

Abstract
Background:
Dentin hypersensitivity is primarily caused due to patent or exposed dentinal tubules. Nonfluoridated-desensitizing agents deposit hydroxycarbonate apatite (HCA), within the dentinal tubules, thereby relieving hypersensitivity. Fluoride-containing bioactive glass-based agents form fluorapatite which is less soluble when compared to hydroxyapatite and HCA.
Materials and Methods:
In this in vitro study forty dentin specimens obtained from extracted human premolars were divided randomly into four groups (n = 10): Group 1 – fluoridated bioactive glass (FBaG); Group 2 – bioactive glass (BaG); Group 3 – arginine calcium carbonate; Group 4 – saline. 37.5% phosphoric acid was used to ensure patent dentinal tubules. Test agents from each group were applied using a rubber cup. Half the treated samples were then subjected to 6% citric acid treatment. The degree of occlusion was evaluated using the scanning electron microscope, and the microscopic images were scored before and after the citric acid challenge by two blinded endodontists. Statistical analysis was performed using SPSS, one-way ANOVA, and post hoc Tukey test (P = 0.05).
Results:
Group 1 demonstrated better tubule occlusion in comparison with Group 2 and a statistically significant difference when compared to Group 3 (P = 0.001). Following acid challenge, Group 2 showed significantly more occluded tubules when compared with Group 3 (P = 0.001) and comparable difference with Group 1.
Conclusion:
All desensitizing agents showed satisfactory dentinal tubule occlusion. While fluoridated bioactive glass demonstrated better occlusion immediately after application, Bioactive glass showed better resistance to acid treatment.
Key Words: Bioactive glass, dentin hypersensitivity, scanning electron microscopy
INTRODUCTION
Dentin hypersensitivity (DH) is described as a short sharp pain that arises from exposed dentinal tubules to thermal, osmotic, evaporative, chemical, or tactile stimuli that cannot be compared to any dental defect or pathology.[1] Satisfactory occlusion of the exposed tubules can be achieved by smear layer or pellicle formation; however, prolonged exposure to oral fluids can negate this effect.[2] Brännstrom and Astroem described the mechanism for hypersensitivity based on the “hydrodynamic theory. ”[3] Hence, the treatment should be aimed at regaining the original state of the dentin, either by occluding the tubules or by gaining control over the neural elements in the pulp tissue that would weaken the stimulatory effects. These modalities bring about partial or complete tubule obliteration or alteration of sensory activity within the pulp or both.[3]
Bioactive glass (BaG, NovaMin®, developed by NovaMin Technology Inc., Alachua, FL, USA) derived from the original 45S5 Bioglass®(US Biomaterials Corp., Jacksonville, FL, USA) composition was incorporated within dentifrices as a remineralizing agent to treat DH. It precipitates the hydroxycarbonate apatite (HCA) on the surface of the tooth and bringing about subsequent occlusion of the dentinal tubules.[4,5,6] As the majority of the dentinal matrix is made up of collagen, the BaG particles were expected to bind to the exposed dentin surfaces and bring about the physical occlusion of dentinal tubules. Studies have demonstrated that the initial reactivity of the BaG particles is attributed to the development of a surface negative charge, that enables binding to Type I collagen fibers.[7] The fluoridated daily use toothpaste containing NovaMin for the treatment of DH and repair of sensitive teeth is based upon 5% w/w calcium sodium phosphosilicate (CSPS) technology. The CSPS technology delivers a hydroxyapatite-like reparative layer to the surface of the dentin in vitro, which has shown to be resistant to acid challenge.[7]
Another novel technology introduced in the recent past advocates the use of 8% arginine calcium carbonate (ACC) to treat DH. The deposition of arginine bicarbonate and calcium carbonate has been shown to physically block and seal open dentinal tubules.[8] Arginine and calcium carbonate act simultaneously in accordance with the natural modes of tubule occlusion and deposit a dentin-like mineral, primarily composed of calcium and phosphate, inside the dentinal tubules.[1] This “Pro-Argin ” technology is known to physically occlude and seal the exposed dentinal tubules, thereby relieving DH.[9]
Fluoride is commonly used in varnishes, mouth rinses, and dentifrices since its introduction in 1941. Fluoride ions can be incorporated into the glass matrix as calcium fluoride by part substituting network modifier oxides or by maintaining relatively constant ratios of the other constituents. It was demonstrated that fluoride-containing bioactive glasses (FBaG) form fluorapatite (FAp) instead of HCA.[10] Due to their ability to release fluoride locally, FBaGs make interesting candidates for a variety of clinical applications, one of which includes dentinal tubule occlusion to treat DH.[11] Therefore, the purpose of this in vitro study was to evaluate the efficacy of fluoridated BaG toothpaste, nonfluoridated BaG toothpaste, and ACC-containing toothpaste in dentinal tubule occlusion using scanning electron microscopy (SEM).
