

Graphical Abstract
INTRODUCTION
Cardiovascular disease (CVD) is becoming more prevalent worldwide and is one of the leading causes of death.1 To lower CVD mortality, aggressive and comprehensive management of its risk factors, including dyslipidemia, hypertension, diabetes mellitus, and smoking, are crucial.2 The incidence of coronary artery disease (CAD) is rising in South Korea and although cerebral hemorrhage has declined since 2002, cerebral infarction is on the rise.3 This is speculated to be due to the elevated prevalence of dyslipidemia and diabetes mellitus with the growing obesity population, while hypertension is well-managed and smoking rate has reached a plateau.4 Thus, aggressive diagnosis and treatment of dyslipidemia, the most important risk factor for atherosclerosis, are critical for lowering the incidence and mortality of CAD and cerebral infarction.
To promote appropriate treatment of dyslipidemia, the Korean Society of Lipid and Atherosclerosis (KSoLA) published the first guidelines for the management of hyperlipidemia in 1996, the second guideline in 2003, the second revision in 2009, and the third guidelines for treatment of dyslipidemia with added contents in 2015, in collaboration with 18 other relevant academic societies and organizations.5 However, new guidelines were published in Europe in 2016 and in the United States in 2017 based on new study findings, and new drugs, such as proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors have been launched.6,7,8 Therefore, the KSoLA Treatment Guideline Committee developed the fourth guidelines for treatment and management of dyslipidemia specific to Koreans based on evidence and expert opinions on the dynamically changing treatment modalities for dyslipidemia.
The fourth guideline consists of information about the epidemiology of dyslipidemia, diagnosis and treatment criteria, lifestyle interventions, drug therapy, and dyslipidemia in specific patient groups. Finally, we present currently available data and the need to develop and validate scales to assess the risk of CVD specific to Koreans and CVD biomarkers appropriate for the Korean population. The level of evidence and strength of recommendations used in the fourth guideline are shown in Table 1. The fourth guideline is available in full text and an abstract form including tables and figures in Korean. This paper is an English summary of the full text. We hope the fourth guidelines for the treatment of dyslipidemia will be useful for health professionals treating dyslipidemia.
Table 1. Levels of evidence: classes of recommendation.
| Definition | Phrasing | |||
|---|---|---|---|---|
| Level of evidence | ||||
| A | Clear evidence for the recommendation | |||
| Clearly proven through multicenter RCTs or meta-analysis with adequate content and power with high generalizability of findings | ||||
| B | Reliable evidence for the recommendation | |||
| Evidence found through well-performed cohort or patient-control group studies | ||||
| C | Possible evidence for the recommendation | |||
| Not reliable, but relevant evidence found through small RCTs, observational studies, or case series | ||||
| E | Expert opinions | |||
| No supporting evidence, but expert opinions based on clinical experience and expertise | ||||
| Classes of recommendation | ||||
| Class I | Clear evidence (A) and benefits, and high applicability in practice | Recommended | ||
| Class IIa | Reliable evidence (B) and benefits, and high or moderate applicability in practice | Should be considered | ||
| Class IIb | Unreliable evidence (C or D) and benefits, but high or moderate applicability in practice | May be considered | ||
| Class III | Unreliable evidence (C or D), may cause harm, and low applicability in practice | Not recommended | ||
RCT, randomized controlled trial.
EPIDEMIOLOGY OF DYSLIPIDEMIA IN KOREANS
Cardiovascular disease in Koreans
CVD is the leading cause of deaths worldwide, with an estimated 17 million people dying from CVD every year.1,2 In South Korea, the death rate resulting from diseases of the circulatory system was 187 men per 100,000 population and 145 women per 100,000 population in 1983 and 111 men per 100,000 population and 125 women per 100,000 in 2016, indicating little change over the years. However, the age-adjusted mortality rate, which excludes the influence of aging of the population during this period, decreased to about one-fifth of the initial rate (Fig. 1). Death from CAD has consistently increased since 1983, when the cause of death statistics were first measured, reaching 31 men per 100,000 and 26 women per 100,000 in 2016. However, age-adjusted mortality of CAD reached a peak in the early and mid-2000s and began to decline since then (Fig. 2). Deaths from cerebrovascular disease declined since 2000s, reaching 44 men per 100,000 and 47 women per 100,000 in 2016. Age-adjusted mortality for cerebrovascular disease has declined very quickly (Fig. 3). Among various cerebrovascular diseases, there were more deaths from cerebral hemorrhage (non-traumatic intracerebral hemorrhage and subarachnoid hemorrhage) until 2002, but deaths from cerebral infarction (ischemic stroke) have become more common since then. This is speculated to be due to the marked decline in the incidence and improved treatment outcomes of cerebral hemorrhage as a result of advances in treatment for hypertension.9
Fig. 1. Trends of cardio-cerebrovascular mortality among Koreans, 1983 to 2016 (source: cause of death statistics). (A) Mortality rate (not age-adjusted). (B) Age-adjusted mortality rate (with reference to 2005 population).

Fig. 2. Trends of coronary artery disease mortality among Koreans, 1983 to 2016 (source: cause of death statistics). (A) Mortality rate (not age-adjusted). (B) Age-adjusted mortality rate (with reference to 2005 population).

Fig. 3. Trends of cerebrovascular disease mortality among Koreans, 1983 to 2016 (source: cause of death statistics). (A) Mortality rate (not age-adjusted). (B) Age-adjusted mortality rate (with reference to 2005 population).

The prevalence and incidence of CVD are not accurately known due to a lack of nationwide statistics. Based on a review of various studies, however, the prevalence of CVD is rising and the trend of incidence is predicted to vary according to the type of disease. Recent studies using health insurance claims data have reported the incidence of acute myocardial infarction (MI) to be about 50 and 10 per 100,000 for men and women, respectively.4,5,9 For cerebrovascular disease, the incidence of cerebral infraction and cerebral hemorrhage differs, where cerebral hemorrhage is declining quickly while cerebral infarction is slowly rising, eventually resulting in the number of cases of cerebral infraction outnumbering those of cerebral hemorrhage. It is generally believed that the incidence of CVD differs across regions and over time due to the changing distribution of CVD risk factors.10 The prevalence of hypertension in South Korea is largely consistent with the smoking rate reaching a lower plateau; however, the prevalence of diabetes mellitus and dyslipidemia is on the rise. Thus, it is predicted that CAD would become the most prevalent CVD in Korea.11,12
CVD risk factors and risk assessment for Koreans
The risk factors for CVD are well known, and the incidence of CVD varies across regions and time paralleling the distribution of these CVD risk factors across regions and time.10 Among CVD risk factors, those that have a significant impact on the disease but are able to be treated are referred to as major modifiable risk factors and include hypertension, diabetes, dyslipidemia, and smoking.12 Other CVD risk factors include family history, old age, lack of exercise, obesity, chronic inflammation, blood coagulation abnormalities, metabolic syndrome, depression, and stress. A Korean cohort study that analyzed the population attributable risk found that the contribution is the highest for hypertension, followed by smoking, dyslipidemia, and diabetes in men; the contribution by all four risk factors reaches 64%. In Korean women, the factor with the highest contribution to CVD risk was hypertension, followed by dyslipidemia, diabetes, and smoking (Table 1).13 Recently, many studies have attempted to assess CVD risk based on a comprehensive review of exposure to various CVD risk factors.14 Since the development of the Framingham risk score by the Framingham Heart Study to compute the 10-year risk of CAD using seven items of information (age, sex, total cholesterol, high density lipoprotein cholesterol [HDL-C], blood pressure, diabetes, and smoking), various CVD prediction models have been developed, and a CVD prediction recommendation guideline has been formulated. In South Korea, there are studies available that developed a stroke risk model, a CAD risk model, and a CVD risk assessment model using data from health check-up recipients.13,15,16,17,18,19
Distribution of lipid concentration in Koreans
The distribution of serum lipid concentrations varies according to sex and age and there is a notable difference among women before and after menopause. Total blood cholesterol concentration was reported to slightly decrease in the 15- to 19-year-old age group compared to that in the 10- to 14-year-old group, but increase again after the age of 20 years in both sexes.20 In the teen years, total cholesterol is higher among women. In individuals in their thirties and forties, total cholesterol is higher among men, but women actually have a higher total cholesterol concentration after the mid-50s (Fig. 4A). Distribution of low density lipoprotein cholesterol (LDL-C) concentration is similar to that of total cholesterol (Fig. 4B).20 Triglyceride concentration on rapidly increases from the age of 10 to 40 years, is maintained at a high level between ages 40 to 60, and gradually decreases after the age of 60 in men. Conversely, in women, triglyceride concentration is very low until the ages of 30 to 40, begins to increase after the mid-40s, and peaks after the age of 65 (Fig. 4C).20 HDL-C concentration is higher among women than men in across all age groups, and the gap is greater in the 20- to 30-year-old group (Fig. 4D).20
Fig. 4. Serum lipid concentrations by age, sex, and menopause in Korean general population. (A) Total cholesterol, (B) low density lipoprotein cholesterol (LDL-C), (C) triglyceride, and (D) high density lipoprotein cholesterol (HDL-C) (data source: Korea National Health and Nutrition Examination Survey 2010 to 2016).20.

The prevalence of hypercholesterolemia in adults aged 30 years or older in South Korea (total cholesterol ≥240 mg/dL or on cholesterol-lowering drugs) has risen consistently, from 7% and 8% in men and women, respectively, in 2005, to 19% and 20%, respectively, in 2016 (Fig. 5A).21 The prevalence of dyslipidemia was more than double that of hypercholesterolemia at 40.5%. Sex- and age-differences indicate that the prevalence of dyslipidemia in men is the highest between the ages of 55 to 59 years (49%) and gradually declines thereafter, while prevalence in women is low between the ages of 20 to 44 years, after which it rapidly increases to 50% between the ages of 60 to 64 years, eventually exceeding that of male counterparts (Fig. 5B).22 The prevalence of dyslipidemia is higher among individuals with other comorbidities, such as obesity, abdominal obesity, and diabetes than among those with no comorbidities.23
Fig. 5. Trends in prevalence of hypercholesterolemia (A, source: National Health and Nutrition Examination Survey [KNHANES] 2005 to 2016) and sex and age-specific prevalence of dyslipidemia (B, source: KNHANES 2010 to 2012).21,22.

Fortunately, indices for management, such as hypercholesterolemia awareness rate, treatment rate, and control rates, have been improving. The hypercholesterolemia awareness rate (the percentage of individuals diagnosed among all those who have hypercholesterolemia) increased from 24% in 2005 to 58% in 2016. In the same period, the treatment rate (the percentage of patients taking cholesterol-lowering drugs) increased from 17% to 49%, the patient control rate (the percentage of patients with total cholesterol <200 mg/dL) increased from 11% to 41%, and the treated patients' control rate (the percentage of treated patients with total cholesterol <200 mg/dL) increased from 62% to 83% (Fig. 6).21 These management indices have improved in both men and women overall, but the awareness rate and treatment rates have remained low at about 20% to 30% among those below age 50 even until recently (Table 2).21
Fig. 6. Trends in hypercholesterolemia management (source: National Health and Nutrition Examination Survey).

Table 2. Management of hypercholesterolemia by age, 30 years or older (2016)21.
| Variable | Total | Male | Female | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Number | % | SD | Number | % | SD | Number | % | SD | ||
| Awareness rate* | ||||||||||
| <30 yr (standardized) | 1,176 | 58.4 | 1.9 | 446 | 56.0 | 2.9 | 730 | 60.5 | 2.3 | |
| 30–49 yr | 249 | 32.0 | 3.3 | 142 | 34.5 | 4.2 | 107 | 27.1 | 5.6 | |
| 50–64 yr | 513 | 62.4 | 3.0 | 172 | 66.8 | 4.4 | 341 | 59.1 | 3.3 | |
| ≥65 yr | 414 | 79.7 | 1.9 | 132 | 76.3 | 3.9 | 282 | 81.3 | 2.4 | |
| Treatment rate† | ||||||||||
| <30 yr (standardized) | 1,176 | 49.1 | 1.8 | 446 | 48.8 | 3.0 | 730 | 49.4 | 2.3 | |
| 30–49 yr | 249 | 22.5 | 3.0 | 142 | 24.7 | 3.9 | 107 | 18.2 | 4.7 | |
| 50–64 yr | 513 | 51.3 | 2.8 | 172 | 60.1 | 4.6 | 341 | 44.7 | 3.3 | |
| ≥65 yr | 414 | 74.3 | 2.0 | 132 | 73.7 | 3.9 | 282 | 74.5 | 2.7 | |
| Control rate (based on patients who have the disease)‡ | ||||||||||
| <30 yr (standardized) | 1,176 | 41.3 | 1.7 | 446 | 42.4 | 2.8 | 730 | 40.5 | 2.0 | |
| 30–49 yr | 249 | 18.9 | 2.8 | 142 | 20.2 | 3.7 | 107 | 16.5 | 4.1 | |
| 50–64 yr | 513 | 42.7 | 2.8 | 172 | 53.0 | 4.5 | 341 | 34.9 | 3.0 | |
| ≥65 yr | 414 | 63.3 | 2.2 | 132 | 64.4 | 4.1 | 282 | 62.9 | 2.8 | |
| Control rate (based on individuals undergoing treatment)§ | ||||||||||
| <30 yr (standardized) | 626 | 82.7 | 1.7 | 238 | 86.1 | 2.5 | 388 | 79.9 | 2.4 | |
| 30–49 yr | 53 | 81.1 | 5.9 | 34 | 81.7 | 7.1 | 19 | - | - | |
| 50–64 yr | 271 | 82.2 | 2.7 | 109 | 87.0 | 3.4 | 162 | 77.2 | 3.9 | |
| ≥65 yr | 302 | 84.0 | 2.2 | 95 | 87.3 | 3.4 | 207 | 82.5 | 2.8 | |
SD, standard deviation.
*Hypercholesterolemia awareness rate (≥30 years): percentage of individuals diagnosed with hypercholesterolemia by a physician from the total number of individuals with hypercholesterolemia.
†Hypercholesterolemia treatment rate (≥30 years): percentage of individuals currently taking cholesterol-lowering drugs for at least 20 days a month from the total number of individuals with hypercholesterolemia.
‡Hypercholesterolemia control rate (≥30 years, based on individuals who have the disease): percentage of individuals with total cholesterol of <200 mg/dL from the total number of individuals with hypercholesterolemia.
§Hypercholesterolemia control rate (≥30 years, based on individuals undergoing treatment): percentage of individuals with total cholesterol of <200 mg/dL from the total number of individuals being treated for hypercholesterolemia.
DIAGNOSIS AND TREATMENT CRITERIA FOR DYSLIPIDEMIA
Recommendation
| Content | Strength of recommendation | Level of evidence | |
| 1 | Patients with CVD (CAD, peripheral artery disease, atherosclerotic ischemic stroke, transient ischemic attack) are classified as a very high-risk group, and the treatment goal is to lower LDL-C levels to <70 mg/dL or by >50% from the baseline level for secondary prevention. | I | A |
| 2 | If acute myocardial infarction occurs, administer statins immediately regardless of the baseline LDL-C level. | I | A |
| 3 | Patients with carotid disease (significant carotid artery stenosis), abdominal aortic aneurysm, or diabetes are classified as a high-risk group. For this group, begin treatment when LDL-C concentration is ≥100 mg/dL for primary prevention. | I | A |
| 4 | Patients with two or more major risk factors other than LDL-C are classified as a moderate-risk group. For this group, administer statin if LDL-C concentration is ≥130 mg/dL even after weeks or months of lifestyle adjustment. | II | B |
| 5 | Patients with one or fewer major risk factors other than LDL-C are classified as low-risk group. For this group, administer statin if LDL-C concentration ≥160 mg/dL even after weeks or months of lifestyle adjustment. | II | B |
| 6 | If LDL-C concentration is ≥190 mg/dL, check whether the patient has other causes for hyperlipidemia, such as biliary obstruction, nephrotic syndrome, hypothyroidism, pregnancy, use of glucocorticoids or cyclosporine and make necessary adjustments. | I | B |
| 7 | If LDL-C concentration is ≥190 mg/dL in absence of secondary causes, begin statin administration regardless of the risk. | I | A |
| 8 | If blood triglyceride concentration rises to ≥500 mg/dL, check for secondary causes of triglyceride elevation, such as weight gain, drinking, carbohydrate intake, chronic kidney disease, diabetes, hypothyroidism, pregnancy, and use of estrogen, tamoxifen, or glucocorticoids and for other genetic problems that may cause abnormal lipid metabolism. | I | A |
| 9 | If triglyceride concentration is consistently ≥500 mg/dL, drug therapy, such as fibrate and omega-3 fatty acid therapy, may be initiated to prevent pancreatitis. | II | A |
| 10 | If triglyceride concentration is between 200–499 mg/dL with high LDL-C level, it is recommended to begin statin administration to primarily lower LDL-C concentration to the targeted level. | I | A |
| 11 | If hypertriglyceridemia persists (≥200 mg/dL) even after lifestyle adjustment and statin administration in very high-risk and high-risk patients, drugs that lower triglyceride levels, such as fibrate or omega-3 fatty acids, may be additionally used to prevent CVD. | II | B |
Diagnostic approach and criteria
Dyslipidemia is generally asymptomatic, so a screening test is essential to identify patients requiring treatment. For screening of dyslipidemia, all adults aged ≥21 years and younger individuals with other risk factors, such as a family history of premature CVD and severe dyslipidemia, should undergo a fasting lipid test every 4 to 6 years to assess total cholesterol, triglyceride, HDL-C, LDL-C (calculated using the Friedewald equation or perform a direct assay when triglyceride level is ≤400 mg/dL), and non-HDL-C levels.6,24
For the measurement of triglyceride and LDL-C levels, individuals must fast for at least 12 hours before blood sampling. LDL-C concentration can be generally estimated from fasting total cholesterol, triglyceride, and HDL-C. That is, if the individual's triglyceride concentration is ≤400 mg/dL, very low density lipoprotein cholesterol (VLDL-C) concentration can be estimated by dividing the triglyceride value by 5. As total cholesterol is the sum of LDL-C, HDL-C, and VLDL-C concentrations, LDL-C concentration can be calculated using the Friedewald equation below:
However, if the individual's triglyceride concentration >400 mg/dL, the LDL-C value estimated from the above equation is less accurate. In such cases, we recommend using the LDL-C direct assay.25 In addition, the cause of hypertriglyceridemia should be further investigated.
Treatment guideline
In this treatment guideline, we maintained the existing system of differentiating target LDL-C concentration based on the level of CVD risk factors, as previously used in the current treatment guideline in Korea, but modified and supplemented the specific risk factors and treatment standards with reference to study findings in Korea and abroad as well as with the 2013 American College of Cardiology (ACC)/American Heart Association (AHA), 2016 European Society of Cardiology (ESC)/European Atherosclerosis Society (EAS), and treatment guidelines published in other countries.6 One benefit of the 2013 ACC/AHA treatment guideline is that it simplified the criteria for statin administration to “four statin benefit groups,” but it has been reported that the practical application of the criteria would be difficult due to several problems.21 Therefore, we did not deviate significantly from the third revision of Korean dyslipidemia guidelines.
Very high-risk group
Patients with CVD (CAD, peripheral artery disease, ischemic stroke, transient ischemic attack) are classified as the very high-risk group. For this group, the goal should be set to lowering LDL-C to <70 mg/dL or by more than 50% of the baseline level for secondary prevention. Furthermore, when acute MI occurs, statin should be immediately administered regardless of the baseline LDL-C concentration (Tables 3 and 4).
Table 3. Treatment according to risk and LDL-C concentration.
| Risk | LDL-C, mg/dL | ||||||
|---|---|---|---|---|---|---|---|
| <70 | 70–99 | 100–129 | 130–159 | 160–189 | ≥190 | ||
| Very high-risk group* | Lifestyle modification and consider drug therapy | Lifestyle modification and begin drug therapy | Lifestyle modification and begin drug therapy | Lifestyle modification and begin drug therapy | Lifestyle modification and begin drug therapy | Lifestyle modification and begin drug therapy | |
| Coronary artery disease | |||||||
| Atherosclerotic ischemic stroke and transient ischemic attack | |||||||
| Peripheral artery disease | |||||||
| High-risk group | Lifestyle modification | Lifestyle modification and consider drug therapy | Lifestyle modification and begin drug therapy | Lifestyle modification and begin drug therapy | Lifestyle modification and begin drug therapy | Lifestyle modification and begin drug therapy | |
| Carotid artery disease† | |||||||
| Abdominal aneurysm | |||||||
| Diabetes‡ | |||||||
| Moderate-risk group§ | Lifestyle modification | Lifestyle modification | Lifestyle modification and consider drug therapy | Lifestyle modification and begin drug therapy | Lifestyle modification and begin drug therapy | Lifestyle modification and begin drug therapy | |
| Two or more major risk factors | |||||||
| Low-risk group§ | Lifestyle modification | Lifestyle modification | Lifestyle modification | Lifestyle modification and consider drug therapy | Lifestyle modification and begin drug therapy | Lifestyle modification and begin drug therapy | |
| One or fewer major risk factors | |||||||
LDL-C, low density lipoprotein cholesterol.
*In case of acute myocardial infarction, begin statin therapy immediately regardless of the baseline LDL-C. Statin therapy may be considered for very high-risk group other than acute myocardial infarction even if LDL-C is <70 mg/dL.
†In case of significant stenosis of the carotid artery
‡Level of risk may be raised depending on the patient if patient has target organ damage or major cardiovascular disease risk factor.
§For moderate-risk and low-risk groups, statin therapy is considered when high LDL-C persists even after weeks or months of lifestyle modification.
Table 4. Target LDL-C and non-HDL-C goals according to risk category.
| Risk | LDL-C, mg/dL | Non-HDL-C, mg/dL | |
|---|---|---|---|
| Very high-risk group | <70 | <100 | |
| Coronary artery disease | |||
| Atherosclerotic ischemic stroke and transient ischemic attack | |||
| Peripheral artery disease | |||
| High-risk group | <100 | <130 | |
| Carotid artery disease* | |||
| Abdominal aneurysm | |||
| Diabetes† | |||
| Moderate-risk group | <130 | <160 | |
| Two or more major risk factors‡ | |||
| Low-risk group | <160 | <190 | |
| One or fewer major risk factors‡ | |||
LDL-C, low density lipoprotein cholesterol; HDL-C, high density lipoprotein cholesterol.
*In case of significant stenosis of the carotid artery.
†The target may be lowered depending on the patient if patient has target organ damage or major cardiovascular disease risk factor.
†Age (male ≥45 years, female ≥55 years), family history of premature coronary artery disease, hypertension, smoking, hypo-HDL-C.
