

Abstract
BACKGROUND AND AIM:
Measuring child abuse and adverse experiences is a critical task with regard to its long-term impact on the health of individuals and communities. The purpose of this study was to validate the Persian version of the International Adverse Childhood Experiences Abuse Short Form (ACE-ASF) in Iranian society.
MATERIALS AND METHODS:
This cross-sectional study was conducted in Kerman, southeast of Iran, in 2019, on 494 students from Kerman University of Medical Sciences, selected by convenience sampling method. Psychometric properties of the questionnaire were examined after the forward and backward translation processes. The factor structure of the questionnaire was evaluated using exploratory factor analysis (EFA) and confirmatory factor analysis (CFA). The concurrent validity of the questionnaire was assessed using the childhood trauma questionnaire (CTQ). Cronbach's alpha and corrected item-total correlation were used to measure reliability.
RESULTS:
The mean age of participants was 24.3 ± 5.3 years. Based on EFA, two physical–emotional abuse and sexual abuse factors were obtained. The CFA fit indices well supported two extracted factors. The CFA showed acceptable factor loadings. The internal consistency coefficient of Cronbach's alpha was 0.75 for the physical–emotional abuse factor and 0.77 for the sexual abuse factor. The correlation coefficient of ACE-ASF and CTQ was r = 0.56. The reliability index of intraclass correlation coefficient was 0.73 (95% confidence interval: 0.60–0.84).
CONCLUSION:
The Persian version of the ACE-ASF questionnaire has acceptable psychometric properties.
Keywords: Adverse childhood experiences, child abuse, child maltreatment, Iran, psychometrics
Introduction
Child abuse is a serious global health concern. Child maltreatment involves all physical, emotional, sexual, or negligent abuses, which can lead to potential damage to the health of children.[1] Physical abuse means harming the health, survival, growth, and prosperity of the child using physical force. Emotional abuse means that the child has not had a suitable supportive environment, such as verbal threats. Child sexual abuse is defined as the involvement of a child in sexual activity in which he/she does not understand and is unable to give informed consent. Failure to provide various aspects of child welfare can be attributed to neglect of the child.[2]
Child maltreatment has important implications for general health. Various evidence shows that maltreatment and psychosocial stress during growth are the determinants of illness and disability in adulthood.[3,4] Observations in many high-income countries and low- and middle-income countries show that the effects of adverse childhood experiences (ACE) have been linked with health, mental, and even functional problems in adulthood.[5]
Problems such as mental disorders; suicide attempts; high-risk behaviors such as smoking, alcohol consumption, and drug abuse; and high-risk sexual behaviors were found to be related to child maltreatment.[6,7,8,9,10] Other consequences such as reduced adult academic performance, reduced cognitive function, and increased risk for some noncommunicable diseases such as cardiovascular disease,[3,5,11,12] cancer,[3,13,14,15] chronic lung disease, skeletal fractures, and liver disease[3] were associated with ACE.
Such effects highlight the need to a valid tool for measuring adverse experiences and maltreatments in early age. There are a variety of tools to measure ACE and child maltreatment, one of which is the ACE abuse short form (ACE-ASF), which is part of the ACE International Questionnaire (ACE-IQ). The World Health Organization (WHO) developed this 43-item questionnaire to measure ACE in different cultures and countries.[16] This questionnaire examines a range of sources of childhood stress, including household disruption, physical, sexual, and emotional abuse and neglect by parents or caregivers; peer violence; witnessing community violence; and exposure to collective violence, designed for people aged 18 years or over.[16]
The ACE-ASF questionnaire has been validated around the world. It has been used in countries such as Iraq, Saudi Arabia, Kenya, Vietnam, Nigeria, Germany, Romania, China, and Malawi.[17,18,19,20,21,22,23,24,25,26] Despite its rapid and wide use in different parts of the world, there is no evidence regarding its psychometric properties in Iran. Also, given that childhood abuse can lead to psychological problems for young people. We decided to validate ACE-ASF questionnaire based on Iranian culture to make it accessible to experts in the field.
