

Abstract
Objective
Digital media conversations can provide important insight into the concerns and struggles of people with epilepsy (PWE) outside of formal clinical settings and help generate useful information for treatment planning. Our study aimed to explore the big data from open‐source digital conversations among PWE with regard to suicidality, specifically comparing teenagers and adults, using machine learning technology.
Methods
Advanced machine‐learning empowered methodology was used to mine and structure open‐source digital conversations of self‐identifying teenagers and adults who endorsed suffering from epilepsy and engaged in conversation about suicide. The search was limited to 12 months and included only conversations originating from US internet protocol (IP) addresses. Natural language processing and text analytics were employed to develop a thematic analysis.
Results
A total of 222 000 unique conversations about epilepsy, including 9000 (4%) related to suicide, were posted during the study period. The suicide‐related conversations were posted by 7.8% of teenagers and 3.2% of adults in the study. Several critical differences were noted between teenagers and adults. A higher percentage of teenagers are: fearful of “the unknown” due to seizures (63% vs 12% adults), concerned about social consequences of seizures (30% vs 21%), and seek emotional support (29% vs 19%). In contrast, a significantly higher percentage of adults show a defeatist (“given up”) attitude compared to teenagers (42% vs 4%). There were important differences in the author's determined sentiments behind the conversations among teenagers and adults.
Significance
In this first of its kind big data analysis of nearly a quarter‐million digital conversations about epilepsy using machine learning, we found that teenagers engage in an online conversation about suicide more often than adults. There are some key differences in the attitudes and concerns, which may have implications for the treatment of younger patients with epilepsy.
Keywords: big data, epilepsy, machine learning, social media, suicide, teenagers
Key Points.
Digital media conversations can provide important insight into the concerns and struggles of people with epilepsy (PWE)
We explored the big data from open‐source digital conversations among PWE in regard to suicidality, using machine learning technology
Results showed that 222 000 unique conversations about epilepsy, including 9000 (4%) related to suicide, were posted during the study period
We found that teenagers engage in online conversation about suicide more often than adults
1. INTRODUCTION
According to the World Health Organization (WHO), around 50 million people worldwide have epilepsy, making it one of the most common neurologic disorders. 1 Suicide accounts for a large proportion of preventable deaths in epilepsy 2 and the estimated annual rate of suicide among adults with epilepsy is 22% higher than in the general population. 3 The rate for suicidal ideation in a structured interview study in youth with epilepsy was reported as 20%. 4 A metanalysis of 51 216 people with epilepsy (PWE) found that 188 individuals died of suicide, which accounted for 32.5% of the deaths in this cohort. 5 One of the major drivers of suicidal thoughts in PWE is the high incidence of depression in this population. 6 , 7 , 8 Such trends have been noted in teenagers with epilepsy as well. In a population study in Denmark, having epilepsy (among other medical conditions) was identified as one of the risk factors for suicide attempts in youth, which remained a major risk factor after adjusting for other relevant variables. 9
Social media presents a novel opportunity for engagement and interaction in a virtual environment. There are many recent examples of successful uses of social media in healthcare research. 10 , 11 , 12 , 13 Some studies have explored the use of social media by PWE to understand and explore their experiences and concerns. 14 Teenagers are the most avid users of social media and spend a substantial portion of their time on it. 15 , 16 However, to the best of our knowledge, no previous studies have analyzed the views, conversations, or sentiments expressed on digital open‐source conversations by teenagers with epilepsy, especially with regard to suicidality. Digital media provides data on a large number of individuals of various age groups that can help us contrast suicidality among teenagers and adults with epilepsy. Therefore, the purpose of our study was to analyze these big data by mining digital open‐source conversations from topical sites, message boards, social networks, and blogs (the full digital footprint) regarding suicidality among teenagers and adults with epilepsy. The primary goal of our research was to use these data to understand the mindset and sentiments about suicidality among teenagers with epilepsy.
2. METHOD
This study was approved by the Cleveland Clinic Institutional review board (IRB). A search strategy was formulated for data extraction, collection, and analysis (see below). All the information gathered from the different online open sources are in the public domain and were deidentified.