In a foreign randomized trial to test low-dose or high-dose statin administration on 10,000 patients with stable angina with LDL-C <130 mg/dL, lowering LDL-C level close to 70 mg/dL with high-dose statin administration reduced CVD risk by about 22%.26 Furthermore, a meta-analysis of patients who received statin reported that preventive effects against CVD were the greatest when LDL-C was reduced to a level <70 mg/dL or by >50% of the baseline level.27
The 2018 AACE/ACE guidelines recommend that patients with atherosclerotic CVD and (1) atherosclerotic CVD continuing to progress even after lowering LDL-C to <70 mg/dL, (2) diabetes, (3) stage 3 or 4 chronic kidney disease, (4) heterozygous familial hypercholesterolemia (heFH), or (5) history of premature atherosclerotic CVD (men <55 years, women <65 years) should be classified into the extreme risk group and that the target for LDL-C should be set to <55 mg/dL.28 This recommendation stems from the Improved Reduction of Outcomes: Vytorin Efficacy International Trial (IMPROVE-IT), which proved the superiority of combined statin and ezetimibe therapy for patients with acute coronary artery syndrome, and the Further Cardiovascular Outcomes Research with PCSK9 Inhibition in Subjects with Elevated Risk (FOURIER) study and the ODYSSEY OUTCOMES trial, which confirmed the effects of PCSK9 inhibitors.29,30,31 These three studies documented that lowering the targeted LDL-C concentration to below the previous target is additionally beneficial for prevention of major CVD events particularly for the extreme risk group. These findings suggest that it may be necessary to lower the LDL-C target level for patients with clinical apparent atherosclerotic CVD (particularly acute coronary artery syndrome). However, additional studies are needed to investigate cost-effectiveness and application in Korean patients.
Furthermore, a foreign randomized trial on 4,700 patients who experienced ischemic stroke or transient ischemic attack within 6 months found that the LDL-C concentration was 73 mg/dL in the statin group and 129 mg/dL in the placebo group and that the risks of stroke and CVD significantly decreased by 16% and 20%, respectively, in the statin group, which suggested that lowering LDL-C to close to 70 mg/dL through statin administration would also be helpful for patients who had an ischemic stroke.32 However, considering that the Korea Medical Insurance Corporation (KMIC) study and Japan's National Integrated Project for Prospective Observation of Non-communicable Disease and its Trends in the Aged (NIPPON DATA80) cohort study reported that hypertension, as opposed to hypercholesterolemia, was more strongly associated with cerebrovascular diseases and that high-dose statin administration reduced the incidence of ischemic stroke but increased that of hemorrhagic stroke, additional Korean studies are needed to further investigate the statin dose and LDL-C targets for preventing ischemic stroke.33
When acute MI occurs, it is recommended to administer statins immediately regardless of the baseline LDL-C level. In a randomized controlled trial on 4,500 patients who experienced an acute MI, the incidence of CVD was lower in the group that received statin immediately after MI than in the group that did not receive statin immediately after MI.34 In a Korean study, though a retrospective follow-up using registry, of about 1,000 patients whose LDL-C concentration was <70 mg/dL at the time of MI, the 1-year incidence of CVD was lower in the group that immediately received statin than in the group that did not.35 Thus, in light of Korean and foreign study findings, it is recommended to administer statin immediately after acute MI regardless of the baseline LDL-C concentration.
High-risk group
Patients with carotid disease (significant carotid artery stenosis), abdominal aortic aneurysm, or diabetes are classified as a high-risk group. For this group, treatment is started when LDL-C concentration is ≥100 mg/dL for primary prevention.36,37 Furthermore, for diabetes patients with target organ damage or major CVD risk factors, the target could be lowered depending on the case (Tables 3 and 4).
In the North American Symptomatic Carotid Endarterectomy Trial (NASCET) that followed-up 1,415 patients who underwent carotid endarterectomy due to carotid artery stenosis, the risk of stroke on the ipsilateral side over a period of 8 years was 17.1% higher among patients with a carotid disease.38 Similarly, the European Carotid Surgery Trial (ECST) study showed that patients with symptomatic carotid artery stenosis had a higher cardiovascular mortality rate, with a 6-year mortality of 27% regardless of the degree of stenosis, and the 10-year cardiovascular mortality was estimated to be 30%.39,40 In addition, many studies reported that among patients with carotid artery stenosis without CVD, lowering LDL-C by administering statin reduced major cardiovascular events and mortality.41 Korean treatment guidelines also classified patients with carotid artery stenosis as the high-risk group but did not indicate a specific degree of stenosis.
Moderate-risk group
In line with existing Korean treatment guidelines, patients with two or more major risk factors other than LDL-C are classified into the moderate-risk group. Statin is administered if LDL-C concentration remains >130 mg/dL even after weeks or months of lifestyle adjustment (Tables 3,4,5). The major risk factors listed in the Adult Treatment Panel (ATP) III and Korean guidelines were used. Among these, smoking, hypertension, age, sex, and low HDL-C have also been adopted by other treatment guidelines, including the 2013 ACC/AHA, ESC/EAS, and Japan Atherosclerosis Society (JAS).6,24,42 However, assessing risk based on these major risk factors is known to predict only about half of the actual cardiovascular risk; thus, individualized treatment goals should be set in consideration of other risk factors, such as obesity, physical activity, diet, levels of triglycerides, high sensitivity C-reactive protein (hs-CRP), lipoprotein(a), apolipoprotein, fibrinogen, homocysteine, and apolipoprotein B, as well as the ankle-brachial blood pressure index, carotid intimal medial thickening (<50% stenosis but with evidence of clinical progression or accompanied by atherosclerotic plaque), and coronary calcium score.6,40
Table 5. Major risk factors other than low density lipoprotein cholesterol*.
| Age: male ≥45 years, female ≥55 years |
| Family history of premature coronary artery disease: coronary artery disease before the age of 55 years for men and 65 years for women among parents and siblings |
| Hypertension: systolic BP ≥140 mmHg or diastolic BP ≥ 90 mmHg or taking antihypertensive drugs |
| Smoking |
| Low HDL-C (<40 mg/dL) |
BP, blood pressure; HDL-C, high density lipoprotein cholesterol.
*High HDL-C (≥60 mg/dL) is considered a protective factor, so one risk factor is deducted.
Low-risk group
Patients with one or fewer major risk factor other than LDL-C are classified as the low-risk group. In line with previous treatment guidelines, statin is administered if LDL-C remains >160 mg/dL even after weeks or months of lifestyle adjustment (Table 3). In the revised guideline, LDL-C target was set to <160 mg/dL, but as other non-major risk factors were taken into consideration for the moderate-risk group, more aggressive treatment goals could be also set for the low-risk group depending on the case.40 If LDL-C concentration is >190 mg/dL, other causes of dyslipidemia, such as biliary obstruction, nephrotic syndrome, hypothyroidism, pregnancy, and use of glucocorticoids or a cyclosporine, should be investigated and corrected. If LDL-C concentration is >190 mg/dL in absence of secondary causes, statin should be started irrespective of the level of risk.
Treatment guidelines for hypertriglyceridemia
The risk of acute pancreatitis is known to increase when blood triglyceride level exceeds 500 mg/dL, and in such cases, it is important to investigate secondary causes that may elevate triglyceride concentration, such as weight gain, drinking, carbohydrate intake, chronic kidney failure, diabetes, hypothyroidism, pregnancy, and use of estrogen, tamoxifen, and glucocorticoids, as well as genetic factors that may cause abnormal lipid metabolism.24,43 If triglyceride concentration remains ≥500 mg/dL even in the absence or correction of secondary causes, it is recommended to begin fibrate or omega-3 fatty acid therapy to prevent pancreatitis. Further, statin should be administered if triglyceride level is between 200 to 499 mg/dL with a high LDL-C level so as to primarily lower the LDL-C concentration to the targeted level. If hypertriglyceridemia persists (≥200 mg/dL) even after lifestyle adjustment and statin administration in the very high-risk and high-risk groups, drugs that lower triglyceride concentration, such as fibrate and omega-3 fatty acid, can additionally be used to prevent CVD.
Statin, as opposed to other effective triglyceride-lowering drugs, such as fibrates, is recommended as the primary drug for patients with hypertriglyceridemia based on the multiple study findings indicating that statin administration is helpful for preventing CVD.44 Whether fibrate administration is effective in preventing CVD remains controversial. In a meta-analysis of randomized controlled trials (RCTs) to investigate the effects of medications for dyslipidemia on mortality, statin significantly decreased cardiovascular mortality, while fibrate did not significantly lower mortality compared to placebo.45 Considering that there have been no study findings suggesting that fibrate has superior effects to statin on preventing CVD in patients with hypertriglyceridemia, it would be appropriate to primarily administer statin in order to prevent CVD caused by hypertriglyceridemia.
Moreover, whether administration of fibrate or omega-3 fatty acid in addition to statin for patients with persistent hypertriglyceridemia even after lifestyle adjustment and statin administration lowers CVD risk is still a matter of debate. The Action to Control Cardiovascular Risk in Diabetes Action to Control Cardiovascular Risk in Diabetes (ACCORD) study reported that additional fibrate administration to about 5,500 patients with type 2 diabetes taking statin did not lower CVD or mortality. However, the same study found that pre-administration triglyceride concentration was low (162 mg/dL) in all patients and an additional analysis showed that among patients with pre-treatment triglyceride concentration ≥204 mg/dL with low HDL-C (≥34 mg/dL), the incidence of CVD differed between the fibrate (12%) and placebo (17%) groups.46 Therefore, adding triglyceride-lowering drugs, such as fibrate and omega-3 fatty acid, to the statin regimen is recommended for high-risk patients with persistent hypertriglyceridemia (≥200 mg/dL) even after lifestyle adjustment and statin administration to prevent CVD.
Follow-up monitoring
In line with previous Korean guidelines and foreign guidelines, the present revision also recommends lipid testing prior to administration and another round of testing 4 to 12 weeks after beginning administration to assess response and compliance, after which it is recommended to perform lipid tests at 3- to 12-month intervals depending on the patient's cardiovascular risk and degree of lipid reduction after drug administration. The revised guideline recommends performing a liver function test in addition to a lipid test.
In line with the existing guideline, the present revision also recommends termination of drug administration if patient develops myopathy symptoms and creatine kinase (CK) levels increase more than 10-fold. In Korea, blood creatinine levels should be measured before fibrate administration and after 3 months of administration and patients should be followed-up every 6 months if there are no other abnormal findings.
Conclusions
The 2013 ACC/AHA treatment guidelines could not be directly applied in Korea, as it did not reflect individual differences in drug responses by uniformly recommending a moderate-to-high dose of statin for all patients without a specific LDL-C target level, did not clearly examine the benefits and adverse reactions of high-dose statin administration, and may overestimate CVD risk in Korea. Additional studies are needed on the Korean population to set an appropriate statin dose and LDL-C target and specific goals for controlling risk factors and hypertriglyceridemia, which serve as the criteria for primary prevention.
LIFESTYLE INTERVENTIONS FOR DYSLIPIDEMIA
Diet therapy: recommendation
| Content | Strength of recommendation | Level of evidence | ||
| 1 | Consume sufficient energy to maintain an appropriate body weight | I | A | |
| 2 | Total fat intake should not exceed 30% of total energy intake | IIa | B | |
| 3 | Limit saturated fat intake to <7% of total energy intake | I | A | |
| 4 | Replace saturated fat with unsaturated fat but limit omega-6 polyunsaturated fat intake to <10% of total energy intake | IIa | B | |
| 5 | Avoid trans fatty acid intake | I | A | |
| 6 | For patients with hypercholesterolemia, limit daily cholesterol intake to 300 mg. | IIa | B | |
| 7 | Limit total carbohydrate intake to <65% of total energy intake and sugar intake to 10% to 20% of total energy intake | IIa | B | |
| 8 | Eat fiber-rich foods to consume >25 g of dietary fiber | I | A | |
| 9 | Limit daily alcohol intake to 1 to 2 shots | I | A | |
| 10 | Eat diets rich in whole grains and multigrain, beans, vegetables, and fish | IIa | B | |
| Eat whole grain and multigrain as the staple | ||||
| Eat sufficient amounts of vegetables | ||||
| Eat fish, particularly blue-back fish 2 to 3 times a week | ||||
| Eat an adequate amount of fresh fruits | ||||
Energy
Obesity and overweight are related to dyslipidemia. Many studies with obese or overweight individuals found that total cholesterol, LDL-C, and triglyceride concentrations decreased with weight loss.47 Therefore, Energy intake should be appropriate to maintain healthy weight. According to WHO criteria, body mass index (BMI) of ≥30 kg/m2 is classified as obesity. However BMI of ≥25 kg/m2 proposed as obesity in Korea.48 Obese people can expect to improve blood cholesterol and triglyceride levels even by losing about 5% to 10% of current weight. In general, a low-calorie diet that is about 500 kcal less than one's usual intake has no particular harm to health and is reasonable to adhere to.
Fat
Traditionally, it was recommended to limit fat intake to treat dyslipidemia. Several studies have reported that limiting fat intake improves LDL-C levels, but in most cases, it is difficult to conclude that such improvement is an outcome of limiting total fat intake, as an interaction of multiple factors, such as weight loss and reducing saturated fats and trans fats, are involved. Moreover, when fat intake is limited, carbohydrate intake relatively increases, which in turn increases blood triglyceride level.49 However, an excessively high-fat diet may have an adverse impact on blood lipid levels by increasing saturated fat and energy intake, so an appropriate amount of fat should be consumed. The 2016 ESC/EAS guideline recommends individualized rules of percent fat intake but to take precaution so as not to exceed 35% of total energy consumption, as it may result in elevated saturated fat and energy intake.6 The average fat intake in Korean is about 20%. In Dietary Reference Intake (DRI) for Koreans 2015, 15% to 30% fat intake is recommended.50,51 However, considering that percent fat intake varies widely across individuals and fat intake has been on the rise recently, individuals should take precaution so as not to consume fats excessively. Overall, fat intake should be limited to within 30% of total energy consumption.
The type of fatty acids has a greater impact on blood lipid levels than total fat amount. Replacing saturated fats to unsaturated fats could lower blood LDL-C level, and substituting trans fats to unsaturated fats contributes to improving blood triglyceride and HDL-C levels.52 The 2016 ESC/EAS guideline recommends to limit saturated fats intake to <7% of total energy intake and to limit trans fat intake to <1% of total energy intake by avoiding processed foods.6 The 2013 AHA/ACC guideline recommends to limit saturated fatty acid intake to 5% to 6% of total energy intake and to avoid trans fat intake.50 Some rich sources of saturated fats include fats of meats, skin of poultry, butter, and palm oil. The major sources of trans fats are hydrogenated oils, such as margarine and shortening, and trans fats are produced during heating oil in high temperature.
N-3 fatty acids do not have a positive effect on blood cholesterol levels but 2 to 4 g of n-3 fatty acids may help lower triglyceride level for those with hypertriglyceridemia.54 Although substituting saturated fat with polyunsaturated fat is effective in improving blood lipid levels, it is recommended to limit n-6 fatty acid intake to 10% of total energy intake.
Cholesterol intake has a less of an impact on blood LDL-C levels than saturated fats and trans fats and the effect varies widely across individuals. Due to insufficient evidence dietary cholesterol restriction in order to prevent serum LDL-C recommendation of dietary cholesterol was excluded from the 2015 Dietary Guideline for Americans. The 2013 AHA/ACC guideline does not include a recommendation about cholesterol intake.53 The 2016 ESC/EAS guideline recommends cholesterol intake be limited to 300 mg only for individuals with high serum cholesterol level.6 In DRI for Koreans 2015, it is recommended to reduce dietary cholesterol less than 300 mg.51 In this context, cholesterol intake need not be limited uniformly for the prevention of dyslipidemia, but excessive intake should be avoided for individuals with hypercholesterolemia.
Carbohydrates
Excessive carbohydrate intake, particularly simple sugar intake, elevates blood triglyceride level. In Western countries, recommendation on carbohydrate restriction is not separately specified, the proportion of carbohydrate intake is not high in general population. Instead, recommendations suggest simple sugar intake to be limited and to eat fiber-rich food sources of carbohydrates. Conversely, carbohydrate is a major portion of Koreans' diet, so Koreans should take precautions so as not to consume carbohydrates excessively. It is recommended that the total carbohydrate consumption be limited to 65% of daily energy intake, which is the upper limit of DRI for Koreans 2015 and simple sugars should be limited to 10% to 20% of daily energy intake.51
Soluble fibers are beneficial in lowering blood cholesterol and triglyceride concentrations, and they are found in rich amounts in whole grains, seaweeds, and vegetables. The 2016 ESC/EAS guideline recommends people to consume 5 to 15 g of soluble fibers (25 to 40 g of total dietary fiber).6,55,56 It is recommended that people eat fiber-rich foods to ingest >25 g of dietary fiber.
Alcohol
Excessive alcohol consumption (≥10 to 30 g/daily) should be avoided, as it increases blood triglyceride levels.57 Hypertriglyceridemia due to alcohol consumption is associated with suppression of chylomicron degradation as a result of reduced lipoprotein lipase (LPL) activity. The 2016 ESC/EAS guideline recommends people to avoid heavy drinking (<20 to 30 g for men, <10 to 20 g for women) and to avoid drinking for patients with hypertriglyceridemia.6 Regardless of the type of alcohol, daily drinking should be limited to one to two drinks.
Dietary pattern
Recent dietary guidelines for CVD tend to emphasize the quality of overall diets, rather than focusing on individual nutrients. These changes are based on the accumulating evidence that quality of fat intake is more important than quantity of fat intake Studies of dietary patterns for the Western population such as Dietary Approaches to Stop Hypertension (DASH) or Mediterranean dietary patterns reported the effects of dietary patterns on blood lipid levels. Based on these results, the ACC/AHA guidelines adopt dietary patterns such as the DASH, the United States Department of Agriculture (USDA) food pattern, and AHA diet for dietary recommendations.53 The 2016 ESC/EAS guideline also emphasizes the importance of healthy food choice.6
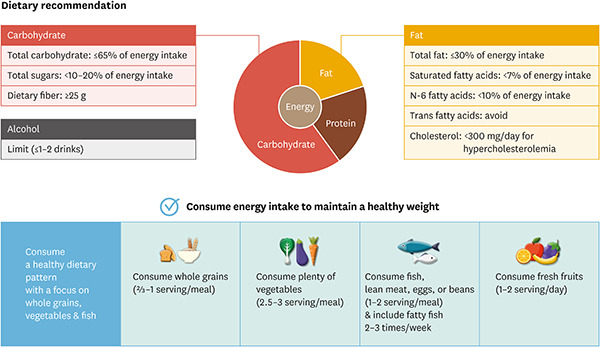
In Korea, few studies have examined the association between dyslipidemia and dietary patterns, but diets rich in whole grains, such as brown rice and whole wheat, with vegetables, legumes, fish, fruits, and dairy products may be helpful. Many Korean adults consume a typical high-carbohydrate low-fat diet compared to Western populations. Therefore, increasing the proportion whole grains instead of refined rice and balanced diet including adequate amounts of fish, beans, and fresh vegetables would be beneficial. Furthermore, although fresh fruits and milk are recommended, fruit concentrates and sweetened milk should be avoided. Table 6 shows a list for food choice, and Table 7 shows an example of the recommended daily meal plan. The dietary guideline to prevent and manage dyslipidemia for Koreans is summarized in Fig. 7.
Table 6. The list of foods to be recommended and to be avoided.
| Food group | Choose these foods, but be careful not to eat excessive | Be careful not to eat too much of these foods and eat them too frequently! |
|---|---|---|
| Fish/beans/eggs | Fish | Ground meat, ribs, internal organs of meats |
| Bean, tofu | Poultry skin, fried chicken | |
| Lean meat | High-fat processed meat products | |
| Poultry without skin | ||
| Eggs | ||
| Dairies | Skim milk, powdered skim milk, low fat milk and their products | Condensed milk and its products |
| Low-fat cheese | Cheese, cream cheese | |
| Ice cream | ||
| Coffee cream | ||
| Fats and oils | Unsaturated fatty acid: corn oil, olive oil, perilla oil, soybean oil, sunflower oil | Butter, pork oil, shortening, bacon oil, beef oil |
| Low-fat/non-fat salad dressing | Cheese- or whole milk-based salad dressing | |
| Hard margarine | ||
| Grains | Whole grains | Butter and margarine-based bread and cake |
| High-fat crackers, biscuits, chips, butter popcorns | ||
| Pastry, cake, donut, high-fat snack | ||
| Soup | Soup with fat removed after cooking | Oily soup, cream soup |
| Vegetables/fruits | Fresh vegetables, seaweeds, fruits | Fried or butter-, cheese-, cream-, or sauce-added vegetables/fruits |
| Sweetened processed products (e.g., canned fruit) | ||
| Others | Nuts: peanut, walnut | Chocolate/sweets |
| Products with coconut oil or palm oil | ||
| Fried snacks |
Table 7. Example of a daily meal plan.
| Food group | Recommendation | Serving size of typical foods |
|---|---|---|
| Grains | Whole grain-based diet | Rice (e.g., multigrain rice, brown rice): 210 g (1 bowl) |
| 2/3 to 1 serving every meal | Bread (e.g., whole-wheat bread, barley bread): 105 g (3 slices) | |
| Vegetables | Diverse types of vegetables | Vegetables: 70 g (cooked 1/3 cup) |
| 2.5 to 3 servings every meal | Seaweeds: 30 g (cooked 1/5 cup) | |
| Fish meat | Fish, lean meat, eggs, tofu | Fish: 60 g (1 piece of medium-size fish) |
| 1 to 2 servings every meal | Lean meat: 60 g (1.5 ping-pong ball size) | |
| Eat blue-backed fish 2 to 3 times a week | Eggs: 60 g (1 medium-sized egg) | |
| Tofu: 80 g (1/5 block) | ||
| Fruits | Fresh fruit | 1 serving: 100 g (1/2 of medium-sized apple) |
| 1 to 2 servings a day |
Fig. 7. Dietary guideline for prevention and treatment dyslipidemia.

Physical activity: recommendation
| Content | Strength of recommendation | Level of evidence |
| Physical activities should be increased. | I | A |
| Regularly perform at least 30 minutes of moderate-intensity aerobic exercise 4 to 6 times a week. | I | A |
| Regularly perform resistance exercise at least twice a week. | IIa | B |
| For individuals with multiple risk factors or CVD, a medical assessment should be made before beginning exercise. | I | A |
Exercise and dyslipidemia
Whether c lipid level is controversial. This is because various results have been reported depending not only on the subjects' sex, age, race, and lipid concentration but also on the type, amount, intensity, duration, and frequency of exercise, as well as on whether lifestyle and body weight changed with regular exercise.58 Furthermore, exercise itself has little effect on lipid concentrations.
There are different types of exercise, including aerobic, resistance, and flexibility exercises. Aerobic exercise is a type of exercise that increases the body's oxygen consumption during exercise and improves cardiopulmonary endurance. Some examples include speed walking, jogging, swimming, and cycling. Resistance exercise refers to exercise in which muscle strength is used to work against a weight or force, and this type of exercise increases muscle strength and muscle mass. Flexibility exercise increases the range of motion of major muscles and improves postural stability and balance through muscle stretching.
