

Abstract
Background
The researches investigating the influence factors of epidemic prevention are not only scarce, but also provide a gap in the domain of perception-based influence factors of intention to adopt COVID-19 epidemic prevention.
Objective
This work has attempted to examine the perception-based influence factors of individuals’ intention to adopt COVID-19 epidemic prevention in a modified behavioral framework.
Theoretical framework
A behavioral framework composed of the theory of reasoned action and the theory of planned behavior is developed to incorporate some additional perception-based influence factors.
Methods
A partial least square-based path analysis has been employed to estimate the path coefficients of those factors in terms of drivers, barriers, and neutral factors based on questionnaire data of 302 respondents from six universities and two hospitals in China.
Results
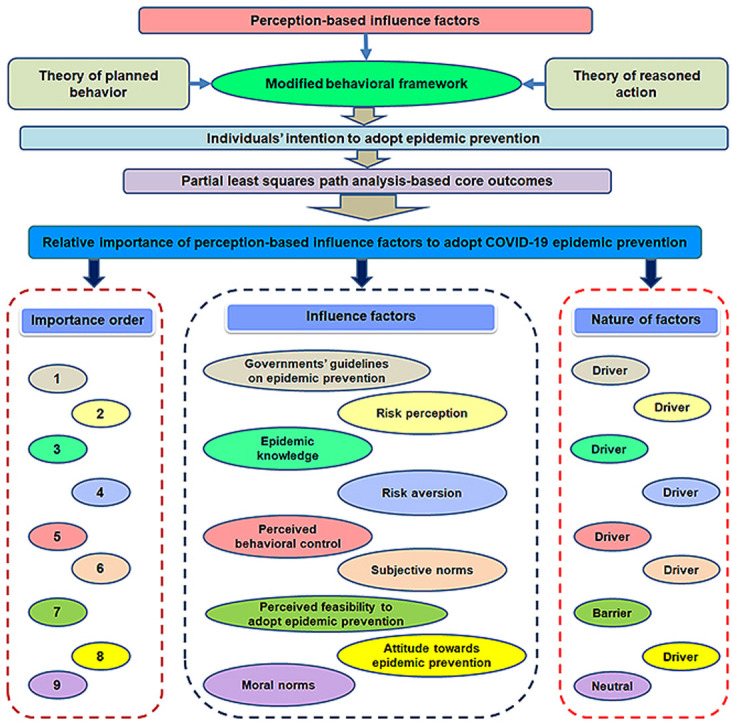
Among the perception-based influence factors, governments' guidelines on epidemic prevention is found to be the most important and influential factor, which was followed by risk perception. Finally, attitude towards epidemic prevention exhibited the least degree of impact on individuals' intention to adopt epidemic prevention. Moral norms did not show any contribution to individuals’ intention to adopt epidemic prevention.
Conclusion
Concerning importance ranking, the governments' guidelines on epidemic prevention, risk perception, and epidemic knowledge are revealed as the top three drivers of individuals' intention to adopt epidemic prevention, while the perceived feasibility to adopt epidemic prevention is found to be a barrier. Moreover, moral norms is identified to have an insignificant influence on individuals' intention to adopt epidemic prevention. Given the empirical results, dissemination of Governments’ guidelines on epidemic prevention, proper risk perception, and knowledge about epidemic would help prevent the COVID-19 pandemic outbreak within China and worldwide.
Keywords: Modified behavioral framework, Risk perception, Epidemic knowledge, Risk aversion, Governments' guidelines on epidemic prevention
Graphical abstract
Highlights
-
•
Examined perception-based influence factors of individuals' intention to adopt epidemic prevention.
-
•
Theory of planned behavior and theory of reasoned actions are modified to introduced new factors.
-
•
Governments' guidelines on epidemic prevention, risk perception, and epidemic knowledge are the top three drivers.
-
•
Perceived feasibility is revealed a barrier to adopt COVID-19 epidemic prevention.
-
•
Moral norms showed an insignificant role in adoption of COVID-19 epidemic prevention.
Nomenclature
Acronyms
- PIFs
Perception-based influence factors
- IAEP
Intention to adopt epidemic prevention
- ToRA
Theory of reasoned action
- ToPB
Theory of planned behavior
Abbreviations
- COVID-19
Coronavirus disease 2019
- SARS-CoV
Severe Acute Respiratory Syndrome Coronavirus
- MERS-CoV
The Middle East Respiratory Syndrome Coronavirus
Methods
- PLS
Partial least square
- CMPR
Composite reliability
- AVE
Average variance extracted
- LTV
Latent variable
- R2
Explained variation
- Q2
Predictive relevance
- f2
Impact size
1. Introduction
Since the global epidemics are increasing day by day due to a lack of the prevention and control of such epidemics, therefore the involvement of all stakeholders, including vaccine companies, medical health officers, governments, and the public is essential (Yang et al., 2020). Recently, an outbreak of Coronavirus Disease 2019 (COVID-19) started in late December 2019 in the Wuhan city of China and gradually became a global pandemic. The Chinese government adopted stringent actions for the containment of the outbreak and remained successful (Wu et al., 2020). As of 21st May 2020, an estimated 4.95 million laboratory-confirmed cases are reported, while about 3.25 million people have lost their lives due to COVID-19 infection around the globe. In contrast, the past outbreaks of “Severe Acute Respiratory Syndrome Coronavirus” (SARS-CoV) infected 8098 people and claimed 774 lives, while “The Middle East Respiratory Syndrome Coronavirus” (MERS-CoV) infected 2494 people and took lives of 858 people worldwide (WHO, 2020). Though all the three viruses belonged to the coronavirus family, COVID-19 is a novel coronavirus that is both highly contagious and extremely fatal (WHO, 2020).
