

Abstract
Background/Aims
Latent tuberculosis screening is mandatory prior to initiating anti-tumor necrosis factor (anti-TNF) medications. Guidelines recommend interferon-gamma release assays (IGRA) as first line screening method for the general population. Studies provided conflicting evidence on IGRA and tuberculin skin test (TST) performance in inflammatory bowel disease (IBD) patients. We assessed test concordance and the effects of immunosuppression on their performance in IBD patients.
Methods
We searched MEDLINE, Embase and Cochrane databases (2011–2018) for studies testing TST and IGRA in IBD. Primary outcome was TST and IGRA concordance. Secondary outcomes were effects of immunosuppressive therapy on performance. Immunosuppression defined as either steroids, thiopurine, methotrexate or cyclosporine use. We used the pooled random effects model to adjust for heterogeneity analyzed using (I2–Q statistics). We compared the fixed model to exclude smaller study effects.
Results
Sixteen studies (2,488 patients) were included. Pooled TST and IGRA concordance was 85% (95% confidence interval [CI], 81%–88%; P=0.01). Effects of immunosuppression were reported in 8 studies (814 patients). The odds ratio of testing positive by IGRA decreased to 0.57 if immunosuppressed (95% CI, 0.31–1.03; P=0.06). The odds ratio of testing positive by TST if immunosuppressed was 1.14 (95% CI, 0.61–2.12; P=0.69). The fixed model yielded similar results, however the negative effect of immunosuppression on IGRA reached statistical significance (P=0.01).
Conclusions
While concordance was 85% between TST and IGRA, the performance of IGRA seems to be negatively affected by immunosuppression. Given the importance of detecting latent tuberculosis prior to anti-TNF initiation, further randomized controlled trials comparing the performance of TST and IGRA in IBD patients are needed.
Keywords: Inflammatory bowel disease; Crohn disease; Colitis, ulcerative; Tuberculosis
INTRODUCTION
Inflammatory bowel disease (IBD), including CD and UC is a chronic autoimmune disease that has a North American prevalence of 400–600 per 100,000 persons [1]. The treatment of CD and UC depends on disease severity and the presence of risk factors for progression. Guidelines recommend biologic medications, including TNF antagonists (anti-TNF-α) to be considered in the treatment of moderate to severe CD and UC [2,3]. In patients starting biologic therapy, particularly anti-TNF-α medications, there is an increased risk of tuberculosis reactivation. A potential mechanism is that TNF is required for chemokine expression and formation of granulomas in mycobacterial infection [4]. Screening for latent tuberculosis infection (LTBI) is mandatory prior to initiating anti-TNF-α treatment, to avoid tuberculosis reactivation.
Screening for LTBI can be done using the traditional tuberpculin skin test (TST) or newer interferon-gamma release assays (IGRA) [2]. New guidelines recommend the use of IGRA rather than TST in the general population [5]. The TST is limited by many confounders, most importantly by prior exposure to tuberculosis or vaccination. Another limiting factor is the need of a follow up visit to interpret subdermal induration. IGRA are blood tests where T cell release of interferon-gamma is quantified in vitro following antigen stimulation that are specific to Mycobacterium tuberculosis [6]. The effect of immunosuppression on both tests remains an area of research interest with limited data on their performance in IBD patients. Shahidi et al [7]. published a meta-analysis and systematic review in 2012 of 9 studies on the concordance of these tests in IBD patients and the effect of immunosuppression on their performance. However, trials have emerged since then with no guidance on optimal tuberculosis screening method in a commonly immunosuppressed IBD population. In this study, we aim to re-examine the evidence to assess the concordance and effects of immunosuppressive therapy (IST) on TST and IGRA in IBD patients prior to anti-TNF exposure.
METHODS
1. Study Protocol
The study protocol was registered using the international prospective register of systematic review (PROSPERO 2016 CRD42016049225) [8]. We followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) protocol to conduct this meta-analysis [9].
2. Search Strategy
Systematic searches performed (June 2011 to April 2018) using MEDLINE, Embase and Cochrane Library databases. Search timelines were chosen to examine evidence published after the Shahidi et al. [7] meta-analysis to pool results with the previous analysis using similar search strategies. The search strategy used text words and relevant indexing to identify articles discussing the diagnostic accuracy of IGRAs compared to TST to detect latent tuberculosis in patients with IBD. The search strategy included the following relevant search terms: (1) inflammatory bowel diseases, (2) tuberculin test, (3) interferon-gamma release tests (Supplementary Table 1). In addition, recursive searches, cross-referencing and subsequent hand-searches were performed. An attempt to contact corresponding authors was made when relevant data was not extractable from published potentially eligible abstracts or full articles.