In general, aerobic exercise decreases triglyceride concentration while increasing HDL-C, with little changes to LDL-C concentration.59,60 There is no debate in that exercise therapy prevents CVD, and CVD prevention is the major goal of dyslipidemia management. Therefore, exercise therapy is important for patients with dyslipidemia.58,61 Exercise has been reported to lower the risk of CVD as well as CVD mortality and all-cause mortality by not only improving lipid metabolism but also stabilizing blood pressure, improving insulin sensitivity, improving inflammation indices, lowering body fat, strengthening cardiopulmonary capacity, improving cardiac muscle function, promoting ischemic pre-conditioning of cardiac muscles, improving vascular endothelial functions, improving myocardial flow, and having anti-thrombotic effects.62,63
The effects of resistance exercise on lipids have been debated.64,65 However, resistance exercise could be useful because increasing muscle mass and muscle strength can increase physical activities and improve activities of daily living in the elderly.58
Exercise prescription
There is no particular exercise prescription for controlling dyslipidemia and the prescriptions are similar to those for CVD prevention.58,63,66 In general, at least 150 minutes of moderate intensity aerobic exercise per week is recommended.63 Exercise should be performed 4 to 6 days a week and at moderate intensity, which is about 55% to 75% of the maximum heart rate (=220−age) is appropriate. However, CVD patients taking β-blockers or non-dihydropyridine calcium channel blockers that markedly lower heart rate must not use the target heart rate. For these patients, the intensity should be set through an exercise stress test, but if no exercise stress test was performed, exercise should be started at a “moderate” level and maintained at “somewhat hard” level. Exercise should consist of 5 to 10 minutes of stretching and light walking as warm-up and 30 to 60 minutes of main aerobic exercise. Each session could be divided into shorter durations depending on one's abilities. After exercise, a cool down with 5 to 10 minutes of light walking and stretching is needed (Table 8).
Table 8. Summary of exercise therapy for patients with dyslipidemia.
| Type and order of exercise | Exercise intensity | Exercise duration | Exercise frequency |
|---|---|---|---|
| Warm-up: light walking after stretching | 55% to 75% of maximum heart rate | Warm-up: 5–10 min | 4–6 days/week |
| Main exercise: speed walking, power walking, cycle ergometer, stepper, cyclone, light hiking | Main exercise: 30–60 min | ||
| Cool-down: stretching after light walking | Cool-down: 5–10 min |
Resistance exercise should be performed twice a week, but intensity should be set according to age and conditions. In general, it is recommended to perform 8 to 10 exercise involving major muscle groups for at least 1 set of 8 to 12 repetitions each.61,63
Smoking cessation: recommendation
| Content | Strength of recommendation | Level of evidence |
| Smoking cessation is strongly recommended, as smoking increases the risk for dyslipidemia and CVD. | I | A |
Smoking increases plasma free fatty acid levels through enhanced lipolysis, which results in insulin resistance. Furthermore, smoking impairs reverse cholesterol transport.67,68,69 According to a meta-analysis, total cholesterol, triglyceride, VLDL-C, and LDL-C concentrations are 3%, 9.1%, 10.4%, and 1.7% higher, respectively, and HDL-C concentration is 5.7% lower among smokers than among non-smokers.70 After quitting smoking, blood HDL-C is significantly increased.71,72
Smoking is a strong risk factor for CVD. The risk associated with smoking is related to the amount of smoking with no lower limit for deleterious effects.73 Reducing the amount of smoking is not recommended, as it does not increase the possibility of smoking cessation and actually makes it more difficult to quit smoking.74 Furthermore, passive smoking also increases the risk of CVD.75 A meta-analysis and RCT confirmed that smoking cessation lowers the incidence and mortality of CVD.76,77
Therefore, smoking cessation is strongly recommended to prevent dyslipidemia and CVD.
PHARMACOLOGICAL THERAPY FOR DYSLIPIDEMIA
Guideline summary of pharmacological therapy for dyslipidemia
| Content | Strength of recommendation | Level of evidence | |
| 1 | The primary goal of dyslipidemia treatment is to lower LDL-C. | I | A |
| 2 | Non-HDL-C can be controlled as a secondary goal after achieving the targeted LDL-C concentration. | II | A |
| 3 | Appropriate statin administration should be considered for high-risk and very high-risk groups in order to meet the LDL-C target. | IIa | B |
| 4 | Statin should be considered to use for low-risk or moderate-risk groups when LDL-C level is not reduced to the target even after weeks and months of lifestyle modification. | IIa | B |
| 5 | Ezetimibe or bile acid sequestrants should be considered for patients with statin intolerance. | IIa | B |
| 6 | Combination with ezetimibe should be considered if LDL-C target is not achieved even after using maximum tolerable dose of statin | IIa | B |
| 7 | PCSK9 inhibitors may be considered to concurrent use for the very high-risk group if LDL-C target is not achieved even after using maximum tolerable dose of statin alone or with ezetimibe. | IIb | A |
| 8 | Bile acid sequestrants may be considered if LDL-C target is not achieved even after administering statin. | IIb | C |
| 9 | Combination of statin and nicotinic acid is not recommended to achieve the LDL-C target. | III | A |
| 10 | If the targeted level is not achieved even after using statin alone or with other agents in the very high-risk group, reducing LDL-C by 50% of the baseline concentration is recommended. | I | A |
| 11 | Administer statin immediately for patients with acute myocardial infarction regardless of the baseline LDL-C concentration. | I | A |
| 12 | For individuals with a triglyceride concentration of 500 mg/dL or higher, immediate drug therapy and lifestyle modification are important to prevent acute pancreatitis. | I | A |
| 13 | For individuals with a triglyceride concentration of 200–499 mg/dL, the primary treatment goal is to lower the LDL-C to the targeted level based on the calculated cardiovascular risk. | I | A |
| 14 | For individuals with a triglyceride concentration of 200–499 mg/dL, pharmacological therapy should be considered to lower triglyceride concentration after achieving the targeted LDL-C level if triglyceride concentration is >200 mg/dL with cardiovascular risk factors, or if non-HDL-C concentration is above the target. | IIa | B |
| 15 | If indicated, fibrates should be used to control triglyceride concentration. | I | B |
| 16 | If indicated, omega-3 fatty acids should be considered to control triglyceride concentration. | IIa | B |
| 17 | Combination drug therapy may be considered if targeted triglyceride level is not met after monotherapy. | IIb | C |
| 18 | The primary goal for low HDL cholesterolemia treatment is to control LDL-C to below the target. | I | A |
Selection of drugs
Pharmacological therapy in addition to therapeutic lifestyle modification, such as diet therapy, exercise, and smoking cessation, is important for the management of dyslipidemia. To determine whether to start drug therapy, a comprehensive consideration should be given to both the CVD risk and LDL-C level for each patient. The CVD risk is classified as low risk, moderate risk, high risk, and very high risk. Pharmacological therapy can be initiated according to established history of CAD, peripheral artery disease, and ischemic stroke and patients with atherosclerotic artery disease (aortic aneurysm, transient ischemic attack, carotid artery disease with significant stenosis) or diabetes as well as to the number of CAD risk factors (smoking, hypertension, low HDL cholesterolemia, family history of premature CAD, age). Statin is the first line drug for hypercholesterolemia and the dosage is recommended to be adjusted to reach the target LDL-C level. The primary treatment goal is to lower the LDL-C to the target level or below and the secondary goal is to lower non-HDL-C concentration to target or below. Prior to drug therapy, it is important to investigate and correct secondary causes that may increase LDL-C or triglyceride levels (Table 9). Table 10 describes selection of drugs according to dyslipidemia treatment standard.
Table 9. Potential causes of secondary hypercholesterolemia or hypertriglyceridemia.
| LDL-C elevation | Triglyceride elevation | |
|---|---|---|
| Diet | Saturated fat intake | Drinking |
| Trans fat intake | Excessive energy intake | |
| Excessive energy intake | High carbohydrate diet | |
| Drugs | Diuretics | Oral estrogen, glucocorticoid, bile acid sequestrant, proteolytic enzyme inhibitor, retinoic acid, anabolic steroid, sirolimus, raloxifene, tamoxifen, β-blocker, thiazide diuretic |
| Glucocorticoids | ||
| Amiodarone | ||
| Cyclosporin | ||
| Disease | Obstructive liver disease | Chronic kidney disease |
| Nephrotic syndrome | Nephrotic syndrome | |
| Anorexia nervosa | Sepsis | |
| Metabolic disorder | Obesity | Obesity |
| Pregnancy | Pregnancy | |
| Hypothyroidism | Uncontrolled diabetes |
LDL-C, low density lipoprotein cholesterol.
Table 10. Drug selection according to dyslipidemia treatment standard (primary goal: LDL-C, secondary goal: non-HDL-C).
| Dyslipidemia classification | Order | Type of drug | Method of administration | Strength of recommendation | Level of evidence |
|---|---|---|---|---|---|
| Hypercholesterolemia | Basic drugs | Statin | Adjust dose according to CVD risk to meet target LDL-C (when meeting target is difficult for high-risk and very high-risk groups, adjust dose to lower LDL-C by >50% of the baseline) | I | A |
| Other drugs | Bile acid sequestrant, ezetimibe | IIa | B | ||
| Combination therapy | Statin+ezetimibe | IIa | B | ||
| Statin+bile acid sequestrant | IIb | C | |||
| Statin (±ezetimibe)+PCSK9 inhibitor | Statin (±ezetimibe) for very high-risk group when target LDL-C is not met even with statin monotherapy or statin/ezetimibe therapy | IIb | A | ||
| Hypercholesterolemia+hypertriglyceridemia | Monotherapy | Statin | I | A | |
| Combination therapy | Statin+fibrate | IIa | A | ||
| Statin+gemfibrozil | III | B | |||
| Statin+omega-3 fatty acid | IIa | C | |||
| Hypertriglyceridemia | Basic drugs | Fibrate | I | B | |
| Omega-3 fatty acid | IIa | B | |||
| When drug therapy is considered for hypo-HDL cholesterolemia | Basic drugs | Statin, fibrate | IIb | B |
LDL-C, low density lipoprotein cholesterol; HDL-C, high density lipoprotein cholesterol; CVD, cardiovascular disease; PCSK9, proprotein convertase subtilisin/kexin type 9.
Hypercholesterolemia
The major independent risk factor associated with improved prognosis in patients with dyslipidemia and CVD is the reduction of LDL-C. Statin has been proved to lower CVD morbidity and mortality in both primary and secondary prevention studies, and according to a meta-analysis, CVD mortality, cardiovascular events, and stroke decreases by 20%, 23%, and 17%, respectively, with every 39 mg/dL reduction of LDL-C.27 Statin is the primary pharmacological agent for hypercholesterolemia, and the dose should be adjusted based on the patient's CVD risk to meet the targeted LDL-C level (I, A).24,78,79
Very high-risk group are the patients with atherosclerotic CVD (CAD, peripheral artery disease, ischemic stroke, transient ischemic attack) are classified as the very high-risk group. For this group, the goal of treatment is to reduce LDL-C concentration to <70 mg/dL or by more than 50% of the baseline for secondary prevention. Statin should be immediately administered regardless of baseline LDL-C concentration for patients with acute MI as well as patients who underwent revascularization therapy due to atherosclerotic ischemic heart disease. For the very high-risk group, use of PCSK9 inhibitors was proven to have cardiovascular protective effects, so PCSK9 inhibitors may be additionally used if the target LDL-C concentration is not achieved even after using maximum tolerable dose of statin and ezetimibe (IIb, A).30,80
High-risk group includes the patients with significant carotid artery disease, abdominal aneurysm, and diabetes. Statin treatment should be started if LDL-C is ≥100 mg/dL, and could be selectively considered even for patients with an LDL-C level of <100 mg/dL. For patients with diabetes with target organ damage or major cardiovascular risk factors, the degree of risk could be elevated depending on the patient.
Moderate-risk group includes the patients with two or more CV risk factors. For these patients, statin therapy should be started when LDL-C is ≥130 mg/dL but could be started even for those with LDL-C level 100 to 129 mg/dL when patients have multiple CV risk factors.
Low-risk group includes the patients with one or fewer risk factors, stain therapy may be used if the patient's LDL-C is ≥160 mg/dL. Drug therapy is used for the low-risk or moderate-risk group if LDL-C concentration level persists to be above the treatment cut-off despite weeks or months of therapeutic lifestyle modification (IIa, B). Pharmacological treatment strategy for hypercholesterolemia is as follows (Fig. 8).
Fig. 8. Drug therapy strategy for hypercholesterolemia. LDL-C, low density lipoprotein cholesterol.

Hypertriglyceridemia
When triglyceride concentration is high, it is recommended to first determine whether there are other factors increasing triglycerides and then to establish the treatment plan by evaluating the cardiovascular risks (Table 9). For individuals with a triglyceride concentration of 500 mg/dL or higher, immediate drug therapy (I, A) and lifestyle modification are important to prevent acute pancreatitis. Life style modification in these patients need to change to a low-fat diet (reduce fat intake to 10% to 15% of total energy intake) and complete abstinence from alcohol. In addition, pharmacological therapy should be started, particularly using fibrate (I, B) or omega-3 fatty acids (IIa, B), which lower triglyceride levels.81,82,83 For patients with diabetes, strictly regulating blood glucose level using insulin is helpful.
When the triglyceride level is between 200 to 499 mg/dL, the primary treatment goal is to lower the LDL-C to below the target on the basis of the calculated cardiovascular risk (I, A) and the secondary goal is to lower non-HDL-C to below the target (IIa, A). Therapeutic lifestyle modification and statin therapy should be considered (I, A). After achieving the target LDL-C goal through therapeutic lifestyle modification and statin therapy, when the triglyceride concentration is still >200 mg/dL or non-HDL-C, triglyceride lowering drug therapy may be considered (IIa, B). Fibrate (I, B) or omega-3 fatty acids (IIa, B) should be used to control triglyceride levels, especially in high-risk and very high-risk groups.82.83 If the target triglyceride goal is not met with monotherapy, combination therapy may be considered (IIa, C).84
Low HDL cholesterolemia
Low HDL cholesterolemia is defined as HDL-C levels <40 mg/dL. It is often observed in patients with type 2 diabetes, mixed dyslipidemia, chronic kidney disease, chronic liver disease, and autoimmune disease. Low HDL cholesterolemia is often found with hypertriglyceridemia. Low HDL cholesterolemia should be considered when assessing the overall CAD risk. In the Korean National Health and Nutritional Examination Survey from 1998 to 2010, hypertriglyceridemia and low HDL cholesterolemia are more common than hypercholesterolemia.85 The primary treatment goal for low HDL cholesterolemia is to lower the LDL-C to the target level based on the patient's CV (I, A). To increase HDL-C while lowering the LDL-C to the target, therapeutic lifestyle modification, such as smoking cessation, weight loss, and exercise, should be concurrently performed. In patients with low HDL cholesterolemia in the very high-risk or high-risk group, the use of agents that elevate HDL-C, such as fibrate or nicotinic acid, may be considered after controlling LDL-C, but the additional cardiovascular protective effects of these agents when combined with statin have not been confirmed in prospective randomized primary and secondary prevention studies. In particular, nicotinic acid products are not currently available in South Korea and treatment to elevate HDL-C is no longer recommended (III, A).
Characteristics of lipid-lowering drug
Statin: 3-hydroxy-3-methyl-glutaryl coenzyme A reductase inhibitor
Statin is currently recommended as the first-line pharmacologic agent among other therapeutic agents, as it has relatively few adverse effects and clearly is beneficial for reducing CVD by lowering LDL-C.86
Mechanism of action
All statins decrease cholesterol synthesis by competitively inhibiting the cholesterol precursor, 3-hydroxy-3-methyl-glutaryl coenzyme A (HMG-CoA) reductase.87 To maintain cellular cholesterol homeostasis, LDL receptors are elevated while cholesteryl ester formation is decreased. As a result, blood LDL-C is further removed and VLDL production in the liver is diminished, consequently lowering LDL. Statins not only block cholesterol synthesis but also inhibit the synthesis of lipid intermediates, which have important biological effects. Lipid intermediates, such as geranylgeranyl pyrophosphate and farnesyl pyrophosphate prenylate proteins, enable them to be attached to the cellular membrane and promote the biological activity of these molecules. One of the mechanisms through which statin increase HDL-C is by inhibiting the phosphorylation of peroxisome proliferator-activated receptor α, which regulates geranylgeranylation of Rho A and apo A1 transcription. Altering the prenylation of a protein appears to partially mediate the statin effects other than their LDL-C-lowering effect.
Types of statin
Seven types of stains, namely lovastatin, pravastatin, simvastatin, fluvastatin, atorvastatin, rosuvastatin, and pitavastatin, are currently used (Table 11).
Table 11. Lipid-controlling efficacy and pharmacological features of currently used statins.
| Lovastatin | Pravastatin | Simvasattin | Fluvastatin | Atorvastatin | Rosuvastatin | Pitavastatin | ||
|---|---|---|---|---|---|---|---|---|
| Daily dose, mg | 20–40 | 10–40* | 20–40 | 20–80 | 10–80 | 5–20† | 1–4 | |
| LDL-C reduction, % | ||||||||
| 24–28 | 20 | 20 | 40 | 1 | ||||
| 30–36 | 40 | 40 | 20 | 80 | 10 | 2 | ||
| 39–45 | 80 | 40 | 20 | 5–10 | 4 | |||
| 46–52 | 40–80 | 20 | ||||||
| Metabolism | CYP3A4 | sulfonation | CYP3A4 | CYP2C9 | CYP3A4 | CYP2C9 | Glucuronidation (partial CYP2C9) | |
| Protin binding, % | >95 | 43–67 | 95–98 | 98 | 98 | 88 | >99 | |
| Half-life, hr | 2–4 | 2–3 | 1–3 | 0.5–3 | 13–30 | 19 | 12 | |
| Hydrophilicity | − | + | − | − | − | + | − | |
| Elimination | Hepatobiliary | Hepatobiliary | Hepatobiliary | Hepatobiliary | Hepatobiliary | Hepatobiliary | Hepatobiliary | |
| Renal elimination fraction, % | 10 | 20 | 13 | <6 | <2 | 28 | 15 | |
LDL-C, low density lipoprotein cholesterol; CYP, cytochrome P450.
*40–80 mg in Caucasian countries.
†5–40 mg in Caucasian countries.
Lipid-lowering effects
Statins vary in absorption, blood protein binding, elimination, and solubility and the LDL-C lowering effects also vary according to dose (Table 11).85,88,89,90,91 In general, increasing statin dose twofold decreases blood LDL-C by 6%. Furthermore, statin inhibits VLDL-C secretion in the liver, thus it lowers triglyceride levels by 22% to 45% in patients with hypertriglyceridemia. HDL-C is slightly (5% to 10%) elevated. Multiple studies on Koreans have reported the effects of each type of statin on lipid indices and some studies have shown that the same dose of statin leads to a greater reduction of LDL-C among Koreans than among foreigners (Figs. 9 and 10).92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113
Fig. 9. Comparison of low density lipoprotein cholesterol (LDL-C) reduction effects of statins between foreigners and Koreans.75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96 Modified from Cholesterol Treatment Trialists' (CTT) Collaboration et al.27.

Fig. 10. Korean data on the lipid-controlling efficacy of currently used statins.75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94 LDL-C, low density lipoprotein cholesterol.

Cardiovascular disease prevention research and indications
1) Secondary prevention of CVD
Patients with a history of CVD (angina, unstable angina, MI, stroke, transient ischemic attack) are known to be more vulnerable to relapse of cardiovascular event or mortality.102,103,104 For these patients, it is recommended to use statins because these drugs prevent the recurrence of cardiovascular events (I, A).24,36,114 These patients are classified as a very high-risk group, and the goal is to reduce LDL-C to <70 mg/dL or by >50% of the baseline for secondary prevention. If MI occurs, immediately administer statin regardless of the baseline LDL-C concentration (I, A). Although there are not many large studies on Asians, preventive effects were greater in CVD patients younger than 75 years old for whom LDL-C was reduced by more than 30% to 50% using statin than in the group of patients whose LDL-C was reduced by a lesser degree using a different dose of statin. Therefore, it is recommended that moderate dose/moderate intensity or high dose/high intensity statin be used such that the baseline LDL-C concentration can be reduced by more than 30% to 50% (IIa, A).24,27,115
For CVD patients age >75 years or older, statin therapy should be used after confirming potential interactions with the patient's comorbidity or between drugs used (IIa, B).24,116
2) Primary preventive effects of CVD in the general population
Adults with a blood LDL-C concentration of 190 mg/dL or higher are likely to develop a CVD in their lifetime, so statin should be used if the blood LDL-C remains >190 mg/dL even after appropriate lifestyle modification (I, A).24,86,117,118
For adults with blood LDL-C of 160 to 190 mg/dL, statin should be used if blood LDL-C remains >160 mg/dL even after 4 to 8 weeks of appropriate lifestyle modification (IIa, B).24,27
For adults with blood LDL-C of 130 to 160 mg/dL, appropriate lifestyle modification should be made, and statin therapy should be determined to start in consideration of the risk for CVD (IIb, C).24,27,119,120
3) Primary preventive effects of CVD in patients with diabetes
Patients with diabetes, carotid artery disease or aortic aneurysm are considered as high risk group. For these patients, statin treatment should be started for primary prevention when LDL-C is >100 mg/dL (I, A).24,117
4) Effects of statin in patients with heart failure and patients undergoing hemodialysis
Statin does not have any preventive effects in patients with heart failure or in hemodialysis patients, so newly adding statin therapy is not recommended for patients beginning hemodialysis (III, B).24
Usage-dosage
Lovastatin: 20 to 80 mg/day, taken with dinner
Pravastatin: 10 to 40 mg/ day, evening administration is more effective
Simvastatin: 20 to 40 mg/ day, evening administration is more effective
Fluvastatin: 20 to 80 mg/day, evening administration is more effective
Atorvastatin: 10 to 80 mg/day, time of administration is not significantly relevant
Rosuvastatin: 5 to 20 mg/day, time of administration is not significantly relevant
Pitavastatin: 1 to 4 mg/day, time of administration is not significantly relevant
Adverse reactions
The most common adverse reactions are indigestion, heartburn, and abdominal pain, which occur in 4% and hepatotoxicity and muscle toxicity are rare but may be fatal.114 For older adults aged ≥75 years, patients taking multiple drugs, particularly when taking drugs with the same metabolic pathway with statin, or in patients with comorbidities requiring multidrug therapy, such as heart transplantation/acquired immune deficiency syndrome, it is helpful to begin with a low dose and gradually increase the dose (IIa, C).