Therefore, in this study, we investigated the psychometric properties of the three types of abuse (physical, emotional, and sexual) using the ACE-ASF questionnaire. This questionnaire was selected due to the importance of the child abuse in the ACEs, the short form and the ease of response of the participants, as well as the experiences of some similar validation studies.[26] The objectives of this research were (1) forward and backward translation of the ACE-ASF questionnaire in Persian and (2) validation of the ACE-ASF questionnaire[26] in an appropriate sample of Iranian youth regarding the content, sensitivity, and criticality of the questions.
Materials and Methods
This cross-sectional study was conducted in Kerman, southeast of Iran, in 2019, on 494 students from Kerman University of Medical Sciences, selected by nonprobability convenience sampling (availability sampling) method. The data were collected with full and voluntary consent of individuals.
The collected data were used anonymously and the sealed ballot box method was applied to ensure confidentiality of the participants' information.
Age over 18 years and the consent of participants to complete the questionnaire were considered as the inclusion criteria. The response rate was 97.1%, and 14 cases were excluded due to failure to complete the questionnaire. Finally, 480 participants who filled out the questionnaires completely were enrolled into the study.
Measurement tool
The first part of the measurement tool consisted of demographic characteristics such as gender, birth year, educational level, occupation, and marital status. The second part included the ACE-ASF. This section includes physical, emotional, and sexual abuse items.
Physical abuse
Physical abuse was evaluated using the following two questions: “ Did a parent, guardian, or other household member spank, slap, kick, punch, or beat you up?” and “Did a parent, guardian, or other household member hit or cut you with objects, such as a stick (or cane), bottle, club, knife, and whip?”
Emotional abuse
Emotional abuse was assessed using the following two questions: “Did a parent, guardian, or other household member yell, scream, or swear at you, insult or humiliate you?” and “ Did a parent, guardian, or other household member threaten to, or actually, abandon you, or throw you out of the house?”
Sexual abuse
This area was evaluated using the following four questions: “Did someone touch or fondle you in a sexual way when you did not want them to?”, “Did someone make you touch their body in a sexual way when you did not want them to?”, “Did someone attempt oral, anal, or vaginal intercourse with you when you did not want them to?”, and “Did someone actually have oral, anal, or vaginal intercourse with you when you did not want them to?”. The options for answering the eight questions above have been many times, a few times, once, never, and refused.
Childhood trauma questionnaire
The childhood trauma questionnaire (CTQ) introduced by Bernstein et al. in 1994 was used to evaluate concurrent validity.[27] This questionnaire was validated in Iran in 2009 and has been used in several studies.[28] The questionnaire has 28 questions and covers five subscales of emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect. Because this questionnaire, like our study questionnaire, evaluates the child maltreatment, it is expected to observe a direct and positive relationship between the scores derived from these two tools. This indicates the proper validity of the target questionnaire.
Translation process
First, a written permission was obtained from the WHO to begin validating the questionnaire, and then the validation began under the WHO protocol.[29] In this study, we emphasized on issues such as the short form of the questionnaire, sense-for-sense translation rather than literal translation, and the appropriateness of the translation with the culture of the destination country according to the WHO protocol.[29]
Subsequently, a person whose mother tongue was Persian and had sufficient English proficiency translated the questionnaire from English to Persian. Afterward, according to the WHO validation guidelines, several experts were asked to comment on the questions. According to the expert panel comments, some words were deleted, simplified, or replaced. Words such as oral, anal, and vaginal sex were found to be very sensitive to Iranian culture and were eliminated. Then, another independent person was asked to translate the questionnaire, which was fluent in the main language and had no information about the questionnaire. The two English versions were compared and the panel confirmed their equivalency. After that, the cognitive analysis of the questionnaire was carried out.[29] The objective of this step was to see whether the audience was aware of the concept and purpose of the questions? And is it necessary to change the wording, vocabulary, and terminology? For this purpose, 16 poorly and highly educated people of different ages were asked to review once the questionnaire. Based on their views, minor changes were made to facilitate the transmission of questions to the audience more clearly.