3. Trial Selection and Patient Population
We included all adult human studies (abstracts and/or letters and/or full-text articles) published in English that were assessing both types of new IGRA generations (QFT-2G or 3G) and TST in IBD. Studies were excluded if they: (1) were not written in English; (2) only used older generation T-SPOT.TB testing (Oxford Immunotec Ltd., Milton, UK); (3) reported insufficient data on outcomes; (4) lacked appropriate study design; (5) had less than 10 IBD patients; (6) lacked IBD-specific outcomes; (7) were review articles lacking extractable data.
4. Study Outcomes
The primary outcome measure was the concordance between TST and IGRA in IBD patients being screened for LTBI prior to anti-TNF exposure. A secondary outcome included effects of IST on both TST and IGRA. Immunosuppression was defined as either exposure to: oral corticosteroids of more than 5 mg daily for at least 4 weeks, thiopurines, methotrexate or cyclosporine. A non-physiologic dose of steroids higher than 5 mg for more than 4 weeks was defined as the inclusion criteria in selected studies while included patients were on higher doses.
5. Data Extraction
We used Covidence, a Cochrane technology platform to upload citations for screening and to review [9]. Two reviewers (S.A. and P.G.) independently screened abstracts for full text review. After full text review, data were extracted using a standardized extraction form between the 2 reviewers. Cross review of data was done to ensure accuracy of data extracted. Disagreements were resolved by active discussion to reach consensus, if no consensus was reached a third reviewer (W.A.) was consulted. We examined the data to extract the following variables: country of origin, year of publication, study design, total number of IBD participants enrolled, number of IBD participants tested by both TST and IGRA, percent of BCG vaccinated, number of IBD patients on IST, IGRA version, timing of IGRA in relation to TST, purified protein derivative dose, TST cutoff, TST results, IGRA results, number of concordant IGRA and TST results; defined by both tests being positive or negative in each individual. A two by two table cross tabulating TST and IGRA results was generated (IGRA+/TST–, IGRA–/TST+, IGRA+/TST+, IGRA–/TST–). To examine the effects of immunosuppression on both TST and IGRA we generated a second table comparing rates of positive TST or IGRA in IBD patients on immunosuppression, compared to no-immunosuppression (IGRA+/IST+, TST+/IST+, IGRA+/IST–, TST+/IST–). Data extraction was generated and calculated from their respective publications. We reached out to respective authors for any missing data or clarifications needed. We excluded any study where authors failed to correspond regarding any missing data or clarifications needed, to prevent any data assumptions which may affect data integrity.
6. Quality Assessment
The quality of the studies was graded by using the new quality assessment tool for diagnostic accuracy studies Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) (Fig. 1) [10]. The QUADAS-2 is a modified version of QUADAS adopted for use by the Cochrane collaboration that is validated and recommended for use in Cochrane reviews. The QUADAS-2 tool contains 4 domains assessing patient selection, index test, reference standard, and flow of patients through the study and timing of the index tests and reference standard. The eligibility and quality of the studies were assessed independently by 2 investigators (S.A. and P.G.), with discrepancies resolved after discussion and reaching a consensus. If no consensus was reached a third reviewer was consulted (W.A).
Fig. 1.
