

Abstract
Background and Objectives:
Hypertension is an important disease of public health concern. Awareness and medication adherence with diet modification have an important effect on the control of blood pressure and its associated morbidity and mortality. Therefore, this study was conducted to assess the awareness of hypertension, medication adherence, and dietary pattern in hypertensive population of western Rajasthan.
Materials and Methods:
The study was hospital based cross-sectional. Blood pressure measurements were taken in a sitting position in right arm after a 5-min rest using nonmercury sphygmomanometer and required cuff size. A prevalidated and pretested questionnaire for the assessment of awareness of hypertension was used.
Results:
Out of the total 384 patients, the majority of the patients were males (62.5%). There was a statistically significant difference found in awareness of hypertension among rural and urban patients. Nonadherence to antihypertensive medications was seen more in males (60.0%) as compared to females (40.0%). The most common reason for nonadherence was found to be forgetfulness (27.6%) followed by poor knowledge about the hypertension and ignorance of long-term treatment (22.9%). Out of the total hypertensive patient studied, 54.9% were taking normal salt intake and 45.1% of the subjects were found to be taking excess intake of salt.
Interpretation and Conclusions:
In the present study, good awareness about hypertension was found with urban patients. Among all the variables, education and employment status showed a positive and significant association with awareness. The most common reason of poor adherence was found to be forgetfulness behavior followed by poor knowledge and lack of awareness about hypertension.
Keywords: Adherence, awareness, diet pattern, hypertension, Rajasthan
Introduction
Hypertension is an important disease of public health concern and is considered to be one of the major risk factors of cardiovascular diseases, stroke, and renal dysfunction. Globally in 2017, hypertension was the leading risk factor, accounting for 10·4 million (9·39–11·5) deaths and 218 million (198–237) disability-adjusted life years (DALYs).[1] It was consistently responsible for the largest number of all-cause deaths between 1990 and 2017. The Indian Hypertension Guidelines, 2013 defines the blood pressure levels between 130–139/80–89 as “high normal,” 120–129/below 80 as “normal,” and below 120/below 80 as “optimal.”[2] Although the latest ACC/AHA hypertension guidelines proposed a lower threshold of >130/or 80 mmHg for diagnosing high blood pressure, most of the Indian studies are based on the threshold of >140/or 90 mmHg.[3] According to Fourth National Family Health Survey (NFHS-4), the overall prevalence of hypertension is 11.3% with prevalence in men (15–54 years) and women (15–49 years) of 13.6% and 8.8%, respectively.[4] The prevalence in Rajasthan in the same study was 12.4% in men and 6.9% in women.
Awareness about the disease and its associated morbidity has an important role in managing the impact of hypertension in public. In addition, low awareness has a direct influence on medication adherence which ultimately leads to poor clinical outcome. World Health Organization defines medication adherence as “the degree to which the person's behavior corresponds with the agreed recommendations from a health care provider.”[5] Adherence to medication regimen is very important in management of any disease as well as in improving the quality life of patients. Due to poor adherence, the blood pressure control is inadequate in 50%–75% of patients being treated for hypertension.[6]
The study of dietary pattern in hypertension is also very important in countries like India with its vast diversity. Most of the population is unaware of the fact that their diet includes most of fat and less of the essential nutrients. As Rajasthani food is famous all over the world and domicile population is fond of ghee and oil preparations in their diet like daal bati, mirchi bada, samosa, etc., it is quite necessary to study the dietary pattern of hypertensive patients and also whether they are aware of DASH diet (Dietary approaches to Stop Hypertension).
Therefore, this study was done to assess the awareness of hypertension, medication adherence, and dietary pattern in a hypertensive population of western Rajasthan.
Materials and Methods
Study design and setting
The study was hospital-based cross-sectional, conducted at Department of Cardiology, All India Institute of Medical Sciences (AIIMS), Jodhpur, a tertiary care teaching institute. The ethical clearance was obtained from Ethical Review Committee, AIIMS Jodhpur (AIIMS/IEC/2019/866). The hypertensive patients above the age of 18 years attending the Out Patient Department (OPD) from February 2019 to May 2019 were included. Informed written consent was taken from all patients and demographic details with clinical history were obtained. Patients below 18 years of age, mentally incompetent to give clinical history or unwilling to participate, and pregnancy were excluded from the study.
