

Abstract
Background:
Functional status assessment may help estimate which patients age ≥85 will benefit from surgical treatment for keratinocyte carcinoma (KC) but predictive value for short-term survival in this population has not been determined.
Objective:
To assess predictive value of functional status for short-term survival in those ≥ age 85 with KC.
Methods:
Retrospective cohort review of 238 patients ≥age 85 presenting for KC management between 2010–2015. Functional status was assessed with the Karnofsky Performance Scale (KPS) and Katz Activities of Daily Living (ADL) index. Overall survival was determined.
Results:
Lower functional status scores of KPS ≤40 and Katz ADL ≤4 were associated with 37% and 53% survival at 2 years, respectively.
Limitations:
Retrospective design and single center study.
Conclusion:
In this study, KPS and Katz ADL predicted short-term survival. Patients with low functional status scores had significantly decreased survival at 2 years, with double the death rate of patients with high functional status. Functional status should be considered during shared decision-making for elderly individuals seeking KC treatment.
Keywords: geriatrics, functional assessment, keratinocyte carcinoma, oncology
Introduction:
The incidence of Keratinocyte Carcinoma (KC) has increased by 35% between 2006 and 2012, with the largest increase in rates among the Medicare fee-for-service population in the United States.1 Given that those aged 85 years and older represent the fastest growing segment of the US population with a projected growth from 5.9 million in 2012 to 8.9 million in 2030,2 the incidence rates and treatment of KC in the very elderly (defined as age of ≥85 years) are also expected to increase.
There is debate regarding the appropriate management of KC in the very elderly, given that the majority of KC are nonfatal, asymptomatic, and demonstrate indolent growth. While some have proposed age as a relative contraindication to surgical treatment of KC due to limited life expectancy,3–5 others have demonstrated relatively prolonged survival in the very elderly and low morbidity with surgical treatment for KC.6–9 With the expected increase in the very elderly seeking KC care, a key issue will be assessing who will benefit from treatment of KC, and determining the most appropriate treatment approach for each patient 6,10–14. Given the limited life expectancy of the very elderly, assessing patient factors that contribute to short-term survival can assist clinicians in choosing the best treatment option for patients presenting with KC. To help estimate these factors, the evaluation of functional status has been proposed.4,6,11 The Karnofsky Performance Scale (KPS) and Katz Activities of Daily Living (ADL) are two validated indices used in geriatric populations to assess overall health, and have been shown to be predictive of survival in older adults.15,16 However, the role of indices such as the KPS and Katz ADL to assess functional status and predict short-term survival has not been explored in this population.
To assess overall health and survival in the very elderly with KC seeking treatment, the objectives of this study were: 1) to describe functional status in patients 85 years and older presenting for management of KC and 2) to assess the predictive value of functional status measures for short-term survival in this specific population using the KPS and Katz ADL.
Methods:
Design, setting and study population
This was a single-center retrospective cohort study of patients age ≥ 85 years who presented for skin cancer management to Dermatology at a tertiary cancer center between 2010–2015. Patients who were diagnosed with basal cell carcinoma (BCC) or cutaneous squamous cell carcinoma (SCC) and completed an ambulatory health assessment including functional status measures were included. Patient charts were reviewed for clinical and functional status metrics. Clinical data extracted included patient demographics, tumor characteristics, treatment details, follow-up and survival.
Treatment types were categorized as the following: (1) Mohs Micrographic Surgery (MMS) (2) Surgical Excision (3) Non-surgical (electrodessication and curettage, cryotherapy, topical therapy, photodynamic therapy (PDT), intralesional therapy, radiation) (4) Observation/Referral (5) Other (e.g. treated elsewhere). To assess survival, the last follow-up with a dermatologist at our institution and date of death were collected. For all patients, time began at the date of procedure or if no procedure was performed, at the date of consultation. Elapsed time was calculated until death or last follow-up. Participants were considered censored if they were alive or lost to follow-up at the date of last assessment.