MATERIALS AND METHODS
The in vitro study was conducted in the department of conservative dentistry and endodontics after obtaining the Institutional Ethical Committee clearance (Ref. No: 17042).
Forty human permanent maxillary and mandibular premolars that were extracted for orthodontic reasons were used to prepare dentin discs. Teeth with any visible or clinically detectable cracks, stains, caries, wear facets, erosive or abrasive lesions, attrition, restorations, white spot lesions, or hypoplasia were excluded from the study.
A high-speed diamond bur (TF-21, Mani Inc., Japan) was used to decoronate the teeth. Dentin discs of 1.0 ± 0.1 mm thickness were obtained from the middle coronal dentin by sectioning the teeth perpendicular to their long axis. Any remaining enamel was removed and a silicon carbide paper (600 grit) was used to eliminate any surface irregularities and to create a smooth and uniform surface. Specimens were then sonicated for 10 min and then thoroughly rinsed with saline to ensure complete removal of the polishing abrasive. 35% phosphoric acid (3M, ESPE, USA) was used for 30 s to etch the dentin and expose the dentinal tubules. Specimens were then rinsed with distilled water and sonicated for 5 min to remove any residual etchant. The samples were then placed in phosphate-buffered solution (PBS) until further use.
Study design
The dentin discs were randomly divided into four groups (n = 10) [Table 1].
Table 1.
Experimental groups
| Group | Test agent |
|---|---|
| Group 1 | FBaG; (Elsenz® Biomin-F, Group Pharmaceuticals Limited, India) |
| Group 2 | BaG; NovaMin (SHY-NM, Group Pharmaceuticals Limited, India) |
| Group 3 | ACC (Colgate® Sensitive Pro-Relief TM, Colgate Oral Pharmaceuticals Inc., New York, NY, USA) |
| Group 4 | Saline (control) |
FBaG: Fluoridated bioactive glass; BaG: Bioactive glass; ACC: Arginine calcium carbonate
Treatment of specimens
The specimens (n = 10) from each group were loaded on microscope slides with the polished surface facing upward and secured using a double-sided tape. The samples were moistened with PBS solution, and a rubber cup attached to a slow-speed handpiece (NSK, Japan) was used to apply the products on the specimens. The samples were left undisturbed for 5 min, following which they were rinsed using distilled water to remove any residual material from the surfaces.
Five specimens were then randomly chosen from each group for SEM analysis.
Acid challenge
Remaining specimens (n = 5) from each of the groups were then exposed to 6% citric acid having a pH = 2 in a Petri dish for 1 min and then rinsed with distilled water for 2 min.
Evaluation of dentinal tubule occlusion
The degree of dentinal tubule occlusion was evaluated with the help of an SEM (TM3000 Tabletop Microscope, Hitachi, Tokyo, Japan). The specimens were sputter coated with gold using a gold/palladium mini sputter coater (Emitech SC7620, UK) and examined at an operating voltage of 5 kV. The SEM images were captured at ×2000.
Dentin specimens were evaluated after each of the following situations:
After etching with phosphoric acid – To confirm that the dentinal tubules are in an open unoccluded state [Figures 1a, 2a and 3a]
After application of test agent – To evaluate the degree of dentinal tubule occlusion [Figures 1b, 2b and 3b]
After acid challenge – To evaluate the resistance of the treated specimens (occluded tubules) to acid challenge [Figures 1c, 2c and 3c].
Figure 1.