Given the transmission of COVID-19 is highly efficient due to its contagion characteristic (Yang et al., 2020), the mitigation of the outbreak may involve social distancing, home quarantine, isolation testing of suspected cases, and treatment of the patients, among others (WHO, 2020). Though the identification and treatment of infected cases are of utmost importance for the containment of the outbreak, however, the social distancing and home quarantine also play a crucial role. The COVID-19 epidemic outbreak and the resulting economic shutdowns have brought chaos to all the sectors of the world economies—namely, the primary sectors that involve the extraction of raw materials, the secondary sectors that produce the finished commodities, and the tertiary sectors which provide services (Nicola et al., 2020). Despite these economic repercussions, as per the mode of transmission of the epidemic, its human to human spread may only be contained through the adoption of epidemic prevention. Therefore, there is a clear scope of identifying perception-based influence factors (PIFs) of individuals’ intention to adopt epidemic prevention (IAEP) during the outbreak of the COVID-19 epidemic.
To begin with, the previous studies fundamentally focussed on the prevention and control of diseases such as Malaria, AIDS,1 West Nile, Dengue, Zika, and Chikungunya (Cui et al., 2019; Omodior et al., 2018; Przybyla et al., 2019; Raude et al., 2019; Xiaoliang et al., 2016). The first group of researches focussed on the epidemiology of diseases like Malaria, Dengue, and AIDS (Bryant-davis et al., 2016; Cui et al., 2019). The second group of researches was based on surveys and their interpretation through the response rate of certain variables on epidemic prevention (Baghbanzadeh et al., 2020; Sued et al., 2016). The third group of the studies was based on the situation analysis of the disease profiles in terms of explaining their prevention and control measures (Elmahdawy et al., 2017; Kiviniemi et al., 2018; Raude et al., 2019). Finally, the fourth group of studies focussed the epidemics like SARS-CoV of 2002, MERS-CoV of 2012, and COVID-19 (Lai et al., 2020; Nishiura et al., 2020; You et al., 2020). Despite the long-standing interest of the previous researches, the tendency to investigate the individual level intention to prevent the epidemics has been largely overlooked. Furthermore, the drivers and barriers of the individuals’ IAEP in a modified behavioral framework have not been considered previously.
This research attempts to investigate the PIFs of individuals' IAEP in terms of both drivers as well as barriers in China. This work extends two-fold contributions to the existing pool of knowledge. First, a behavioral framework composed of the theory of reasoned action (ToRA) and the theory of planned behavior (ToPB) is modified to incorporate additional PIFs determining the individuals' IAEP. Those factors include risk perception, epidemic knowledge, perceived feasibility to adopt epidemic prevention, risk aversion, moral norms, and governments’ guidelines on epidemic prevention. Second, to carry out analysis, the survey-based data collection has been done for six universities and two hospitals in China. The data based on 302 respondents are examined using a partial least square (PLS)-based path analysis.
To sum up, first, governments' guidelines on epidemic prevention, risk perception, epidemic knowledge, risk aversion, perceived behavioral control, subjective norms, and attitude towards epidemic prevention are suspected to be the drivers of individuals' IAEP. Secondly, the perceived feasibility to adopt epidemic prevention may be a barrier to individuals' IAEP. Lastly, the moral norms played a neutral role in shaping individuals’ IAEP.
The rest of the research is structured as follows: Section 2 is based on a modified behavioral framework. Section 3 documents the materials and methods. Section 4 describes the results. Section 5 is based on the discussion. Finally, section 6 concludes this work.
2. A modified behavioral framework
The fundamentals of the ToRA stated that individuals' behavior is in accordance with their intention (Fishbein and Ajzen, 1975). It substantiated that individuals ponder over the perceived consequence of behaviors instead of performing immediate actual behavior. In this way, individuals choose to perform actual behaviors that they think would lead to desired results. Based on this, the intention-based behavior to adopt epidemic prevention depends on subjective norms and attitudes towards epidemic prevention (Ajzen, 1991). Besides, subjective norms may be considered as a set of perceptions of the ways other people judge the individuals’ behavior and their motive to deal with intention-based behavior (Ajzen and Fishbein, 1970).
Later on, Ajzen (1985) introduced an extended version of ToRA by incorporating a vital component of perceived behavioral control and called it ToPB (as can be seen in Fig. 1 ). According to Ajzen (1991), the perceived behavioral control is described as the control which individuals perceived to own in order to perform any behavior. The ToRA and ToPB are widely used in behavioral sciences to describe diversified intention-based behavioral scenarios (Elyasi et al., 2020; Msn and Kang, 2020). This work has advanced the behavioral framework of ToRA and ToPB through integrating some additional PIFs of individuals’ IAEP (see Fig. 1).
Fig. 1.

A modified behavioral framework depicting the influence factors of individuals' intention to adopt epidemic prevention.
3. Materials and methods
3.1. Study site
The data are compiled from academic as well as technical channels to examine the proposed hypotheses. In this respect, an online questionnaire survey was undertaken from a scholarly channel, which involved 6 Chinese universities. Among those universities, Guangdong Medical University is located in the seaport city of Zhanjiang, and Southern Medical University is located in Guangzhou city of Guangdong province. Next, Xinxiang Medical University is located in Xinxiang city of Henan province, Zhejiang University is located in Hangzhou city, and North China Electric Power University and Peking University are located in the capital city of Beijing. (see Fig. 2 )
Fig. 2.

Study site.
Further, the survey was also administered at a technical platform, including Tianjin First Central Hospital located in Tianjin city, and Shanghai United Family Hospital in Shanghai city, which is located near to the first epicenter of the epidemic outbreak called Wuhan city of Hubei province. The fundamental rationale to include two universities of Beijing as a study location was that the persons to be surveyed in the capital city contained heterogeneous communities belonging to diverse provinces of China. Moreover, other locations were opted, first, based on their proximity to the province of Hubei being the epicenter of the COVID-19 outbreak. Secondly, those locations were selected based on the feasibility of the conduction of the survey.
3.2. Study participants
A questionnaire was planned and sent for evaluation and pre-testing to professors of Psychology and Medicine, and researchers for their expert opinions. Those professors and researchers belonged to various universities. In this regard, the profiles of the participants are provided in Table 1 . Moreover, expert medical technicians from two hospitals also commented on the planned questionnaire. Finally, a few health advisors from the Chinese Centre for Disease Control and Prevention located in Beijing were contacted to comment on the structured questionnaire for further refinement. All of the conversations with those experts were regulated through emails (see Table 1).