Functional Status Assessment
Functional status metrics were collected from the health assessment form filled out by patients during their initial evaluation and graded according to the Karnofsky Performance Scale (KPS)17 and the Katz Activities of Daily Living (ADL).18 Assessments were included if they were completed within a year of the pertinent KC diagnosis. The KPS describes functional status as an 11-point scale with values ranging from 100% (normal, no symptoms) to 0% (death). The Katz ADL grades whether a patient can independently perform six functions: bathing, dressing, toileting, transferring, continence and feeding. The scores are coded as a “0’ for no and “1” for yes. Total scores range from 0–6, with a 0 indicating no functional independence and a 6 indicating the highest level of functional independence.
Statistical Analysis
Analyses were performed with StataSE Software (version 14.2, College Station, TX). Alpha was set at 5% and all analyses were 2-tailed. Patient characteristics were summarized by procedure status (MMS, Excision, Non-surgical, Observation/Referral, Other). The one-way Anova and chi-square test were used to assess differences in the distribution of patient characteristics, tumor characteristics, and patient functional status scores for continuously and categorically scaled variables. For univariate assessments of overall survival, Kaplan-Meier survival curves were stratified by KPS and Katz ADL scores
Results:
Patient and lesion characteristics
A total of 345 patients 85 years or older presented for management of a KC. After patients with incomplete health assessments were excluded, 238 patients were included in this study. Of these, 127 patients (53.4%) underwent MMS and 18 patients (7.56%) underwent excision. Of patients who did not undergo surgery, 68 patients (28.6%) underwent non-surgical treatment. 12 were observed and 13 opted for treatment elsewhere or were lost to follow-up. Characteristics of participants and the presenting skin cancer are presented in Table 1. The mean age was 88.2 years and 50.8% of patients were female. The location of lesions included 43.7% on the head and neck area, 31.9% on the trunk and 24.4% of lesions on extremities.
Table 1.
Distribution of participant characteristics by treatment type.
| Variable | Coding | Overall | Mohs | Excision | Nonsurgical | Observation/Referral | Other | p-value | ||
|---|---|---|---|---|---|---|---|---|---|---|
| n=238 | n=127 | n=18 | n=68 | n=12 | n=13 | |||||
| mean (SD) | mean (SD) | mean (SD) | mean (SD) | mean (SD) | mean (SD) | |||||
| Age | Continuous | 88.2 (3.5) | 87.8 (3.3) | 88.2 (3.0) | 88.6 (3.5) | 89.8 (3.6) | 88.7 (3.5) | 0.22a | ||
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |||||