Representative scanning microscopic images of the dentin surfaces showing the degree of tubule occlusion (a) after etching with phosphoric acid; (b) after treatment; (c) after treatment followed by the acid challenge for Group 1 – FBaG. FBaG: Fluoridated bioactive glass
Figure 2.

Representative scanning microscopic images of the dentin surfaces showing the degree of tubule occlusion (a) after etching with phosphoric acid; (b) after treatment; (c) after treatment followed by the acid challenge for Group 2 –BaG, BaG: Bioactive glass
Figure 3.

Representative scanning microscopic images of the dentin surfaces showing the degree of tubule occlusion (a) after etching with phosphoric acid; (b) after treatment; (c) after treatment followed by the acid challenge for Group 3 – ACC, ACC: Arginine calcium carbonate
Each treated surface of every specimen was analyzed, and four images were captured to minimize subjectivity. Two well-trained blinded endodontists assessed and scored the degree of tubule occlusion. The tubule occlusion classification scoring system was used, and scoring was based on a categorical scale of 1–5: (1) occluded (100% of tubules occluded); (2) mostly occluded (50–< 100% of tubules occluded); (3) partially occluded (25–< 50% of tubules occluded); (4) mostly unoccluded (< 25% of tubules occluded); (5) unoccluded (0%, no tubule occlusion).
Statistical analysis
The SPSS 20.0 version was used for the statistical analysis. The mean occlusion scores were analyzed using one-way ANOVA and the post hoc Tukey test. Paired t-test was used for intragroup comparison before and after the acid challenge (P = 0.05).
RESULTS
Specimens treated with fluoridated bioactive glass (FBaG) demonstrated higher tubule occlusion with a mean value of 3.27, followed by ACC and BaG with mean values of 3.31 and 3.43, respectively [Chart 1]. Following acid challenge, BaG demonstrated the highest degree of tubule occlusion with a mean value of 3.09, followed by FBaG with a mean value of 3.68, and the least number of occluded tubules was observed in the ACC group, with a mean value of 4.3 [Chart 1] and Figures 1b, 2b, 3b.
Chart 1.
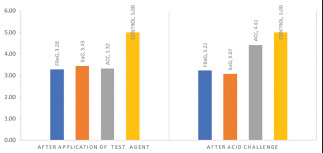
Degree of tubule occlusion seen after application of test agents and after acid challenge. Group 1: FBaG, Group 2: BaG, Group 3: ACC, Group 4: Control (saline). FBaG: Fluoridated bioactive glass; BaG: Bioactive glass; ACC: Arginine calcium carbonate.
Following acid challenge, intergroup comparison revealed a statistically significant difference between the BaG and the ACC groups [Table 2 and Figures 2c, 3c].
Table 2.
One-way ANOVA and post hoc Tukey test to assess the tubule occlusion scores before application of test agent and following acid challenge
| Treatment of specimens | FBaG | BaG | ACC | Control | F | P |
|---|---|---|---|---|---|---|
| Test | 3.28±0.87* | 3.43±0.59# | 3.31±0.40ϑ | 5±0*,#,ϑ | 22.897 | <0.001 |
| Postacid challenge | 3.68±0.79* | 3.09±0.80φ,# | 4.3±0.62φ | 5±0*,# | 18.51 | <0.001 |
*The standard deviations of the values measured in test and postacid challenge are less than half the mean values, this is an indicator of a normally distributed data; thus, one-way ANOVA parametric test was utilized for the same. *,#,ϑ,φMatching symbols indicate significant difference. Post hoc Tukey test <0.05 is considered statistically significant. The standard deviation is less than half the mean indicating a normal distribution of the data. Hence, ANOVA test (parametric test) is justified. FBaG: Fluoridated bioactive glass; BaG: Bioactive glass; ACC: Arginine calcium carbonate
While FBaG and BaG groups showed no significant intragroup difference in dentinal tubule occlusion before and after citric acid challenge, significant intragroup differences were noted with the ACC group [Table 2 and Figure 3a-c]. SEM image evaluation of dentin surface treated with fluoridated BaG demonstrated peritubular particle depositions and coverage of the dentinal tubules [Figure 1b]. In the BaG group, few dentinal tubules demonstrated complete occlusion along with some unoccluded tubules [Figure 2b]. The samples subjected to treatment with ACC showed crystal-like depositions within the dentinal tubules [Figure 3b]. Postacid challenge, most tubules in the FBaG and BaG specimens remained fairly occluded [Figures 1c and 2c]. However, more unoccluded tubules were seen in the specimens treated with ACC [Figure 3c]. The specimens treated with saline no change in tubule patency before and after the acid challenge [Figure 4a-c].