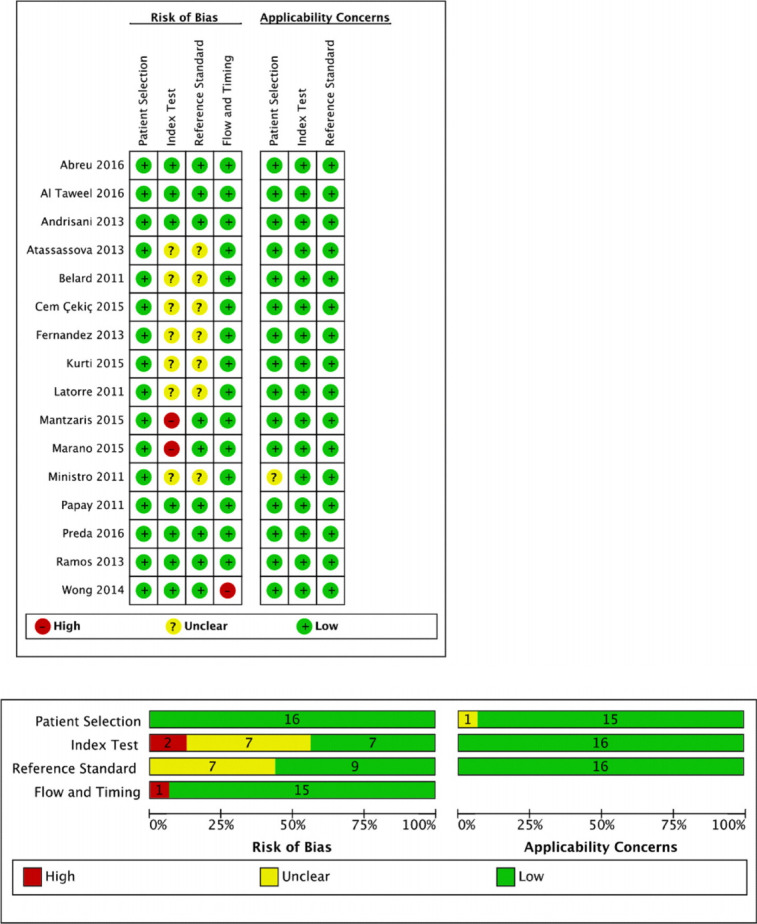
Assessment of risk of bias of studies: QUADAS-2 tool. QUADAS-2, Quality Assessment of Diagnostic Accuracy Studies-2.
7. Statistical Methods and Sensitivity Analyses
All statistical analyses were performed using RevMan (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014) [10]. First, the concordance and 95% CI of IGRA results versus TST results were calculated for each study (concordance was calculated by dividing the sum of patients with IGRA+/TST+ and those with IGRA–/TST– by the total number of subjects tested). Test results that are reported by authors to be indeterminate and required repetition were not included in the concordant group, which is defined as both tests being positive or negative. The decision to exclude indeterminate results was made to better capture the performance of both tests in real time, rather than affecting the concordance rate by repetition which affects performance by changing the number of true and false positives or negatives. Finally, the pooled concordance with the 95% CI was calculated using the random effects model. We then examined the effect of IST on both TST and IGRA performances by calculating the pooled odds ratio and 95% CI of testing positive if exposed to IST, compared to no exposure to IST. This was achieved by dividing the rate of positive results in IBD patients on IST over those who are not on IST. This analysis was done separately for TST and IGRA to calculate an independent pooled odds ratio for each test to assess individual performance. While pooled concordance rate of TST and IGRA was possible in IBD patients at large, data was insufficient to calculate separate concordance rates in patients on IST compared to those who were not. We used the Mantel-Haenszel method for a pooled random effects model, given anticipated heterogeneity of studies included. Heterogeneity was mainly driven by population size, demographics (i.e., BCG vaccination, tuberculosis prevalence, immunosuppressive medication use) and study design. We also compared the fixed effects model to exclude any effect of smaller studies. Heterogeneity between studies was analyzed using the statistical I [2], Q, and tau-square tests.
RESULTS
1. Literature Search
Of the 209 citations identified through the systematic review, 148 were excluded based on titles and abstracts, and 61 publications were fully reviewed (Fig. 2). A total of 45 studies were excluded after excluding studies that were in duplicate (n=13), did not have sufficient data (n=13), had inappropriate study design (n=11), outcomes (n=5) or population (n=3). From the 45 excluded studies, 8 studies were excluded at the end of review due to inability to reach the author for missing data or clarifications. Two authors responded and supplemented all missing data and clarifications needed for inclusion [11,12]. A total of 16 articles were finally included in our final analysis (5 conference abstracts [13-17], 1 correspondence letter [18], 10 full-text articles [11,12,19-26]). All eligible studies examined by Shahidi et al. [7] were similarly reviewed prior to inclusion in the final 16 analyzed studies. A total of 2,488 patients were included in the 16 selected studies.
Fig. 2.
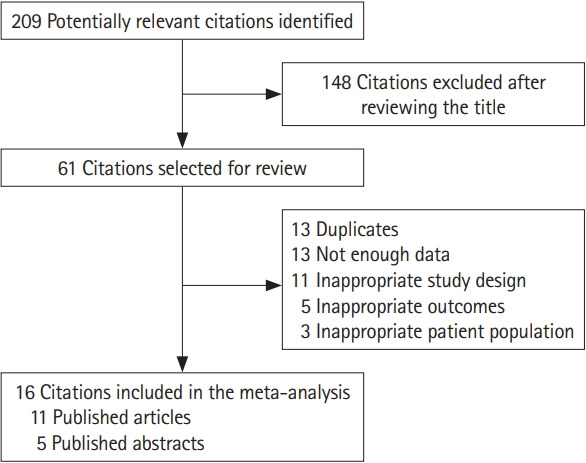
Diagram of selection process for studies identified by search protocol.
