

Abstract
Background: Cowper's syringocele is cystic dilation of the excretory bulbourethral gland duct. This entity is common in the pediatric population but is rare or underdiagnosed in the adult population. Syringoceles are usually classified based on the configuration of the duct's orifice to the urethra with symptoms varying between irritative and/or obstructive accordingly. To the best of our knowledge, only few cases were reported in the literature.
Case Presentation: We present the case of a 27-year-old male patient presenting with obstructive lower urinary tract symptoms. Pelvis MRI, retrograde urethrography, and flexible cystourethroscopy were performed and a diagnosis of imperforate Cowper's syringocele was made. Endoscopic unroofing with holmium:YAG laser was performed. The patient is free of symptoms 12 months postoperatively.
Conclusion: Cowper's syringocele is a rare entity that should be considered in certain adult patients presenting with either storage or voiding symptoms. Ultrasonography is useful in detecting closed cystic lesions; however, antegrade urethrography and retrograde urethrography are gold standards to rule out communication with the urethra. Symptoms tend to resolve spontaneously and initial treatment is conservative. With persistent symptoms, endoscopic unroofing or marsupialization with cold knife or holmium:YAG laser is recommended as standard treatment.
Keywords: endourology, Cowper's syringocele, LUTS, laser
Introduction
Cowper's glands, or Bulbourethral glands, are paired accessory sexual organs situated posterolateral to the membranous portion of the male urethra at the level of the urogenital diaphragm.1,2 Alkaline mucus-like secretions of these pea-shaped glands account for neutralizing the acidity of the vagina, semen coagulation, and urethral lubrication during ejaculation.1 The glands form two collecting ducts, measuring 2.5 cm each that eventually combine to enter the ventral bulbous urethra near the midline by piercing the Corpus Spongiosum.3
Cowper's syringocele refers to the cystic dilation of these ducts. Syringoceles are traditionally rare, underdiagnosed, and affect the pediatric population. Maizels and coworkers4 first classified this entity into four types: (1) simple syringocele with mild dilation of the duct, (2) perforated syringocele with dilated distal duct that communicates with the urethra through a patulous ostium, (3) imperforate syringocele that does not communicate with the urethra, and (4) ruptured syringocele with fragile membrane remaining in the urethra after distal dilated duct ruptures.4 We hereby report a case of a young adult male with type III imperforate syringocele.
Case Report
A 27-year-old male patient, previously healthy, presented to our outpatient clinic for a 6-month history of obstructive lower urinary tract symptom (LUTS). He reported weak urinary stream, straining, and sensation of incomplete voiding with an International Prostate Symptom Score of 14. Patient denied dysuria and hematuria. Physical examination was unremarkable. Urine analysis and culture were negative. Uroflowmetry was performed that revealed a slightly decreased Qmax with an obstructive flow pattern. Retrograde urethrography showed a filling defect at the level of the anterior urethra without any evident communication into the urethra (Fig. 1). MRI showed an 8 × 5 × 4 mm well-defined heterogeneous T2 hyperintense structure at the base of penis extending from the bulbourethral glands and slightly impressing at 2.5 cm distal to the posterior edge of the bulbar urethra (Fig. 2). Finally, flexible cystourethroscopy under local anesthesia confirmed the diagnosis of an imperforate Cowper's syringocele.
FIG. 1.
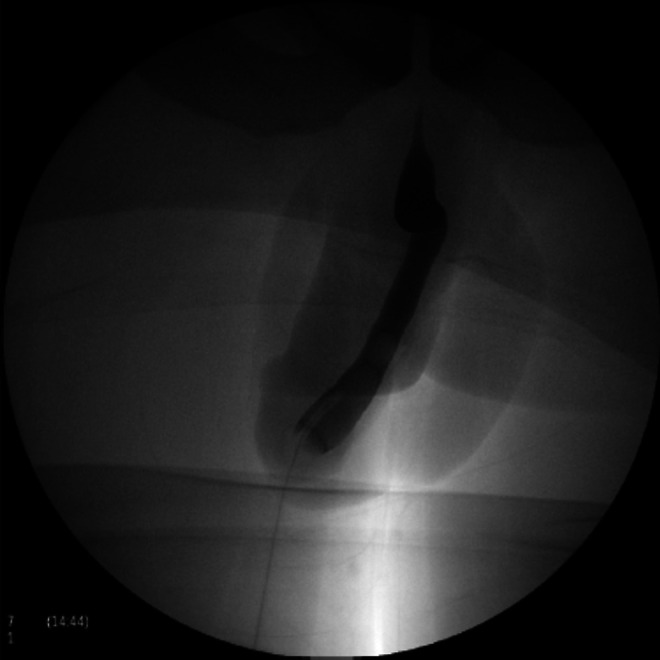
A retrograde urethrogam showing a filling defect at the level of the anterior urethra.
