

Abstract
There is a need for research to identify effective implementation strategies for injury prevention training within real‐world community sports. The aim of this ecological participatory study was to identify facilitators, among stakeholders at multiple levels, that could help injury prevention training become part of regular training routines in youth team handball. Concept mapping, a mixed‐method approach for qualitative data collection and quantitative data analysis, was used. Stakeholders (n = 196) of two community team handball clubs (29% players, 13% coaches, 38% caregivers, 11% club, district and national handball administrators, 9% unknown) participated in a brainstorming process. After the research team synthesized the 235 generated statements, 50 stakeholders (34% players, 22% coaches, 24% caregivers, 20% administrators) sorted 89 unique facilitator statements into clusters and rated them for importance and feasibility. Multidimensional scaling and hierarchical cluster analysis yielded five clusters (stress value 0.231): “Understanding and applying knowledge,” “Education, knowledge, and consistency,” “Set‐up and exercises,” “Inspiration, motivation, and routines,” and “Club policy and expert collaboration.” The cluster “Understanding and applying knowledge” had the highest mean importance (3.17 out of 4) and feasibility (2.93) ratings. The 32 statements rated as both highly important and feasible (Go‐zone) indicate action is required at the individual (end‐users) and organizational (policymakers) levels to implement injury prevention training. Results suggest that developing evidence‐based context‐specific injury prevention training, incorporating physiological, biomechanical and psychological components, and an associated context‐specific implementation plan in partnership with all stakeholders should be a high priority to facilitate the implementation of injury prevention training in youth team handball.
Keywords: adolescent, concept mapping, health plan implementation, preventive therapy, sports injuries, team ball sports
1. INTRODUCTION
Sport is the principal cause of injury in youth, and the risk of injury is related to high levels of training exposure at a time of great physiological and psychological development.1 In ball sports, such as team handball, the lower extremities are particularly vulnerable to acute and overuse injury.2, 3 The rate of injuries in youth handball has been reported to be as high as at the senior level,4 highlighting the need for injury prevention training also in youth players.
Specific training programs have been developed to prevent lower extremity injuries in youth participating in team ball sports. Meta‐analyses of randomized controlled trials (RCTs) show that such programs can reduce the overall injury rate by approximately 40%.5, 6, 7 However, RCTs do not accurately reflect the real‐world sport context in which the intervention is going to be implemented.8 Post‐research, these programs are not widely adopted or sustained in regular training routines, thus, restricting their public health impact.8, 9
To facilitate adoption and sustained high fidelity use of injury prevention training, we need to understand the barriers and facilitators to program implementation within the specific sport context.8 Previous studies within youth team ball sports have focused on the coaches who deliver injury prevention training.10, 11, 12, 13, 14 Although coaches are key program deliverers, integrating injury prevention training into the team's regular training routines requires behavior change among numerous stakeholders, including players, coaches, clubs and organizational representatives, alongside increased awareness and knowledge among individuals in the broader community.14, 15
The need for research to identify effective implementation strategies for injury prevention training within real‐world community sports has increasingly been recognized.7, 8, 9, 16 However, very few studies have examined or reported on the implementation of injury prevention interventions.17, 18 The current study addresses an important knowledge gap by investigating facilitators to support the implementation of injury prevention training. The aim of the present study, within the “Implementing injury Prevention exercise ROutines in TEams and Clubs in youth Team handball (I‐PROTECT)” project, was to identify facilitators among stakeholders at multiple levels of the sport delivery system, that could help make injury prevention training part of regular training routines in community youth handball.
2. PARTICIPANTS AND METHODS
2.1. Study design and theoretical framework
The study has an ecological participatory design, incorporating perspectives of multiple stakeholders involved in the safety and health of youth handball players.15 The Translating Research into Injury Prevention Practice (TRIPP), developed specifically for sports injury prevention research,19 and the seven steps for Implementing Injury Preventive Training20 were used as guiding frameworks. Specifically, stage 5 (“Describe intervention context to inform implementation strategies”) of the 6‐stage TRIPP framework19 and Step 3 (“Identify logistical barriers and solutions”) of the seven steps for Implementing Injury Preventive Training20 were followed.
2.2. Concept mapping
Concept Mapping (CM) was used to collect data. Concept mapping is a mixed‐method participatory approach for qualitative data collection and quantitative data analysis.21 The method can be used to develop theoretical frameworks, action planning, need assessments and evaluation,21 and has been reported to have good validity and reliability.22 Concept mapping is consistent with methods recommended by researchers in the sport injury prevention implementation field to provide participants’ real‐world perspectives23 and is recommended as a method to identify context‐specific factors that influence the use of a specific evidence‐based practice.24 Concept mapping has been used in one previous study in which the barriers to coaches implementing injury prevention training within adolescent female soccer were identified.14
The CM process was followed as described by Kane and Trochim.25 The key steps were as follows: (a) brainstorming to generate “facilitator” statements; (b) sorting and rating of unique facilitator statements; and (c) discussion of results in key stakeholder groups.
2.3. Focus and participants
The two community team handball clubs in a city in southern Sweden, offering organized training for youth male and female players, were asked and agreed to participate. Following the CM process,25 the focus of the study—how to make injury prevention part of regular training routines—was decided upon through close collaboration between a multidisciplinary researcher team and key representatives from each participating club.