Table 1.
Profiles of experts involved in the evaluation and pre-testing of the questionnaire.
| No. | Participant | Institute/Organization | Working experience (years) | Interview mode |
|---|---|---|---|---|
| 1 | Professors (Psychology, Medicine) | SNU, PU, SPU | 15–25 | |
| 2 | Researchers | NMU, XMU, ZJU | 5–10 | |
| 3 | Medical technicians | TFCH, SUFH | 5–8 | |
| 4 | Health advisors | CDC | 15–10 |
Notes: SNU: Shaanxi Normal University, PU: Peking University, SPU: Shenyang Pharmaceutical University, NMU: Nanjing Medical University, XMU: Xuzhou Medical College, ZJU: Zhejiang University, TFCH: Tianjin First Central Hospital, SUFH: Shanghai United Family Hospital, CDC: Chinese Center for Disease Control and Prevention.
3.3. Questionnaire administration
A bilingual questionnaire involving both English and Chinese versions was floated to eliminate the language barrier and to obtain unbiased responses. The survey was conducted through a Chinese multipurpose cell phone application called “WeChat” in Chinese “微信 (weixin).” To this end, the questionnaire was floated in different WeChat-based groups of students, instructors, and researchers belonging to 6 Chinese universities. Additionally, the questionnaires were also circulated in the WeChat-based group of medical practitioners from the two Chinese hospitals. On the whole, 324 respondents completed the questionnaire survey. After examination, 302 questionnaires were confirmed valid for analysis purposes.
Besides, the Harman single-factor diagnostic test was made use of to deal with the problem of common-method-bias to verify the presence of the possible bias from collected evidence. Although the data was obtained from respondents responding based on their previous activities correlated with their internal environments, this may influence the empirical performance. Thus, variation in the method may extend the spotted associations between predicted and observed variables (Lindell and Whitney, 2001). This method is one of the most common and easiest methods in this regard, using the likelihood of particular device variance (Podsakoff et al., 2003). The check confirmed the absence of any possible inclination in the findings.
3.4. Data analysis
Table 2 shows the demographic features of the respondents. Concerning the sex of the respondents, the proportion of males (59.93%) was greater than females (40.07%). A key share of respondents (44.04%) consisted of a young category (below 30 years), whereas the second major age category (37.09%) was middle-age (30–50 years). The respondents had the qualification ranging from Master to Postdoctoral. The major share of respondents (38.74%) had no working experience, while the second-prime share of them (30.13%) had up to 10 years of working experience. On the contrary, a very small proportion of respondents (8.28%) had working experience of more than 20 years. The major proportion of them (40.73%) was Master, whereas the PhDs (39.07%) were next to it. Students constituted the major proportion of the respondents (43.38%), while instructors constituted the second-major proportion of respondents (23.84%).
Table 2.
Demographic features of respondents.
| Respondents' demography | Frequencies | Percentage |
|---|---|---|
| Sex | ||
| Male | 181 | 59.93 |
| Female | 121 | 40.07 |
| Age categories (years) | ||
| Young (below 30) | 133 | 44.04 |
| Middle-age (30–50) | 112 | 37.09 |
| Old-age (above 50) | 57 | 18.87 |
| Qualification | ||
| Master | 123 | 40.73 |
| PhD | 118 | 39.07 |
| Postdoctoral | 61 | 20.20 |
| Working experience (years) | ||
| 0 | 117 | 38.74 |
| Less than 10 | 91 | 30.13 |
| 10 to 20 | 69 | 22.85 |
| More than 20 | 25 | 8.28 |
| Occupation | ||
| Student | 131 | 43.38 |
| Instructor | 72 | 23.84 |
| Medical practitioner | 48 | 15.89 |
| Researcher | 51 | 16.89 |
3.5. Statistical analyses
The factors influencing the individuals’ IAEP explored by making use of content analysis are empirically analyzed through the PLS-based path modeling technique. A five-point Likert scale is employed, which involved “5 = strong agreement,” “4 = agreement,” “3 = neutral,” “2 = disagreement,” and “1 = strong disagreement.” In order to estimate the measurement and structural models, the statistical package called STATA 13 is employed.
In order to estimate the influence factors of individuals’ IAEP, this work has employed partial least square (PLS) based path analysis. To this end, for the assessment of whether the constructs are reliable as well as valid, confirmatory factor analysis is performed. In this connection, at the outset, the evaluation of outer loadings is done in Table A1 (see Appendix A). In this context, it has been argued that outer loading of equal to or more than 0.7 denotes approximately more than 50 percent of the explained variance (Hair et al., 2014). It implicates that the measured factor accomplished an admissible extent of reliability. As a consequence, the values of outer loadings exceeding 0.7 indicate the retention of the loading (Hair et al., 2016).
Bortoleto et al. (2012) suggested that the internal consistency of a construct determines its reliability. For appraisal purposes of reliability, ρ-A, Cronbach-α, and composite reliability (CMPR) are employed. The values between 0.7 and 0.95 are considered within an acceptable degree of reliability (Elmustapha et al., 2018). The Cronbach-α explains the reliability of the opted scales that how precisely they measure the latent construct. However, the range of its values (usually 7.0 to 9.0) does not implicate the degree of strength of reliability; it rather tells that beyond that range of values, the opted scales are not reliable.
Bearing in mind the possibility that Cronbach-α is a customary measure and thus may have the possibility to underplay the reliability in case of a relatively small sample, there comes suggestion to consider the additional measure of CMPR (Hair et al., 2016). The CMPR can be explained as the variance of the total true score relative to the variance of the total scale score (Netemeyer et al., 2003). Like Cronbach-α, the CMPR is also a measure of scale reliability, and it has a threshold level value to indicate whether the opted scales of a construct are reliable. Though its threshold value is reported as 0.7 by Hair et al. (2013) and 0.6 by Bagozzi and Heartherton (1994), the number of items taken for a construct is important for deciding whether the construct is internally reliable (Netemeyer et al., 2003). It has been further envisaged that the value of ρ-A between CMPR and Cronbach-α is suggested reliable (Lopes et al., 2019), which implies that the selected items are considered reliable for the value of ρ-A within the stated range.
