in 2019. A total of 70 women with reproductive ages who were referred to the community health centers of Shahid Beheshti University of Medical Sciences were enrolled in this study using a multistage cluster sampling method. To implement this research, after acquiring the necessary permissions from Educational Deputy of the Nursing School of Shahid Beheshti University of Medical Sciences and Ministry of Health and Medical Education's Deputy of Health, determining the researched community health centers, identifying women qualifying for the research unit characteristics, and gaining both oral and written consent; the samples were included. Specifically, at first, all community health centers of Shahid Beheshti University of Medical Sciences were classified into four clusters based on geographical regions. Then, inside the clusters, one center was randomly chosen. Overall, four community health centers were considered; and two centers were randomly assigned to the intervention group (n = 35) and two others as control groups (n = 35) (drawcard). Inside the community health centers, the samples fulfilling the inclusion criteria were chosen through convenience sampling. The inclusion criteria were as follows: being married and living with their spouse, having nuclear family, age ranged from 18 to 49 years (reproductive ages), willingness to respond to the research instruments, and literacy (reading and writing). On the other hand, the exclusion criteria included absence of more than two sessions from the training sessions and incomplete research instruments. Furthermore, the research tools were as follows:
General questionnaire
It contained 11 questions on demographic and health characteristics of women enrolled in the study (age, educational status, employment status, educational status of the spouse, employment status of the spouse, the number of marital life years, the number of family members, the family income sufficiency, history of chronic disease, history of nervous and psychological disease, and incidence of emotional problems over the past 2 weeks).
Kansas Marital Satisfaction Scale
This scale has three items with a seven-point Likert scale ranging from extremely dissatisfied[1] to extremely satisfied[7] to measure the marital satisfaction. The minimum and maximum possible scores are 3 and 21, respectively. Accordingly, high scores represent greater marital satisfaction. The designers of this scale believe that scores 17 and above indicate the highest level of marital satisfaction.[25] The validity of this instrument in Iran has been investigated by Arab Alidousti et al. (2015) through three methods of convergent validity, known-group comparison, and factorial validity, and the results suggested the desired validity of this instrument. The reliability of this instrument was examined through Cronbach's alpha method as well as item-scale correlations. The Cronbach's alpha coefficient was obtained as α = 0.98, whereas the item-scale correlation for all items was at least r = 0.2 and above, which represents the desired reliability of this questionnaire.[26]
Iranian version of Sexual Quality of Life-Female questionnaire
It was designed by Maasoumi et al., evaluating sexual quality of life in married Iranian women during their reproductive ages. This questionnaire contains 61 items with a five-point Likert type scale (1 = strongly disagree and 5 = strongly agree). The minimum score acquired in this instrument is 61, while the maximum is 305. The basis for analyzing the acquired score is the mean score of the covered population, in which the scores higher than the average score signal a better status of sexual quality of life, while the scores lower than that reflect less desirable status of sexual quality of life. The content validity and face validity of Sexual Quality of Life-Female (SQOL-F) questionnaire (Iranian version) were investigated both quantitatively and qualitatively, where CVI and CVR were obtained as 0.97 and 0.74, respectively, demonstrating desired validity of this questionnaire. Finally, the reliability of this questionnaire was calculated using two methods as follows: Cronbach's alpha (α = 0.94) and stability determination within a 2-week interval (r = 0.95, P < 0.001), indicating the desirable reliability of this instrument.[27,28]
World Health Organization Five Well-Being Index
It is a short self-report index measuring positive well-being over the past 2 weeks based on a 6-point Likert scale ranging from 0 (never) to 6 (always). The raw score of the respondent theoretically spans from 0 (no well-being) up to 25 (maximum well-being). Furthermore, through multiplying the total score by 4, the range of scores can be converted to 0–100 scale, in which higher scores reflect greater well-being, while lower scores indicate depression.[29] The convergent validity and reliability of the World Health Organization Five Well-Being Index in Iran were investigated by Dehshiri and Mousavi, indicating desired convergent validity of the instrument. Further, the Cronbach's alpha coefficient of this scale was found as α = 089, suggesting high internal consistency and desired reliability of this index.[30]
In the present research, the content validity and face validity of the questionnaires were confirmed by 10 professors of Nursing and Midwifery School of Shahid Beheshti University of Medical Sciences. In order to determine the reliability of instruments, internal consistency method and stability determination were used. Furthermore, to specify the internal consistency, the Cronbach's alpha of instruments was determined, and in marital satisfaction, sexual quality of life, and well-being index, the coefficients were found to be 0.92, 0.86, and 0.88, respectively, representing desired reliability of the questionnaires.