1) Hepatotoxicity: There is no need to stop drug administration when transaminase is slightly elevated. If transaminase is increased by more than three times the normal range, stop administration, and once normal levels are restored, restarting statin with a low dose or use another agent may be considered (IIb, C). If symptoms suggesting liver injury, such as fatigue, reduced appetite, abdominal pain, dark urine, and jaundice, manifest during statin therapy, liver function tests, including aspartate transaminase/alanine transaminase (AST/ALT), should be performed promptly (IIa, C).24
2) Muscle toxicity: The most common adverse reaction to statin is muscle pain.114 About 10% of patients taking statin develop muscle pain and weakness and stop taking statin, but in many cases, it is uncertain whether the muscle symptoms are indeed caused by statin.121 The incidence of muscle injury is reported to be 0.01% higher in the statin group than that in the control group. It is reported that muscle injury, defined as elevated muscle enzymes, rhabdomyolysis, hemoglobinuria, and acute kidney failure, occur in a small minority of patients. The risk for statin-induced muscle damage increases with multiple comorbidities or when statin is combined with cyclosporine, fibrate, macrolide antibiotics, and some antifungal agents.122 Gemfibrozil especially increases the risk of muscle damage when combined with statin, but fenofibrate is known to have low risk. Regular measurement of muscle enzyme levels is not recommended for asymptomatic patients, as it has shown no benefits (III, A).24 However, for patients with muscle pain, stiffness, muscle knots, weakness, and general fatigue, it is recommended to check for muscle injury by measuring muscle enzyme levels (IIa, C).24
3) Diabetes: A recent study reported that statin increases new onset diabetes.120 Most new-onset diabetes occurred in individuals who had glucose intolerance prior to taking statin and there is a possibility that it may occur more frequently in patients who had taken a high-dose of statin. Thus, checking fasting blood glucose is helpful prior to beginning statin therapy (I, B).24 Even for patients who developed diabetes after beginning statin therapy, it is better to continue taking statin and make necessary lifestyle modification, such as exercise, weight reduction, and smoking cessation, than to stop statin therapy altogether in order to prevent CVD (I, B).24
4) Cognitive impairment: There has been some report that cognitive impairment was observed among patients taking statin. Nonetheless, to date, it is more beneficial to check for adverse reactions of combined neuropsychiatric medications than to conclude that cognitive impairment is an outcome of statin administration (IIb, C).24
Contraindications
Active or chronic liver disease is an absolute contraindication. Statin administration should be stopped immediately once pregnancy is confirmed or in lactating woman. Combination with cyclosporin, macrolide antibiotics, antifungal agents, and cytochrome P-450 inhibitors is a relative contraindication and must be determined with caution.
Follow-up observation before and after statin therapy
1) Pre-test: Prior to statin therapy, blood transaminase concentration (AST/ALT) should be measured (I, B).24 If ALT concentration is 3 times higher than the normal range prior to therapy, statin therapy should be initiated only after assessing and treating liver disease and confirming that liver functions have been improved [24]. Muscle enzyme CK should be measured as well, and if the concentration is three times higher than the normal range, identify the cause first and decide on whether to begin statin therapy.24
2) Follow-up test after statin therapy: Assess cholesterol, triglyceride, and HDL levels about 4 to 12 weeks after statin therapy (I, B). If LDL-C is <40 mg/dL in two consecutive measurements, consider lowering the dose of statin. Evaluation of liver function should be considered at 4 to 12 weeks after administration and every 3 to 12 months thereafter check statin effects and hepatotoxicity. Furthermore, the physician may prescribe a follow-up-test to ensure patient safety even in the absence of symptoms.24
3) Effects of cessation statin therapy: Blood LDL-C level rises again about 2 to 3 months later and reverts back to the pre-treatment levels.116 In addition, the CV protective effects of statin disappear from 1 to 2 days after stopping administration, so it is crucial to continue taking the drug. Particularly, multiple studies have reported that pausing statin therapy in the acute phase for patients with CVD, such as acute coronary artery syndrome or cerebral infarction, leads to poor outcomes.
Summary
| Statin: HMG-CoA reductase inhibitor | |
| Usage/dosage | Lovastatin: 20–80 mg/day, taken with dinner |
| Pravastatin: 10–40 mg/day, evening administration is more effective | |
| Simvastatin: 20–40 mg/day, evening administration is more effective | |
| Fluvastatin: 20–80 mg/day, evening administration is more effective | |
| Atorvastatin: 10–80 mg/day, time of administration is not significantly relevant | |
| Rosuvastatin: 5–20 mg/day, time of administration is not significantly relevant | |
| Pitavastatin: 1–4 mg/day, time of administration is not significantly relevant | |
| Follow-up test | Lipid profile, liver function test, muscle enzymes (when there is unexplainable muscle pain or muscle weakening) |
| Adverse reaction | Indigestion, heartburn, abdominal pain, hepatotoxicity, muscle toxicity, diabetes |
| Contraindication | Active or chronic liver disease, pregnancy, and breastfeeding are absolute contraindications. Combining with cyclosporin, macrolide antibiotics, antifungal agents, or cytochrome P-450 inhibitors is a relative contraindication and requires caution. |
Ezetimibe
Indications and action mechanism
Ezetimibe is commonly combined with statin therapy, as it lowers LDL-C by inhibiting cholesterol reabsorption in the small intestine (IIa, B).
Usage-dosage
Take 10 mg of ezetimibe once a day. There is no relevant time of administration.
Follow-up test
Blood lipid profile may be tested every 3 to 6 months.
Adverse reactions
The most common adverse reactions to ezetimibe monotherapy are abdominal pain, diarrhea, flatulence, and fatigue and other uncommon adverse reactions include indigestion, gastroesophageal reflux, reduced appetite, arthralgia, muscle spasm, and chest pain. In blood tests, elevation of transaminase, gamma-glutamyl transferase (GT), and CK have been reported.
Contraindications
Ezetimibe is prohibited for individuals who show hypersensitivity to this agent. It is also prohibited for pregnant and lactating women, as its safety has not been established. It is also prohibited for patients with acute liver disease or moderate to severe chronic liver dysfunction.
Summary
| Ezetimibe | |
| Usage/dosage | 10 mg once daily |
| Follow-up test | Lipid profile tests every 3–6 months |
| Adverse reactions | Abdominal pain, diarrhea, flatulence, fatigue, indigestion, gastroesophageal reflux, reduced appetite, arthralgia, muscle spasm, and chest pain |
| Elevated transaminase, gamma-GT, and CK | |
| Contraindications | Drug hypersensitivity (III, C) |
| Pregnancy and breastfeeding (III, C) | |
| Acute liver disease or moderate to severe chronic liver dysfunction (III, C) | |
Fibrate
Indications
Fibrate are used as monotherapy (I,B) or combination therapy with statin for hypertriglyceridemia (IIa,A).
Usage-dosage
Bezafibrate: 400 to 600 mg/day, 1 to 3 times a day, after meals
Fenofibrate: 160 to 200 mg/day, once a day, immediately after meals
Gemfibrozil: 600 to 1,200 mg/day, twice a day, 30 minutes before meals
Follow-up tests before and after treatment
Lipid profile, liver function test, kidney function test, general blood test, muscle enzymes (when there is unexplainable muscle pain or weakness)
Adverse reaction
The most common adverse reaction is indigestion, and cholesterol gallstones may occur more frequently. Myopathy may occur, but the incidence is not high. The risk for adverse reactions is elevated when kidney functions (estimated glomerular filtration rate [eGFR]) are reduced, as blood drug concentration is increased. In particular, combination therapy with gemfibrozil and statin increases the risk for myopathy. Fenofibrate is the preferred agent for combination therapy with statin, as it does not relatively increase the risk for myopathy. It binds to albumin, which increases warfarin concentration and, therefore, bleeding tendency, and it may also increase the effects of hypoglycemic agents.123
Contraindications
Severe liver disease, gallbladder disease, and hypersensitivity to fibrate is absolute contraindications, and use of the drug requires precaution for individuals with reduced kidney functions.123
Summary
| Fibrate | |
| Usage/dosage | Bezafibrate: 400–600 mg/day, 1–3 times a day, after meals |
| Fenofibrate: 160–200 mg/day, once a day, immediately after meals | |
| Gemfibrozil: 600–1,200 mg/day, twice a day, 30 minutes before meals (avoid combination therapy with statin) | |
| Follow-up test | Lipid profile, liver function test, general blood test, CK (when there is unexplainable muscle pain or muscle weakness) |
| Adverse reaction | Indigestion, cholesterol gallstones, myopathy |
| Contraindications | Severe liver disease, gallbladder disease, and hypersensitivity to fibrate is absolute contraindications, and use of the drug requires precaution for individuals with reduced kidney function |
Monoclonal antibody type PCSK9 inhibitors
Indications
For patients with familial hypercholesterolemia and the very high-risk group whose LDL-C levels do not reach target LDL-C level despite statin monotherapy with a maximum tolerable dose or statin and ezetimibe combination therapy, PCSK9 inhibitors may be combined with statin with or without ezetimibe (IIb, A).
Usage-dosage
Alirocumab: 75 or 150 mg via disposable pen or syringe
At first, subcutaneous injection of 75 mg in 2-week intervals or 300 mg in 4-week intervals. If not reached to target LDL-C level, dosage could be increased to 150 mg in 2-week intervals.
Evolocumab: 140 mg/mL via disposable syringe or automatic injector, or 420 mg/3.5 mL via disposable on-body infuser with a prefilled cartridge is injected subcutaneous in the abdomen, thigh, or upper arm (140 mg in 2-week interval or 420 mg in 1-month interval).
Inject 420 mg over 9 minutes using a disposable infuser or inject 140 mg three times consecutively within 30 minutes.
Follow-up test
Lipid profile, and liver function test every 3 to 6 months.
Adverse reactions
There may be adverse reactions in the injection site after subcutaneous injection of monoclonal antibody, but the reactions are generally mild, and other reactions include nasopharyngitis. PCSK 9 inhibitors are not known to increase hepatotoxicity, and compared to ezetimibe, there are is no elevation in muscle pain or CK levels. There are no known interactions with other drugs and adverse reactions from prolonged administration.
Contraindications
Hypersensitivity to alirocumab or evolocumab is an absolute contraindication.
Summary
| PCSK9 inhibitor | |
| Usage/dosage | Alirocumab: subcutaneous injection of 75 mg or 150 mg |
| Evolocumab: subcutaneous injection of 140 mg/mL in 2-week interval or 420 mg in 1-month interval | |
| Follow-up test | Lipid profile |
| Adverse reaction | Adverse reactions in the injection site |
| Contraindications | Hypersensitivity to alirocumab or evolocumab |
Omega-3 fatty acids
Indications
Omega-3 fatty acids may be used alone for hypertriglyceridemia (IIa, B) or combined with statin for mixed hyperlipidemia (IIa, C).
Usage-dosage
Dosage that showed lipid-reduction effects was 2 to 4 g a day. This dose should be taken at once or at two split times.
Follow-up test
Lipid profile and liver function tests every 3 to 6 months.
Adverse reaction
There have been some reports of the occurrence of hemorrhagic stroke, elevated blood glucose, and elevated immunosuppression.124,125,126,127,128,129,130,131,132 There have also been reports of nausea, vomiting, burps, fish-smelling burps, or fishy taste in mouth, as well as elevated liver indices, headache or itching, and arthralgia.
Contraindications
There are no contraindications other than hypersensitivity to the drug. The U.S. Food and Drug Administration classifies this drug as class C; thus, for pregnant women, the drug should be used only when there are clear benefits (II, C). Omega-3 fatty acids extracted from fish with incomplete purification or excessive intake pose a risk for heavy metal exposure, so it is not recommended for pregnant women. It is also not known if this drug is secreted in breast milk.
Summary
| Omega-3 fatty acids | |
| Usage/dosage | 2–4 g/day |
| Follow-up test | Lipid profile, liver function test every 3–6 months |
| Adverse reaction | Hemorrhagic stroke, elevated blood glucose, immunosuppression, nausea, vomiting, burp, fish-smelling burp, fishy taste in mouth, elevated liver indices, headache, itching, arthralgia |
| Contraindications | Hypersensitivity to drug |
Nicotinic acid (niacin)
To date, studies have not found significant improvements of clinical outcomes after nicotinic acid and statin combination therapy, and there were actually more adverse reactions.133 Furthermore, there is no approved product available in South Korea, and niacin and statin combination therapy is no longer recommended to increase HDL-C (III A).
Combination therapy
Adding another pharmacologic agent to statin can be considered if LDL-C remains high even after adequate statin administration and lifestyle modification or patient has mixed dyslipidemia.
Statin and ezetimibe combination therapy
Combination of statin and ezetimibe additionally lowers LDL-C by 15% to 20% compared to statin monotherapy. Ezetimibe (10 mg) and simvastatin (40 mg) combination therapy significantly reduced major cardiovascular events compared to simvastatin (40 mg) monotherapy in the Simvastatin and Ezetimibe in Aortic Stenosis (SEAS) study that assessed simvastatin/ezetimibe therapy in patients with asymptomatic aortic stenosis, in the Study of Heart And Renal Protection (SHARP) on patients with chronic kidney disease, and in the IMPROVE-IT on patients with acute coronary syndrome.24,33,134,135,136 As clinical trials proved, further lowering LDL-C by adding ezetimibe to statin therapy has benefits for improving clinical outcomes, so ezetimibe should be added if the target LDL-C goal is not met even with maximum tolerable dose of statin (IIa, B).
Statin and PCSK9 inhibitor combination therapy
PCSK9 inhibitors may be considered for very high-risk group if the target LDL-C is not met even with maximum tolerable dose of statin with or without ezetimibe or if the patient has statin intolerance. Two types of PCSK9 inhibitors, currently available evolocumab and alirocumab, lower LDL-C by 50% to 70% regardless of statin/ezetimibe therapy for hyperlipidemia.30,137,138 Furthermore, FOURIER study proved that the evolocumab group had a 59% reduction of LDL-C with 15% less risk of combined primary outcome, including cardiovascular mortality, MI, cerebral infarction, hospitalization due to unstable angina, and coronary artery intervention.30 Therefore, PCSK9 inhibitors may be combined with statin therapy for the very high-risk group if LDL-C remains high even after using maximum tolerable dose of statin (IIb, A).
Statin and fibrate combination therapy
In the Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) and ACCORD studies that studied of statin and fenofibrate therapy in patients with diabetes, statin and fibrate combination therapy did not significantly lower cardiovascular risk, the primary endpoint of the study. However, in a retrospective subgroup analysis, the total CVD incidence was 27% lower in the dyslipidemia group, who had high triglyceride and low HDL-C.46,139,140 Fibrate, when combined with statin, was found to be effective in lowering CVD risk in some high-risk patients with high triglyceride and low HDL-C levels; thus, additional studies are needed to prove the clinical efficacy. However, there may be an elevation of muscle-related symptoms and diseases as a result of fibrate and statin combination therapy, so clinicians should choose agents appropriately and be well aware of the indications.
Stain and bile acid sequestrant combination therapy
Combination of statin and bile acid sequestrants may be considered for achieving the target LDL-C goal. Adding bile acid sequestrants to statin therapy may additionally lower LDL-C by 10% to 20%. However, there has been no clinical trial assessing whether statin/bile acid sequestrant therapy decreases CVD, while a study using coronary artery angiography reported that it lowers atherosclerosis.141
Statin and omega-3 fatty acid combination therapy
These two agents are generally used when aiming to lower both LDL-C and triglyceride levels (IIa, C). In some early studies, combining low-dose statin with eicosapentaenoic acid decreased major cardiovascular events compared to statin monotherapy, but multiple subsequent studies could not observe significant reduction of mortality with use of alpha-omega, supplementation with folate, vitamin B6 and B12 and/or omega-3 fatty acids, and other studies also did not find significant improvements of outcome.83,142
Statin and niacin combination therapy
The “Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy,” the Atherothrombosis Intervention in Metabolic Syndrome with low HDL/HIGH Triglycerides (AIM-HIGH) Trial reported that statin and niacin combination therapy sufficiently controlled LDL-C in patients with CVD, but the study was prematurely terminated, as there were no significant improvements of outcomes in patients with atherogenic dyslipidemia after adding niacin (1.5 to 2 g/day) to statin therapy.133 However, this study also reported that it may lower CVD risk in patients with high triglyceride but low HDL-C levels. Unfortunately, niacin was associated with some adverse reactions such as elevated blood glucose, blushing, infection, and skin disease, and consequently, it became unavailable in some countries. Furthermore, the “Effects of extended-release niacin with laropiprant in high-risk patients,” HPS2-THRIVE study reported that adding niacin and facial flushing inhibitor laropiprant to statin therapy could not reduce major cardiovascular events and actually led to an increase of adverse reactions, such as myopathy, liver dysfunction, and increased risk of diabetes.143 Therefore, statin and niacin combination therapy is not recommended (III, A).
DYSLIPIDEMIA IN SPECIAL GROUPS
Dyslipidemia in stroke patients
Dyslipidemia's contribution to stroke varies across subtypes, and the association between dyslipidemia and ischemic stroke caused by atherosclerosis is the most well known. Dyslipidemia is an important risk factor for atherosclerotic ischemic stroke, and multiple clinical trials have shown that aggressive statin therapy can lower the incidence of stroke. Conversely, some cohort studies have also reported an association between low blood cholesterol levels and incidence and mortality of hemorrhagic stroke. Therefore, different approaches should be taken to treat dyslipidemia in stroke patients depending on the type of stroke involved.
Primary prevention of stroke and dyslipidemia
Elevated total blood cholesterol and LDL-C are risk factors for ischemic stroke and statin therapy is helpful for primary prevention of ischemic stroke.27,144 In summary,
(1) Statin therapy is recommended for primary prevention of ischemic stroke for patients with a vascular disease or those at a high risk of CVD. The target LDL-C goal is set according to the general recommendations.
(2) For patients with a vascular disease, statin/ezetimibe combination therapy may be used for primary prevention of ischemic stroke.
Secondary prevention of stroke and dyslipidemia
Statin therapy for secondary prevention of stroke is the most effective for atherosclerotic ischemic stroke, and its preventive effects are yet unclear for other subtypes of stroke.32,145 High-dose statin therapy has been associated with increased risk of bleeding in ischemic stroke patients with hemorrhagic stroke.32,146 Considering the large number of hemorrhagic stroke patients in Korea, high-dose statin therapy should be used carefully. Although research data on the goal of dyslipidemia treatment for secondary prevention in stroke patients is yet thin, aggressive LDL-C correction is important for atherosclerotic ischemic stroke.
In summary,
(1) Dyslipidemia must be corrected for ischemic stroke patients and for secondary prevention of ischemic stroke, lifestyle adjustment, dietary therapy, and pharmacologic therapy, particularly statin therapy are recommended.
(2) High-dose statin therapy is recommended for secondary prevention of stroke for patients with ischemic stroke, atherosclerotic ischemic stroke, or transient ischemic attack with CVD. The treatment goal is to lower LDL-C to < 70 mg/dL or by more than 50% of the baseline level.
Dyslipidemia in patients with chronic kidney disease
Early phase of chronic kidney disease is characterized by elevated levels of triglyceride, reduced HDL-C, and increased LDL, particularly small dense LDL particles. As renal function declines, the rate of LDL-C breakdown is further slowed and, consequently, total cholesterol and LDL-C levels are elevated.
Unlike patients with normal kidney function, the primary or secondary prevention effects of statin on CVD are yet unclear for patients with chronic kidney disease. The 2013 The Kidney Disease: Improving Global Outcomes (KDIGO) guidelines recommended to remove LDL-C as a criterion for assessing appropriateness of treatment target in the management of dyslipidemia for patients with chronic kidney disease and instead proposed the use of future cardiovascular risk (rates per 1,000 person years).147
Usage and dosage
The same pharmacologic agent/dose used for healthy counterparts is permitted for patients with chronic kidney disease with an eGFR of ≥60 mL/min/1.73 m2 (excluding patients who had kidney transplantation). There are no clear data on the safety of high-dose statin in patients with chronic kidney disease with an eGFR of < 60 mL/min/1.73 m2, and there may be potential adverse reactions. Hence, the documented dose in large-scale studies is recommended for these patients (Table 12).135,148,149,150
Table 12. Recommended statin dosage for adult patients with chronic kidney disease (mg/day) (KDIGO)*.
| Statin | eGFR G1–G2 | eGFR G3a–G5, including patients on dialysis or with a kidney transplant |
|---|---|---|
| Lovastatin | GP† | ND |
| Pravastatin | GP | 40 |
| Simvastatin | GP | 40 |
| Simvastatin/ezetimibe | GP | 20/10 |
| Atorvastatin | GP | 20 |
| Fluvastatin | GP | 80 |
| Rosuvastatin | GP | 10 |
| Pitavastatin | GP | 2 |
KDIGO, Kidney Disease Improving Global Outcomes; eGFR, estimated glomerular filtration; GP, general population; ND, not done or not studied.
*KDIGO (2013).
†Any dose approved for general population.
Approach to dyslipidemia in patients with chronic kidney disease
There is no direct evidence that performing blood lipid test at the time of diagnosis with chronic kidney disease is helpful for the patient's outcomes. However, blood lipid testing is recommended, as it is relatively cheap and is helpful for detecting and distinguishing secondary dyslipidemia, such as that caused by hypothyroidism, excessive drinking, nephrotic syndrome, diabetes, liver disease, and use of other corticosteroid. Uniform and regular follow-up tests for LDL-C are not recommended after the diagnosis of chronic kidney disease. However, individual follow-up tests may be needed depending on the patient, such as for assessing patient adherence, considering change of dialysis method, diagnosing other secondary dyslipidemia, or assessing 10-year cardiovascular risk in patients under the age of 50 to begin statin therapy.
Cholesterol-lowering drug therapy in adult patients with chronic kidney disease
Regarding cholesterol-lowering therapy for patients with chronic kidney disease, the 2011 guidelines by ESC/EAS stresses that chronic kidney disease is considered a CAD risk equivalent and lowering LDL-C is the primary treatment goal for these patients.151 The 2013 KDIGO guidelines suggest classifying individuals with a 10% or higher 10-year risk for coronary death or non-fatal MI as the statin therapy group.147 Among patients with chronic kidney disease, those aged 50 years or older are recommended to undergo statin/ezetimibe or statin monotherapy regardless of their eGFR. For patients under the age of 50 years, statin or statin/ezetimibe is recommended if the patient has a history of CAD, diabetes, or ischemic stroke or if the 10-year risk for CAD mortality or non-fatal MI exceeds 10%.
For patients with chronic kidney disease requiring maintenance dialysis, newly adding statin therapy is not recommended, as statin was not found to have significant effects in three large-scale prospective randomized controlled studies.135,149,150 Although it is not clear whether individuals on statin therapy prior to dialysis should stop statin therapy, it is necessary to analyze the risk/effects for continuing statin in consideration that statin is less effective on these patients compared to non-dialysis patients.
Among patients with chronic kidney disease who had a kidney transplantation, the incidence of CAD is very high compared to that of the normal population, at about 21.5 events/1,000 patient-year.148 In the same study, fluvastatin reduced, though statistically insignificant, the incidence of CAD by 17% in those patients. For the treatment of lipid abnormality, statin is the recommended first-line treatment, but it should be started at a low dose and be increased gradually. Considering pharmacologic interactions, fluvastatin and pravastatin are recommended for transplant patients taking cyclosporine.6
Triglyceride-lowering drug therapy for adult patients with chronic kidney disease
Therapeutic lifestyle modification should be considered first. Using fibric acid derivatives, which had been recommended in previous guidelines for the prevention of pancreatitis, is no longer recommended, as the supporting evidence is very weak. However, fibric acid derivatives may be considered for those with a fasting triglyceride of ≥1,000 mg/dL, and if used, the dose should be appropriately adjusted depending on the patient's kidney functions. In such cases, patients are considered at a high risk for adverse reactions, so combination therapy with statin is not recommended. A large meta-analysis on the general population reported that fibrate therapy decreased major cardiovascular events and coronary events by 10% and 13%, respectively.45 However, the effects are relatively weak compared to that of statin, and it elevates serum creatinine levels; thus, fibrate is not recommended for the purpose of lowering cardiovascular risks for those with chronic kidney disease.152 In addition to pharmacological therapy, non-pharmacological therapy, such as dietary therapy, weight loss, increasing physical activity, lowering alcohol consumption, and blood glucose control, should be performed.