Study methodology
Blood pressure measurements were taken in a sitting position in right arm after a 5-min rest using nonmercury sphygmomanometer and required cuff size. Two readings were taken 5 min apart and the mean of the two was taken as the blood pressure. Hypertension was defined as SBP >140 mmHg and or DBP >90 mmHg or was known case of hypertension and on antihypertensive medications. A prevalidated and pretested questionnaire for the assessment of awareness of hypertension was used. The medication adherence was assessed using Morisky Medication Adherence Scale (MMAS-8). The original version of this self-reported scale had 4 items regarding common medication taking behaviors leading to the omission of drug.[7] Later, it was modified to overcome some of its limitations by adding 4 more items addressing the circumstances surrounding adherence behavior and hence named as 8-item Morisky Medication Adherence Scale (MMAS-8).[8] It consists of 8-point questions (never/rarely/sometimes/often/always) and the last of which is a 5 point Likert-scale rating. Scores for the scale range within low adherence (<6), medium adherence (6 to <8), and high adherence (=8). Patients who answered “yes” for at least one question were considered as nonadherent. Diet plan was assessed with the help of Dietary guidelines for Indians by National Institute of Nutrition. Seven-day diet recall pattern was used.
Statistical analysis
A sample size of 383 was estimated by using the formula N = Z2 PQ/l2 where Z = 1.96, P = prevalence, Q = 100-P, and l = precision, where P is taken to be 52.6%. Data was entered in Microsoft excel and was analyzed using Statistical Package for the Social Sciences (SPSS) version 21. Nominal data like gender, presence or absence of knowledge, etc. was described using counts and proportions and analyzed using Chi-square test or Fisher's exact test as applicable. Interval/ratio type of data, e.g., age, was described using mean and standard deviation and was analyzed using unpaired t-test. Inferences are drawn using Chi-square test and univariate logistic regression. A P value of less than 0.05 was considered significant. Appropriate tables and graphs have been prepared.
Results
In this study, out of the total 384 patients, the maximum number (47.4%) were in the age group of 41–60 years. The young hypertensives <40 years of age were 15.9%, whereas >60 years of age were 36.7%. The majority of the patients were males (240, 62.5%). The distribution among rural and urban area was almost equal (Rural, 191; Urban, 193) [Table 1 and Figure 1]. Out of the total, 7.9% of males and 47.2% of females were found to be illiterate [Table 1]. Almost all the females in rural (98.3%) and in urban (93%) area were housewives. 19.5% of males in rural and 32.7% in urban were found to be unemployed [Table 1 and Figure 2].
Table 1.
Distribution of subjects according to sociodemographic characteristics
| Sociodemographic | Rural (n=191) | Urban (n=193) | Total (n=384) | |||
|---|---|---|---|---|---|---|
| Male (n=133) No. (%) | Female (n=58) No. (%) | Male (n=107) No. (%) | Female (n=86) No. (%) | Male (n=240) No. (%) | Female (n=144) No. (%) | |
| Age group | ||||||
| 20-40 years | 28 (21.1) | 6 (10.3) | 16 (15.0) | 11 (12.8) | 44 (18.3) | 17 (11.8) |
| 40-60 years | 64 (48.1) | 31 (53.4) | 44 (41.1) | 43 (50.0) | 108 (45.0) | 74 (51.4) |
| >60 years | 41 (30.8) | 21 (36.2) | 47 (43.9) | 32 (37.2) | 88 (36.7) | 53 (36.8) |
| Marital status | ||||||
| Married | 131 (98.5) | 58 (100.0) | 103 (96.3) | 84 (97.7) | 234 (97.5) | 142 (98.6) |
| Unmarried | 2 (1.5) | 0 (0.0) | 4 (3.7) | 2 (2.3) | 6 (2.5) | 2 (1.4) |
| Education | ||||||
| Illiterate | 14 (10.5) | 40 (69.0) | 5 (4.7) | 28 (32.6) | 19 (7.9) | 68 (47.2) |
| Primary school | 62 (46.6) | 17 (29.3) | 20 (18.7) | 24 (27.9) | 82 (34.2) | 41 (28.5) |
| Secondary education | 21 (15.8) | 1 (1.7) | 23 (21.5) | 11 (12.8) | 44 (18.3) | 12 (8.3) |
| Senior secondary education | 12 (9.0) | 0 (0.0) | 11 (10.3) | 4 (4.7) | 23 (9.6) | 4 (2.8) |
| Graduation | 16 (12.0) | 0 (0.0) | 34 (31.8) | 7 (8.1) | 50 (20.8) | 7 (4.9) |
| Post graduation | 8 (6.0) | 0 (0.0) | 14 (13.1) | 12 (14.0) | 22 (9.2) | 12 (8.3) |
| Occupation | ||||||
| Self-employed | 23 (17.3) | 0 (0.0) | 34 (31.8) | 1 (1.2) | 57 (23.8) | 1 (0.7) |
| Unemployed (Housewives) | 26 (19.5) | 57 (98.3) | 35 (32.7) | 80 (93.0) | 61 (25.4) | 137 (95.1) |
| Daily wage workers | 6 (4.5) | 0 (0.0) | 4 (3.7) | 0 (0.0) | 10 (4.2) | 0 (0.0) |
| In service (Govt./Private) | 36 (27.1) | 1 (1.7) | 31 (29.0) | 5 (5.8) | 67 (27.9) | 6 (4.2) |
| Farmers | 42 (31.6) | 0 (0.0) | 3 (2.8) | 0 (0.0) | 45 (18.8) | 0 (0.0) |
Figure 1.