2.1. Search strategy, data extraction, and collection
The population of interest for this study were teenagers (13‐ to 19‐year‐olds) and adults (≥20 years of age), based on their self‐identification during digital conversations or on their public online profile who endorsed suffering from epilepsy and engaged in conversation about suicide, including suicidal thoughts, intent, plan, attempt, and so on. Gender‐related data were not collected. CulturIntel used its advanced artificial intelligence (AI)–empowered methodology to mine and structure the unstructured, qualitative online data on the topic of interest (epilepsy and suicide). The search was limited to 12 months, ending on September 25, 2018, and included only conversations originating from the US internet protocol (IP) addresses.
CulturIntel big data and AI suite of tools “scrapes and listens” to open conversations online. The data mining and collection occurs across various sites (topical sites, blogs, social network, and message boards) where relevant discussions are taking place. It encompasses a complete range of social discussion channels, including sites directed toward selected segments and directed by (but not limited to) their predefined topic of interest (epilepsy patients and suicide). Advanced search techniques of web spiders, crawlers, and site scrapings were applied. CulturIntel then extracted topical data and tagged data with the origin and user, which is deidentified before creating a large, unstructured “big” data set. After completion of the comprehensive data collection, natural language processing and text analytics were employed to examine previously described and undescribed patterns in the data. Natural language processing is a subfield of artificial intelligence that helps computers to process and analyze large amounts of natural human language data. Text analytics refers to the computer‐based processes used for deriving high‐quality information from text through the devising of patterns and trends, using means such as statistical pattern learning, for example, theme modeling, topical frequency, named entity recognition, and event extraction. These analyses were human‐assisted and included repeated training, testing, and reviewing of the program output by CulturIntel with the authors. In this thematic analysis, authors tagged and sorted the data, determined key motivations of topics being discussed, and assigned underlying drivers, sentiments, and barriers, as described in Table 1.
Table 1.
Sentiment analysis of conversation “drivers”
| Drivers (n) |
Teens (% of the drivers) |
Adults (% of drivers) | Quotes from teenagers | |
|---|---|---|---|---|
| Negative drivers (barriers) N = 2100 | Feeling alone | 32 | 23 | “I'm 16 and…I was wondering if anyone else feels kinda alone with epilepsy and like when you tell someone they'll just freak out…” |
| Low spirit | 25 | 31 | “My math teacher called me up in front of the class and said, "If you feel like 'something' is going to happen, just leave the room." there was a huge amount of twittering and giggling!” | |
| Social embarrassment | 28 | 17 | “I am having a really hard time lately… I'm very depressed (suicidal even), and not finding much joy in life." | |
| Sense of loss | 15 | 29 | “I'm just super annoyed with my epilepsy. It's been limiting what I can do…I can't do anything. Not only have I been having more seizures, but I also have panic and anxiety attacks.” | |
| Positive drivers, N = 96 | Encouragement via connection | 50 | 38 | “I haven't been treated any differently around my friends because of my epilepsy but I have GREAT friends. “ |
| Empowerment over the epilepsy | 41 | 23 | “ Forget the shame u may feel figure out what it is u wanna do in life make it happen it's all still possible." | |
| Adaptation to epilepsy | 9 | 39 | “Asking myself "Why me" I'm on my 3rd year of gran[d] mal epilepsy disorder doing much better… “ | |
| Neutral drivers, N = 960 | Emotional connection | 45 | 29 | “I was diagnosed with epilepsy about 6 months ago and I have been having some trouble processing everything. Does anyone have any suggestions to help? “ |
| Support | 37 | 22 | “Hey everyone! …I was wondering if anyone would like me to start a snapchat so we could chat on there?” | |
| Information and resources | 18 | 49 | “Hey everyone… I got epilepsy when I was two 1/2… I am trying to look for a support group and meet new people in my area with epilepsy… Does anyone know any places? I am going to try this one too.” |
2.2. Data analysis
To avoid duplicity of posts/conversation, subjects with more than one posting could be included in the analysis, but only if their comment was part of a unique post. A single user with multiple posts/comments within a conversation was counted once. However, users posting multiple unique comments across discussions/posts/sites were counted for each comment. A single comment, if appearing repeatedly through sharing/linking was counted and analyzed only once.