Figure 4.

Representative scanning microscopic images of the dentin surfaces showing the degree of tubule occlusion (a) after etching with phosphoric acid; (b) after treatment; (c) after treatment followed by the acid challenge for Group 4 – Saline.
Scoring criteria: 1 = occluded (100% of tubules occluded); 2 = mostly occluded (50–< 100% of tubules occluded); 3 = partially occluded (25–< 50% of tubules occluded); 4 = mostly unoccluded (< 25% of tubules occluded); 5 = unoccluded (0%, no tubule occlusion).
DISCUSSION
Saliva has shown to naturally occlude dentinal tubules by forming a protective glycoprotein layer with the help of calcium and phosphate ions.[1] This process of natural tubule occlusion is reported to be extremely slow, and the tubule plugging is easily dislodged by dietary acid, thereby rendering it ineffective in providing lasting relief. Hence, various chemical formulations have been developed to occlude the dentinal tubules to reduce dentinal sensitivity.
According to the results of this study, fluoridated BaG [Figure 1] demonstrated better occlusion of dentinal tubules when compared with the ACC group. This difference in occlusion can be attributed to the formation of FAp seen in the FBaG group.[4,10,11] Based on research by Lynch et al., fluoride-containing BaGs form FAp, which is shown to be more acid resistant than HCA.[4,12] According to Mneimne et al., an increase in phosphate content in the glass allows the formation of FAp rather than fluorite, even at a lower pH.[13] Furthermore, FAp is less soluble when compared to hydroxyapatite and HCA, thus making it more resistant to attack by acid. Hence, it can be presumed that these particles would be lost less readily, especially on exposure to acidic insults.[4]
The results also demonstrated that the BaG-containing group had the highest number of occluded tubules, especially after the acid challenge. This can be attributed to the mechanism by which these BaGs act. According to Burwell et al., NovaMin present within the BaGs binds to the exposed dentinal surface and reacts with it to form a mineralized layer. The layer formed is not only mechanically strong but also resistant to acid attack. Further, the continuous release of calcium over time has been shown to maintain the protective effects on dentin and maintain occlusion of the dentin tubules.[14,15] The result obtained in our study is in agreement with other in vitro studies.[16,17] Another study concluded that when NovaMin particles come into contact with saliva, an immediate release of sodium ions occurs, which increases the local environmental pH.[16] This combination of sodium ion release and pH rise facilitates the rapid precipitation of a calcium phosphate HCA layer, following the subsequent release of calcium and phosphate ions.[7] Furthermore, the CSPS particles can act as reservoirs to release calcium and phosphate ions continuously into the local environment.[17]
Earlier in vitro studies have also demonstrated that NovaMin was quick in occluding dentinal tubules and forming a protective layer on the dentinal surface.[18,19] Mony et al.,[20] in their comparative study, observed that there was better deposition of material over decalcified enamel by NovaMin than with fluoride. This finding can be further substantiated by various in vivo studies that have demonstrated better tubule occlusion over a prolonged period with BaGs (NovaMin).[21,22,23,24] Based on a randomized controlled trial carried out by Neuhaus et al., it was observed that a single application of both fluoridated and nonfluoridated prophylaxis pastes containing 15% CSPS (NovaMin) provided a significant reduction of DH immediately after a single application that lasted up to 28 days.[25]
Group III (ACC) exhibited significantly poor tubule occlusion when compared with both the BaG-containing groups. This was consistent with the findings obtained by West et al.; except in their study, the test agents were applied with the help of electric toothbrushes.[26] According to Kleinberg, when arginine and calcium carbonate act together, they form a positively charged complex that enables it to bind to the dentin surface which is negatively charged. Furthermore, the alkaline pH aids in tubule occlusion by enabling the deposition of calcium and phosphate from the saliva and dentinal fluid, thereby enhancing the tubular occlusion.[27] However, the results obtained in this study are similar to an in vivo study by Rao et al.[28] and an in vitro study by Bakri et al.,[12] where it was demonstrated that NovaMin-containing desensitizing paste provided better relief than ACC-containing paste.