Before implementing the educational intervention, the training contents of components of emotional intelligence were prepared which validity was confirmed by two psychiatric nursing and community health nursing professors at Shahid Beheshti University of Medical Sciences. Before holding the educational sessions, the research instruments were provided to the participants in order to be completed. Then, the participants in the intervention group (n = 35) in 10–15-member groups participated in seven 90-min sessions to acquire emotional intelligence skills for approximately 2 months and once per week. The educational program was implemented by one of the researchers through lecture, question and answer, group discussion, and practice (both theoretical and practical). During each session, 60 min was devoted to training of emotional intelligence, 10 min to rest and catering, and final 20 min of each session to the practicing of the taught skills, answering of participants' questions, and the final evaluation of the session. Schedule including the topic, date, and time of each session was also given to the participants. To ensure that the participants practiced and performed their assignments, the researcher contacted them through phone calls once a week during the intervals between sessions. Accordingly, emotional intelligence skills were trained in terms of the theoretical principles of emotional intelligence developed by Goleman (emotional intelligence components including self-awareness, self-regulation, motivation, as well as social components of emotional intelligence including empathy and social skills), Gottman emotional intelligence training techniques (awareness of emotions, seeing emotions as an opportunity for connection and teaching, listening and validating feelings, assisting individuals to label the emotions, and helping a person discover appropriate ways to solve a problem or deal with an upsetting situation), and based on the Bar-On's emotional intelligence components (interpersonal function, intrapersonal skills, adaptability, stress management, and general mood). The summary of the content of the seven sessions for training the components of emotional intelligence was as follows:
Session 1: Briefing and pretest
Session 2: Training the skills for emotional self-awareness and identifying the emotions and feelings belonged to others (in terms of the individual components of emotional intelligence of Goleman along with emotional intelligence training techniques of Gottman)
Session 3: Training the proper ways of self-expression and self-respect, interpersonal, and empathy skills (in terms of the social components of emotional intelligence of Goleman as well as Bar-On's emotional intelligence components)
Session 4: Training the methods of stress management and social responsibility (in terms of the Bar-On's emotional intelligence components)
Session 5: Training problem-solving skills and flexibility (in terms of the Bar-On's emotional intelligence components and emotional intelligence training techniques by Gottman)
Session 6: Training the skills of happiness and optimism (in terms of the Bar-On's emotional intelligence components)
Session 7: Reassessing the participants and posttest.
All the participants recompleted the instruments immediately and 1 month after the educational intervention. At the end of the study, since the control group received no intervention, in order to respect ethical considerations; a brochure about what had been explained in the training sessions was prepared and provided to all participants (both intervention and control groups). For data analysis, SPSS version 18 software was used. Statistical tests including Chi-square test and Fisher's exact test (to investigate the difference between the two groups regarding qualitative demographic variables), independent t-test (to compare the intervention and control groups), and repeated measures ANOVA were used (ANOVA was employed since the response variable was measured three times in the course of the follow-up period).
Ethical considerations
This study was approved by the Ethics Committee of Shahid Beheshti University of medical sciences with the ethics code of IR.SBMU.PHARMACY.REC.1398.063. The study was registered at the Iranian Registry of Clinical Trials (https://www.irct.ir) with the IRCT ID: IRCT20190530043772N1. In addition, informed consent form was taken from all participants and confidentiality of information was assured.
Results
First, both control and intervention groups were assessed to indicate if they are matched; only, the number of marital years was significantly different between the two groups. Based on the results of independent t-test, no significant difference was observed in the mean age of the two groups (P = 0.5). According to the Fisher's exact test, the participants in both intervention and control groups were almost matched in terms of the educational status (P = 0.735), spouse educational status (P = 0.53), employment status of spouse (P = 0.421), number of children (P = 0.661), history of chronic disease (P = 0.198), and history of neurological and psychological diseases (P < 0.99). The results of Chi-square test indicated that the employment status (P = 0.808), family income sufficiency (P = 0.81), and incidence of emotional problems over the past 2 weeks (P = 0.192) had no significant differences between the two groups. None of the intervention or control groups' participants had a history of participating in emotional intelligence training courses.