The analysis of digital conversation was divided into five primary domains:
“Who” (speaker analysis): Percentage distribution of self‐identified teenagers vs adults talking about the topic of interest online
“Where” (channel profile): Types of sites used by subjects for talking about the topic of interest online
“What” (topic analysis): Topics associated with discussions about “epilepsy and suicide”
“Why” (psychographic mindset analysis): Different psychographic (typically includes activities, interests, and opinions) mindsets of subjects talking about the topic of interest
“How” (sentiment analysis of conversation drivers): Perceived feelings (negative [barriers], positive, neutral) of subjects talking about the topic of interest
The five domains were analyzed separately for teenagers and adults. Categorical variables were analyzed as frequency or percentages. The comparison between teenagers and adults on categorical variables were made using Pearson chi‐square tests. A P‐value of <.05 was considered statistically significant.
3. RESULTS
A total of 222 000 unique conversations about epilepsy were posted online (topical sites [38%], message boards [39%], social networks [19%], and blogs [4%]) during the study period among adults and teens. Of those, 9000 (4%) conversations were related to epilepsy and suicide.
3.1. “Who” (speaker analysis)
Of all the discussions, a total of 41 000 were posted online by teenagers and 181 000 by adults. Further analysis showed that 3200 posts (7.8%) among teens were related to suicide compared to 5800 (3.2%) among adults (odds ratio [OR] 2.44, 95% confidence interval [CI] 2.33‐2.55; P < .001).
3.2. “Where” (channel profile)
The 3200 posts about suicide by teenagers with epilepsy were further analyzed for their source. A total of 2464 (77%) of them originated from message boards (eg, Epilepsy Foundation website) and topical sites (eg, Medscape) compared to 608 (19%) on social media. A complete breakdown of the source of posts from teenagers is provided in Figure 1.
FIGURE 1.
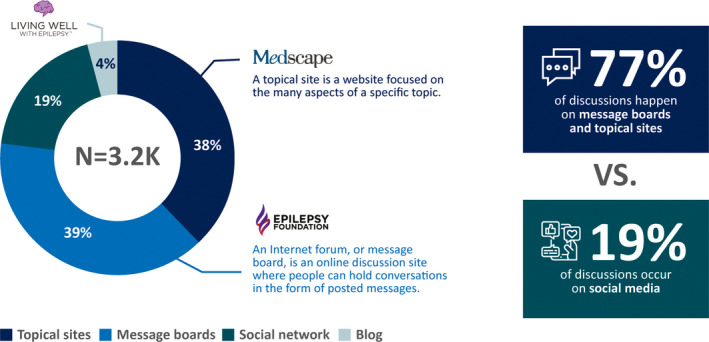
Origins of posts on suicide and epilepsy among teenagers
3.3. “What” (topic analysis)
The content analysis showed that 960 (30%) of posts by teenagers discussed social consequences of seizures (eg, “I want to be able to go out to parties with friends and date and not have to worry about having a seizure. The fact that I'm 19 and I'm unable to drive is pretty hard as well.”) compared to 1218 (21%) posts by adults (OR 1.61, 95% CI 1.46‐1.78; P < .001). Another 928 (29%) were looking for emotional support to deal with all the impact the illness has on them, both physically and emotionally (eg, “I'm 16 and I have staring seizures I was wondering if anyone else feels kinda alone with epilepsy and like when you tell someone they'll just freak out.”) as compared to 1102 (19%) adults (OR 1.74, 95% CI 1.57‐1.92; P < .001). A total of 672 (21%) of teenagers were concerned about physical impairments from seizure including pre‐ and postseizure symptoms such as dizziness, upset stomach, and temporary confusion, among others (eg, “About a month ago I was at school, I felt really sick‐ like I wanted to die, I felt dizzy, had stomach ache, and I could barely remember or pay attention to anything going on. My friend said I looked like I almost passed out but I didn't understand what she meant because my mind went blank and I was confused on what I was doing or talking about 5 seconds ago.”) compared to 1682 (29%) adults (OR 0.65, 95% CI 0.59‐0.72; P < .001). Similarly, 640 (20%) of teenagers came online for generic support and resources (eg, “Hi my name is Isabelle, I'm 14 years old and I've had epilepsy for about a year (…) 3 days ago I had a seizure and bit my tongue really hard, my tongue still hurts and it's hard to talk and eat. Idk anyone else with epilepsy and I don't have any friends so I want a friend that understands what I go through and we can both be there for each other to make each other feel better and happy.”) as compared to 1798 (31%) of adults (OR 0.56, 95% CI 0.5‐0.61; P < .001).