Adverse reactions and contraindications
Statin therapy in patients with stage 3 or higher chronic kidney disease may increase the risk of adverse reactions such as drug overdose and increased blood drug concentration, so choosing pharmacologic agents with low renal excretion is desirable (Table 11).153 Furthermore, using drugs that are not metabolized by CYP-3A4 enzymes would lower adverse reactions caused by drug interactions.
In general, fibric acids are not recommended for patients with chronic kidney disease, but they may be considered in special cases. In such cases, the dosage should be adjusted based on patient's renal functions, and it should be noted that fibric acids may increase serum creatinine levels and that combining with statin may increase the risk of rhabdomyolysis.154,155
Dyslipidemia in patients with diabetes
| Content | Strength of recommendation | Level of evidence |
| Patients with diabetes are recommended to take blood lipid test at the time of diagnosis and every year thereafter. | I | E |
| In addition to the routine lipid testing (total cholesterol, HDL-C, LDL-C, triglyceride), non-HDL-C or apoB may be measured to assess diabetic dyslipidemia. | IIa | A |
| In diabetic patients without CVD, the recommended target for LDL-C is <100 mg/dL. | I | A |
| In diabetic patients with CVD risk factors or target organ damage such as albuminuria and chronic kidney disease, an LDL-C target of <70 mg/dL should be considered. | I | B |
| Patients with diabetes and dyslipidemia must engage in aggressive lifestyle modifications. | I | A |
| Strict glycemic control is helpful to control hypertriglyceridemia. | I | C |
| Statin is the first line treatment for patients with diabetes and dyslipidemia. | I | A |
| If statin therapy is not sufficient to achieve the target LDL-C goal in patients with diabetes and CVD, adding ezetimibe should be considered. | IIa | B |
| If statin therapy is not sufficient to achieve the target LDL-C goal in patients with diabetes and CVD, adding PCSK9 inhibitors may be considered. | IIb | B |
The risk of CVD is substantially increased with metabolic syndrome or diabetes, and CVD is one of the leading causes of death among patients with diabetes.156 Because CVD mortality is about two to four times higher among patients with diabetes than among those without diabetes, dyslipidemia in these patients should be treated aggressively.157
Typical diabetic dyslipidemia is characterized by hypertriglyceridemia and decreased HDL-C. Furthermore, it is associated with an increased risk of atherosclerosis even without a high LDL-C, as small and dense LDL particles increase. Therefore, patients with diabetes are recommended to measure a lipid profile at the time of diagnosis and every year thereafter. In addition to the routine lipid tests (total cholesterol, HDL-C, LDL-C, triglyceride), non-HDL-C or apoB may be measured to assess diabetic dyslipidemia.158
The present guidelines for the management of dyslipidemia classifies patients with CVD as the very high-risk group regardless of diabetes and recommends aggressive regulation of LDL-C to <70 mg/dL for this group. For patients with diabetes without CVD, the goal of LDL-C <100 mg/dL is recommended, but for those patients with CVD risk factors or target organ damage, such as proteinuria and chronic kidney disease, the target LDL-C may be further lowered to <70 mg/dL.
Patients with diabetes and dyslipidemia need to engage in aggressive lifestyle modification.159 Individualized education needs to be applied to each patient. For patients with diabetes who have poor glycemic control and high triglyceride levels, optimizing glycemic control is helpful for controlling dyslipidemia. Statin is the first-line treatment for patients with diabetes and dyslipidemia. In a study on patients with diabetes, statin therapy significantly contributed to both primary and secondary prevention of CVD.160,161 If the target LDL-C goal is not met with the general statin dose, the dose should be increased to maximally tolerable dose or be substituted by high-intensity statins. Discontinuation of therapy was found to aggravate dyslipidemia in type 2 diabetes, so maintenance therapy is crucial, and confirming the continuity of medication is also essential.162
Whether lowering triglyceride and increasing HDL-C with statin/fibric acid derivative therapy are beneficial for patients with type 2 diabetes is controversial. The ACCORD study found that statin/fibric acid derivative therapy did not significantly lower the incidence of CVD compared to statin monotherapy. However, in a subgroup analysis, the ACCORD study suggested that statin/fibric acid derivative therapy may have CVD preventive effects in patients with triglyceride ≥200 mg/dL and an HDL-C <34 mg/dL.50,163
In the IMPROVE-IT conducted on 18,144 patients who were admitted for acute coronary syndrome within 10 days of the study, simvastatin/ezetimibe therapy reduced relative risk for CVD by 6.4%. In the subgroup analysis, relative risk was reduced by 14% in the diabetes group, showing a greater CVD preventive effect among patients with diabetes.29 Adding PCSK9 inhibitors, namely evolocumab or alirocumab, to patients with high CVD risk who are using maximum statin dose lowered LDL-C by 36% to 59%.164,165 Based on these studies, adding ezetimibe or PCSK9 inhibitor may be considered for patients with diabetes and CVD if the target LDL-C goal is not met with maximum tolerable dose of statin.
Older adults and dyslipidemia
South Korea has already become an aged society in 2017, as the older adult population (≥65 years) reached 14% of the total population and it is expected to become a super-aged society by 2026, with the older adult population estimated to exceed 20%.166 As a result of the growing elderly population, the prevalence and mortality of CVD are also expected to rise continuously. In particular, the prevalence of dyslipidemia increases among the elderly and many older adults are in the high-risk group for CVD; thus, lipid-lowering therapy is expected to be highly beneficial.
The primary preventive effects of statin on older adults aged ≥70 years have been proven to lower CVD and CVD mortality in a study of subjects aged 70 years or older and in a subgroup analysis of several large-scale studies.116,167,168 Furthermore, the subgroup analyses on older adults in studies that attempted to examine the secondary prevention effects of statin therapy also found that statin significantly lowered the incidence of CVD without safety problems.169,170 Therefore, statin therapy is recommended for primary and secondary prevention of CVD for older adults. However, evidence supporting the association between cholesterol levels, CVD, and mortality as well as the efficacy of statin therapy in patients excluded in these clinical trials, such as older adults aged ≥80 years or frail older adults, is lacking.
Because elderly patients often have multiple comorbidities and reduced organ functions, they are expected to have exhibited pharmacological differences in drug absorption, distribution, metabolism, and excretion, which may increase the risk of adverse drug interaction. However, current clinical trials of statin therapy did not find a significant increase of adverse reactions, such as rhabdomyolysis or increased liver enzyme levels, in older adults. Because many elderly patients have multiple comorbidities or take multiple medications, statin should be used while carefully monitoring its interactions with other drugs and its adverse reactions.
Dyslipidemia in children and adolescents
For Korean children and adolescents, dyslipidemia is defined as total cholesterol ≥200 mg/dL, LDL-C ≥130 mg/dL, non-HDL-C ≥145 mg/dL, triglyceride ≥130 mg/dL (children below age 10, ≥100 mg/dL), and HDL-C <40 mg/dL according to the 2011 National Heart, Lung, and Blood Institute (NHLBI) guideline (Table 13).171 However, according to the fourth National Health and Nutrition Examination Survey (2007 to 2010), triglyceride levels of 130 mg/dL falls under the 75th to 90th percentile and 150 mg/dL falls under the 90th percentile for Korean children and adolescents, which differs from the NHLBI's definition of dyslipidemia. This may be attributable to the fact that a carbohydrate-based diet is the typical staple in South Korea, but additional studies are needed to substantiate the criteria for hypertriglyceridemia for Korean children and adolescents.
Table 13. Diagnostic criteria of dyslipidemia for children and adolescents.
| Unit, mg/dL | Permissible | Borderline | Abnormal | |
|---|---|---|---|---|
| Total cholesterol | < 170 | 170–199 | ≥ 200 | |
| LDL-C | <110 | 110–129 | ≥130 | |
| Non-HDL-C | <120 | 120–144 | ≥145 | |
| Triglyceride | ||||
| 0–9 yr171 | <75 | 75–99 | ≥100 | |
| 10–19 yr | <90 | 90–129 | ≥130 | |
| HDL-C | >45 | 40–45 | <40 | |
LDL-C, low density lipoprotein cholesterol; HDL-C, high density lipoprotein cholesterol.
In general, a screening test is not recommended for children under the age of 9, and non-HDL-C that does not require fasting is recommended for children aged 9 to 11 years and adolescents aged 17 to 21 years. Children not in these age groups are recommended to undergo fasting lipid test if they present a risk factor for dyslipidemia or have family members with a risk factor (Table 14).172,173,174,175
Table 14. Screening test for dyslipidemia in children and adolescents.
| Age, yr | Recommendation |
|---|---|
| Birth–2 years | No screening test necessary |
| 2–8 | Screening test not recommended |
| Fasting lipid test in presence of family history and risk factor* | |
| 9–11 | Non-HDL-C test without fasting |
| If non-HDL-C ≥145 mg/dL, fasting lipid test* | |
| 12–16 | Screening test not recommended |
| Fasting lipid test when new risk factor or condition is discovered among family members* | |
| 17–21 | Non-HDL-C test without fasting |
| If non-HDL-C ≥145 mg/dL, fasting lipid test* |
HDL-C, high density lipoprotein cholesterol.
*Tests for fasting lipid profiles should be performed twice at intervals of more than two weeks within 3 months.
Statin therapy should not be immediately initiated in children and adolescents even if dyslipidemia is discovered. The decision for drug therapy must be based on the mean results of two rounds of fasting lipid test performed in 2-week intervals within the past three months, and family history and risk factors must be assessed. In general, drug therapy is not performed in children under the age of 10, and only lifestyle adjustment and dietary therapy (Cardiovascular Health Integrated Lifestyle Diet 1 [CHILD1] → CHILD2-LDL) is performed for about six months. However, statin therapy may be considered if LDL-C persists to be >190 mg/dL.171,172,173,174,175,176 Furthermore, drug therapy may be considered for patients with severe primary hyperlipidemia or risk factors for medical complications.177
Three to 6 months of dietary therapy is applied for children and adolescents between the ages of 10 to 21 years with mean LDL < 250 mg/dL or triglyceride <500 mg/dL. Those with a BMI in the 85th percentile should be encouraged to reduce calories by increasing physical activities and altering lifestyle.178 If the target lipid concentration is not met even with these modalities, drug therapy may be considered (Fig. 11). If the target LDL-C has been met but non-HDL-C is >145 mg/dL in children above the age of 10, statin agents, fibrates, or niacin may be considered, and the patients must be referred to a specialist.171,179 If fasting triglyceride is between 200 to 499 mg/dL and non-HDL-C is >145 mg/dL even after lifestyle adjustment and dietary therapy (CHILD1 → CHILD2-triglyceride), the use of omega-3 fatty acids may be considered.171 There have been only a few cases of pediatric use of omega-3 fatty acid, but no safety problems have been reported thus far. Those with triglyceride levels >500 mg/dL must consult a specialist, as they have a risk for pancreatitis.
Fig. 11. Dyslipidemia treatment algorithm in children and adolescents.

LDL-C, low density lipoprotein cholesterol; TG, triglyceride; CHILD, Cardiovascular Health Integrated Lifestyle Diet; CVD, cardiovascular disease; HDL-C, high density lipoprotein cholesterol.
Familial hypercholesterolemia
Heterozygous familial hypercholesterolemia
Traditionally, the prevalence of heFH is known to be 1/500.180 Since patients with heFH are exposed to high levels of LDL-C over their life-time, they have an obviously high-risk of CVD. Accordingly, it is definitely important to appropriately diagnose patients as early as possible and prevent vascular complications.
Diagnosis
A patient is likely to have heFH when they present with premature CAD at age of <50 years (male) or <60 years (female) or has family history of FH. Diagnosis can be made based on clinical criteria or DNA mutation. Clinical criteria include Simon Broome criteria (Table 15), Dutch criteria, and Make Early Diagnosis to Prevent Premature Deaths (MEDPED) criteria.181,182 Cascade screening is recommended for family members of a diagnosed proband of heFH.
Table 15. Simon Broome criteria for the diagnosis of heFH.
| Definite FH | If the patient has |
| 1) cholesterol level as defined* and tendon xanthoma, or evidence of these signs in first- or second degree relative or | |
| 2) DNA-based evidence of an LDL-receptor mutation, familial defective apo B-100, or a PCSK9 mutation | |
| Possible FH | If the patient has cholesterol level as defined* and at least one of the following |
| 1) family history of myocardial infarction: aged <50 years in second-degree relative or aged <60 years in first degree relative. | |
| 2) family history of raised total cholesterol: >290 mg/dL in adult first- or second degree relative or >260 mg/dL in child, brother or sister aged <16 years. |
heFH, heterozygous hypercholesterolemia; FH, familial hypercholesterolemia; DNA, deoxyribonucleic acid; LDL, low density lipoprotein; apo-B, apolipoprotein B; PCSK9, proprotein convertase subtilisin/kexin type 9.
*Total cholesterol >260 mg/dL or LDL-C >155 mg/dL (child/young person); total cholesterol 290 mg/dL or LDL-C >190 mg/dL (adult).
Treatment
1) Principles of management of heFH include lifestyle modification, lipid-lowering agents, and screening for atherosclerotic CVD.
2) First target of lipid lowering therapy is to reduce LDL-C by 50% of baseline levels. Thereafter, it is desirable to lower LDL-C to <100 mg/dL (when the patient has no CAD or other major risk factors) or to <70 mg/dL (when the patient has CAD or other major risk factors). However, the target is not frequently achieved in real world practice and reduction of LDL-C as much as possible with maximal tolerable treatment is often a practical objective.183
3) It is recommended to attempt to achieve the LDL-C goal by maximal tolerable dose of statins, the first line drug. If the target is not achieved, ezetimibe can be added. A considerable proportion of patients cannot reach the target and cholesterol binding resins or PCSK9 inhibitors can be added as third line agents.6,184 When patients experience adverse events related to statins, second line or third line agents can be used instead.
4) For children of parents with heFH, DNA testing is recommended when a gene mutation in the father or mother is identified. Otherwise, it is better that they undergo LDL-C measurement. Statin therapy can be started at the age of 8–10 years and the target is 135 mg/dL at age >10 years.6
Homozygous familial hypercholesterolemia (hoFH)
The prevalence of hoFH is known to be 1/1,000,000 or higher. Because the exposure of vessels of hoFH patients to lipid is more severe than that of heFH patients, the incidence of CAD under the age of 20 years is not uncommon.
Diagnosis
One of the most well known international criteria for hoFH is that of EAS (2014). It includes DNA mutation, LDL-C levels, and family history.
Screening of complications
For examination of CAD or aortic disease, it is desirable to consult to cardiologist. Regular screening for complications is recommended.
Treatment
The aim of treatment in hoFH is to reduce LDL-C as early as possible and as much as possible. Treatment targets are 100, 135, and 70 mg/dL in adults, children, and patients with atherosclerotic CVD, respectively. Lifestyle modification, statins (with ezetimibe), and LDL apheresis (if available) are essentials of treatment. LDL apheresis is recommended at the age of 5 years or at least at age 8 years. New therapeutics such as lomitapide, mipomersen, or PCSK9 can be added.
Cholesterol during pregnancy
Changes in lipid metabolism during pregnancy
Lipids in plasma during pregnancy decrease at the first stage and then begin to increase after gestational age (GA) of 8 weeks. Increased insulin resistance and estrogen stimulation are responsible for the maternal hyperlipidemia observed during pregnancy.185 In the first and second trimesters, fat accumulates due to increased food intake and lipogenesis; however, fat accumulation decreases during the third trimester because of enhanced lipolytic activity and decreased LPL activity.186 In the later period of pregnancy, insulin resistance increases lipolysis, gluconeogenesis, and ketogenesis in the fasting state in pregnant women. Insulin increases the activity of LPL in adipose tissue and reduces the activity of hormone-sensitive lipase, which is a lipolytic enzyme. In addition, insulin inhibits hepatic gluconeogenesis and ketogenesis. Peripheral insulin resistance develops in women with gestational diabetes and plays a role in increasing blood nonessential fatty acids and ketone body concentration.187
Hyperlipidemia during pregnancy
In the later period of pregnancy, triglycerides, phospholipids, and cholesterol levels increase. In particular, the increase of triglycerides is most prominent. Whereas HDL-C increases after the GA 12 weeks of pregnancy due to the increase of estrogen, the total cholesterol and LDL-C increase in the second and third trimesters. During pregnancy, hepatic lipase decreases the size of triglyceride-rich LDL-C and increases its density. Such changes damage endothelial cells and cause atheroma formation.
Treatment of dyslipidemia during pregnancy
Lifestyle modifications
Physical activity is effective in preventing gestational diabetes and gestational hypertension. The average triglyceride level, of any kind, is lower in women who are physically active. For diet therapy, it is difficult to make a definitive conclusion and additional studies are required.
Omega-3 fatty acid
Omega-3 fatty acids are elements of the diet and are not considered to increase adverse effects during pregnancy. There are insufficient data to recommend omega-3 fatty acid supplements instead of fish intake to normal pregnant women. However, supplementation of docosahexaenoic acid is recommended in pregnant women who do not usually eat fish at all.
Statins
Statins are contraindicated during pregnancy. Statins are not thought to increase fetal anomalies during pregnancy. Statin therapy is not recommended during pregnancy because there is no evidence that dyslipidemia treatment is beneficial to pregnant women or that cholesterol is required for the growth of embryo during pregnancy. A woman who is planning pregnancy or is already pregnant, should stop statins, if she is taking statins.
FUTURE RESEARCH TOPICS
Cardiovascular biomarkers
Carotid plaque and intima-media thickness
In addition to coronary artery calcification, carotid intima-media thickness is one of the most well-known surrogate markers of CVD.188 Adding intima-media thickness to the traditional assessment of cardio-cerebrovascular disease using vascular risk factors enables a more detailed classification of risks.66,189
Furthermore, carotid plaques are also considered an indicator of asymptomatic atherosclerosis.189 Coronary plaque is associated with an elevated CVD risk, and a plaque of ≥4 mm in the aortic arch is a risk factor for stroke recurrence.188,190,191 However, the increase in risk associated with coronary plaques is low.188,191
According to a systematic literature review, statin therapy slows the increase of carotid intima-media thickness.192 Furthermore, high-dose statin therapy is known to be more effective in treating carotid intima-media thickness and carotid plaques.193 However, whether targeting the carotid intima-media thickness prevents CVD has not been confirmed. Similarly, studies examining whether carotid plaques can be the target of treatment are lacking. In the future, therapeutic efficacy should be investigated in more detail for high-risk groups (e.g., echolucent plaques or plaque ulcers).
Vascular calcification
Vascular calcification is commonly observed throughout the body among older adults. In the past, vascular calcification was believed to be a passive change that occurred with aging or harmless changes observed in atherosclerosis. However, recent studies have revealed that vascular calcification is associated with hypertension, dyslipidemia, diabetes, and renal diseases and that it is an actively regulated process similar to bone formation.194,195
Calcification of various systemic arteries, including the coronary artery, carotid artery, aorta, and iliac artery, is associated, and may be mutually causally related with an elevation of systemic blood pressure, pulse pressure, and vascular stiffness.195,196,197,198,199 Further, a systematic literature review reported that vascular calcification increases the risk for mortality, CAD, and cerebrovascular disease by two to four times.197 Cerebrovascular calcification is most commonly observed in the intracranial internal carotid artery and it has been associated with cerebral small vessel diseases, which are a cause of dementia or stroke.200,201
In particular, coronary arteries have been studied more extensively than other blood vessels. Coronary artery calcification generally occurs as a result of atherosclerosis and the amount of calcium deposited in coronary arteries is believed to be proportional to the total amount of atherosclerosis.202,203,204 Furthermore, multiple studies have reported that coronary artery calcification is associated with vascular disease.203 In a study that investigated the incidence of CVD in four racial groups, the risk for CAD was about 10 times higher in the group with a calcium score of 300 or higher compared to the group without coronary artery calcification.205 In consideration of these findings, existing guidelines suggest the use of coronary artery calcification and its severity as an indicator for vascular disease risk and statin therapy.24,66,206
However, despite mounting evidence, whether vascular calcification is an appropriate target of treatment is still doubtful. First, evidence supporting that vascular calcification is the sole cause of vascular diseases is lacking.188 Second, although vascular calcification is related to the overall disease burden from atherosclerosis, coronary artery calcification is not directly proportional to the degree of stenosis of the coronary artery.204,207 Coronary arteries without calcification may have stenosis and severely calcified coronary arteries may not have stenosis. Therefore, it is difficult to use coronary artery calcification as a surrogate index of vascular stenosis. Finally, effective treatment for vascular calcification has yet to be identified.
Subsequent studies should determine the causal relationship between vascular calcification and vascular diseases and develop treatment modalities for vascular calcification.
Novel serum markers of atherosclerosis
Atherosclerosis, a major cause of cardio-cerebrovascular disease, is a chronic inflammatory disease caused by injuries of vascular epithelial cells. Foreign treatment guidelines present inflammation and thrombus as novel serum markers of atherosclerosis.6,7,24 However, the strength of recommendation is low due to a lack of adequate study findings and evidence for novel serum markers. Whether serum markers can be used for assessing the risk and treating cardio-cerebrovascular diseases requires further research.
In summary,
(1) There is insufficient evidence supporting the use of serum markers for atherosclerosis (e.g., hs-CRP, fibrinogen, Lipoprotein-associated phospholipase A2 (Lp-PLA2), homocysteine) in the assessment of CVD risk in adults.
(2) Serum markers of atherosclerosis (e.g., hs-CRP, fibrinogen, Lp-PLA2, homocysteine) may be considered for assessing potential risk factors in order to determine the intensity of treating the risk factors for patients at moderate risk of CVD.
Development and validation of CVD risk assessment tool
The ACC/AHA cholesterol guideline uses CVD risk as an essential factor for determining drug therapy.24 Table 16 compares the major CVD risk assessment tools developed in the United States and the risk factors and scope of diseases differ across the models. The ACC/AHA guideline adopted the Pooled Cohort Equations developed by the ACC/AHA Risk Assessment Work Group. This tool is characterized by the use of five community cohort data to increase the representativeness of the data and that the scope of target diseases was expanded to include acute MI, stroke, CAD mortality, and stroke mortality.208
Table 16. Comparison of major cardiovascular disease risk assessment models in the United States11,33,186,187,188,189.
| Framingham CHD | ATP III | Framingham Global | Reynolds | Pooled Cohort Equation | ||
|---|---|---|---|---|---|---|
| Year of publication | 1998 | 2001 | 2008 | 2008 | 2013 | |
| Risk factor used | ||||||
| Age | X | X | X | X | X | |
| Sex | X | X | X | X | ||
| Total cholesterol | X | X | X | X | X | |
| LDL-C | X | |||||
| HDL-C | X | X | X | X | X | |
| CRP | X | |||||
| Systolic BP | X | X | X | X | X | |
| Use of antihypertensive drugs | X | X | X | |||
| Diabetes | X | X | X | |||
| HbA1c | X (only female) | |||||
| Smoking | X | X | X | X | X | |
| Family history | X | |||||
| Target disease | ||||||
| Coronary artery reperfusion | X | |||||
| Angina | X | |||||
| Unstable angina | X | |||||
| Myocardial infarction | X | X | X | X | X | |
| Coronary artery disease mortality | X | X | X | X | X | |
| Stroke | X | X | X | |||
| Stroke mortality | X | X | X | |||
| Heart failure | X | |||||
CHD, coronary heart disease; ATP, Adult Treatment Panel; LDL-C, low density lipoprotein cholesterol; HDL-C, high density lipoprotein cholesterol; CRP, C-reactive protein; BP, blood pressure.