Because of the significant difference in the number of marital years in the two groups, the effect of this variable was modified as a confounding variable in the repeated measures ANOVA model.
As shown in Table 1, the results of repeated measures ANOVA indicated that time had a different impact on the mean scores of marital satisfaction (P < 0.001), and as shown in Table 2, in the control group based on the results of independent t-test, the mean scores of marital satisfaction had no significant differences before, immediately after, and 1 month after the intervention (P = 0.895). However, in the intervention group, over time, the mean score of marital satisfaction increased (P = 0.001), and the difference between the groups was significant (P < 0.001) [Figure 1].
Table 1.
The effect of time on mean scores of study variables in women referring to community health centers
| Variable | Time | Group | Group × time | |||
|---|---|---|---|---|---|---|
| F | P* | F | P* | F | P* | |
| Marital satisfaction | 11.458 | 0.001 | 4.911 | 0.030 | 34.473 | <0.001 |
| SQOL | 5.698 | 0.020 | 14.702 | <0.001 | 55.776 | <0.001 |
| Psychological well-being | 7.652 | 0.007 | 5.499 | 0.022 | 39.492 | <0.001 |
*Using Two-way repeated measures ANOVA. SQOL=Sexual quality of life
Table 2.
Comparison of the mean scores±standard deviation of study variables in the participants of intervention and control groups before, immediately after, and 1 month after the intervention
| Group Time | Intervention group, mean±SD | P* Between three time points | Control group, mean±SD | P* Between three time points | P value between the groups** | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Before the intervention | Immediately after the intervention | 1 month after the intervention | Before the intervention | Immediately after the intervention | 1 month after the intervention | Before the intervention | Immediately after the intervention | 1 month after the intervention | |||
| Variables | |||||||||||
| Marital satisfaction | 12.46±3.66 | 12.94±3.40 | 15.11±2.05 | 0.001 | 11.74±3.84 | 11.97±3.36 | 12.03±3.61 | 0.895 | 0.428 | 0.233 | <0.001 |
| SQOL | 180.11±16.13 | 209.29±14.72 | 203.37±14.70 | <0.001 | 186.49±22.59 | 183.34±22.77 | 182.34±21.36 | 0.739 | 0.179 | <0.001 | <0.001 |
| Psychological well-being | 11.14±2.94 | 16.69±2.61 | 16.31±2.18 | <0.001 | 13.60±3.96 | 13.43±2.66 | 13.63±2.76 | 0.590 | 0.004 | <0.001 | <0.001 |
*Using one-way repeated measures ANOVA, **Using independent t-test. SD=Standard deviation, SQOL=Sexual quality of life
Figure 1.
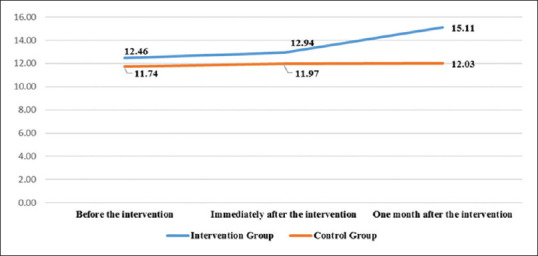
Comparison of the mean scores of marital satisfaction in the participants of intervention and control groups during the time
Furthermore, based on the results of repeated measures ANOVA, the impact of time on the mean scores of sexual quality of life has also been different (P = 0.020) [Table 1]. As shown in Table 2, the mean scores in the control group had no significant differences before, immediately after, and bypassing one month from the intervention (P = 0.739). However, over time, in the intervention group, the mean score of sexual quality of life first increased and then decreased (P < 0.001), where the difference between the two groups has been significant (P < 0.001) [Figure 2].
Figure 2.