3.4. “Why” (psychographic mindset analysis)
As noted in Figure 2, 2016 (63%) of teenagers as compared to only 696 (12%) of adults (OR 12.49, 95% CI 11.22‐13.89; P < .001) about the "unknown" more than fearful of being depressed (eg, “I'm worried because I don't want to miss out on things and I live right on the beach and now I can't swim by myself. I'm also really worried that I will get a seizure at school [it happened once]. I've told my close friends but not really anyone else because I don't want to be known as 'the girl with epilepsy.’”). One‐third (1056, 33%) of teenagers felt helpless in front of the difficulties they face compared to 2668 (46%) of adults (OR 0.57, 95% CI 0.52‐0.62; P < .001) (eg, “Even with correct eating, diet, and meds I still have them, everyone is different (…) epilepsy patients need to understand conditions similar to addiction meds every day, the shits from the meds, the heat, climate change, stress, depression, alcohol, drug use, over the counter prescription, sugar, caffeine, diary with meds; Any one of these can hit you differently than it did the last person. First off stop pointing the finger (…) epilepsy is hard. In all aspects.”) Only 128 (4%) of teens discussing epilepsy and suicide have given up (eg, “I've still struggled to make my way, to live and enjoy life in spite of it all. I admit the thought of suicide seems the best solution for me.”) compared to 2436 (42%) of the adult population (OR 0.05, 95% CI 0.05‐0.07; P < .001).
FIGURE 2.
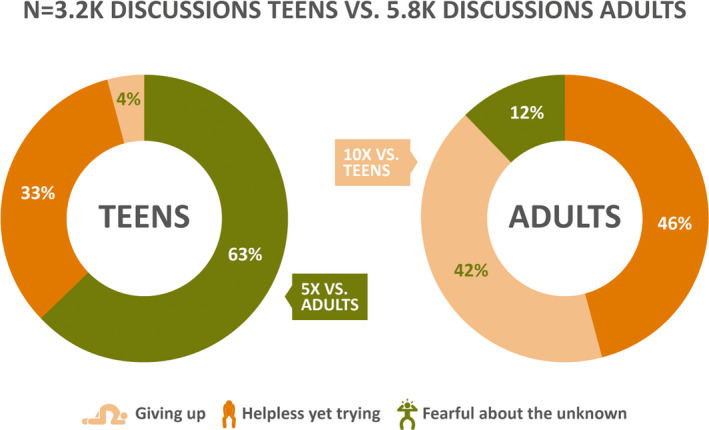
Mindset analysis behind online conversations among teenagers and adults
3.5. “How” (sentiment analysis of conversation “drivers”)
The primary sentiment (“driver”) of each conversation was divided into the positive, negative, and neutral categories. The distribution of drivers for conversations by teenagers and adults is shown in Figure 3. The negative drivers of conversations were classified as barriers and divided into four subcategories: feeling alone, social embarrassment, low spirit, and sense of loss. The positive drivers were divided into three subcategories: Encouragement via connection, empowerment over the condition, and adaptation to the condition. Finally, the neutral drivers were divided into three subcategories: Emotional connection, support, and information and resources. The distribution of various conversations based on the analysis of their driver is shown in Table 1.