Known group comparison
Using the Known-Group Comparison[30] approach, two questions of “Have you considered seriously committing suicide over the past 12 months?” and “Totally, how do you assess your general health?” were used to evaluate construct validity. This method is a way to find out the construct validity of the questionnaire using known groups.
The question of “Totally, how do you evaluate your general health?” had the options of very good, good, fairly good, bad, and very bad. In the analysis, the options of good and very good as well as bad and very bad were merged, and finally three options of good, fairly good, and bad were considered.[26]
To find out the convergent validity of the questionnaire, the relationship between ACE-ASF and CTQ questionnaires was evaluated using Pearson's correlation coefficient.[31] The degree of correlation between the scores of these two questionnaires shows the evidence of their similarity. The amplitude of this correlation coefficient is ±1, so that +1 and −1 show the strongest direct and reverse correlations, respectively, and zero indicates a lack of linear correlation.
Statistical analysis
In this study, exploratory factor analysis (EFA) was used initially to explore the main factor structure of the questionnaire (ACE-IQ). A principal component analysis (PCA) with direct oblimin rotation was performed on the 8 items in the questionnaire. Then, confirmatory factor analysis (CFA) was done using the maximum likelihood method. After that, four indices were applied to determine the fitting of the model,[32] including the χ2/df ratio, the root mean square error approximation (RMSEA), the comparative fit index (CFI), and the Tucker–Lewis Index (TLI).
The ACE-ASF questionnaire was evaluated for reliability and validity as follows. To determine the reliability and homogeneity of the items used in this questionnaire, Cronbach's alpha was used as the internal consistency coefficient and intraclass correlation coefficient (ICC). The data were analyzed using SPSS software version 19 (Licensed Materials-property of SPSS, Inc., an IBM company © copyright 1989, 2010 SPSS, Inc., an IBM company. Java and all Java-based trademarks and logos of trademarks of Sun Microsystems, Inc.in the United States, other contries, or both.) and AMOS software version 5.0.
Ethics approval
In this research, verbal consent was obtained from individuals before entering into the study. The Ethics Committee of Kerman University of Medical Sciences (Approval No. IR.KMU.REC.1397.338) approved this study. Consent was obtained from the inventors of the questionnaire via E-mail.
Results
Sociodemographic characteristics
In this study, 480 students with a mean age of 24.3 ± 5.3 years were included. This batch encompassed 70% females. In addition, 78.4% of participants were single.
Translation
Finally, the questions were changed as follows and were made available to the audience.
”Have your parents, guardians, or other members of your family ever slapped, kicked, unched, or beaten you up?”
”Have your parents, guardians, or other members of your family ever injured you with objects such as stick, club, bottle, belt, or stuff like that?”
”Have your parents, guardians, or other members of your family ever yelled at you or shouted abuse at you?”
”Have your parents, guardians, or other members of your family ever threatened not to let you in home or actually thrown you out of the house?”
”Has anyone ever touched you or fondled you sexually despite your will?”
”Has anyone ever made you touch their body in a sexual way despite your will?”
”Has anyone ever tried to have sexual intercourse with you despite your will?”
”Has anyone ever had sexual intercourse with you despite your will?”
Exploratory factor analysis
The values of Kaiser–Meyer–Olkin (KMO) = 0.78 and Bartlett's test were also significant (P < 0.001). Finally, a model with two factors was selected as the best fit of the model. These two factors accounted for 61.5% of the total variance.
The first factor included the questions related to physical–emotional abuse, and the second factor involved the items related to sexual abuse. The structure of the extracted factors from the relationship between factor loadings and questions using the PCA method and the oblimin rotation is shown in Table 1. All factor loadings of the two factors were high. The factor loadings of physical–emotional abuse factor were between 0.716 and 0.866 and the factor loadings of sexual abuse factor varied from 0.696 to 0.876.