Stakeholders at multiple levels were established a priori: players, coaches, caregivers, club, district and national handball administrators (Figure 1). Inclusion criteria for players were: ages 13‐17 years and training ≥2 times/wk in a team. Inclusion criterion for coaches was leading ≥1 training session/wk. Caregivers who were directly associated with the eligible players were also included. The inclusion criterion for club, district and national handball administrators was engagement in the issues of sports injury, coach education, or policy development for youth players. The only exclusion criterion was employed/paid players.
Figure 1.
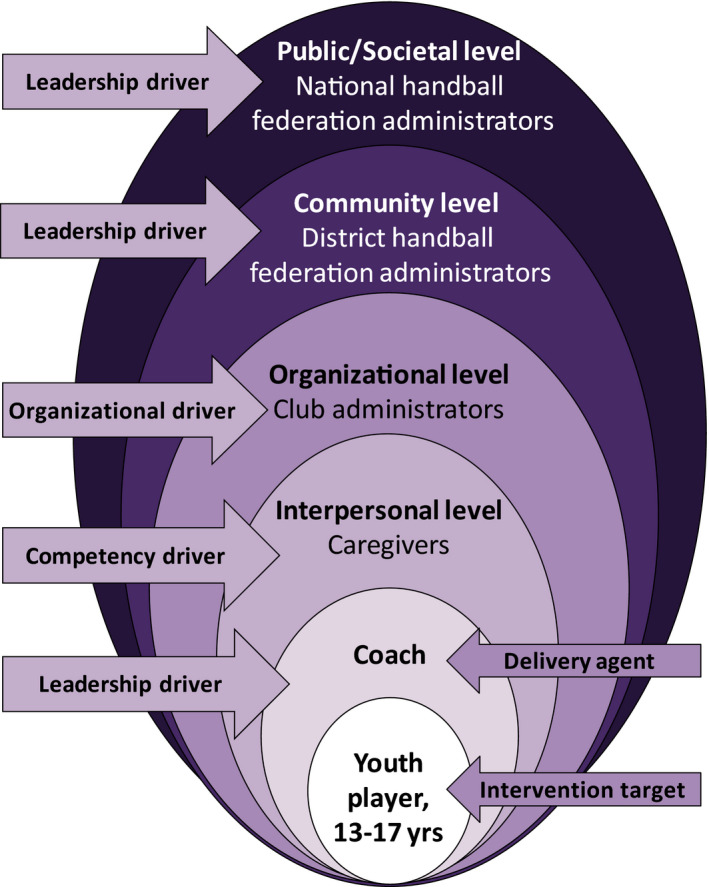
An ecological model, adapted from Emery et al (Injury prevention in child and adolescent sport: whose responsibility is it? Clin J Sport Med. 2006;16:514‐521. https://journals.lww.com/cjsportsmed/pages/default.aspx),15 defining a responsibility hierarchy in preventing injuries in youth sport. The lowest level of responsibility assigned to the child (player) and highest level to organizations with the potential to affect the most. The modification of this Figure has been reviewed and approved by the publisher, Lippincott Williams & Wilkins
The Regional Ethical Review Board in Lund, Sweden approved the study (EPN 2014/713). All participants provided informed consent. Where players were younger than 15 years, informed consent was provided by players and their caregivers.
2.4. Brainstorming process
To reach a saturation of statements from the participants, we aimed to include at least 150 participants.22 Because the two clubs have approx. 600 youth male and female handball players, players from 10 teams (n ≈ 260) were randomly selected, stratified according to club, age and sex, to take part in the brainstorming process. An e‐mail was sent to one caregiver of each youth player, although, caregivers of one youth handball player could answer together. Caregivers with more than one child in any two clubs were sent one e‐mail to avoid multiple responses from the same person. For players under 15 years, study information was sent to the caregiver, and the caregiver was informed that the child should complete the questionnaire independently. All coaches (n ≈ 90) and administrators (n ≈ 25) in the two clubs, and administrators from the district and national (n ≈ 15) handball federations were invited to participate. Participants representing more than one stakeholder group (eg, a coach who was also a club administrator) were asked to choose the group they considered to be their main task.
All participants received an e‐mail with a link to The Concept Systems® Global MAX™ web‐based platform. Two reminder e‐mails were distributed five and ten days after the initial invitation e‐mail. Relevant demographic data (stakeholder group, age, sex) were collected for each participant. Participants were given, and asked to read, the following background information before they continued to the prompt: “Our starting‐point is that injury prevention training is organized training which is done regularly and includes exercises that reduce the risk of injury. The challenge is to get injury prevention training to become a natural part of handball training.” The prompt was formulated as an open‐ended statement which participants were asked to complete: “In order to make injury prevention training a part of our regular handball training routines I need….”. The instructions for the prompt were: “Read and complete the sentence based on your own experience. Provide as many examples as possible”.
Pilot testing of the brainstorming process with a group of players and coaches showed that the provided information and focus prompt were clearly formulated, and that the prompt generated ideas that were relevant to the study. Therefore, no changes were made before data collection commenced.