FIGURE 3.
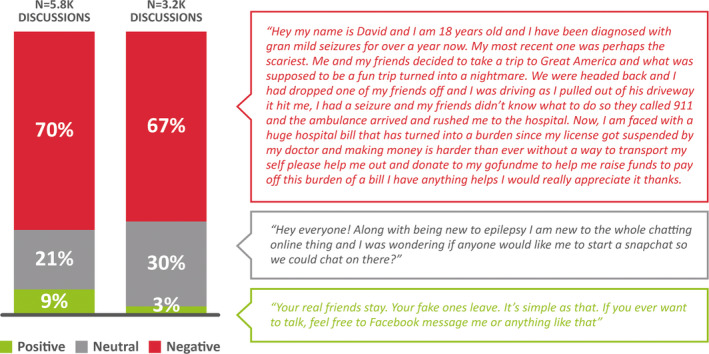
Distribution of various drivers of conversation in teenagers and adults
4. DISCUSSION
This is the first of its kind study using big data to analyze online digital conversations about epilepsy and suicide using machine learning techniques. After analyzing close to a quarter‐million online conversations, we found that a small percentage of people with epilepsy engage in digital conversation about suicide. However, the comparison of teenagers to adults with epilepsy reveals that a disproportionately larger number of the former (7.8%) engage in online conversations about suicide compared to their adult counterparts (3.2%). This may be due to several factors including a larger proportion of teenagers feeling alone, given that 32% of their 2100 negatively driven conversations express such sentiment. Teenagers’ comfort with the internet and technology could also make them more likely to discuss their personal concerns, including suicidality, online. A recent Pew Center study among teenagers showed that 95% of them had access to smartphones and 45% said that they are online “almost constantly.” 15 But this trend is not limited to teenagers, and the online access and use of the internet is increasing rapidly in adults and even in the elderly population. 16 Therefore, digital and social media presents a potential opportunity for early engagement and intervention among teenagers and adults with suicidality. It has been found that around 72% of the internet users say they looked online for health information within the past year. 17 Developing relevant content with hashtags (#) and search engine optimization strategies will help PWE find the information that they seek online.
Of interest, more than three of four conversations about suicide by teenagers with epilepsy occurs on message boards and topical sites rather than social media (Figure 1). The higher likelihood of knowledgeable support and the anonymity provided by these websites is in contrast to the possible risk to their social well‐being posed by discussing their mental and physical condition among peers and friends on social media. This is reflected in the significantly larger number of conversations by teenagers compared to adults that discuss the social impact of epilepsy (30% vs 21%, respectively). Teens consider that seizures affect their relationships and social life as they miss out on events and experiences. This is also supported by the fact that one of the major negative sentiments (drivers) in the online conversation of teenagers was social embarrassment (28% of 2100 negative conversations). It may be because of epilepsy misconceptions and stigmatization among teenagers. 18 , 19 Although we did not perform subanalysis of the digital conversations based on their source—topical sites and message boards vs social media (eg, Facebook), one may speculate that the choice of engaging in a particular form of online medium may inform as well as be influenced by an individual's health literacy. It is likely that individuals conversing on topical sites have higher health literacy than their counterparts who engage on social media, and therefore, the scenario of suicidality may be much worse in the latter group.