FIG. 2.
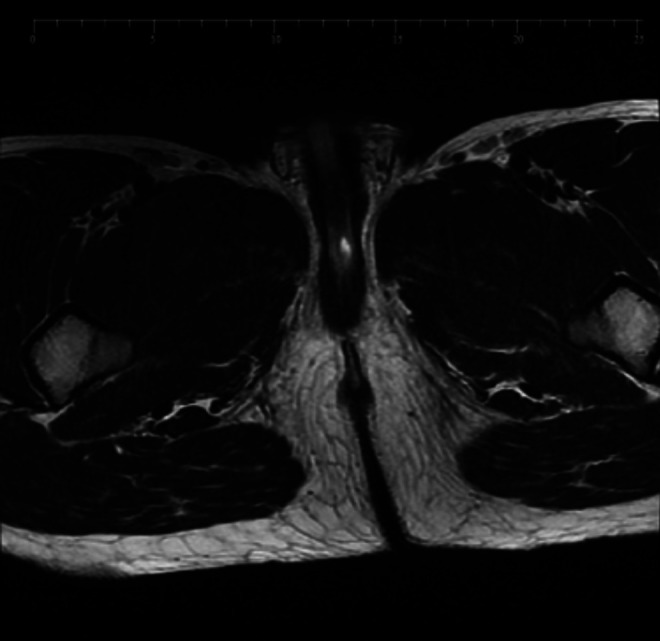
A T2 weighted sequence on pelvis MRI showing a well-defined hyperintense structure impressing the bulbous urethra.
Under spinal anesthesia, surgical endoscopic unroofing of the syringocele was performed using holmium:YAG laser (Fig. 3). An 18F Foley catheter was placed. Postoperative recovery was uneventful. The patient was discharged on the first postoperative day with the urinary catheter maintained in place for 1 week. The patient remained asymptomatic during the 12-month follow-up period.
FIG. 3.

(A) Identification of Cowper's syringocele during flexible cystourethroscopy. (B) Endoscopic unroofing with holmium:YAG laser. (C) Unroofing of Cowper's syringocele. (D) Endoscopic view after completion of unroofing.
Discussion
Originally described in 1881 by English, Cowper's syringoceles result when the main duct of the gland undergoes cystic dilation. This entity is usually diagnosed in the pediatric age group and in considered rare in adults. To our knowledge, only few cases have been reported in the literature.1,4 According to Maizels and coworkers.,4 syringoceles have been classified into four types: (1) simple syringocele with a modestly dilated duct, (2) perforated syringocele with patulous communication with the urethra, (3) imperforate syringocele with a dilated bulbous duct, and (4) ruptured syringocele that leaves its covering membrane in the urethra often acting in a “ball-on-chain” manner to cause obstruction.3 The etiology of Cowper's syringocele is not well understood. Stasis and pressure changes may cause obstruction to the duct orifices, resulting in accumulation of mucous and leading to cystic dilation. Based on building luminal pressures within the ducts, cystic dilations may follow a standard maturation from simple to imperforate or to either perforated or ruptured. This hypothesis is referred to as “congenital retention cyst” and could be particularly accurate in the pediatric population.1,3 However, recent literature suggests that syringoceles can be acquired in adult population, and are rather underdiagnosed or misdiagnosed than rare. Bevers et al. reported a case series of seven cases diagnosed within a timespan of 18 months only, as discussed in Melquist et al.3 It can be, therefore, speculated that symptoms are preferentially appreciated at a younger age group and neglected or not well understood in the adult population. Thus, Maizels et al.'s classification could lack clinical significance.4 Existing studies propose dividing syringoceles according to the configuration of the duct's orifice to the urethra and their symptomology into two groups: (1) closed syringoceles and (2) open syringoceles.3 For instance, closed syringoceles have occluded ducts because of a distended cyst-like swelling in the ventral wall of the urethra that causes obstructive or storage symptoms, dysuria, perineal pain, or urinary retention.1,3 Whereas open syringoceles have a continuous lumen between the cystic duct and the urethra and may present with postvoid dribbling, urethral discharge, recurrent urinary tract infections, perineal pain, or hematuria.2 In our case, the patient had a type III imperforate syringocele or a closed syringocele with obstructive LUTS as his only symptom.