Table 1.
Extracted factors structure using the principal components method and oblimin ratio
| Items | Factors | |
|---|---|---|
| Physical-emotional abuse | Sexual abuse | |
| Q24: Have your parents, guardians, or other members of your family ever slapped, kicked, punched, or beaten you up? | 0.738 | |
| Q25: Have your parents, guardians, or other members of your family ever injured you with objects such as stick, club, bottle, belt, or stuff like that? | 0.716 | |
| Q26: Have your parents, guardians, or other members of your family ever yelled at you or shouted abuse at you? | 0.866 | |
| Q27: Have your parents, guardians, or other members of your family ever threatened not to let you in home or actually thrown you out of the house? | 0.781 | |
| Q28: Has anyone ever touched you or fondled you sexually despite your will? | 0.696 | |
| Q29: Has anyone ever made you touch their body in a sexual way despite your will? | 0.876 | |
| Q30: Has anyone ever tried to have sexual intercourse with you despite your will? | 0.825 | |
| Q31: Has anyone ever had sexual intercourse with you despite your will? | 0.722 | |
Each of the physical–emotional abuse and sexual abuse factors included four questions. The first factor examined physical–emotional abuse from respondents' point of view, which included questions 24, 25, 26, and 27. The second factor was related to sexual abuse, which covered questions 28, 29, 30, and 31.
Confirmatory factor analysis
The CFA was performed based on the two-factor model known by the EFA. These findings suggest that this model is well fitted. The RMSEA index was 0.06 (90% confidence interval [CI] = 0.04–0.08) and <0.1, which indicates that the mean square error of the model is appropriate and acceptable. Also, the value of χ2/df = 2.7 <5 and the values of the CFI, goodness of fit index and Incremental fit index 0.97 were obtained. Standardized loadings of indexes on latent variables were above 0.59. Graph of factors and factor loadings is shown in Figure 1.
Figure 1.
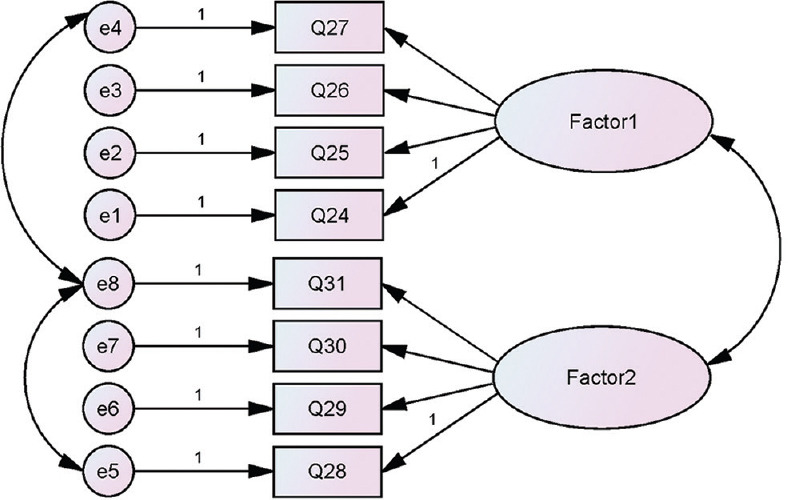
Diagram of the two factors and factor loadings model by confirmatory factor analysis
Internal consistency
The internal consistency coefficient of Cronbach's alpha was 0.75 for the physical–emotional abuse factor and 0.77 for the sexual abuse factor [Table 2].
Table 2.