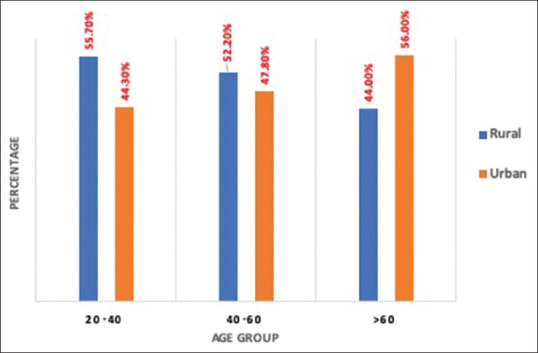
Bar chart showing distribution of study subjects according to age and area of residence
Figure 2.

Pie chart showing distribution of subjects according to their occupation
There was no significant difference found in the distribution of subjects between controlled and uncontrolled blood pressure. The majority of the patients (65.4%) had uncontrolled blood pressure, out of which 63.7% were males and 36.3% were females. In total, 47.4% of study subjects in rural area and 52.6% in urban area had uncontrolled blood pressure. More than half of the unemployed subjects were found to be having controlled blood pressure (55.6%). Among the illiterate, 24.1% had controlled blood pressure and 21.9% had uncontrolled blood pressure [Table 2].
Table 2.
Distribution of subjects with controlled and uncontrolled blood pressure as per their gender, marital status, area of residence, educational level, and their occupation (n=384)
| Variables | Blood pressure | P | |||
|---|---|---|---|---|---|
| Controlled (110-140/60-90 mmHg) | Uncontrolled (>140/90 mmHg) | ||||
| n=133 | 34.6% | n=251 | 65.4% | ||
| Gender | |||||
| Male | 80 | 60.2 | 160 | 63.7 | 0.508 |
| Female | 53 | 39.8 | 91 | 36.3 | |
| Marital status | |||||
| Married | 130 | 97.7 | 246 | 98.0 | 1.00 |
| Unmarried | 3 | 2.3 | 5 | 2.0 | |
| Residence | |||||
| Rural | 72 | 54.1 | 119 | 47.4 | 0.238 |
| Urban | 61 | 45.9 | 132 | 52.6 | |
| Education | |||||
| Illiterate | 32 | 24.1 | 55 | 21.9 | 0.876 |
| Primary school | 44 | 33.1 | 79 | 31.5 | |
| Secondary education | 17 | 12.8 | 39 | 15.5 | |
| Senior secondary education | 8 | 6.0 | 19 | 7.6 | |
| Graduation | 22 | 16.5 | 35 | 13.9 | |
| Post-graduation | 10 | 7.5 | 24 | 9.6 | |
| Occupation | |||||
| Self-employed | 14 | 10.5 | 44 | 17.5 | 0.148 |
| Unemployed | 74 | 55.6 | 124 | 49.4 | |
| Daily wage workers | 5 | 3.8 | 5 | 2.0 | |
| In service (Govt./Private) | 21 | 15.8 | 52 | 20.7 | |
| Farmers | 19 | 14.3 | 26 | 10.4 | |
There was a statistically significant difference found in awareness of hypertension among the rural and urban patients. The majority of the population in rural (85.3%) as well as in urban (94.3%) were aware about their hypertension status. Almost half of the urban patients were knowing about the normal value of blood pressure (120/80 mmHg; 50.8% vs 29.8% rural) and >140/90 mmHg as high blood pressure (49.7% vs 30.4%) and also remembered their recent visit blood pressure value (52.3% vs 28.3%). Almost 85% of urban patients were knowing that hypertension is a treatable condition and control of high blood pressure prevents complications and organ damage. But only 64.2% of urban patients and 50.8% of rural patients were knowing that smoking is a risk factor for hypertension [Table 3]. There was a significant difference between rural and urban population regarding awareness scoring. 88.1% of urban patients had good to excellent awareness score as compared to 63.9% of rural patients [Figure 3]. With univariate logistic regression analysis, predictors of good awareness were urban residence, employed, and higher education, whereas male gender and age <60 years were statistically not significant predictors [Table 4].