Owing to the rarity of this entity, diagnostic evaluation is essentially challenging and unconventional. Proper voiding history taking and physical examination should be performed. The differential diagnosis could include urethral duplication, anterior urethral valve, anterior urethral diverticulum, congenital narrowing of bulbar urethra, urethral stricture, hydrocele, megalourethra, periurethral abscess, perianal abscess, congenital urethral folds, prolapsed posterior urethral valve, urethral tumors, and urethral stones.3 Ultrasonography is useful in detecting closed cystic lesions; however, antegrade urethrography and retrograde urethrography are gold standard to rule out communication with the urethra.4 If readily available, flexible cystourethroscopy is a safe technique that should be used to confirm diagnosis. MRI is another very useful diagnostic tool that is noninvasive and allows a wider range of vision and superior reproducibility.3,4 It allows higher soft tissue resolution allowing a precise definition of the anatomic location, size, and extent of the cyst.3
Asymptomatic syringoceles that are found incidentally are often managed conservatively. If symptoms are not relieved, surgical endoscopic intervention had become the preferred treatment modality for both open and closed syringoceles.2 Unroofing of the cyst or marsupialization using cold knife or holmium:YAG laser is relatively a simple and efficient technique that is recommended. Open procedures are only indicated if endoscopic treatment fails or if syringoceles present as a large perineal mass.2 Our patient was treated with endoscopic unroofing with holmium:YAG laser, the procedure was performed without any complications and postoperative recovery was fast and uneventful.
Conclusion
Although a rare entity in adults, Cowper's syringocele should be considered in certain adult patients presenting with either storage or voiding symptoms. Once the index of suspicion is high, ultrasonography followed by retrograde or antegrade urethrography should be performed. Cystourethroscopy and MRI are two other essential confirmatory modalities. Treatment could initially be conservative as symptoms tend to resolve spontaneously. With persistent symptoms, endoscopic unroofing or marsupialization with cold knife or holmium:YAG laser is recommended as standard treatment for both closed and open syringoceles.
Acknowledgment
We thank our colleagues from the division of urology at Saint George Hospital University Medical Center who provided insight and expertise that greatly assisted this research.
Abbreviations Used
- LUTS
lower urinary tract symptom
- MRI
magnetic resonance imaging
Disclosure Statement
No competing financial interests exist.
Cite this article as: Matta I, Chalhoub K, Abou Zahr R, Ghazal G, Huyghe E, Nohra J (2019) A case of symptomatic Cowper's syringocele in an adult male: diagnosis and management, Journal of Endourology Case Reports 5:2, 56–59, DOI: 10.1089/cren.2019.0011.
References
- 1. Awad M, Alwaal A, Harris C, Zaid U, Gaither T, Osterberg E, Breyer B. Transurethral unroofing of a symptomatic imperforate Cowper's syringocele in an adult male. Case Rep Urol 2016;2016:1–4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Taskovska M, Hawlina S. Cowper's syringocele in adolescent male: Case report. J Endourol Case Rep 2017;3:130–133 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Melquist J, Sharma V, Sciullo D, McCaffrey H, Ali Khan S. Current diagnosis and management of syringocele: A review. Int Braz J Urol 2010;36:3–9 [DOI] [PubMed] [Google Scholar]
- 4. Maizels M, Stephens F, King L, Firlit C. Cowpek's syringocele: A classification of dilatations of Cowper's gland duct based upon clinical characteristics of 8 boys. J Urol 1983;129:111–114 [DOI] [PubMed] [Google Scholar]