2.5. Sorting and rating
When the brainstorming process closed, the lead researchers (EA, SB) synthesized (ie, combined, reduced, and edited)25 the list of statements to produce a set of unique, relevant, and clearly formulated ideas. Participants in the sorting and rating were not required to have participated in the brainstorming process.25 It has been suggested that between 20 and 30 participants are needed to maximize the consistency of fit in the CM representation and to minimize the variability in the stress value.22 We aimed to include at least 10 players, coaches, caregivers, and administrators, respectively, to ensure all stakeholder groups were represented in the sorting and rating process, and because a larger number of sorters and raters yields higher reliability.22
Following statement synthesis, an e‐mail was sent to the participants, directing them to the Concept Systems® Global MAX™ web‐based platform. As this process was more time‐consuming and challenging to complete than the brainstorming process, only players ≥15 years of age were invited to participate. Players performed the sorting and rating in live groups supervised by researchers (EA, SB), to allow them to ask questions about the process. The remaining participants (adults) performed these tasks online.
For sorting statements, participants were asked to group the statements into piles “in a way that makes sense to you,” based on perceived similarity, and to name each pile to reflect its theme or core content. The following information was given to the participants: (a) sort all statements into meaningful and comprehensive piles; (b) sort statements into piles containing at least two statements; (c) group conceptually similar statements into the same category; and (d) name piles in a way that reflects the combined core content of the pile (exclude explanations such as “other,” “irrelevant,” or “important”).
After sorting, the participants rated each statement on a 4‐point Likert scale, based on importance and feasibility. They were asked to use the full rating range (1‐4) and rate each statement relative to the other statements. The instructions for importance read: “How important is each statement to make injury prevention training part of regular handball training routines?” The Likert scale corresponded to 1 = Not at all important; 2 = Somewhat important; 3 = Important; and 4 = Very important. The instructions for feasibility read:”How feasible is each statement to make injury prevention training a part of regular handball training routines?” The Likert scale corresponded to 1 = Not at all feasible; 2 = Somewhat feasible; 3 = Feasible; and 4 = Very feasible.
2.6. Statistical analysis and graphic representation
The analyses were performed using The Concept Systems® Global MAX™ software (Concept Systems, Incorporated, Ithaca, NY, USA) (Build 2013.322.11, Web‐based platform).26 Based on sorting data, multidimensional scaling and hierarchical cluster analysis were conducted to create visual representations (maps) of the relationships between the statements. The stress index, a key diagnostic statistics, was generated to indicate goodness of fit, that is, the congruence between raw data and processed data (map configuration). A low‐stress value indicates a better overall fit of the data. In meta‐analyses of CM studies, an average stress value of 0.28 (95% confidence interval 0.205‐0.365) was estimated.25
The number of clusters was based on qualitative analysis by the researchers, with the aim to generate a final map with clusters comprising different themes/contents with each cluster containing statements considered to belong together.25 To determine the most appropriate number of clusters, the lead researchers (EA, SB) examined cluster maps from a 15 cluster‐solution through to a cluster‐solution at which further merging combined statements that were considered distinct from one another. For each cluster‐solution, the researchers reviewed the statements in the clusters that were merged together.
Mean ratings for importance and feasibility, respectively, of each statement and cluster were calculated. Pattern matching graphs were used to visually demonstrate the agreement in mean cluster ratings between rating variables (importance vs feasibility) and between stakeholder groups (the two clubs, players vs coaches, and coaches vs club administrators). Pearson's product moment correlation coefficient (r) was calculated to indicate the strength of the relationship between variables/stakeholder groups, and the t test was used to compare mean ratings. Finally, a two‐dimensional Go‐zone graph was generated to plot the ratings of statements on both importance and feasibility simultaneously. Statements that were rated above the mean for both importance and feasibility were positioned in the top right quadrant, that is., the “Go‐zone,” indicating high priority for planning or evaluation.
2.7. Interpretation and Use
The final cluster map and Go‐zone statements were discussed with key representatives from the two clubs, and the district and national handball federations. This ensured all stakeholder groups were involved in interpreting the visual maps and the Go‐zone statements, deciding on how the maps and Go‐zone statements could be used, and owning the results.
3. RESULTS
3.1. Participants
In total, 196 people (39% females, 51% males, 10% unknown) participated in the brainstorming to generate statements, and 50 participants (44% females, 56% males) sorted and rated the synthesized statements (Table 1). In the brainstorming, 18% were players aged 13‐14 years, 13% were players aged 15‐17 years, and the majority (38%) of the adults (coaches, caregivers, club, district/national administrators) were aged 41‐50 years. In the sorting and rating, 16%, 8%, and 10%, respectively, were players aged 15, 16, and 17 years, respectively, and the largest proportion (48%) of the adults (coaches, caregivers, club, district/national administrators) were 41‐50 years.
Table 1.
Participants included in the brainstorming, sorting, and rating
| Participantsa |
Brainstorming n (%) |
Sorting and rating n (%) |
|---|---|---|
| Players | 57 (29) | 17 (34) |
| Coaches | 26 (13) | 11 (22) |
| Caregivers | 75 (38) | 12 (24) |
| Club administrators | 11 (6) | 5 (10) |
| District/national administrators | 10 (5) | 5 (10) |
| Unknownb | 17 (9) | 0 (0) |
| Total | 196 (100) | 50 (100) |
Not all participants in the brainstorming participated in the sorting and rating and vice versa.
Did not respond to stakeholder group question, but provided brainstorming statements.
3.2. Statements, sorting and rating
The participants contributed 235 statements during the brainstorming. The synthesis of data generated 89 unique statements which participants sorted into groups (mean number of groups 7.9; range 3‐16 groups) and rated for importance and feasibility (Table S1, Appendix S1).