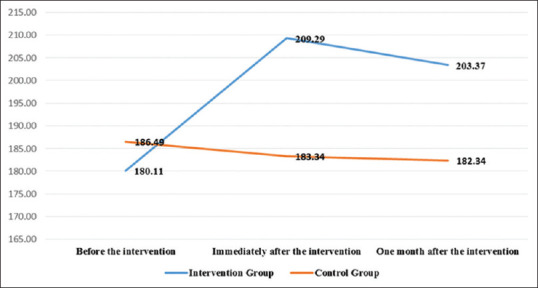
Comparison of the mean scores of sexual quality of life in the participants of intervention and control groups during the time
According to the results of repeated measures ANOVA, the influence of time on the mean scores of psychological well-being has been different (P = 0.007) [Table 1]; also, the mean scores of psychological well-being had no significant difference in the control group before, immediately after, and 1 month after the intervention (P = 0.590). However, in the intervention group, over time, the mean score of psychological well-being first increased and then decreased (P < 0.001), and the difference between the groups was significant (P < 0.001) [Table 2 and Figure 3].
Figure 3.
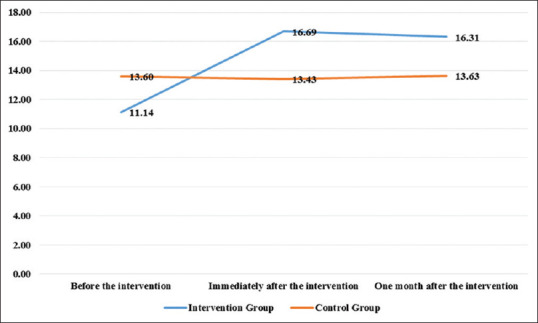
Comparison of the mean scores of psychological well-being in the participants of intervention and control groups during the time
Discussion
Based on the results of this study, emotional intelligence training resulted in enhanced marital satisfaction in women. These findings are in line with the results of a study by Jafaribalalmi et al. who examined the impact of skill-based emotional intelligence training program on the extent of marital satisfaction among university students. They stated that the scores of subjects' emotional intelligence and marital satisfaction increased after participation in the training program; thus, augmentation of emotional intelligence can be effective on enhancing the marital satisfaction.[31] The findings of this research are in agreement with the results of various studies.[19,32,33] In interpreting these results, it can be stated that those who are able to maintain their emotional intelligence at high levels and can well control their emotions and feelings are more fixable during sensitive and stressful situations. Accordingly, they refrain from any clash or row, thereby promoting their marital satisfaction. Emotional intelligence can support the development of stability and peace in marital life. In the individuals with a poor emotional intelligence, instability in the life (economic instability and cough financial conditions) can adversely affect the application of emotional intelligence skills, whereby they cannot use their normal emotional knowledge.[34] The results of the present research showed that before the intervention, the mean scores of sexual quality of life in the participants had no significant difference; however, immediately as well as 1 month after the intervention, the difference of means became significant and the sum of the scores increased. Previous research suggested that high sexual quality of life is one of the factors leading to enhanced marital satisfaction.[35,36] Willi and Buri for the first time evaluated the impact of emotional intelligence on sexual function and marital satisfaction. They concluded that emotional intelligence was effective in sexual satisfaction and sexual quality of life in women,[37] which is congruent with the results of the present study. It seems that training, diagnosis, and treatment of sexual disorders should be one of the components of screening and health-care programs, so that psychological disorders, impaired quality of life as well as interpersonal relations could be prevented.
The findings of the present research showed that before the intervention, the mean scores of psychological well-being of the two groups differed significantly; the mean score was lower in the intervention group compared to the control. However, immediately and 1 month after the intervention (in spite of reduction in the mean score), the difference of means was significant, where the mean score of psychological well-being was higher in the intervention group compared to the control group. Furthermore, Vicente-Galindo et al. reported similar results. They found that emotional intelligence can significantly affect the promotion of physical and psychological well-being of priests.[38] The results of other studies in this area are also congruent with ours.[39,40] Hence, it can be said that in the course of emotional intelligence training, the way psychological stress and tensions should be addressed as well as positive assessment of events and incidents are learned; in addition to reducing stress, through enhancing the general mood, it can cause positive changes in psychological well-being. Different studies suggest the fact that in today's societies, spouses have various problems to establish and maintain intimate relationships with each other and also to understand each other's feelings. Evidently, the current deficiencies in emotional competence of spouses alongside various other factors adversely affect their marital life. Satisfaction with the marital relationship is equal to personal satisfaction with the family and the life in general. In this regard, application of emotional skills, identifying one's own emotions and feelings, and the methods of properly regulating and expressing the emotions are among the most important issues in life skills.