2. Study Quality and Heterogeneity
We assessed quality of studies by using QUADAS-2, taking TST as the reference test and IGRA as index test. The assessment suggested possible high risk of bias for 3 studies [11,16,24], 2 regarding the index test [16,24] and 1 regarding flow and timing [11] (Fig. 1). Heterogeneity observed mainly in population demographics (Table 1) during full text review of included studies made the random effects model the method of choice. We also included the fixed effects model to examine the effects of smaller studies. Meta-analysis recommendations are to choose the effects model prior to data analysis based on observed study heterogeneity during full text review to avoid any publication bias. In our study based on the variability of study designs, population size and demographics the random effects model was the model of choice [27]. However, we also report the fixed effect model to assess effects of smaller studies when low heterogeneity is observed.
Table 1.
Characteristics of Included Studies
| Study | Year | Country | 2017 WHO estimated TB incidence (thousand) | Study design | No. | Age (yr) | BCG vaccinated (%) | PPD cutoff (mm) |
|---|---|---|---|---|---|---|---|---|
| Abreu et al. [19] | 2016 | Portugal | 1.8 | Prospective observational cohort | 186 | NR | 100 | 5 |
| Al-Taweel et al. [20] | 2018 | Canada | 1.8 | Prospective observational cohort | 146 | Mean 39.6 | 16.4 | 5 If on IST, 10 if high risk population, 15 if no risk |
| Andrisani et al. [21] | 2013 | Italy | 3.8 | Prospective observational cohort | 92 | Range 36–43 | 1.0 | 5 If on IST,10 others |
| Atanassova [13]a | 2013 | Bulgaria | 1.5 | Prospective observational cohort | 34 | Mean 39 | 100 | NR |
| Bélard et al. [22] | 2011 | Denmark | 0.26 | Prospective observational cohort | 89 | Range 18–84 | 33.7 | 5 (BCG–), 10 (BCG+) |
| Çekiç et al. [23] | 2015 | Turkey | 12 | Retrospective observational cohort | 76 | Mean 42 | NR | 5 |
| Fernandez et al. [14]a | 2013 | Spain | 4.2 | Prospective observational cohort | 87 | Mean 40 | 23.0 | NR |
| Kurti et al. [12] | 2015 | Hungary | 0.65 | Prospective observational cohort | 65 | Mean 24 | 100 | 5 |
| Latorre et al. [15]a | 2011 | Spain | 4.2 | Prospective observational cohort | 13 | NR | NR | NR |
| Mantzaris et al. [24] | 2015 | Greece | 0.41 | Prospective observational cohort | 75 | Mean 37 | 34.7 | 5 If IST, 10 others |
| Marano et al. [16]a | 2015 | USA | 9.1 | Prospective randomized control trial | 1,283 | Mean 40 | 39.0 | 5 |
| Ministro et al. [17]a | 2011 | Portugal | 1.8 | Prospective observational cohort | 24 | NR | 100 | 5 |
| Papay et al. [25]a | 2011 | Austria | 0.57 | Prospective observational cohort | 208 | Mean 37 | 100 | 5 If IST, 10 others |
| Preda et al. [18]b | 2016 | Romania | 13 | Retrospective observational cohort | 16 | Mean 38 | NR | 5 |
| Ramos et al. [26] | 2013 | Spain | 4.2 | Prospective observational cohort | 25 | Median 32 | 8.0 | 5 |
| Wong et al. [11] | 2014 | China | 790 | Prospective observational cohort | 69 | NR | 73.0 | 5 |
Abstract only.
Letter.
WHO, World Health Organization; TB, tuberculosis; PPD, protein derivative dose; NR, not recorded; IST, immunosuppressive therapy.