The 2016 ESC/EAS treatment guidelines mentioned the usefulness of CVD risk assessment. Although it recommends the use of the Systematic Coronary Risk Estimation (SCORE) system, it also introduced other risk assessment models, including Framingham, ASSIGN (CV risk estimation model from the Scottish Intercollegiate Guidelines Network), Q-Risk, Prospective Cardiovascular Munster Study (PROCAM), and the World Health Organization (WHO).6 The SCORE system was developed based on the data from 200,000 individuals in 12 cohorts across the European region, and separate charts were developed for low-risk countries and high-risk countries.209
There have been studies in Korea aiming to develop risk assessment models to predict stroke, CAD, and overall CVD, and the Globorisk score also provides a risk assessment chart for Koreans.13,18,19,210 However, treatment guidelines still do not recommend the use of these tools in the decision-making for drug therapy. There are concerns that the generalizability of these risk assessment tools developed in Korea needs to be further examined as they have not been adequately validated, while others are concerned that even if individual CVD risks are assessed, it is difficult to reflect them in treatment guidelines because evidence supporting the clinical efficacy and cost-effectiveness of drug therapy according to the level of risk is lacking. Additional studies on CVD risk assessment are needed to develop a guideline for the management of dyslipidemia appropriate for Koreans.
Acknowledgments
We want to thank the efforts of the former members of Committee of Clinical Practice Guideline of Korean Society of Lipid and Atherosclerosis, Chang Hee Jung, and the new members, Bum Joon Kim Hyo-Kyoung Nam, and Young Youl Hyun. We also thank the support of the former members of board of directors of Korean Society of Lipid and Atherosclerosis, Inkyu Lee, Myung Ho Jeong, Yangha Kim, Youngmi Kim, Jae-Ryong Kim, Myoungsook Lee, Hyo-Soo Kim, Kyung Woo Park, Jae Hyoung Park, Ji Cheol Bae, Sang Youl Rhee, Young-Hyo Lim, Ki Hoon Han, Goo Taeg Oh, Sang-Hyun Kim, Myung-A Kim, Jae Hyeon Kim, Zu han Kim, Jaetaek Kim, Sang-Hak Lee, In-Kyung Jeong, Hyun-Jae Kang, Kyung-Hyun Cho, Hyojee Joung, Jin Han, Soo Lim, Sung Hee Choi, Woo Je Lee, Young-Guen Kwon, and Ho Jeong Kwon. We also thank the support of current members of board of directors of Korean Society of Lipid and Atherosclerosis, Jeong Taek Woo, Sang Hong Baek, Sun Ha Jee, Joong-Yeol Park, Woo Je Lee, Sung Wan Chun, Jung-Hwan Park, Sangmo Hong, Jong-Chan Youn, Jung Myung Lee, Jae Hyeon Kim, Sung Rae Kim, Cheol-Young Park, Jaetaek Kim, Soon Jun Hong, Kee Ho Song, Wang-Soo Lee, Sang-Hak Lee, In-Kyung Jeong, Ki Hoon Han, Goo Taeg Oh, Jeongseon Kim, Kyung Woo Park, Young Mi Park, Byung Wan Lee, Sang-Hyun Kim, and Jin Han.
Footnotes
Funding: None.
Conflict of interest: No potential conflict of interest relevant to this article was reported.
References
- 1.World Health Organization. Global Health Observatory (GHO) data [Internet] Geneva: World Health Organization; c2019. [cited 2019 Jun 20]. Available from: http://www.who.int/gho/ncd/mortality_morbidity/ncd_total/en/index.html. [Google Scholar]
- 2.World Health Organization. Preventing chronic diseases: a vital investment [Internet] Geneva: World Health Organization; c2019. [cited 2019 Jun 20]. Available from: http://www.who.int/chp/chronic_disease_report/en. [Google Scholar]
- 3.Hong JS, Kang HC, Lee SH, Kim J. Long-term trend in the incidence of acute myocardial infarction in Korea: 1997-2007. Korean Circ J. 2009;39:467–476. doi: 10.4070/kcj.2009.39.11.467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kim RB, Kim BG, Kim YM, Seo JW, Lim YS, Kim HS, et al. Trends in the incidence of hospitalized acute myocardial infarction and stroke in Korea, 2006-2010. J Korean Med Sci. 2013;28:16–24. doi: 10.3346/jkms.2013.28.1.16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Committee for the Korean Guidelines for the Management of Dyslipidemia. 2015 Korean guidelines for the management of dyslipidemia: executive summary (English Translation) Korean Circ J. 2016;46:275–306. doi: 10.4070/kcj.2016.46.3.275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS guidelines for the management of dyslipidaemias. Eur Heart J. 2016;37:2999–3058. doi: 10.1093/eurheartj/ehw272. [DOI] [PubMed] [Google Scholar]
- 7.Jellinger PS, Handelsman Y, Rosenblit PD, Bloomgarden ZT, Fonseca VA, Garber AJ, et al. American association of clinical endocrinologists and American college of endocrinology guidelines for management of dyslipidemia and prevention of cardiovascular disease. Endocr Pract. 2017;23(Suppl 2):1–87. doi: 10.4158/EP171764.APPGL. [DOI] [PubMed] [Google Scholar]
- 8.Dicembrini I, Giannini S, Ragghianti B, Mannucci E, Monami M. Effects of PCSK9 inhibitors on LDL cholesterol, cardiovascular morbidity and all-cause mortality: a systematic review and meta-analysis of randomized controlled trials. J Endocrinol Invest. 2019 Feb 14; doi: 10.1007/s40618-019-01019-4. [DOI] [PubMed] [Google Scholar]
- 9.Yonsei University, Korea Centers for Disease Control and Prevention. 2012 Private Subsidized Project on the Computation of the Incidence of Myocardial Infarction. Seoul (KR): Yonsei University; 2013. [Google Scholar]
- 10.The World Health Organization MONICA Project. Ecological analysis of the association between mortality and major risk factors of cardiovascular disease. Int J Epidemiol. 1994;23:505–516. doi: 10.1093/ije/23.3.505. [DOI] [PubMed] [Google Scholar]
- 11.Korea Centers for Disease Control and Prevention. 2017 Chronic Diseases and Issues: Chronic Disease Factbook. Cheongju (KR): Korea Centers for Disease Control and Prevention; 2017. [Google Scholar]
- 12.Kim HC, Oh SM. Noncommunicable diseases: current status of major modifiable risk factors in Korea. J Prev Med Public Health. 2013;46:165–172. doi: 10.3961/jpmph.2013.46.4.165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Jee SH, Jang Y, Oh DJ, Oh BH, Lee SH, Park SW, et al. A coronary heart disease prediction model: the Korean Heart Study. BMJ Open. 2014;4:e005025. doi: 10.1136/bmjopen-2014-005025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Korean Society for Preventive Medicine. Clinical Preventive Medicine Based on Scientific Evidence. Seoul (KR): Gyechuk Munhwasa; 2011. pp. 183–221. [Google Scholar]
- 15.Wilson PW, D'Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of coronary heart disease using risk factor categories. Circulation. 1998;97:1837–1847. doi: 10.1161/01.cir.97.18.1837. [DOI] [PubMed] [Google Scholar]
- 16.D'Agostino RB, Sr, Grundy S, Sullivan LM, Wilson P CHD Risk Prediction Group. Validation of the Framingham coronary heart disease prediction scores: results of a multiple ethnic groups investigation. JAMA. 2001;286:180–187. doi: 10.1001/jama.286.2.180. [DOI] [PubMed] [Google Scholar]
- 17.Eichler K, Puhan MA, Steurer J, Bachmann LM. Prediction of first coronary events with the Framingham score: a systematic review. Am Heart J. 2007;153:722–731. doi: 10.1016/j.ahj.2007.02.027. [DOI] [PubMed] [Google Scholar]
- 18.Jee SH, Park JW, Lee SY, Nam BH, Ryu HG, Kim SY, et al. Stroke risk prediction model: a risk profile from the Korean study. Atherosclerosis. 2008;197:318–325. doi: 10.1016/j.atherosclerosis.2007.05.014. [DOI] [PubMed] [Google Scholar]
- 19.Park GM, Han S, Kim SH, Jo MW, Her SH, Lee JB, et al. Model for assessing cardiovascular risk in a Korean population. Circ Cardiovasc Qual Outcomes. 2014;7:944–951. doi: 10.1161/CIRCOUTCOMES.114.001305. [DOI] [PubMed] [Google Scholar]
- 20.Park JH, Lee MH, Shim JS, Choi DP, Song BM, Lee SW, et al. Effects of age, sex, and menopausal status on blood cholesterol profile in the Korean population. Korean Circ J. 2015;45:141–148. doi: 10.4070/kcj.2015.45.2.141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ministry of Health and Welfare, Korea Centers for Disease Control and Prevention. 2016 National Health Statistics I, 7th National Health and Nutrition Examination Survey: First Year (2016) Cheongju (KR): Korea Centers for Disease Control and Prevention; 2017. [Google Scholar]
- 22.Kim HC. Epidemiology of dyslipidemia in Korea. J Korean Med Assoc. 2016;59:352–357. [Google Scholar]
- 23.Korean Society of Lipidology and Atherosclerosis. Dyslipidemia fact sheets in Korea, 2018 [Internet] Seoul (KR): Korean Society of Lipidology and Atherosclerosis; 2018. [cited 2019 Jun 20]. Available from: http://www.lipid.or.kr/file/Dyslipidemia%20Fact%20Sheets%20in%20Korea%202018.pdf. [Google Scholar]
- 24.Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 Suppl 2):S1–S45. doi: 10.1161/01.cir.0000437738.63853.7a. [DOI] [PubMed] [Google Scholar]
- 25.Vaucher J, Marques-Vidal P, Preisig M, Waeber G, Vollenweider P. Population and economic impact of the 2013 ACC/AHA guidelines compared with European guidelines to prevent cardiovascular disease. Eur Heart J. 2014;35:958–959. doi: 10.1093/eurheartj/ehu064. [DOI] [PubMed] [Google Scholar]
- 26.LaRosa JC, Grundy SM, Waters DD, Shear C, Barter P, Fruchart JC, et al. Intensive lipid lowering with atorvastatin in patients with stable coronary disease. N Engl J Med. 2005;352:1425–1435. doi: 10.1056/NEJMoa050461. [DOI] [PubMed] [Google Scholar]
- 27.Cholesterol Treatment Trialists' (CTT) Collaboration. Baigent C, Blackwell L, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376:1670–1681. doi: 10.1016/S0140-6736(10)61350-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Garber AJ, Abrahamson MJ, Barzilay JI, Blonde L, Bloomgarden ZT, Bush MA, et al. Consensus statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the comprehensive type 2 diabetes management algorithm: 2018 executive summary. Endocr Pract. 2018;24:91–120. doi: 10.4158/CS-2017-0153. [DOI] [PubMed] [Google Scholar]
- 29.Cannon CP, Blazing MA, Giugliano RP, McCagg A, White JA, Theroux P, et al. Ezetimibe added to statin therapy after acute coronary syndromes. N Engl J Med. 2015;372:2387–2397. doi: 10.1056/NEJMoa1410489. [DOI] [PubMed] [Google Scholar]
- 30.Sabatine MS, Giugliano RP, Keech AC, Honarpour N, Wiviott SD, Murphy SA, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376:1713–1722. doi: 10.1056/NEJMoa1615664. [DOI] [PubMed] [Google Scholar]
- 31.Schwartz GG, Steg PG, Szarek M, Bhatt DL, Bittner VA, Diaz R, et al. Alirocumab and cardiovascular outcomes after acute coronary syndrome. N Engl J Med. 2018;379:2097–2107. doi: 10.1056/NEJMoa1801174. [DOI] [PubMed] [Google Scholar]
- 32.Amarenco P, Bogousslavsky J, Callahan A, 3rd, Goldstein LB, Hennerici M, Rudolph AE, et al. High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med. 2006;355:549–559. doi: 10.1056/NEJMoa061894. [DOI] [PubMed] [Google Scholar]
- 33.NIPPON DATA80 Research Group. Risk assessment chart for death from cardiovascular disease based on a 19-year follow-up study of a Japanese representative population. Circ J. 2006;70:1249–1255. doi: 10.1253/circj.70.1249. [DOI] [PubMed] [Google Scholar]
- 34.de Lemos JA, Blazing MA, Wiviott SD, Lewis EF, Fox KA, White HD, et al. Early intensive vs a delayed conservative simvastatin strategy in patients with acute coronary syndromes: phase Z of the A to Z trial. JAMA. 2004;292:1307–1316. doi: 10.1001/jama.292.11.1307. [DOI] [PubMed] [Google Scholar]
- 35.Lee KH, Jeong MH, Kim HM, Ahn Y, Kim JH, Chae SC, et al. Benefit of early statin therapy in patients with acute myocardial infarction who have extremely low low-density lipoprotein cholesterol. J Am Coll Cardiol. 2011;58:1664–1671. doi: 10.1016/j.jacc.2011.05.057. [DOI] [PubMed] [Google Scholar]
- 36.Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet. 2002;360:7–22. [Google Scholar]
- 37.Grundy SM, Cleeman JI, Merz CN, Brewer HB, Jr, Clark LT, Hunninghake DB, et al. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines. J Am Coll Cardiol. 2004;44:720–732. doi: 10.1016/j.jacc.2004.07.001. [DOI] [PubMed] [Google Scholar]
- 38.Ferguson GG, Eliasziw M, Barr HW, Clagett GP, Barnes RW, Wallace MC, et al. The North American Symptomatic Carotid Endarterectomy Trial : surgical results in 1415 patients. Stroke. 1999;30:1751–1758. doi: 10.1161/01.str.30.9.1751. [DOI] [PubMed] [Google Scholar]
- 39.Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST) Lancet. 1998;351:1379–1387. [PubMed] [Google Scholar]
- 40.National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:3143–3421. [PubMed] [Google Scholar]
- 41.Furberg CD, Adams HP, Jr, Applegate WB, Byington RP, Espeland MA, Hartwell T, et al. Effect of lovastatin on early carotid atherosclerosis and cardiovascular events. Asymptomatic Carotid Artery Progression Study (ACAPS) Research Group. Circulation. 1994;90:1679–1687. doi: 10.1161/01.cir.90.4.1679. [DOI] [PubMed] [Google Scholar]
- 42.Teramoto T, Sasaki J, Ishibashi S, Birou S, Daida H, Dohi S, et al. Executive summary of the Japan Atherosclerosis Society (JAS) guidelines for the diagnosis and prevention of atherosclerotic cardiovascular diseases in Japan: 2012 version. J Atheroscler Thromb. 2013;20:517–523. doi: 10.5551/jat.15792. [DOI] [PubMed] [Google Scholar]
- 43.Toskes PP. Hyperlipidemic pancreatitis. Gastroenterol Clin North Am. 1990;19:783–791. [PubMed] [Google Scholar]
- 44.Studer M, Briel M, Leimenstoll B, Glass TR, Bucher HC. Effect of different antilipidemic agents and diets on mortality: a systematic review. Arch Intern Med. 2005;165:725–730. doi: 10.1001/archinte.165.7.725. [DOI] [PubMed] [Google Scholar]
- 45.Jun M, Foote C, Lv J, Neal B, Patel A, Nicholls SJ, et al. Effects of fibrates on cardiovascular outcomes: a systematic review and meta-analysis. Lancet. 2010;375:1875–1884. doi: 10.1016/S0140-6736(10)60656-3. [DOI] [PubMed] [Google Scholar]
- 46.ACCORD Study Group. Ginsberg HN, Elam MB, et al. Effects of combination lipid therapy in type 2 diabetes mellitus. N Engl J Med. 2010;362:1563–1574. doi: 10.1056/NEJMoa1001282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Poobalan A, Aucott L, Smith WC, Avenell A, Jung R, Broom J, et al. Effects of weight loss in overweight/obese individuals and long-term lipid outcomes: a systematic review. Obes Rev. 2004;5:43–50. doi: 10.1111/j.1467-789x.2004.00127.x. [DOI] [PubMed] [Google Scholar]
- 48.Korean Society for the Study of Obesity. Guideline for the Management of Obesity. Seoul (KR): Chungwoon; 2018. pp. 26–30. [Google Scholar]
- 49.Rees K, Dyakova M, Wilson N, Ward K, Thorogood M, Brunner E. Dietary advice for reducing cardiovascular risk. Cochrane Database Syst Rev. 2013;12:CD002128. doi: 10.1002/14651858.CD002128.pub5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Ministry of Health and Welfare, Korea Centers for Disease Control and Prevention. 2015 National Health Statistics: 6th National Health and Nutrition Examination Survey: Third Year (2015) Cheongju (KR): Korea Centers for Disease Control and Prevention; 2015. [Google Scholar]
- 51.Ministry of Health and Welfare, Korean Nutrition Society. Dietary Reference Intake for Koreans 2015. Seoul (KR): Korean Nutrition Society; 2015. [Google Scholar]
- 52.Mensink RP, Zock PL, Kester AD, Katan MB. Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: a meta-analysis of 60 controlled trials. Am J Clin Nutr. 2003;77:1146–1155. doi: 10.1093/ajcn/77.5.1146. [DOI] [PubMed] [Google Scholar]
- 53.Eckel RH, Jakicic JM, Ard JD, de Jesus JM, Houston Miller N, Hubbard VS, et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: a report of the American College of Cardiology/American Heart Association task force on practice guidelines. Circulation. 2014;129(25 Suppl 2):S76–S99. doi: 10.1161/01.cir.0000437740.48606.d1. [DOI] [PubMed] [Google Scholar]
- 54.Harris WS. n-3 fatty acids and serum lipoproteins: human studies. Am J Clin Nutr. 1997;65(5 Suppl):1645S–1654S. doi: 10.1093/ajcn/65.5.1645S. [DOI] [PubMed] [Google Scholar]
- 55.Brown L, Rosner B, Willett WW, Sacks FM. Cholesterol-lowering effects of dietary fiber: a meta-analysis. Am J Clin Nutr. 1999;69:30–42. doi: 10.1093/ajcn/69.1.30. [DOI] [PubMed] [Google Scholar]
- 56.Anderson JW, Randles KM, Kendall CW, Jenkins DJ. Carbohydrate and fiber recommendations for individuals with diabetes: a quantitative assessment and meta-analysis of the evidence. J Am Coll Nutr. 2004;23:5–17. doi: 10.1080/07315724.2004.10719338. [DOI] [PubMed] [Google Scholar]
- 57.Chrysohoou C, Panagiotakos DB, Pitsavos C, Skoumas J, Toutouza M, Papaioannou I, et al. Effects of chronic alcohol consumption on lipid levels, inflammatory and haemostatic factors in the general population: the ‘ATTICA’ Study. Eur J Cardiovasc Prev Rehabil. 2003;10:355–361. doi: 10.1097/01.hjr.0000065928.57001.4d. [DOI] [PubMed] [Google Scholar]
- 58.Fletcher GF, Ades PA, Kligfield P, Arena R, Balady GJ, Bittner VA, et al. Exercise standards for testing and training: a scientific statement from the American Heart Association. Circulation. 2013;128:873–934. doi: 10.1161/CIR.0b013e31829b5b44. [DOI] [PubMed] [Google Scholar]
- 59.Taylor RS, Brown A, Ebrahim S, Jolliffe J, Noorani H, Rees K, et al. Exercise-based rehabilitation for patients with coronary heart disease: systematic review and meta-analysis of randomized controlled trials. Am J Med. 2004;116:682–692. doi: 10.1016/j.amjmed.2004.01.009. [DOI] [PubMed] [Google Scholar]
- 60.Kraus WE, Houmard JA, Duscha BD, Knetzger KJ, Wharton MB, McCartney JS, et al. Effects of the amount and intensity of exercise on plasma lipoproteins. N Engl J Med. 2002;347:1483–1492. doi: 10.1056/NEJMoa020194. [DOI] [PubMed] [Google Scholar]
- 61.Haskell WL, Lee IM, Pate RR, Powell KE, Blair SN, Franklin BA, et al. Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation. 2007;116:1081–1093. doi: 10.1161/CIRCULATIONAHA.107.185649. [DOI] [PubMed] [Google Scholar]
- 62.Kavazis AN. Exercise preconditioning of the myocardium. Sports Med. 2009;39:923–935. doi: 10.2165/11317870-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 63.2018 Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report. Washington, DC: U.S. Department of Health and Human Services; 2018. [Google Scholar]
- 64.Kelley GA, Kelley KS. Impact of progressive resistance training on lipids and lipoproteins in adults: a meta-analysis of randomized controlled trials. Prev Med. 2009;48:9–19. doi: 10.1016/j.ypmed.2008.10.010. [DOI] [PubMed] [Google Scholar]
- 65.Kelley GA, Kelley KS. Impact of progressive resistance training on lipids and lipoproteins in adults: another look at a meta-analysis using prediction intervals. Prev Med. 2009;49:473–475. doi: 10.1016/j.ypmed.2009.09.018. [DOI] [PubMed] [Google Scholar]
- 66.Perk J, De Backer G, Gohlke H, Graham I, Reiner Z, Verschuren M, et al. European Guidelines on cardiovascular disease prevention in clinical practice (version 2012). The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts) Eur Heart J. 2012;33:1635–1701. doi: 10.1093/eurheartj/ehs092. [DOI] [PubMed] [Google Scholar]
- 67.Moriguchi EH, Fusegawa Y, Tamachi H, Goto Y. Effects of smoking on HDL subfractions in myocardial infarction patients: effects on lecithin-cholesterol acyltransferase and hepatic lipase. Clin Chim Acta. 1991;195:139–143. doi: 10.1016/0009-8981(91)90134-x. [DOI] [PubMed] [Google Scholar]
- 68.Hellerstein MK, Benowitz NL, Neese RA, Schwartz JM, Hoh R, Jacob P, 3rd, et al. Effects of cigarette smoking and its cessation on lipid metabolism and energy expenditure in heavy smokers. J Clin Invest. 1994;93:265–272. doi: 10.1172/JCI116955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.McCall MR, van den Berg JJ, Kuypers FA, Tribble DL, Krauss RM, Knoff LJ, et al. Modification of LCAT activity and HDL structure. New links between cigarette smoke and coronary heart disease risk. Arterioscler Thromb. 1994;14:248–253. doi: 10.1161/01.atv.14.2.248. [DOI] [PubMed] [Google Scholar]