4. Results
Following the recommended criteria by Hair et al. (2013), the estimated value of average variance extracted (AVE) is recorded to exceed the cut off value of 0.5 and hence to hold the constructs reliable. It shows that the included research questions provide a good representation of a particular LTV. Keeping this in view, the estimations have supplied with statistical results translating the convergent validity and reliability to declare the measurement model to be appropriate. The AVE is recorded in Table A1 (Appendix A). Conclusively, considering the valid discriminant validity, Hair et al. (2014) postulated that the square root of AVE should be above the measure of inter-constructs association. Then it may be employed to manipulate the discriminant validity value. Each of the calculated association values among the LTVs is noted to be below the square roots of AVE, which proved the existence of the discriminant validity. It means the difference between each of the LTVs is stronger (Hair et al., 2016). These findings are documented in Table A2 (Appendix A).
Following the critical benchmarks of the t-statistic and probability score, the path coefficients for all the PIFs are found relevant, except for moral norms (see Table 3 ). This is because the t-statistic are documented to be more than or were equal to the threshold level of 1.96, and the probability score is below or equal to 0.05. It means that, except moral norms, all of the PIFs significantly contribute to individuals' IAEP. In the structural model, given the estimated path coefficients' magnitudes, the relative importance of the PIFs of individuals' IAEP is depicted in Fig. 3 . Considering the relative importance of the PIFs, governments' guidelines on epidemic prevention, risk perception, and epidemic knowledge are exposed to be the top three PIFs having path coefficient values of 0.574, 0.458, and 0.401, accordingly. On the other hand, attitude towards epidemic prevention remained the least contributor (0.205), while moral norms revealed no contribution to individuals’ IAEP.
Table 3.
Results of path analysis and post-analysis model criteria.
| Hypothesis | Hypothesized path | PC | t-ratio | Decision | Driver/Barrier | VIF | f2 | R2 | Q2 |
|---|---|---|---|---|---|---|---|---|---|
| H1 | RP → IAEP | 0.458a | 2.69 | Supported | Driver | 1.625 | 0.316 | 0.713 | 0.446 |
| H2 | EPK → IAEP | 0.401a | 2.83 | Supported | Driver | 1.283 | 0.277 | ||
| H3 | ATEP → IAEP | 0.205a | 2.15 | Supported | Driver | 3.081 | 0.141 | ||
| H4 | PFEP → IAEP | −0.291a | 2.42 | Supported | Barrier | 2.156 | 0.201 | ||
| H5 | PBC → IAEP | 0.343a | 3.10 | Supported | Driver | 3.459 | 0.237 | ||
| H6 | SBN → IAEP | 0.321a | 2.95 | Supported | Driver | 1.923 | 0.221 | ||
| H7 | MNS → IAEP | 0.102 | 1.16 | Not supported | Neutral | 2.384 | 0.070 | ||
| H8 | RA → IAEP | 0.367a | 3.11 | Supported | Driver | 2.779 | 0.253 | ||
| H9 | GGEP → IAEP | 0.574a | 2.78 | Supported | Driver | 4.142 | 0.396 |
Notes: PC: path coefficient
p < 0.05.
Fig. 3.

The relative importance of perception-based factors influencing the individuals' intention to adopt epidemic prevention.
Taking the nature of the PIFs of individuals' IAEP into consideration, the perceived feasibility to adopt epidemic prevention is revealed as the only barrier to individuals' IAEP. Whereas the remaining PIFs are exposed as the drivers of individuals' IAEP, while the moral norms is exposed to be the neutral factor. Among the drivers of individuals' IAEP, governments’ guidelines on epidemic prevention is unveiled to be the strongest driver (see Fig. 3).
5. Discussion
5.1. Comprehensive guidelines by governments
The governments' guidelines are revealed to be a driving force to motivate the individuals' intention to adopt epidemic prevention in China. These guidelines are perceived to be simple, positive, enriched with a motivational appeal, and rational. This finding implicates that in times of epidemic outbreaks, particularly global pandemics, the governments and state administrations of countries practicing the totalitarian system, such as China, should step up to put forward comprehensive guidelines on epidemic prevention. This is also important because the situation of every country or state may vary. Therefore, situation-specific guidelines would be targeted and useful. Concerning the role of government, Swinburn et al. (2013) conducted research proposing a monitoring framework based on governments' evaluations and measures adopted to enforce health environment conditions. They concluded that steps taken by the governments accelerated the reduction in obesity and non-communicable diseases. Regarding risks of avian influenza, Cui et al. (2019b) recommended that the governments should build a communication system to convey the guidelines to the poultry farmers on avian influence epidemic protection. The need for the role of strategic leadership is emphasized by Carrel (2005) in Switzerland concerning the future epidemic outbreaks. Another most recent research showed a significant mediating role of government on epidemic prevention (Yasir et al., 2020). In this way, governments’ role would be central in shaping the behaviors of individuals for adopting epidemic prevention.
5.2. Level of risk perception
Risk perception is found to have a positive contribution to shaping individuals' intention to adopt epidemic prevention. It implicates that if people perceive the severity, susceptibility, and fatality of the infection, then it will enhance their intention to adopt epidemic prevention. In brief, better the risk of infection is perceived; quicker it would be to shape individual intentions to accept protection measures. In their research, Raude et al. (2019) examined the changes in health behavior in times of infectious disease outbreaks in French Guiana. They found the positive impact of perceived risk on epidemic prevention. However, this impact reduced over time. Furthermore, Valeeva et al. (2011) studied the risk perception behaviors of Dutch farmers towards the health risk of the animals. They found that risk management is possible only if the risk is properly assessed and perceived. Additionally, Cui et al. (2019a) measured the association between farmers’ perceived risk and the utilization of biosecurity measures in Anhui and Jiangsu provinces of China. They revealed that the adoption of biosecurity measures during highly pathogenic avian influenza was related to the risk perception of the farmers. Those researches, among others, confirmed the role of risk perception in shaping the adoption behaviors during the epidemic outbreaks, which may equally apply for the case of the present outbreak of COVID-19 pandemic.