3.3. Cluster map
A five cluster‐solution was considered to be the most appropriate with statements within each cluster logically belonging together (Figure 2, Table S1, Appendix S1). The cluster names were chosen by the lead researchers (EA, SB) to reflect the core contents of the statements within each cluster. The number of statements in the clusters ranged from 9 (“Inspiration, motivation, and routines”) to 38 (“Set‐up and exercises”). The cluster “Understanding and applying knowledge” had the highest mean importance (3.17 out of 4) and feasibility (2.93) ratings. The cluster “Set‐up and exercises” received the lowest mean importance rating (2.68), while the cluster “Club policy and expert collaboration” received the lowest mean feasibility rating (2.50; Table S1, Appendix S1). The stress value was 0.231.
Figure 2.
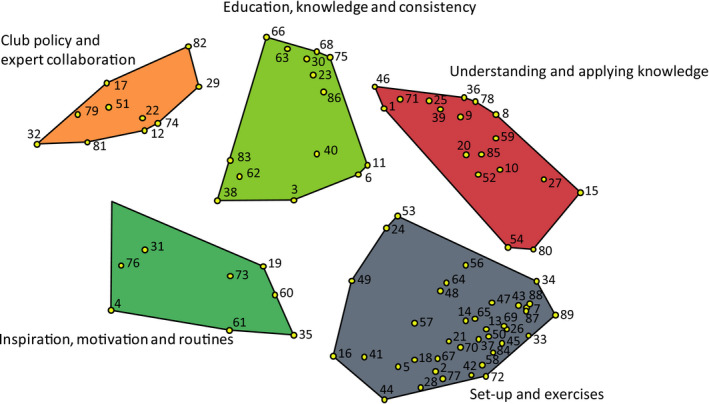
The five‐cluster map of facilitators, perceived by stakeholders, to enhance the implementation of injury prevention training in youth team handball. Statements that were more frequently sorted together are positioned closer together on the map, and statements that were less frequently sorted together are positioned further away from each other
3.4. Comparison of average cluster ratings between stakeholder groups
Pattern matching showed high agreement between the two clubs for average cluster ratings of importance (r = 0.99) and feasibility (r = 0.88; Figure S1, Appendix S2). Therefore, no further analyses were conducted for clubs separately. The agreement for average cluster ratings on importance vs feasibility was low (r = 0.17; Figure 3). Importance was rated higher than feasibility for the clusters “Understanding and applying knowledge” (P < 0.05), “Education, knowledge, and consistency” (P < 0.02), and “Club policy and expert collaboration” (P < 0.001), but not for the clusters “Inspiration, motivation, and routines” or “Set‐up and exercises” (P > 0.05; Figure 3). There was generally high agreement for average cluster ratings between players and coaches (importance r = 0.62, feasibility r = 0.80), and between coaches and club administrators (importance r = 0.57, feasibility r = 0.74; Figures S2 and S3, Appendix S2).
Figure 3.
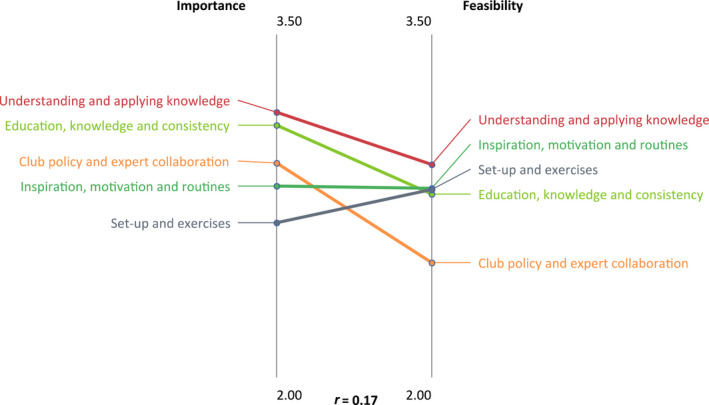
Pattern matching graph for average cluster ratings between importance and feasibility (all stakeholders), indicating low agreement between the rating variables (r = 0.17). Significant differences observed between the ratings for the clusters “Understanding and applying knowledge” (P < 0.05), “Education, knowledge, and consistency” (P < 0.02), and “Club policy and expert collaboration” (P < 0.001), but not for the clusters “Inspiration, motivation, and routines” or “Set‐up and exercises” (P > 0.05)
3.5. Go‐zone
Statements rated above the mean for both importance and feasibility are shown in the Go‐zone (top right hand quadrant of Figure 4, Table S1, Appendix S1). Go‐zone statements were drawn from all five clusters: “Club policy and expert collaboration” (n = 1); “Education, knowledge, and consistency” (n = 8); “Understanding and applying knowledge” (n = 10); “Inspiration, motivation, and routines” (n = 5); and “Set‐up and exercises” (n = 8).
Figure 4.