Table 3.
Area wise distribution of subjects as per their awareness of hypertension (n=384)
| Questions | Rural (n=191) | Urban (n=193) | P |
|---|---|---|---|
| Knowing about having hypertension | 163 (85.3) | 182 (94.3) | 0.004* |
| Knowing normal values of BP as 120/80 mmHg | 57 (29.8) | 98 (50.8) | 0.001* |
| Knowing values of BP at recent visit | 54 (28.3) | 101 (52.3) | 0.001* |
| Increase in BP >140/90 mmHg called hypertension | 58 (30.4) | 96 (49.7) | 0.001* |
| Both the sexes have equal chance of developing hypertension | 85 (44.5) | 126 (65.3) | 0.001* |
| Hypertension is a treatable condition | 136 (71.2) | 170 (88.1) | 0.001* |
| Controlling of BP reduces your complications | 119 (62.3) | 166 (86.0) | 0.001* |
| Uncontrolled hypertension can lead to your organ’s damage | 119 (62.3) | 164 (85.0) | 0.001* |
| Smoking is a risk factor for hypertension | 97 (50.8) | 124 (64.2) | 0.008* |
| Changing your lifestyle helps to lower your BP | 103 (53.9) | 151 (78.2) | 0.001* |
*P<0.05 was considered as statistically significant
Figure 3.
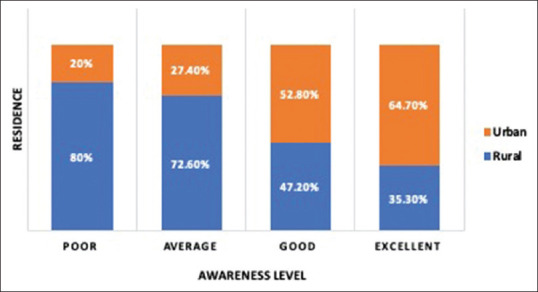
Distribution of awareness level as per area of residence
Table 4.
Univariate logistic regression analysis showing predictors of good awareness
| Variable | Awareness (Good) 354 (92.2%) | OR (95%CI) | P |
|---|---|---|---|
| Age (<60 years) | 229 (94.2%) | 2.094 (0.98-4.43) | 0.05 |
| Gender (Male) | 226 (94.2%) | 2.018 (0.95-4.26) | 0.06 |
| Residence (Urban) | 187 (96.9%) | 4.48 (1.79-11.22) | 0.001* |
| Education (Higher education) | 167 (96.0%) | 2.934 (1.228-7.01) | 0.015* |
| Occupation (Employed) | 128 (97.7%) | 5.097 (1.516-17.134) | 0.008* |
*P<0.05 was considered as statistically significant
Out of 359 patients who were known case of hypertension, 245 (68.2%) were nonadherent to medications and 114 (31.8%) were adherent. There was statistically no significant association found for medication adherence as per their gender, marital status, area of residence, education status, and occupation [Table 5]. But nonadherence to antihypertensive medications was seen more in males (60.0%) as compared to females (40.0%). With univariate logistic regression, no single predictor was found to be statistically significant for nonadherence of medications [Table 6].
Table 5.
Distribution of subjects with medication adherence as per their gender, marital status, area of residence, educational level, and their occupation (n=359)
| Variables | Adherent | Nonadherent | P | ||
|---|---|---|---|---|---|
| n=114 | 31.8% | n=245 | 68.2% | ||
| Gender | |||||
| Male | 73 | 64.0 | 147 | 60.0 | 0.465 |
| Female | 41 | 36.0 | 98 | 40.0 | |
| Marital status | |||||
| Married | 112 | 98.2 | 241 | 98.4 | 0.933 |
| Unmarried | 2 | 1.8 | 4 | 1.6 | |
| Residence | 0.474 | ||||
| Rural | 60 | 52.6 | 119 | 48.6 | |
| Urban | 54 | 47.4 | 126 | 51.4 | |
| Education | |||||
| Illiterate | 21 | 18.4 | 62 | 25.3 | 0.148 |
| Primary school | 41 | 36.0 | 74 | 30.2 | |
| Secondary education | 17 | 14.9 | 35 | 14.3 | |
| Senior secondary education | 3 | 2.6 | 20 | 8.2 | |
| Graduation | 22 | 19.3 | 32 | 13.1 | |
| Post graduation | 10 | 8.8 | 22 | 9.0 | |
| Occupation | 0.077 | ||||
| Self-employed | 16 | 14.0 | 36 | 14.7 | |
| Unemployed | 56 | 49.1 | 135 | 55.1 | |
| Daily wage workers | 1 | 0.9 | 7 | 2.9 | |
| In service (Govt./Private) | 20 | 17.5 | 46 | 18.8 | |
| Farmers | 21 | 18.4 | 21 | 8.6 | |
Table 6.