3. Concordance between IGRA and TST and Impact of IST
The pooled concordance between TST and IGRA was 85% (95% CI, 81%–88%; P=0.01) (Fig. 3), with notable heterogeneity (I2=76%, P<0.001). The proportion and data for immunosuppressed population was reported and sufficient in 8 studies (n=811) [17,19-21,23-26]. The odds ratio of testing positive by IGRA if immunosuppressed was 0.57 (95% CI, 0.31–1.03; P=0.06) with possibly no important heterogeneity (I2=32%, P=0.17) (Fig. 4). However, TST had an odds ratio of 1.14 of testing positive (95% CI, 0.61–2.12; P=0.69), with possible moderate heterogeneity (I2=42%, P=0.10) (Fig. 5). Considering the low heterogeneity for the negative effect of immunosuppression on IGRA we also calculated the results with the fixed effect model (Supplementary Fig. 1). Using the fixed effects model, the OR of testing positive if immunosuppressed was 0.57 (95% CI, 0.37–0.89) and reached statistical significance (P=0.01).
Fig. 3.

Concordance between interferon-gamma release assay and tuberculin skin test. Ev, event; Trt, treatment.
Fig. 4.

OR of positive interferon-gamma release assay in immunosuppressed patients (IST+) compared to non-immunosuppressed (IST–). IST, immunosuppressive therapy; M-H, Mantel-Haenszel method.
Fig. 5.

OR of positive tuberculin skin test in immunosuppressed patients (IST+) compared to non-immunosuppressed (IST–). IST, immunosuppressive therapy; M-H, Mantel-Haenszel method.
DISCUSSION
Many studies reported variable performances of TST or IGRA in patient populations who are either at low risk of tuberculosis demographically or due to prior exposure to TNF therapies. These studies do not report significant data on concordance in TNF naïve patients only [28-30]. Older meta-analysis by Shahidi et al. [7] also included patients with prior TNF exposure. This is the first meta-analysis to date that investigates the concordance of both TST and IGRA and the effect of IST on test performances, in patients naïve to anti-TNF therapy. Excluding patients on anti-TNF therapy better addresses the clinical indication to screen for tuberculosis prior to initiating anti-TNF therapy in IBD patients. Including these studies could potentially bias the results by decreasing the sensitivity of both tests due to negative tuberculosis screening prior to anti-TNF initiation. In addition, this meta-analysis (16 studies encompassing 2,488 patients) adds further data to the 2010 meta-analysis published in 2012 by Shahidi (9 studies encompassing 1,309 patients). Studies included differ by excluding studies using older T-SPOT.TB form of IGRA, and including only patient naïve to anti-TNF therapy, reflecting real time practice and decreasing between test variability.
Our analysis results echo the 85% pooled concordance between TST and IGRA in 2,488 IBD patients, as observed in Shahidi et al. [7]. After excluding patients on anti-TNF therapy, our pooled analysis did not significantly show that TST and IGRA performances were negatively affected by IST using the random effects model. The random effects model was best chosen for significant heterogeneity. However, the negative effect of IST on IGRA did reach statistical significance when examining the fixed effects model (P<0.01). The fixed model minimizes the effect of smaller studies given heterogeneity between studies is low, giving more weight to larger studies. Despite current guidelines to use IGRA as first line screening in the general population, our analysis suggests that IGRA may be negatively affected in IBD patients on IST [5]. This reflects the most common clinical dilemma, as most IBD patients are screened for tuberculosis after prolonged use of IST (corticosteroids, methotrexate or thiopurines) to initiate biologic therapy. Currently, no guidelines exist to suggest the optimal test in IBD patients who are commonly immunosuppressed. While our analysis suggests that IGRA can be negatively affected by immunosuppression, TST positive result lacks statistical significance making its clinical utility in the setting of immunosuppression unclear. TST can be also be affected by many variables. TST can be laborious requiring 2 clinical visits to interpret results making it suboptimal and prone to noncompliance. Clinical judgement and understanding of the patient’s demographics, risk factors, vaccination status and local guidelines are crucial to correctly interpret TST results. Because of the many variables affecting TST performance we were unable to retrieve enough data to analyze the studies included based on prior exposure and risk factors. Evidence exists to support the cost effectiveness of a dual strategy screening method for tuberculosis and is most prominent in areas with low tuberculosis prevelance [31].