A recent analysis of data from Centers for Disease Control and Prevention (CDC) showed that the suicide rates among teenagers 15 to 19 years of age increased to its highest levels in 2017 since the year 2000. 20 The incidence of suicidality is known to be higher in teenagers compared to the general population. However, not much is known about suicide risk in teenagers with epilepsy compared to their peers in the general population. A recent study from Taiwan compared suicide attempts in children with epilepsy who were younger than 18 years to age‐ and gender‐matched controls (1:4 matching) from general populations in Taiwan. 21 The teenagers older than 12 years, especially male teenagers, were at increased risk of suicide attempt. The overall risk was 2.34 (95% CI 2.17‐2.52) times higher in children with epilepsy compared to the matched general population. 21 This suggests that the problem of suicidality may be even more grave for teenagers with epilepsy compared to their healthy peers. A common yearning among teenagers to be able to just live a “normal life” was noted in the analysis. A prior international survey exploring the impact of epilepsy on teenagers has shown that more than one‐third of them expect it to affect their future lives. 18 A considerably smaller percentage of adults consider that epilepsy impacts their social life, likely due to a longer duration of epilepsy and hence, better life adjustment. Almost one‐third (29%) of the conversations among teenagers are centered around the topic of finding emotional encouragement and support. They are interested in finding their peers who have a similar shared experience and create a space for emotional bonding. Such basic emotional needs probably explain the availability and thriving of internet sites like www.patientslikeme.com, which encourage sharing experience with a disease condition online. A systematic review analyzing the utility of social media in suicide prevention found that it can be used to reach “hard‐to‐engage: individuals, and may provide avenues for timely intervention while allowing a forum for nonjudgmental experience sharing. 22 A study analyzing the social media behavior of adolescents found that the time spent on it was significantly higher among depressed compared to nondepressed adolescents. 23 The finding that teenagers and young adults are more likely to share their suicide risk factors on social media sites than with their doctors 24 highlight the importance of availability of such online venues and the need for harnessing this readily available individualized information to prevent tragedies like suicide. In fact, the analysis of social media content of military personnel who died by suicide compared to deaths from other causes showed that it could not only predict the cause of death but also the timing of suicide. 25
Previous studies have analyzed the use of social media for epilepsy. 26 One study showed that the number of online users interested in epilepsy is likely the highest among all neurologic conditions. 14 It also found that the most common content on social media on the topic relates to providing more information and resolving misconceptions about epilepsy. 14 Such information should be very useful to teenagers because the analysis of the mindset behind epilepsy and suicide‐related online conversations suggest that a large majority (63%) of teenagers are bothered by not knowing what to expect from their condition and live in fear of the “unknown.” This is a stark difference from adults, as only 12% of them are fearful of the “unknown,” likely due to their longer life experience.
A great window of opportunity for supportive and therapeutic intervention among teenagers is provided by the fact that only 4% of 3200 conversations among teenagers reflected a mindset suggestive of having given up. Therefore, social media–based outreach programs may have a substantial impact on suicide prevention in a teenage population that is motivated to improve their well‐being. Unfortunately, a very large proportion of adults (42%) had a negative, defeatist attitude in the face of epilepsy. It may be because of a longer period of disease and comorbidity, highly prevalent depression association with epilepsy. 27 This is a really worrisome finding in adults as it may be postulated that such a dispirited outlook may be harbinger for attempted suicide. Our study was not designed to analyze the real‐life consequences of these digital conversation. However, future studies are required to understand triggers that lead to conversion of conversation and thoughts into grievous actions like suicide attempt.
Although the incidence of suicidal ideation in PWE in clinical studies has been reported to be around 12%, 7 we found only 4% of total conversations online by PWE, including teenagers, to be about suicide. These are two very different metrics; however, it is possible that our study may underestimate the burden of suicidality among adults and teenagers with epilepsy. This is primarily due to the limitation related to how these conversations were gathered: from self‐identified individuals discussing epilepsy online. It is also important to note that only the publicly accessible online conversations were mined; the ones protected behind firewalls, depending on individual social media profile settings, could not be included in the analysis. In addition, not all teenagers and adults use social media. Therefore, it is likely that the data analyzed is a portion of the entire digital conversations among PWE about suicide. Another limitation is the lack of data individual socioeconomic and cultural background, which may influence their access to the internet and comfort with expressing suicidal thoughts online. On similar lines, we were not able to gather data on the gender of the individual engaging in digital conversations or their seizure status, which may also influence their potential for suicidal ideation. Our findings are applicable to the US population only, given that only the conversations originating from IP addresses in the United States were used in the study.