Corrected item-scale correlations and Cronbach’s alpha values if item deleted
| Item | Item-scale correlation | Cronbach’s alpha if item deleted |
|---|---|---|
| Factor physical-emotional abuse | ||
| Q1 | 0.52 | 0.75 |
| Q2 | 0.53 | 0.71 |
| Q3 | 0.68 | 0.61 |
| Q4 | 0.59 | 0.69 |
| Factor sexual abuse | ||
| Q5 | 0.51 | 0.76 |
| Q6 | 0.69 | 0.66 |
| Q7 | 0.62 | 0.69 |
| Q8 | 0.54 | 0.74 |
Concurrent criterion validity
Pearson's correlation coefficient was obtained between the ACE-ASF and CTQ questionnaires (r = 0.56). Furthermore, the Pearson's correlation coefficient between ACE-ASF and the questions of “Have you considered seriously committing suicide over the past 12 months” and “Totally, how do you assess your general health?” was positive and was obtained to be 0.24 and 0.19, respectively (P < 0.001).
The test–retest reliability coefficient was also evaluated by ICC and the value of this index was 0.73 (95% CI = 0.60–0.84).
Discussion
This study provides a comprehensive analysis of the psychometric properties of the ACE-ASF in Iranian context. It is the first study to translate and evaluate the factorial structure, internal consistency, and criterion validity of the ACE-ASF. Analyses revealed a two-factor structure with physical/emotional abuse and sexual abuse dimensions, adequate internal consistency, and criterion validity.
Several studies validated the ACE-ASF questionnaire and its international version. A study[26] examined the psychometric properties of the ACE-ASF questionnaire (8 out of 11 questions) in a 15-year-old population of Romania. A study in Malawi validated the ACE-ASF questionnaire among adolescents aged 10–16 years.[24] Individuals aged 18 years or over were enrolled in our study, and there was a possibility of recall bias, while studies in Romania and Malawi were conducted among young people and the probability of recall bias was decreased. Similar to our study, other researches also included adults in their sample. A study in China also evaluated the ACE-IQ among students aged 18–24 years.[25] The psychometric properties of the ACE scale were also studied in Nigeria. The validation process of 43-item ACE-IQ in Nigeria[22] was conducted among a number of prisoners, which seems to be less representative of the general population compared to our study on the student population. It seems that sample selection from prisoners leads to a kind of selection bias. In a study by Ford et al.[33] in the US, a representative sample of the general population was included in the study of psychometric properties of ACE-ASF.
In this study, the values of KMO index and Bartlett's test were found to be appropriate and significant using the EFA results. Hence, the sample size collected was sufficient for the factor analysis, and the factor analysis was quite appropriate for these data. Finally, two dimensions of physical–emotional abuse and sexual abuse were extracted. The CFA was used to find the best model, which was an acceptable model based on the findings, including χ2/df ≥3, CFI and TLI of more than 0.95, and RMSEA index between 0.00 and 0.06 with a CI of 0.00–0.08.[34]
In line with our research, Meinck et al. in Romania categorized the physical–emotional abuse in a dimension and the sexual abuse in another dimension in the process of measuring the psychometric properties of ACE-ASF.[26] Kidman et al. in Malawi extracted three dimensions of neglect, abuse, and household disruption during ACE-IQ validation.[25] Ford et al. extracted three dimensions of physical–emotional abuse, sexual abuse, and then household physical violence in evaluating the ACE questionnaire, which resulted in physical–emotional abuse and sexual abuse in two separate dimensions, similar to our study.[33]