5.3. Essential knowledge of the epidemic
Epidemic knowledge is found to drive individuals’ intention to adopt epidemic prevention. It entails that without knowing about some infection, it is unrealistic to have its precautions. In this regard, the knowledge of how an infection can be transmitted, and to which degree it is contagious is likely to be proved the fundamental breakthroughs to motivate the individuals to prevent that infection. For instance, in the case of COVID-19 global pandemic, hand washing, and social distancing are the key rules to break the transmission chain of infection. Considering the epidemic knowledge, Delpont et al. (2020) studied the influence factors of biosecurity measures in French duck farms in South West France. For this, they considered the influence of epidemic knowledge and attitude of farmers on the adoption of highly pathogenic avian influenza epidemic prevention. They found a significant influence of both attitude and epidemic knowledge on the on-farm adoption of biosecurity practices by farmers. Moreover, this is also argued that knowledge gaps in health risks play an essential role in the prevention of AIDS (Kiviniemi et al., 2018). In light of this, epidemic knowledge may play an integral role in shaping the epidemic prevention behaviors of individuals.
5.5. Limitations and future research
Some limitations should be considered while conducting future work in this domain of this work. First, this is a perception-based work, and therefore the intention of individuals to adopt COVID-19 epidemic prevention might change for pre and post-adoption scenarios. Hence, it would be useful to consider the data from adopters and non-adopters of epidemic prevention for drawing even better implications. Second, the sample compiled from individuals was just enough to conduct a single estimation to yield homogeneous findings. In the future, the conduction of an extensive and large-scale questionnaire survey is advisable to compile large samples enough to perform regional estimations to yield heterogeneous findings. It would provide deep insights into heterogeneity concerning the individuals' adoption behavior of epidemic prevention across regional disparities. Thirdly, the selection of a specific class of people, particularly highly educated people holding at least a Master's degree, may fault our generalization for China. Therefore, future research should select a good representative sample of the entire population in China, in terms of the level of education, income, and type of employment, for a more generalized and informed understanding.
6. Conclusions
The core focus of this work was to examine the perception-based factors influencing the individuals' intention to adopt COVID-19 epidemic prevention in a modified behavioral framework in terms of estimating the relevance as well as the relative importance of those factors. First, governments' guidelines on epidemic prevention, risk perception, epidemic knowledge, risk aversion, perceived behavioral control, subjective norms, and attitude towards epidemic prevention are revealed to be drivers of individuals' intention to adopt epidemic prevention. Second, perceived feasibility to adopt epidemic prevention measures was exposed to be the barrier to individuals' intention to adopt epidemic prevention. Third, moral norms was identified to perform a neutral role in shaping individuals' intentions to adopt epidemic prevention. Fourth, concerning the relative importance of perception-based influence factors, governments' guidelines on epidemic prevention is found to be the most important and influential factor which is followed by the risk perception. Finally, attitude towards epidemic prevention showed least contributed in shaping the individuals’ intention to adopt epidemic prevention.
Credit author statement
Munir Ahmad: Conceptualization, Writing - original draft, Data curation Khadeeja Iram: Writing-Reviewing and Editing Gul Jabeen: Investigation, Software, Visualization, Methodology.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Acknowledgments
The authors have no conflict of interest to disclose. The authors are highly thankful to the editor, and the two anonymous reviewers as their suggestions have extensively improved this work.
Footnotes
acquired immunodeficiency syndrome.
Supplementary data to this article can be found online at https://doi.org/10.1016/j.envres.2020.109995.
Appendix A. Supplemental materials
Table A.1Factor loading of influence factors by measurement model test
| Constructs | Items | Outer loadings | Cronbach-α | ρ-A | CMPR | AVE |
|---|---|---|---|---|---|---|
| Risk perception (RP) | RP1 | 0.813 | 0.746 | 0.805 | 0.815 | 0.791 |
| RP2 | 0.848 | |||||
| RP3 | 0.901 | |||||
| RP4 | 0.862 | |||||
| RP5 | 0.824 | |||||
| Epidemic knowledge (EPK) | EPK1 | 0.837 | 0.773 | 0.816 | 0.896 | 0.776 |
| EPK2 | 0.811 | |||||
| EPK3 | 0.786 | |||||
| EPK4 | 0.829 | |||||
| EPK5 | 0.714 | |||||
| EPK6 | 0.850 | |||||
| EPK7 | 0.902 | |||||
| EPK8 | 0.793 | |||||
| Attitude towards epidemic prevention (ATEP) | ATEP1 | 0.921 | 0.726 | 0.753 | 0.865 | 0.800 |
| ATEP2 | 0.871 | |||||
| ATEP3 | 0.880 | |||||
| ATEP4 | 0.738 | |||||
| ATEP5 | 0.904 | |||||
| Perceived feasibility to adopt epidemic prevention (PFEP) | PFEP1 | 0.885 | 0.738 | 0.837 | 0.850 | 0.766 |
| PFEP2 | 0.881 | |||||
| PFEP3 | 0.820 | |||||
| PFEP4 | 0.790 | |||||
| Perceived behavioural control (PBC) | PBC1 | 0.838 | 0.822 | 0.839 | 0.857 | 0.751 |
| PBC2 | 0.854 | |||||
| PBC3 | 0.862 | |||||
| PBC4 | 0.756 | |||||
| PBC5 | 0.744 | |||||
| Subjective norms (SBN) | SBN1 | 0.756 | 0.761 | 0.782 | 0.790 | 0.789 |
| SBN2 | 0.704 | |||||
| SBN3 | 0.758 | |||||
| SBN4 | 0.749 | |||||
| Moral Norms (MNS) | MNS1 | 0.761 | 0.845 | 0.891 | 0.902 | 0.701 |
| MNS2 | 0.803 | |||||
| MNS3 | 0.727 | |||||
| MNS4 | 0.772 | |||||
| MNS5 | 0.813 | |||||
| Risk aversion (RA) | RA1 | 0.732 | 0.873 | 0.887 | 0.899 | 0.801 |
| RA2 | 0.791 | |||||
| RA3 | 0.721 | |||||
| RA4 | 0.786 | |||||
| RA5 | 0.734 | |||||
| Governments' guidelines on epidemic prevention (GGEP) | GGEP1 | 0.920 | 0.766 | 0.829 | 0.872 | 0.748 |
| GGEP2 | 0.875 | |||||
| GGEP3 | 0.889 | |||||
| GGEP4 | 0.763 | |||||
| GGEP5 | 0.825 | |||||
| Intention to adopt epidemic (COVID-19) prevention (IAEP) | IAEP1 | 0.867 | 0.798 | 0.805 | 0.840 | 0.795 |
| IAEP2 | 0.838 | |||||
| IAEP3 | 0.753 | |||||
| IAEP4 | 0.808 | |||||
| IAEP5 | 0.906 | |||||
| IAEP6 | 0.719 | |||||
Notes: the level of agreement is categorized as: 5 = “strong agreement”, 4 = “agreement”, 3 = “neutral”, 2 = “disagreement”, 1 = “strong disagreement.”