- 70.Craig WY, Palomaki GE, Haddow JE. Cigarette smoking and serum lipid and lipoprotein concentrations: an analysis of published data. BMJ. 1989;298:784–788. doi: 10.1136/bmj.298.6676.784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Stubbe I, Eskilsson J, Nilsson-Ehle P. High-density lipoprotein concentrations increase after stopping smoking. Br Med J (Clin Res Ed) 1982;284:1511–1513. doi: 10.1136/bmj.284.6328.1511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Gepner AD, Piper ME, Johnson HM, Fiore MC, Baker TB, Stein JH. Effects of smoking and smoking cessation on lipids and lipoproteins: outcomes from a randomized clinical trial. Am Heart J. 2011;161:145–151. doi: 10.1016/j.ahj.2010.09.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Prescott E, Scharling H, Osler M, Schnohr P. Importance of light smoking and inhalation habits on risk of myocardial infarction and all cause mortality: a 22 year follow up of 12 149 men and women in the Copenhagen City Heart Study. J Epidemiol Community Health. 2002;56:702–706. doi: 10.1136/jech.56.9.702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.National Institute for Health and Clinical Excellence. NICE Public Health Guidance 10. Smoking cessation services in primary care, pharmacies, local authorities and workplaces, particularly for manual working groups, pregnant women and hard to reach communities [Internet] London: National Institute for Health and Clinical Excellence; c2019. [cited 2019 Jun 20]. Available from: http://www.nice.org.uk/nicemedia/pdf/PH010guidance.pdf. [Google Scholar]
- 75.Law MR, Morris JK, Wald NJ. Environmental tobacco smoke exposure and ischaemic heart disease: an evaluation of the evidence. BMJ. 1997;315:973–980. doi: 10.1136/bmj.315.7114.973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Mohiuddin SM, Mooss AN, Hunter CB, Grollmes TL, Cloutier DA, Hilleman DE. Intensive smoking cessation intervention reduces mortality in high-risk smokers with cardiovascular disease. Chest. 2007;131:446–452. doi: 10.1378/chest.06-1587. [DOI] [PubMed] [Google Scholar]
- 77.Anthonisen NR, Skeans MA, Wise RA, Manfreda J, Kanner RE, Connett JE Lung Health Study Research Group. The effects of a smoking cessation intervention on 14.5-year mortality: a randomized clinical trial. Ann Intern Med. 2005;142:233–239. doi: 10.7326/0003-4819-142-4-200502150-00005. [DOI] [PubMed] [Google Scholar]
- 78.Reiner Z. Combined therapy in the treatment of dyslipidemia. Fundam Clin Pharmacol. 2010;24:19–28. doi: 10.1111/j.1472-8206.2009.00764.x. [DOI] [PubMed] [Google Scholar]
- 79.Khang AR, Song YS, Kim KM, Moon JH, Lim S, Park KS, et al. Comparison of different statin therapy to change low-density lipoprotein cholesterol and high-density lipoprotein cholesterol level in Korean patients with and without diabetes. J Clin Lipidol. 2016;10:528–537. doi: 10.1016/j.jacl.2015.12.013. [DOI] [PubMed] [Google Scholar]
- 80.American College of Cardiology. ODYSSEY Outcomes: results suggest use of PCSK9 inhibitor reduces CV events, LDL-C in ACS patients [Internet] Washington, DC: American College of Cardiology; 2018. [cited 2019 Jun 20]. Available from: https://www.acc.org/latest-in-cardiology/articles/2018/03/05/15/53/sat-9am-odyssey-outcomes-cv-outcomes-with-alirocumab-after-acs-acc-2018. [Google Scholar]
- 81.Keech A, Simes RJ, Barter P, Best J, Scott R, Taskinen MR, et al. Effects of long-term fenofibrate therapy on cardiovascular events in 9795 people with type 2 diabetes mellitus (the FIELD study): randomised controlled trial. Lancet. 2005;366:1849–1861. doi: 10.1016/S0140-6736(05)67667-2. [DOI] [PubMed] [Google Scholar]
- 82.Balk EM, Lichtenstein AH, Chung M, Kupelnick B, Chew P, Lau J. Effects of omega-3 fatty acids on serum markers of cardiovascular disease risk: a systematic review. Atherosclerosis. 2006;189:19–30. doi: 10.1016/j.atherosclerosis.2006.02.012. [DOI] [PubMed] [Google Scholar]
- 83.Yokoyama M, Origasa H, Matsuzaki M, Matsuzawa Y, Saito Y, Ishikawa Y, et al. Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): a randomised open-label, blinded endpoint analysis. Lancet. 2007;369:1090–1098. doi: 10.1016/S0140-6736(07)60527-3. [DOI] [PubMed] [Google Scholar]
- 84.Davidson MH, Stein EA, Bays HE, Maki KC, Doyle RT, Shalwitz RA, et al. Efficacy and tolerability of adding prescription omega-3 fatty acids 4 g/d to simvastatin 40 mg/d in hypertriglyceridemic patients: an 8-week, randomized, double-blind, placebo-controlled study. Clin Ther. 2007;29:1354–1367. doi: 10.1016/j.clinthera.2007.07.018. [DOI] [PubMed] [Google Scholar]
- 85.Vaughan CJ, Gotto AM., Jr Update on statins: 2003. Circulation. 2004;110:886–892. doi: 10.1161/01.CIR.0000139312.10076.BA. [DOI] [PubMed] [Google Scholar]
- 86.Cholesterol Treatment Trialists' (CTT) Collaborators. Mihaylova B, Emberson J, et al. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. Lancet. 2012;380:581–590. doi: 10.1016/S0140-6736(12)60367-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Tobert JA. Lovastatin and beyond: the history of the HMG-CoA reductase inhibitors. Nat Rev Drug Discov. 2003;2:517–526. doi: 10.1038/nrd1112. [DOI] [PubMed] [Google Scholar]
- 88.Gotto AM, Jr, Opie LH. Lipid-modifying and antiatherosclerotic drugs. In: Opie L, Gersh B, editors. Drugs for the Heart. 8th ed. Philadelphia (PA): Elsevier Saunders; 2013. pp. 398–435. [Google Scholar]
- 89.Jones PH, Davidson MH, Stein EA, Bays HE, McKenney JM, Miller E, et al. Comparison of the efficacy and safety of rosuvastatin versus atorvastatin, simvastatin, and pravastatin across doses (STELLAR* Trial) Am J Cardiol. 2003;92:152–160. doi: 10.1016/s0002-9149(03)00530-7. [DOI] [PubMed] [Google Scholar]
- 90.Nicholls SJ, Brandrup-Wognsen G, Palmer M, Barter PJ. Meta-analysis of comparative efficacy of increasing dose of Atorvastatin versus Rosuvastatin versus Simvastatin on lowering levels of atherogenic lipids (from VOYAGER) Am J Cardiol. 2010;105:69–76. doi: 10.1016/j.amjcard.2009.08.651. [DOI] [PubMed] [Google Scholar]
- 91.Smith MEB, Lee NJ, Haney E, Carson S. Drug class review: HMG-CoA reductase inhibitors (statins) and fixed-dose combination products containing a statin: final report update 5 [Internet] Portland (OR): Oregon Health & Science University; 2009. [cited 2019 Jun 20]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK47273. [PubMed] [Google Scholar]
- 92.Lee HJ, Min CH, Choi KS, Ryu WS, Ryoo UH. Effects of lovastatin (Mevacor®) on lowering plasma lipids in patients with hyperlipidemia. Korean Circ J. 1991;21:781–785. [Google Scholar]
- 93.Yoo WS, Lee SB, Ahn JH, Kim K, Lee DC, Rhee KJ, et al. Effect of lovastatin (Mevacor®) on serum lipids of patients with primary hyperlipidemia. Korean Circ J. 1989;19:489–496. [Google Scholar]
- 94.Bae JH, Choue CW, Kim KS, Kim MS, Song JS. Hypolipidemic effects and safety of lovastatin in patients with primary hypercholesterolemia. Korean Circ J. 1991;21:129–136. [Google Scholar]
- 95.Koh KK, Quon MJ, Sakuma I, Han SH, Choi H, Lee K, et al. Differential metabolic effects of rosuvastatin and pravastatin in hypercholesterolemic patients. Int J Cardiol. 2013;166:509–515. doi: 10.1016/j.ijcard.2011.11.028. [DOI] [PubMed] [Google Scholar]
- 96.Koh KK, Lim S, Choi H, Lee Y, Han SH, Lee K, et al. Combination pravastatin and valsartan treatment has additive beneficial effects to simultaneously improve both metabolic and cardiovascular phenotypes beyond that of monotherapy with either drug in patients with primary hypercholesterolemia. Diabetes. 2013;62:3547–3552. doi: 10.2337/db13-0566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Kim SH, Kim MK, Lee HY, Kang HJ, Kim YJ, Kim HS. Prospective randomized comparison between omega-3 fatty acid supplements plus simvastatin versus simvastatin alone in Korean patients with mixed dyslipidemia: lipoprotein profiles and heart rate variability. Eur J Clin Nutr. 2011;65:110–116. doi: 10.1038/ejcn.2010.195. [DOI] [PubMed] [Google Scholar]
- 98.Kim SH, Kim MK, Seo HS, Hyun MS, Han KR, Cho SW, et al. Efficacy and safety of morning versus evening dose of controlled-release simvastatin tablets in patients with hyperlipidemia: a randomized, double-blind, multicenter phase III trial. Clin Ther. 2013;35:1350–1360. doi: 10.1016/j.clinthera.2013.06.020. [DOI] [PubMed] [Google Scholar]
- 99.Park S, Kang HJ, Rim SJ, Ha JW, Oh BH, Chung N, et al. A randomized, open-label study to evaluate the efficacy and safety of pitavastatin compared with simvastatin in Korean patients with hypercholesterolemia. Clin Ther. 2005;27:1074–1082. doi: 10.1016/j.clinthera.2005.07.007. [DOI] [PubMed] [Google Scholar]
- 100.Atorvastatin Study Group in Korea. Flexible initial dosing of atorvastatin based upon initial low-density lipoprotein cholesterol levels in type 2 diabetic patients. Korean J Intern Med. 2008;23:22–29. doi: 10.3904/kjim.2008.23.1.22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Koh KK, Quon MJ, Han SH, Lee Y, Kim SJ, Shin EK. Atorvastatin causes insulin resistance and increases ambient glycemia in hypercholesterolemic patients. J Am Coll Cardiol. 2010;55:1209–1216. doi: 10.1016/j.jacc.2009.10.053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Park JS, Kim YJ, Choi JY, Kim YN, Hong TJ, Kim DS, et al. Comparative study of low doses of rosuvastatin and atorvastatin on lipid and glycemic control in patients with metabolic syndrome and hypercholesterolemia. Korean J Intern Med. 2010;25:27–35. doi: 10.3904/kjim.2010.25.1.27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Her AY, Kim JY, Kang SM, Choi D, Jang Y, Chung N, et al. Effects of atorvastatin 20 mg, rosuvastatin 10 mg, and atorvastatin/ezetimibe 5 mg/5 mg on lipoproteins and glucose metabolism. J Cardiovasc Pharmacol Ther. 2010;15:167–174. doi: 10.1177/1074248409357922. [DOI] [PubMed] [Google Scholar]
- 104.Kim SH, Park K, Hong SJ, Cho YS, Sung JD, Moon GW, et al. Efficacy and tolerability of a generic and a branded formulation of atorvastatin 20 mg/d in hypercholesterolemic Korean adults at high risk for cardiovascular disease: a multicenter, prospective, randomized, double-blind, double-dummy clinical trial. Clin Ther. 2010;32:1896–1905. doi: 10.1016/j.clinthera.2010.10.004. [DOI] [PubMed] [Google Scholar]
- 105.Kim SH, Seo MK, Yoon MH, Choi DH, Hong TJ, Kim HS. Assessment of the efficacy and tolerability of 2 formulations of atorvastatin in Korean adults with hypercholesterolemia: a multicenter, prospective, open-label, randomized trial. Clin Ther. 2013;35:77–86. doi: 10.1016/j.clinthera.2012.11.009. [DOI] [PubMed] [Google Scholar]
- 106.Lee CW, Kang SJ, Ahn JM, Song HG, Lee JY, Kim WJ, et al. Comparison of effects of atorvastatin (20 mg) versus rosuvastatin (10 mg) therapy on mild coronary atherosclerotic plaques (from the ARTMAP trial) Am J Cardiol. 2012;109:1700–1704. doi: 10.1016/j.amjcard.2012.01.399. [DOI] [PubMed] [Google Scholar]
- 107.Lee JH, Kang HJ, Kim HS, Sohn DW, Oh BH, Park YB. Effects of ezetimibe/simvastatin 10/20 mg vs. atorvastatin 20 mg on apolipoprotein B/apolipoprotein A1 in Korean patients with type 2 diabetes mellitus: results of a randomized controlled trial. Am J Cardiovasc Drugs. 2013;13:343–351. doi: 10.1007/s40256-013-0031-6. [DOI] [PubMed] [Google Scholar]
- 108.Lee SH, Kang SM, Park S, Jang Y, Chung N, Choi D. The effects of statin monotherapy and low-dose statin/ezetimibe on lipoprotein-associated phospholipase A₂. Clin Cardiol. 2011;34:108–112. doi: 10.1002/clc.20853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Hong YJ, Jeong MH, Hachinohe D, Ahmed K, Choi YH, Cho SH, et al. Comparison of effects of rosuvastatin and atorvastatin on plaque regression in Korean patients with untreated intermediate coronary stenosis. Circ J. 2011;75:398–406. doi: 10.1253/circj.cj-10-0658. [DOI] [PubMed] [Google Scholar]
- 110.Lee SH, Cho KI, Kim JY, Ahn YK, Rha SW, Kim YJ, et al. Non-lipid effects of rosuvastatin-fenofibrate combination therapy in high-risk Asian patients with mixed hyperlipidemia. Atherosclerosis. 2012;221:169–175. doi: 10.1016/j.atherosclerosis.2011.12.042. [DOI] [PubMed] [Google Scholar]
- 111.Lee SH, Chung N, Kwan J, Kim DI, Kim WH, Kim CJ, et al. Comparison of the efficacy and tolerability of pitavastatin and atorvastatin: an 8-week, multicenter, randomized, open-label, dose-titration study in Korean patients with hypercholesterolemia. Clin Ther. 2007;29:2365–2373. doi: 10.1016/j.clinthera.2007.11.002. [DOI] [PubMed] [Google Scholar]
- 112.Weng TC, Yang YH, Lin SJ, Tai SH. A systematic review and meta-analysis on the therapeutic equivalence of statins. J Clin Pharm Ther. 2010;35:139–151. doi: 10.1111/j.1365-2710.2009.01085.x. [DOI] [PubMed] [Google Scholar]
- 113.Mukhtar RY, Reid J, Reckless JP. Pitavastatin. Int J Clin Pract. 2005;59:239–252. doi: 10.1111/j.1742-1241.2005.00461.x. [DOI] [PubMed] [Google Scholar]
- 114.Baigent C, Keech A, Kearney PM, Blackwell L, Buck G, Pollicino C, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. 2005;366:1267–1278. doi: 10.1016/S0140-6736(05)67394-1. [DOI] [PubMed] [Google Scholar]
- 115.Cannon CP, Braunwald E, McCabe CH, Rader DJ, Rouleau JL, Belder R, et al. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med. 2004;350:1495–1504. doi: 10.1056/NEJMoa040583. [DOI] [PubMed] [Google Scholar]
- 116.Shepherd J, Blauw GJ, Murphy MB, Bollen EL, Buckley BM, Cobbe SM, et al. PROspective Study of Pravastatin in the Elderly at Risk. Pravastatin in elderly individuals at risk of vascular disease (PROSPER): a randomised controlled trial. Lancet. 2002;360:1623–1630. doi: 10.1016/s0140-6736(02)11600-x. [DOI] [PubMed] [Google Scholar]
- 117.Taylor F, Ward K, Moore TH, Burke M, Davey Smith G, Casas JP, et al. Statins for the primary prevention of cardiovascular disease. Cochrane Database Syst Rev. 2011;1:CD004816. doi: 10.1002/14651858.CD004816.pub4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Mills EJ, Rachlis B, Wu P, Devereaux PJ, Arora P, Perri D. Primary prevention of cardiovascular mortality and events with statin treatments: a network meta-analysis involving more than 65,000 patients. J Am Coll Cardiol. 2008;52:1769–1781. doi: 10.1016/j.jacc.2008.08.039. [DOI] [PubMed] [Google Scholar]
- 119.Nakamura H, Arakawa K, Itakura H, Kitabatake A, Goto Y, Toyota T, et al. Primary prevention of cardiovascular disease with pravastatin in Japan (MEGA Study): a prospective randomised controlled trial. Lancet. 2006;368:1155–1163. doi: 10.1016/S0140-6736(06)69472-5. [DOI] [PubMed] [Google Scholar]
- 120.Ridker PM, Danielson E, Fonseca FA, Genest J, Gotto AM, Jr, Kastelein JJ, et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med. 2008;359:2195–2207. doi: 10.1056/NEJMoa0807646. [DOI] [PubMed] [Google Scholar]
- 121.Eckel RH. Approach to the patient who is intolerant of statin therapy. J Clin Endocrinol Metab. 2010;95:2015–2022. doi: 10.1210/jc.2009-2689. [DOI] [PubMed] [Google Scholar]
- 122.Dale KM, White CM, Henyan NN, Kluger J, Coleman CI. Impact of statin dosing intensity on transaminase and creatine kinase. Am J Med. 2007;120:706–712. doi: 10.1016/j.amjmed.2006.07.033. [DOI] [PubMed] [Google Scholar]
- 123.Berglund L, Brunzell JD, Goldberg AC, Goldberg IJ, Sacks F, Murad MH, et al. Evaluation and treatment of hypertriglyceridemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2012;97:2969–2989. doi: 10.1210/jc.2011-3213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Harris WS, Ginsberg HN, Arunakul N, Shachter NS, Windsor SL, Adams M, et al. Safety and efficacy of Omacor in severe hypertriglyceridemia. J Cardiovasc Risk. 1997;4:385–391. [PubMed] [Google Scholar]
- 125.Gruppo Italiano per lo Studio della Sopravvivenza nell'Infarto miocardico. Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: results of the GISSI-Prevenzione trial. Lancet. 1999;354:447–455. [PubMed] [Google Scholar]
- 126.Glauber H, Wallace P, Griver K, Brechtel G. Adverse metabolic effect of omega-3 fatty acids in non-insulin-dependent diabetes mellitus. Ann Intern Med. 1988;108:663–668. doi: 10.7326/0003-4819-108-5-663. [DOI] [PubMed] [Google Scholar]
- 127.Annuzzi G, Rivellese A, Capaldo B, Di Marino L, Iovine C, Marotta G, et al. A controlled study on the effects of n-3 fatty acids on lipid and glucose metabolism in non-insulin-dependent diabetic patients. Atherosclerosis. 1991;87:65–73. doi: 10.1016/0021-9150(91)90233-s. [DOI] [PubMed] [Google Scholar]
- 128.Kaushik M, Mozaffarian D, Spiegelman D, Manson JE, Willett WC, Hu FB. Long-chain omega-3 fatty acids, fish intake, and the risk of type 2 diabetes mellitus. Am J Clin Nutr. 2009;90:613–620. doi: 10.3945/ajcn.2008.27424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Wu JH, Micha R, Imamura F, Pan A, Biggs ML, Ajaz O, et al. Omega-3 fatty acids and incident type 2 diabetes: a systematic review and meta-analysis. Br J Nutr. 2012;107(Suppl 2):S214–S227. doi: 10.1017/S0007114512001602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Pedersen HS, Mulvad G, Seidelin KN, Malcom GT, Boudreau DA. N-3 fatty acids as a risk factor for haemorrhagic stroke. Lancet. 1999;353:812–813. doi: 10.1016/S0140-6736(98)05918-2. [DOI] [PubMed] [Google Scholar]
- 131.Gajos G, Zalewski J, Rostoff P, Nessler J, Piwowarska W, Undas A. Reduced thrombin formation and altered fibrin clot properties induced by polyunsaturated omega-3 fatty acids on top of dual antiplatelet therapy in patients undergoing percutaneous coronary intervention (OMEGA-PCI clot) Arterioscler Thromb Vasc Biol. 2011;31:1696–1702. doi: 10.1161/ATVBAHA.111.228593. [DOI] [PubMed] [Google Scholar]
- 132.Wu D, Meydani SN. n-3 polyunsaturated fatty acids and immune function. Proc Nutr Soc. 1998;57:503–509. doi: 10.1079/pns19980074. [DOI] [PubMed] [Google Scholar]
- 133.AIM-HIGH Investigators. Boden WE, Probstfield JL, et al. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med. 2011;365:2255–2267. doi: 10.1056/NEJMoa1107579. [DOI] [PubMed] [Google Scholar]
- 134.Rossebø AB, Pedersen TR, Boman K, Brudi P, Chambers JB, Egstrup K, et al. Intensive lipid lowering with simvastatin and ezetimibe in aortic stenosis. N Engl J Med. 2008;359:1343–1356. doi: 10.1056/NEJMoa0804602. [DOI] [PubMed] [Google Scholar]
- 135.Baigent C, Landray MJ, Reith C, Emberson J, Wheeler DC, Tomson C, et al. The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of Heart and Renal Protection): a randomised placebo-controlled trial. Lancet. 2011;377:2181–2192. doi: 10.1016/S0140-6736(11)60739-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Cannon CP, Giugliano RP, Blazing MA, Harrington RA, Peterson JL, Sisk CM, et al. Rationale and design of IMPROVE-IT (IMProved Reduction of Outcomes: Vytorin Efficacy International Trial): comparison of ezetimbe/simvastatin versus simvastatin monotherapy on cardiovascular outcomes in patients with acute coronary syndromes. Am Heart J. 2008;156:826–832. doi: 10.1016/j.ahj.2008.07.023. [DOI] [PubMed] [Google Scholar]
- 137.Sabatine MS, Giugliano RP, Wiviott SD, Raal FJ, Blom DJ, Robinson J, et al. Efficacy and safety of evolocumab in reducing lipids and cardiovascular events. N Engl J Med. 2015;372:1500–1509. doi: 10.1056/NEJMoa1500858. [DOI] [PubMed] [Google Scholar]
- 138.Robinson JG, Farnier M, Krempf M, Bergeron J, Luc G, Averna M, et al. Efficacy and safety of alirocumab in reducing lipids and cardiovascular events. N Engl J Med. 2015;372:1489–1499. doi: 10.1056/NEJMoa1501031. [DOI] [PubMed] [Google Scholar]
- 139.Athyros VG, Papageorgiou AA, Athyrou VV, Demitriadis DS, Pehlivanidis AN, Kontopoulos AG. Atorvastatin versus four statin-fibrate combinations in patients with familial combined hyperlipidaemia. J Cardiovasc Risk. 2002;9:33–39. doi: 10.1177/174182670200900105. [DOI] [PubMed] [Google Scholar]
- 140.Farnier M, Steinmetz A, Retterstøl K, Császár A. Fixed-dose combination fenofibrate/pravastatin 160/40 mg versus simvastatin 20 mg monotherapy in adults with type 2 diabetes and mixed hyperlipidemia uncontrolled with simvastatin 20 mg: a double-blind, randomized comparative study. Clin Ther. 2011;33:1–12. doi: 10.1016/j.clinthera.2011.02.006. [DOI] [PubMed] [Google Scholar]