The results of the present study demonstrated that the reliability of the Persian version of the ACE-ASF questionnaire was reasonable and acceptable based on two methods of Cronbach's alpha and ICC, so that the Cronbach's alpha coefficient was 0.77 in the subscale of sexual abuse and 0.75 in the subscale of physical–emotional abuse. The ICC was also 0.73; the range of more than 0.6 indicates a good agreement based on documentation.[35]
According to a study by Ho et al. among the Chinese youth, the ICC for the ACE-IQ was generally good (0.9). They also examined the ICC value for three subscales of neglect, abuse, and household disruption and reported community violence in the range of 0.78–0.9.[25] In the study by Kazeem in Nigeria on the ACE-IQ questionnaire, Cronbach's alpha coefficient was 0.8, indicating an appropriate internal consistency.[22] Ford et al. also observed an appropriate internal consistency in the ACE questionnaire and the subscales of physical–emotional abuse and sexual abuse.[33] Wingenfeld et al. in Germany also confirmed the internal consistency appropriate for the 10-item ACE questionnaire,[23] while poor internal consistency was observed in the physical–emotional abuse subscale in the study conducted by Meinck et al., and the sexual abuse subscale and the ACE-ASF questionnaire generally had a good internal consistency.[26]
In the current study, the ACE-ASF had an acceptable concurrent validity in relation to the CTQ questionnaire. The overall correlation between ACE-IQ and CTQ was positive. As previously explained, the psychometric properties of the CTQ questionnaire were reviewed to evaluate the CTQ questionnaire in Iran in 2009. Therefore, the existence of a positive correlation between ACE-IQ and CTQ can indicate an acceptable concurrent validity for ACE-ASF. In confirming the results of this study, Kazeem in Nigeria also reported a significant correlation for the total score of ACE-IQ and its subscales with CTQ.[22] Wingenfeld et al. also observed a very high correlation between CTQ and ACE, while there was a low-to-moderate correlation between the total ACE score and depression, anxiety, and physical symptoms.[23] Ford et al. in the United States did not study construct validity,[33] and Meinck et al. did not collect more information about childhood trauma.[26]
Limitations
First, this research focused on the dimensions of child abuse. Hence, only part of the ACE-IQ questionnaire has been validated in relation to solely measures of abuse. Second, this study was conducted in the student population of Kerman University of Medical Sciences; therefore, further caution should be taken in generalizing the results to the whole population.
Conclusion
The Persian version of the ACE-ASF questionnaire has acceptable psychometric properties. It is a valid tool and appropriate with cultural context in Iran for measuring physical, emotional, and sexual abuse.
Financial support and sponsorship
This research is supported by Kerman University of Medical Sciences (Grant Reference Number 97000283).
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The authors extend their appreciation to the participants for their cooperation throughout the study. They also appreciate the assistance of Kerman University of Medical Sciences.
References
- 1.Cook A, Spinazzola J, Ford J, Lanktree C, Blaustein M, Cloitre M, et al. Complex trauma in children and adolescents. Psychiatr Ann. 2017;35:390–8. [Google Scholar]
- 2.Norman RE, Byambaa M, De R, Butchart A, Scott J, Vos T. The long-term health consequences of child physical abuse, emotional abuse, and neglect: A systematic review and meta-analysis. PLoS Med. 2012;9:e1001349. doi: 10.1371/journal.pmed.1001349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, et al. Reprint of: Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The adverse childhood experiences (ACE) study. Am J Prev Med. 2019;56:774–86. doi: 10.1016/j.amepre.2019.04.001. [DOI] [PubMed] [Google Scholar]