Strengths and Limitations of the study
Investigating sexual quality of life through a specific and Iranian version of sexual quality of life questionnaire and determining the effect of emotional intelligence training program on marital satisfaction, sexual quality of life, and psychological well-being is considered as one of the strengths of the present study. Collecting information through self-reporting and affecting the mental states of the study participants was the limitation of this study.
Conclusions
According to this study, training emotional intelligence and its components are effective for enhancing the couples' marital satisfaction, sexual quality of life, and their psychological well-being. It should be noted that since one of the duties of nurses is educating, they can raise emotional intelligence by group counseling or classes, especially before marriage, to promote emotional intelligence, women's awareness, improve sexual relationships, and consequently increase sexual satisfaction and family health.
Practical suggestions
Based on the findings of the research, it is suggested that since the concept of emotional intelligence is acquired and can be learned, educational planners should pay more attention to this issue and deal with training emotional intelligence skills through mass media. Furthermore, since typically Iranian women feel ashamed of expressing their sexual problems and often neglect their sexual issues and needs, considering the importance of quality of marital relationships on psychological health, training workshops should be organized regarding the importance of expressing sexual problems, training marital relationship techniques, and sexual health. Furthermore, it is suggested that for couples with conflict referring to counseling centers, emotional intelligence training sessions and courses should be considered so that their marital satisfaction and adaptability would increase.
Financial support and sponsorship
This study was financially supported by the “Student Research Committee” and “Research and Technology Chancellor” in Shahid Beheshti University of Medical Sciences.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
This study is related to the project no. IR.SBMU.PHARMACY.REC.1398.063 from the Student Research Committee, Shahid Beheshti University of Medical Sciences, Tehran, Iran. We also appreciate the “Student Research Committee” and “Research and Technology Chancellor” in Shahid Beheshti University of Medical Sciences for their financial support of this study.
References
- 1.Javanmard GH, Garegozlo RM. The study of relationship between marital satisfaction and personality characteristics in Iranian families. Procedia Soc Behav Sci. 2013;84:396–9. [Google Scholar]
- 2.Taghizadeh M, Kalhori E. Relation between self esteem with marital satisfaction of employed women in Payam-e-Noor University. Mediterr J Soc Sci. 2015;6:41–5. [Google Scholar]
- 3.Ghofranipour F, Aminshokravi F, Torkashvand R. The relationship between demographic factors and marital satisfaction of couples intended to divorce referred to family Judicial Complex in Borujerd county. Iran J Health Educ Health Promot. 2017;5:43–50. [Google Scholar]
- 4.Zineldin M. TCS is to blame: The impact of divorce on physical and mental health. Int J Prev Med. 2019;10:141. doi: 10.4103/ijpvm.IJPVM_472_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.DeLongis A, Zwicker A. Marital satisfaction and divorce in couples in stepfamilies. Curr Opin Psychol. 2017;13:158–61. doi: 10.1016/j.copsyc.2016.11.003. [DOI] [PubMed] [Google Scholar]
- 6.Molaei M. Relationship between martial satisfaction and life style. Int J Humanit Cult Stud. 2016;Special Issue:874–84. [Google Scholar]