| Sex | Female | 121 (50.8) | 64 (50.4) | 7 (38.9) | 42 (61.8) | 2 (16.7) | 6 (46.2) | 0.04b | ||
| Male | 117 (49.2) | 63 (49.6) | 11 (61.1) | 26 (38.2) | 10 (83.3) | 7 (53.9) | ||||
| Marital Status | Married | 88 (37) | 58 (45.7) | 6 (33.3) | 17 (25) | 5 (41.7) | 2 (15.4) | 0.01b | ||
| Widowed | 99 (41.6) | 44 (34.7) | 10 (55.6) | 37 (54.4) | 5 (41.7) | 3 (23.1) | ||||
| Single | 21 (8.8) | 12 (9.5) | 1 (5.6) | 6 (8.8) | 0 (0) | 2 (15.4) | ||||
| Divorced | 6 (2.5) | 3 (2.4) | 1 (5.6) | 1 (1.5) | 0 (0) | 1 (7.7) | ||||
| Unknown | 24 (10.1) | 10 (7.9) | 0 (0) | 7 (10.3) | 2 (16.7) | 5 (38.5) | ||||
| Diagnosis | BCC | 119 (50) | 73 (57.5) | 8 (44.4) | 28 (41.2) | 5 (41.7) | 5 (38.5) | 0.18b | ||
| SCC | 119 (50) | 54 (42.5) | 10 (55.6) | 40 (58.8) | 7 (58.3) | 8 (61.5) | ||||
| mean (SD) | mean (SD) | mean (SD) | mean (SD) | mean (SD) | mean (SD) | |||||
| Karnofsky Performance Scale | Continuous | 81.1 (19.8) | 81.1 (19.8) | 80.6 (19.1) | 80.4 (20.5) | 88.3 (14.7) | 78.3 (15.8) | 0.75a | ||
| Katz ADL Performance Scale | Continuous | 4.8 (1.6) | 4.8 (1.5) | 4.3 (2.2) | 4.8 (1.8) | 5.7 (0.5) | 4.8 (1.9) | 0.32a |
Based on a one-way ANOVA
Based on Pearson’s Chi-square
Functional Status and Survival
Functional status scores demonstrated a relatively high level of independence with a mean KPS score of 81.1 and a mean Katz ADL of 4.8 (Table 1). For patients with follow-up, estimates of 7-year overall survival by KPS and Katz ADL functional status indices are presented in Figures 1A and 1B. In addition, 24-month survival is demarcated for each functional status index in the survival curves and presented with lower and upper bounds (95% confidence interval [CI]) for each index in Table 2. Survival estimates for KPS were calculated using three groups: low functional status (KPS=0–40), medium functional status (KPS=50–70), and high functional status (KPS=80–100). Katz ADL survival estimates were calculated using three groups: low to moderate functional status (Katz=0–4), high functional status (Katz=5) and the highest functional status (Katz=6). Patients with a low KPS score had a 2-year survival of 37% (95% CI, 0.01–0.80), compared to 75% in the high KPS score group (95% CI, 0.64–0.83). Similarly, patients with low to moderate Katz ADL scores had a 2-year survival of 53% (95% CI, 0.34–0.69), compared to 79% in the highest scoring Katz ADL group (95% CI, 0.68–0.87).
Figure 1A:

Overall survival by Karnofsky Performance Scale categorized as low (0–40), medium (50–70), and high (80–100). A vertical reference line depicts 2-year survival.
Figure 1B:
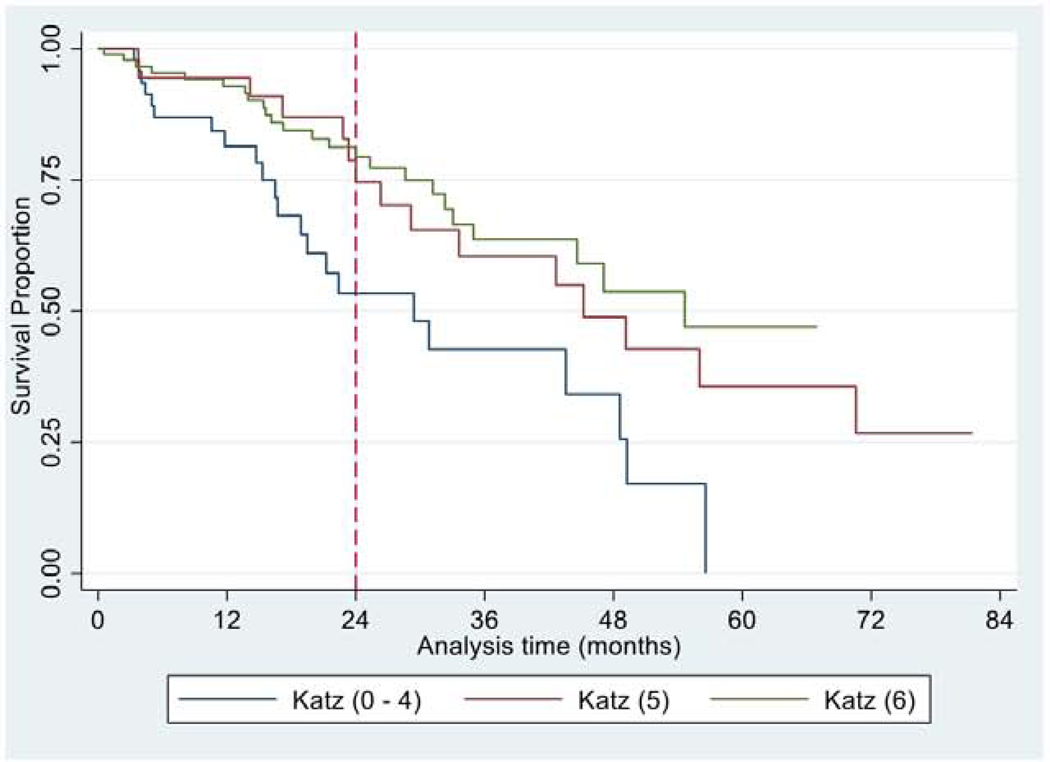
Overall survival by Katz ADL scores categorized as 0–4, 5 and 6. A vertical reference line depicts 2-year survival.