A.1. Structural model test
After the measurement model is proven accurate and effective, the structural model is tested. As a key requirement, the R2 score of the construct is manipulated. The R2 score calculates the variance accounted by every endogenously found construct. This measure has the function of validating the prediction capability of the structural model. In other words, it demonstrates the explanatory power of the model. It has been suggested that its score values exceeding the threshold level of 0.25 would be an average score. However, its score of about 0.13 would not be a very appropriate one in the behavioral sciences. On the other hand, its score less than or equal to 0.03 is absolutely a weak score (Davison and Hinkley, 1997). As can be seen from Table 3, the R2 score is 0.713, which is way greater than 0.25 and thus satisfying the first requirement. It implicates that the eight significant PIFs collectively explain 71.3% of the variations in the individuals' IAEP. It means that the model has reasonably high statistical power to present the explained variations. As a further requirement Q2 score by Stone-Geisser is tested. Its score exceeding zero (positive number) demonstrates the accuracy and the prediction significance of the construct under consideration (Ringle et al., 2018). In the same vein, the extent of impact estimated by the Q2 score provides the relative impact of the predictive relevance. To this end, the Q2 score exceeding 0.35 means that an exogenously found construct supplied enough amount of predictive relevance for the corresponding endogenously found construct of a variable (Hair et al., 2014). Based on the calculated score of Q2 (i.e., 0.446), the precision and accuracy of the structural model are verified. It implies that the predictive relevance of the PIFs on individuals' IAEP is acceptable. The measure of explained variation (i.e., R2) as well as the measure of predictive relevance (Q2) yields a single value for each model. In present scenario, a model is estimated involving path modeling from nine PIFs to individuals’ IAEP, therefore it estimated single value for each of the measures including R2 and Q2.
Table A.2Factors' correlations and discriminant validity testing.
| Factors | RP | EPK | ATEP | PFEP | PBC | SBN | MNS | RA | GGEP | IAEP |
|---|---|---|---|---|---|---|---|---|---|---|
| RP | (0.79) | |||||||||
| EPK | 0.296 | (0.83) | ||||||||
| ATEP | 0.162 | 0.153 | (0.80) | |||||||
| PFEP | 0.401 | 0.322 | 0.099 | (0.81) | ||||||
| PBC | 0.273 | 0.162 | 0.172 | 0.259 | (0.76) | |||||
| SBN | 0.352 | 0.371 | 0.368 | 0.281 | 0.273 | (0.79) | ||||
| MNS | 0.178 | 0.273 | 0.243 | 0.174 | 0.188 | 0.412 | (0.82) | |||
| RA | 0.392 | 0.166 | 0.182 | 0.309 | 0.254 | 0.276 | 0.382 | (0.78) | ||
| GGEP | 0.284 | 0.400 | 0.277 | 0.265 | 0.310 | 0.192 | 0.155 | 0.218 | (0.87) | |
| IAEP | 0.147 | 0.350 | 0.364 | −0.311 | 0.284 | 0.337 | 0.369 | 0.302 | 0.325 | (0.89) |
Notes: The diagonal values reported in brackets ( ) are square root of AVEs.
As a further requirement, the path coefficients are taken under advisement. In this regard, it is suggested that the estimated scores of path coefficients above 0.1 demonstrate effective impact within a structural model (Hair et al., 2013). Additionally, f2 is manipulated as a further requirement. Its score shows the impact size to describe the contributing capacity of a construct, through which the explained variations in endogenously determined LTVs are found by exogenous constructs (Davison and Hinkley, 1997). In the case of this work, governments' guidelines on epidemic prevention has depicted the greatest score in terms of its impact size. Similarly, risk perception has exposed the second greatest score, which is preceded by the impact size of epidemic knowledge. On the contrary, the moral norms demonstrated the slightest impact size from the set of all influence factors. Thus, the impact size determines the relative contribution of each of the PIFs to individuals’ IAEP. Any value of variance inflation factor (VIF) below 10 demonstrates the presence of acceptable level of multicollinearity issue, while VIF more than 10 is considered high level of multicollinearity. In present case the VIF values remained below 10, which showed its acceptable level.
The PLS-based path analysis is free of normality assumption applied to the parameter-based bootstrap procedure, which serves to determine the significance of outer loading and path coefficients. The bootstrap procedure considers contemplation of about 5 × 103 sampling units derived and extracted based on the original sampling unit through making use of the ‘with swap’ choice to get each sampling unit estimated. A bootstrap-based distribution originates, which is served to manipulate estimates' standard errors and the standard deviation. In this regard, the student's t-statistic is manipulated. For hypothesis testing, the null hypothesis for each established path is given as Hi = 0 for i = 1, 2, 3, …, 9. While the alternative hypothesis for each established path is given as Hi ≠ 0 for i = 1, 2, 3, …, 9. The path coefficients are taken to be relevant for any score of t-statistic equal to or exceeding the threshold level of 1.96 (Ringle et al., 2018). As for its equivalent, the path coefficients are considered significant at a 5% level for any probability score below ore equal to 0.05 (Lopes et al., 2019). Taking this requirement as a benchmark, for all of the hypotheses, with the exception of H7, the null hypotheses are rejected, and thus support has been found. In other words, except for moral norms, all of the influence factors significantly contribute to the individuals' IAEP.