- 7.Gharibi M, Sanagouymoharer G, Yaghoubinia F. The relationship between quality of life with marital satisfaction in nurses in social security hospital in Zahedan. Glob J Health Sci. 2015;8:178–84. doi: 10.5539/gjhs.v8n2p178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nooripour R, ZadeMohammadi A, Dastras M, Sargolzai M. The effectiveness of life skills training on the enhancement of self-esteem and marital satisfaction among addicts in treatment period. Res Addict Q J Drug Abuse. 2014;8:31–9. [Google Scholar]
- 9.Aggarwal S, Kataria D, Prasad S. A comparative study of quality of life and marital satisfaction in patients with depression and their spouses. Asian J Psychiatr. 2017;30:65–70. doi: 10.1016/j.ajp.2017.08.003. [DOI] [PubMed] [Google Scholar]
- 10.Masoumi SZ, Garousian M, Khani S, Oliaei SR, Shayan A. Comparison of quality of life, sexual satisfaction and marital satisfaction between fertile and infertile couples. Int J Fertil Steril. 2016;10:290–6. doi: 10.22074/ijfs.2016.5045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gazibara T, Nurkovic S, Kovacevic N, Kurtagic I, Rancic B, Radovanovic S, et al. Factors associated with sexual quality of life among midlife women in Serbia. Qual Life Res. 2017;26:2793–804. doi: 10.1007/s11136-017-1608-3. [DOI] [PubMed] [Google Scholar]
- 12.Arrington R, Cofrancesco J, Wu AW. Questionnaires to measure sexual quality of life. Qual Life Res. 2004;13:1643–58. doi: 10.1007/s11136-004-7625-z. [DOI] [PubMed] [Google Scholar]
- 13.DeLamater J, Karraker A. Sexual functioning in older adults. Curr Psychiatry Rep. 2009;11:6–11. doi: 10.1007/s11920-009-0002-4. [DOI] [PubMed] [Google Scholar]
- 14.Cybulski M, Cybulski L, Krajewska-Kulak E, Orzechowska M, Cwalina U, Jasinski M. Sexual quality of life, sexual knowledge, and attitudes of older adults on the example of inhabitants over 60s of Bialystok, Poland. Front Psychol. 2018;9:483. doi: 10.3389/fpsyg.2018.00483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lee DM, Nazroo J, O'Connor DB, Blake M, Pendleton N. Sexual health and well-being among older men and women in England: Findings from the English longitudinal study of ageing. Arch Sex Behav. 2016;45:133–44. doi: 10.1007/s10508-014-0465-1. [DOI] [PubMed] [Google Scholar]
- 16.McSharry P, Timmins F. Promoting healthy lifestyle behaviours and well-being among nursing students. Nurs Stand. 2017;31:51–63. doi: 10.7748/ns.2017.e10588. [DOI] [PubMed] [Google Scholar]
- 17.Akhavan Tafti M, Mofradnezhad N. The relationship of emotional intelligence and social skills with psychological well-being in the elderly. Salmand Iran J Ageing. 2018;13:334–45. [Google Scholar]
- 18.Roth CG, Eldin KW, Padmanabhan V, Friedman EM. Twelve tips for the introduction of emotional intelligence in medical education. Med Teach. 2019;41:746–9. doi: 10.1080/0142159X.2018.1481499. [DOI] [PubMed] [Google Scholar]
- 19.Heidari M, Shahbazi S, Ghafourifard M, Ali Sheikhi R. Prediction of marital satisfaction based on emotional intelligence in postmenopausal women. J Menopausal Med. 2017;23:196–201. doi: 10.6118/jmm.2017.23.3.196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Goleman D. Emotional Intelligence. New York: Bantam Books; 1995. [Google Scholar]
- 21.Shirzad G. The role of the Myers-Briggs personality type and emotional intelligence in marital satisfaction among married female students at Tehran University. Glob J Health Sci. 2016;8:55516. doi: 10.5539/gjhs.v8n10p50. [DOI] [PubMed] [Google Scholar]
- 22.Silva P, Pereira H, Esgalhado G, Monteiro S, Afonso R, Loureiro M. Emotional intelligence, sexual functioning, and subjective sexual well-being in Portuguese adults. Br J Educ Soc Behav Sci. 2016;15:1–11. [Google Scholar]
- 23.Guerra-Bustamante J, León-Del-Barco B, Yuste-Tosina R, López-Ramos VM, Mendo-Lázaro S. Emotional intelligence and psychological well-being in adolescents. Int J Environ Res Public Health. 2019;16:1720. doi: 10.3390/ijerph16101720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Siavoshi H, Jahanian A, Abbasi Asl M, Mafakheri M. The relationships between emotional intelligence, sensation seek-ing, and marital satisfaction among female teachers. Soc Determ Health. 2016;2:148–54. [Google Scholar]