Table 2:
2-year Estimated Survival with 95% Confidence Intervals
| Scale | n | Survival Proportion (95% CI) | Hazard Ratio (95% CI) | p-value | |
|---|---|---|---|---|---|
| Karnofsky | Low (0–40) | 13 | 0.37 (0.01 – 0.80) | 3.39 (1.18 – 9.69) | 0.023 |
| Medium (50–70) | 59 | 0.67 (0.48 – 0.81) | 1.69 (0.96 – 2.98) | 0.069 | |
| High (80–100) | 155 | 0.75 (0.64 – 0.83) | 1.0 | Referent | |
| Katz | 0–4 | 62 | 0.53 (0.34 – 0.69) | 2.49 (1.39 – 4.47) | 0.002 |
| 5 | 62 | 0.74 (0.53 – 0.87) | 1.17 (0.60 – 2.27) | 0.641 | |
| 6 | 113 | 0.79 (0.68 – 0.87) | 1.0 | Referent |
Hazard ratios with lower and upper bounds (95%CI) for each index are presented in Table 2. Compared to the highest KPS scores (80–100), patients with the lowest KPS scores (0–40) had significantly worse survival (hazard ratio [HR], 3.39; 95% CI, 1.18–9.69, p = 0.023). Similar results were found for Katz ADL, with patients in the lowest functioning group (0–4) having significantly worse survival compared to patients in the highest functioning group (HR, 2.49; 95% CI, 1.39–4.47, p = 0.002).
Discussion:
In this study, patients ≥85 years of age presenting for treatment of KC at a tertiary care center had a mean age of 88.2 years old and demonstrated high functionality comparable to that in previous studies.19,20A large cohort of patients 75 years and older presenting for MMS was previously shown to have a mean KPS score of 90.1, demonstrating excellent functionality.19 In that study, a small percentage of patients (7.3%) had a KPS score of ≤70, and these lower-functioning patients were more likely to be older with larger, more symptomatic tumors. The lower mean KPS score of 81.1 in this study is likely due to the older population (≥85 years) included. Based on the mean functional status scores, it can be extrapolated that this cohort is generally high functioning with normal activities of daily living and few symptomatic comorbidities that would interfere with access to dermatologic care.
Karnofsky Performance Scale (KPS) and Katz ADL scores were similar across treatment groups in this study. 16,21,22 A prior study of patients receiving MMS, excision, and electrodessication and curettage similarly found no difference in functional status, along with other factors predictive of limited life expectancy.3 However, another study found that dermatologists consider patient functionality when selecting treatment for KC, using non-surgical management options in patients with poor functional status even when tumors met appropriate use criteria for Mohs surgery.20 In this study, functional status scores were similar across treatment groups and may be due to the overall higher functional status of this population. The study setting in a metropolitan city and tertiary care center may have caused preselection of patients with higher functionality and therefore may not be representative of the average 85-year-old in the community or rural practices. High functioning patients in this study were likely offered more treatment choices leading to factors such as lesion risk and patient preference having a greater influence on the treatment received.
This study showed that functional status scores stratify for survival, with lower scores associated with shorter survival. This finding supports the importance of functional status in assessing life expectancy in the very elderly presenting for KC treatment. In addition to life expectancy, tumor biology and patient preferences should be considered during the shared decision-making process for the very elderly.10 Other factors to consider in management decisions include tumor symptomatology and growth rate, expected treatment morbidity, and the patient’s ability to perform post-procedure care. These additional factors may have been drivers for the Observation/Referral group as they opted for minimal management despite their high functional status. Gender and marital status were also significantly associated with treatment modality in this patient cohort. Marital status has been established as a factor impacting treatment choice and faster recovery.23 It is possible that less aggressive treatments for KC in elderly, unmarried patients were favored when decisions were not influenced by a spouse.