Univariate logistic regression analysis showing predictors of medication adherence
| Variable | Medication adherence (nonadherent) 245 (68.2%) | OR (95%CI) | P |
|---|---|---|---|
| Age (≤60 years) | 153 (68.9%) | 1.085 (0.69-1.71) | 0.72 |
| Gender (Female) | 98 (70.5%) | 1.187 (0.75-1.89) | 0.46 |
| Residence (Urban) | 126 (70.0%) | 1.176 (0.75-1.83) | 0.47 |
| Education (Primary education) | 136 (68.7%) | 1.046 (0.67-1.63) | 0.84 |
| Occupation (Employed) | 82 (69.5%) | 1.090 (0.67-1.75) | 0.72 |
| Awareness (Poor) | 18 (72.0%) | 1.212 (0.49-2.9) | 0.67 |
Based on the Morisky adherence questionnaire, 39.7% of rural patients forgot to take medication as compared to 14.4% of urban patients, although which was statistically not significant. Irregularity in compliance was more in rural patients (38.5%) as compared to urban patients (22.8%) and this behavior was statistically significantly different [P < 0.001; Table 7]. The most common reason for nonadherence was found to be forgetfulness (27.6%) followed by poor knowledge about the hypertension and ignorance of long - term treatment (22.9%; Table 8). Few of the patients (8.9%) gave the reason that their medicines became out of stock so they were unable to take their medicines. Only 1.3% patients found expenses as the reason for noncompliance. Out of the total uncontrolled blood pressure patients, 55.4% were taking normal salt intake and 44.6% were taking in excess but was statistically nonsignificant [P = 0.816; Table 9].
Table 7.
Patient’s drug adherence of hypertension as per area of residence (n=359)
| Questions | Rural (n=179) | Urban (n=180) | P |
|---|---|---|---|
| 1. Do you sometimes forget to take your medication? | 71 (39.7) | 83 (14.4) | 0.217 |
| If Yes - Rarely | 17 (9.5) | 26 (27.8) | 0.439 |
| Sometimes | 46 (25.7) | 50 (3.9) | |
| Usually | 8 (4.5) | 7 (53.9) | |
| All the time | 0 (0.0) | 0 (0.0) | |
| 2. Thinking over the past 2 weeks, were there any days when you did not take your medication? | 72 (40.2) | 52 (28.9) | 0.024* |
| 3. Have you ever stopped or taken again medication without telling doctor? | 69 (38.5) | 41 (22.8) | 0.001* |
| 4. When you leave/travel home, do you sometimes forget to take your medication? | 26 (14.5) | 28 (15.6) | 0.785 |
| 5. Did you take your medicine yesterday? | 37 (20.7) | 18 (10.0) | 0.005* |
| 6. When you feel like your health is under control, do you sometimes stop your medication? | 61 (34.1) | 48 (26.7) | 0.127 |
| 7. Do you ever feel hassled about sticking to your treatment plan? | 22 (12.3) | 20 (11.1) | 0.728 |
| 8. How often do you have difficulty in remembering to take all your medicines? | |||
| Rarely | 0 (0.0) | 1 (0.6) | 0.383 |
| Sometimes | 16 (8.9) | 17 (9.4) | |
| Usually | 6 (3.4) | 2 (1.1) | |
| All the time | 0 (0.0) | 0 (0.0) |
*P<0.05 was considered as statistically significant
Table 8.