- 25.Omani-Samani R, Maroufizadeh S, Ghaheri A, Amini P, Navid B. Reliability and validity of the Kansas Marital Satisfaction Scale (KMSS) in infertile people. Middle East Fertil Soc J. 2018;23:154–7. [Google Scholar]
- 26.Arab Alidousti A, Nakhaee N, Khanjani N. Reliability and validity of the persian versions of the ENRICH Marital Satisfaction (Brief version) and Kansas Marital Satisfaction Scales. J Health Dev. 2015;4:158–67. [Google Scholar]
- 27.Maasoumi R, Lamyian M, Montazeri A, Azin SA, Aguilar-Vafaie ME, Hajizadeh E. The sexual quality of life-female (SQOL-F) questionnaire: Translation and psychometric properties of the Iranian version. Reprod Health. 2013;10:25. doi: 10.1186/1742-4755-10-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Masoumi R. Phd thesis. Iran: Tarbiat Modares University; 2014. Exploring the Concept of Female Quality of Sexual Life, Factors and Dimentions: Development and Psychometric Properties of a Cultural-Based Instrument. [Google Scholar]
- 29.Topp CW, Østergaard SD, Søndergaard S, Bech P. The WHO-5 Well-Being Index: A systematic review of the literature. Psychother Psychosom. 2015;84:167–76. doi: 10.1159/000376585. [DOI] [PubMed] [Google Scholar]
- 30.Dehshiri G, Mousavi S. An investigation into psychometric properties of persian version of World Health Organization Five Well-Being Index. J Clin Psychol. 2016;8:67–75. [Google Scholar]
- 31.Jafaribalalmi N, Khalilian A, Poghosyan R, Navabinezhad S. Effects of skill-based emotional intelligence training program on marital satisfaction in married students. J Mazandaran Univ Med Sci. 2016;25:329–34. [Google Scholar]
- 32.Kamel Abbasi AR, Tabatabaei SM, Aghamohammadiyan Sharbaf H, Karshki H. Relationship of attachment styles and emotional intelligence with marital satisfaction. Iran J Psychiatry Behav Sci. 2016;10:e2778. doi: 10.17795/ijpbs-2778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Eslami AA, Hasanzadeh A, Jamshidi F. The relationship between emotional intelligence health and marital satisfaction: A comparative study. J Educ Health Promot. 2014;3:24. doi: 10.4103/2277-9531.127616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Nasiri Zarch Z, Marashi SM, Raji H. The relationship between emotional intelligence and marital satisfaction: 10-year outcome of partners from three different economic levels. Iran J Psychiatry. 2014;9:188–96. [PMC free article] [PubMed] [Google Scholar]
- 35.Tayfun D, Tugut N, Golbasi Z. The relationship between sexual quality of life, happiness, and satisfaction with life in married Turkish women. Sex Disabil. 2013;31:239–47. [Google Scholar]
- 36.Kisa S, Zeyneloǧlu S, Yilmaz D, Güner T. Quality of sexual life and its effect on marital adjustment of Turkish women in pregnancy. J Sex Marital Ther. 2014;40:309–22. doi: 10.1080/0092623X.2012.751071. [DOI] [PubMed] [Google Scholar]
- 37.Willi J, Burri A. Emotional Intelligence and sexual functioning in a sample of Swiss men and women. J Sex Med. 2015;12:2051–60. doi: 10.1111/jsm.12990. [DOI] [PubMed] [Google Scholar]
- 38.Vicente-Galindo MP, López-Herrera H, Pedrosa I, Suárez-Álvarez J, Galindo-Villardón MP, García-Cueto E. Estimating the effect of emotional intelligence in wellbeing among priests. Int J Clin Health Psychol. 2017;17:46–55. doi: 10.1016/j.ijchp.2016.10.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Ju C, Lan J, Li Y, Feng W, You X. The mediating role of workplace social support on the relationship between trait emotional intelligence and teacher burnout. Teach Teacher Educ. 2015;51:58–67. [Google Scholar]
- 40.Sharif F, Rezaie S, Keshavarzi S, Mansoori P, Ghadakpoor S. Teaching emotional intelligence to intensive care unit nurses and their general health: A randomized clinical trial. Int J Occup Environ Med. 2013;4:141–8. [PubMed] [Google Scholar]