Appendix A. Supplementary data
The following is/are the supplementary data to this article:
References
- Ajzen I. Theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991;50:179–211. [Google Scholar]
- Ajzen I. Action-Control: from Cognitions to Behavior. 1985. From Intentions to Actions : A Theory of Planned Behavior; pp. 11–39. [Google Scholar]
- Ajzen I., Fishbein M. The prediction of behavior from attitudinal and normative variables. J. Exp. Soc. Psychol. 1970;6:466–487. [Google Scholar]
- Baghbanzadeh M., Kumar Dewesh, Yavasoglu S.I., Manning S., Ali A., Ghasemzadeh H., Sikder I., Kumar Dilip, Murmu N., Haque U. Malaria epidemics in India : role of climatic condition and control measures. Sci. Total Environ. 2020;712 doi: 10.1016/j.scitotenv.2019.136368. [DOI] [PubMed] [Google Scholar]
- Bagozzi R.P., Heatherton T.F. Structural Equation Modeling : a general approach to representing multifaceted personality constructs : application to state self ‐ esteem. Struct. Equ. Model. 1994;1:35–67. doi: 10.1080/10705519409539961. [DOI] [Google Scholar]
- Bortoleto A.P., Kurisu K.H., Hanaki K. Model development for household waste prevention behaviour. Waste Manag. 2012;32:2195–2207. doi: 10.1016/j.wasman.2012.05.037. [DOI] [PubMed] [Google Scholar]
- Bryant-davis T., Ellis M.U., Edwards N., Adams T.P., Counts P., Arline-bradley S., Sadler K. The role of the black church in HIV Prevention : exploring barriers and. Best Pract. 2016;408:388–408. doi: 10.1002/casp. [DOI] [Google Scholar]
- Carrel L.F. ‘“ epidemic in Switzerland ”’: description of a strategic leadership exercise by the Swiss government. J. Contingencies Cris. Manag. 2005;13:170–175. [Google Scholar]
- Cui B., Liu Z.P., Ke J., Tian Y. Determinants of highly pathogenic avian influenza outbreak information sources, risk perception and adoption of biosecurity behaviors among poultry farmers in China. Prev. Vet. Med. 2019;167:25–31. doi: 10.1016/j.prevetmed.2019.03.018. [DOI] [PubMed] [Google Scholar]
- Cui B., Wang L.D.L., Ke J., Tian Y. Chinese poultry farmers' decision-making for avian influenza prevention: a qualitative analysis. Zoonoses Public Health. 2019;66:647–654. doi: 10.1111/zph.12617. [DOI] [PubMed] [Google Scholar]
- Davison A., Hinkley D. Statistical and Probabilistic Mathematics. Cambridge University Press; 1997. Bootstrap methods and their application; pp. 1–10. [DOI] [Google Scholar]
- Delpont M., Guerin J., Racicot M., Durivage A., Fornili L., Paul J.V.M.C. Determinants of biosecurity practices in French duck farms after a H5N8 Highly Pathogenic Avian Influenza epidemic : the effect of farmer knowledge , attitudes and personality traits. Transbound. Emerg. Dis. 2020:1–11. doi: 10.1111/tbed.13462. [DOI] [PubMed] [Google Scholar]
- Elmahdawy M., Elsisi G.H., Carapinha J., Lamorde M., Habib A., Agyie-baffour P., Soualmi R., Ragab S., Udezi A.W., Usifoh C., Usifoh S. Ebola virus epidemic in west Africa : global health economic challenges , lessons learned , and policy recommendations. Value Heal. Reg. Issues. 2017;13:67–70. doi: 10.1016/j.vhri.2017.08.003. [DOI] [PubMed] [Google Scholar]
- Elmustapha H., Hoppe T., Bressers H. Consumer renewable energy technology adoption decision-making; comparing models on perceived attributes and attitudinal constructs in the case of solar water heaters in Lebanon. J. Clean. Prod. 2018;172:347–357. doi: 10.1016/j.jclepro.2017.10.131. [DOI] [Google Scholar]
- Elyasi M., Lai H., Major P.W., Baker S.R., Amin M. 2020. Modeling the Theory of Planned Behaviour to Predict Adherence to Preventive Dental Visits in Preschool Children 1–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fishbein M., Ajzen I. Addison-Wesley; Boston: 1975. Belief, Attitude, Intention, and Behavior: an Introduction to Theory and Research. [Google Scholar]
- Hair J.F., Hult G.T.M., Ringle C.M. PLS-SEM); 2016. A Primer on Partial Least Squares Structural Equation Modeling. [Google Scholar]
- Hair J.F., Hult G.T.M., Ringle C.M., Sarstedt M. 2013. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM) Thousand Oaks. Sage 165. [Google Scholar]
- Hair J.F., Sarstedt M., Hopkins L., Kuppelwieser V.G. Partial least squares structural equation modeling (PLS-SEM): an emerging tool in business research. Eur. Bus. Rev. 2014;26:106–121. doi: 10.1108/EBR-10-2013-0128. [DOI] [Google Scholar]
- Kiviniemi M.T., Orom H., Waters E.A., McKillip M., Hay J.L. Education-based disparities in knowledge of novel health risks: the case of knowledge gaps in HIV risk perceptions. Br. J. Health Psychol. 2018;23:420–435. doi: 10.1111/bjhp.12297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lai C., Shih T., Ko W., Tang H., Hsueh P. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): the epidemic and the challenges. Int. J. Antimicrob. Agents. 2020;2:105924. doi: 10.1016/j.ijantimicag.2020.105924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lindell M.K., Whitney D.J. Accounting for common method variance in cross-sectional research designs. J. Appl. Psychol. 2001;86:114–121. doi: 10.1037//0021-9010.86.1.114. [DOI] [PubMed] [Google Scholar]