A larger philosophical question, which cannot be addressed by our study but may be relevant, is the correlation between the digital representation of an individual and their “true” self. Although it may be argued that an individual may feel freer to express their true feelings and sentiments online, the contrary possibility that the digital portrayal is only a portion of the totality of an individual's actual personality or emotions could be an equally valid point.
In conclusion, our big data study analyzing the online conversations among PWE finds a small but significant percentage of them discussing epilepsy and suicide. A substantially higher percentage of teenagers indulge in such conversations, which reveals their increased vulnerability compared to adults with epilepsy. The various topics, mindsets, and concerns regarding suicidality among PWE and their differences among teenagers and adults revealed by our study provide us an opportunity for devising more effective, early interventions.
Future studies validating our findings in clearly identified and characterized PWE are required to improve the mental well‐being of our patients.
CONFLICT OF INTEREST
Dr Falcone and Dr Timmons‐Mitchell receive federal funds from Health Resources Services Administration's Maternal and Child Health Bureau Project IMPACTT (Grant H98MC20269). Dr Ruby Castilla‐Puentes is working full‐time for Janssen, Pharmaceuticals. The content of this article is solely the responsibility of Dr. Castilla‐Puentes and the authors, and does not necessarily represent the official views of Janssen, Pharmaceuticals. The other authors report no biomedical financial interests or potential conflicts of interest. We confirm that we have read the Journal's position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Falcone T, Dagar A, Castilla-Puentes RC, et al. Digital conversations about suicide among teenagers and adults with epilepsy: A big‐data, machine learning analysis. Epilepsia. 2020;61:951–958. 10.1111/epi.16507
Tatiana Falcone and Anjali Dagar contributed equally to this work.
FUNDING INFORMATION
Supported by the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS) (Grant H98MC26260).
REFERENCES
- 1. World Health Organization . Atlas: Epilepsy Care in the World. Geneva, Switzerland: WHO; 2015. http://www.who.int/mental_health/neurology/Epilepsy_atlas_r1.pdf [Google Scholar]
- 2. Devinsky O, Spruill T, Thurman D, Friedman D. Recognizing and preventing epilepsy‐related mortality: a call for action. Neurology. 2016;86:779–86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Tian N, Cui W, Zack M, Kobau R, Fowler KA, Hesdorffer DC. Suicide among people with epilepsy: a population‐based analysis of data from the U.S. National Violent Death Reporting System, 17 states, 2003–2011. Epilepsy Behav. 2016;61:210–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Jones JE, Siddarth P, Gurbani S, Shields WD. Caplan R Screening for suicidal ideation in children with epilepsy. Epilepsy Behav. 2013;29:521–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Pompili M, Girardi P, Tatarelli R. Death from suicide versus mortality from epilepsy in the epilepsies: a meta‐analysis. Epilepsy Behav. 2006;9:641–8. [DOI] [PubMed] [Google Scholar]
- 6. Hecimovic H, Santos JM, Carter J, Attarian HP, Fessler AJ, Vahle V, et al. Depression but not seizure factors or quality of life predicts suicidality in epilepsy. Epilepsy Behav. 2012;24:426–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Jones JE, Hermann BP, Barry JJ, Gilliam FG, Kanner AM, Meador KJ. Rates and risk factors for suicide, suicidal ideation, and suicide attempts in chronic epilepsy. Epilepsy Behav. 2003;4:31–8. [DOI] [PubMed] [Google Scholar]
- 8. Reilly C, Atkinson P, Chin RF, Das KB, Gillberg C, Aylett SE, et al. Symptoms of anxiety and depression in school‐aged children with active epilepsy: a population‐based study. Epilepsy Behav. 2015;52:174–9. [DOI] [PubMed] [Google Scholar]