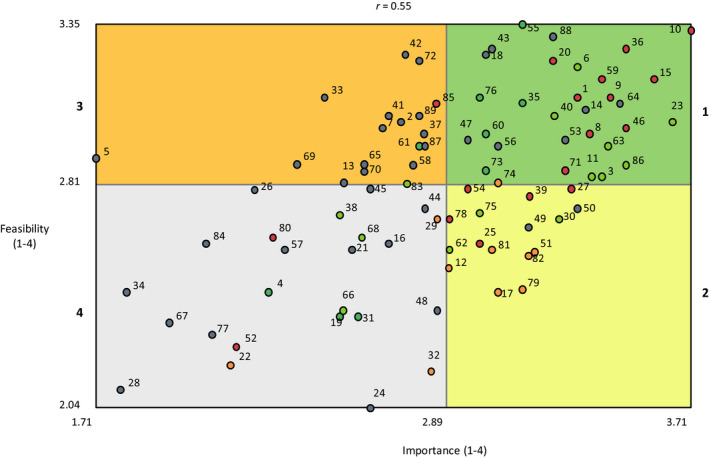
The “Go‐Zone” graph showing ratings of importance and feasibility. The top right quadrant indicates the Go‐Zone, including statements that were rated above the mean for both importance and feasibility. Go‐Zone quadrants: 1 = Top right; 2 = Bottom right, 3 = Top left; 4 = Bottom left. The statements in the Go‐Zone (quadrant 1) represent the most actionable statements
3.6. Discussion with key representatives
The cluster map, pattern maps, and the Go‐zone were discussed with key representatives from the clubs, district and national handball federations. Statement 60 (“Give youths exercises they can carry out individually outside training sessions, not least during the summer”) was considered age‐dependent, and relevant to the older (15‐17 years) but not younger (13‐14 years) players. Although statement 66 (“Educate parents so that the “thinking” spreads beyond handball“) was rated below the mean for both importance and feasibility by participants (ie, in quadrant 4 of the Go‐zone), stakeholders agreed to include it in the Go‐zone. Statement 55 (“Zero tolerance for continued play during matches/training after a blow to the head”) was regarded as not relevant to the focus prompt, but an important issue and responsibility for the governing bodies (district and national handball federations) to consider. Therefore, it was agreed to refer this statement to these organizations and to exclude it from the next phase of the I‐PROTECT project. The Go‐zone statements were also discussed from a psychological perspective. Psychological issues such as how to provide feedback (statement 3), coach communication (statement 10), behavior change (statements 11, 71), and creating a positive and accepting training environment (statement 53), were identified. It was agreed to continue the I‐PROTECT study with both clubs jointly (high agreement for cluster ratings between clubs, Appendix S2) focusing on developing evidence‐ and theory‐based injury prevention training, including both physiological/biomechanical and psychological components, that are specific to a youth community handball context. It was also agreed that the injury prevention training should be integrated into the coach education. Therefore, the district handball federation, the organization responsible for coach education in southern Sweden, was identified as an essential collaborative partner in this process. Finally, it was also agreed that an associated context‐specific implementation plan was needed to accompany the injury prevention program.
4. DISCUSSION
This is the first study with an ecological approach, involving stakeholders at multiple levels, to identify facilitators to support the implementation of injury prevention training in youth team ball sports. The findings suggest that context‐specific injury prevention training, incorporating both physiological/biomechanical and psychological components, and accompanied by a context‐specific implementation plan should be developed in collaboration with stakeholders specifically for youth team handball.
The five clusters of facilitators to implementing injury prevention training constituted a conceptual framework with aspects involving end‐users (players and coaches), as well as organizational and leadership drivers (club, district and national handball federations). The stress value of 0.231 observed in the present study is within the 95% CI (0.205‐0.365) from a meta‐analysis of CM projects,22 indicating that the visual map is a good overall representation of the collected data. At least one statement from each cluster was located in the Go‐zone quadrant indicating that action is required across multiple levels of the sports delivery system to facilitate the implementation of injury prevention training in youth team handball. This is in accordance with previous research that highlights the importance of engaging intervention end‐users at the individual and organizational levels to plan, develop, and successfully implement any evidence‐based practice,24 including injury prevention training.9, 16
The cluster “Understanding and applying knowledge” had the highest mean rating for importance, followed by “Education, knowledge, and consistency”, and both clusters had a high proportion of statements placed in the Go‐zone. In contrast, the cluster “Set‐up and exercises” received the lowest mean importance rating, had a relatively low proportion of statements in the Go‐zone, and was the only cluster where mean feasibility was rated higher than mean importance (Table 1, Figure 3). Also, the Go‐zone statements in the cluster “Set‐up and exercises” mainly focused on integrating injury prevention exercises in the handball training, and on the principles of exercises rather than specific exercises per se. These results suggest that activities to facilitate the implementation of an injury prevention intervention for youth team handball players should focus on ensuring that the end‐users know and understand the importance, benefits, and principles of such training, in conjunction with providing them with a set of specific exercises to perform. In other words, the end‐users want to know “why” as well as “what.” In line with this, previous studies within soccer have identified coaches’ lack of understanding and/or knowledge as barriers to implementing injury prevention programs.10, 13, 14 Although some injury prevention programs are freely accessible online (eg, Norwegian: www.skadefri.no, English version: www.fittoplay.org) or as mobile applications, this passive dissemination approach is usually insufficient to generate behavior change among the target audience.9, 12 Supported by previous calls,9, 27 the results of our study underscore the importance of involving end‐users when developing injury prevention training, to achieve high levels of competence and self‐efficacy among end‐users and program deliverers.