- Lopes J.R.N., Kalid R. de A., Rodríguez J.L.M., Ávila Filho S. A new model for assessing industrial worker behavior regarding energy saving considering the theory of planned behavior, norm activation model and human reliability. Resour. Conserv. Recycl. 2019;145:268–278. doi: 10.1016/j.resconrec.2019.02.042. [DOI] [Google Scholar]
- Msn J.L., Kang S.J. 2020. Factors Influencing Nurses ’ Intention to Care for Patients with Emerging Infectious Diseases : Application of the Theory of Planned Behavior 82–90. [DOI] [PubMed] [Google Scholar]
- Netemeyer R.G., Bearden W.O., Sharma S. SAGE Publications, Inc; 2003. Scaling Procedures: Issues and Applications. [Google Scholar]
- Nicola M., Alsafi Z., Sohrabi C., Kerwan A., Al-Jabir A., Christos I., Agha M., Agha R. The socio-economic implications of the coronavirus and COVID-19 pandemic: a review. Int. J. Surg. 2020 doi: 10.1016/j.ijsu.2020.04.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nishiura Hiroshi, Linton N.M., Akhmetzhanov A.R., Nishiura H. 2020. Title : Serial Interval of Novel Coronavirus ( COVID-19 ) Infections Authors : Affiliations : Correspondence To : medRxiv. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Omodior O., Luetke M.C., Nelson E.J. Mosquito-borne infectious disease, risk-perceptions, and personal protective behavior among U.S. international travelers. Prev. Med. Reports. 2018;12:336–342. doi: 10.1016/j.pmedr.2018.10.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Podsakoff P.M., Mackenzie S.B., Lee J., Podsakoff N.P. Common method biases in behavioral Research : a critical review of the literature and recommended remedies. J. Appl. Psychol. 2003;88:879–903. doi: 10.1037/0021-9010.88.5.879. [DOI] [PubMed] [Google Scholar]
- Przybyla S.M., Parks K., Bleasdale J., Sawyer J., Morse D. Awareness , knowledge , and attitudes towards human immunodeficiency virus ( HIV ) pre-exposure prophylaxis ( PrEP ) among pharmacy students. Curr. Pharm. Teach. Learn. 2019;11:352–360. doi: 10.1016/j.cptl.2019.01.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raude J., MCColl K., Flamand C., Apostolidis T. Understanding health behaviour changes in response to outbreaks: findings from a longitudinal study of a large epidemic of mosquito-borne disease. Soc. Sci. Med. 2019;230:184–193. doi: 10.1016/j.socscimed.2019.04.009. [DOI] [PubMed] [Google Scholar]
- Ringle C.M., Sarstedt M., Mitchell R., Gudergan S.P. Partial least squares structural equation modeling in HRM research. Int. J. Hum. Resour. Manag. 2018;5192:1–27. doi: 10.1080/09585192.2017.1416655. [DOI] [Google Scholar]
- Sued O., Figueroa M.I., Cahn P. Clinical challenges in HIV/AIDS : hints for advancing prevention and patient management strategies ☆. Adv. Drug Deliv. Rev. 2016;103:5–19. doi: 10.1016/j.addr.2016.04.016. [DOI] [PubMed] [Google Scholar]
- Swinburn B., Vandevijvere S., Kraak V., Sacks G., Snowdon W., Hawkes C., Barquera S., Friel S., Kelly B., Kumanyika S., L'Abbé M., Lee A., Lobstein T., Ma J., Macmullan J., Mohan S., Monteiro C., Neal B., Rayner M., Sanders D., Walker C. Monitoring and benchmarking government policies and actions to improve the healthiness of food environments: a proposed government healthy food environment policy index. Obes. Rev. 2013;14:24–37. doi: 10.1111/obr.12073. [DOI] [PubMed] [Google Scholar]
- Valeeva N.I., van Asseldonk M.A.P.M., Backus G.B.C. Perceived risk and strategy efficacy as motivators of risk management strategy adoption to prevent animal diseases in pig farming. Prev. Vet. Med. 2011;102:284–295. doi: 10.1016/j.prevetmed.2011.08.005. [DOI] [PubMed] [Google Scholar]
- WHO World health organization [WWW document]. Coronavirus dis. Pandemic. 2020. https://www.who.int/emergencies/diseases/novel-coronavirus-2019 URL.
- Wu P., Hao X., Lau E.H.Y., Wong J.Y., Leung K.S.M., Wu J.T., Cowling B.J., Leung G.M. Real-time tentative assessment of the epidemiological characteristics of novel coronavirus infections in Wuhan , China , as at 22 January 2020. Rapid Commun. 2020;1–6 doi: 10.2807/1560-7917.ES.2020.25.3.2000044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Xiaoliang M., Hansen A., Hanson-easey S., Xiang J., Cameron S., Liu Q., Liu X., Sun Y., Weinstein P., Han G., Williams C., Bi P. Perceptions of capacity for infectious disease control and prevention to meet the challenges of dengue fever in the face of climate change : a survey among CDC staff in Guangdong Province , China. Environ. Res. 2016;148:295–302. doi: 10.1016/j.envres.2016.03.043. [DOI] [PubMed] [Google Scholar]
- Yang Y., Peng F., Wang R., Guan K., Jiang T., Xu G., Sun J., Chang C. The deadly coronaviruses : the 2003 SARS pandemic and the 2020 novel coronavirus epidemic in China. J. Autoimmun. 2020;102434 doi: 10.1016/j.jaut.2020.102434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yasir A., Hu X., Ahmad M., Rauf A., Shi J., Nasir S.A. Modeling impact of word of mouth and E-government on online social presence during COVID-19 Outbreak : a multi-mediation approach. Int. J. Environ. Res. Publ. Health. 2020;17 doi: 10.3390/ijerph17082954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- You C., Deng Y., Hu W., Sun J. medRxiv; 2020. Estimation of the Time-Varying Reproduction Number of COVID-19 Outbreak in China. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.