- 9. Christensen J, Vestergaard M, Mortensen PB, Sidenius P, Agerbo E. Epilepsy and risk of suicide: a population‐based case–control study. Lancet Neurol. 2007;6:693–8. [DOI] [PubMed] [Google Scholar]
- 10. Casañas i Comabella C, Wanat M. Using social media in supportive and palliative care research. BMJ Support Palliat Care. 2015;5:138–45. [DOI] [PubMed] [Google Scholar]
- 11. Hopewell‐Kelly N, Baillie J, Sivell S, Harrop E, Bowyer A, Taylor S, et al. Palliative care research centre's move into social media: constructing a framework for ethical research, a consensus paper. BMJ Support Palliat Care. 2019;9:219–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Gustafson DL, Woodworth CF. Methodological and ethical issues in research using social media: a metamethod of Human Papillomavirus vaccine studies. BMC Med Res Methodol. 2014;14:127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Moorhead SA, Hazlett DE, Harrison L, Carroll JK, Irwin A, Hoving C. A new dimension of health care: systematic review of the uses, benefits, and limitations of social media for health communication. J Med Internet Res. 2013;15:e85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Meng Y, Elkaim L, Wang J, Liu J, Alotaibi NM, Ibrahim GM, et al. Social media in epilepsy: a quantitative and qualitative analysis. Epilepsy Behav. 2017;71(Pt A):79–84. [DOI] [PubMed] [Google Scholar]
- 15. PewResearchCenter . Teens, Social Media & Technology; 2018. http://www.pewinternet.org/2018/05/31/teens‐social‐media‐technology‐2018/ Accessed 09/25/2019
- 16. PewResearchCenter . Tech adoption climbs among older adults. http://www.pewinternet.org/2017/05/17/tech‐adoption‐climbs‐among‐older‐adults/. Accessed 09/25/2019.
- 17. Health Fact Sheet , n.d. http://www.pewinternet.org/fact‐sheets/health‐fact‐sheet/. Accessed 09/29/2019.
- 18. Baker GA, Hargis E, Hsih M‐S, Mounfield H, Arzimanoglou A, Glauser T, et al. Perceived impact of epilepsy in teenagers and young adults: an international survey. Epilepsy Behav. 2008;12:395–401. [DOI] [PubMed] [Google Scholar]
- 19. Herrmann LK, Welter E, Berg AT, Perzynski AT, Van Doren JR, Sajatovic M. Epilepsy misconceptions and stigma reduction: current status in Western countries. Epilepsy Behav. 2016;60:165–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Miron O, Yu KH, Wilf‐Miron R, Kohane IS. Suicide rates among adolescents and young adults in the United States, 2000–2017. JAMA. 2019;321:2362–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Harnod T, Lin CL, Kao CH. Prevalence of suicide attempts and their risk factors in school‐aged patients with epilepsy: a population‐based study. Eur Child Adolesc Psychiatry. 2018;27:1047–53. [DOI] [PubMed] [Google Scholar]
- 22. Robinson JO, Cox G, Bailey E, Hetrick S, Rodrigues M, Fisher S, et al. Social media and suicide prevention: a systematic review. Early Interv Psychiatry. 2016;10:103–21. [DOI] [PubMed] [Google Scholar]
- 23. Gürbüz HGA, Demir T, Özcan BG, Kadak MT, Poyraz BC. Use of social network sites among depressed adolescents. Behav Inform Technol. 2017;36:517–23. [Google Scholar]
- 24. Pourmand A, Roberson J, Caggiula A, Monsalve N, Rahimi M, Torres‐Llenza V, et al. Social media and suicide: a review of technology‐based epidemiology and risk assessment. Telemed J E Health. 2019;25:880–8. [DOI] [PubMed] [Google Scholar]
- 25. Bryan CJ, Butner JE, Sinclair S, Bryan ABO, Hesse CM, Rose AE, et al. Predictors of emerging suicide death among military personnel on social media networks. Suicide Life Threat Behav. 2018;48:413–30. [DOI] [PubMed] [Google Scholar]
- 26. McNeil K, Brna PM, Gordon KE. Epilepsy in the Twitter era: a need to re‐tweet the way we think about seizures. Epilepsy Behav. 2012;23:127–30. [DOI] [PubMed] [Google Scholar]
- 27. Josephson CB, Jetté N. Psychiatric comorbidities in epilepsy. Int Rev Psychiatry. 2017;29:409–24. [DOI] [PubMed] [Google Scholar]