- 141.Zhao XQ, Krasuski RA, Baer J, Whitney EJ, Neradilek B, Chait A, et al. Effects of combination lipid therapy on coronary stenosis progression and clinical cardiovascular events in coronary disease patients with metabolic syndrome: a combined analysis of the Familial Atherosclerosis Treatment Study (FATS), the HDL-Atherosclerosis Treatment Study (HATS), and the Armed Forces Regression Study (AFREGS) Am J Cardiol. 2009;104:1457–1464. doi: 10.1016/j.amjcard.2009.07.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Galan P, Kesse-Guyot E, Czernichow S, Briancon S, Blacher J, Hercberg S SU.FOL.OM3 Collaborative Group. Effects of B vitamins and omega 3 fatty acids on cardiovascular diseases: a randomised placebo controlled trial. BMJ. 2010;341:c6273. doi: 10.1136/bmj.c6273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.HPS2-THRIVE Collaborative Group. Landray MJ, Haynes R. Effects of extended-release niacin with laropiprant in high-risk patients. N Engl J Med. 2014;371:203–212. doi: 10.1056/NEJMoa1300955. [DOI] [PubMed] [Google Scholar]
- 144.Amarenco P, Labreuche J, Lavallée P, Touboul PJ. Statins in stroke prevention and carotid atherosclerosis: systematic review and up-to-date meta-analysis. Stroke. 2004;35:2902–2909. doi: 10.1161/01.STR.0000147965.52712.fa. [DOI] [PubMed] [Google Scholar]
- 145.Hosomi N, Nagai Y, Kohriyama T, Ohtsuki T, Aoki S, Nezu T, et al. The Japan Statin Treatment Against Recurrent Stroke (J-STARS): a multicenter, randomized, open-label, parallel-group study. EBioMedicine. 2015;2:1071–1078. doi: 10.1016/j.ebiom.2015.08.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Goldstein LB, Amarenco P, Szarek M, Callahan A, 3rd, Hennerici M, Sillesen H, et al. Hemorrhagic stroke in the stroke prevention by aggressive reduction in cholesterol levels study. Neurology. 2008;70(24 Pt 2):2364–2370. doi: 10.1212/01.wnl.0000296277.63350.77. [DOI] [PubMed] [Google Scholar]
- 147.Tonelli M, Wanner C Kidney Disease: Improving Global Outcomes Lipid Guideline Development Work Group Members. Lipid management in chronic kidney disease: synopsis of the Kidney Disease: Improving Global Outcomes 2013 clinical practice guideline. Ann Intern Med. 2014;160:182. doi: 10.7326/M13-2453. [DOI] [PubMed] [Google Scholar]
- 148.Holdaas H, Fellström B, Jardine AG, Holme I, Nyberg G, Fauchald P, et al. Effect of fluvastatin on cardiac outcomes in renal transplant recipients: a multicentre, randomised, placebo-controlled trial. Lancet. 2003;361:2024–2031. doi: 10.1016/S0140-6736(03)13638-0. [DOI] [PubMed] [Google Scholar]
- 149.Wanner C, Krane V, März W, Olschewski M, Mann JF, Ruf G, et al. Atorvastatin in patients with type 2 diabetes mellitus undergoing hemodialysis. N Engl J Med. 2005;353:238–248. doi: 10.1056/NEJMoa043545. [DOI] [PubMed] [Google Scholar]
- 150.Fellström BC, Jardine AG, Schmieder RE, Holdaas H, Bannister K, Beutler J, et al. Rosuvastatin and cardiovascular events in patients undergoing hemodialysis. N Engl J Med. 2009;360:1395–1407. doi: 10.1056/NEJMoa0810177. [DOI] [PubMed] [Google Scholar]
- 151.European Association for Cardiovascular Prevention & Rehabilitation. Reiner Z, Catapano AL, et al. ESC/EAS guidelines for the management of dyslipidaemias: the task force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS) Eur Heart J. 2011;32:1769–1818. doi: 10.1093/eurheartj/ehr158. [DOI] [PubMed] [Google Scholar]
- 152.Zhao YY, Weir MA, Manno M, Cordy P, Gomes T, Hackam DG, et al. New fibrate use and acute renal outcomes in elderly adults: a population-based study. Ann Intern Med. 2012;156:560–569. doi: 10.7326/0003-4819-156-8-201204170-00003. [DOI] [PubMed] [Google Scholar]
- 153.Harper CR, Jacobson TA. Managing dyslipidemia in chronic kidney disease. J Am Coll Cardiol. 2008;51:2375–2384. doi: 10.1016/j.jacc.2008.03.025. [DOI] [PubMed] [Google Scholar]
- 154.Kidney Disease Outcomes Quality Initiative (K/DOQI) Group. K/DOQI clinical practice guidelines for management of dyslipidemias in patients with kidney disease. Am J Kidney Dis. 2003;41(4 Suppl 3):S1–S91. [PubMed] [Google Scholar]
- 155.Davidson MH, Armani A, McKenney JM, Jacobson TA. Safety considerations with fibrate therapy. Am J Cardiol. 2007;99(6A):3C–18C. doi: 10.1016/j.amjcard.2006.11.016. [DOI] [PubMed] [Google Scholar]
- 156.Mottillo S, Filion KB, Genest J, Joseph L, Pilote L, Poirier P, et al. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J Am Coll Cardiol. 2010;56:1113–1132. doi: 10.1016/j.jacc.2010.05.034. [DOI] [PubMed] [Google Scholar]
- 157.Haffner SM, Lehto S, Rönnemaa T, Pyörälä K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med. 1998;339:229–234. doi: 10.1056/NEJM199807233390404. [DOI] [PubMed] [Google Scholar]
- 158.Boekholdt SM, Arsenault BJ, Mora S, Pedersen TR, LaRosa JC, Nestel PJ, et al. Association of LDL cholesterol, non-HDL cholesterol, and apolipoprotein B levels with risk of cardiovascular events among patients treated with statins: a meta-analysis. JAMA. 2012;307:1302–1309. doi: 10.1001/jama.2012.366. [DOI] [PubMed] [Google Scholar]
- 159.Ilanne-Parikka P, Eriksson JG, Lindström J, Peltonen M, Aunola S, Hämäläinen H, et al. Effect of lifestyle intervention on the occurrence of metabolic syndrome and its components in the Finnish Diabetes Prevention Study. Diabetes Care. 2008;31:805–807. doi: 10.2337/dc07-1117. [DOI] [PubMed] [Google Scholar]
- 160.Colhoun HM, Betteridge DJ, Durrington PN, Hitman GA, Neil HA, Livingstone SJ, et al. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. Lancet. 2004;364:685–696. doi: 10.1016/S0140-6736(04)16895-5. [DOI] [PubMed] [Google Scholar]
- 161.Shepherd J, Barter P, Carmena R, Deedwania P, Fruchart JC, Haffner S, et al. Effect of lowering LDL cholesterol substantially below currently recommended levels in patients with coronary heart disease and diabetes: the Treating to New Targets (TNT) study. Diabetes Care. 2006;29:1220–1226. doi: 10.2337/dc05-2465. [DOI] [PubMed] [Google Scholar]
- 162.Lee SH, Kwon HS, Park YM, Ko SH, Choi YH, Yoon KH, et al. Statin discontinuation after achieving a target low density lipoprotein cholesterol level in type 2 diabetic patients without cardiovascular disease: a randomized controlled study. Diabetes Metab J. 2014;38:64–73. doi: 10.4093/dmj.2014.38.1.64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 163.Sacks FM, Carey VJ, Fruchart JC. Combination lipid therapy in type 2 diabetes. N Engl J Med. 2010;363:692–694. doi: 10.1056/NEJMc1006407. [DOI] [PubMed] [Google Scholar]
- 164.Moriarty PM, Jacobson TA, Bruckert E, Thompson PD, Guyton JR, Baccara-Dinet MT, et al. Efficacy and safety of alirocumab, a monoclonal antibody to PCSK9, in statin-intolerant patients: design and rationale of ODYSSEY ALTERNATIVE, a randomized phase 3 trial. J Clin Lipidol. 2014;8:554–561. doi: 10.1016/j.jacl.2014.09.007. [DOI] [PubMed] [Google Scholar]
- 165.Zhang XL, Zhu QQ, Zhu L, Chen JZ, Chen QH, Li GN, et al. Safety and efficacy of anti-PCSK9 antibodies: a meta-analysis of 25 randomized, controlled trials. BMC Med. 2015;13:123. doi: 10.1186/s12916-015-0358-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 166.Statistics Korea. Statistical report of population and housing census in 2017 [Internet] Daejeon (KR): Statistics Korea; c1996. [cited 2019 Jun 20]. Available from: http://kostat.go.kr/portal/eng/index.action. [Google Scholar]
- 167.Glynn RJ, Koenig W, Nordestgaard BG, Shepherd J, Ridker PM. Rosuvastatin for primary prevention in older persons with elevated C-reactive protein and low to average low-density lipoprotein cholesterol levels: exploratory analysis of a randomized trial. Ann Intern Med. 2010;152:488–496. doi: 10.1059/0003-4819-152-8-201004200-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 168.Neil HA, DeMicco DA, Luo D, Betteridge DJ, Colhoun HM, Durrington PN, et al. Analysis of efficacy and safety in patients aged 65-75 years at randomization: Collaborative Atorvastatin Diabetes Study (CARDS) Diabetes Care. 2006;29:2378–2384. doi: 10.2337/dc06-0872. [DOI] [PubMed] [Google Scholar]
- 169.Wenger NK, Lewis SJ, Herrington DM, Bittner V, Welty FK Treating to New Targets Study Steering Committee and Investigators. Outcomes of using high- or low-dose atorvastatin in patients 65 years of age or older with stable coronary heart disease. Ann Intern Med. 2007;147:1–9. doi: 10.7326/0003-4819-147-1-200707030-00002. [DOI] [PubMed] [Google Scholar]
- 170.Lewis SJ, Moye LA, Sacks FM, Johnstone DE, Timmis G, Mitchell J, et al. Effect of pravastatin on cardiovascular events in older patients with myocardial infarction and cholesterol levels in the average range. Results of the Cholesterol and Recurrent Events (CARE) trial. Ann Intern Med. 1998;129:681–689. doi: 10.7326/0003-4819-129-9-199811010-00002. [DOI] [PubMed] [Google Scholar]
- 171.Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents; National Heart, Lung, and Blood Institute. Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: summary report. Pediatrics. 2011;128(Suppl 5):S213–S256. doi: 10.1542/peds.2009-2107C. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 172.Yang S, Hwang JS, Park HK, Lee HS, Kim HS, Kim EY, et al. Serum lipid concentrations, prevalence of dyslipidemia, and percentage eligible for pharmacological treatment of Korean children and adolescents; data from the Korea National Health and Nutrition Examination Survey IV (2007-2009) PLoS One. 2012;7:e49253. doi: 10.1371/journal.pone.0049253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 173.Srinivasan SR, Frontini MG, Xu J, Berenson GS. Utility of childhood non-high-density lipoprotein cholesterol levels in predicting adult dyslipidemia and other cardiovascular risks: the Bogalusa Heart Study. Pediatrics. 2006;118:201–206. doi: 10.1542/peds.2005-1856. [DOI] [PubMed] [Google Scholar]
- 174.Cui Y, Blumenthal RS, Flaws JA, Whiteman MK, Langenberg P, Bachorik PS, et al. Non-high-density lipoprotein cholesterol level as a predictor of cardiovascular disease mortality. Arch Intern Med. 2001;161:1413–1419. doi: 10.1001/archinte.161.11.1413. [DOI] [PubMed] [Google Scholar]
- 175.Frontini MG, Srinivasan SR, Xu JH, Tang R, Bond MG, Berenson G. Utility of non-high-density lipoprotein cholesterol versus other lipoprotein measures in detecting subclinical atherosclerosis in young adults (The Bogalusa Heart Study) Am J Cardiol. 2007;100:64–68. doi: 10.1016/j.amjcard.2007.01.071. [DOI] [PubMed] [Google Scholar]
- 176.Daniels SR. Pediatric guidelines for dyslipidemia. J Clin Lipidol. 2015;9(5 Suppl):S5–S10. doi: 10.1016/j.jacl.2015.03.105. [DOI] [PubMed] [Google Scholar]
- 177.McCrindle BW, Urbina EM, Dennison BA, Jacobson MS, Steinberger J, Rocchini AP, et al. Drug therapy of high-risk lipid abnormalities in children and adolescents: a scientific statement from the American Heart Association Atherosclerosis, Hypertension, and Obesity in Youth Committee, Council of Cardiovascular Disease in the Young, with the Council on Cardiovascular Nursing. Circulation. 2007;115:1948–1967. doi: 10.1161/CIRCULATIONAHA.107.181946. [DOI] [PubMed] [Google Scholar]
- 178.National Cholesterol Education Program (NCEP): highlights of the report of the Expert Panel on Blood Cholesterol Levels in Children and Adolescents. Pediatrics. 1992;89:495–501. [PubMed] [Google Scholar]
- 179.Manlhiot C, Larsson P, Gurofsky RC, Smith RW, Fillingham C, Clarizia NA, et al. Spectrum and management of hypertriglyceridemia among children in clinical practice. Pediatrics. 2009;123:458–465. doi: 10.1542/peds.2008-0367. [DOI] [PubMed] [Google Scholar]
- 180.Austin MA, Hutter CM, Zimmern RL, Humphries SE. Genetic causes of monogenic heterozygous familial hypercholesterolemia: a HuGE prevalence review. Am J Epidemiol. 2004;160:407–420. doi: 10.1093/aje/kwh236. [DOI] [PubMed] [Google Scholar]
- 181.Marks D, Thorogood M, Neil HA, Humphries SE. A review on the diagnosis, natural history, and treatment of familial hypercholesterolaemia. Atherosclerosis. 2003;168:1–14. doi: 10.1016/s0021-9150(02)00330-1. [DOI] [PubMed] [Google Scholar]
- 182.Hovingh GK, Davidson MH, Kastelein JJ, O'Connor AM. Diagnosis and treatment of familial hypercholesterolaemia. Eur Heart J. 2013;34:962–971. doi: 10.1093/eurheartj/eht015. [DOI] [PubMed] [Google Scholar]
- 183.Gidding SS, Champagne MA, de Ferranti SD, Defesche J, Ito MK, Knowles JW, et al. The agenda for familial hypercholesterolemia: a scientific statement from the American Heart Association. Circulation. 2015;132:2167–2192. doi: 10.1161/CIR.0000000000000297. [DOI] [PubMed] [Google Scholar]
- 184.Landmesser U, Chapman MJ, Stock JK, Amarenco P, Belch JJF, Borén J, et al. 2017 Update of ESC/EAS task force on practical clinical guidance for proprotein convertase subtilisin/kexin type 9 inhibition in patients with atherosclerotic cardiovascular disease or in familial hypercholesterolaemia. Eur Heart J. 2018;39:1131–1143. doi: 10.1093/eurheartj/ehx549. [DOI] [PubMed] [Google Scholar]
- 185.Butte NF. Carbohydrate and lipid metabolism in pregnancy: normal compared with gestational diabetes mellitus. Am J Clin Nutr. 2000;71(5 Suppl):1256S–1261S. doi: 10.1093/ajcn/71.5.1256s. [DOI] [PubMed] [Google Scholar]
- 186.Herrera E, Lasunción MA, Gomez-Coronado D, Aranda P, López-Luna P, Maier I. Role of lipoprotein lipase activity on lipoprotein metabolism and the fate of circulating triglycerides in pregnancy. Am J Obstet Gynecol. 1988;158(6 Pt 2):1575–1583. doi: 10.1016/0002-9378(88)90193-7. [DOI] [PubMed] [Google Scholar]
- 187.Jovanovic L, Metzger BE, Knopp RH, conley MR, Park E, Lee YJ, et al. The Diabetes in Early Pregnancy Study: beta-hydroxybutyrate levels in type 1 diabetic pregnancy compared with normal pregnancy. NICHD-Diabetes in Early Pregnancy Study Group (DIEP). National Institute of Child Health and Development. Diabetes Care. 1998;21:1978–1984. doi: 10.2337/diacare.21.11.1978. [DOI] [PubMed] [Google Scholar]
- 188.Jellinger PS, Smith DA, Mehta AE, Ganda O, Handelsman Y, Rodbard HW, et al. American association of clinical endocrinologists' guidelines for management of dyslipidemia and prevention of atherosclerosis. Endocr Pract. 2012;18(Suppl 1):1–78. doi: 10.4158/ep.18.s1.1. [DOI] [PubMed] [Google Scholar]
- 189.Touboul PJ, Hennerici MG, Meairs S, Adams H, Amarenco P, Bornstein N, et al. Mannheim carotid intima-media thickness and plaque consensus (2004-2006-2011). An update on behalf of the advisory board of the 3rd, 4th and 5th watching the risk symposia, at the 13th, 15th and 20th European Stroke Conferences, Mannheim, Germany, 2004, Brussels, Belgium, 2006, and Hamburg, Germany, 2011. Cerebrovasc Dis. 2012;34:290–296. doi: 10.1159/000343145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 190.French Study of Aortic Plaques in Stroke Group. Amarenco P, Cohen A, et al. Atherosclerotic disease of the aortic arch as a risk factor for recurrent ischemic stroke. N Engl J Med. 1996;334:1216–1221. doi: 10.1056/NEJM199605093341902. [DOI] [PubMed] [Google Scholar]
- 191.Task Force Members , Montalescot G, Sechtem U, et al. 2013 ESC guidelines on the management of stable coronary artery disease: the task force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. 2013;34:2949–3003. doi: 10.1093/eurheartj/eht296. [DOI] [PubMed] [Google Scholar]
- 192.Bedi US, Singh M, Singh PP, Bhuriya R, Bahekar A, Molnar J, et al. Effects of statins on progression of carotid atherosclerosis as measured by carotid intimal: medial thickness: a meta-analysis of randomized controlled trials. J Cardiovasc Pharmacol Ther. 2010;15:268–273. doi: 10.1177/1074248410369110. [DOI] [PubMed] [Google Scholar]
- 193.Meschia JF, Bushnell C, Boden-Albala B, Braun LT, Bravata DM, Chaturvedi S, et al. Guidelines for the primary prevention of stroke: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45:3754–3832. doi: 10.1161/STR.0000000000000046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 194.McClelland RL, Chung H, Detrano R, Post W, Kronmal RA. Distribution of coronary artery calcium by race, gender, and age: results from the Multi-Ethnic Study of Atherosclerosis (MESA) Circulation. 2006;113:30–37. doi: 10.1161/CIRCULATIONAHA.105.580696. [DOI] [PubMed] [Google Scholar]
- 195.Allison MA, Criqui MH, Wright CM. Patterns and risk factors for systemic calcified atherosclerosis. Arterioscler Thromb Vasc Biol. 2004;24:331–336. doi: 10.1161/01.ATV.0000110786.02097.0c. [DOI] [PubMed] [Google Scholar]
- 196.Jensky NE, Criqui MH, Wright MC, Wassel CL, Brody SA, Allison MA. Blood pressure and vascular calcification. Hypertension. 2010;55:990–997. doi: 10.1161/HYPERTENSIONAHA.109.147520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 197.Rennenberg RJ, Kessels AG, Schurgers LJ, van Engelshoven JM, de Leeuw PW, Kroon AA. Vascular calcifications as a marker of increased cardiovascular risk: a meta-analysis. Vasc Health Risk Manag. 2009;5:185–197. doi: 10.2147/vhrm.s4822. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 198.Park KY, Kim YB, Moon HS, Suh BC, Chung PW. Association between cerebral arterial calcification and brachial-ankle pulse wave velocity in patients with acute ischemic stroke. Eur Neurol. 2009;61:364–370. doi: 10.1159/000210549. [DOI] [PubMed] [Google Scholar]
- 199.Tsuchiya M, Suzuki E, Egawa K, Nishio Y, Maegawa H, Inoue S, et al. Stiffness and impaired blood flow in lower-leg arteries are associated with severity of coronary artery calcification among asymptomatic type 2 diabetic patients. Diabetes Care. 2004;27:2409–2415. doi: 10.2337/diacare.27.10.2409. [DOI] [PubMed] [Google Scholar]
- 200.Chung PW, Park KY, Moon HS, Kim YB, Youn YC, Byun JS, et al. Intracranial internal carotid artery calcification: a representative for cerebral artery calcification and association with white matter hyperintensities. Cerebrovasc Dis. 2010;30:65–71. doi: 10.1159/000314622. [DOI] [PubMed] [Google Scholar]
- 201.Chung PW, Park KY, Kim JM, Shin DW, Ha SY. Carotid artery calcification is associated with deep cerebral microbleeds. Eur Neurol. 2014;72:60–63. doi: 10.1159/000358513. [DOI] [PubMed] [Google Scholar]
- 202.Tinana A, Mintz GS, Weissman NJ. Volumetric intravascular ultrasound quantification of the amount of atherosclerosis and calcium in nonstenotic arterial segments. Am J Cardiol. 2002;89:757–760. doi: 10.1016/s0002-9149(01)02349-9. [DOI] [PubMed] [Google Scholar]
- 203.O'Rourke RA, Brundage BH, Froelicher VF, Greenland P, Grundy SM, Hachamovitch R, et al. American College of Cardiology/American Heart Association Expert Consensus Document on electron-beam computed tomography for the diagnosis and prognosis of coronary artery disease. J Am Coll Cardiol. 2000;36:326–340. doi: 10.1016/s0735-1097(00)00831-7. [DOI] [PubMed] [Google Scholar]
- 204.Sangiorgi G, Rumberger JA, Severson A, Edwards WD, Gregoire J, Fitzpatrick LA, et al. Arterial calcification and not lumen stenosis is highly correlated with atherosclerotic plaque burden in humans: a histologic study of 723 coronary artery segments using nondecalcifying methodology. J Am Coll Cardiol. 1998;31:126–133. doi: 10.1016/s0735-1097(97)00443-9. [DOI] [PubMed] [Google Scholar]
- 205.Detrano R, Guerci AD, Carr JJ, Bild DE, Burke G, Folsom AR, et al. Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med. 2008;358:1336–1345. doi: 10.1056/NEJMoa072100. [DOI] [PubMed] [Google Scholar]
- 206.American Diabetes Association. 9. Cardiovascular disease and risk management: standards of medical care in diabetes: 2018. Diabetes Care. 2018;41(Suppl 1):S86–S104. doi: 10.2337/dc18-S009. [DOI] [PubMed] [Google Scholar]
- 207.Marwan M, Ropers D, Pflederer T, Daniel WG, Achenbach S. Clinical characteristics of patients with obstructive coronary lesions in the absence of coronary calcification: an evaluation by coronary CT angiography. Heart. 2009;95:1056–1060. doi: 10.1136/hrt.2008.153353. [DOI] [PubMed] [Google Scholar]
- 208.Goff DC, Jr, Lloyd-Jones DM, Bennett G, Coady S, D'Agostino RB, Gibbons R, et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 Suppl 2):S49–S73. doi: 10.1161/01.cir.0000437741.48606.98. [DOI] [PubMed] [Google Scholar]
- 209.Conroy RM, Pyörälä K, Fitzgerald AP, Sans S, Menotti A, De Backer G, et al. Estimation of ten-year risk of fatal cardiovascular disease in Europe: the SCORE project. Eur Heart J. 2003;24:987–1003. doi: 10.1016/s0195-668x(03)00114-3. [DOI] [PubMed] [Google Scholar]
- 210.Hajifathalian K, Ueda P, Lu Y, Woodward M, Ahmadvand A, Aguilar-Salinas CA, et al. A novel risk score to predict cardiovascular disease risk in national populations (Globorisk): a pooled analysis of prospective cohorts and health examination surveys. Lancet Diabetes Endocrinol. 2015;3:339–355. doi: 10.1016/S2213-8587(15)00081-9. [DOI] [PMC free article] [PubMed] [Google Scholar]