There are several limitations to our study. The different rates of BCG vaccination across studies affecting interpretation cutoffs in different countries is a limitation. Data was insufficient to analyze the result of each TST based on BCG vaccination, given vaccination rates were reported as overall percentages, rather than the vaccination status of each result reported. To address this limitation, we reported vaccination rates and cutoffs used when available (Table 1). We used each authors interpretation of a positive test based on local guidelines and when possible, a 5 mm cutoff was included in the analysis. This was done to minimize heterogeneity when assessing concordance, as most included studies used a 5 mm cutoff. While this may affect concordance rate, it does not affect our conclusion that IGRA can be negatively affected by immunosuppression. The inclusion of abstracts and in 1 case a letter to the editor is another potential limitation. However, leaving out data from Preda et al. [18] letter did not change results and overall concordance (0.847; 95% CI, 0.81–0.88) was similar, mainly due to small size of this cohort of patients. The inclusion of abstracts that have not been fully published could not be avoided, as there is a lack of sufficient data to generate a meta-analysis using only published randomized controlled trials. The inclusion of letters and abstracts in a meta-analysis, helps minimize the common issue of publication bias [32]. The lack of RCT published data is mainly due to the relatively rare occurrence of tuberculosis reactivation and the lack of availability of IGRA in high prevalence areas, where cost issues may arise. To better guide physicians, a prospective randomized clinical trial is needed to randomize IBD patients to 3 arms using TST, IGRA, TST and IGRA prior to anti-TNF therapy initiation. Such a study could help examine the rates of tuberculosis reactivation and assess the cost effectiveness of combining both tests as opposed to a single test. Until such evidence is available, our analysis suggests that relying on IGRA alone in IBD patients on IST may lead to tuberculosis reactivation. In fact, one recent study indicated that while IGRA was negatively affected by IST, patients that tested positive for IGRA and negative for TST, underwent treatment for LTBI [20]. These results highlight the need for perhaps a dual testing strategy in IBD patients that are immunosuppressed.
Acknowledgments
We thank all authors who responded to our correspondences to provide the required data and clarifications needed for their data to be included in this meta-analysis.
Footnotes
FINANCIAL SUPPORT
The authors received no financial support for the research, authorship, and/or publication of this article.
CONFLICT OF INTEREST
Bessissow T is a speaker or advisory board for Janssen, AbbVie, Takeda, Pfizer, Shire, Ferring, PendoPharm, Merck. He was supported by unrestricted research grants from Janssen, Abbvie, Pentax, and Echosense. But, all authors had no conflicts of interests to declare pertaining to submission.
AUTHOR CONTRIBUTION
Conceptualization: Alrajhi S, Afif W. Methodology: Alrajhi S, Germain P, Martel M, Afif W. Formal analysis: Alrajhi S, Germain P, Martel M. Project administration: Alrajhi S, Afif W. Visualization: Alrajhi S, Germain P, Martel M, Afif W. Writing - original draft: Alrajhi S, Germain P, Martel M, Afif W. Writing - review and editing: Alrajhi S, Germain P, Martel M, Lakatos P, Bessissow T, Al-Taweel T, Afif W. Approval of final manuscript: all authors.
SUPPLEMENTARY MATERIALS
Supplementary materials are available at the Intestinal Research website (https://www.irjournal.org).
Supplementary Table 1. Search Strings
Supplementary Fig. 1. OR positive interferon-gamma release assays in immunosuppressed patients (IST+) compared to non-immunosuppressed (IST–) with fixed model. IST, immunosuppressive therapy; M-H, Mantel-Haenszel method.
REFERENCES
- 1.Loftus EV., Jr Update on the incidence and prevalence of inflammatory bowel disease in the United States. Gastroenterol Hepatol (N Y) 2016;12:704–707. [PMC free article] [PubMed] [Google Scholar]
- 2.Sadowski DC, Bernstein CN, Bitton A, et al. Canadian Association of Gastroenterology Clinical Practice Guidelines: the use of tumour necrosis factor-alpha antagonist therapy in Crohn’s disease. Can J Gastroenterol. 2009;23:185–202. doi: 10.1155/2009/201430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bressler B, Marshall JK, Bernstein CN, et al. Clinical practice guidelines for the medical management of nonhospitalized ulcerative colitis: the Toronto consensus. Gastroenterology. 2015;148:1035–1058. doi: 10.1053/j.gastro.2015.03.001. [DOI] [PubMed] [Google Scholar]
- 4.Algood HM, Lin PL, Flynn JL. Tumor necrosis factor and chemokine interactions in the formation and maintenance of granulomas in tuberculosis. Clin Infect Dis. 2005:41–Suppl 3:S189-S193. doi: 10.1086/429994. [DOI] [PubMed] [Google Scholar]
- 5.Lewinsohn DM, Leonard MK, LoBue PA, et al. Official American Thoracic Society/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: diagnosis of tuberculosis in adults and children. Clin Infect Dis. 2017;64:111–115. doi: 10.1093/cid/ciw778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Pai M, Riley LW, Colford JM., Jr Interferon-gamma assays in the immunodiagnosis of tuberculosis: a systematic review. Lancet Infect Dis. 2004;4:761–776. doi: 10.1016/S1473-3099(04)01206-X. [DOI] [PubMed] [Google Scholar]
- 7.Shahidi N, Fu YT, Qian H, Bressler B. Performance of interferon-gamma release assays in patients with inflammatory bowel disease: a systematic review and meta-analysis. Inflamm Bowel Dis. 2012;18:2034–2042. doi: 10.1002/ibd.22901. [DOI] [PubMed] [Google Scholar]
- 8.Alrajhi S, Afif W, Altaweel T. TST and IGRA for tuberculosis screening in inflammatory bowel disease. PROSPERO Web site. https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42016049225. Accessed January 3, 2020.