- 4.Gilbert LK, Breiding MJ, Merrick MT, Thompson WW, Ford DC, Dhingra SS, et al. Childhood adversity and adult chronic disease: An update from ten states and the district of Columbia, 2010. Am J Prev Med. 2015;48:345–9. doi: 10.1016/j.amepre.2014.09.006. [DOI] [PubMed] [Google Scholar]
- 5.Hughes K, Bellis MA, Hardcastle KA, Sethi D, Butchart A, Mikton C, et al. The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. Lancet Public Health. 2017;2:e356–66. doi: 10.1016/S2468-2667(17)30118-4. [DOI] [PubMed] [Google Scholar]
- 6.Turner S, Taillieu T, Carleton RN, Sareen J, Afifi TO. Association between a history of child abuse and suicidal ideation, plans and attempts among Canadian public safety personnel: A cross-sectional survey. CMAJ Open. 2018;6:E463–70. doi: 10.9778/cmajo.20170153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.O'Mahen HA, Karl A, Moberly N, Fedock G. The association between childhood maltreatment and emotion regulation: Two different mechanisms contributing to depression? J Affect Disord. 2015;174:287–95. doi: 10.1016/j.jad.2014.11.028. [DOI] [PubMed] [Google Scholar]
- 8.Shin SH, Miller DP, Teicher MH. Exposure to childhood neglect and physical abuse and developmental trajectories of heavy episodic drinking from early adolescence into young adulthood. Drug Alcohol Depend. 2013;127:31–8. doi: 10.1016/j.drugalcdep.2012.06.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Campbell JA, Walker RJ, Egede LE. Associations between adverse childhood experiences, high-risk behaviors, and morbidity in adulthood. Am J Prev Med. 2016;50:344–52. doi: 10.1016/j.amepre.2015.07.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Thompson R, Lewis T, Neilson EC, English DJ, Litrownik AJ, Margolis B, et al. Child maltreatment and risky sexual behavior: Indirect effects through trauma symptoms and substance use. Child Maltreat. 2017;22:69–78. doi: 10.1177/1077559516674595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Pretty C, O'Leary DD, Cairney J, Wade TJ. Adverse childhood experiences and the cardiovascular health of children: A cross-sectional study. BMC Pediatr. 2013;13:208. doi: 10.1186/1471-2431-13-208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Su S, Jimenez MP, Roberts CT, Loucks EB. The role of adverse childhood experiences in cardiovascular disease risk: A review with emphasis on plausible mechanisms. Curr Cardiol Rep. 2015;17:88. doi: 10.1007/s11886-015-0645-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Brown DW, Anda RF, Felitti VJ, Edwards VJ, Malarcher AM, Croft JB, et al. Adverse childhood experiences are associated with the risk of lung cancer: A prospective cohort study. BMC Public Health. 2010;10:20. doi: 10.1186/1471-2458-10-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Brown MJ, Thacker LR, Cohen SA. Association between adverse childhood experiences and diagnosis of cancer. PLoS One. 2013;8:e65524. doi: 10.1371/journal.pone.0065524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kelly-Irving M, Mabile L, Grosclaude P, Lang T, Delpierre C. The embodiment of adverse childhood experiences and cancer development: Potential biological mechanisms and pathways across the life course. Int J Public Health. 2013;58:3–11. doi: 10.1007/s00038-012-0370-0. [DOI] [PubMed] [Google Scholar]
- 16.World Health Organization. Adverse Childhood Experiences International Questionnaire (ACE-IQ) World Health Organization; 2018. [Last accessed on 2020 Feb 21]. Available from: http://www.who.int/violence_injury_preve ntion/violence/activities/adverse_childhood_expe riences/en/ [Google Scholar]
- 17.Goodman ML, Martinez K, Keiser PH, Gitari S, Seidel SE. Why do Kenyan children live on the streets. Evidence from a cross-section of semi-rural maternal caregivers? Child Abuse Negl. 2017;63:51–60. doi: 10.1016/j.chiabu.2016.10.018. [DOI] [PubMed] [Google Scholar]