Reasons for nonadherence of drugs (n=359)
| Reasons | Multiple responses |
|---|---|
| Forgetfulness | 106 (27.6%) |
| Poor knowledge of disease and ignorance of long-term treatment | 88 (22.9%) |
| Drug out of stock | 34 (8.9%) |
| Adverse drug reactions | 33 (8.6%) |
| Being busy or late for work | 21 (5.5%) |
| Poor communication/insufficient information by a healthcare provider | 17 (4.4%) |
| Being away on weekend/vacation | 12 (3.1%) |
| Patient not believing that health depends on medicine | 12 (3.1%) |
| Too many medications to take | 8 (2.1%) |
| Expenses (doctor’s fees, transport, medicines, and hospitalization) | 5 (1.3%) |
| Lack of reminders | 3 (0.8%) |
| Interruptions of daily routine | 2 (0.5%) |
| Religious beliefs and cultural practices | 1 (0.3%) |
Table 9.
Distribution of study subjects as per their level of awareness on salt intake
| Awareness | Salt intake (n=384) | P | |
|---|---|---|---|
| Normal intake | Excess intake | ||
| Poor | 12 (5.7%) | 18 (10.4%) | 0.087 |
| Good | 199 (94.3%) | 155 (89.6%) | |
Discussion
Hypertension is one of the most important risk factors for chronic disease burden in India. It adheres to “rule of halves,” i.e., half of the patients are undiagnosed, half of the diagnosed are not treated, and half of those treated have uncontrolled blood pressure. This rule of halves was earlier observed in United States and Britain in various surveys of blood pressure and is still well suited to developing countries like India.[9,10] Therefore, it is one of the important public health challenges to population in socioeconomic and epidemiological transition and imposes a significant burden on healthcare system. As it is a modifiable disease, public health personnel should focus on increasing the awareness about the hypertension, its risk factors, and associated morbidities. The present study was conducted to assess the hypertension awareness, medication adherence, and diet pattern among hypertensive patients or newly diagnosed hypertension attending tertiary level health care facility in Western Rajasthan.
The age of the participants selected for the study varied widely from minimum 20 years to 65 years and above. Most of the study participants (47.4%) were in the age group of 40 to 60 years. The age was not found to be significantly associated with the awareness of hypertension. The effect of gender on the awareness of hypertension varied in different studies. The study from Algeria has shown that women were more aware of hypertension, receiving treatment, and had better control.[11] In our study, males had good awareness as compared to females but it was statistically insignificant. This finding is similar to the study conducted in elderly Nigerians where there was statistically insignificant difference between males and females.[12] The distribution of hypertensive patients in our study among the rural and urban area was almost equal. The urban population had 4.48 times higher odds of having good awareness as compared to rural (OR = 4.48, 95% CI), which was statistically significant (P = 0.001). This study replicates the findings of metanalysis in Indian patients which showed that 25% of rural and 42% of urban patients were aware of their hypertensive status.[13] The relationship of education with awareness is directly proportional. In our study, subjects with higher education had 2.93 times higher odds of having good awareness (OR = 2.934, 95%CI) and it was statistically significant (P = 0.01) and the results correspond with the study in more than 400 patients in Pakistan.[14] Employed subjects were having more awareness as compared to unemployed (OR = 5.09, 95%CI) and result was statistically significant (P = 0.008). This finding can be directly related to education level as those who had higher education were mostly employed and in turn had direct and significant association with good awareness about hypertension.
The awareness of normal and abnormal values of blood pressure is important in the management of the disease. But in our study, only 40% of participants were aware about normal values of blood pressure and their values of recorded blood pressure at recent visit. The study in 303 hypertensive Sri Lankan patients showed that 40.5% of patients were unaware of their disease status, 75.8% of patients could not recall their blood pressure values at the time of diagnosis, and 72.3% of patients were unaware of their last values of blood pressure during their hospital visit.[15] In our study, nearly 75% of patients had awareness of target organ damage due to hypertension and 66% of the patients had awareness about lifestyle modification's role in lowering blood pressure. Nearly 40% of the total patients were unaware about smoking as one of the risk factors for hypertension; therefore, better awareness is needed among the general population. The awareness score in our study showed that 41.4% had good score and 16.1% had average score. These findings correspond with the study carried out by at a tertiary care hospital in Pune, Maharashtra, India where out of 962 patients studied, 52.6% had good awareness score and 33.99% had average score.[16]
Awareness of the disease has an impact on the control of blood pressure, but in our study in spite of good awareness, 65.4% had uncontrolled blood pressure. The proportion of uncontrolled BP was found higher in males (66.7%) than females (63.2%) and was relatively more in patients residing in the urban area (52.6%) as compared to rural area (47.4%) although it was statistically insignificant. Reason for the high prevalence among urban could be their lifestyle like lack or inadequate exercise, sedentary pattern, and consumption of unhealthy diets like fast food which are high in salt and fat. The study in 200 Sudanese patients showed 36% had uncontrolled blood pressure with a significantly higher prevalence in males (61%).[17] The higher proportion of uncontrolled BP in males may be explained with increased work stress level and poor adherence to medications. The association of education status with control of blood pressure was not significant in our study although the study by Gupta et al. has related low educational status as strong marker for low hypertension awareness.[18] Subjects who were employed and had higher education level had more proportion of uncontrolled BP as compared to primary education, illiterate, or unemployed subjects. This may be due to various lifestyle factors in urban population like increased stress level due to work demand and low salaries, abnormal diet pattern, and lack of exercise.