The results have demonstrated that the degree of tubule occlusion seen with fluoridated BaG was comparable with the BaG group, and both the BaG-containing agents demonstrated resistance to a citric acid challenge and showed better tubule occlusion compared to ACC-containing agent. This result, when compared with other experimental studies by Parkinson and Wilson,[29] Shah et al.,[30] and Sauro et al.,[31] showed similar findings. As observed, Group III (ACC) demonstrated satisfactory tubule occlusion, but poor resistance to citric acid challenge, similar to other experimental studies by Davies et al, Rajguru et al[32,33] and Parkinson and Wilson[29] thereby suggesting that occlusion by arginine based dentifrices is not stable following prolonged acid challenge and is more susceptible to dissolution by acids.
Thus, the results obtained reveal that the degree of tubule occlusion seen with fluoridated BaG was comparable with the BaG group. However, both the BaG-containing agents demonstrated resistance to a citric acid challenge and showed better tubule occlusion compared to ACC-containing agent.
Inability to precisely mimic the intraoral environment, the potential action of saliva, and its buffering ability in the presence of acidic environment could not be evaluated in our study and can be considered as a limitation of this study.
CONCLUSION
Within the limitations of this study, it can be concluded that fluoridated and nonfluoridated BaG-containing toothpaste showed a significant degree of dentinal tubule occlusion and can be recommended as desensitizing agents in cases of hypersensitivity. BaGs demonstrated better resistance to acid attack; hence, their use in the treatment of noncarious or erosive lesions is recommended.
Financial support and sponsorship
Nil.
Conflicts of interest
The authors of this manuscript declare that they have no conflicts of interest, real or perceived, financial or non-financial in this article.
REFERENCES
- 1.Chen CL, Parolia A, Pau A, Celerino de Moraes Porto IC. Comparative evaluation of the effectiveness of desensitizing agents in dentine tubule occlusion using scanning electron microscopy. Aust Dent J. 2015;60:65–72. doi: 10.1111/adj.12275. [DOI] [PubMed] [Google Scholar]
- 2.Bartold PM. Dentinal hypersensitivity: A review. Aust Dent J. 2006;51:212–8. [PubMed] [Google Scholar]
- 3.Brannstrom M, Johnson G, Nordenvall KJ. Transmission and control of dental pain: Resin impregnation for the desensitization of dentin. J Am Dent Assoc. 1979;99:612–618. doi: 10.14219/jada.archive.1979.0337. [DOI] [PubMed] [Google Scholar]
- 4.Lynch E, Brauer DS, Karpukhina N, Gillam DG, Hill RG. Multi-component bioactive glasses of varying fluoride content for treating dentin hypersensitivity. Dent Mater. 2012;28:168–78. doi: 10.1016/j.dental.2011.11.021. [DOI] [PubMed] [Google Scholar]
- 5.Vollenweider M, Brunner TJ, Knecht S, Grass RN, Zehnder M, Imfeld T, et al. Remineralization of human dentin using ultrafine bioactive glass particles. Acta Biomater. 2007;3:936–43. doi: 10.1016/j.actbio.2007.04.003. [DOI] [PubMed] [Google Scholar]
- 6.Kumar A, Singh S, Thumar G, Mengji A. Bioactive glass nanoparticles (NovaMin®) for applications in dentistry. J Dent Med Sci. 2015;14:30–5. [Google Scholar]
- 7.Layer TM. Development of a fluoridated, daily-use toothpaste containing NovaMin technology for the treatment of dentin hypersensitivity. J Clin Dent. 2011;22:59–61. [PubMed] [Google Scholar]