From the Go‐zone statements, including age‐related, fun, varied, and handball‐specific exercises should also be considered when developing injury prevention training for youth handball players. Previous studies have reported that coaches frequently modify programs developed for senior players for use in youth team ball sports.10, 11 Available injury prevention programs for handball players typically target senior players and include specific exercises without explaining the training principles that underpin them.28, 29, 30, 31 Therefore, existing injury prevention training programs need to be modified for youth handball players, but there is limited information available about how to do this appropriately. In line with our findings, linking injury prevention exercises more closely to game‐related skills may help facilitate regular and sustained implementation of such training.14, 32 Another advantage of introducing sport‐specific exercises is that players may perceive such exercises as more fun,10 thus, increasing their motivation to perform the exercises.33 Injury prevention exercises for youth players could also include varied training, such as coordination, balance, and strength (eg, statements 14, 64, 73), to encourage progressive athletic development.1 Although no statements on sex‐related injury prevention training were generated in the current study, female handball players are at higher risk of injuries than males,2 so sex is another factor to consider. Taken together, injury prevention training for youth handball players should be age, sex, and sport specific.
Psychological aspects of injury prevention, related to some Go‐zone statements, were identified and discussed with the key stakeholders. Available injury prevention programs for youth team ball sports include physiological and/or biomechanical components,10, 11, 14, 32 but do not tend to address the psychological aspects of injury prevention. However, this may be important to consider given that an International Olympic Committee consensus statement suggests that youth athletes are at high risk of psychological stress.1 Moreover, a recent systematic review and meta‐analysis, identified that high levels of negative life‐event stress, and strong stress responses, were associated with athletic injury, and that interventions aimed at down‐regulating stress‐related brain activations (eg, relaxation and mindfulness training) were effective in preventing injury.34 In addition to life stress, somatic trait anxiety, mistrust, and ineffective coping have been shown to predict injury among youth soccer players.35 In the current study, creating a positive and accepting training environment (Statement 53) was rated highly important. The way in which coaches communicate with players appears to play a role here. Recent studies have reported that a democratic leadership style (involving motivating and inspiring players) is related to a lower incidence of severe injuries among male soccer players,36 and that strong coach feedback results in worse game performance than mild, unobtrusive coach feedback in youth soccer players.37 In addition, Go‐zone statements 11 and 71 underline the long‐term benefits of preventing sport‐related injuries, and highlight the importance of maintaining injury prevention training over time. Previous research has identified an “intention‐behavior gap,”38 which suggests the importance of using social‐cognitive behavior change theory and habit theory to explain how a positive intention, initiation, and maintenance of a desired behavior can be attained. Reviews of sport injury prevention studies underline the inadequate use of theory‐based methods to increase the effectiveness of such behavior change interventions.33, 39 To conclude, the findings of our study, and similar results reported by others,1, 33, 34, 35, 36, 37, 39 indicate that psychological components may constitute an important part of injury prevention training for youth handball players.
The one Go‐zone statement (Statement 74) from the “Club policy and expert collaboration” cluster concerned the importance of leadership from the club and that injury prevention training should be included in the coach education syllabus. The clubs, in turn, need support from the district and national handball federations, that is, the organizations responsible for the coach education. Strong organizational leadership and policy is essential for successful implementation,9, 16 and although clubs may have experienced and qualified people to deliver injury prevention training (eg, physical therapists), program implementation will be facilitated if it is supported by club, district and national policy.27 Several Go‐zone statements concerned the integration of injury prevention training into regular handball practice. This approach is proposed to help tackle challenges related to time, engagement, and resources.9, 11 In the present study, the agreement was low (r = 0.17) between importance and feasibility for average cluster ratings. This may reflect the fact that some factors related to developing and implementing injury prevention training, while considered important, are perceived to outside the control of players and coaches. This suggests that clear policy statements and education development at the club and organizational level are needed to facilitate injury prevention training among youth handball players. It is important to avoid programs that are developed solely by researchers, as these are frequently not considered useful or accessible by organization representatives40 or end‐users.27 Therefore, combining the evidence available from the scientific literature with the clinical experience of researchers and the context‐specific knowledge of stakeholders and end‐users is suggested as a key component of succeeding in developing and implementing injury prevention exercises in community sport.27 Alongside the injury prevention program, an associated context‐specific implementation plan is needed. Our results will be used to select appropriate implementation strategies24 to address the needs identified in the present study and facilitate injury prevention training in a youth team handball setting.
4.1. Strengths and limitations
The ecological participatory approach is an important strength of the current study since it allows for multiple stakeholder perspectives to be incorporated. Another strength is that CM allows participants to brainstorm, sort and rate the statements, thereby, addressing some of the methodological limitations associated with surveys and qualitative interviews,24 and enhancing the likelihood of stakeholder ownership of results. A web‐based data collection process was considered the practical choice considering the large sample. As the sorting and rating was challenging for the youth players, these tasks were performed under the supervision of the researchers, whereas the adult participants performed this process online. We cannot exclude that live groups for all participants, with a chance to ask questions, could have generated different results. Suggested disadvantages for CM are less interaction between participants, lower response rate, and low external validity.22 However, a web‐based approach has been used successfully in previous CM studies, and a pooled study analysis of 69 CM studies showed good internal validity and high‐reliability estimates in sorting and rating, regardless of data collection method (face‐to‐face, web‐based, mixed methods).22 Generalizability of the findings may be compromised due to the two participating clubs being active in the same city.
5. PERSPECTIVES
Our results suggest that developing evidence‐based context‐specific injury prevention training, including both physiological/biomechanical and psychological components, as well as an associated context‐specific implementation plan in partnership with all stakeholders should be a high priority to ensure successful implementation of injury prevention training in youth team handball.