Medication adherence also plays an important role in the control of blood pressure along with awareness. Out of 359 subjects, 68.2% were found to be nonadherent and subjects who were ≤60 years had 1.1 times higher odds of having poor or nonadherence to antihypertensive drugs. The reason could be forgetfulness as they were busy or getting late for work. A systematic review and metanalysis of more than 90,000 subjects from low and middle income countries have shown older age, female, increased knowledge, and having controlled blood pressure to be associated with more adherence.[19] However, a study in Pakistan has shown no association between education level and medication adherence.[20] In our study, the most common reason found for nonadherence was forgetfulness (27.6%) followed by poor knowledge and awareness about the hypertension and ignorance of long-term treatment (22.9%). The third common reason given by the study subjects was that they often run short of medicines and not able to purchase on time. This finding was consistent with the other study where forgetfulness was the main cause for nonadherence.
The rising affluence of urbanization has led to change in the lifestyle and has modified the dietary pattern characterized by increased consumption of diets rich in fat, sugar, and calories. The diet has a significant effect on the blood pressure and there is a reduction of 4-5 mmHg of systolic BP with the dietary modification.[21] The dietary pattern in western Rajasthan mainly consists of milk and milk products with vegetables and the same was observed in our study also with consumption of tea, green leafy vegetables, fruits, buttermilk, other vegetables like potato and besan preparations and pulse in their daily diet. Out of 384 subjects, 58.8% were consuming milk and 98.6% were taking tea almost daily. Fruits were consumed by most of them (79.68%) with 32.3% having twice a week. Almost all the subjects were consuming green leafy vegetables as well as other vegetables daily with only 10.93% of the population was nonvegetarian. The consumption of salt is directly related to increased blood pressure. In the Indian diet context, salt intake depends on several sources: salt used in the cooking, salt added at the table directly, and in the form of pickles, pappads, etc. Pickle and oil were consumed by only 24.21% of the total subjects. Out of the total hypertensive patient studied, 54.9% were taking normal salt intake and 45.1% of the subjects were found to be taking excess intake of salt. It was observed that out of total subjects who were taking excess salt intake, 45.9% were having controlled blood pressure and 44.6% were having uncontrolled blood pressure although statistically not significant. This insignificant relation was surprising but could be due to various factors like biased responses by the participants or observation bias and also sometimes, patients are not able to quantify their intake.
Conclusion
In the present study, good awareness about hypertension was found with urban patients and among all the variables, education and employment status showed a positive and significant association with awareness. The most common reason of poor adherence was found to be forgetfulness behavior followed by poor knowledge and lack of awareness about hypertension. The dietary pattern revealed that more than half of the study subjects who were found to be consuming excess salt than recommended had uncontrolled blood pressure and therefore needs modification in diet. The role of primary care physician at various primary and community health centers (PHCs and CHCs) in educating the mass about the disease and its consequences will definitely help in better management of the disease. Such measures, if carried out across the whole population, will significantly reduce the morbidity and mortality related to raised blood pressure.