- 9.Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Whiting PF, Rutjes AW, Westwood ME, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155:529–536. doi: 10.7326/0003-4819-155-8-201110180-00009. [DOI] [PubMed] [Google Scholar]
- 11.Wong SH, Ip M, Tang W, et al. Performance of interferon-gamma release assay for tuberculosis screening in inflammatory bowel disease patients. Inflamm Bowel Dis. 2014;20:2067–2072. doi: 10.1097/MIB.0000000000000147. [DOI] [PubMed] [Google Scholar]
- 12.Kurti Z, Lovasz BD, Gecse KB, et al. Tuberculin skin test and Quantiferon in BCG vaccinated, immunosuppressed patients with moderate-to-severe inflammatory bowel disease. J Gastrointestin Liver Dis. 2015;24:467–472. doi: 10.15403/jgld.2014.1121.244.bcg. [DOI] [PubMed] [Google Scholar]
- 13.Atanassova A, Kotzev I. P0308 IBD: screening for tuberculosis in patients candidates for anti‐TNF terapy in IBD. J Gastroenterol Hepatol. 2013;28(S3):23–693. [Google Scholar]
- 14.Fernandez S, Riera J, Balza N, et al. P124 Use of interferon-gamma release assay (IGRA) and tuberculin skin test (TST) for tuberculosis screening in patients candidates for anti-TNF terapy in inflammatory bowel disease (IBD) J Crohns Colitis. 2013;7(Suppl 1):S58. [Google Scholar]
- 15.Latorre I, Minguez S, Vilavella M, et al. Detection of IFN-gamma responses for diagnosis of tuberculosis infection in chronic inflammatory disease patients. Eur Respir J. 2011;38(Suppl 55):p305. [Google Scholar]
- 16.Marano C, Hsia EC, Xu S, Sandborn W, Rutgeerts P. P0361: Interferon-gamma release assay versus tuberculin skin test in patients with moderate-to-severely active ulcerative colitis: results from the pursuit UC program. United European Gastroenterol J. 2015;3(5 Suppl):146–687. [Google Scholar]
- 17.Ministro P, Machado J, Araújo R, Castanheira A, Cancela EM, Silva A. Diagnosis of latent tuberculosis in patients with inflammatory bowel disease: prospective comparison between tuberculin skin test and interferon gamma release assay (IGRA) test. Gastroenterology. 2011;140(5 Suppl 1):S776. [Google Scholar]
- 18.Preda CM, Fulger LE, Gheorghe C, et al. Tuberculin skin test and Quantiferon TB Gold in Romanian BCG vaccinated, immunosuppressed patients with moderate-to-severe Crohn’s disease: a comparison with a Hungarian cohort. J Gastrointestin Liver Dis. 2016;25:260–261. doi: 10.15403/jgld.2014.1121.252.tbg. [DOI] [PubMed] [Google Scholar]
- 19.Abreu C, Almeida F, Ferraz R, Dias CC, Sarmento A, Magro F. The tuberculin skin test still matters for the screening of latent tuberculosis infections among inflammatory bowel disease patients. Dig Liver Dis. 2016;48:1438–1443. doi: 10.1016/j.dld.2016.08.107. [DOI] [PubMed] [Google Scholar]
- 20.Al-Taweel T, Strohl M, Pai M, et al. A study of optimal screening for latent tuberculosis in patients with inflammatory bowel disease. Dig Dis Sci. 2018;63:2695–2702. doi: 10.1007/s10620-018-5178-1. [DOI] [PubMed] [Google Scholar]
- 21.Andrisani G, Armuzzi A, Papa A, et al. Comparison of Quantiferon-TB Gold versus tuberculin skin test for tuberculosis screening in inflammatory bowel disease patients. J Gastrointestin Liver Dis. 2013;22:21–25. [PubMed] [Google Scholar]
- 22.Bélard E, Semb S, Ruhwald M, et al. Prednisolone treatment affects the performance of the QuantiFERON Gold in-tube test and the tuberculin skin test in patients with autoimmune disorders screened for latent tuberculosis infection. Inflamm Bowel Dis. 2011;17:2340–2349. doi: 10.1002/ibd.21605. [DOI] [PubMed] [Google Scholar]