While previous studies on injury prevention in youth team ball sports have focused on the perspectives of coaches,10, 11, 12, 13 or coaches and administrators,14 we included all stakeholders involved in youth players safety and health, in line with the ecological model introduced by Emery et al. 15
There is no “one size fits all” for either injury prevention training or implementation strategies.27 Applying knowledge from a variety of stakeholders enables an effective researcher‐practitioner partnership, enhancing the likelihood of developing appropriate and meaningful context‐specific injury prevention training and implementation activities, to optimize the translation of the program.
Integrating behavioral and social science theories and models in studies to facilitate the implementation of health promoting behaviors, including injury prevention in sports,8, 15 is required to achieve behavioral change at multiple levels.41 In the context of sports, behavior change among players (health beneficiaries), coaches, and other staff (program deliverers) as well as club and organizational representatives (policymakers) is needed to ensure the adoption and sustain high fidelity implementation of injury prevention training.
Supporting information
ACKNOWLEDGEMENTS
The authors would like to thank all participants, in particular the key representatives from the two handball clubs, for their collaboration in the study. The study was funded by the Swedish Research Council for Sport Science, the Crafoord Foundation, Anna‐Greta Crafoord's Foundation, the Kocks Foundation, and Pia Ståhl's Foundation.
Ageberg E, Bunke S, Lucander K, Nilsen P, Donaldson A. Facilitators to support the implementation of injury prevention training in youth handball: A concept mapping approach. Scand J Med Sci Sports. 2019;29:275–285. 10.1111/sms.13323
REFERENCES
- 1. Bergeron MF, Mountjoy M, Armstrong N, et al. International Olympic Committee consensus statement on youth athletic development. Br J Sports Med. 2015;49:843‐851. [DOI] [PubMed] [Google Scholar]
- 2. Åman M, Forssblad M, Larsen K. Incidence and body location of reported acute sport injuries in seven sports using a national insurance database. Scand J Med Sci Sports. 2017;28:1147‐1158. [DOI] [PubMed] [Google Scholar]
- 3. Cheron C, Le Scanff C, Leboeuf‐Yde C. Association between sports type and overuse injuries of extremities in children and adolescents: a systematic review. Chiropr Man Therap. 2016;24:41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Olsen OE, Myklebust G, Engebretsen L, Bahr R. Injury pattern in youth team handball: a comparison of two prospective registration methods. Scand J Med Sci Sports. 2006;16:426‐432. [DOI] [PubMed] [Google Scholar]
- 5. Soomro N, Sanders R, Hackett D, et al. The efficacy of injury prevention programs in adolescent team aports: a Meta‐analysis. Am J Sports Med. 2016;44:2415‐2424. [DOI] [PubMed] [Google Scholar]
- 6. Rössler R, Donath L, Verhagen E, Junge A, Schweizer T, Faude O. Exercise‐based injury prevention in child and adolescent sport: a systematic review and meta‐analysis. Sports Med. 2014;44:1733‐1748. [DOI] [PubMed] [Google Scholar]
- 7. Emery CA, Roy TO, Whittaker JL, Nettel‐Aguirre A, van Mechelen W. Neuromuscular training injury prevention strategies in youth sport: a systematic review and meta‐analysis. Br J Sports Med. 2015;49:865‐870. [DOI] [PubMed] [Google Scholar]
- 8. Finch CF, Donaldson A. A sports setting matrix for understanding the implementation context for community sport. Br J Sports Med. 2010;44:973‐978. [DOI] [PubMed] [Google Scholar]
- 9. Donaldson A, Finch CF. Applying implementation science to sports injury prevention. Br J Sports Med. 2013;47:473‐475. [DOI] [PubMed] [Google Scholar]
- 10. O'Brien J, Finch CF. Injury prevention exercise programmes in professional youth soccer: understanding the perceptions of programme deliverers. BMJ Open Sport Exerc Med. 2016;2:e000075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Saunders N, Otago L, Romiti M, Donaldson A, White P, Finch C. Coaches' perspectives on implementing an evidence‐informed injury prevention programme in junior community netball. Br J Sports Med. 2010;44:1128‐1132. [DOI] [PubMed] [Google Scholar]
- 12. Norcross MF, Johnson ST, Bovbjerg VE, Koester MC, Hoffman MA. Factors influencing high school coaches' adoption of injury prevention programs. J Sci Med Sport. 2016;19:299‐304. [DOI] [PubMed] [Google Scholar]
- 13. Lindblom H, Carlfjord S, Hägglund M. Adoption and use of an injury prevention exercise program in female football: a qualitative study among coaches. Scand J Med Sci Sports. 2017;28(3):1295‐1303. [DOI] [PubMed] [Google Scholar]
- 14. Donaldson A, Callaghan A, Bizzini M, Jowett A, Keyzer P, Nicholson M. A concept mapping approach to identifying the barriers to implementing an evidence‐based sports injury prevention programme. Inj Prev. 2018. 10.1136/injuryprev-2017-042639. [DOI] [PubMed] [Google Scholar]
- 15. Emery CA, Hagel B, Morrongiello BA. Injury prevention in child and adolescent sport: whose responsibility is it? Clin J Sport Med. 2006;16:514‐521. [DOI] [PubMed] [Google Scholar]
- 16. O'Brien J, Donaldson A, Finch CF. It will take more than an existing exercise programme to prevent injury. Br J Sports Med. 2016;50:264‐265. [DOI] [PubMed] [Google Scholar]