In this study both the KPS and Katz ADL were useful in stratifying survival. A KPS ≤ 40 and Katz ADL ≤ 4 were associated with 37% and 53% survival at 2 years, respectively, while more than 75% of patients with higher KPS (>40) and Katz ADL (>4) scores were estimated to survive; demonstrating the utility of these measures as predictive tools in this population. Rogers et al. found that the very elderly treated with MMS survived by a median of 20 months longer compared to those who did not have MMS despite comparable comorbidity status,6 indicating that additional factors such as functional status may impact survival and/or choice of treatment modality. Hazard ratios for the KPS and Katz ADL indicate that the rate of death in patients with low functional status scores is significantly greater than high functioning patients. Notably, the rate of death in patients with low KPS scores is greater than three times the rate at 2 years compared to those with high KPS scores, indicating that the KPS may be particularly useful in predicting survival in the elderly seeking skin cancer treatment.
Our study categorized low functional status as a KPS score ≤ 40 and a Katz ADL score ≤ 4, consistent with definitions used in similar studies.24–26 Cancer patients with a KPS score between 60–100 are generally considered to be fit enough to receive standard cancer treatment, such as surgery or chemotherapy.27 However, treatment of an advanced melanoma or an aggressive head and neck SCC with systemic chemotherapy or an operating room surgical procedure has a different risk/benefit ratio than an in-office procedure; therefore a discussion taking into consideration factors such as functional status, comorbidity, life-expectancy, cost of care and patient desires, is warranted. As our study has shown, both the KPS and Katz ADL are effective tools in predicting short-term survival in very elderly patients seeking skin cancer treatment and can be formally implemented into patient counseling during a shared decision-making process.
There are limitations to this study including its retrospective, observational design. The patient population was from a tertiary care center that may have a socioeconomic, and functional status profile different from similar patients presenting for management in other settings. Future studies with geographic diversity may lead to greater generalizability of the data. The KPS and Karnofsky ADL indices were originally developed to assess functional status in patients with high mortality cancers and may not accurately capture the functional status of a healthier population presenting with slow growing, lower mortality malignancies. Patients who are very ill are unlikely to be referred and/or prioritize skin cancer treatment leading to selection bias as well. Basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) were also analysed together due to the limited number of cases in this specific population (≥85); however, we acknowledge that the tumor biology and progression of a BCC and SCC can differ.
Conclusions:
The vast majority of patients age 85 and older presenting to a tertiary care center for management of KC had high functional status scores and prolonged survival. Low functional status correlated with poorer short-term survival. A KPS score ≤ 40 and Katz ADL score ≤ 4 were significantly associated with decreased survival at 2 years, with the rate of death of patients with low KPS scores greater than three times those with high KPS scores. While low functional status was shown to correlate with poorer short-term survival, it should not be used as the sole determinant in choice of treatment. However, functional status can contribute to a comprehensive patient-centered approach in the very elderly presenting for management of KC. The KPS or Katz ADL can be a component of patient intake and should be considered during patient counseling and the shared decision-making process. Further research should be conducted on functional status in the elderly presenting for KC management in outpatient dermatology centers with a wider demographic and socioeconomic background.
Capsule Summary:
Very elderly patients presenting for keratinocyte carcinoma management had overall high functionality and prolonged survival.
The Karnofsky Performance Scale and Katz Activities of Daily Living predicted short-term survival in this study. Functional status should be considered during shared decision-making for elderly individuals seeking keratinocyte carcinoma treatment.