- 8.Docimo R, Montesani L, Maturo P, Costacurta M, Bartolino M, DeVizio W, et al. Comparing the efficacy in reducing dentin hypersensitivity of a new toothpaste containing 8.0% arginine, calcium carbonate, and 1450 ppm fluoride to a commercial sensitive toothpaste containing 2% potassium ion: An eight-week clinical study in Rome, Italy. J Clin Dent. 2009;20:17–22. [PubMed] [Google Scholar]
- 9.Hamlin D, Williams KP, Delgado E, Zhang YP, DeVizio W, Mateo LR. Clinical evaluation of the efficacy of a desensitizing paste containing 8% arginine and calcium carbonate for the in-office relief of dentin hypersensitivity associated with dental prophylaxis. Am J Dent. 2009;22(Spec No A):16A–20A. [PubMed] [Google Scholar]
- 10.Brauer DS, Karpukhina N, O'Donnell MD, Law RV, Hill RG. Fluoride-containing bioactive glasses: Effect of glass design and structure on degradation, pH and apatite formation in simulated body fluid. Acta Biomater. 2010;6:3275–82. doi: 10.1016/j.actbio.2010.01.043. [DOI] [PubMed] [Google Scholar]
- 11.Shah FA. Fluoride-containing bioactive glasses: Glass design, structure, bioactivity, cellular interactions, and recent developments. Mater Sci Eng C Mater Biol Appl. 2016;58:1279–89. doi: 10.1016/j.msec.2015.08.064. [DOI] [PubMed] [Google Scholar]
- 12.Bakri MM, Hossain MZ, Razak FA, Saqina ZH, Misroni AA, Ab-Murat N, et al. Dentinal tubules occluded by bioactive glass-containing toothpaste exhibit high resistance toward acidic soft drink challenge. Aust Dent J. 2017;62:186–91. doi: 10.1111/adj.12484. [DOI] [PubMed] [Google Scholar]
- 13.Mneimne M, Hill RG, Bushby AJ, Brauer DS. High phosphate content significantly increases apatite formation of fluoride-containing bioactive glasses. Acta Biomater. 2011;7:1827–34. doi: 10.1016/j.actbio.2010.11.037. [DOI] [PubMed] [Google Scholar]
- 14.Pradeep AR, Sharma A. Comparison of clinical efficacy of a dentifrice containing calcium sodium phosphosilicate to a dentifrice containing potassium nitrate and to a placebo on dentinal hypersensitivity: A randomized clinical trial. J Periodontol. 2010;81:1167–73. doi: 10.1902/jop.2010.100056. [DOI] [PubMed] [Google Scholar]
- 15.Burwell A, Jennings D, Muscle D, Greenspan DC. NovaMin and dentin hypersensitivity –in vitro evidence of efficacy. J Clin Dent. 2010;21:66–71. [PubMed] [Google Scholar]
- 16.Wang Z, Sa Y, Sauro S, Chen H, Xing W, Ma X, et al. Effect of desensitising toothpastes on dentinal tubule occlusion: A dentine permeability measurement and SEM in vitro study. J Dent. 2010;38:400–10. doi: 10.1016/j.jdent.2010.01.007. [DOI] [PubMed] [Google Scholar]
- 17.Litkowski LJ, Hack GD, Sheaffer HB, Greenspan DC. Occlusion of dentine tubules by 45S5 bioglass bioceramics 10. In: Sedel L, Rey C, editors. Proceedings of the 10th International Symposium on Ceramics in Medicine. Paris, France: 1997. [Google Scholar]
- 18.Huang X, Li R, Feng Y, Wang Y. Remineralization of demineralized dentin induced by bioactive glass NovaMin. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2018;43:619–24. doi: 10.11817/j.issn.1672-7347.2018.06.007. [DOI] [PubMed] [Google Scholar]
- 19.Taha AA, Patel MP, Hill RG, Fleming PS. The effect of bioactive glasses on enamel remineralization: A systematic review. J Dent. 2017;67:9–17. doi: 10.1016/j.jdent.2017.09.007. [DOI] [PubMed] [Google Scholar]
- 20.Mony S, Rao A, Shenoy R, Suprabha BS. Comparative evaluation of the remineralizing efficacy of calcium sodium phosphosilicate agent and fluoride based on quantitative and qualitative analysis. J Indian Soc Pedod Prev Dent. 2015;33:291–5. doi: 10.4103/0970-4388.165667. [DOI] [PubMed] [Google Scholar]