- 18.Soares AL, Howe LD, Matijasevich A, Wehrmeister FC, Menezes AM, Gonçalves H. Adverse childhood experiences: Prevalence and related factors in adolescents of a Brazilian birth cohort. Child Abuse Negl. 2016;51:21–30. doi: 10.1016/j.chiabu.2015.11.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Almuneef M, Qayad M, Aleissa M, Albuhairan F. Adverse childhood experiences, chronic diseases, and risky health behaviors in Saudi Arabian adults: A pilot study. Child Abuse Negl. 2014;38:1787–93. doi: 10.1016/j.chiabu.2014.06.003. [DOI] [PubMed] [Google Scholar]
- 20.Al-Shawi AF, Lafta RK. Effect of adverse childhood experiences on physical health in adulthood: Results of a study conducted in Baghdad city. J Family Community Med. 2015;22:78–84. doi: 10.4103/2230-8229.155374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Tran QA, Dunne MP, Vo TV, Luu NH. Adverse childhood experiences and the health of university students in eight provinces of Vietnam. Asia Pac J Public Health. 2015;27:26S–32S. doi: 10.1177/1010539515589812. [DOI] [PubMed] [Google Scholar]
- 22.Kazeem OT. A validation of the adverse childhood experiences scale in Nigeria. Res Humanit Soc Sci. 2015;5:18–23. [Google Scholar]
- 23.Wingenfeld K, Schäfer I, Terfehr K, Grabski H, Driessen M, Grabe H, et al. The reliable, valid and economic assessment of early traumatization:First psychometric characteristics of the German version of the adverse childhood experiences questionnaire (ACE) Psychother Psychosom Med Psychol. 2011;61:e10–4. doi: 10.1055/s-0030-1263161. [DOI] [PubMed] [Google Scholar]
- 24.Kidman R, Smith D, Piccolo LR, Kohler HP. Psychometric evaluation of the adverse childhood experience international questionnaire (ACE-IQ) in Malawian adolescents. Child Abuse Negl. 2019;92:139–45. doi: 10.1016/j.chiabu.2019.03.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ho GW, Chan AC, Chien WT, Bressington DT, Karatzias T. Examining patterns of adversity in Chinese young adults using the adverse childhood experiences-international questionnaire (ACE-IQ) Child Abuse Negl. 2019;88:179–88. doi: 10.1016/j.chiabu.2018.11.009. [DOI] [PubMed] [Google Scholar]
- 26.Meinck F, Cosma AP, Mikton C, Baban A. Psychometric properties of the adverse childhood experiences abuse short form (ACE-ASF) among Romanian high school students. Child Abuse Negl. 2017;72:326–37. doi: 10.1016/j.chiabu.2017.08.016. [DOI] [PubMed] [Google Scholar]
- 27.Bernstein DP, Fink L, Handelsman L, Foote J, Lovejoy M, Wenzel K, et al. Initial reliability and validity of a new retrospective measure of child abuse and neglect. Am J Psychiatry. 1994;151:1132–6. doi: 10.1176/ajp.151.8.1132. [DOI] [PubMed] [Google Scholar]
- 28.Garrusi B, Nakhaee N. Validity and reliability of a Persian version of the Childhood Trauma Questionnaire. Psychol Rep. 2009;104:509–16. doi: 10.2466/PR0.104.2.509-516. [DOI] [PubMed] [Google Scholar]
- 29.World Health Organization. 2018. [Last accessed on 2020 Feb 21]. Available from: http://www.who.int/substance_abuse/research_tools/translation .
- 30.Hattie J, Cooksey RW. Procedures for assessing the validities of tests using the “known-groups” method. Appl Psychol Meas. 1984;8:295–305. [Google Scholar]
- 31.Heale R, Twycross A. Validity and reliability in quantitative studies. Evid Based Nurs. 2015;18:66–7. doi: 10.1136/eb-2015-102129. [DOI] [PubMed] [Google Scholar]
- 32.Schreiber JB, Nora A, Stage FK, Barlow EA, King J. Reporting structural equation modeling and confirmatory factor analysis results: A review. J Educ Res. 2006;99:323–38. [Google Scholar]
- 33.Ford DC, Merrick MT, Parks SE, Breiding MJ, Gilbert LK, Edwards VJ, et al. Examination of the factorial structure of adverse childhood experiences and recommendations for three subscale scores. Psychol Violence. 2014;4:432–44. doi: 10.1037/a0037723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct Equ Modeling. 1999;6:1–55. [Google Scholar]
- 35.Fleiss JL, Levin B, Paik MC. Statistical Methods for Rates and Proportions. Vol. 2. John Wiley & Sons, Inc; 1981. The measurement of interrater agreement; pp. 22–3. [Google Scholar]