Acknowledgments
Funding Sources: The National Cancer Institute of the National Institutes of Health under Award Number R25CA020449 and the National Institutes of Health/National Cancer Institute Cancer Center Support Grant P30 CA008748
IRB approval status: Reviewed and approved by Memorial Sloan Kettering Cancer Center; approval 16–283
Footnotes
Conflicts of Interest: None declared
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Reference List:
- 1.Rogers HW, Weinstock MA, Feldman SR, Coldiron BM. Incidence Estimate of Nonmelanoma Skin Cancer (Keratinocyte Carcinomas) in the US Population, 2012. JAMA Dermatology. 2015;151(10):1081. doi: 10.1001/jamadermatol.2015.1187 [DOI] [PubMed] [Google Scholar]
- 2.Ortman JM, Velkoff VA, Hogan H. An Aging Nation: The Older Population in the United States Population Estimates and Projections Current Population Reports.; 2014. www.census.gov/population. Accessed November 12, 2018.
- 3.Linos E, Chren M-M, Stijacic Cenzer I, Covinsky KE. Skin Cancer in U.S. Elderly Adults: Does Life Expectancy Play a Role in Treatment Decisions? J Am Geriatr Soc. 2016;64(8):1610–1615. doi: 10.1111/jgs.14202 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Linos E, Parvataneni R, Stuart SE, Boscardin WJ, Landefeld CS, Chren M-M. Treatment of Nonfatal Conditions at the End of Life. JAMA Intern Med. 2013;173(11):1006. doi: 10.1001/jamainternmed.2013.639 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Chauhan R, Munger BN, Chu MW, et al. Age at Diagnosis as a Relative Contraindication for Intervention in Facial Nonmelanoma Skin Cancer. JAMA Surg. 2018;153(4):390. doi: 10.1001/jamasurg.2017.5073 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rogers EM, Connolly KL, Nehal KS, Dusza SW, Rossi AM, Lee E. Comorbidity scores associated with limited life expectancy in the very elderly with nonmelanoma skin cancer. J Am Acad Dermatol. 2018;78(6):1119–1124. doi: 10.1016/j.jaad.2017.12.048 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Delaney A, Shimizu I, Goldberg LH, MacFarlane DF. Life expectancy after Mohs micrographic surgery in patients aged 90 years and older. J Am Acad Dermatol. 2013;68(2):296–300. doi: 10.1016/j.jaad.2012.10.016 [DOI] [PubMed] [Google Scholar]
- 8.Charles AJ, Otley CC, Pond GR. Prognostic factors for life expectancy in nonagenarians with nonmelanoma skin cancer: Implications for selecting surgical candidates. J Am Acad Dermatol. 2002;47(3):419–422. doi: 10.1067/mjd.2002.122740 [DOI] [PubMed] [Google Scholar]
- 9.Mac Farlane DF, Pustelny B l., Goldberg LH. An Assessment of the Suitability of Mohs Micrographic Surgery in Patients Aged 90 years and Older. Dermatologic Surg. 1997;23(5):389–392. doi: 10.1111/j.1524-4725.1997.tb00067.x [DOI] [PubMed] [Google Scholar]
- 10.Lee EH, Brewer JD, MacFarlane DF. Optimizing Informed Decision Making for Basal Cell Carcinoma in Patients 85 Years or Older. JAMA Dermatology. 2015;151(8):817. doi: 10.1001/jamadermatol.2015.1454 [DOI] [PubMed] [Google Scholar]
- 11.Renzi M, Schimmel J, Decker A, Lawrence N. Management of Skin Cancer in the Elderly. Dermatol Clin. 2019;37(3):279–286. doi: 10.1016/j.det.2019.02.003 [DOI] [PubMed] [Google Scholar]
- 12.Grove DC. Age and Treatment of Nonmelanoma Skin Cancer. JAMA Surg. 2018;153(9):867. doi: 10.1001/jamasurg.2018.1696 [DOI] [PubMed] [Google Scholar]