- 21.Rajesh KS, Hedge S, Arun Kumar MS, Shetty DG. Evaluation of the efficacy of a 5% calcium sodium phosphosilicate (Novamin) containing dentifrice for the relief of dentinal hypersensitivity: A clinical study. Indian J Dent Res. 2012;23:363–7. doi: 10.4103/0970-9290.102228. [DOI] [PubMed] [Google Scholar]
- 22.Kakar A, Kakar K, Sreenivasan PK, DeVizio W, Kohli R. Comparison of the clinical efficacy of a new dentifrice containing 8.0% arginine, calcium carbonate, and 1000 ppm fluoride to a commercially available sensitive toothpaste containing 2% potassium ion on dentin hypersensitivity: A randomized clinical trial. J Clin Dent. 2012;23:40–7. [PubMed] [Google Scholar]
- 23.Madan N, Madan N, Sharma V, Pardal D, Madan N. Tooth remineralization using bio-active glass-A novel approach. J Acad Adv Dent Res. 2011;2:45–50. [Google Scholar]
- 24.Athuluru D, Reddy C, Sudhir KM, Kumar K, Gomasani S, Nagarakanti S. Evaluation and comparison of efficacy of three desensitizing dentifrices on dentinal hypersensitivity and salivary biochemical characteristics: A randomized controlled trial. Dent Res J (Isfahan) 2017;14:150–7. [PMC free article] [PubMed] [Google Scholar]
- 25.Neuhaus KW, Milleman JL, Milleman KR, Mongiello KA, Simonton TC, Clark CE, et al. Effectiveness of a calcium sodium phosphosilicate-containing prophylaxis paste in reducing dentine hypersensitivity immediately and 4 weeks after a single application: A double-blind randomized controlled trial. J Clin Periodontol. 2013;40:349–57. doi: 10.1111/jcpe.12057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.West NX, Hughes JA, Addy M. The effect of pH on the erosion of dentine and enamel by dietary acids in vitro. J Oral Rehabil. 2001;28:860–4. doi: 10.1046/j.1365-2842.2001.00778.x. [DOI] [PubMed] [Google Scholar]
- 27.Kleinberg I. SensiStat. A new saliva-based composition for simple and effective treatment of dentinal sensitivity pain. Dent Today. 2002;21:42–7. [PubMed] [Google Scholar]
- 28.Rao A, Mitra D, Prabhakar A, Soni S, Ahmed S, Arya S. The reduction efficacy of dentinal hypersensitivity by two commercially available desensitizing toothpastes: Vantej and Colgate Pro-Argin. Saudi Endod J. 2014;4:7. [Google Scholar]
- 29.Parkinson CR, Willson RJ. A comparative in vitro study investigating the occlusion and mineralization properties of commercial toothpastes in a four-day dentin disc model. J Clin Dent. 2011;22:74–81. [PubMed] [Google Scholar]
- 30.Shah S, Shivakumar A, Khot O, Patil C, Hosmani N. Efficacy of NovaMin-and Pro-Argin-containing desensitizing dentifrices on occlusion of dentinal tubules. Dent Hypotheses. 2017;8:104. [Google Scholar]
- 31.Sauro S, Watson TF, Thompson I. Dentine desensitization induced by prophylactic and air-polishing procedures: An in vitro dentine permeability and confocal microscopy study. J Dent. 2010;38:411–22. doi: 10.1016/j.jdent.2010.01.010. [DOI] [PubMed] [Google Scholar]
- 32.Davies M, Paice EM, Jones SB, Leary S, Curtis AR, West NX. Efficacy of desensitizing dentifrices to occlude dentinal tubules. Eur J Oral Sci. 2011;119:497–503. doi: 10.1111/j.1600-0722.2011.00872.x. [DOI] [PubMed] [Google Scholar]
- 33.Rajguru SA, Padhye AM, Gupta HS. Effects of two desensitizing dentifrices on dentinal tubule occlusion with citric acid challenge: Confocal laser scanning microscopy study. Indian J Dent Res. 2017;28:450–6. doi: 10.4103/ijdr.IJDR_53_17. [DOI] [PubMed] [Google Scholar]