- 23.Çekiç C, Aslan F, Vatansever S, et al. Latent tuberculosis screening tests and active tuberculosis infection rates in Turkish inflammatory bowel disease patients under anti-tumor necrosis factor therapy. Ann Gastroenterol. 2015;28:241–246. [PMC free article] [PubMed] [Google Scholar]
- 24.Mantzaris GJ, Tsironikos D, Tzanetakou X, et al. The impact of immunosuppressive therapy on QuantiFERON and tuberculin skin test for screening of latent tuberculosis in patients with inflammatory bowel disease scheduled for anti-TNF therapy. Scand J Gastroenterol. 2015;50:1451–1455. doi: 10.3109/00365521.2015.1064470. [DOI] [PubMed] [Google Scholar]
- 25.Papay P, Eser A, Winkler S, et al. Factors impacting the results of interferon-gamma release assay and tuberculin skin test in routine screening for latent tuberculosis in patients with inflammatory bowel diseases. Inflamm Bowel Dis. 2011;17:84–90. doi: 10.1002/ibd.21427. [DOI] [PubMed] [Google Scholar]
- 26.Ramos JM, Masiá M, Rodríguez JC, et al. Negative effect of immunosuppressive therapy in the performance of the QuantiFERON Gold in-tube test in patients with immune-mediated inflammatory diseases. Clin Exp Med. 2013;13:177–186. doi: 10.1007/s10238-012-0192-7. [DOI] [PubMed] [Google Scholar]
- 27.Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. Fixed-effect versus random-effects models. In: Borenstein M, Hedges LV, Higgins JPT, Rothstein HR, editors. Introduction to meta-analysis. Hoboken: John Wiley & Sons Inc; 2009. pp. 61–102. [Google Scholar]
- 28.Schoepfer AM, Flogerzi B, Fallegger S, et al. Comparison of interferon-gamma release assay versus tuberculin skin test for tuberculosis screening in inflammatory bowel disease. Am J Gastroenterol. 2008;103:2799–2806. doi: 10.1111/j.1572-0241.2008.02050.x. [DOI] [PubMed] [Google Scholar]
- 29.Qumseya BJ, Ananthakrishnan AN, Skaros S, et al. QuantiFERON TB Gold testing for tuberculosis screening in an inflammatory bowel disease cohort in the United States. Inflamm Bowel Dis. 2011;17:77–83. doi: 10.1002/ibd.21329. [DOI] [PubMed] [Google Scholar]
- 30.Mow WS, Abreu-Martin MT, Papadakis KA, Pitchon HE, Targan SR, Vasiliauskas EA. High incidence of anergy in inflammatory bowel disease patients limits the usefulness of PPD screening before infliximab therapy. Clin Gastroenterol Hepatol. 2004;2:309–313. doi: 10.1016/s1542-3565(04)00060-6. [DOI] [PubMed] [Google Scholar]
- 31.Pooran A, Booth H, Miller RF, et al. Different screening strategies (single or dual) for the diagnosis of suspected latent tuberculosis: a cost effectiveness analysis. BMC Pulm Med. 2010;10:7. doi: 10.1186/1471-2466-10-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Hopewell S, Clarke M, Mallett S. Grey literature and systematic reviews. In: Rothstein HR, Sutton AJ, Borenstein M, editors. Publication bias in meta-analysis: prevention, assessment and adjustments. Chichester: John Wiley & Sons Ltd; 2005. pp. 49–72. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary materials are available at the Intestinal Research website (https://www.irjournal.org).
Supplementary Table 1. Search Strings
Supplementary Fig. 1. OR positive interferon-gamma release assays in immunosuppressed patients (IST+) compared to non-immunosuppressed (IST–) with fixed model. IST, immunosuppressive therapy; M-H, Mantel-Haenszel method.