- 13.Lee EH, Rossi AM, Nehal KS. Age and Treatment of Nonmelanoma Skin Cancer. JAMA Surg. 2018;153(9):865. doi: 10.1001/jamasurg.2018.1675 [DOI] [PubMed] [Google Scholar]
- 14.Lubeek SFK, van Vugt LJ, Aben KKH, van de Kerkhof PCM, Gerritsen M-JP. The Epidemiology and Clinicopathological Features of Basal Cell Carcinoma in Patients 80 Years and Older. JAMA Dermatology. 2017;153(1):71. doi: 10.1001/jamadermatol.2016.3628 [DOI] [PubMed] [Google Scholar]
- 15.Keeler E, Guralnik JM, Tian H, Wallace RB, Reuben DB. The impact of functional status on life expectancy in older persons. J Gerontol A Biol Sci Med Sci. 2010;65(7):727–733. doi: 10.1093/gerona/glq029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Extermann M, Overcash J, Lyman GH, Parr J, Balducci L. Comorbidity and functional status are independent in older cancer patients. J Clin Oncol. 1998;16(4):1582–1587. doi: 10.1200/JCO.1998.16.4.1582 [DOI] [PubMed] [Google Scholar]
- 17.Mor V, Laliberte L, Morris JN, Wiemann M. The Karnofsky Performance Status Scale. An examination of its reliability and validity in a research setting. Cancer. 1984;53(9):2002–2007. doi: [DOI] [PubMed] [Google Scholar]
- 18.Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of Illness in the Aged. The Index of ADL: A Standardized Measure Of Biological and Psychosocial Function. JAMA. 1963;185:914–919. http://www.ncbi.nlm.nih.gov/pubmed/14044222. Accesssed November 12, 2018. [DOI] [PubMed] [Google Scholar]
- 19.Regula CG, Alam M, Behshad R, et al. Functionality of Patients 75 Years and Older Undergoing Mohs Micrographic Surgery. Dermatologic Surg. 2017;43(7):904–910. doi: 10.1097/DSS.0000000000001111 [DOI] [PubMed] [Google Scholar]
- 20.Renzi MA, Belcher M, Brod B, et al. Assessment of Functionality in Elderly Patients When Determining Appropriate Treatment for Nonmelanoma Skin Cancers. Dermatologic Surg. July 2019:1. doi: 10.1097/DSS.0000000000002028 [DOI] [PubMed] [Google Scholar]
- 21.Garman KS, Cohen HJ. Functional status and the elderly cancer patient. Crit Rev Oncol Hematol. 2002;43(3):191–208. doi: 10.1016/S1040-8428(02)00062-8 [DOI] [PubMed] [Google Scholar]
- 22.West H (Jack) Jin JO Performance Status in Patients With Cancer. JAMA Oncol. 2015;1(7):998. doi: 10.1001/jamaoncol.2015.3113 [DOI] [PubMed] [Google Scholar]
- 23.Eskander MF, Schapira EF, Bliss LA, et al. Keeping it in the family: the impact of marital status and next of kin on cancer treatment and survival. Am J Surg. 2016;212(4):691–699. doi: 10.1016/j.amjsurg.2016.07.004 [DOI] [PubMed] [Google Scholar]
- 24.Yates JW, Chalmer B, McKegney FP. Evaluation of patients with advanced cancer using the karnofsky performance status. Cancer. 1980;45(8):2220–2224. doi: [DOI] [PubMed] [Google Scholar]
- 25.Couderc A-L, Boulahssass R, Nouguerède E, et al. Functional status in a geriatric oncology setting: A review. J Geriatr Oncol. February 2019. doi: 10.1016/j.jgo.2019.02.004 [DOI] [PubMed] [Google Scholar]
- 26.Sonmez OU, Arslan UY, Esbah O, et al. Effects of comorbidities and functional living activities on survival in geriatric breast cancer patients. Contemp Oncol (Poznan, Poland). 2014;18(3):204–210. doi: 10.5114/wo.2014.42252 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Terret C, Albrand G, Moncenix G, Droz JP. Karnofsky Performance Scale (KPS) or Physical Performance Test (PPT)? That is the question. Crit Rev Oncol Hematol. 2011;77(2):142–147. doi: 10.1016/j.critrevonc.2010.01.015 [DOI] [PubMed] [Google Scholar]