Limitations
Convenience sampling technique was done which might lead to selection bias in the study. The study was limited to one study setting; hence, the results of the study may not be generalizable. Since it is a cross-sectional study design, the correlation between cause and effect could not be identified.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1923–94. doi: 10.1016/S0140-6736(18)32225-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Association of Physicians of India. Indian guidelines on hypertension (IGH) - III 2013. J Assoc Physicians India. 2013;61:6–36. [PubMed] [Google Scholar]
- 3.Whelton PK, Carey RM, Aronow WS, Casey DE, Jr, Collins KJ, Himmelfarb C, et al. ACC/AHA/AAPA/ABS/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation and management of high blood pressure in adults: Executive summary. J Am Coll Cardiol. 2018;71:2199–269. [Google Scholar]
- 4.Ram F, Paswan B, Singh SK, Lhungdim H, Sekhar C, Singh A, et al. National family health survey-4 (2015-16) Econ Pol Wkly. 2017;52:66–70. [Google Scholar]
- 5.Sabaté E. Adherence to Long-Term Therapies: Evidence for Action. Geneva, Switzerland: World Health Organization; 2003. [Google Scholar]
- 6.Berlowitz DR, Ash AS, Hickey EC, Friedman RH, Glickman M, Kader B, et al. Inadequate management of blood pressure in a hypertensive population. N Engl J Med. 1998;339:1957–63. doi: 10.1056/NEJM199812313392701. [DOI] [PubMed] [Google Scholar]
- 7.Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24:67–74. doi: 10.1097/00005650-198601000-00007. [DOI] [PubMed] [Google Scholar]
- 8.Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens. 2008;10:348–54. doi: 10.1111/j.1751-7176.2008.07572.x. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 9.Wilber JA, Barrow JG. Hypertension: A community problem. Am J Med. 1972;52:653–63. doi: 10.1016/0002-9343(72)90055-1. [DOI] [PubMed] [Google Scholar]
- 10.Kurji KH, Haines AP. Detection and management of hypertension in general practices in North West London. Br Med J. 1984;288:903–6. doi: 10.1136/bmj.288.6421.903. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bachir Cherif A, Bouamra A, Taleb A, Nedjar R, Bouraghda A, Hamida F, et al. Differences in prevalence, treatment and control rates of hypertension between male and female in the area of Blida (Algeria) Ann Cardiol Angeiol (Paris) 2017;66:123–9. doi: 10.1016/j.ancard.2017.04.009. [DOI] [PubMed] [Google Scholar]
- 12.Raji YR, Abiona T, Gureje O. Awareness of hypertension and its impact on blood pressure control among elderly Nigerians: Report from the Ibadan study of aging. Pan Afr Med J. 2017;27:190. doi: 10.11604/pamj.2017.27.190.11682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Anchala R, Kannuri NK, Pant H, Khan H, Franco OH, Di Angelantonio E, et al. Hypertension in India: A systematic review and meta-analysis of prevalence, awareness, and control of hypertension. J Hypertens. 2014;32:1170–7. doi: 10.1097/HJH.0000000000000146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Almas A, Godil SS, Lalani S, Samani ZA, Khan AH. Good knowledge about hypertension is linked to better control of hypertension; A multicentre cross sectional study in Karachi, Pakistan. BMC Res Notes. 2012;5:579. doi: 10.1186/1756-0500-5-579. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Pirasath S, Kumanan T, Guruparan M. A study on knowledge, awareness, and medication adherence in patients with hypertension from a tertiary care centre from northern Sri Lanka. Int J Hypertens. 2017;2017:9656450. doi: 10.1155/2017/9656450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Patil VN, Sangeeta D, Sagar K, Pandit PT, Ghongane BB. Survey of knowledge and awareness in patients of hypertension and survey of information that patients receive from physician for hypertension in a tertiary care hospital. WJPPS. 2015;4:980–1. [Google Scholar]
- 17.Babiker FA, Elkhalifa LA, Moukhyer ME. Awareness of hypertension and factors associated with uncontrolled hypertension in Sudanese adults. Cardiovasc J Afr. 2013;24:208–12. doi: 10.5830/CVJA-2013-035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Gupta R, Kaur M, Islam S, Mohan V, Mony P, Kumar R, et al. Association of household wealth index, educational status, and social capital with hypertension awareness, treatment, and control in South Asia. Am J Hypertens. 2017;30:373–81. doi: 10.1093/ajh/hpw169. [DOI] [PubMed] [Google Scholar]
- 19.Nielsen JO, Shrestha AD, Neupane D, Kallestrup P. Non-adherence to anti-hypertensive medication in low- and middle-income countries: A systematic review and meta-analysis of 92443 subjects. J Hum Hypertens. 2017;31:14–21. doi: 10.1038/jhh.2016.31. [DOI] [PubMed] [Google Scholar]
- 20.Khan MN, Soomro N, Ashraf T, Naseeb K, Kumar R, Bhatti U, et al. Perceptions and practices towards medication non-adherence among hypertensive patients: An observational study. Cureus. 2019;11:e5917. doi: 10.7759/cureus.5917. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ndanuko RN, Tapsell LC, Charlton KE, Neale EP, Batterham MJ. Dietary patterns and blood pressure in adults: A systematic review and meta-analysis of randomized controlled trials. Adv Nutr. 2016;7:76–89. doi: 10.3945/an.115.009753. [DOI] [PMC free article] [PubMed] [Google Scholar]