- 17. Klugl M, Shrier I, McBain K, et al. The prevention of sport injury: an analysis of 12,000 published manuscripts. Clin J Sport Med. 2010;20:407‐412. [DOI] [PubMed] [Google Scholar]
- 18. O'Brien J, Finch CF. The implementation of musculoskeletal injury‐prevention exercise programmes in team ball sports: a systematic review employing the RE‐AIM framework. Sports Med. 2014;44:1305‐1318. [DOI] [PubMed] [Google Scholar]
- 19. Finch C. A new framework for research leading to sports injury prevention. J Sci Med Sport. 2006;9:3‐9. [DOI] [PubMed] [Google Scholar]
- 20. Padua DA, Frank B, Donaldson A, et al. Seven steps for developing and implementing a preventive training program: lessons learned from JUMP‐ACL and beyond. Clin Sports Med. 2014;33:615‐632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Trochim W, Kane M. Concept mapping: an introduction to structured conceptualization in health care. Int J Qual Health Care. 2005;17:187‐191. [DOI] [PubMed] [Google Scholar]
- 22. Rosas SR, Kane M. Quality and rigor of the concept mapping methodology: a pooled study analysis. Eval Program Plann. 2012;35:236‐245. [DOI] [PubMed] [Google Scholar]
- 23. Donaldson A, Finch CF. Planning for implementation and translation: seek first to understand the end‐users' perspectives. Br J Sports Med. 2012;46:306‐307. [DOI] [PubMed] [Google Scholar]
- 24. Powell BJ, Beidas RS, Lewis CC, et al. Methods to improve the selection and tailoring of implementation strategies. J Behav Health Serv Res. 2017;44:177‐194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Kane M, Trochim W. Concept Mapping for Planning and Evaluation. Thousand Oaks, CA: Sage Publications; 2007. [Google Scholar]
- 26. Concept Systems, Incorporated . Build 2013.322.11. Web‐based Platform. 2012; https://www.conceptsystemsglobal.com
- 27. Donaldson A, Lloyd DG, Gabbe BJ, et al. Scientific evidence is just the starting point: a generalizable process for developing sports injury prevention interventions. Journal of Sport and Health Science. 2016;5:334‐341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Myklebust G, Engebretsen L, Braekken IH, Skjolberg A, Olsen OE, Bahr R. Prevention of anterior cruciate ligament injuries in female team handball players: a prospective intervention study over three seasons. Clin J Sport Med. 2003;13:71‐78. [DOI] [PubMed] [Google Scholar]
- 29. Petersen W, Braun C, Bock W, et al. A controlled prospective case control study of a prevention training program in female team handball players: the German experience. Arch Orthop Trauma Surg. 2005;125:614‐621. [DOI] [PubMed] [Google Scholar]
- 30. Wedderkopp N, Kaltoft M, Lundgaard B, Rosendahl M, Froberg K. Prevention of injuries in young female players in European team handball. A prospective intervention study. Scand J Med Sci Sports. 1999;9:41‐47. [DOI] [PubMed] [Google Scholar]
- 31. Andersson SH, Bahr R, Clarsen B, Myklebust G. Preventing overuse shoulder injuries among throwing athletes: a cluster‐randomised controlled trial in 660 elite handball players. Br J Sports Med. 2017;51:1073‐1080. [DOI] [PubMed] [Google Scholar]
- 32. Soligard T, Nilstad A, Steffen K, et al. Compliance with a comprehensive warm‐up programme to prevent injuries in youth football. Br J Sports Med. 2010;44:787‐793. [DOI] [PubMed] [Google Scholar]
- 33. Keats MR, Emery CA, Finch CF. Are we having fun yet? Fostering adherence to injury preventive exercise recommendations in young athletes. Sports Med. 2012;42:175‐184. [DOI] [PubMed] [Google Scholar]
- 34. Ivarsson A, Tranaeus U, Johnson U, Stenling A. Negative psychological responses of injury and rehabilitation adherence effects on return to play in competitive athletes: a systematic review and meta‐analysis. Open Access J Sports Med. 2017;8:27‐32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Johnson U, Ivarsson A. Psychological predictors of sport injuries among junior soccer players. Scand J Med Sci Sports. 2011;21:129‐136. [DOI] [PubMed] [Google Scholar]
- 36. Ekstrand J, Lundqvist D, Lagerback L, Vouillamoz M, Papadimitiou N, Karlsson J. Is there a correlation between coaches' leadership styles and injuries in elite football teams? A study of 36 elite teams in 17 countries. Br J Sports Med. 2017;52:527‐531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Brandes M, Elvers S. Elite youth soccer players' physiological responses, time‐motion characteristics, and game performance in 4 vs. 4 small‐sided games: the influence of coach feedback. J Strength Cond Res. 2017;31:2652‐2658. [DOI] [PubMed] [Google Scholar]
- 38. Nilsen P, Roback K, Broström A, Ellström PE. Creatures of habit: accounting for the role of habit in implementation research on clinical behaviour change. Implement Sci. 2012;7:53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. McGlashan AJ, Finch CF. The extent to which behavioural and social sciences theories and models are used in sport injury prevention research. Sports Med. 2010;40:841‐858. [DOI] [PubMed] [Google Scholar]
- 40. Bekker S, Paliadelis P, Finch CF. The translation of sports injury prevention and safety promotion knowledge: insights from key intermediary organisations. Health Res Policy Syst. 2017;15:25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Nilsen P. Making sense of implementation theories, models and frameworks. Implement Sci. 2015;10:53. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials