

Abstract
Background
Maternal hypotension is the most frequent complication of spinal anaesthesia for caesarean section. It can be associated with nausea or vomiting and may pose serious risks to the mother (unconsciousness, pulmonary aspiration) and baby (hypoxia, acidosis, neurological injury).
Objectives
To assess the effects of prophylactic interventions for hypotension following spinal anaesthesia for caesarean section.
Search methods
We searched Cochrane Pregnancy and Childbirth's Trials Register (9 August 2016) and reference lists of retrieved studies.
Selection criteria
Randomised controlled trials, including full texts and abstracts, comparing interventions to prevent hypotension with placebo or alternative treatment in women having spinal anaesthesia for caesarean section. We excluded studies if hypotension was not an outcome measure.
Data collection and analysis
Two review authors independently assessed study quality and extracted data from eligible studies. We report 'Summary of findings' tables using GRADE.
Main results
We included 125 studies involving 9469 women. Interventions were to prevent maternal hypotension following spinal anaesthesia only, and we excluded any interventions considered active treatment. All the included studies reported the review's primary outcome. Across 49 comparisons, we identified three intervention groups: intravenous fluids, pharmacological interventions, and physical interventions. Authors reported no serious adverse effects with any of the interventions investigated. Most trials reported hypotension requiring intervention and Apgar score of less than 8 at five minutes as the only outcomes. None of the trials included in the comparisons we describe reported admission to neonatal intensive care unit.
Crystalloid versus control (no fluids)
Fewer women experienced hypotension in the crystalloid group compared with no fluids (average risk ratio (RR) 0.84, 95% confidence interval (CI) 0.72 to 0.98; 370 women; 5 studies; low‐quality evidence). There was no clear difference between groups in numbers of women with nausea and vomiting (average RR 0.19, 95% CI 0.01 to 3.91; 1 study; 69 women; very low‐quality evidence). No baby had an Apgar score of less than 8 at five minutes in either group (60 babies, low‐quality evidence).
Colloid versus crystalloid
Fewer women experienced hypotension in the colloid group compared with the crystalloid group (average RR 0.69, 95% CI 0.58 to 0.81; 2009 women; 27 studies; verylow‐quality evidence). There were no clear differences between groups for maternal hypertension requiring intervention (average RR 0.64, 95% CI 0.09 to 4.46, 3 studies, 327 women; very low‐quality evidence), maternal bradycardia requiring intervention (average RR 0.98, 95% CI 0.54 to 1.78, 5 studies, 413 women; very low‐quality evidence), nausea and/or vomiting (average RR 0.89, 95% CI 0.66 to 1.19, 14 studies, 1058 women, I² = 29%; very low‐quality evidence), neonatal acidosis (average RR 0.83, 95% CI 0.15 to 4.52, 6 studies, 678 babies; very low‐quality evidence), or Apgar score of less than 8 at five minutes (average RR 0.24, 95% CI 0.03 to 2.05, 10 studies, 730 babies; very low‐quality evidence).
Ephedrine versus phenylephrine
There were no clear differences between ephedrine and phenylephrine groups for preventing maternal hypotension (average RR 0.92, 95% CI 0.71 to 1.18; 401 women; 8 studies; very low‐quality evidence) or hypertension (average RR 1.72, 95% CI 0.71 to 4.16, 2 studies, 118 women, low‐quality evidence). Rates of bradycardia were lower in the ephedrine group (average RR 0.37, 95% CI 0.21 to 0.64, 5 studies, 304 women, low‐quality evidence). There was no clear difference in the number of women with nausea and/or vomiting (average RR 0.76, 95% CI 0.39 to 1.49, 4 studies, 204 women, I² = 37%, very low‐quality evidence), or babies with neonatal acidosis (average RR 0.89, 95% CI 0.07 to 12.00, 3 studies, 175 babies, low‐quality evidence). No baby had an Apgar score of less than 8 at five minutes in either group (321 babies; low‐quality evidence).
Ondansetron versus control
Ondansetron administration was more effective than control (placebo saline) for preventing hypotension requiring treatment (average RR 0.67, 95% CI 0.54 to 0.83; 740 women, 8 studies, low‐quality evidence), bradycardia requiring treatment (average RR 0.49, 95% CI 0.28 to 0.87; 740 women, 8 studies, low‐quality evidence), and nausea and/or vomiting (average RR 0.35, 95% CI 0.24 to 0.51; 653 women, 7 studies, low‐quality evidence). There was no clear difference between the groups in rates of neonatal acidosis (average RR 0.48, 95% CI 0.05 to 5.09; 134 babies; 2 studies, low‐quality evidence) or Apgar scores of less than 8 at five minutes (284 babies, low‐quality evidence).
Lower limb compression versus control
Lower limb compression was more effective than control for preventing hypotension (average RR 0.61, 95% CI 0.47 to 0.78, 11 studies, 705 women, I² = 65%, very low‐quality evidence). There was no clear difference between the groups in rates of bradycardia (RR 0.63, 95% CI 0.11 to 3.56, 1 study, 74 women, very low‐quality evidence) or nausea and/or vomiting (average RR 0.42, 95% CI 0.14 to 1.27, 4 studies, 276 women, I² = 32%, very‐low quality evidence). No baby had an Apgar score of less than 8 at five minutes in either group (130 babies, very low‐quality evidence).
Walking versus lying
There was no clear difference between the groups for women with hypotension requiring treatment (RR 0.71, 95% CI 0.41 to 1.21, 1 study, 37 women, very low‐quality evidence).
Many included studies reported little to no information that would allow an assessment of their risk of bias, limiting our ability to draw meaningful conclusions. GRADE assessments of the quality of evidence ranged from very low to low. We downgraded evidence for limitations in study design, imprecision, and indirectness; most studies assessed only women scheduled for elective caesarean sections.
External validity also needs consideration. Readers should question the use of colloids in this context given the serious potential side effects such as allergy and renal failure associated with their administration.
Authors' conclusions
While interventions such as crystalloids, colloids, ephedrine, phenylephrine, ondansetron, or lower leg compression can reduce the incidence of hypotension, none have been shown to eliminate the need to treat maternal hypotension in some women. We cannot draw any conclusions regarding rare adverse effects associated with use of the interventions (for example colloids) due to the relatively small numbers of women studied.
Plain language summary
Techniques for preventing a decrease in blood pressure during spinal anaesthesia for caesarean section
What is the issue?
Spinal anaesthesia is a commonly used technique for caesarean birth as the mother is able to be awake for the birth and usually remains comfortable afterwards. In addition, the technique avoids the risks of general anaesthesia. The most common adverse effect of spinal anaesthesia is a fall in blood pressure (hypotension).
This study reviews the evidence for preventing hypotension following spinal anaesthesia for caesarean birth.
Why is this important?
Hypotension following spinal anaesthesia for caesarean birth occurs frequently. When it occurs, the mother may feel faint or nauseous and may vomit. If her blood pressure falls excessively, the mother runs serious risks (such as loss of consciousness), as does the baby (such as lack of oxygen and brain damage). Hypotension may be prevented by administering intravenous fluids, giving medications (such as ephedrine, phenylephrine, and ondansetron), by leg compression, or by the mother either lying down or walking around before the spinal anaesthesia.
What evidence did we find?
We searched the evidence in August 2016 and found a total of 125 studies involving 9469 women. Included studies investigated 49 different comparisons, which we split into three groups: intravenous fluid therapy, medications, and physical methods. Here we describe the results of the six main comparisons (crystalloid versus control; colloid versus crystalloid; ephedrine versus phenylephrine; ondansetron versus control; leg compression versus control; walking versus lying).
Fluid therapy (crystalloid versus control; colloid versus crystalloid)
It is uncertain whether crystalloids prevent hypotension because the quality of the evidence is very low. Giving colloids instead of crystalloids may mean that fewer women have low blood pressure after having spinal anaesthesia.
We cannot be certain due to the very low quality evidence whether crystalloid or colloid are better at preventing maternal low heart rate (bradycardia), high blood pressure, nausea and vomiting, neonatal acidosis, or low Apgar scores. Whether women received crystalloids or no fluids did not affect the number of women who experienced nausea and/or vomiting.
Medications (ephedrine versus phenylephrine; ondansetron versus control)
Lower rates of bradycardia occurred in women receiving ephedrine versus phenylephrine, and with ondansetron versus no ondansetron, but the evidence is low quality. Ondansetron may prevent low blood pressure and nausea/vomiting but made little or no difference to neonatal acidosis or Apgar scores. There was little difference between ephedrine and phenylephrine for low or high blood pressure, nausea and vomiting, neonatal acidosis, or Apgar scores. We cannot be certain of these results due to the low or very low quality of the evidence.
Physical methods (leg compression versus control; walking versus lying)
It is uncertain whether leg compression reduces the number of women with hypotension compared with no leg compression because the quality of evidence is very low. Similarly, we cannot be certain whether leg compression made any difference to women experiencing bradycardia or nausea and vomiting, or to babies' Apgar scores. It is also uncertain whether walking or lying down before the spinal anaesthesia reduces low blood pressure.
What does this mean?
We found that no single method completely prevents hypotension in women receiving spinal anaesthesia during caesarean birth. Administering intravenous fluids or certain medications, and compressing the legs with bandages, stockings, or inflatable devices may reduce the incidence of hypotension. However, we found the quality of the evidence to be low or very low, so there is still a need for large, high‐quality studies using these clinically relevant interventions, either alone or in combination.
Future research in this setting could focus on combinations of these effective strategies or on new innovative strategies.
Summary of findings
Background
The choice of anaesthesia for caesarean birth is made by balancing women's preferences with the risks and benefits of a particular technique to the mother and her baby (Glosten 2000).
Anaesthesia‐related maternal mortality occurs most frequently when using general anaesthesia for caesarean delivery (Hawkins 1997; Hibbard 1996; Rasmussen 1994). Other risks of general anaesthesia include: failed endotracheal intubation, failed ventilation, aspiration pneumonitis, dental trauma, postoperative nausea and vomiting, delayed breastfeeding, and sedation of the baby (Atlee 1999; Reisner 1999). Regional techniques such as epidural or spinal anaesthesia avoid these risks, allow the mother to be awake at the baby's birth, and may reduce the need for systemic opioid administration postoperatively. Epidural analgesia during labour can be extended to provide surgical anaesthesia should caesarean section be necessary (Lucas 1999). However, a spinal anaesthetic technique has the advantage of simplicity, rapid onset, low failure rate, minimal drug dose, and excellent muscle relaxation during surgery (Glosten 2000). This frequently makes it the anaesthetic technique of choice for both elective and emergency caesarean delivery when a functioning epidural catheter is not in place. Indeed, at least 40% of women having caesarean sections in the USA receive spinal anaesthesia (Hawkins 1997), as do most women undergoing elective caesarean operations in the UK (Husaini 1998; Shibli 2000).
Spinal anaesthesia to the level of T4 is necessary to provide an adequate block for caesarean birth (Glosten 2000; Ousley 2012; Russell 1995). As a consequence, an almost inevitable complete sympathetic block occurs, and decreased venous return to the heart – exacerbated by a degree of inferior vena caval compression – results in hypotension and decreased cardiac output (Rocke 1995). Hypotension during spinal anaesthesia for elective caesarean delivery occurs in as many as 70% to 80% of women receiving pharmacological prophylaxis (Mercier 2013).
Despite all regional techniques being associated with maternal hypotension, the slower onset and lower incidence of this complication during epidural anaesthesia may make the need for prophylactic medications such as ephedrine unnecessary (Glosten 2000; May 1995). In contrast, the frequent occurrence and rapid onset of hypotension during spinal anaesthesia has encouraged anaesthetists to try and prevent or minimise the associated maternal symptoms of vomiting, nausea, and impaired consciousness during the establishment of the block. The concomitant reduction in the utero‐placental blood supply associated with maternal hypotension has deleterious effects such as fetal acidosis (Roberts 1995; Robson 1992), which may result in weak rooting and sucking reflexes of infants (Hollmen 1978); these can severely compromise the establishment of breastfeeding postdelivery (May 1995).
Preventing spinal hypotension appears more likely to decrease the frequency and severity of associated adverse maternal symptoms than treating established hypotension (Datta 1982; Husaini 1998; Kang 1982). Surprisingly few pre‐eclamptic women having caesarean birth under spinal anaesthesia require intervention for hypotension (Clark 2005; Sharwood‐Smith 1999), so routine prophylaxis is probably unnecessary in this particular patient group. Women in established labour who subsequently undergo spinal anaesthesia seem similarly unaffected by hypotension (Lapins 2001).
Description of the condition
Maternal hypotension is the most frequent complication of spinal anaesthesia, with an incidence approaching 100% (Glosten 2000; May 1995). Untreated severe hypotension can pose serious risks to both mother (unconsciousness, pulmonary aspiration, apnoea, or even cardiac arrest) and baby (impaired placental perfusion leading to hypoxia, fetal acidosis, and neurological injury). Although there is some variation, most workers define hypotension as a maternal systolic blood pressure below 70% to 80% of baseline recordings, an absolute value of less than 90 mmHg to 100 mmHg, or both (Glosten 2000).
Description of the intervention
Clinicians currently use a range of strategies including intravenous fluids, pharmacological treatments, and physical interventions to minimise or prevent hypotension. These strategies may include proper maternal position with the uterus displaced off the vena cava, infusion of fluids to increase effective blood volume, and the administration of ephedrine to vasoconstrict the peripheral circulation and increase heart rate (Glosten 2000). Other workers have administered the alpha agonists phenylephrine or metaraminol, which act primarily by vasoconstriction (Alahuhta 1992; Morgan 1994). Physical interventions such as leg wrappings are also used and may act by minimising venous pooling of blood in the legs (Van Bogaert 1998). All these methods aim to maintain blood pressure by increasing venous return to the heart, increasing the resistance of the peripheral circulation, or both. There is, however, no established ideal technique.
How the intervention might work
Health professionals can administer intravenous fluids, including crystalloids and colloids, to increase maternal blood volume, resulting in an increase in venous return, stroke volume, and blood pressure. Intravenous fluid administration prior to spinal anaesthesia for caesarean birth is accepted standard practice (Rout 1993b). The choice of fluid depends on individual and institutional habit, material cost (crystalloid is considerably cheaper), and the perceived relative benefits and risks. Uncommon but potentially serious adverse effects of colloids include anaphylactoid reactions (MIMS 1995), impaired coagulation (Sharma 1999), and the risk of infection such as hepatitis C from human albumin preparations. In addition, some authors have raised concerns regarding prior transmission of bovine spongiform encephalopathy from bovine‐derived pharmaceuticals such as the gelatin Haemaccel (Wickham 1996).
Vasopressors, such as the alpha‐agonist phenylephrine, cause peripheral vasoconstriction and an increase in systemic vascular resistance. This subsequently results in an increase in blood pressure. Combined alpha and beta‐agonists, such as ephedrine, may also prevent hypotension by increasing both heart rate and systemic vascular resistance. Furthermore, anti‐muscarinic agents, such as glycopyrrolate, may be useful to increase heart rate, resulting in a subsequent increase in blood pressure. Possible adverse effects of vasopressors include anaphylaxis, hypertension, and cardiac dysrhythmias (MIMS 1995). Furthermore, there is the potential for impaired utero‐placental perfusion secondary to vasoconstriction (despite maintenance or restoration of maternal blood pressure) with fetal or neonatal consequences as described above.
Physical interventions, such as leg wrapping and calf compression devices, may be helpful in improving venous return and therefore can improve blood pressure. However, these techniques may also have unintentional effects such as localised ischaemia, nerve injury, or unacceptable maternal discomfort.
Why it is important to do this review
Most women will experience hypotension after spinal anaesthesia for caesarean section if they do not receive a preventive intervention. There is no single widely accepted and evidence‐based ideal intervention to prevent maternal hypotension associated with spinal anaesthesia.
Objectives
To assess the effects of prophylactic interventions for hypotension following spinal anaesthesia for caesarean section.
Methods
Criteria for considering studies for this review
Types of studies
All published or unpublished randomised controlled trials that compare an intervention to prevent hypotension with placebo or alternative treatment in women having spinal anaesthesia for caesarean section. We did not include quasi‐randomised, cluster or cross‐over trials in this review update, in a departure from the protocol of the original version. We included abstracts if they reported sufficient information to enable an adequate assessment of methodology and risk of bias.
We excluded studies if hypotension was not an outcome measure or was not clearly defined prior to administering a rescue treatment.
Types of participants
Women having spinal anaesthesia for caesarean section.
Types of interventions
Intravenous fluids
Colloids
Crystalloids
Drugs
Sympathomimetics: ephedrine, metaraminol, phenylephrine
Other medications used to prevent hypotension, for example, ondansetron
Physical methods
Leg bindings
Compression stockings
Other manoeuvres
We did not make comparisons between different anaesthetic techniques since this review question is concerned with preventive techniques in the context of standardised anaesthetic methods. We excluded studies in which women received combined spinal‐epidural anaesthesia or epidural anaesthesia.
Types of outcome measures
Primary outcomes
The incidence of maternal hypotension requiring pharmacological intervention (after intrathecal injection and prior to delivery), where hypotension was a certain decrease in systolic or mean blood pressure, as defined and measured by the authors of included studies (Table 8).
1. Hypotension definitions (mmHg or % fall in systolic/mean arterial pressure).
MAP: mean arterial pressure; SAP: systolic arterial pressure.
We excluded studies if hypotension was not an outcome measure or was not clearly defined prior to administering a rescue treatment.
Secondary outcomes
We considered any maternal or neonatal outcome that could reflect a consequence of the intervention.
Maternal
Hypertension requiring intervention
Cardiac dysrhythmia defined as any rhythm requiring intervention (e.g. bradycardia, tachycardia)
Nausea, vomiting
Anaphylaxis
Impaired consciousness, dizziness
Neonatal
Acidosis as defined by cord or neonatal bloods with a pH of less than 7.2
Apgar scores of less than 7 or 8 at five minutes
Admission to neonatal intensive care unit
The included studies rarely reported these secondary outcomes.
Search methods for identification of studies
The following Methods section of this review is based on a standard template used by Cochrane Pregnancy and Childbirth.
Electronic searches
We searched Cochrane Pregnancy and Childbirth Trials Register by contacting their information specialist (9 August 2016).
The register is a database containing over 22,000 reports of controlled trials in the field of pregnancy and childbirth. For full search methods used to populate Pregnancy and Childbirth’s Trials Register, including the detailed search strategies for CENTRAL, MEDLINE, Embase and CINAHL; the list of handsearched journals and conference proceedings; and the list of journals reviewed via the current awareness service, please follow the link to the editorial information about the Cochrane Pregnancy and Childbirth in the Cochrane Library and select the 'Specialized Register' section from the options on the left side of the screen.
Briefly, Cochrane Pregnancy and Childbirth's Trials Register is maintained by their information specialist and contains trials identified from:
monthly searches of the Cochrane Central Register of Controlled Trials (CENTRAL);
weekly searches of MEDLINE (Ovid);
weekly searches of Embase (Ovid);
monthly searches of CINAHL (EBSCO);
handsearches of 30 journals and the proceedings of major conferences;
weekly current awareness alerts for a further 44 journals plus monthly BioMed Central email alerts.
Two people screen search results, and the full text or abstract (where full text was unavailable) of all relevant trial reports identified is reviewed. Based on the intervention described, each trial report is assigned a number that corresponds to a specific Pregnancy and Childbirth review topic (or topics) and is then added to the register. The information specialist searches the register for each review using this topic number rather than keywords. This results in a more specific search set which has been fully accounted for in the relevant review sections (Included studies; Excluded studies; Studies awaiting classification; Ongoing studies).
Searching other resources
We also retrieved additional relevant references referred to in the reviewed papers to see if they met the criteria for inclusion in this review.
We did not apply any language or date restrictions.
Data collection and analysis
For methods used in the previous version of this review, see Cyna 2006.
For this update, we used the following methods for assessing the reports identified during the updated search.
Selection of studies
Two review authors independently assessed for inclusion all the potential studies we identified as a result of the search strategy. We resolved any disagreement through discussion or, if required, consulted a third author.
We excluded studies for the following reasons.
Hypotension was not an outcome measure or was not clearly defined prior to administering a rescue treatment.
The study did not explicitly report incidence of hypotension.
The report did not mention randomisation.
Randomisation is clearly unsatisfactory.
The spinal anaesthetic technique or dose of local anaesthetic is compared, or varies between participants, and is therefore not controlled.
The studies investigated combined spinal‐epidural anaesthetic technique.
The studied intervention is implemented in response to a fall in blood pressure rather than for prevention (for the purposes of this specific update, review authors felt that the use of automated infusion devices responding to a perceived drop in blood pressure fell into this category, so we excluded these).
Data extraction and management
We designed a form to extract data. For eligible studies, at least two review authors extracted the data using the agreed form. We resolved discrepancies through discussion or, if required, consulted a third person. We entered data into Review Manager 5 software (RevMan 5) and checked for accuracy (RevMan 2014).
When information regarding any of the above was unclear, we attempted to contact authors of the original reports to provide further details.
Assessment of risk of bias in included studies
At least two review authors independently assessed risk of bias for each study using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We resolved any disagreement by discussion or by involving a third assessor.
Random sequence generation (checking for possible selection bias)
We described for each included study the method used to generate the allocation sequence in sufficient detail to allow an assessment of whether it should produce comparable groups.
We assessed the method as being at:
low risk of bias (any truly random process, e.g. random number table, computer random number generator);
high risk of bias (any non‐random process, e.g. odd or even date of birth, hospital or clinic record number);
unclear risk of bias.
Allocation concealment (checking for possible selection bias)
We described for each included study the method used to conceal the allocation sequence and determined whether intervention allocation could have been foreseen in advance of, or during recruitment, or changed after assignment.
We assessed the methods as being at:
low risk of bias (e.g. telephone or central randomisation, consecutively numbered sealed opaque envelopes);
high risk of bias (open random allocation, unsealed or non‐opaque envelopes, alternation, date of birth);
unclear risk of bias.
Blinding of participants and personnel (checking for possible performance bias)
We described for each included study the methods used, if any, to blind study participants and personnel from knowledge of which intervention a participant received. We considered that studies were at low risk of bias if they were blinded or if we judged that the lack of blinding would be unlikely to affect results. We assessed blinding separately for different outcomes or classes of outcomes.
We assessed the methods as being at:
low, high,or unclear risk of bias for participants;
low, high, or unclear risk of bias for personnel.
Blinding of outcome assessment (checking for possible detection bias)
We described for each included study the methods used, if any, to blind outcome assessors from knowledge of which intervention a participant received. We assessed blinding separately for different outcomes or classes of outcomes.
We assessed methods used to blind outcome assessment as being at low, high, or unclear risk of bias.
Incomplete outcome data (checking for possible attrition bias through withdrawals, dropouts, protocol deviations)
We described for each included study, and for each outcome or class of outcomes, the completeness of data including attrition and exclusions from the analysis. We stated whether studies reported attrition and exclusions, the numbers included in the analysis at each stage (compared with the total randomised participants), reasons for attrition or exclusion where reported, and whether missing data were balanced across groups or were related to outcomes. Where trial authors reported or could supply sufficient information, we re‐included missing data in the analyses. We assessed methods as being at:
low risk of bias (e.g. no missing outcome data, missing outcome data balanced across groups);
high risk of bias (e.g. numbers or reasons for missing data imbalanced across groups, 'as treated' analysis done with substantial departure of intervention received from that assigned at randomisation, missing more than 20% of total outcome data collected);
unclear risk of bias.
Selective reporting bias
We described for each included study how we investigated the possibility of selective outcome reporting bias and what we found.
We assessed the methods as being at:
low risk of bias (where it is clear that authors reported all of the study's pre‐specified outcomes and all expected outcomes of interest to the review);
high risk of bias (where authors did not report all the study's pre‐specified outcomes; did not pre‐specify one or more reported primary outcomes; incompletely reported outcomes of interest, rendering them unusable; or failed to include results of a key outcome that would have been expected to have been reported);
unclear risk of bias.
Other sources of bias
We described for each included study any important concerns we had about other possible sources of bias. This may have included concerns regarding specific study design or extreme baseline characteristic imbalance between study groups.
We assessed whether each study was free of other problems that could put it at risk of bias, assessing this domain as being at:
low risk of other bias;
high risk of other bias;
unclear risk of other bias.
Overall risk of bias
We made explicit judgements about whether studies were at high risk of bias according to the criteria given in Higgins 2011. With reference to random sequence generation and other sources of bias, we assessed the likely magnitude and direction of the bias and whether we considered it likely to impact on the findings. We explored the impact of the level of bias through undertaking sensitivity analyses – see Sensitivity analysis.
Measures of treatment effect
Dichotomous data
For dichotomous data, we presented the results as summary risk ratio (RR) with 95% confidence intervals (CI).
Continuous data
This update does not include any continuous data. In future updates, if appropriate, we will use the mean difference for continuous data if trials measure outcomes in the same way. We will use the standardised mean difference to combine trials that measure the same outcome but use different methods.
Unit of analysis issues
Cluster‐randomised trials
Cluster‐randomised trials were not eligible for inclusion in this review.
Cross‐over trials
Cross‐over trials were not were not eligible for inclusion in this review.
Trials with more than two treatment groups
We describe all intervention groups for multi‐intervention studies in the Characteristics of included studies table. Depending on the comparisons investigated in the study, we used the methods for data analysis as detailed in section 16.5.4 of Higgins 2011. We combined groups to create a single pair‐wise comparison, or we split the 'shared' or control group into two or more groups with smaller sample size and included two or more (reasonably independent) comparisons.
Dealing with missing data
For included studies, we noted levels of attrition. We explored the impact of including studies with high levels of missing data in the overall assessment of treatment effect by using sensitivity analysis.
For all outcomes, we carried out analyses, as far as possible, on an intention‐to‐treat basis, that is, we attempted to include all participants randomised to each group in the analyses, and we analysed all participants in the group to which they were allocated, regardless of whether or not they received the allocated intervention. The denominator for each outcome in each trial was the number randomised minus any participants whose outcomes were known to be missing.
Assessment of heterogeneity
We assessed statistical heterogeneity in each meta‐analysis using the Tau², I² and Chi² statistics and used a random‐effects model throughout to account for heterogeneity resulting from the relatively small number of participants in each study (less than 200 participants).
Assessment of reporting biases
If there were 10 or more studies in the meta‐analysis, we investigated reporting biases (such as publication bias) using funnel plots. We assessed funnel plot asymmetry visually. If a visual assessment suggested asymmetry, we discussed possible reasons for this. We only performed this analysis for the primary outcome.
Data synthesis
We carried out statistical analysis using RevMan 2014. We planned to use fixed‐effect meta‐analysis for combining data where it was reasonable to assume that studies were estimating the same underlying treatment effect, that is, where trials examined the same intervention and used sufficiently similar trial populations and methods. However, due to the small number of participants in trials contributing data, we used a random‐effects model throughout this review. We treated the random‐effects summary as the average range of possible treatment effects, and we discussed the clinical implications of treatment effects differing between trials. If the average treatment effect was not clinically meaningful, we did not combine trials.
For the random‐effects analyses, we presented the results as the average treatment effect with its 95% CI along with the estimates of Tau² and I².
Subgroup analysis and investigation of heterogeneity
In exploring heterogeneity when a comparison with three or more trials had an I² of more than 40%, we originally planned to investigate this using subgroup analyses and sensitivity analyses. Due to the small number of participants in each trial, we opted to use random‐effects analysis.
We carried out the following subgroup analyses where possible.
Doses or volume of the intervention given.
Fluid preloading or coloading in addition to the intervention.
We used the outcome of maternal hypotension requiring intervention in subgroup analysis.
We assessed subgroup differences by interaction tests available within RevMan 2014. We reported the results of subgroup analyses, quoting the Chi² statistic and P value, plus the interaction test I² value. We did not perform subgroup analysis where we thought the different regimens or types of the interventions meant that subgroup analysis would not be appropriate or helpful (Analysis 7.1; Analysis 8.1; Analysis 12.1; Analysis 24.1; Analysis 37.1). Instead, we explored the different regimens in separate comparisons.
7.1. Analysis.

Comparison 7: Colloid vs crystalloid, Outcome 1: Women with hypotension requiring intervention
8.1. Analysis.

Comparison 8: Colloid vs control, Outcome 1: Women with hypotension requiring intervention
12.1. Analysis.

Comparison 12: Ephedrine vs control, Outcome 1: Women with hypotension requiring intervention
24.1. Analysis.

Comparison 24: Phenylephrine vs control, Outcome 1: Women with hypotension requiring intervention
37.1. Analysis.

Comparison 37: Lower limb compression vs control, Outcome 1: Women with hypotension requiring intervention
Sensitivity analysis
We performed sensitivity analyses by removing studies in which one or more factors indicated a higher risk of bias than in the rest of studies. We assessed only 2 trials as being at high risk of bias in two or more domains (Calvache 2011; Sutherland 2001), while another 15 were at high risk of bias in one domain (Bhagwanjee 1990; Bottiger 2010; Cardoso 2004a; Carvalho 2009; Cyna 2010; Dahlgren 2005; Dyer 2004; Eldaba 2015; Gulhas 2012; Magalhaes 2009; Mercier 2014; Muzlifah 2009; Pouliou 2006; Romdhani 2014; Ueyama 1999).
Summary of findings tables
For this update, we assessed the quality of the body of evidence using the GRADE approach, as outlined in the GRADE handbook and in relation to the following outcomes for the main comparisons. We chose six key comparisons for a specific focus, as they represent the most clinically relevant comparisons in this updated review.
Comparisons
Crystalloid versus control
Colloid versus crystalloid
Ephedrine versus phenylephrine
Ondansetron versus control
Lower limb compression versus control
Walking versus lying
Outcomes
Incidence of maternal hypotension requiring intervention
Incidence of maternal hypertension requiring intervention
Incidence of maternal bradycardia
Incidence of maternal nausea and/or vomiting
Neonatal acidosis as defined by cord or neonatal bloods with a pH of less than 7.2
Neonatal Apgar score of less than 8 at five minutes
Admission to neonatal intensive care unit
We also prepared a 'Summary of findings' table for the primary outcome (women with hypotension requiring intervention) for all of the six key comparisons for illustrative purposes.
We used the GRADEpro Guideline Development Tool to import data from RevMan 2014 in order to create 'Summary of findings' tables, creating a summary of the intervention effect and a measure of quality for each of the above outcomes. The GRADE approach uses five considerations (study limitations, consistency of effect, imprecision, indirectness and publication bias) to assess the quality of the body of evidence for each outcome. We downgraded the evidence from 'high quality' by one level for serious (or by two levels for very serious) limitations, depending on assessments for risk of bias, indirectness of evidence, serious inconsistency, imprecision of effect estimates or potential publication bias.
Results
Description of studies
For details of included and excluded studies, see Characteristics of included studies and Characteristics of excluded studies tables. Studies took place in Europe, North America, India, and the Middle East.
Results of the search
We assessed 380 studies in total. Our review includes 125 studies involving 9469 women.
In Cyna 2017 we excluded 228 studies; 13 of these were included in Cyna 2006, but we excluded them from the update due to a change in the inclusion criteria (see below for reasons). There are 25 studies awaiting further classification and 1 ongoing study. Since publication of Cyna 2017 one study (Mitra 2014) has been retracted and this has now been reclassified from included to excluded, giving a total of 229 excluded studies.
Included studies
Interventions
We grouped the 125 included trials into three main categories of interventions.
Administration of fluids
Crystalloid versus control (Idehen 2014; Imam 2012; King 1998; Morgan 2000; Ouerghi 2010)
Different regimens of crystalloids (Alimian 2014; Dyer 2004; Farid 2016; Faydaci 2011; Jacob 2012; Jorgensen 2000; Khan 2013; Muzlifah 2009; Oh 2014; Rout 1992; Tercanli 2005; Wilson 1999)
Colloids versus crystalloids (Alimian 2014; Arora 2015; Bottiger 2010; Bouchnak 2012; Cardoso 2004a; Dahlgren 2005; Dahlgren 2007; El‐Mekawy 2012; Embu 2011; French 1999; Gunaydin 2009; Hasan 2012; Jabalameli 2011; Karinen 1995; Lin 1999; Madi‐Jebara 2008; Mercier 2014; Ozkan 2004; Perumal 2004; Romdhani 2014; Selvan 2004; Siddik 2000; Singh 2009; Ueyama 1999; Unlugenc 2015; Upadya 2016; Yorozu 2002)
Different regimens of colloids (Arora 2015; Carvalho 2009; Davies 2006; Nishikawa 2007; Selvan 2004; Siddik‐Sayyid 2009; Ueyama 1999)
Colloid versus control (Hasan 2012; Mathru 1980; Nishikawa 2007; Riley 1995; Tawfik 2014)
Colloid plus crystalloid versus another colloid or crystalloid (Marciniak 2015; Mathru 1980)
Drugs
Ephedrine versus control (Carvalho 1999a; Carvalho 1999b; Carvalho 2000; Damevski 2011; Gomaa 2003; Grubb 2004; Hall 1994; Imam 2012; King 1998; Loughrey 2002; Mathru 1980; Morgan 2000; Moslemi 2015; Ngan Kee 2000; Olsen 1994; Ozkan 2004; Ramin 1994; Singh 2016; Torres unpub; Tsen 2000; Turkoz 2002; Ueyama 1992; Webb 1998)
Ephedrine versus crystalloids (Carvalho 2000; Chan 1997; Damevski 2011; El‐Mekawy 2012; Imam 2012; Jabalameli 2011; King 1998; Kundra 2008; Morgan 2000)
Ephedrine plus crystalloid versus colloid (Ozkan 2004)
Ephedrine plus colloid versus crystalloid (Ozkan 2004)
Ephedrine versus phenylephrine (Alahuhta 1992; Bhardwaj 2013; Gomaa 2003; Hall 1994; Magalhaes 2009; Moslemi 2015; Nazir 2012; Ueyama 2002)
Ephedrine versus angiotensin (Ramin 1994)
Different regimens of ephedrine (Carvalho 1999a; Carvalho 1999b; Carvalho 2000; Chohedri 2007; Hall 1994; King 1998; Loughrey 2002; Morgan 2000; Ngan Kee 2000; Ozkan 2004; Pouliou 2006)
Ephedrine versus colloid (El‐Mekawy 2012; Jabalameli 2011)
Ephedrine versus metaraminol (Bhardwaj 2013)
Phenylephrine versus control (Gomaa 2003; Kuhn 2016; Loughrey 2005; Moslemi 2015; Ngan Kee 2004a)
Different regimens of phenylephrine (Doherty 2012)
Phenylephrine versus mephentermine (Mohta 2010)
Phenylephrine versus metaraminol (Bhardwaj 2013)
Phenylephrine plus crystalloid different regimens (Ansari 2011)
Phenyleprine versus leg compression (Kuhn 2016)
Glycopyrrolate versus control (Ngan Kee 2013a; Ure 1999)
Ondansetron versus control (Marciniak 2015; Nivatpumin 2016; Ortiz‐Gomez 2014; Sahoo 2012; Terkawi 2015; Trabelsi 2015; Wang 2014a; Wang 2014b)
Ondansetron versus ephedrine (Nivatpumin 2016)
Granisetron versus control (Eldaba 2015)
Ketamine versus saline (Gulhas 2012)
Angiotension versus control (Ramin 1994)
Dopamine versus control (Yokoyama 1997)
Physical methods
Lower limb compression versus control (Adsumelli 2003; Bhagwanjee 1990; James 1973; Jorgensen 1996; Kohli 2013; Kuhn 2016; Rout 1993a; Singh 2014; Sood 1996; Sujata 2012; Sutherland 2001)
Wedge versus supine (Calvache 2011)
Head‐up tilt versus horizontal (Loke 2002)
Head‐down tilt versus horizontal (Miyabe 1997)
Crawford's wedge versus manual uterine displacement (Amaro 1998)
Supine versus sitting (Kohler 2002)
Walking versus lying (Cyna 2010)
Lateral versus supine wedged position (Hartley 2001; Hwang 2012)
Left lateral versus left lateral tilt (Rees 2002)
Left lateral tilt versus left manual uterine displacement (Kundra 2007)
Leg elevation versus control (Rout 1993a)
Acupressure versus placebo (Stein 1997)
Acupressure versus metoclopramide (Stein 1997)
Furthermore, we chose to focus on six key comparisons (crystalloid versus control, colloid versus crystalloid, ephedrine versus phenylephrine, ondansetron versus control, lower limb compression versus control, walking versus lying) in the Table 1, as we felt these represented the most important clinical comparisons.
Summary of findings 1. Techniques for preventing hypotension during spinal anaesthesia for caesarean section: key interventions for the primary outcome (women with hypotension requiring intervention).
| Techniques for preventing hypotension during spinal anaesthesia for caesarean section | |||||
|
Patient or population: women having spinal anaesthesia for caesarean section Setting: hospital (inpatient) Outcome: maternal hypotension requiring intervention | |||||
| Comparisons | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with control | Risk with Intervention | ||||
| Crystalloid vs control | Control | Crystalloid | average RR 0.84 (0.72 to 0.98) | 370 (5 RCTs) | ⊕⊕⊝⊝ Lowa,b |
| 535 per 1000 | 449 per 1000 (385 to 524) | ||||
| Colloid vs crystalloid | Crystalloid | Colloid | average RR 0.68 (0.58 to 0.80) | 2105 (28 RCTs) | ⊕⊝⊝⊝ Very lowa,c,d |
| 586 per 1000 | 398 per 1000 (340 to 468) | ||||
| Ephedrine vs phenylephrine | Phenylephrine | Ephedrine | average RR 0.92 (0.71 to 1.18) | 401 (8 RCTs) | ⊕⊝⊝⊝ Very lowa,d,e |
| 465 per 1000 | 428 per 1000 (330 to 549) | ||||
| Ondansetron vs control | Control | Ondansetron | average RR 0.67 (0.54 to 0.83) | 740 (8 RCTs) | ⊕⊕⊝⊝ Lowa,f |
| 579 per 1000 | 388 per 1000 (313 to 481) | ||||
| Lower limb compression vs control | Control | Lower limb compression | average RR 0.61 (0.47 to 0.78) | 705 (11 RCTs) | ⊕⊝⊝⊝ Very lowa,c,d |
| 663 per 1000 | 404 per 1000 (312 to 517) | ||||
| Walking vs lying | Lying | Walking | RR 0.71 (0.41 to 1.21) |
37 (1 RCT) |
⊕⊝⊝⊝ Very lowf,g |
| 706 per 1000 | 501 per 1000 (289 to 854) | ||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio. | |||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | |||||
aInclusion criteria not representative of wider population (e.g. only elective caesarean sections) (−1). bConfidence interval includes potential for benefit or no benefit from the intervention (−1). cDowngraded one level for serious risk of bias (due to unclear risk of selection bias in most included studies (−1). dSubstantial heterogeneity (−1). eInadequate sample size (−1). fParticipants and anaesthetists not blinded in 1 study with 100% weight in analysis (−1). gWide CI that includes potential for benefit or no benefit from the intervention. Small sample size (−2).
Methods and techniques
Although definitions of hypotension in the included studies varied, most fell within the generally accepted range. Table 8 presents details (where trials did not specify systolic or mean arterial pressure, we assumed the definition to be systolic).
Participants
All but one of the included trials assessed women having (or probably having) elective caesarean sections. In Ueyama 1992, 40 women in labour were scheduled for emergency caesareans and 60 women not in labour were scheduled for elective caesareans.
Reviewed interventions were not necessarily applied prior to spinal injection. Clinicians administered pharmacological interventions prior or immediately after spinal injection, before onset of hypotension.
Excluded studies
Please see Characteristics of excluded studies.
Since the Cyna 2017 update was published, the study by Mitra 2014 has been retracted. We have now moved this study from included to excluded.
In Cyna 2017, we excluded 228 studies for the following reasons.
Women received combined spinal epidural anaesthesia.
Women received epidural anaesthesia.
Trials did not report incidence of hypotension requiring intervention.
Researchers did not investigate prevention of hypotension due to spinal anaesthesia (including studies investigating treatment of hypotension or prevention of oxytocin‐induced hypotension)
Authors reporting of data was inadequate for analysis (for example, the number of women in each study group).
Anaesthetic regimen differed between study groups.
Not a prospective randomised study.
Quasi‐randomised study.
Unclear definition of hypotension.
Study compared prevention of hypotension to treatment of hypotension.
Retracted study.
We excluded 13 studies from the original 2006 review for the following reasons (Cyna 2006).
Combined spinal‐epidural (Mendonca 2003; Rucklidge 2002; Rucklidge 2005; Russell 2002; Vercauteren 2000; Yun 1998; Yentis 2000).
Number of women allocated to each study group not reported (Miller 2000).
Incidence of hypotension not reported (Van Bogaert 1998).
Quasi‐randomised (Rout 1993b).
Intervention was to treat, not prevent, hypotension (Cooper 2007; Yadav 2012; Young 1996).
Risk of bias in included studies
Please see Figure 1 and Figure 2 for a summary of 'Risk of bias' assessments.
1.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
2.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Fifty‐one studies reported adequate randomisation sequence generation, so we considered them to be at low risk of selection bias (Alimian 2014; Allen 2010; Arora 2015; Bhardwaj 2013; Bottiger 2010; Calvache 2011; Cardoso 2004a; Carvalho 2009; Cyna 2010; Dahlgren 2007; Das Neves 2010; Doherty 2012; Eldaba 2015; Faydaci 2011; Gulhas 2012; Gunusen 2010; Hwang 2012; Idehen 2014; Jabalameli 2011; Jacob 2012; Jorgensen 1996; Jorgensen 2000; Kohler 2002; Kuhn 2016; Kundra 2007; Loughrey 2002; Magalhaes 2009; Marciniak 2015; Mercier 2014; Moslemi 2015; Muzlifah 2009; Ngan Kee 2004a; Ngan Kee 2013a; Nishikawa 2007; Nivatpumin 2016; Oh 2014; Ortiz‐Gomez 2014; Rees 2002; Romdhani 2014; Sahoo 2012; Siddik‐Sayyid 2009; Singh 2016; Tawfik 2014; Terkawi 2015; Torres unpub; Trabelsi 2015; Ueyama 1999; Unlugenc 2015; Wang 2014a; Wang 2014b; Wilson 1999). The remaining 74 studies reported that the study was randomised; however, authors did not report the method of random sequence generation.
Only 22 studies contained a description of adequate allocation concealment (Bhardwaj 2013; Cyna 2010; Faydaci 2011; French 1999; Hasan 2012; Hwang 2012; King 1998; Kohler 2002; Kuhn 2016; Loughrey 2002; Magalhaes 2009; Marciniak 2015; Ngan Kee 2000; Ngan Kee 2004a; Ngan Kee 2013a; Nivatpumin 2016; Ortiz‐Gomez 2014; Tawfik 2014; Tercanli 2005; Trabelsi 2015; Unlugenc 2015; Wang 2014b), mostly of opaque, sealed envelopes. One hundred and three studies did not report whether allocation was concealed or not, while one study did not conceal allocation at all (Ueyama 1999).
The Characteristics of included studies table includes details of the randomisation and allocation concealment processes.
Blinding
Participants and anaesthetists were blinded in 53 studies (Adsumelli 2003; Alahuhta 1992; Allen 2010; Ansari 2011; Bhardwaj 2013; Dahlgren 2005; Dahlgren 2007; Davies 2006; Doherty 2012; Eldaba 2015; El‐Mekawy 2012; Embu 2011; French 1999; Gomaa 2003; Gulhas 2012; Gunaydin 2009; Hall 1994; Hasan 2012; Hwang 2012; Idehen 2014; Inglis 1995; Karinen 1995; Khan 2013; King 1998; Kuhn 2016; Loughrey 2002; Loughrey 2005; Marciniak 2015; Mercier 2014; Moslemi 2015; Nazir 2012; Ngan Kee 2004a; Ngan Kee 2013a; Nishikawa 2007; Nivatpumin 2016; Oh 2014; Ortiz‐Gomez 2014; Ouerghi 2010; Riley 1995; Siddik 2000; Siddik‐Sayyid 2009; Singh 2014; Singh 2016; Sujata 2012; Tawfik 2014; Terkawi 2015; Trabelsi 2015; Unlugenc 2015; Ure 1999; Wang 2014a; Wang 2014b; Wilson 1998; Wilson 1999). In the remaining studies, blinding was either not performed (8 studies) or not reported (64 studies). We assessed the eight studies in which it was clear that the participants and anaesthetists were not blinded as being at high risk of bias (Bhagwanjee 1990; Calvache 2011; Carvalho 2009; Cyna 2010; Dyer 2004; Pouliou 2006; Romdhani 2014; Sutherland 2001).
The outcome assessors were blinded in 42 studies (Ansari 2011; Bhardwaj 2013; Dahlgren 2007; Das Neves 2010; Davies 2006; Doherty 2012; Eldaba 2015; El‐Mekawy 2012; Embu 2011; French 1999; Gomaa 2003; Gulhas 2012; Gunaydin 2009; Hall 1994; Hasan 2012; Hwang 2012; Idehen 2014; Khan 2013; Kohler 2002; Kuhn 2016; Loke 2002; Loughrey 2005; Marciniak 2015; Mercier 2014; Moslemi 2015; Nazir 2012; Ngan Kee 2013a; Nivatpumin 2016; Oh 2014; Ortiz‐Gomez 2014; Ouerghi 2010; Sahoo 2012; Siddik‐Sayyid 2009; Singh 2014; Singh 2016; Sujata 2012; Tawfik 2014; Terkawi 2015; Trabelsi 2015; Unlugenc 2015; Wang 2014a; Wang 2014b), and they were not blinded in 2 (Magalhaes 2009; Sutherland 2001). The remaining 81 studies did not report blinding of the outcome assessor.
Incomplete outcome data
There were no or only unlikely losses to follow‐up in 70 studies. In 52 studies there was some evidence of incomplete data and small losses to follow‐up, or insufficient information reported to assess this domain adequately (Adsumelli 2003; Alimian 2014; Allen 2010; Amaro 1998; Ansari 2011; Bhagwanjee 1990; Carvalho 1999a; Carvalho 1999b; Davies 2006; Farid 2016; Faydaci 2011; Grubb 2004; Gunusen 2010; Hall 1994; Imam 2012; Inglis 1995; Jacob 2012; James 1973; Jorgensen 1996; Jorgensen 2000; King 1998; Kohli 2013; Lin 1999; Loo 2002; Loughrey 2005; Marciniak 2013; Mathru 1980; Miyabe 1997; Morgan 2000; Ngan Kee 2000; Olsen 1994; Ozkan 2004; Pouliou 2006; Pouta 1996; Riley 1995; Romdhani 2014; Rout 1992; Rout 1993a; Selvan 2004; Siddik 2000; Singh 2009; Sood 1996; Stein 1997; Turkoz 2002; Ueyama 1992; Ueyama 1999; Webb 1998; Wilson 1998; Wilson 1999; Yokoyama 1997; Yorozu 2002). We assessed these studies as being at unclear risk of attrition bias. We considered the remaining four studies to be at high risk of bias due to losses to follow‐up (Bottiger 2010 reported the exclusion of 3 women for unspecified reasons at an unclear point along the study pathway; Eldaba 2015 reported 5/200 exclusions due to failed blocks; Gulhas 2012 excluded 3/105 patients due to failed blocks; Sutherland 2001 reported 46/100 protocol violations).
The Characteristics of included studies table provides reasons for losses to follow‐up.
Selective reporting
Selective reporting was not present in 70 studies (Adsumelli 2003; Alimian 2014; Allen 2010; Amaro 1998; Ansari 2011; Arora 2015; Bhagwanjee 1990; Bhardwaj 2013; Bottiger 2010; Dahlgren 2007; Das Neves 2010; Dyer 2004; Eldaba 2015; El‐Mekawy 2012; Embu 2011; Farid 2016; Faydaci 2011; French 1999; Gomaa 2003; Grubb 2004; Gulhas 2012; Gunaydin 2009; Gunusen 2010; Hall 1994; Hartley 2001; Hasan 2012; Hwang 2012; Idehen 2014; Imam 2012; Inglis 1995; Jabalameli 2011; Jorgensen 2000; Khan 2013; King 1998; Kohler 2002; Kuhn 2016; Loke 2002; Loughrey 2002; Loughrey 2005; Magalhaes 2009; Marciniak 2015; Mercier 2014; Mohta 2010; Moslemi 2015; Nazir 2012; Ngan Kee 2000; Ngan Kee 2004a; Ngan Kee 2013a; Nishikawa 2007; Nivatpumin 2016; Oh 2014; Ortiz‐Gomez 2014; Romdhani 2014; Sahoo 2012; Singh 2014; Singh 2016; Stein 1997; Sujata 2012; Tawfik 2014; Tercanli 2005; Terkawi 2015; Torres unpub; Trabelsi 2015; Tsen 2000; Ueyama 2002; Unlugenc 2015; Upadya 2016; Ure 1999; Wang 2014a; Wang 2014b). It was not clear in a further 51 studies whether selective reporting was present, with the remaining four studies demonstrating evidence of selective reporting (Calvache 2011; Cardoso 2004a; Dahlgren 2005; Muzlifah 2009).
Other potential sources of bias
We found no other potential sources of bias in 84 studies. It was unclear in a further 37 studies whether there was potential source of bias (Ansari 2011; Carvalho 1999a; Carvalho 1999b; Carvalho 2000; Das Neves 2010; Jacob 2012; James 1973; Jorgensen 1996; Kohli 2013; Lin 1999; Magalhaes 2009; Miyabe 1997; Morgan 2000; Nishikawa 2007; Olsen 1994; Ouerghi 2010;; Perumal 2004; Pouliou 2006; Pouta 1996; Ramin 1994; Rees 2002; Riley 1995; Rout 1992; Rout 1993a; Selvan 2004; Siddik 2000; Singh 2009; Singh 2016; Sood 1996; Sutherland 2001; Turkoz 2002; Ueyama 1992; Ueyama 1999; Webb 1998; Wilson 1999; Yokoyama 1997; Yorozu 2002). There was a potential source of bias with respect to funding source in one study: Mercier 2014 performed a study comparing colloid (HES) preload to crystalloid (Ringer's lactate) preload, which was fully funded by Fresenius Kabi, the company that produces HES. We assessed this study as being at high risk of other bias. Some evidence of asymmetry is apparent in two of the three funnel plots (Figure 3, Figure 4 and Figure 5), which suggests possible publication bias due to the number of small studies.
3.

Funnel plot of comparison: 7 Colloid vs crystalloid, outcome: 7.1 Women with hypotension requiring intervention.
4.

Funnel plot of comparison: 13 Ephedrine vs control, outcome: 13.1 Women with hypotension requiring intervention.
5.

Funnel plot of comparison: 47 Lower limb compression vs control, outcome: 47.1 Women with hypotension requiring intervention.
There were 2 studies assessed as high risk as study participants received variable doses of local anaesthetic in their spinal block (Alahuhta 1992; Mathru 1980). Also, there were 2 studies assessed as high risk of bias as it was unclear whether the spinal anaesthetic technique and dose was standardised between the study groups (Ozkan 2004; Wilson 1998). It was unlikely that with randomisation this source of bias would have an important effect on the review findings.
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4; Table 5; Table 6; Table 7
Summary of findings 2. Crystalloid versus control.
| Crystalloid versus control for preventing hypotension during spinal anaesthesia for caesarean section | |||||
| Patient or population: women having spinal anaesthesia for caesarean section Setting: hospital settings in Europe, North America, India, and the Middle East Intervention: crystalloid Comparison: control | |||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with control | Risk with crystalloid | ||||
| Maternal hypotension requiring intervention | Study population | RR 0.84 (0.72 to 0.98) | 370 (5 RCTs) | ⊕⊕⊝⊝ Lowa,b | |
| 535 per 1000 | 449 per 1000 (385 to 524) | ||||
| Maternal hypertension requiring intervention | No studies reported this outcome. | ||||
| Maternal bradycardia requiring intervention | No studies reported this outcome. | ||||
| Maternal nausea and/or vomiting | Study population | RR 0.19 (0.01 to 3.91) | 69 (1 RCT) |
⊕⊝⊝⊝ Very lowa,c |
|
| 59 per 1000 | 11 per 1000 (1 to 230) |
||||
| Neonatal acidosis as defined by cord or neonatal blood with a pH < 7.2 | No studies reported this outcome. | ||||
| Neonatal Apgar score < 8 at 5 minutes | Study population | Not estimable | 60 (1 RCT) | ⊕⊕⊝⊝ Lowa,d | |
| 0 per 1000 | 0 per 1000 (0 to 0) | ||||
| Admission to neonatal intensive care unit | No studies reported this outcome. | ||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio. | |||||
|
GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | |||||
aOnly elective caesarean sections included (−1). bSmall sample size and CI includes potential for benefit or no benefit from the intervention (−1). cOne study with small sample size, few events, and wide confidence intervals that cross the line of no effect (−2). dNo events and small sample size (−1).
Summary of findings 3. Colloid versus crystalloid.
| Colloid versus crystalloid for preventing hypotension during spinal anaesthesia for caesarean section | |||||
| Patient or population: women having spinal anaesthesia for caesarean section Setting: hospital settings in Europe, North America, India, and the Middle East Intervention: colloid Comparison: crystalloid | |||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with crystalloid | Risk with colloid | ||||
| Maternal hypotension requiring intervention | Study population | RR 0.69 (0.58 to 0.81) | 2009 (27 RCTs) | ⊕⊝⊝⊝ Very lowa,b,c | |
| 595 per 1000 | 411 per 1000 (345 to 484) | ||||
| Maternal hypertension requiring intervention | Study population | RR 0.64 (0.09 to 4.46) | 327 (3 RCTs) | ⊕⊝⊝⊝ Very lowc,d,e | |
| 55 per 1000 | 35 per 1000 (5 to 246) | ||||
| Maternal bradycardia requiring intervention | Study population | RR 0.98 (0.54 to 1.78) | 413 (5 RCTs) | ⊕⊝⊝⊝ Very lowc,d,e | |
| 87 per 1000 | 86 per 1000 (47 to 156) | ||||
| Maternal nausea and/or vomiting | Study population | RR 0.89 (0.66 to 1.19) | 1058 (14 RCTs) | ⊕⊝⊝⊝ Very lowa,b,c,d,e | |
| 230 per 1000 | 205 per 1000 (152 to 274) | ||||
| Neonatal acidosis as defined by cord or neonatal blood with a pH < 7.2 | Study population | RR 0.83 (0.15 to 4.52) | 678 (6 RCTs) | ⊕⊝⊝⊝ Very lowc,d,e | |
| 26 per 1000 | 21 per 1000 (4 to 116) | ||||
| Neonatal Apgar score < 8 at 5 minutes | Study population | RR 0.24 (0.03 to 2.05) | 730 (10 RCTs) | ⊕⊝⊝⊝ Very lowc,d,e,f | |
| 10 per 1000 | 3 per 1000 (0 to 22) | ||||
| Admission to neonatal intensive care unit | No studies reported this outcome. | ||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio. | |||||
|
GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | |||||
aDowngraded one level for serious risk of bias (due to unclear risk of selection bias in most included studies) (−1). bSubstantial heterogeneity (−1). cInclusion criteria not representative of wider population (e.g. elective caesarean section only) (−1). dWide CI (−1). eInadequate sample size (−1). fMultiple studies did not report method of randomisation (−1).
Summary of findings 4. Ephedrine versus phenylephrine.
| Ephedrine versus phenylephrine for preventing hypotension during spinal anaesthesia for caesarean section | ||||||
| Patient or population: women having spinal anaesthesia for caesarean section Setting: hospital setting in Europe, North America, India, and the Middle East Intervention: ephedrine Comparison: phenylephrine | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with phenylephrine | Risk with ephedrine | |||||
| Maternal hypotension requiring intervention | Study population | RR 0.92 (0.71 to 1.18) | 401 (8 RCTs) | ⊕⊝⊝⊝ Very lowa,b,c | — | |
| 465 per 1000 | 428 per 1000 (330 to 549) | |||||
| Maternal hypertension requiring intervention | Study population | RR 1.72 (0.71 to 4.16) | 118 (2 RCT) | ⊕⊕⊝⊝ Lowb,d | — | |
| 113 per 1000 | 194 per 1000 (80 to 470) | |||||
| Maternal bradycardia requiring intervention | Study population | RR 0.37 (0.21 to 0.64) | 304 (5 RCTs) | ⊕⊕⊝⊝ Lowb,c | — | |
| 243 per 1000 | 90 per 1000 (51 to 156) | |||||
| Maternal nausea and/or vomiting | Study population | RR 0.76 (0.39 to 1.49) | 204 (4 RCTs) | ⊕⊝⊝⊝ Very lowa,b,e | — | |
| 216 per 1000 | 164 per 1000 (84 to 321) | |||||
| Neonatal acidosis as defined by cord or neonatal blood with a pH < 7.2 | Study population | RR 0.89 (0.07 to 12.00) | 175 (3 RCTs) | ⊕⊕⊝⊝ Lowb,f | — | |
| 11 per 1000 | 10 per 1000 (1 to 133) | |||||
| Neonatal Apgar score < 8 at 5 minutes | Study population | Not estimable | 321 (6 RCTs) | ⊕⊕⊝⊝ Lowb,c | No events observed in any studies. Relative effect could not be estimated. | |
| Not pooled | Not pooled | |||||
| Admission to neonatal intensive care unit | No studies reported this outcome. | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio. | ||||||
|
GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
aSubstantial heterogeneity (−1). bInclusion criteria not representative of wide population (e.g. elective caesarean section only) (−1). cInadequate sample size (−1). dSample size inadequate and wide CI (−1). eWide CI (−1). fCI includes potential for ephedrine to cause either increased or decreased incidence of outcome compared to phenylephrine (−1).
Summary of findings 5. Ondansetron versus control.
| Ondansetron versus saline placebo for preventing hypotension during spinal anaesthesia for caesarean section | |||||
| Patient or population: women having spinal anaesthesia for caesarean section Setting: hospital setting in Europe, North America, India, and the Middle East Intervention: ondansetron Comparison: saline placebo | |||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with control | Risk with ondansetron | ||||
| Maternal hypotension requiring intervention | Study population | RR 0.67 (0.54 to 0.83) | 740 (8 RCTs) | ⊕⊕⊝⊝ Lowa,b | |
| 579 per 1000 | 388 per 1000 (313 to 481) | ||||
| Maternal hypertension requiring intervention | No studies reported this outcome. | ||||
| Maternal bradycardia requiring intervention | Study population | RR 0.49 (0.28 to 0.87) | 740 (8 RCTs) | ⊕⊕⊝⊝ Lowa,b | |
| 100 per 1000 | 49 per 1000 (28 to 87) | ||||
| Maternal nausea and/or vomiting | Study population | RR 0.35 (0.24 to 0.51) | 653 (7 RCTs) | ⊕⊕⊝⊝ Lowa,b | |
| 296 per 1000 | 103 per 1000 (71 to 151) | ||||
| Neonatal Apgar score < 8 at 5 minutes | Study population | Not estimable | 284 (3 RCTs) | ⊕⊕⊝⊝ Lowa,b | |
| Not pooled | Not pooled | ||||
| Neonatal acidosis as defined by cord or neonatal blood with a pH < 7.2 | Study population | RR 0.48 (0.05 to 5.09) | 134 (2 RCT) | ⊕⊕⊝⊝ Lowa,b | |
| 30 per 1000 | 15 per 1000 (2 to 154) | ||||
| Admission to neonatal care unit | No studies reported this outcome. | ||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio. | |||||
|
GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | |||||
a Inclusion criteria not representative of wider population (e.g. elective caesarean section only) (−1). b Inadequate sample size (−1).
Summary of findings 6. Lower limb compression versus control.
| Leg compression versus control for preventing hypotension during spinal anaesthesia for caesarean section | ||||||
| Patient or population: women having spinal anaesthesia for caesarean section Setting: hospital setting in Europe, North America, India, and the Middle East Intervention: lower limb compression Comparison: control | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with control | Risk with lower limb compression | |||||
| Maternal hypotension requiring intervention | Study population | RR 0.61 (0.47 to 0.78) | 705 (11 RCTs) | ⊕⊝⊝⊝ Very lowa,b,c | — | |
| 663 per 1000 | 404 per 1000 (312 to 517) | |||||
| Maternal hypertension requiring intervention | No studies reported this outcome. | |||||
| Maternal bradycardia requiring intervention | Study population | RR 0.63 (0.11 to 3.56) | 74 (1 RCTs) |
⊕⊝⊝⊝ Very lowc,d,e | — | |
| 83 per 1000 | 53 per 1000 (9 to 297) | |||||
| Maternal nausea and/or vomiting | Study population | RR 0.42 (0.14 to 1.27) | 276 (4 RCTs) | ⊕⊝⊝⊝ Very lowa,b,c,d | — | |
| 162 per 1000 | 68 per 1000 (23 to 205) | |||||
| Neonatal acidosis as defined by cord or neonatal blood with a pH < 7.2 | No studies reported this outcome. | |||||
| Neonatal Apgar score < 8 at 5 minutes | Study population | Not estimable | 130 (3 RCTs) | ⊕⊝⊝⊝ Very lowa,c,e | No events observed in any studies. Relative effect could not be estimated. | |
| Not pooled | Not pooled | |||||
| Admission to neonatal intensive care unit | No studies reported this outcome. | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio. | ||||||
|
GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
aDowngraded one level for serious risk of bias (due to unclear risk of selection bias in the majority of included studies (−1). bSubstantial heterogeneity (−1). cInclusion criteria not representative of wider population (e.g. elective caesarean sections only) (−1). dWide CI that includes potential benefit or no benefit from the intervention (−1). eInadequate sample size (−1).
Summary of findings 7. Walking versus lying.
| Walking versus lying for reducing risk of maternal hypotension during spinal anaesthesia for caesarean section | |||||
| Patient or population: women having spinal anaesthesia for caesarean section Setting: hospital setting in Australia Intervention: walking Comparison: lying | |||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with lying | Risk with walking | ||||
| Maternal hypotension requiring intervention | Study population | RR 0.71 (0.41 to 1.21) | 37 (1 RCT) | ⊕⊝⊝⊝ Very lowa,b | |
| 706 per 1000 | 501 per 1000 (289 to 854) | ||||
| Maternal hypertension requiring intervention | No studies reported this outcome. | ||||
| Maternal bradycardia requiring intervention | No studies reported this outcome. | ||||
| Maternal nausea and/or vomiting | No studies reported this outcome. | ||||
| Neonatal acidosis as defined by cord or neonatal blood with a pH < 7.2 | No studies reported this outcome. | ||||
| Neonal Apgar score < 8 at 5 minutes | No studies reported this outcome. | ||||
| Admission to neonatal intensive care unit | No studies reported this outcome. | ||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio. | |||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | |||||
aParticipants and anaesthetists not blinded in 1 study with 100% weight in analysis (−1). bWide CI that includes potential for benefit or no benefit from the intervention. Small sample size (−2).
We included 125 studies involving 9469 women and assessing 49 comparisons of different methods to prevent hypotension following spinal anaesthesia at caesarean.
As noted above, we grouped the comparisons into three main categories of interventions: fluids (data and analyses 1 to 11), drugs (data and analyses 12 to 36), and physical methods (data and analyses 37 to 49). Comparisons 1, 7, 16, 31, 37, and 43 constitute our key review comparisons; see Table 1 for a summary of the findings of each for our main review outcome: maternal hypotension requiring pharmacological intervention.
Fluids
This group of interventions comprises comparisons corresponding to data analyses 1 to 11. The section first presents comparisons with crystalloids, including crystalloid versus control (comparison 1; see Table 2), different regimens of crystalloids, and different types of crystalloids. Comparison 7 assesses colloid versus crystalloid directly (see Table 3), while the remaining comparisons focus on colloids alone (versus control: different regimens of colloids: and different types of colloids).
Crystalloids
Crystalloid versus control
See Table 2.
Primary outcome: maternal hypotension requiring pharmacological intervention
Crystalloids appeared to be more effective than control for preventing maternal hypotension requiring intervention (average RR 0.84, 95% CI 0.72 to 0.98; 5 studies; 370 women; low‐quality evidence; Analysis 1.1).
1.1. Analysis.

Comparison 1: Crystalloid vs control, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups (RR 0.19, 95% CI 0.01 to 3.91; 1 study; 69 women; very low‐quality evidence; Analysis 1.2).
1.2. Analysis.

Comparison 1: Crystalloid vs control, Outcome 2: Nausea and/or vomiting
Anaphylaxis
One study reported this outcome (Idehen 2014, 69 women). There were no events in either group (Analysis 1.3).
1.3. Analysis.

Comparison 1: Crystalloid vs control, Outcome 3: Anaphylaxis
Neonatal
Apgar scores of less than 7 or 8 at five minutes
One study reported this outcome (Idehen 2014, 60 babies; low‐quality evidence). There were no events in either group (Analysis 1.4).
1.4. Analysis.

Comparison 1: Crystalloid vs control, Outcome 4: Apgar < 8 at 5 min
No trials reported other secondary outcomes for this comparison.
Different regimens of crystalloids
Crystalloid: rapid infusion versus slow infusion
Primary outcome: maternal hypotension requiring pharmacological intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 0.86, 95% CI 0.45 to 1.64; 1 study, 20 women; Analysis 2.1).
2.1. Analysis.

Comparison 2: Crystalloid: rapid infusion vs slow infusion, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
No trials reported secondary outcomes for this comparison.
Crystalloid: high versus low preload volume
Primary outcome: maternal hypotension requiring pharmacological intervention
There was no conclusive evidence of a difference between the groups in rates of hypotension when comparing high volume preload (15 mL/kg to 20 mL/kg) to lower volume preload (10 mL/kg or less) (average RR 0.55, 95% CI 0.29 to 1.02; I² = 57%, 3 studies, 192 women; Analysis 3.1). There was considerable heterogeneity in the 20 mL subgroup (I² = 85%) but no evidence of subgroup differences (test for subgroup differences: Chi² = 0.01, df = 1 (P = 0.92), I² = 0%).
3.1. Analysis.

Comparison 3: Crystalloid: high vs low preload volume, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups (RR 1.20, 95% CI 0.40 to 3.62, one study, 80 women; Analysis 3.2).
3.2. Analysis.

Comparison 3: Crystalloid: high vs low preload volume, Outcome 2: Nausea and/or vomiting
Neonatal
Apgar scores of less than 7 or 8 at five minutes
One study reported this outcome (Faydaci 2011, 90 babies). There were no events in either group (Analysis 3.3).
3.3. Analysis.

Comparison 3: Crystalloid: high vs low preload volume, Outcome 3: Apgar < 8 at 5 min
No trials reported other secondary outcomes for this comparison.
Sensitivity analysis
Removing Muzlifah 2009 from Analysis 3.1 resulted in fewer women in the high volume preloading group experiencing hypotension than in the low volume group (average RR 0.43, 95% CI 0.23 to 0.78); data not shown.
Crystalloid: rapid coload versus preload
Primary outcome: maternal hypotension requiring pharmacological intervention
A rapid crystalloid coload was associated with a lower incidence of hypotension than a preload (average RR 0.70, 95% CI 0.59 to 0.83, 5 studies, 384 women; Analysis 4.1).
4.1. Analysis.

Comparison 4: Crystalloid: rapid coload vs preload, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Hypertension requiring intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 1.67, 95% CI 0.42 to 6.60, 1 study, 100 women; Analysis 4.2).
4.2. Analysis.

Comparison 4: Crystalloid: rapid coload vs preload, Outcome 2: Hypertension requiring intervention
Cardiac dysrhythmia
There was insufficient evidence to determine whether there was a difference between the groups in rates of bradycardia (RR 1.43, 95% CI 0.59 to 3.45, 1 study, 100 women; Analysis 4.3).
4.3. Analysis.

Comparison 4: Crystalloid: rapid coload vs preload, Outcome 3: Women with bradycardia
Nausea and/or vomiting
Rapid coload was associated with a higher risk of nausea than preload (average RR 1.98, 95% CI 1.26 to 3.12, 3 studies, 201 women; Analysis 4.4).
4.4. Analysis.

Comparison 4: Crystalloid: rapid coload vs preload, Outcome 4: Women with nausea or vomiting
There was insufficient evidence to determine conclusively whether there was a difference between the groups in rates of vomiting (average RR 2.33, 95% CI 0.98 to 5.58, 2 studies, 160 women).
Neonatal
Acidosis
Two studies reported this outcome (Dyer 2004; Oh 2014, 110 babies). There were no events in either group (Analysis 4.5).
4.5. Analysis.

Comparison 4: Crystalloid: rapid coload vs preload, Outcome 5: Neonates with acidosis (pH < 7.2)
Apgar scores of less than 7 or 8 at five minutes
Three studies reported this outcome (Dyer 2004; Jacob 2012; Oh 2014, 210 babies). There were no events in either group (Analysis 4.6).
4.6. Analysis.

Comparison 4: Crystalloid: rapid coload vs preload, Outcome 6: Apgar < 8 at 5 min
No trials reported other secondary outcomes for this comparison.
Sensitivity analysis
Removing Dyer 2004 from the analysis did not impact the results.
Crystalloid: warm versus cold saline
Primary outcome: maternal hypotension requiring pharmacological intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 1.03, 95% CI 0.65 to 1.62, one study,113 women; Analysis 5.1).
5.1. Analysis.

Comparison 5: Crystalloid: warm vs cold, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Nausea and/or vomiting
There was insufficient evidence to determine whether warm or cold saline had an effect on nausea (RR 1.64, 95% CI 0.97 to 2.76, one study, 113 women) or vomiting (RR 2.95, 95% CI 0.12 to 70.87, one study, 113 women); see Analysis 5.2.
5.2. Analysis.

Comparison 5: Crystalloid: warm vs cold, Outcome 2: Women with nausea and/or vomiting
No trials reported other secondary outcomes for this comparison.
Different types of crystalloids
Dextrose plus saline versus saline alone
Primary outcome: maternal hypotension requiring pharmacological intervention
There was no clear evidence of a difference between the interventions (RR 0.88, 95% CI 0.68 to 1.14, 1 study, 120 women; Analysis 6.1.1).
6.1. Analysis.

Comparison 6: Crystalloid vs another crystalloid, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Neonatal
Acidosis
There was insufficient evidence to determine whether there was a difference between the groups (RR 1.20, 95% CI 0.39 to 3.72, 1 study, 120 babies; Analysis 6.3).
6.3. Analysis.

Comparison 6: Crystalloid vs another crystalloid, Outcome 3: Neonates with acidosis: dextrose vs saline
Apgar scores of less than 7 at five minutes
One study reported this outcome (Wilson 1999, 120 babies). There were no events in either group (Analysis 6.4).
6.4. Analysis.

Comparison 6: Crystalloid vs another crystalloid, Outcome 4: Neonates with Apgar score < 7 at 5 min
No trials reported other secondary outcomes for this comparison.
Glucose versus saline
Primary outcome: maternal hypotension requiring pharmacological intervention
There was no clear evidence of a difference between the interventions (RR 1.05, 95% CI 0.74 to 1.48, 1 study, 70 women; Analysis 6.1.2).
Secondary outcomes
No studies reported secondary outcomes for this comparison.
Ringers lactate versus saline
Primary outcome: maternal hypotension requiring pharmacological intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 1.17, 95% CI 0.65 to 2.09, 1 study, 60 women; Analysis 6.1.3).
Secondary outcomes
Neonatal
Acidosis
One study reported this outcome (Alimian 2014, 60 babies). There were no events in either group (Analysis 6.2).
6.2. Analysis.

Comparison 6: Crystalloid vs another crystalloid, Outcome 2: Neonates with acidosis: Ringer's lactate vs saline
Apgar scores of less than 8 at five minutes
One study reported this outcome (Alimian 2014, 60 babies). There were no events in either group (Analysis 6.5).
6.5. Analysis.

Comparison 6: Crystalloid vs another crystalloid, Outcome 5: Neonates with Apgar score < 8 at 5 min
No trials reported other secondary outcomes for this comparison.
Colloids versus crystalloids
See Table 3.
Primary outcome: maternal hypotension requiring pharmacological intervention
The incidence of hypotension was lower with colloids compared to crystalloids (average RR 0.69, 95% CI 0.58 to 0.81; 27 studies, 2009 women; very low‐quality evidence; Analysis 7.1). Substantial heterogeneity (I² = 82%, Tau² = 0.12) was likely due to differences in formulation and volume of fluid administered between studies. However, due to the variation in regimens between studies, it was not possible to conduct formal subgroup analyses. There was some evidence of asymmetry on funnel plot (Figure 3), which could be due to the large number of small studies contributing to this analysis.
Secondary outcomes
Maternal
Hypertension requiring intervention
There was insufficient evidence to determine whether there was a difference between the groups (average RR 0.64, 95% CI 0.09 to 4.46, 3 studies, 327 women; very low‐quality evidence; Analysis 7.2).
7.2. Analysis.

Comparison 7: Colloid vs crystalloid, Outcome 2: Women with hypertension requiring intervention
Cardiac dysrhythmia
There was no clear evidence of a difference in the groups in rates of tachycardia (RR 1.10, 95% CI 0.79, 1.53, 1 study, 60 women) or bradycardia (RR 0.98, 95% CI 0.54 to 1.78, 5 studies, 413 women; very low‐quality evidence); see Analysis 7.3.
7.3. Analysis.

Comparison 7: Colloid vs crystalloid, Outcome 3: Women with cardiac dysrhythmia
Nausea and/or vomiting
There was no clear evidence of a difference in the groups for rates of nausea or vomiting (average RR 0.89, 95% CI 0.66 to 1.19, 14 studies, 1058 women, I² = 29%; very low‐quality evidence), nausea alone (average RR 1.10, 95% CI 0.77 to 1.58, 5 studies, 390 women, I² = 10%), vomiting alone (average RR 1.35, 95% CI 0.55 to 3.27, 4 studies, 320 women, I² = 33%); see Analysis 7.4.
7.4. Analysis.

Comparison 7: Colloid vs crystalloid, Outcome 4: Women with nausea and/or vomiting
Neonatal
Acidosis
There was insufficient evidence to determine whether there was a difference between the groups (average RR 0.83, 95% CI 0.15 to 4.52, 6 studies, 678 babies, I² = 24%; very low‐quality evidence; Analysis 7.5).
7.5. Analysis.

Comparison 7: Colloid vs crystalloid, Outcome 5: Neonates with acidosis (pH < 7.2)
Apgar scores of less than 7 or 8 at five minutes
There was insufficient evidence to determine whether there was a difference between the groups in the rates of Apgar scores of less than 7 (average RR 0.16, 95% CI 0.01 to 2.90, 2 studies,127 babies) or of less than 8 (average RR 0.24, 95% CI 0.03 to 2.05, 10 studies, 730 babies; very low‐quality evidence) at five minutes; see Analysis 7.6.
7.6. Analysis.

Comparison 7: Colloid vs crystalloid, Outcome 6: Neonates: Apgar score
No trials reported other secondary outcomes for this comparison.
Sensitivity analysis
Removing studies for at high risk of bias in one or more domain made little difference to the results of any analysis under this comparison (Bottiger 2010; Cardoso 2004a; Dahlgren 2005; Mercier 2014; Romdhani 2014; Ueyama 1999).
Colloids versus control
Primary outcome: maternal hypotension requiring pharmacological intervention
There was a reduced incidence of hypotension in the colloid group (average RR 0.40, 95% CI 0.16 to 0.96, 5 studies, 426 women; Analysis 8.1). There was substantial heterogeneity (I² = 85%, Tau² = 0.71), likely due to differences in formulation and volume of fluid administered. In addition, Tawfik 2014 reported higher event rates than other studies.
Secondary outcomes
Maternal
Cardiac dysrhythmia
There was insufficient evidence to determine whether there was a difference between the groups (RR 7.70, 95% CI 0.46 to 127.78; 54 women; 1 study; Analysis 8.2).
8.2. Analysis.

Comparison 8: Colloid vs control, Outcome 2: Women with bradycardia
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups (average RR 1.65, 95% CI 0.75 to 3.64, 2 studies, 245 women; Analysis 8.3).
8.3. Analysis.

Comparison 8: Colloid vs control, Outcome 3: Women with nausea and/or vomiting
Neonatal
Acidosis
There was insufficient evidence to determine whether there was a difference between the groups (RR 1.24, 95% CI 0.34 to 4.48, 1 study, 205 babies; Analysis 8.4).
8.4. Analysis.

Comparison 8: Colloid vs control, Outcome 4: Neonates with acidosis (pH < 7.2)
Apgar scores of less than 7 or 8 at five minutes
There was insufficient evidence to determine whether there was a difference between the groups in Apgar scores of less than 7 at five minutes (average RR 0.07, 95% CI 0.00 to 1.24, 4 studies, 205 babies; Analysis 8.5). Three of the four studies in this analysis reported no events in either arm. One study reported Apgar score of less than 8 at five minutes (Tawfik 2014, 205 women), and there were no events in either arm (Analysis 8.6).
8.5. Analysis.

Comparison 8: Colloid vs control, Outcome 5: Neonates with Apgar score < 7 at 5 min
8.6. Analysis.

Comparison 8: Colloid vs control, Outcome 6: Neonatal Apgar < 8 at 5 min
No trials reported other secondary outcomes for this comparison.
Different regimens of colloids
Colloids: high versus low volume
Primary outcome: maternal hypotension requiring pharmacological intervention
In three studies, there was no difference in the incidence of hypotension when comparing high volume versus low volume colloids (average RR 0.75, 95% CI 0.27 to 2.08; 134 women; Analysis 9.1). Substantial heterogeneity (I² = 78, Tau² = 0.63) was present. None of the studies contributing to the analysis were good quality, and all were at unclear or high risk of selection bias, which may have impacted results (Davies 2006; Selvan 2004; Ueyama 1999).
9.1. Analysis.

Comparison 9: Colloid: different volumes, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Neonatal
Apgar of less than 9 at five minutes (non‐prespecified outcome)
One study reported this outcome (Davies 2006, 70 babies). There were no events in either arm (Analysis 9.2).
9.2. Analysis.

Comparison 9: Colloid: different volumes, Outcome 2: Apgar < 9 at 5 min
No trials reported other secondary outcomes for this comparison.
Colloid: preload versus coload
Note: the comparison for crystalloid is coload versus preload.
Primary outcome: maternal hypotension requiring pharmacological intervention
There was no clear evidence of a difference between the groups (average RR 0.93, 95% CI 0.78 to 1.10, 4 studies, 320 women; Analysis 10.1).
10.1. Analysis.

Comparison 10: Colloid preload vs colloid coload, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Cardiac dysrhythmia
There was insufficient evidence to determine whether there was a difference between the groups in rates of bradycardia (average RR 0.75, 95% CI 0.20 to 2.88, 2 studies, 82 women; Analysis 10.2. One study had no events). One study reported tachycardia (Carvalho 2009, 46 women); there were no events in either arm (Analysis 10.2).
10.2. Analysis.

Comparison 10: Colloid preload vs colloid coload, Outcome 2: Women with cardiac dysrhythmia
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups in rates of nausea or vomiting (RR 0.92, 95% CI 0.63 to 1.35, 1 study, 178 women), rates of nausea alone (RR 1.00, 95% CI 0.15 to 6.51, 1 study, 46 women). One study reported rates of vomiting alone (Carvalho 2009, 46 women); there were no events in either arm (Analysis 10.3).
10.3. Analysis.

Comparison 10: Colloid preload vs colloid coload, Outcome 3: Women with nausea and/or vomiting
Anaphylaxis
One study reported this outcome (Siddik‐Sayyid 2009, 178 women). There were no events in either group (Analysis 10.4).
10.4. Analysis.

Comparison 10: Colloid preload vs colloid coload, Outcome 4: Women with anaphylaxis
Neonatal
Apgar scores of less than 7 or 8 at five minutes
One study reported this outcome (Nishikawa 2007, 36 babies): there were no events in either arm (Analysis 10.5).
10.5. Analysis.

Comparison 10: Colloid preload vs colloid coload, Outcome 5: Neonates with Apgar score < 7 at 5 min
No trials reported other secondary outcomes for this comparison.
Sensitivity analysis
Removing Carvalho 2009 made very little difference to Analysis 10.1 and Analysis 10.2.
Different types of colloids
Two studies compared colloid + crystalloid versus another colloid or dextrose + crystalloid (Marciniak 2015; Mathru 1980)
Albumen and dextrose plus crystalloid versus dextrose plus crystalloid
Primary outcome: maternal hypotension requiring pharmacological intervention
One study compared colloid plus crystalloid versus another colloid or dextrose plus crystalloid (Mathru 1980).There was insufficient evidence to determine whether there was a difference between the groups (RR 0.13, 95% CI 0.01 to 2.30, 1 study, 45 women; Analysis 11.1.1).
11.1. Analysis.

Comparison 11: Colloid + crystalloid vs another colloid + crystalloid, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Neonatal
Apgar scores of less than 7 at five minutes
There was insufficient evidence to determine whether there was a difference between the groups for Apgar scores of less than 7 (RR 0.13, 95% CI 0.01 to 2.30, 1 study, 45 babies; Analysis 11.2).
11.2. Analysis.

Comparison 11: Colloid + crystalloid vs another colloid + crystalloid, Outcome 2: Neonates: Apgar score < 7
No trials reported other secondary outcomes for this comparison.
Unbalanced versus balanced hydroxyethyl starch
Primary outcome: maternal hypotension requiring pharmacological intervention
One study compared unbalanced versus balanced hydroxyethyl starch (Marciniak 2015). There was no clear evidence of a difference between the groups (RR 1.04, 95% CI 0.78 to 1.39, 1 study, 51 women; Analysis 11.1.2).
Secondary outcomes
Neonatal
Apgar scores of less than 8 at five minutes
Marciniak 2013 (51 women) reported this outcome. There were no events in either arm (Analysis 11.3).
11.3. Analysis.

Comparison 11: Colloid + crystalloid vs another colloid + crystalloid, Outcome 3: Neonates with Apgar score < 8 at 5 min
No trials reported other secondary outcomes for this comparison.
Summary: fluids
In preventing hypotension following spinal anaesthesia at caesarean section, we found the following.
Crystalloids may be more effective than control.
Rapid crystalloid coload is more effective than crystalloid preload.
Colloids are more effective than crystalloids.
For colloids, there is no clear difference with high versus low volumes or with preloading versus coloading.
Drugs
This group of interventions comprises comparisons corresponding to data analyses 12 to 36. The section begins by reporting comparisons involving ephedrine, including ephedrine versus control, ephedrine versus other drugs; see Table 4 for comparison 'ephedrine versus phenylephrine'), different regimens of ephedrine, and different ephedrine regimens plus crystalloid or colloid. Other comparisons assess phenylephrine versus control, other drugs, different regimens of phenylephrine, and phenylephrine combined with crystalloid. Finally, we assess other drugs: glycopyrrolate, ondansetron; see Table 5 for 'ondansetron versus control'), granisetron, ketamine, angiotensin, and dopamine.
Ephedrine
Ephedrine versus control
Primary outcome: maternal hypotension requiring pharmacological intervention
There was a lower incidence of hypotension in the ephedrine prophylaxis groups than in controls (average RR 0.65, 95% CI 0.53 to 0.80; 22 studies, 1401 women; Analysis 12.1). Substantial heterogeneity was present (I² = 75%, Tau² = 0.14), which was most likely due to differences in dosing of prophylactic ephedrine, rescue treatments for hypotension when it occurred, and administration routes for the ephedrine. Of note, most studies were unclear in reporting methods of sequence generation, allocation concealment, and blinding.
All studies examined intravenous (IV) ephedrine except for two studies where ephedrine was given intramuscularly (Gomaa 2003; Grubb 2004). Excluding these two studies from analyses reduced heterogeneity only slightly (I² = 69%, Tau² = 0.09). The asymmetrical funnel plot (Figure 4) may be due to small study effects or publication‐type bias.
Secondary outcomes
Maternal
Hypertension requiring intervention
There was no conclusive evidence of a difference between the groups (average RR 1.61, 95% CI 1.00 to 2.61, 7 studies, 520 women; Analysis 12.2).
12.2. Analysis.

Comparison 12: Ephedrine vs control, Outcome 2: Women with hypertension requiring intervention
Cardiac dysrhythmia
There was no clear evidence of a difference between the groups in rates of tachycardia (average RR 1.12, 95% CI 0.74 to 1.70, 2 studies, 93 women) and no conclusive evidence with respect to bradycardia (average RR 14.46, 95% CI 0.87, 241.09, 2 studies, 103 women, no events in one study). There were only seven events in the analysis for bradycardia, but they were all in the ephedrine group (Analysis 12.3).
12.3. Analysis.

Comparison 12: Ephedrine vs control, Outcome 3: Women with cardiac arrhythmia
Nausea and/or vomiting
There was no conclusive evidence of a difference between the groups for rates of nausea or vomiting (average RR 0.71, 95% CI 0.22 to 2.34, 5 studies, 219 women, I² = 62%), or rates of vomiting alone (average RR 0.68, 95% CI 0.44 to 1.07, 6 studies, 516 women, I² = 47%). Rates of nausea alone were lower in the ephedrine group (average RR 0.68, 95% CI 0.48 to 0.96, 8 studies, 620 women, I² = 25%; Analysis 12.4).
12.4. Analysis.

Comparison 12: Ephedrine vs control, Outcome 4: Women with nausea and/or vomiting
Neonatal
Acidosis
There was insufficient evidence to determine whether there was a difference between the groups (RR 1.29, 95% CI 0.67 to 2.49, 9 studies, 576 babies; Analysis 12.5).
12.5. Analysis.

Comparison 12: Ephedrine vs control, Outcome 5: Neonates with acidosis (pH < 7.2)
Apgar scores of less than 7 or 8 at five minutes
There was insufficient evidence to determine whether there was a difference between the groups in Apgar scores of less than 7 at five minutes (RR 1.14, 95% CI 0.34 to 3.81, 4 studies, 263 women). Ten studies (N = 579) reported Apgar score of less than 8 at five minutes and there were no events in either arm (Analysis 12.6).
12.6. Analysis.

Comparison 12: Ephedrine vs control, Outcome 6: Neonates: Apgar score
No trials reported other secondary outcomes for this comparison.
Ephedrine versus other drug regimens
Ephedrine versus crystalloid
Primary outcome: maternal hypotension requiring pharmacological intervention
Fewer women in the ephedrine group developed hypotension compared with the crystalloid group (average RR 0.60, 95% CI 0.47 to 0.78, 9 studies, 613 women; Analysis 13.1). There was moderate heterogeneity between the studies (I² = 40%), which may be related to variation in methods and dose of ephedrine between the different studies.
13.1. Analysis.

Comparison 13: Ephedrine vs crystalloid, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Hypertension requiring intervention
There was insufficient evidence to determine whether there was a difference between the groups (average RR 1.10, 95% CI 0.37 to 3.28, 3 studies, 280 women, I² = 43%; Analysis 13.2).
13.2. Analysis.

Comparison 13: Ephedrine vs crystalloid, Outcome 2: Women with hypertension requiring intervention
Cardiac dysrhythmia
There was insufficient evidence to determine whether there was a difference between the groups in rates of bradycardia (RR 0.33, 95% CI 0.01 to 7.99, 1 study, 100 women; Analysis 13.3).
13.3. Analysis.

Comparison 13: Ephedrine vs crystalloid, Outcome 3: Women with bradycardia
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups for rates of nausea or vomiting (average RR 1.00, 95% CI 0.48 to 2.08, 2 studies, 146 women) and no conclusive evidence of a difference for rates of vomiting alone (average RR 0.57, 95% CI 0.31 to 1.05, 3 studies, 220 women, I² = 33%). Rates of nausea alone were lower in the ephedrine group (average RR 0.54, 95% CI 0.31 to 0.93, 3 studies, 220 women); see Analysis 13.4.
13.4. Analysis.

Comparison 13: Ephedrine vs crystalloid, Outcome 4: Women with nausea and/or vomiting
Impaired consciousness, dizziness
There was insufficient evidence to determine whether there was a difference between the groups (RR 0.40, 95% CI 0.37 to 3.28, 1 study, 46 women; Analysis 13.5).
13.5. Analysis.

Comparison 13: Ephedrine vs crystalloid, Outcome 5: Women with impaired consciousness
Neonatal
Acidosis
There was insufficient evidence to determine whether there was a difference between the groups (average RR 1.41, 95% CI 0.48 to 4.15, 2 studies, 218 babies). There were no events in one of the two studies (Analysis 13.6).
13.6. Analysis.

Comparison 13: Ephedrine vs crystalloid, Outcome 6: Neonates with acidosis (pH < 7.2)
Apgar scores of less than 7 or 8 at five minutes
One study (Carvalho 2000, 100 women) reported Apgar score of less than 7 at five minutes; no events occurred in either arm. Four studies (226 women) reported Apgar scores of less than 8 at five minutes; only one event occurred, which was in the ephedrine group (average RR 3.00, 95% CI 0.13 to 71.92; Analysis 13.7).
13.7. Analysis.

Comparison 13: Ephedrine vs crystalloid, Outcome 7: Neonatal Apgar score
No trials reported other secondary outcomes for this comparison.
Ephedrine plus crystalloid versus colloid
Primary outcome: maternal hypotension requiring pharmacological intervention
One study investigating this comparison found no evidence of a difference in the incidence of hypotension (RR 0.65, 95% CI 0.38 to 1.12; Analysis 14.1).
14.1. Analysis.

Comparison 14: Ephedrine + crystalloid vs colloid, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Nausea and/or vomiting
One study investigating this comparison found nausea (RR 0.42, 95% CI 0.22 to 0.81; 75 women) and vomiting (RR 0.17, 95% CI 0.04 to 0.77; 75 women) were less common in the ephedrine plus crystalloid group than in the colloid group (Analysis 14.2).
14.2. Analysis.

Comparison 14: Ephedrine + crystalloid vs colloid, Outcome 2: Women with nausea and/or vomiting
Ephedrine plus colloid versus crystalloid
Primary outcome: maternal hypotension requiring pharmacological intervention
Hypotension was less common in the ephedrine plus colloid group than in the crystalloid group (RR 0.39, 95% CI 0.21 to 0.74, 1 study, 75 women; Analysis 15.1).
15.1. Analysis.

Comparison 15: Ephedrine + colloid vs crystalloid, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Nausea and/or vomiting
Nausea was less common in the ephedrine plus colloid group than in the crystalloid group (RR 0.27, 95% CI 0.11 to 0.65, 1 study, 75 women. There was insufficient evidence to determine whether there was a difference between the groups in rates of vomiting (RR 0.38, 95% CI 0.09 to 1.55, 1 study, 75 women); see Analysis 15.2.
15.2. Analysis.

Comparison 15: Ephedrine + colloid vs crystalloid, Outcome 2: Women with nausea and/or vomiting
No trials reported other secondary outcomes for this comparison.
Ephedrine versus phenylephrine
See Table 4.
Primary outcome: maternal hypotension requiring pharmacological intervention
There was no clear evidence of a difference between the groups (average RR 0.92, 95% CI 0.71 to 1.18, 8 studies, 401 women, I² = 37%; very low‐quality evidence; Analysis 16.1).
16.1. Analysis.

Comparison 16: Ephedrine vs phenylephrine, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Hypertension requiring intervention
There was insufficient evidence to determine whether there was a difference between the groups (average RR 1.72, 95% CI 0.71 to 4.16, 2 studies, 118 women, low‐quality evidence; Analysis 16.2).
16.2. Analysis.

Comparison 16: Ephedrine vs phenylephrine, Outcome 2: Women with hypertension requiring intervention
Cardiac dysrhythmia
Rates of bradycardia were lower in the ephedrine group (average RR 0.37, 95% CI 0.21 to 0.64, 5 studies, 304 women, low‐quality evidence). There was insufficient evidence to determine whether there was a difference between the groups in rates of tachycardia (RR 2.22, 95% CI 0.44 to 11.18, 1 study, 57 women). See Analysis 16.3.
16.3. Analysis.

Comparison 16: Ephedrine vs phenylephrine, Outcome 3: Cardiac dysrhythmia
Nausea and/or vomiting
There was no clear evidence of a difference between the groups (average RR 0.76, 95% CI 0.39 to 1.49, 4 studies, 204 women, I² = 37%, very low‐quality evidence; Analysis 16.4).
16.4. Analysis.

Comparison 16: Ephedrine vs phenylephrine, Outcome 4: Women with nausea and/or vomiting
Neonatal
Acidosis
There was no clear evidence of a difference between the groups (average RR 0.89, 95% CI 0.07 to 12.00, 3 studies, 175 babies, low‐quality evidence). Only two events occurred, both in the same study (Analysis 16.5).
16.5. Analysis.

Comparison 16: Ephedrine vs phenylephrine, Outcome 5: Neonates with acidosis (pH < 7.2)
Apgar scores of less than 7 or 8 at five minutes
Six studies (321 babies, low‐quality evidence) measured this outcome. There were no events in either group (Analysis 16.6).
16.6. Analysis.

Comparison 16: Ephedrine vs phenylephrine, Outcome 6: Neonates with Apgar score < 8 at 5 min
No trials reported other secondary outcomes for this comparison.
Sensitivity analysis
Removing Magalhaes 2009 from Analysis 16.1, Analysis 16.3, Analysis 16.2, Analysis 16.6, and Analysis 16.4 made very little difference to the overall results.
Ephedrine versus angiotension
Primary outcome: maternal hypotension requiring pharmacological intervention
One study reported this outcome (Ramin 1994, 20 women). No events occurred in either arm (Analysis 17.1).
17.1. Analysis.

Comparison 17: Ephedrine vs angiotensin, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups (RR 3.00, 95% CI 0.14 to 65.90, 1 study, 20 women; Analysis 17.2).
17.2. Analysis.

Comparison 17: Ephedrine vs angiotensin, Outcome 2: Women with nausea and/or vomiting
Neonatal
Acidosis
There was insufficient evidence to determine whether there was a difference between the groups (RR 9.00, 95% CI 0.55 to 147.95, 1 study, 20 babies). Only four events occurred, all in the ephedrine arm (Analysis 17.3).
17.3. Analysis.

Comparison 17: Ephedrine vs angiotensin, Outcome 3: Neonates with acidosis (pH < 7.2)
No trials reported other secondary outcomes for this comparison.
Ephedrine versus colloid
Primary outcome: maternal hypotension requiring pharmacological intervention
Rates of hypotension were lower in the ephedrine group (average RR 0.53, 95% CI 0.36 to 0.79, 2 studies, 160 women; Analysis 18.1).
18.1. Analysis.

Comparison 18: Ephedrine vs colloid, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Hypertension requiring intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 3.00, 95% CI 0.32 to 27.87, 1 study, 100 women; Analysis 18.2).
18.2. Analysis.

Comparison 18: Ephedrine vs colloid, Outcome 2: Women with hypertension requiring intervention
Cardiac dysrhythmia
One study reported bradycardia (Jabalameli 2011, 100 women). There were no events in either arm (Analysis 18.3).
18.3. Analysis.

Comparison 18: Ephedrine vs colloid, Outcome 3: Women with bradycardia
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups in rates of nausea or vomiting (RR 5.00, 95% CI 0.25 to 101.58, 1 study, 100 women) or in rates of vomiting alone (RR 0.14, 95% CI 0.01 to 2.65, 1 study, 60 women). Rates of nausea alone were lower in the ephedrine group (RR 0.22, 95% CI 0.05, 0.94, 1 study, 60 women); see Analysis 18.4.
18.4. Analysis.

Comparison 18: Ephedrine vs colloid, Outcome 4: Women with nausea and vomiting
Neonatal
Acidosis
One study reported this outcome (Jabalameli 2011, 100 babies). There were no events in either arm (Analysis 18.5).
18.5. Analysis.

Comparison 18: Ephedrine vs colloid, Outcome 5: 5 Neonates with acidosis (pH < 7.2)
Apgar scores of less than 7 or 8 at five minutes
There was insufficient evidence to determine whether there was a difference between the groups (RR 3.00, 95% CI 0.13 to 71.92, 1 study, 100 babies; Analysis 18.6).
18.6. Analysis.

Comparison 18: Ephedrine vs colloid, Outcome 6: Apgar score < 8 at 5 min
No trials reported other secondary outcomes for this comparison.
Ephedrine versus metaraminol
Primary outcome: maternal hypotension requiring pharmacological intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 1.56,95% CI 0.50 to 4.89, 1 study, 53 women; Analysis 19.1).
19.1. Analysis.

Comparison 19: Ephedrine vs metaraminol, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Hypertension requiring intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 0.62, 95% CI 0.26 to 1.47, 1 study, 53 women; Analysis 19.2).
19.2. Analysis.

Comparison 19: Ephedrine vs metaraminol, Outcome 2: Women with hypertension requiring intervention
Cardiac dysrhythmia
One study reported bradycardia (Bhardwaj 2013, 53 women). There were no events in either arm (Analysis 19.3).
19.3. Analysis.

Comparison 19: Ephedrine vs metaraminol, Outcome 3: Women with bradycardia
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups (RR 7.26, 95% CI 0.39 to 134.01, 1 study, 53 women; Analysis 19.4).
19.4. Analysis.

Comparison 19: Ephedrine vs metaraminol, Outcome 4: Women with nausea and/or vomiting
Neonatal
Acidosis
One study reported this outcome (Bhardwaj 2013, 53 babies). There were no events in either arm (Analysis 19.5).
19.5. Analysis.

Comparison 19: Ephedrine vs metaraminol, Outcome 5: 5 Neonates with acidosis (pH < 7.2)
Apgar scores of less than 8 at five minutes
One study reported this outcome (Bhardwaj 2013, 53 babies). There were no events in either arm (Analysis 19.6).
19.6. Analysis.

Comparison 19: Ephedrine vs metaraminol, Outcome 6: Neonatal Apgar score < 8 at 5 min
No trials reported other secondary outcomes for this comparison.
Different ephedrine regimens
Ephedrine: lower dose versus higher dose
Primary outcome: maternal hypotension requiring pharmacological intervention
There was no clear evidence of a difference between the groups in dose comparisons of 5 mg versus 10 mg (RR 1.05, 95% CI 0.65 to 1.69, 2 studies, 100 women), 6 mg versus 12 mg (RR 1.83, 95% CI 0.83 to 4.04, 1 study, 46 women), 5 mg versus 15 mg (RR 2.00, 95% CI 0.94 to 4.27, 1 study, 40 women), 10 mg versus 15 mg (RR 1.83, 95% CI 0.84 to 3.99, 1 study, 40 women), 10 mg versus 20 mg (RR 1.06, 95% CI 0.80 to 1.39, 2 studies, 60 women), or 15 mg compared to 30 mg ephedrine (RR 2.11, 95% CI 1.06 to 4.21, 1 study, 100 women). However, rates of hypotension were higher with 10 mg compared to 30 mg (RR 2.43, 95% CI 1.30 to 4.54, 1 study, 40 women), and 20 mg compared to 30 mg (RR 2.29, 95% CI 1.21 to 4.32, 1 study, 40 women); see Analysis 20.1.
20.1. Analysis.

Comparison 20: Ephedrine: different doses, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Hypertension requiring intervention
There was insufficient evidence to determine whether there was a difference between the groups in comparisons of 5 mg versus 10 mg ephedrine (RR 1.20, 95% CI 0.44 to 3.30, 1 study, 40 women), 5 mg versus 15 mg (RR 0.50, 95% CI 0.23 to 1.07, 1 study, 40 women), 10 mg versus 15 mg (RR 0.42, 95% CI 0.18 to 0.96, 1 study, 40 women), 10 mg versus 20mg (RR 0.20, 95% CI 0.03 to 1.56, 1 study, 40 women), 10 mg versus 30 mg (RR 0.11, 95% CI 0.02 to 0.80, 1 study, 40 women), or 20 mg versus 30 mg ephedrine (RR 0.56, 95% CI 0.23 to 1.37, 1 study, 40 women); see Analysis 20.2.
20.2. Analysis.

Comparison 20: Ephedrine: different doses, Outcome 2: Women with hypertension requiring intervention
Nausea and/or vomiting
There was no clear evidence of a difference between the groups in rates of nausea and/or vomiting in comparisons of 6 mg versus 12 mg ephedrine (RR 0.81, 95% CI 0.38 to 1.74, 1 study, 46 women); see Analysis 20.3.1.
20.3. Analysis.

Comparison 20: Ephedrine: different doses, Outcome 3: Women with nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the dosing groups in rates of vomiting in comparisons of 5 mg versus 10 mg (RR 3.00, 95% CI 0.34 to 26.45, 1 study, 40 women), 5 mg versus 15 mg (RR 1.50, 95% CI 0.28 to 8.04, 1 study, 40 women), 10 mg versus 15 mg (RR 0.50, 95% CI 0.05 to 5.08, 1 study, 40 women), or 15 mg versus 30 mg ephedrine (RR 0.67, 95% CI 0.12 to 3.82, 1 study, 100 women); see Analysis 20.3.
There was insufficient evidence to determine whether there was a difference between the groups in rates of nausea, in comparisons of 5 mg versus 10 mg (RR 2.00, 95% CI 0.83 to 4.81, 1 study, 40 women), 5 mg versus 15 mg (RR 2.50, 95% CI 0.94 to 6.66, 1 study, 40 women), 10 mg versus 15 mg (RR 1.25, 95% CI 0.39 to 3.99, 1 study, 40 women, 10 mg versus 20 mg (RR 0.69, 95% CI 0.39 to 1.24, 1 study, 40 women), 10 mg versus 30 mg (RR 1.80, 95% CI 0.73 to 4.43, 1 study, 40 women), 15 mg versus 30 mg (RR 1.43, 95% CI 0.59 to 3.45, 1 study, 100 women), or 20 mg versus 30 mg ephedrine (RR 2.60, 95% CI 1.14 to 5.93, 1 study, 40 women); see Analysis 20.3.
Neonatal
Acidosis (pH less than 7.2)
There was insufficient evidence to determine whether there was a difference between the groups in comparisons of 5 mg versus 10 mg ephedrine (RR 0.20, 95% CI 0.01 to 3.92, 1 study, 40 babies), 5 mg versus 15 mg (RR 0.33, 95% CI 0.01 to 7.72, 1 study, 40 babies), 6 mg versus 12 mg (RR 0.31, 95% CI 0.01 to 7.16, 1 study, 46 babies), 10 mg versus 15 mg (RR 2.00, 95% CI 0.20 to 20.33, 1 study, 40 babies), 10 mg versus 20 mg (RR 0.59, 95% CI 0.24 to 1.50, 1 study, 39 babies), 10 mg versus 30 mg (RR 1.13, 95% CI 0.36 to 3.55, 1 study, 38 babies), or 20 mg versus 30 mg (RR 1.89, 95% CI 0.69 to 5.21, 1 study, 37 babies); see Analysis 20.4.
20.4. Analysis.

Comparison 20: Ephedrine: different doses, Outcome 4: Neonates with acidosis (pH < 7.2)
Apgar scores of less than 7 or 8 at five minutes
There was insufficient evidence to determine whether there was a difference between the groups, in comparisons of 6 mg versus 12 mg ephedrine (RR 0.31, 95% CI 0.01 to 7.16, 1 study, 46 babies).
No events occurred in comparisons of 5 mg versus 10 mg ephedrine (1 study, 40 babies), 5 mg versus 15 mg (1 study, 40 babies), 10 mg versus 15 mg (1 study, 40 babies), 10 mg versus 20 mg (1 study, 40 babies), 10 mg versus 30 mg (1 study, 40 babies), 20 mg versus 30 mg (1 study, 40 babies); see Analysis 20.5.
20.5. Analysis.

Comparison 20: Ephedrine: different doses, Outcome 5: Neonatal Apgar score at 5 min
No trials reported other secondary outcomes for this comparison.
Ephedrine: slower rate versus faster rate
Primary outcome: maternal hypotension requiring pharmacological intervention
One study compared ephedrine given as a 10 mg in bolus followed by continuous infusion of 2 mg/min versus ephedrine 8 mg/min for 3 min, followed by 4 mg/min for 2 min, then 2 mg/min (Carvalho 2000). Rates of hypotension requiring intervention were higher in the bolus group (RR 3.50, 95% CI 1.26 to 9.72, 1 study, 80 women).
There was insufficient evidence to determine whether there was a difference between the groups, in comparisons of 0.5 mg/min versus 1 mg/min (RR 1.22, 95% CI 0.65 to 2.29, 1 study, 40 women), 0.5 mg/min versus 2 mg/min (RR 1.57, 95% CI 0.77 to 3.22, 1 study, 40 women), 0.5 mg/min versus 4 mg/min (1.22, 95% CI 0.65 to 2.29, 1 study, 40 women), 1 mg/min versus 2 mg/min (average RR 1.24, 95% CI 0.83 to 1.84, 3 studies, 107 women, I2=0%), 1 mg/min versus 3 to 4 mg/min (average RR 1.29, 95% CI 0.81 to 2.05, 2 studies, 99 women, I² = 0%), 2 mg/min versus 3 to 4 mg/min (average RR 1.21, 95% CI 0.60 to 2.43, 2 studies, 239 women, I² = 38%; Analysis 21.1).
21.1. Analysis.

Comparison 21: Ephedrine: different rates, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Cardiac dysrhythmia
One study in 19 women comparing ephedrine 1 mg/min versus 2 mg/min reported bradycardia as an outcome (Hall 1994). There were no events in either arm (Analysis 21.3).
21.3. Analysis.

Comparison 21: Ephedrine: different rates, Outcome 3: Women with bradycardia
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups in rates of nausea or vomiting, in a comparison of infusion at 1 mg/min versus 2 mg/min (RR 8.18, 95% CI 0.50 to 133.66, 1 study, 19 women; Analysis 21.4).
21.4. Analysis.
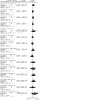
Comparison 21: Ephedrine: different rates, Outcome 4: Women with nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups in rates of nausea alone in comparisons of ephedrine bolus plus slow infusion versus faster infusion (as described above) (RR 1.83, 95% CI 0.75 to 4.48, 1 study, 80 women), or infusion of 0.5 mg/min versus 1 mg/min (RR 1.29, 95% CI 0.60 to 2.77, 1 study, 40 women), 0.5 mg/min versus 2 mg/min (RR 1.50, 95% CI 0.66 to 3.43, 1 study, 40 women), 0.5 mg/min versus 4 mg/min (RR 1.29, 95% CI 0.60 to 2.77, 1 study, 40 women), 1 mg/min versus 2 mg/min (RR 1.17, 95% CI 0.48, 2.86, 1 study, 40 women), 1 mg/min versus 4 mg/min (RR 1.00, 95% CI 0.43, 2.33, 1 study, 40 women), or 2 mg/min versus 4 mg/min (RR 0.86, 95% CI 0.35 to 2.10, 1 study, 40 women). See Analysis 21.4.
There was insufficient evidence to determine whether there was a difference between the groups in rates of vomiting alone, in comparisons of ephedrine bolus plus slow infusion versus faster infusion (as described above) (RR 1.67, 95% CI 0.43 to 6.51, 1 study, 80 women), or infusion of 0.5 mg/min versus 1 mg/min (RR 0.67, 95% CI 0.12, 3.57, 1 study, 40 women), 0.5 mg/min versus 2 mg/min (RR 2.00, 95% CI 0.20 to 20.33, 1 study, 40 women), 0.5 mg/min versus 4 mg/min (RR 2.00, 95% CI 0.20 to 20.33, 1 study, 40 women), 1 mg/min versus 2 mg/min (RR 3.00, 95% CI 0.34, 26.45, 1 study, 40 women), 1 mg/min versus 4 mg/min (RR 3.00, 95% CI 0.34 to 26.45, 1 study, 40 women) or 2 mg/min versus 4 mg/min (RR 1.00, 95% CI 0.07 to 14.90, 1 study, 40 women). See Analysis 21.4.
Neonatal
Acidosis
There was insufficient evidence to determine whether there was a difference between the groups in comparisons of ephedrine bolus plus slow infusion versus faster infusion (as described above) (RR 1.66, 95% CI 0.53 to 5.23, 1 study, 78 babies), or infusion of 0.5 mg/min versus 1 mg/min (RR 0.33, 95% CI 0.04 to 2.94, 1 study, 40 babies), 0.5 mg/min versus 2 mg/min (3.00, 95% CI 0.13 to 69.52, 1 study, 40 babies), 0.5 mg/min versus 4 mg/min (RR 0.25, 95% CI 0.03, 2.05, 1 study, 40 babies), 1 mg/min versus 2 mg/min (RR 7.00, 95% CI 0.38 to 127.32, 1 study, 40 babies), 1 mg/min versus 4 mg/min (RR 0.75, 95% CI 0.19 to 2.93, 1 study, 40 babies), or 2 mg/min versus 4 mg/min (RR 0.11, 95% CI 0.01 to 1.94, 1 study, 40 babies); see Analysis 21.5.
21.5. Analysis.

Comparison 21: Ephedrine: different rates, Outcome 5: Neonates with acidosis (pH < 7.2)
Apgar scores of less than 7 or 8 at five minutes
One study in 80 women reported this outcome (Carvalho 2000), comparing ephedrine bolus plus slow infusion versus faster infusion (as described above), and one study in 40 babies compared 0.5 mg/min versus 1 mg/min, 0.5 mg/min versus 2 mg/min, 0.5 mg/min versus 4 mg/min, 1 mg/min versus 2 mg/min, 1 mg/min versus 4 mg/min, and 2 mg/min versus 4 mg/min (Carvalho 1999b). There were no events in either arm of any of these studies (Analysis 21.6).
21.6. Analysis.

Comparison 21: Ephedrine: different rates, Outcome 6: Neonatal Apgar score at 5 min
No trials reported other secondary outcomes for this comparison.
Ephedrine: oral versus intramuscular (IM) or intravenous (IV)
Primary outcome: maternal hypotension requiring pharmacological intervention
There was no conclusive evidence of a difference between the groups when comparing oral versus IM administration of ephedrine (RR 3.00, 95% CI 0.95 to 9.48, 1 study, 40 women). Rates of maternal hypotension were higher in the oral group compared with the IV group (RR 19.00, 95% CI 1.18 to 305.88, 1 study, 40 women). See Analysis 22.1.
22.1. Analysis.

Comparison 22: Ephedrine: oral vs IM or IV, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Hypertension requiring intervention
There were no events in either arm when comparing oral ephedrine with IM or IV (1 study, 40 women; Analysis 22.2).
22.2. Analysis.

Comparison 22: Ephedrine: oral vs IM or IV, Outcome 2: Women with hypertension requiring intervention
Nausea and/or vomiting
There was no conclusive evidence of a difference between the groups in rates of nausea or vomiting when comparing oral versus IM (RR 1.33, 95% CI 0.34 to 5.21, 1 study, 40 women) or IV administration (RR 9.00, 95% CI 0.52 to 156.91, 1 study, 40 women); see Analysis 22.3.
22.3. Analysis.

Comparison 22: Ephedrine: oral vs IM or IV, Outcome 3: Women with nausea and vomiting
No trials reported other secondary outcomes for this comparison.
Ephedrine: IM versus IV
Primary outcome: maternal hypotension requiring pharmacological intervention
There was no clear evidence of a difference between the groups (RR 0.75, 95% CI 0.43 to 1.30, 1 study, 60 women; Analysis 23.1).
23.1. Analysis.

Comparison 23: Ephedrine: IM vs IV, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Hypertension requiring intervention
There were no events in either arm when comparing IM ephedrine versus IV (1 study, 60 women; Analysis 23.2).
23.2. Analysis.

Comparison 23: Ephedrine: IM vs IV, Outcome 2: Women with hypertension requiring intervention
Neonatal
Apgar scores of less than 7 or 8 at five minutes
There were no events in either arm when comparing IM ephedrine with IV (1 study, 60 babies; Analysis 23.3).
23.3. Analysis.

Comparison 23: Ephedrine: IM vs IV, Outcome 3: Apgar < 8 at 5 min
No trials reported other secondary outcomes for this comparison.
Sensitivity analysis
Sensitivity analysis was not possible for this comparison.
Phenylephrine versus control (placebo)
Primary outcome: maternal hypotension requiring pharmacological intervention
Five studies investigating this comparison found less hypotension with phenylephrine compared with control (average RR 0.45, 95% CI 0.26 to 0.80, 280 women, 5 studies, I² = 86%, Tau² = 0.34; Analysis 24.1).
Secondary outcomes
Maternal
Cardiac dysrhythmia
There was insufficient evidence to determine whether there was a difference between the groups in rates of tachycardia (RR 0.87, 95% CI 0.13 to 5.73, 1 study, 56 women) or bradycardia (average RR 3.23, 95% CI 0.17 to 61.85, 3 studies, 180 women, I² = 73%, Tau² = 4.97); see Analysis 24.2.
24.2. Analysis.
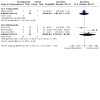
Comparison 24: Phenylephrine vs control, Outcome 2: Women with cardiac dysrhythmia
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups in rates of nausea or vomiting (average RR 0.70, 95% CI 0.16 to 0.80, 3 studies, 180 women, I² = 67%, Tau² = 0.34; Analysis 24.3).
24.3. Analysis.

Comparison 24: Phenylephrine vs control, Outcome 3: Women with nausea and/or vomiting
Neonatal
Acidosis
There was insufficient evidence to determine whether there was a difference between the groups (RR 0.96, 95% CI 0.06 to 14.50, 1 study, 49 babies; Analysis 24.4).
24.4. Analysis.

Comparison 24: Phenylephrine vs control, Outcome 4: Neonates with acidosis (pH < 7.2)
Apgar scores of less than 7 or 8 at five minutes
Three studies reported Apgar scores of less than 7 (Ngan Kee 2004a, 50 babies), or of less than 8 (Loughrey 2005; Moslemi 2015, 96 babies). There were no events in any study arm (Analysis 24.5; Analysis 24.6).
24.5. Analysis.

Comparison 24: Phenylephrine vs control, Outcome 5: Neonates with Apgar < 7 at 5 min
24.6. Analysis.

Comparison 24: Phenylephrine vs control, Outcome 6: Neonates with Apgar < 8 at 5 min
No trials reported other secondary outcomes for this comparison.
Phenylephrine versus other regimens or interventions
Phenylephrine versus mephentermine
Primary outcome: maternal hypotension requiring pharmacological intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 2.00, 95% CI 0.19 to 20.90, 1 study, 60 women; Analysis 25.1).
25.1. Analysis.

Comparison 25: Phenylephrine vs mephentermine, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Hypertension requiring intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 17.00, 95% CI 1.03 to 281.91, 1 study, 60 women; Analysis 25.2).
25.2. Analysis.

Comparison 25: Phenylephrine vs mephentermine, Outcome 2: Women with hypertension requiring intervention
Cardiac dysrhythmia
There was insufficient evidence to determine whether there was a difference between the groups in rates of bradycardia (RR 15.00, 95% CI 0.89 to 251.42, 1 study, 60 women; Analysis 25.3).
25.3. Analysis.

Comparison 25: Phenylephrine vs mephentermine, Outcome 3: Cardiac dysrhythmia
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups in rates of nausea (RR 0.20, 95% CI 0.01 to 4.00, 1 study, 60 women) or vomiting (RR 1.00, 95% CI 0.07 to15.26 1 study, 60 women); see Analysis 25.4.
25.4. Analysis.

Comparison 25: Phenylephrine vs mephentermine, Outcome 4: Nausea and/or vomiting
No trials reported other secondary outcomes for this comparison.
Phenylephrine versus metaraminol
Primary outcome: maternal hypotension requiring pharmacological intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 0.84, 95% CI 0.23 to 3.06, 1 study, 59 women; Analysis 26.1).
26.1. Analysis.

Comparison 26: Phenylephrine vs metaraminol, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Hypertension requiring intervention
Rates of hypertension were lower in the phenylephrine arm (RR 0.25, 95% CI 0.08 to 0.83, 1 study, 59 women; Analysis 26.2).
26.2. Analysis.

Comparison 26: Phenylephrine vs metaraminol, Outcome 2: Women with hypertension requiring intervention
Cardiac dysrhythmia
One study reported bradycardia (Bhardwaj 2013, 59 women). No events occurred in either arm (Analysis 26.3).
26.3. Analysis.

Comparison 26: Phenylephrine vs metaraminol, Outcome 3: Women with bradycardia
Nausea and/or vomiting
One study reported this outcome (Bhardwaj 2013, 59 women). No events occurred in either arm (Analysis 26.4).
26.4. Analysis.

Comparison 26: Phenylephrine vs metaraminol, Outcome 4: Women with nausea and/or vomiting
Neonatal
Acidosis
One study reported this outcome (Bhardwaj 2013, 59 babies). No events occurred in either arm (Analysis 26.5).
26.5. Analysis.

Comparison 26: Phenylephrine vs metaraminol, Outcome 5: Neonatal pH < 7.2
Apgar scores of less than 7 or 8 at five minutes
One study reported this outcome (Bhardwaj 2013, 59 babies). No events occurred in either arm (Analysis 26.6).
26.6. Analysis.

Comparison 26: Phenylephrine vs metaraminol, Outcome 6: Neonatal Apgar score < 8 at 5 min
No trials reported other secondary outcomes for this comparison.
Phenylephrine versus leg compression
Primary outcome: maternal hypotension requiring pharmacological intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 0.73, 95% CI 0.46 to 1.15, 1 study, 76 women; Analysis 27.1).
27.1. Analysis.

Comparison 27: Phenylephrine vs leg compression, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Cardiac dysrhythmia
There was insufficient evidence to determine whether there was a difference between the groups in rates of bradycardia (RR 0.50, 95% CI 0.05 to 5.28, 1 study, 76 women; Analysis 27.2).
27.2. Analysis.

Comparison 27: Phenylephrine vs leg compression, Outcome 2: Women with bradycardia
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups (RR 1.00, 95% CI 0.32 to 3.17 1 study, 76 women; Analysis 27.3).
27.3. Analysis.

Comparison 27: Phenylephrine vs leg compression, Outcome 3: Women with nausea and/or vomiting
No trials reported other secondary outcomes for this comparison.
Phenylephrine: different regimens
Phenylephrine infusion versus bolus
Primary outcome: maternal hypotension requiring pharmacological intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 1.40, 95% CI 0.50 to 3.92, 1 study, 60 women; Analysis 28.1).
28.1. Analysis.

Comparison 28: Phenylephrine: infusion vs bolus, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Cardiac dysrhythmia
There was insufficient evidence to determine whether there was a difference between the groups in rates of bradycardia (RR 1.22, 95% CI 0.59 to 2.51, 1 study, 60 women; Analysis 28.2).
28.2. Analysis.

Comparison 28: Phenylephrine: infusion vs bolus, Outcome 2: Women with cardiac dysrhythmia
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups in rates of nausea or vomiting (RR 0.45, 95% CI 0.18 to 1.15, 1 study, 60 women; Analysis 28.3).
28.3. Analysis.

Comparison 28: Phenylephrine: infusion vs bolus, Outcome 3: Women with nausea/vomiting
Neonatal
Apgar scores of less than 8 at five minutes
One study reported this outcome (Doherty 2012, 60 babies). No events occurred in either arm (Analysis 28.4).
28.4. Analysis.

Comparison 28: Phenylephrine: infusion vs bolus, Outcome 4: Neonatal Apgar score < 8 at 5 min
No trials reported other secondary outcomes for this comparison.
Phenylephrine: lower dose versus higher dose
Primary outcome: maternal hypotension requiring pharmacological intervention
When comparing 50 μg/mL phenylephrine versus 100 μg/mL phenylephrine used as an infusion starting at 60mL/h, rates of hypotension were higher in the lower dose group (RR 8.17, 95% CI 1.04 to 64.30, 1 study, 117 women; Analysis 29.1).
29.1. Analysis.

Comparison 29: Phenylephrine: different doses, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Hypertension requiring intervention
When comparing crystalloid plus 50 μg/mL versus 100 μg/mL phenylephrine, there was no conclusive evidence of a difference between the groups (RR 0.23, 95% CI 0.05 to 1.02, 1 study, 117 women; Analysis 29.2).
29.2. Analysis.

Comparison 29: Phenylephrine: different doses, Outcome 2: Women with hypertension requiring intervention
Cardiac dysrhythmia
When comparing crystalloid plus 50 μg/mL versus 100 μg/mL phenylephrine, fewer episodes of bradycardia occurred in the lower dose group (RR 0.11, 95% CI 0.01 to 0.80, 1 study, 117 women; Analysis 29.3).
29.3. Analysis.

Comparison 29: Phenylephrine: different doses, Outcome 3: Women with cardiac dysrhythmia
Nausea and/or vomiting
When comparing crystalloid plus 50 μg/mL versus 100 μg/mL phenylephrine, there was insufficient evidence to determine whether there was a difference between the groups in rates of nausea or vomiting (RR 3.50, 95% CI 0.37 to 32.67, 1 study, 117 women; Analysis 29.4).
29.4. Analysis.

Comparison 29: Phenylephrine: different doses, Outcome 4: Women with nausea and/or vomiting
Neonatal
Acidosis
One study reported this outcome (Ansari 2011, 117 babies). No events occurred in either arm (Analysis 29.5).
29.5. Analysis.

Comparison 29: Phenylephrine: different doses, Outcome 5: Neonatal cord blood pH < 7.2
Apgar scores of less than 7 or 8 at five minutes
One study reported this outcome (Ansari 2011, 117 babies). No events occurred in either arm (Analysis 29.6).
29.6. Analysis.

Comparison 29: Phenylephrine: different doses, Outcome 6: Neonatal Apgar score < 8 at 5 min
No trials reported other secondary outcomes for this comparison.
Glycopyrrolate versus control
Primary outcome: maternal hypotension requiring pharmacological intervention
There was insufficient evidence to determine whether there was a difference between the groups (average RR 0.63, 95% CI 0.21 to 1.91, 2 studies, 142 women; Analysis 30.1).
30.1. Analysis.

Comparison 30: Glycopyrrolate vs control, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Hypertension requiring intervention
Rates of hypertension were higher in the glycopyrrolate group (RR 2.67, 95% CI 1.31 to 5.43, 1 study, 93 women; Analysis 30.2).
30.2. Analysis.

Comparison 30: Glycopyrrolate vs control, Outcome 2: Women with hypertension requiring intervention
Cardiac dysrhythmia
There was insufficient evidence to determine whether there was a difference between the groups in rates of bradycardia (RR 0.21, 95% CI 0.01 to 4.32, 1 study, 93 women; Analysis 30.3).
30.3. Analysis.

Comparison 30: Glycopyrrolate vs control, Outcome 3: Women with bradycardia
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups in rates of nausea or vomiting (RR 2.49, 95% CI 0.69 to 9.04, 1 study, 93 women), or rates of nausea alone (0.61, 95% CI 0.36 to 1.06, 1 study, 49 women) or vomiting alone (RR 0.52, 95% CI 0.10 to 2.59, 1 study, 49 women; Analysis 30.4).
30.4. Analysis.

Comparison 30: Glycopyrrolate vs control, Outcome 4: Women with nausea and/or vomiting
Neonatal
Apgar scores of less than 7 or 8 at five minutes
Two studies reported this outcome (Ngan Kee 2013a, Ure 1999, 142 babies). No events occurred in either study (Analysis 30.5).
30.5. Analysis.

Comparison 30: Glycopyrrolate vs control, Outcome 5: Neonates with Apgar score < 8 at 5 min
No trials reported other secondary outcomes for this comparison.
Ondansetron versus control
See Table 5.
Primary outcome: maternal hypotension requiring pharmacological intervention
There was a lower incidence of hypotension in the ondansetron group (average RR 0.67, 95% CI 0.54 to 0.83, 8 studies, 740 women, I² = 35%, Tau² = 0.05, low‐quality evidence).
The studies compared doses of 2 mg, 4 mg, 6 mg, and 8 mg ondansetron versus control. The test for subgroup differences indicated a significant difference between the subgroups (Chi² = 11.97, df = 3 (P = 0.008), I² = 74.9%). The treatment effect was strongest in the 4 mg subgroup, and when we excluded this subgroup from the analysis there was no longer any indication of a difference between the subgroups (Chi² = 2.07, df = 2 (P = 0.36), I² = 3.3%). The possible explanation for the effectiveness of this lower dose compared with higher doses is unclear (Analysis 31.1).
31.1. Analysis.

Comparison 31: Ondansetron vs control, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Cardiac dysrhythmia
There was a lower rate of bradycardia in the ondansetron group (average RR 0.49, 95% CI 0.28 to 0.87, 8 studies, 740 women, low‐quality evidence; Analysis 31.2).
31.2. Analysis.

Comparison 31: Ondansetron vs control, Outcome 2: Women with bradycardia
Nausea and/or vomiting
There was a lower rate of nausea or vomiting in the ondansetron group (average RR 0.35, 95% CI 0.24 to 0.51, 7 studies, 653 women, low‐quality evidence; Analysis 31.3).
31.3. Analysis.

Comparison 31: Ondansetron vs control, Outcome 3: Women with nausea or vomiting
Anaphylaxis
One study measured this outcome (Wang 2014a, 150 women). There were no events in either arm (Analysis 31.4).
31.4. Analysis.

Comparison 31: Ondansetron vs control, Outcome 4: Women with anaphylaxis
Neonatal
Acidosis
Two studies measured this outcome. There was insufficient evidence to determine whether there was any difference between the groups (average RR 0.48, 95% CI 0.05 to 5.09, 2 studies, 134 babies, low‐quality evidence). There were no events in one of the studies (Analysis 31.6).
31.6. Analysis.

Comparison 31: Ondansetron vs control, Outcome 6: Neonatal pH < 7.2
Apgar scores of less than 8 at five minutes
Three studies measured this outcome (Wang 2014a, Wang 2014b, Marciniak 2015, 284 babies, low‐quality evidence). There were no events in any of the studies (Analysis 31.5).
31.5. Analysis.

Comparison 31: Ondansetron vs control, Outcome 5: Neonatal Apgar score < 8 at 5 min
No trials reported other secondary outcomes for this comparison.
Ondansetron versus ephedrine
Primary outcome: maternal hypotension requiring pharmacological intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 1.07, 95% CI 0.76 to 1.49, 1 study, 112 women; Analysis 32.1).
32.1. Analysis.

Comparison 32: Ondansetron vs ephedrine, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Cardiac dysrhythmia
There was no clear evidence of a difference between the groups in the rate of bradycardia (RR 3.00, 95% CI 0.12 to 72.10, 1 study, 112 women; Analysis 32.2).
32.2. Analysis.

Comparison 32: Ondansetron vs ephedrine, Outcome 2: Women with bradycardia
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups in the rate of nausea or vomiting (RR 0.38, 95% CI 0.10 to 1.34, 1 study, 112 women; Analysis 32.3).
32.3. Analysis.

Comparison 32: Ondansetron vs ephedrine, Outcome 3: Women with nausea and/or vomiting
No trials reported other secondary outcomes for this comparison.
Granisetron versus control
Primary outcome: maternal hypotension requiring pharmacological intervention
One study, Eldaba 2015, investigated this comparison and found rates of hypotension were lower with granisetron than with saline control (RR 0.05, 95% CI 0.02 to 0.14, 1 study, 200 women; Analysis 33.1).
33.1. Analysis.

Comparison 33: Granisetron vs control, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
No studies reported secondary outcomes for this comparison.
Sensitivity analysis
Sensitivity analysis was not possible under this comparison.
Ketamine versus saline
Primary outcome: maternal hypotension requiring pharmacological intervention
There was no conclusive evidence of a difference between the groups (RR 0.79, 95% CI 0.62 to 1.01, 1 study, 105 women). The study compared two different doses of IV ketamine (0.25 mg/kg and 0.5 mg/kg) versus saline.There was no evidence of a difference between the effects of the two doses (test for subgroup differences: Chi² = 0.25, df = 1 (P = 0.62), I² = 0%; Analysis 34.1).
34.1. Analysis.

Comparison 34: Ketamine vs saline, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups in rates of nausea or vomiting (RR 0.79, 95% CI 0.50 to 1.25, 1 study, 105 women; Analysis 34.2).
34.2. Analysis.

Comparison 34: Ketamine vs saline, Outcome 2: Women with nausea and/or vomiting
Neonatal
Apgar scores of less than 8 at five minutes
One study reported this outcome (Gulhas 2012, 105 women). No events occurred in either arm (Analysis 34.3).
34.3. Analysis.

Comparison 34: Ketamine vs saline, Outcome 3: Apgar score < 8 at 5 min
No trials reported other secondary outcomes for this comparison.
Sensitivity analysis
Sensitivity analysis was not possible under this comparison.
Angiotensin versus control
Primary outcome: maternal hypotension requiring pharmacological intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 0.09, 95% CI 0.01 to 1.45, 1 study, 20 women; Analysis 35.1).
35.1. Analysis.

Comparison 35: Angiotensin vs control, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups (RR 0.20, 95% CI 0.01 to 3.70, 1 study, 20 women; Analysis 35.2).
35.2. Analysis.

Comparison 35: Angiotensin vs control, Outcome 2: Women with nausea and/or vomiting
Neonatal
Acidosis
One study reported this comparison (Ramin 1994, 20 babies). There were no events in either arm (Analysis 35.3).
35.3. Analysis.

Comparison 35: Angiotensin vs control, Outcome 3: Neonates with acidosis (pH < 7.2)
No trials reported other secondary outcomes for this comparison.
Dopamine versus control
Primary outcome: maternal hypotension requiring pharmacological intervention
One small study, Yokoyama 1997, found that dopamine was more effective than control in preventing hypotension (RR 0.05, 95% CI 0.00 to 0.75, 1 study, 30 women; Analysis 36.1).
36.1. Analysis.

Comparison 36: Dopamine vs control, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Neonatal
Apgar scores of less than 8 at five minutes
One study reported this outcome (Yokoyama 1997, 30 babies). There were no events in either arm (Analysis 36.2).
36.2. Analysis.

Comparison 36: Dopamine vs control, Outcome 2: Neonatal Apgar score < 8 at 5 min
No trials reported other secondary outcomes for this comparison.
Summary: drugs
In preventing hypotension following spinal anaesthesia at caesarean section, we found the following.
Ephedrine is more effective than control, crystalloid, or colloid.
There were no differences in hypotension between ephedrine and phenylephrine, ephedrine and metaraminol, or ephedrine and angiotension. Higher doses or higher rates of ephedrine infusions result in no differences in hypotension. IV ephedrine is associated with less hypotension than oral ephedrine. There is no difference when comparing IM to IV ephedrine.
Phenylephrine is more effective than control in preventing hypotension. We found no difference in hypotension between phenylephrine and metaraminol.
We found no clear differences in the incidence of hypotension between glycopyrrolate and control.
We found no clear differences between ondansetron and control.
We found no clear differences in hypotension between angiotensin and control, or between ketamine and control.
Dopamine appears effective for preventing hypotension.
Physical methods
This group of interventions comprises comparisons corresponding to data analyses 37 to 49. Comparison 37 assesses lower limb compression versus control (Table 6), while other comparisons assess different positioning techniques (see Table 7 on comparison, 'walking versus lying'), and acupressure.
Lower limb compression versus control
See Table 6.
Primary outcome: maternal hypotension requiring pharmacological intervention
Lower limb compression was more effective than control for preventing hypotension (average RR 0.61, 95% CI 0.47 to 0.78, 11 studies, 705 women, very low‐quality evidence; Analysis 37.1). There was substantial heterogeneity (I² = 65, Tau² = 0.10), which may be due to the different types of compression used (bandages, boots, or stockings). We did not perform a subgroup analysis here as we did not feel it would be meaningful. It also may have been due to differences in formulation and volume of IV fluids given. The asymmetrical funnel plot (Figure 5) may be due to small study effects or publication‐type bias.
Secondary outcomes
Maternal
Cardiac dysrhythmia
There was insufficient evidence to determine whether there was a difference between the groups in rates of bradycardia (RR 0.63, 95% CI 0.11 to 3.56, 1 study, 74 women, very low‐quality evidence; Analysis 37.2).
37.2. Analysis.

Comparison 37: Lower limb compression vs control, Outcome 2: Women with bradycardia
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups in rates of nausea or vomiting (average RR 0.42, 95% CI 0.14 to 1.27, 4 studies, 276 women, I² = 32%, very‐low quality evidence) or rates of nausea alone (RR 1.44, 95% CI 0.25 to 8.20, 1 study, 92 women). One study in 92 women measured rates of vomiting; there were no events in either arm (Sujata 2012; Analysis 37.3).
37.3. Analysis.

Comparison 37: Lower limb compression vs control, Outcome 3: Women with nausea and/or vomiting
Neonatal
Apgar scores of less than 7 or 8 at five minutes
Three studies measured this outcome (Adsumelli 2003; Jorgensen 1996; Sood 1996, 130 babies, very low‐quality evidence). There were no events in any of the studies (Analysis 37.4).
37.4. Analysis.

Comparison 37: Lower limb compression vs control, Outcome 4: Neonates with Apgar score < 8 at 5 min
No trials reported other secondary outcomes for this comparison.
Sensitivity analysis
Removing Bhagwanjee 1990 and Sutherland 2001 made little difference to the overall results in Analysis 37.1.
Comparisons of positioning
Wedge versus supine
Primary outcome: maternal hypotension requiring pharmacological intervention
There was insufficient evidence to determine whether there was a difference between the groups in the incidence of hypotension (RR 0.85, 95% CI 0.53 to 1.37, 1 study, 80 women; Analysis 38.1).
38.1. Analysis.

Comparison 38: Wedge vs supine, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups in rates of nausea (RR 0.27, 95% CI 0.12 to 0.60, 1 study, 80 women) or vomiting (RR 0.11, 95% CI 0.01 to 2.00, 1 study, 80 women); see Analysis 38.2.
38.2. Analysis.

Comparison 38: Wedge vs supine, Outcome 2: Women with nausea and/or vomiting
No trials reported other secondary outcomes for this comparison.
Sensitivity analysis
Sensitivity analysis was not possible under this comparison.
Head‐up tilt versus horizontal
Primary outcome: maternal hypotension requiring pharmacological intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 0.71, 95% CI 0.47 to 1.06, 1 study, 40 women; Analysis 39.1).
39.1. Analysis.

Comparison 39: Head‐up tilt vs horizontal, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Neonatal
Apgar scores of less than 8 at five minutes
One study measured this outcome (Loke 2002, 40 babies). There were no events in either arm (Analysis 39.2).
39.2. Analysis.

Comparison 39: Head‐up tilt vs horizontal, Outcome 2: Neonates with Apgar score < 8 at 5 min
No trials reported other secondary outcomes for this comparison.
Head‐down tilt versus horizontal
Primary outcome: maternal hypotension requiring pharmacological intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 1.07, 95% CI 0.81 to 1.42, 1 study, 40 women; Analysis 40.1).
40.1. Analysis.

Comparison 40: Head‐down tilt vs horizontal, Outcome 1: Women with hypotension requiring intervention
No studies reported secondary outcomes for this comparison.
Crawford's wedge versus manual uterine displacement
Primary outcome: maternal hypotension requiring pharmacological intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 0.92, 95% CI 0.57 to 1.49, 1 study, 40 women; Analysis 41.1).
41.1. Analysis.

Comparison 41: Crawford's wedge vs manual uterine displacement, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Neonatal
Apgar scores of less than 8 at five minutes
One study measured this outcome (Amaro 1998, 40 babies). There were no events in either arm (Analysis 41.2).
41.2. Analysis.

Comparison 41: Crawford's wedge vs manual uterine displacement, Outcome 2: Neonates with Apgar score < 8 at 5 min
No trials reported other secondary outcomes for this comparison.
Supine versus sitting
Primary outcome: maternal hypotension requiring pharmacological intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 0.81, 95% CI 0.58 to 1.12, 1 study, 98 women; Analysis 42.1).
42.1. Analysis.

Comparison 42: Supine vs sitting, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups in rates of nausea (RR 0.65, 95% CI 0.40 to 1.07, 1 study, 98 women) or vomiting (RR 0.38, 95% CI 0.02 to 9.01, 1 study, 98 women; Analysis 42.2).
42.2. Analysis.

Comparison 42: Supine vs sitting, Outcome 2: Women with nausea and/or vomiting
Neonatal
Acidosis
One study measured this outcome (Kohler 2002, 98 babies). There were no events in either arm (Analysis 42.3).
42.3. Analysis.

Comparison 42: Supine vs sitting, Outcome 3: Neonates with acidosis (pH < 7.2)
Apgar scores of less than 7 or 8 at five minutes
One study measured this outcome (Kohler 2002, 98 women). There were no events in either arm (Analysis 42.4).
42.4. Analysis.

Comparison 42: Supine vs sitting, Outcome 4: Neonates with Apgar < 7 at 5 min
No trials reported other secondary outcomes for this comparison.
Walking versus lying
See Table 7.
Primary outcome: maternal hypotension requiring pharmacological intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 0.71, 95% CI 0.41 to 1.09, 1 study, 37 women, very low‐quality evidence; Analysis 43.1).
43.1. Analysis.

Comparison 43: Walking vs lying, Outcome 1: Women requiring intervention for hypotension
No studies reported secondary outcomes for this comparison.
Sensitivity analysis
Sensitivity analysis was not possible under this comparison.
Lateral versus supine wedged position
Primary outcome: maternal hypotension requiring pharmacological intervention
There was no clear evidence of a difference between the groups (average RR 0.91, 95% CI 0.75 to 1.09, 2 studies, 126 women; Analysis 44.1).
44.1. Analysis.

Comparison 44: Lateral vs supine wedged position, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups in rates of nausea (RR 0.81, 95% CI 0.45 to 1.48, 1 study, 86 women; Analysis 44.4).
44.4. Analysis.

Comparison 44: Lateral vs supine wedged position, Outcome 4: Women with nausea
Cardiac dysrhythmia
There was insufficient evidence to determine whether there was a difference between the groups (RR 0.50, 95% CI 0.05 to 5.08, 1 study, 40 women; Analysis 44.2.
44.2. Analysis.

Comparison 44: Lateral vs supine wedged position, Outcome 2: Women with cardiac dysrhythmia requiring intervention
Neonatal
Admission to neonatal intensive care unit
One study measured this outcome (Hartley 2001, 40 babies). There were no events in either arm (Analysis 44.3).
44.3. Analysis.

Comparison 44: Lateral vs supine wedged position, Outcome 3: Neonates admitted to neonatal intensive care unit
No trials reported other secondary outcomes for this comparison.
Left lateral versus left lateral tilt
Primary outcome: maternal hypotension requiring pharmacological intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 1.20, 95% CI 0.80 to 1.79, 1 study, 58 women; Analysis 45.1).
45.1. Analysis.

Comparison 45: Left lateral vs left lateral tilt, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Cardiac dysrhythmia
There was no conclusive evidence of a difference between the groups in rates of bradycardia (RR 0.10, 95% CI 0.01 to 1.68, 1 study, 58 women; Analysis 45.2).
45.2. Analysis.

Comparison 45: Left lateral vs left lateral tilt, Outcome 2: Women with cardiac dysrhythmia requiring intervention
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups in rates of nausea (RR 0.45, 95% CI 0.18 to 1.11, 1 study, 58 women) or vomiting (RR 0.15, 95% CI 0.01 to 2.83, 1 study, 58 women; Analysis 45.3).
45.3. Analysis.

Comparison 45: Left lateral vs left lateral tilt, Outcome 3: Women with nausea and/or vomiting
No trials reported other secondary outcomes for this comparison.
Left lateral tilt versus left manual uterine displacement
Primary outcome: maternal hypotension requiring pharmacological intervention
Left uterine displacement was associated with a reduced rate of hypotension compared to left lateral tilt (RR 0.63, 95% CI 0.49 to 0.80, 1 study, 90 women; Analysis 46.1).
46.1. Analysis.

Comparison 46: Left lateral tilt vs left manual uterine displacement, Outcome 1: Women with hypotension requiring intervention
No studies reported other outcomes for this comparison.
Leg elevation versus control
Primary outcome: maternal hypotension requiring pharmacological intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 0.73, 95% CI 0.42 to 1.26, 1 study, 63 women; Analysis 47.1).
47.1. Analysis.

Comparison 47: Leg elevation vs control, Outcome 1: Women with hypotension requiring intervention
No other outcomes were reported for this comparison
Comparisons of acupressure
Acupressure versus placebo
Primary outcome: maternal hypotension requiring pharmacological intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 0.84, 95% CI 0.58 to 1.22, 1 study, 50 women; Analysis 48.1).
48.1. Analysis.

Comparison 48: Acupressure vs placebo, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Nausea and/or vomiting
Rates of nausea were lower in the acupressure group than in the placebo group (RR 0.32, 95% CI 0.15 to 0.66, 1 study, 50 women). There was no clear evidence of a difference between the groups in rates of vomiting (RR 0.50, 95% CI 0.14 to 1.78, 1 study, 50 women). See Analysis 48.2.
48.2. Analysis.

Comparison 48: Acupressure vs placebo, Outcome 2: Women with nausea and/or vomiting
Apgar scores of less than 7 at five minutes
One study measured this outcome (Stein 1997, 50 babies). There were no events in either arm (Analysis 48.3).
48.3. Analysis.

Comparison 48: Acupressure vs placebo, Outcome 3: Neonates with Apgar < 7 at 5 min
No trials reported other secondary outcomes for this comparison.
Acupressure versus metoclopramide
Primary outcome: maternal hypotension requiring pharmacological intervention
There was insufficient evidence to determine whether there was a difference between the groups (RR 0.94, 95% CI 0.63 to 1.40, 1 study, 50 women; Analysis 49.1).
49.1. Analysis.

Comparison 49: Acupressure vs metoclopramide, Outcome 1: Women with hypotension requiring intervention
Secondary outcomes
Maternal
Nausea and/or vomiting
There was insufficient evidence to determine whether there was a difference between the groups in rates of nausea (RR 1.50, 95% CI 0.48 to 4.68, 1 study, 50 women) or vomiting (RR 3.00, 95% CI 0.33 to 26.92, 1 study, 50 women; Analysis 49.2).
49.2. Analysis.

Comparison 49: Acupressure vs metoclopramide, Outcome 2: Women with nausea and/or vomiting
Neonatal
Apgar scores of less than 7 or 8 at five minutes
One study measured Apgar scores of less than 7 at five minutes (Stein 1997, 50 babies). There were no events in either arm (Analysis 49.3).
49.3. Analysis.

Comparison 49: Acupressure vs metoclopramide, Outcome 3: Neonates with Apgar < 7 at 5 min
No trials reported other secondary outcomes for this comparison.
Summary: physical methods
In preventing hypotension following spinal anaesthesia at caesarean section, we found the following.
Lower leg compression is more effective than control (i.e. no leg compression) for preventing hypotension, although different methods of compression appear to vary in their effectiveness.
Manual left uterine displacement while supine is more effective than left lateral tilt of the bed for preventing hypotension.
In other comparisons between different physical methods such as position, wedging or leg elevation, we found none to be effective, but these trials were often small and may benefit from further research. Similarly, walking into the operating theatre as opposed to lying on the barouche is a non‐invasive, safe, and simple intervention and may also be worth further investigating in a larger study.
There was insufficient evidence to show whether acupressure is more effective than placebo or metoclopramide.
Discussion
This review is the most comprehensive to date examining the effects of interventions used to prevent hypotension following spinal anaesthesia for caesarean section.
Summary of main results
Although some interventions assessed in this review (such as colloids, ephedrine, or lower leg compression) can reduce the incidence of hypotension, we found none that eliminate the need to treat maternal hypotension during spinal anaesthesia for caesarean section. It is likely that one or more interventions used together, as commonly occurs in clinical practice, is most effective.
Our key findings include the following.
Fluids
Crystalloids alone may be inadequate for preventing hypotension.
Crystalloids may be most effective when given in higher volume as a rapid coload.
Colloids may be more effective than crystalloids.
Drugs
Vasopressors, such as ephedrine, phenylephrine, and metaraminol appear to be effective and may be more effective than fluids alone or control.
Ondansetron may be more effective than control for preventing hypotension.
There is no clear evidence to show that glycopyrrolate, ketamine, or angiotensin are effective for preventing hypotension.
Physical methods
Lower leg compression is more effective than control for preventing hypotension.
Manual uterine displacement while supine may be more effective than left lateral tilt.
We did not find other physical methods such as position, wedging, or leg elevation to be effective, but these trials were often small and may benefit from further research.
Mortality and serious morbidity in this population are rare (Hibbard 1996). The reviewed trials report no serious adverse events such as anaphylaxis, cerebral haemorrhage, or maternal death. We did not see any differences in the incidence of fetal acidosis when comparing ephedrine with phenylephrine for preventing hypotension during spinal anaesthesia, although Ngan Kee 2006 has suggested an increased risk when using ephedrine to treat, rather than prevent, hypotension.
Overall completeness and applicability of evidence
This review is very likely to represent the key research findings to date and to be applicable to clinical practice. We suggest some caution about the magnitude of the findings of some intervention comparisons given that many of these comparisons are only supported by either a single study or several small studies of unclear quality. Despite our finding that colloids were more effective than crystalloids for reducing maternal hypotension after spinal anaesthesia, the included trials were too small to show the well‐recognised and serious potential risks that colloid administration represents.
The findings of this review will be less relevant for women with pre‐eclampsia, who appear less likely to require prophylactic measures or emergency procedures than normotensive women (Clark 2005). Most studies in this review excluded women with pre‐existing hypertension.
One of the main limitations of a review of this type is outcome definition. There were multiple different definitions of hypotension between studies (Table 8). In this review, we used the definition of hypotension provided by study authors to pool these data in our meta‐analyses.
All studies investigated women having elective caesarean births except for one study that included women undergoing emergency caesarean sections.
As can be seen from the Results section and from the meta‐analyses, we found a large number of small studies with little to no information for enabling an adequate 'Risk of bias' assessment. Many studies did not report details about their method of randomisation, allocation concealment, and blinding, which limits our ability to draw clear conclusions. Furthermore, several pooled results showed high levels of heterogeneity between studies, which is most likely due to differences in study design interventions, anaesthetic techniques and variations in definition of hypotension.
We note that there are several studies awaiting assessment and acknowledge that there will be a lag time in assessing and incorporating these studies in future reviews. However, it appears unlikely that these studies will impact our key findings.
Quality of the evidence
The GRADE assessments for the key outcomes (incidence of maternal hypotension/hypertension requiring intervention; incidence of maternal bradycardia; incidence of maternal nausea and/or vomiting; neonatal acidosis as defined by cord or neonatal bloods with a pH of less than 7.2; neonatal Apgar score of less than 8 at five minutes; admission to neonatal intensive care unit) showed either low or very low quality. We chose six key comparisons for GRADE quality assessments because they represent the most clinically relevant comparisons in the updated review (see Table 1; Table 2; Table 3; Table 4; Table 5; Table 6; Table 7). Many studies were small, and their lack of detail in reporting led us to assess them as being at unclear risk of bias in method of randomisation, allocation concealment, and blinding. Seventeen studies had one or more factors designated as causing high risk of bias, but sensitivity analyses removing 12 studies where possible did not change the findings (Bhagwanjee 1990; Bottiger 2010; Cardoso 2004a; Carvalho 2009; Dahlgren 2005; Dyer 2004; Magalhaes 2009; Mercier 2014; Muzlifah 2009; Romdhani 2014; Sutherland 2001; Ueyama 1999). The remaining five studies were single studies for which sensitivity analyses were not possible (Calvache 2011; Cyna 2010; Eldaba 2015; Gulhas 2012; Pouliou 2006). As well as for study design, we downgraded evidence for indirectness (because most studies included only women having elective caesarean sections), inconsistency, and imprecision.
We noted significant heterogeneity for some comparisons, namely crystalloid versus colloid, colloid of different volumes, ephedrine versus control, ephedrine versus crystalloid, ephedrine versus phenylephrine. Sensitivity analysis showed minimal changes in overall findings.
Potential biases in the review process
There are several potential sources of bias in this review process.
Firstly, there were several differences between previous published versions and this version, including:
specific exclusion of quasi‐randomised, cluster, and cross‐over trials; and
specific exclusion of studies investigating prevention of hypotension with combined spinal‐epidural techniques.
Given the large number of randomised controlled trials investigating the core review objective (assessing the effects of prophylactic interventions for hypotension following spinal anaesthesia for caesarean section), the authors agreed that incorporating these trials into this review would contribute to a lower quality and less robust review.
Secondly, one of the review authors (AMC) was the lead author on an included study (Cyna 2010). We minimised this potential source of bias by ensuring that review authors independent of this study (RSL and CC) performed the data extraction.
Thirdly, there were 2 studies assessed as high risk as study participants received variable doses of local anaesthetic in their spinal block (Alahuhta 1992; Mathru 1980). Also, there were 2 studies assessed as high risk of bias as it was unclear whether the spinal anaesthetic technique and dose was standardised between the study groups (Ozkan 2004; Wilson 1998). It was unlikely that with randomisation this source of bias would have an important effect on the review findings.
Finally, for the purposes of this review, we specifically excluded the use of infusion pumps programmed with algorithms to address hypotension. It was difficult to determine whether this approach constituted prevention or treatment of hypotension, but discussion among review authors produced a consensus that it was the latter. Future reviews may consider whether it may be appropriate to include the results of these other computer‐controlled techniques.
Agreements and disagreements with other studies or reviews
Our results are consistent with one meta‐analysis that found that prophylactic ondansetron reduces the incidence of spinal induced hypotension (Gao 2015). This meta‐analysis also suggested that given the large heterogeneity and small sample sizes, there should be further large and high‐quality randomised trials investigating the efficacy of ondansetron for preventing hypotension in this setting.
Our results are also consistent with a systematic review that found limited evidence to support or clearly disprove the value of maternal positioning, including the use of table tilting and wedges (Cluver 2013). They also found that manual displacement of the uterus may be better than a left lateral tilt, but larger studies need to confirm this – a conclusion consistent with our results.
Finally, a recent review determined the effects of colloids and crystalloids in the incidence of hypotension induced by spinal anaesthesia in elective caesarean section and also showed that colloid administration reduced the incidence of hypotension associated with spinal anaesthesia in elective caesarean section compared with crystalloid use (Rippoles 2015). However, these authors make no mention of the serious potential risks that colloid administration may represent or the additional costs involved. Indeed, a recent Cochrane Review found no evidence that resuscitation with colloids reduces the risk of death compared to resuscitation with crystalloids in patients with trauma, burns, or following surgery. The review authors suggest that as colloids were no more effective for preventing mortality than crystalloid and were considerably more expensive, it is hard to see any justification for their continued use in clinical practice (Perel 2013).
Authors' conclusions
Implications for practice.
The results of this review will be mostly applicable to obstetric anaesthesia where women are having planned caesarean section under spinal anaesthesia. No single or combined prophylactic intervention avoids the need to treat some women for hypotension following spinal anaesthesia for caesarean section. Colloid or crystalloid preloading or coloading, the administration of parenteral ephedrine, phenylephrine, metaraminol, and ondansetron, and lower limb compression (by bandages, stockings or inflatable boots) reduce but do not eliminate the incidence of spinal hypotension requiring intervention in this setting. Despite colloids being more effective than crystalloids for reducing the incidence of maternal hypotension, the well‐recognised serious potential risks and additional costs that colloid administration may represent also need consideration. It is not possible to draw conclusions with respect to the optimum volume of intravenous fluid, route or timing of administration of vasopressors, or method of lower limb compression. Ephedrine may produce a dose‐related increase in blood pressure and heart rate. We cannot draw any other conclusions regarding adverse effects of the studied interventions, probably due to their low incidence, the small number of women studied, and the incompleteness of data for these outcomes. It is likely that combinations of interventions will be more effective than individual ones.
Implications for research.
Suggested clinical trials
Timing of sympathomimetic administration (for example: ephedrine, phenylephrine)
Optimum fluid‐preloading or coloading volume (dose‐finding)
Comparison of the relative efficacy and adverse effects of different methods of lower limb compression, for example, inflatable boots or thromboembolic deterrent stockings
Further study of haemodynamic stability in labouring versus non‐labouring women receiving spinal anaesthesia for caesarean section (one small study to date, Lapins 2001)
Optimal dose of ondansetron
Other drugs such as norepinephrine
Walking versus lying on a bed when entering the operating theatre prior to spinal anaesthesia
Computer‐controlled closed loop infusion algorithms
Future studies in this area could: include clearer reporting of methodological aspects, such as allocation, to confirm internal validity; have larger sample sizes (i.e. at least 100 participants); and include an assessment of maternal acceptability of the various prophylactic interventions under investigation. Future research could avoid interventions that fail to use standard, externally valid comparisons. Most importantly, future studies need to report the incidence of hypotension requiring an intervention. For comparisons where there are many existing studies, any further studies need to be higher quality and involve larger sample sizes.
It would also be important to obtain further information on the potential serious but rare side effects of colloid administration in this setting, from large‐scale epidemiological studies or registries.
Suggested systematic reviews
Our initial search identified several trials comparing different anaesthetic techniques or drugs, which may have an impact on haemodynamics, for example the possible local anaesthetic‐sparing effect of spinal opioids such as morphine, fentanyl, or the shorter‐acting sufentanil. It may also be that the incidence of hypotension can be predictably affected by the technique itself rather than (or in addition to) the prophylactic measures we have examined.
What's new
| Date | Event | Description |
|---|---|---|
| 5 June 2020 | Amended | The study by Mitra 2014, previously included in comparison 7 (colloid vs crystalloid), has been retracted. We have therefore reclassified this study from included to excluded and edited the review analysis and text accordingly. |
| 5 June 2020 | New citation required but conclusions have not changed | Since publication of this updated review in 2017 (Cyna 2017), the Mitra 2014 study has now been retracted by the Saudi Journal of Anaesthesia because it has "..been found to have a number of unattributed sections of content with high rate of similarity from various other articles along with overwhelming evidence of data fabrication". Removing this study from analysis 7.1, 7.3.2, 7.4.21 and 7.6.2 has not changed the results or the conclusions of this review. |
History
Protocol first published: Issue 3, 2000 Review first published: Issue 3, 2001
| Date | Event | Description |
|---|---|---|
| 9 August 2016 | New search has been performed | Search updated– last published included 75 trials, now includes 126 trials. Note: we excluded 13 trials included in last update because they assessed combined spinal‐epidurals rather than spinal anaesthesia, and we excluded one study because it failed to report our primary outcome. Author list and order updated for this version of the review. We excluded quasi‐randomised trials in this version. We also excluded trials where women received epidural anaesthesia or combined spinal‐epidural anaesthesia. We have incorporated seven 'Summary of findings' tables into this update. |
| 9 August 2016 | New citation required and conclusions have changed | Conclusions changed with this update. Ondansetron may be a useful intervention, and fluid coloading is more effective than preloading. |
| 30 June 2010 | Amended | Search updated.Eighty‐five trial reports added to Studies awaiting classification. |
| 18 February 2008 | Amended | Converted to new review format. |
| 6 June 2006 | New search has been performed | The 2006 update now contains 75 included studies. Forty new studies have been added and 10 previously excluded studies have now been included. These studies were previously excluded as there was some variation between women in the dose of anaesthetic. An additional 38 studies were excluded and appear in the Characteristics of excluded studies table with reasons for their exclusion. The new studies reinforce the previous conclusions and also show that phenylephrine is also likely to be effective in preventing hypotension. |
Notes
The study by Mitra 2014, previously included in comparison 7 (colloid vs crystalloid), has been retracted. We have therefore reclassified this study from included to excluded and edited the review analysis and text accordingly.
Acknowledgements
Thanks to Caroline Crowther and Charlotte Howell for helpful comments on the protocol. We also thank Gill Gyte and Beth Shearer for their extremely useful consumer feedback, and Jacques Riad for assistance with translation. Thanks also to Marion Andrew for her contribution as an author on the original protocol and review.
We would like to thank Anna Cuthbert and Lambert Felix, Cochrane Pregnancy and Childbirth and Jane Marjoribanks, Cochrane Editorial Unit, for their contribution to the current update (2017).
This project was supported by the National Institute for Health Research, via Cochrane Infrastructure funding to Cochrane Pregnancy and Childbirth. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS, or the Department of Health.
Data and analyses
Comparison 1. Crystalloid vs control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1.1 Women with hypotension requiring intervention | 5 | 370 | Risk Ratio (M‐H, Random, 95% CI) | 0.84 [0.72, 0.98] |
| 1.2 Nausea and/or vomiting | 1 | 69 | Risk Ratio (M‐H, Random, 95% CI) | 0.19 [0.01, 3.91] |
| 1.3 Anaphylaxis | 1 | 69 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 1.4 Apgar < 8 at 5 min | 1 | 60 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 2. Crystalloid: rapid infusion vs slow infusion.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 2.1 Women with hypotension requiring intervention | 1 | 20 | Risk Ratio (M‐H, Random, 95% CI) | 0.86 [0.45, 1.64] |
Comparison 3. Crystalloid: high vs low preload volume.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 3.1 Women with hypotension requiring intervention | 3 | 192 | Risk Ratio (M‐H, Random, 95% CI) | 0.55 [0.29, 1.02] |
| 3.1.1 15 mL/kg crystalloid | 2 | 67 | Risk Ratio (M‐H, Random, 95% CI) | 0.56 [0.33, 0.96] |
| 3.1.2 20 mL/kg crystalloid | 2 | 125 | Risk Ratio (M‐H, Random, 95% CI) | 0.51 [0.11, 2.44] |
| 3.2 Nausea and/or vomiting | 1 | 80 | Risk Ratio (M‐H, Random, 95% CI) | 1.20 [0.40, 3.62] |
| 3.3 Apgar < 8 at 5 min | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 3.3.1 15 mL/kg crystalloid | 1 | 45 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 3.3.2 20 mL/kg crystalloid | 1 | 45 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 4. Crystalloid: rapid coload vs preload.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 4.1 Women with hypotension requiring intervention | 5 | 384 | Risk Ratio (M‐H, Random, 95% CI) | 0.70 [0.59, 0.83] |
| 4.2 Hypertension requiring intervention | 1 | 100 | Risk Ratio (M‐H, Random, 95% CI) | 1.67 [0.42, 6.60] |
| 4.3 Women with bradycardia | 1 | 100 | Risk Ratio (M‐H, Random, 95% CI) | 1.43 [0.59, 3.45] |
| 4.4 Women with nausea or vomiting | 3 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 4.4.1 Women with nausea | 3 | 210 | Risk Ratio (M‐H, Random, 95% CI) | 1.98 [1.26, 3.12] |
| 4.4.2 Women with vomiting | 2 | 160 | Risk Ratio (M‐H, Random, 95% CI) | 2.33 [0.98, 5.58] |
| 4.5 Neonates with acidosis (pH < 7.2) | 2 | 110 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 4.6 Apgar < 8 at 5 min | 3 | 210 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 5. Crystalloid: warm vs cold.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 5.1 Women with hypotension requiring intervention | 1 | 113 | Risk Ratio (M‐H, Random, 95% CI) | 1.03 [0.65, 1.62] |
| 5.2 Women with nausea and/or vomiting | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 5.2.1 Nausea | 1 | 113 | Risk Ratio (M‐H, Random, 95% CI) | 1.64 [0.97, 2.76] |
| 5.2.2 Vomiting | 1 | 113 | Risk Ratio (M‐H, Random, 95% CI) | 2.95 [0.12, 70.87] |
Comparison 6. Crystalloid vs another crystalloid.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 6.1 Women with hypotension requiring intervention | 3 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 6.1.1 Dextrose + saline vs saline | 1 | 120 | Risk Ratio (M‐H, Random, 95% CI) | 0.88 [0.68, 1.14] |
| 6.1.2 Glucose vs saline | 1 | 70 | Risk Ratio (M‐H, Random, 95% CI) | 1.05 [0.74, 1.48] |
| 6.1.3 Ringer's lactate vs saline | 1 | 60 | Risk Ratio (M‐H, Random, 95% CI) | 1.17 [0.65, 2.09] |
| 6.2 Neonates with acidosis: Ringer's lactate vs saline | 1 | 60 | Risk Ratio (M‐H, Fixed, 95% CI) | Not estimable |
| 6.3 Neonates with acidosis: dextrose vs saline | 1 | 120 | Risk Ratio (M‐H, Random, 95% CI) | 1.20 [0.39, 3.72] |
| 6.4 Neonates with Apgar score < 7 at 5 min | 1 | 120 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 6.5 Neonates with Apgar score < 8 at 5 min | 1 | 60 | Risk Ratio (M‐H, Fixed, 95% CI) | Not estimable |
Comparison 7. Colloid vs crystalloid.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 7.1 Women with hypotension requiring intervention | 27 | 2009 | Risk Ratio (M‐H, Random, 95% CI) | 0.69 [0.58, 0.81] |
| 7.2 Women with hypertension requiring intervention | 3 | 327 | Risk Ratio (M‐H, Random, 95% CI) | 0.64 [0.09, 4.46] |
| 7.3 Women with cardiac dysrhythmia | 6 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 7.3.1 Tachycardia | 1 | 60 | Risk Ratio (M‐H, Random, 95% CI) | 1.10 [0.79, 1.53] |
| 7.3.2 Bradycardia | 5 | 413 | Risk Ratio (M‐H, Random, 95% CI) | 0.98 [0.54, 1.78] |
| 7.4 Women with nausea and/or vomiting | 15 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 7.4.1 Nausea and/or vomiting | 14 | 1058 | Risk Ratio (M‐H, Random, 95% CI) | 0.89 [0.66, 1.19] |
| 7.4.2 Nausea | 5 | 390 | Risk Ratio (M‐H, Random, 95% CI) | 1.10 [0.77, 1.58] |
| 7.4.3 Vomiting | 4 | 320 | Risk Ratio (M‐H, Random, 95% CI) | 1.35 [0.55, 3.27] |
| 7.5 Neonates with acidosis (pH < 7.2) | 6 | 678 | Risk Ratio (M‐H, Random, 95% CI) | 0.83 [0.15, 4.52] |
| 7.6 Neonates: Apgar score | 12 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 7.6.1 Apgar < 7 at 5 min | 2 | 127 | Risk Ratio (M‐H, Random, 95% CI) | 0.16 [0.01, 2.90] |
| 7.6.2 Apgar < 8 at 5 min | 10 | 730 | Risk Ratio (M‐H, Random, 95% CI) | 0.24 [0.03, 2.05] |
Comparison 8. Colloid vs control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 8.1 Women with hypotension requiring intervention | 5 | 426 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.16, 0.96] |
| 8.2 Women with bradycardia | 1 | 54 | Risk Ratio (M‐H, Random, 95% CI) | 7.70 [0.46, 127.78] |
| 8.3 Women with nausea and/or vomiting | 2 | 245 | Risk Ratio (M‐H, Random, 95% CI) | 1.65 [0.75, 3.64] |
| 8.4 Neonates with acidosis (pH < 7.2) | 1 | 205 | Risk Ratio (M‐H, Random, 95% CI) | 1.24 [0.34, 4.48] |
| 8.5 Neonates with Apgar score < 7 at 5 min | 4 | 221 | Risk Ratio (M‐H, Random, 95% CI) | 0.07 [0.00, 1.24] |
| 8.6 Neonatal Apgar < 8 at 5 min | 1 | 205 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 9. Colloid: different volumes.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 9.1 Women with hypotension requiring intervention | 3 | 134 | Risk Ratio (M‐H, Random, 95% CI) | 0.75 [0.27, 2.08] |
| 9.2 Apgar < 9 at 5 min | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only |
Comparison 10. Colloid preload vs colloid coload.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 10.1 Women with hypotension requiring intervention | 4 | 320 | Risk Ratio (M‐H, Random, 95% CI) | 0.93 [0.78, 1.10] |
| 10.2 Women with cardiac dysrhythmia | 3 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 10.2.1 Bradycardia | 2 | 82 | Risk Ratio (M‐H, Random, 95% CI) | 0.75 [0.20, 2.88] |
| 10.2.2 Tachycardia | 1 | 46 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 10.3 Women with nausea and/or vomiting | 2 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 10.3.1 Nausea and/or vomiting | 1 | 178 | Risk Ratio (M‐H, Random, 95% CI) | 0.92 [0.63, 1.35] |
| 10.3.2 Nausea | 1 | 46 | Risk Ratio (M‐H, Random, 95% CI) | 1.00 [0.15, 6.51] |
| 10.3.3 Vomiting | 1 | 46 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 10.4 Women with anaphylaxis | 1 | 178 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 10.5 Neonates with Apgar score < 7 at 5 min | 1 | 36 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 11. Colloid + crystalloid vs another colloid + crystalloid.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 11.1 Women with hypotension requiring intervention | 2 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 11.1.1 Albumin or dextrose vs dextrose | 1 | 45 | Risk Ratio (M‐H, Random, 95% CI) | 0.13 [0.01, 2.30] |
| 11.1.2 Unbalanced vs balanced hydroxyethyl starch | 1 | 51 | Risk Ratio (M‐H, Random, 95% CI) | 1.04 [0.78, 1.39] |
| 11.2 Neonates: Apgar score < 7 | 1 | 45 | Risk Ratio (M‐H, Random, 95% CI) | 0.13 [0.01, 2.30] |
| 11.2.1 Albumin or dextrose vs dextrose | 1 | 45 | Risk Ratio (M‐H, Random, 95% CI) | 0.13 [0.01, 2.30] |
| 11.3 Neonates with Apgar score < 8 at 5 min | 1 | 51 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 11.3.1 Unbalanced vs balanced hydroxyethyl starch | 1 | 51 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 12. Ephedrine vs control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 12.1 Women with hypotension requiring intervention | 22 | 1401 | Risk Ratio (M‐H, Random, 95% CI) | 0.65 [0.53, 0.80] |
| 12.2 Women with hypertension requiring intervention | 7 | 520 | Risk Ratio (M‐H, Random, 95% CI) | 1.61 [1.00, 2.61] |
| 12.3 Women with cardiac arrhythmia | 3 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 12.3.1 Tachycardia | 2 | 93 | Risk Ratio (M‐H, Random, 95% CI) | 1.12 [0.74, 1.70] |
| 12.3.2 Bradycardia | 2 | 103 | Risk Ratio (M‐H, Random, 95% CI) | 14.46 [0.87, 241.09] |
| 12.4 Women with nausea and/or vomiting | 13 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 12.4.1 Nausea and/or vomiting | 5 | 219 | Risk Ratio (M‐H, Random, 95% CI) | 0.71 [0.22, 2.34] |
| 12.4.2 Nausea | 8 | 620 | Risk Ratio (M‐H, Random, 95% CI) | 0.68 [0.48, 0.96] |
| 12.4.3 Vomiting | 6 | 516 | Risk Ratio (M‐H, Random, 95% CI) | 0.68 [0.44, 1.07] |
| 12.5 Neonates with acidosis (pH < 7.2) | 9 | 576 | Risk Ratio (M‐H, Random, 95% CI) | 1.29 [0.67, 2.49] |
| 12.6 Neonates: Apgar score | 14 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 12.6.1 Apgar < 8 at 5 min | 10 | 579 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 12.6.2 Apgar < 7 at 5 min | 4 | 263 | Risk Ratio (M‐H, Random, 95% CI) | 1.14 [0.34, 3.81] |
Comparison 13. Ephedrine vs crystalloid.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 13.1 Women with hypotension requiring intervention | 9 | 613 | Risk Ratio (M‐H, Random, 95% CI) | 0.60 [0.47, 0.78] |
| 13.2 Women with hypertension requiring intervention | 3 | 280 | Risk Ratio (M‐H, Random, 95% CI) | 1.10 [0.37, 3.28] |
| 13.3 Women with bradycardia | 1 | 100 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.01, 7.99] |
| 13.4 Women with nausea and/or vomiting | 5 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 13.4.1 Nausea and/or vomiting | 2 | 146 | Risk Ratio (M‐H, Random, 95% CI) | 1.00 [0.48, 2.08] |
| 13.4.2 Nausea | 3 | 220 | Risk Ratio (M‐H, Random, 95% CI) | 0.54 [0.31, 0.93] |
| 13.4.3 Vomiting | 3 | 220 | Risk Ratio (M‐H, Random, 95% CI) | 0.57 [0.31, 1.05] |
| 13.5 Women with impaired consciousness | 1 | 46 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.09, 1.86] |
| 13.6 Neonates with acidosis (pH < 7.2) | 2 | 218 | Risk Ratio (M‐H, Random, 95% CI) | 1.41 [0.48, 4.15] |
| 13.7 Neonatal Apgar score | 5 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 13.7.1 Apgar < 8 at 5 min | 4 | 226 | Risk Ratio (M‐H, Random, 95% CI) | 3.00 [0.13, 71.92] |
| 13.7.2 Apgar < 7 at 5 min | 1 | 120 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 14. Ephedrine + crystalloid vs colloid.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 14.1 Women with hypotension requiring intervention | 1 | 75 | Risk Ratio (M‐H, Random, 95% CI) | 0.65 [0.38, 1.12] |
| 14.2 Women with nausea and/or vomiting | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 14.2.1 Nausea | 1 | 75 | Risk Ratio (M‐H, Random, 95% CI) | 0.42 [0.22, 0.81] |
| 14.2.2 Vomiting | 1 | 75 | Risk Ratio (M‐H, Random, 95% CI) | 0.17 [0.04, 0.77] |
Comparison 15. Ephedrine + colloid vs crystalloid.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 15.1 Women with hypotension requiring intervention | 1 | 75 | Risk Ratio (M‐H, Random, 95% CI) | 0.39 [0.21, 0.74] |
| 15.2 Women with nausea and/or vomiting | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 15.2.1 Nausea | 1 | 75 | Risk Ratio (M‐H, Random, 95% CI) | 0.27 [0.11, 0.65] |
| 15.2.2 Vomiting | 1 | 75 | Risk Ratio (M‐H, Random, 95% CI) | 0.38 [0.09, 1.55] |
Comparison 16. Ephedrine vs phenylephrine.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 16.1 Women with hypotension requiring intervention | 8 | 401 | Risk Ratio (M‐H, Random, 95% CI) | 0.92 [0.71, 1.18] |
| 16.2 Women with hypertension requiring intervention | 2 | 118 | Risk Ratio (M‐H, Random, 95% CI) | 1.72 [0.71, 4.16] |
| 16.3 Cardiac dysrhythmia | 5 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 16.3.1 Bradycardia | 5 | 304 | Risk Ratio (M‐H, Random, 95% CI) | 0.37 [0.21, 0.64] |
| 16.3.2 Tachycardia | 1 | 57 | Risk Ratio (M‐H, Random, 95% CI) | 2.22 [0.44, 11.18] |
| 16.4 Women with nausea and/or vomiting | 4 | 204 | Risk Ratio (M‐H, Random, 95% CI) | 0.76 [0.39, 1.49] |
| 16.5 Neonates with acidosis (pH < 7.2) | 3 | 175 | Risk Ratio (M‐H, Random, 95% CI) | 0.89 [0.07, 12.00] |
| 16.6 Neonates with Apgar score < 8 at 5 min | 6 | 321 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 17. Ephedrine vs angiotensin.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 17.1 Women with hypotension requiring intervention | 1 | 20 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 17.2 Women with nausea and/or vomiting | 1 | 20 | Risk Ratio (M‐H, Random, 95% CI) | 3.00 [0.14, 65.90] |
| 17.3 Neonates with acidosis (pH < 7.2) | 1 | 20 | Risk Ratio (M‐H, Random, 95% CI) | 9.00 [0.55, 147.95] |
Comparison 18. Ephedrine vs colloid.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 18.1 Women with hypotension requiring intervention | 2 | 160 | Risk Ratio (M‐H, Random, 95% CI) | 0.53 [0.36, 0.79] |
| 18.2 Women with hypertension requiring intervention | 1 | 100 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.00 [0.32, 27.87] |
| 18.3 Women with bradycardia | 1 | 100 | Risk Ratio (M‐H, Fixed, 95% CI) | Not estimable |
| 18.4 Women with nausea and vomiting | 2 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 18.4.1 Women with nausea and/or vomiting | 1 | 100 | Risk Ratio (M‐H, Random, 95% CI) | 5.00 [0.25, 101.58] |
| 18.4.2 Women with nausea | 1 | 60 | Risk Ratio (M‐H, Random, 95% CI) | 0.22 [0.05, 0.94] |
| 18.4.3 Women with vomiting | 1 | 60 | Risk Ratio (M‐H, Random, 95% CI) | 0.14 [0.01, 2.65] |
| 18.5 5 Neonates with acidosis (pH < 7.2) | 1 | 100 | Risk Ratio (M‐H, Fixed, 95% CI) | Not estimable |
| 18.6 Apgar score < 8 at 5 min | 2 | 160 | Risk Ratio (M‐H, Random, 95% CI) | 3.00 [0.13, 71.92] |
Comparison 19. Ephedrine vs metaraminol.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 19.1 Women with hypotension requiring intervention | 1 | 53 | Risk Ratio (M‐H, Random, 95% CI) | 1.56 [0.50, 4.89] |
| 19.2 Women with hypertension requiring intervention | 1 | 53 | Risk Ratio (M‐H, Random, 95% CI) | 0.62 [0.26, 1.47] |
| 19.3 Women with bradycardia | 1 | 53 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 19.4 Women with nausea and/or vomiting | 1 | 53 | Risk Ratio (M‐H, Random, 95% CI) | 7.26 [0.39, 134.01] |
| 19.5 5 Neonates with acidosis (pH < 7.2) | 1 | 53 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 19.6 Neonatal Apgar score < 8 at 5 min | 1 | 53 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 20. Ephedrine: different doses.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 20.1 Women with hypotension requiring intervention | 6 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 20.1.1 5 mg vs 10 mg | 2 | 100 | Risk Ratio (M‐H, Random, 95% CI) | 1.05 [0.65, 1.69] |
| 20.1.2 6 mg vs 12 mg | 1 | 46 | Risk Ratio (M‐H, Random, 95% CI) | 1.83 [0.83, 4.04] |
| 20.1.3 5 mg vs 15 mg | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 2.00 [0.94, 4.27] |
| 20.1.4 10 mg vs 15 mg | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 1.83 [0.84, 3.99] |
| 20.1.5 10 mg vs 20 mg | 2 | 60 | Risk Ratio (M‐H, Random, 95% CI) | 1.06 [0.80, 1.39] |
| 20.1.6 10 mg vs 30 mg | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 2.43 [1.30, 4.54] |
| 20.1.7 15 mg vs 30 mg | 1 | 100 | Risk Ratio (M‐H, Random, 95% CI) | 2.11 [1.06, 4.21] |
| 20.1.8 20 mg vs 30 mg | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 2.29 [1.21, 4.32] |
| 20.2 Women with hypertension requiring intervention | 2 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 20.2.1 5 mg vs 10 mg | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 1.20 [0.44, 3.30] |
| 20.2.2 5 mg vs 15 mg | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.50 [0.23, 1.07] |
| 20.2.3 10 mg vs 15 mg | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.42 [0.18, 0.96] |
| 20.2.4 10 mg vs 20 mg | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.20 [0.03, 1.56] |
| 20.2.5 10 mg vs 30 mg | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.11 [0.02, 0.80] |
| 20.2.6 20 mg vs 30 mg | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.56 [0.23, 1.37] |
| 20.3 Women with nausea and/or vomiting | 4 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 20.3.1 6 mg vs 12 mg (nausea and/or vomiting) | 1 | 46 | Risk Ratio (M‐H, Random, 95% CI) | 0.81 [0.38, 1.74] |
| 20.3.2 5 mg vs 10 mg (vomiting) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 3.00 [0.34, 26.45] |
| 20.3.3 5 mg vs 15 mg (vomiting) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 1.50 [0.28, 8.04] |
| 20.3.4 10 mg vs 15 mg (vomiting) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.50 [0.05, 5.08] |
| 20.3.5 5 mg vs 10 mg (nausea) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 2.00 [0.83, 4.81] |
| 20.3.6 5 mg vs 15 mg (nausea) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 2.50 [0.94, 6.66] |
| 20.3.7 10 mg vs 15 mg (nausea) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 1.25 [0.39, 3.99] |
| 20.3.8 10 mg vs 20 mg (nausea) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.69 [0.39, 1.24] |
| 20.3.9 10 mg vs 30 mg (nausea) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 1.80 [0.73, 4.43] |
| 20.3.10 15 mg vs 30 mg (nausea) | 1 | 100 | Risk Ratio (M‐H, Random, 95% CI) | 1.43 [0.59, 3.45] |
| 20.3.11 20 mg vs 30 mg (nausea) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 2.60 [1.14, 5.93] |
| 20.3.12 15 mg vs 30 mg (vomiting) | 1 | 100 | Risk Ratio (M‐H, Random, 95% CI) | 0.67 [0.12, 3.82] |
| 20.4 Neonates with acidosis (pH < 7.2) | 3 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 20.4.1 5 mg vs 10 mg | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.20 [0.01, 3.92] |
| 20.4.2 5 mg vs 15 mg | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.33 [0.01, 7.72] |
| 20.4.3 6 mg vs 12 mg | 1 | 46 | Risk Ratio (M‐H, Random, 95% CI) | 0.31 [0.01, 7.16] |
| 20.4.4 10 mg vs 15 mg | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 2.00 [0.20, 20.33] |
| 20.4.5 10 mg vs 20 mg | 1 | 39 | Risk Ratio (M‐H, Random, 95% CI) | 0.59 [0.24, 1.50] |
| 20.4.6 10 mg vs 30 mg | 1 | 38 | Risk Ratio (M‐H, Random, 95% CI) | 1.12 [0.36, 3.55] |
| 20.4.7 20 mg vs 30 mg | 1 | 37 | Risk Ratio (M‐H, Random, 95% CI) | 1.89 [0.69, 5.21] |
| 20.5 Neonatal Apgar score at 5 min | 4 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 20.5.1 6 mg vs 12 mg (Apgar < 7) | 1 | 46 | Risk Ratio (M‐H, Random, 95% CI) | 0.31 [0.01, 7.16] |
| 20.5.2 5 mg vs 10 mg (Apgar < 8) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 20.5.3 5 mg vs 15 mg (Apgar < 8) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 20.5.4 10 mg vs 15 mg (Apgar < 8) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 20.5.5 10 mg vs 20 mg (Apgar < 7) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 20.5.6 10 mg vs 30 mg (Apgar < 7) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 20.5.7 20 mg vs 30 mg (Apgar < 7) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 20.5.8 10 mg vs 20 mg (Apgar < 8) | 1 | 20 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 21. Ephedrine: different rates.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 21.1 Women with hypotension requiring intervention | 4 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 21.1.1 Bolus + infusion vs infusion | 1 | 80 | Risk Ratio (M‐H, Random, 95% CI) | 3.50 [1.26, 9.72] |
| 21.1.2 0.5 mg/min vs 1 mg/min | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 1.22 [0.65, 2.29] |
| 21.1.3 0.5 mg/min vs 2 mg/min | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 1.57 [0.77, 3.22] |
| 21.1.4 0.5 mg/min vs 4 mg/min | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 1.22 [0.65, 2.29] |
| 21.1.5 1 mg/min vs 2 mg/min | 3 | 107 | Risk Ratio (M‐H, Random, 95% CI) | 1.24 [0.83, 1.84] |
| 21.1.6 1 mg/min vs 3 to 4 mg/min | 2 | 99 | Risk Ratio (M‐H, Random, 95% CI) | 1.29 [0.81, 2.05] |
| 21.1.7 2 mg/min vs 3 to 4 mg/min | 2 | 239 | Risk Ratio (M‐H, Random, 95% CI) | 1.21 [0.60, 2.43] |
| 21.2 Women with hypertension requiring intervention | 2 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 21.2.1 Bolus + infusion vs infusion | 1 | 80 | Risk Ratio (M‐H, Random, 95% CI) | 1.00 [0.39, 2.59] |
| 21.2.2 0.5 mg/min vs 1 mg/min | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 5.00 [0.26, 98.00] |
| 21.2.3 0.5 mg/min vs 2 mg/min | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.67 [0.12, 3.57] |
| 21.2.4 0.5 mg/min vs 4 mg/min | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.20 [0.05, 0.80] |
| 21.2.5 1 mg/min vs 2 mg/min | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.14 [0.01, 2.60] |
| 21.2.6 1 mg/min vs 4 mg/min | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.05 [0.00, 0.76] |
| 21.2.7 2 mg/min vs 4 mg/min | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.30 [0.10, 0.93] |
| 21.3 Women with bradycardia | 1 | 19 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 21.3.1 1 mg/min vs 2 mg/min | 1 | 19 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 21.4 Women with nausea and/or vomiting | 3 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 21.4.1 Bolus + infusion vs infusion (nausea) | 1 | 80 | Risk Ratio (M‐H, Random, 95% CI) | 1.83 [0.75, 4.48] |
| 21.4.2 0.5 mg/min vs 1 mg/min (nausea) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 1.29 [0.60, 2.77] |
| 21.4.3 0.5 mg/min vs 2 mg/min (nausea) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 1.50 [0.66, 3.43] |
| 21.4.4 0.5 mg/min vs 4 mg/min (nausea) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 1.29 [0.60, 2.77] |
| 21.4.5 1 mg/min vs 2 mg/min (nausea) | 2 | 60 | Risk Ratio (M‐H, Random, 95% CI) | 2.19 [0.30, 15.85] |
| 21.4.6 1 mg/min vs 4 mg/min (nausea) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 1.00 [0.43, 2.33] |
| 21.4.7 2 mg/min vs 4 mg/min (nausea) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.86 [0.35, 2.10] |
| 21.4.8 Bolus + infusion vs infusion (vomiting) | 1 | 80 | Risk Ratio (M‐H, Random, 95% CI) | 1.67 [0.43, 6.51] |
| 21.4.9 0.5 mg/min vs 1 mg/min (vomiting) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.67 [0.12, 3.57] |
| 21.4.10 0.5 mg/min vs 2 mg/min (vomiting) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 2.00 [0.20, 20.33] |
| 21.4.11 0.5 mg/min vs 4 mg/min (vomiting) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 2.00 [0.20, 20.33] |
| 21.4.12 1 mg/min vs 2 mg/min (vomiting) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 3.00 [0.34, 26.45] |
| 21.4.13 1 mg/min vs 4 mg/min (vomiting) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 3.00 [0.34, 26.45] |
| 21.4.14 2 mg/min vs 4 mg/min (vomiting) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 1.00 [0.07, 14.90] |
| 21.4.15 1 mg/min vs 2 mg/min (nausea or vomiting) | 1 | 19 | Risk Ratio (M‐H, Random, 95% CI) | 8.18 [0.50, 133.66] |
| 21.5 Neonates with acidosis (pH < 7.2) | 2 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 21.5.1 Bolus + infusion vs infusion | 1 | 78 | Risk Ratio (M‐H, Random, 95% CI) | 1.66 [0.53, 5.23] |
| 21.5.2 0.5 mg/min vs 1 mg/min | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.33 [0.04, 2.94] |
| 21.5.3 0.5 mg/min vs 2 mg/min | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 3.00 [0.13, 69.52] |
| 21.5.4 0.5 mg/min vs 4 mg/min | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.25 [0.03, 2.05] |
| 21.5.5 1 mg/min vs 2 mg/min | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 7.00 [0.38, 127.32] |
| 21.5.6 1 mg/min vs 4 mg/min | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.75 [0.19, 2.93] |
| 21.5.7 2 mg/min vs 4 mg/min | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.11 [0.01, 1.94] |
| 21.6 Neonatal Apgar score at 5 min | 3 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 21.6.1 Bolus + infusion vs infusion (Apgar < 7) | 1 | 80 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 21.6.2 0.5 mg/min vs 1 mg/min (Apgar < 8) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 21.6.3 0.5 mg/min vs 2 mg/min (Apgar < 8) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 21.6.4 0.5 mg/min vs 4 mg/min (Apgar < 8) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 21.6.5 1 mg/min vs 2 mg/min (Apgar < 8) | 2 | 59 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 21.6.6 1 mg/min vs 4 mg/min (Apgar < 8) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 21.6.7 2 mg/min vs 4 mg/min (Apgar < 8) | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
21.2. Analysis.

Comparison 21: Ephedrine: different rates, Outcome 2: Women with hypertension requiring intervention
Comparison 22. Ephedrine: oral vs IM or IV.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 22.1 Women with hypotension requiring intervention | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 22.1.1 Oral vs IM | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 3.00 [0.95, 9.48] |
| 22.1.2 Oral vs IV | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 19.00 [1.18, 305.88] |
| 22.2 Women with hypertension requiring intervention | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 22.2.1 Oral vs IM | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 22.2.2 Oral vs IV | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 22.3 Women with nausea and vomiting | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 22.3.1 Oral vs IM | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 1.33 [0.34, 5.21] |
| 22.3.2 Oral vs IV | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 9.00 [0.52, 156.91] |
Comparison 23. Ephedrine: IM vs IV.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 23.1 Women with hypotension requiring intervention | 1 | 60 | Risk Ratio (M‐H, Random, 95% CI) | 0.75 [0.43, 1.30] |
| 23.2 Women with hypertension requiring intervention | 1 | 60 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 23.3 Apgar < 8 at 5 min | 1 | 60 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 24. Phenylephrine vs control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 24.1 Women with hypotension requiring intervention | 5 | 280 | Risk Ratio (M‐H, Random, 95% CI) | 0.45 [0.26, 0.80] |
| 24.2 Women with cardiac dysrhythmia | 3 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 24.2.1 Tachycardia | 1 | 56 | Risk Ratio (M‐H, Random, 95% CI) | 0.87 [0.13, 5.73] |
| 24.2.2 Bradycardia | 3 | 180 | Risk Ratio (M‐H, Random, 95% CI) | 3.23 [0.17, 61.85] |
| 24.3 Women with nausea and/or vomiting | 3 | 180 | Risk Ratio (M‐H, Random, 95% CI) | 0.70 [0.16, 2.98] |
| 24.4 Neonates with acidosis (pH < 7.2) | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 0.96 [0.06, 14.50] |
| 24.5 Neonates with Apgar < 7 at 5 min | 1 | 50 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 24.6 Neonates with Apgar < 8 at 5 min | 2 | 96 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 25. Phenylephrine vs mephentermine.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 25.1 Women with hypotension requiring intervention | 1 | 60 | Risk Ratio (M‐H, Random, 95% CI) | 2.00 [0.19, 20.90] |
| 25.2 Women with hypertension requiring intervention | 1 | 60 | Risk Ratio (M‐H, Random, 95% CI) | 17.00 [1.03, 281.91] |
| 25.3 Cardiac dysrhythmia | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 25.3.1 Bradycardia | 1 | 60 | Risk Ratio (M‐H, Random, 95% CI) | 15.00 [0.89, 251.42] |
| 25.4 Nausea and/or vomiting | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 25.4.1 Nausea | 1 | 60 | Risk Ratio (M‐H, Random, 95% CI) | 0.20 [0.01, 4.00] |
| 25.4.2 Vomiting | 1 | 60 | Risk Ratio (M‐H, Random, 95% CI) | 1.00 [0.07, 15.26] |
Comparison 26. Phenylephrine vs metaraminol.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 26.1 Women with hypotension requiring intervention | 1 | 59 | Risk Ratio (M‐H, Random, 95% CI) | 0.84 [0.23, 3.06] |
| 26.2 Women with hypertension requiring intervention | 1 | 59 | Risk Ratio (M‐H, Random, 95% CI) | 0.25 [0.08, 0.83] |
| 26.3 Women with bradycardia | 1 | 59 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 26.4 Women with nausea and/or vomiting | 1 | 59 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 26.5 Neonatal pH < 7.2 | 1 | 59 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 26.6 Neonatal Apgar score < 8 at 5 min | 1 | 59 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 27. Phenylephrine vs leg compression.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 27.1 Women with hypotension requiring intervention | 1 | 76 | Risk Ratio (M‐H, Random, 95% CI) | 0.73 [0.46, 1.15] |
| 27.2 Women with bradycardia | 1 | 76 | Risk Ratio (M‐H, Random, 95% CI) | 0.50 [0.05, 5.28] |
| 27.3 Women with nausea and/or vomiting | 1 | 76 | Risk Ratio (M‐H, Random, 95% CI) | 1.00 [0.32, 3.17] |
Comparison 28. Phenylephrine: infusion vs bolus.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 28.1 Women with hypotension requiring intervention | 1 | 60 | Risk Ratio (M‐H, Random, 95% CI) | 1.40 [0.50, 3.92] |
| 28.2 Women with cardiac dysrhythmia | 1 | 60 | Risk Ratio (M‐H, Random, 95% CI) | 1.22 [0.59, 2.51] |
| 28.2.1 Bradycardia | 1 | 60 | Risk Ratio (M‐H, Random, 95% CI) | 1.22 [0.59, 2.51] |
| 28.3 Women with nausea/vomiting | 1 | 60 | Risk Ratio (M‐H, Random, 95% CI) | 0.45 [0.18, 1.15] |
| 28.4 Neonatal Apgar score < 8 at 5 min | 1 | 60 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 29. Phenylephrine: different doses.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 29.1 Women with hypotension requiring intervention | 1 | 117 | Risk Ratio (M‐H, Random, 95% CI) | 8.17 [1.04, 64.30] |
| 29.1.1 50 μg/mL vs 100 μg/mL | 1 | 117 | Risk Ratio (M‐H, Random, 95% CI) | 8.17 [1.04, 64.30] |
| 29.2 Women with hypertension requiring intervention | 1 | 117 | Risk Ratio (M‐H, Random, 95% CI) | 0.23 [0.05, 1.02] |
| 29.2.1 50 μg/mL vs 100 μg/mL | 1 | 117 | Risk Ratio (M‐H, Random, 95% CI) | 0.23 [0.05, 1.02] |
| 29.3 Women with cardiac dysrhythmia | 1 | 117 | Risk Ratio (M‐H, Random, 95% CI) | 0.11 [0.01, 0.80] |
| 29.3.1 Bradycardia: 50 μg/mL vs 100 μg/mL | 1 | 117 | Risk Ratio (M‐H, Random, 95% CI) | 0.11 [0.01, 0.80] |
| 29.4 Women with nausea and/or vomiting | 1 | 117 | Risk Ratio (M‐H, Random, 95% CI) | 3.50 [0.37, 32.67] |
| 29.4.1 Nausea and vomiting: 50 μg/mL vs 100 μg/mL | 1 | 117 | Risk Ratio (M‐H, Random, 95% CI) | 3.50 [0.37, 32.67] |
| 29.5 Neonatal cord blood pH < 7.2 | 1 | 117 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 29.5.1 50 μg/mL vs 100 μg/mL | 1 | 117 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 29.6 Neonatal Apgar score < 8 at 5 min | 1 | 117 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 29.6.1 50 μg/mL vs 100 μg/mL | 1 | 117 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 30. Glycopyrrolate vs control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 30.1 Women with hypotension requiring intervention | 2 | 142 | Risk Ratio (M‐H, Random, 95% CI) | 0.63 [0.21, 1.91] |
| 30.2 Women with hypertension requiring intervention | 1 | 93 | Risk Ratio (M‐H, Random, 95% CI) | 2.67 [1.31, 5.43] |
| 30.3 Women with bradycardia | 1 | 93 | Risk Ratio (M‐H, Random, 95% CI) | 0.21 [0.01, 4.32] |
| 30.4 Women with nausea and/or vomiting | 2 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 30.4.1 Nausea or vomiting | 1 | 93 | Risk Ratio (M‐H, Random, 95% CI) | 2.49 [0.69, 9.04] |
| 30.4.2 Nausea | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 0.61 [0.36, 1.06] |
| 30.4.3 Vomiting | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 0.52 [0.10, 2.59] |
| 30.5 Neonates with Apgar score < 8 at 5 min | 2 | 142 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 31. Ondansetron vs control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 31.1 Women with hypotension requiring intervention | 8 | 740 | Risk Ratio (M‐H, Random, 95% CI) | 0.67 [0.54, 0.83] |
| 31.1.1 2 mg vs control | 2 | 79 | Risk Ratio (M‐H, Random, 95% CI) | 0.90 [0.51, 1.58] |
| 31.1.2 4 mg vs control | 5 | 277 | Risk Ratio (M‐H, Random, 95% CI) | 0.46 [0.34, 0.63] |
| 31.1.3 6 mg vs control | 1 | 38 | Risk Ratio (M‐H, Random, 95% CI) | 0.48 [0.22, 1.03] |
| 31.1.4 8 mg vs control | 5 | 346 | Risk Ratio (M‐H, Random, 95% CI) | 0.85 [0.70, 1.03] |
| 31.2 Women with bradycardia | 8 | 740 | Risk Ratio (M‐H, Random, 95% CI) | 0.49 [0.28, 0.87] |
| 31.2.1 2 mg vs control | 2 | 79 | Risk Ratio (M‐H, Random, 95% CI) | 0.23 [0.02, 3.29] |
| 31.2.2 4 mg vs control | 5 | 277 | Risk Ratio (M‐H, Random, 95% CI) | 0.33 [0.16, 0.71] |
| 31.2.3 6 mg vs control | 1 | 38 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 31.2.4 8 mg vs control | 5 | 346 | Risk Ratio (M‐H, Random, 95% CI) | 0.94 [0.38, 2.37] |
| 31.3 Women with nausea or vomiting | 7 | 653 | Risk Ratio (M‐H, Random, 95% CI) | 0.35 [0.24, 0.51] |
| 31.3.1 2 mg vs control | 2 | 79 | Risk Ratio (M‐H, Random, 95% CI) | 0.54 [0.18, 1.59] |
| 31.3.2 4 mg vs control | 5 | 277 | Risk Ratio (M‐H, Random, 95% CI) | 0.32 [0.17, 0.60] |
| 31.3.3 6 mg vs control | 1 | 38 | Risk Ratio (M‐H, Random, 95% CI) | 0.09 [0.01, 0.74] |
| 31.3.4 8 mg vs control | 4 | 259 | Risk Ratio (M‐H, Random, 95% CI) | 0.38 [0.19, 0.76] |
| 31.4 Women with anaphylaxis | 1 | 150 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 31.4.1 2 mg vs control | 1 | 37 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 31.4.2 4 mg vs control | 1 | 37 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 31.4.3 6 mg vs control | 1 | 38 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 31.4.4 8 mg vs control | 1 | 38 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 31.5 Neonatal Apgar score < 8 at 5 min | 3 | 284 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 31.5.1 2 mg vs control | 1 | 37 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 31.5.2 4 mg vs control | 2 | 102 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 31.5.3 6 mg vs control | 1 | 38 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 31.5.4 8 mg vs control | 2 | 107 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 31.6 Neonatal pH < 7.2 | 2 | 134 | Risk Ratio (M‐H, Random, 95% CI) | 0.48 [0.05, 5.09] |
| 31.6.1 4 mg vs control | 1 | 65 | Risk Ratio (M‐H, Random, 95% CI) | 0.48 [0.05, 5.09] |
| 31.6.2 8 mg vs control | 1 | 69 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 32. Ondansetron vs ephedrine.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 32.1 Women with hypotension requiring intervention | 1 | 112 | Risk Ratio (M‐H, Random, 95% CI) | 1.07 [0.76, 1.49] |
| 32.2 Women with bradycardia | 1 | 112 | Risk Ratio (M‐H, Random, 95% CI) | 3.00 [0.12, 72.10] |
| 32.3 Women with nausea and/or vomiting | 1 | 112 | Risk Ratio (M‐H, Random, 95% CI) | 0.38 [0.10, 1.34] |
Comparison 33. Granisetron vs control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 33.1 Women with hypotension requiring intervention | 1 | 200 | Risk Ratio (M‐H, Random, 95% CI) | 0.05 [0.02, 0.14] |
Comparison 34. Ketamine vs saline.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 34.1 Women with hypotension requiring intervention | 1 | 105 | Risk Ratio (M‐H, Random, 95% CI) | 0.79 [0.62, 1.01] |
| 34.1.1 0.25 mg/kg IV ketamine | 1 | 52 | Risk Ratio (M‐H, Random, 95% CI) | 0.83 [0.61, 1.14] |
| 34.1.2 0.5 mg/kg IV ketamine | 1 | 53 | Risk Ratio (M‐H, Random, 95% CI) | 0.73 [0.50, 1.07] |
| 34.2 Women with nausea and/or vomiting | 1 | 105 | Risk Ratio (M‐H, Random, 95% CI) | 0.79 [0.50, 1.25] |
| 34.2.1 0.25 mg/kg IV ketamine | 1 | 52 | Risk Ratio (M‐H, Random, 95% CI) | 0.91 [0.48, 1.71] |
| 34.2.2 0.5 mg/kg IV ketamine | 1 | 53 | Risk Ratio (M‐H, Random, 95% CI) | 0.69 [0.36, 1.31] |
| 34.3 Apgar score < 8 at 5 min | 1 | 105 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 34.3.1 0.25 mg/kg IV ketamine | 1 | 52 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 34.3.2 0.5 mg/kg IV ketamine | 1 | 53 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 35. Angiotensin vs control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 35.1 Women with hypotension requiring intervention | 1 | 20 | Risk Ratio (M‐H, Random, 95% CI) | 0.09 [0.01, 1.45] |
| 35.2 Women with nausea and/or vomiting | 1 | 20 | Risk Ratio (M‐H, Random, 95% CI) | 0.20 [0.01, 3.70] |
| 35.3 Neonates with acidosis (pH < 7.2) | 1 | 20 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 36. Dopamine vs control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 36.1 Women with hypotension requiring intervention | 1 | 30 | Risk Ratio (M‐H, Random, 95% CI) | 0.05 [0.00, 0.75] |
| 36.2 Neonatal Apgar score < 8 at 5 min | 1 | 30 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 37. Lower limb compression vs control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 37.1 Women with hypotension requiring intervention | 11 | 705 | Risk Ratio (M‐H, Random, 95% CI) | 0.61 [0.47, 0.78] |
| 37.2 Women with bradycardia | 1 | 74 | Risk Ratio (M‐H, Random, 95% CI) | 0.63 [0.11, 3.56] |
| 37.3 Women with nausea and/or vomiting | 4 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 37.3.1 Women with nausea and/or vomiting | 4 | 276 | Risk Ratio (M‐H, Random, 95% CI) | 0.42 [0.14, 1.27] |
| 37.3.2 Women with nausea | 1 | 92 | Risk Ratio (M‐H, Random, 95% CI) | 1.44 [0.25, 8.20] |
| 37.3.3 Women with vomiting | 1 | 92 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 37.4 Neonates with Apgar score < 8 at 5 min | 3 | 130 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 38. Wedge vs supine.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 38.1 Women with hypotension requiring intervention | 1 | 80 | Risk Ratio (M‐H, Random, 95% CI) | 0.85 [0.53, 1.37] |
| 38.2 Women with nausea and/or vomiting | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 38.2.1 Women with nausea | 1 | 80 | Risk Ratio (M‐H, Random, 95% CI) | 0.27 [0.12, 0.60] |
| 38.2.2 Women with vomiting | 1 | 80 | Risk Ratio (M‐H, Random, 95% CI) | 0.11 [0.01, 2.00] |
Comparison 39. Head‐up tilt vs horizontal.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 39.1 Women with hypotension requiring intervention | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.71 [0.47, 1.06] |
| 39.2 Neonates with Apgar score < 8 at 5 min | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 40. Head‐down tilt vs horizontal.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 40.1 Women with hypotension requiring intervention | 1 | 34 | Risk Ratio (M‐H, Random, 95% CI) | 1.07 [0.81, 1.42] |
Comparison 41. Crawford's wedge vs manual uterine displacement.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 41.1 Women with hypotension requiring intervention | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.92 [0.57, 1.49] |
| 41.2 Neonates with Apgar score < 8 at 5 min | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 42. Supine vs sitting.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 42.1 Women with hypotension requiring intervention | 1 | 98 | Risk Ratio (M‐H, Random, 95% CI) | 0.81 [0.58, 1.12] |
| 42.2 Women with nausea and/or vomiting | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 42.2.1 Nausea | 1 | 98 | Risk Ratio (M‐H, Random, 95% CI) | 0.65 [0.40, 1.07] |
| 42.2.2 Vomiting | 1 | 98 | Risk Ratio (M‐H, Random, 95% CI) | 0.38 [0.02, 9.01] |
| 42.3 Neonates with acidosis (pH < 7.2) | 1 | 98 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 42.4 Neonates with Apgar < 7 at 5 min | 1 | 98 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 43. Walking vs lying.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 43.1 Women requiring intervention for hypotension | 1 | 37 | Risk Ratio (M‐H, Random, 95% CI) | 0.71 [0.41, 1.21] |
Comparison 44. Lateral vs supine wedged position.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 44.1 Women with hypotension requiring intervention | 2 | 126 | Risk Ratio (M‐H, Random, 95% CI) | 0.91 [0.75, 1.09] |
| 44.2 Women with cardiac dysrhythmia requiring intervention | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.50 [0.05, 5.08] |
| 44.3 Neonates admitted to neonatal intensive care unit | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
| 44.4 Women with nausea | 1 | 86 | Risk Ratio (M‐H, Random, 95% CI) | 0.81 [0.45, 1.48] |
Comparison 45. Left lateral vs left lateral tilt.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 45.1 Women with hypotension requiring intervention | 1 | 58 | Risk Ratio (M‐H, Random, 95% CI) | 1.20 [0.80, 1.79] |
| 45.2 Women with cardiac dysrhythmia requiring intervention | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 45.2.1 Bradycardia | 1 | 58 | Risk Ratio (M‐H, Random, 95% CI) | 0.10 [0.01, 1.68] |
| 45.3 Women with nausea and/or vomiting | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 45.3.1 Nausea: 15 degree tilt | 1 | 58 | Risk Ratio (M‐H, Random, 95% CI) | 0.45 [0.18, 1.11] |
| 45.3.2 Vomiting: 15 degree tilt | 1 | 58 | Risk Ratio (M‐H, Random, 95% CI) | 0.15 [0.01, 2.83] |
Comparison 46. Left lateral tilt vs left manual uterine displacement.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 46.1 Women with hypotension requiring intervention | 1 | 90 | Risk Ratio (M‐H, Random, 95% CI) | 0.63 [0.49, 0.80] |
Comparison 47. Leg elevation vs control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 47.1 Women with hypotension requiring intervention | 1 | 63 | Risk Ratio (M‐H, Random, 95% CI) | 0.73 [0.42, 1.26] |
Comparison 48. Acupressure vs placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 48.1 Women with hypotension requiring intervention | 1 | 50 | Risk Ratio (M‐H, Random, 95% CI) | 0.84 [0.58, 1.22] |
| 48.2 Women with nausea and/or vomiting | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 48.2.1 Nausea | 1 | 50 | Risk Ratio (M‐H, Random, 95% CI) | 0.32 [0.15, 0.66] |
| 48.2.2 Vomiting | 1 | 50 | Risk Ratio (M‐H, Random, 95% CI) | 0.50 [0.14, 1.78] |
| 48.3 Neonates with Apgar < 7 at 5 min | 1 | 50 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Comparison 49. Acupressure vs metoclopramide.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 49.1 Women with hypotension requiring intervention | 1 | 50 | Risk Ratio (M‐H, Random, 95% CI) | 0.94 [0.63, 1.40] |
| 49.2 Women with nausea and/or vomiting | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 49.2.1 Nausea | 1 | 50 | Risk Ratio (M‐H, Random, 95% CI) | 1.50 [0.48, 4.68] |
| 49.2.2 Vomiting | 1 | 50 | Risk Ratio (M‐H, Random, 95% CI) | 3.00 [0.33, 26.92] |
| 49.3 Neonates with Apgar < 7 at 5 min | 1 | 50 | Risk Ratio (M‐H, Random, 95% CI) | Not estimable |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Adsumelli 2003.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 50 women Inclusion criteria: healthy term parturients, elective CS under spinal anaesthesia, ASA I‐II. Exclusion criteria: women with chronic hypertension, multiple pregnancy, pregnancy‐induced hypertension, diabetes mellitus, body weight > 110 kg and contraindications to a spinal anaesthetic Setting: USA |
|
| Interventions |
Compression device versus no compression device Group 1 (n = 25): sequential compression device; with thigh‐high sleeves and a preset pressure of 50 mmHg Group 2 (n = 25): no sleeves on lower limbs Preloading with 20 mL/kg Ringer's lactate Standardised anaesthetic technique and dose for all women |
|
| Outcomes |
Maternal: hypotension Neonatal: Apgar score < 8 at 5 min |
|
| Notes | Hypotension: defined as decrease MAP measurement by > 20% of baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomisation method unknown |
| Allocation concealment (selection bias) | Unclear risk | "Sealed envelopes." No further detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Hypotension treated by an anaesthetist who was blinded to the assigned group |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Low risk | Not apparent |
| Other bias | Low risk | Not apparent |
Alahuhta 1992.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 19 women Inclusion criteria: healthy women undergoing elective caesarean under spinal anaesthesia (38‐42 weeks' gestation) for fetal breech presentation or cephalopelvic disproportion in otherwise uncomplicated singleton pregnancies Exclusion criteria: not reported Setting: Finland |
|
| Interventions |
Ephedrine versus phenylephrine Group 1 (n = 9): ephedrine (mean 27.9 mg, range 16.7 to 32.5) Group 2 (n = 8): phenylephrine (mean 488 µg, range 334 to 767) Standardised anaesthetic technique for all women but variable heavy 0.5% bupivicaine dose (range 2.3‐2.6 mL) |
|
| Outcomes | Maternal: hypotension (defined as a fall in SAP of more than 10 mmHg from baseline); heart rate Neonatal: arterial umbilical blood < pH 7.2; Apgar < 8 at 5 min; fetal heart rate; birthweight | |
| Notes | Hypotension requiring intervention: not stated | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Described as "double blind" – third‐party preparation and coding of solutions |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses to follow‐up: 2/19 – 1 from each group; 1 technical failure, 1 maternal bradycardia requiring atropine treatment |
| Selective reporting (reporting bias) | Unclear risk | Not all expected outcomes were reported |
| Other bias | High risk | Similar baseline characteristics Variable dose of local anaesthetic used for spinal anaesthesia |
Alimian 2014.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 90 women undergoing elective caesarean section Inclusion criteria: normal single pregnancy, gestational age > 37 weeks, no history of hypertension Exclusion criteria: contraindications for spinal anaesthesia, third trimester bleeding, BMI > 30 kg/m², previous allergy to hydroxyethyl starch (HES) preparations, known cardiomyopathy, height < 155 cm, sympathetic block higher than T4 Setting: France and USA |
|
| Interventions |
Ringer's lactate preload vs sodium chloride preload vs HES preload
Group 1: Ringer's lactate group, 1000 mL Group 2: sodium chloride 0.9% group, 1000 mL Group 3: HES group, 7.5 mL/kg |
|
| Outcomes |
Maternal: BP, heart rate Neonatal: umbilical cord pH, Apgar score |
|
| Notes | Hypotension was defined as a drop in systolic blood pressure of > 20% from baseline or systolic blood pressure < 100 mmHg. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Block randomisation technique |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "Double blind" – no further detail provided |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | "Double blind" – no further detail provided |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Low risk | Most expected outcomes reported |
| Other bias | Low risk | None evident |
Allen 2010.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 109 women Inclusion criteria: ASA physical status I and II pregnant women scheduled for elective caesarean delivery under spinal anaesthesia; singleton gestation at a gestational age of > 36 weeks Exclusion criteria: women who were in labour, BMI > 45 kg/m², type 1 diabetes mellitus, hypertensive disease, cardiac disease, a fetus with severe congenital anomalies, history of monoamine oxidase inhibitor use, or those who were included in any other anaesthesia drug studies Setting: USA |
|
| Interventions |
Phenylephrine dosage variations versus placebo Group 1: phenylephrine infusion 25 μg/min Group 2: phenylephrine infusion 50 μg/min Group 3: phenylephrine infusion 75 μg/min Group 4: phenylephrine infusion 100 μg/min Group 5: placebo (normal saline 50 mL) infusion All infusions were commenced immediately after spinal injection, at 60 mL/h in combination with a standardised fluid coload. The study drug was infused until 10 min after delivery, after which the study ended and further management was at the discretion of the anaesthesiologist. All women received a standardised aspiration prophylaxis, a standardised spinal anaesthetic technique and dose, and a standardised oxytocin bolus and subsequent infusion after delivery. Hypotension (requiring intervention) was treated by administering a 100 μg bolus of phenylephrine. Hypertension treatment: treated by stopping the infusion. Infusions were only restarted when the SBP decreased to below the upper limit of the target range above baseline). NOTE: if the study drug infusion had to be stopped on 3 occasions, then it was stopped permanently, and BP was maintained with phenylephrine boluses for the remainder of the study. Bradycardia treatment: administration of glycopyrrolate 0.4 mg |
|
| Outcomes |
Maternal: hypotension, pre and postdelivery birth; hypotension requiring intervention; nausea and vomiting; cardiac dysrhythmia; pre and postbirth reactive hypertension; bradycardia Neonatal: acidosis (cord or neonatal bloods with pH < 7.2); neonatal Apgar score < 8 at 5 min |
|
| Notes | Hypotension defined as SBP < 20% below baseline Hypotension requiring intervention defined as SBP decrease > 20% baseline or < 90 mmHg Hypertension defined as SBP > 20% above baseline Bradycardia defined as < 50 bpm |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation in blocks of 20 |
| Allocation concealment (selection bias) | Unclear risk | Each study syringe was identified by a study number. The infusions were prepared in identical 50 mL syringes by a physician not involved in the study. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "Double blind". To maintain blinding, the infusions were prepared in identical 50 mL syringes containing normal saline for the placebo, or the appropriate concentrations of phenylephrine (25 μg, 50 μg, 75 μg, or 100 μg) for the drug interventions. A physician not involved in the study coded and prepared the syringes. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not stated who was responsible for recording of outcomes, and whether they were blinded to the allocated intervention |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 8/109 patients excluded (not specified which groups they were from), due to inadequate or failed spinal anaesthesia. Insufficient samples were obtained for umbilical cord blood gases for some babies because of insufficient samples, clotted samples or sampling errors: 1 (placebo group); 2 (phenylephrine 25 μg group); 2 (phenylephrine 50 μg group) and 5 (phenylephrine 100 μg group). |
| Selective reporting (reporting bias) | Low risk | Most expected outcomes reported |
| Other bias | Low risk | No apparent sources of other bias Study funded by Duke University Medical Center Department of Anesthesiology, Division of Women's Anesthesia |
Amaro 1998.
| Study characteristics | ||
| Methods | Randomisation: method not described | |
| Participants | 40 women Inclusion criteria: ASA I, term, singleton, cephalic, elective CS Exclusion criteria: not specified Setting: Brazil |
|
| Interventions |
Crawford's wedge versus uterine displacement Group 1 (n = 20): wedged lateral position using modified Crawford's wedge (15 degrees left lateral tilt) Group 2 (n = 20): manual uterine displacement by surgical assistant All women received a standardised preload and standardised spinal anaesthetic technique and dose |
|
| Outcomes |
Maternal: hypotension, magnitude of BP reduction and time of occurrence, block height, ephedrine consumption, induction – and hysterotomy – birth times. Neonatal: umbilical artery pH (expressed as mean and SD), Apgar scores at 1 min and 5 min |
|
| Notes | Hypotension defined as decrease in SBP > 20% baseline or < 100 mmHg absolute | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomisation methods not described |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up not stated |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Ansari 2011.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 128 women Inclusion criteria: women with a normal singleton pregnancy at 37 weeks' gestation or more scheduled for elective CS Exclusion criteria: ASA grade III or more; height < 150 cm or > 180 cm; body mass < 60 kg or > 100 kg; pre‐eclampsia; known fetal abnormality; or any other contraindication to spinal anaesthesia Setting: United Arab Emirates |
|
| Interventions |
Phenylephrine 50 μg versus 100 μg infusion Group 1: phenylephrine 50 μg/mL infusion Group 2: phenylephrine 100 μg/mL infusion Phenylephrine infusion was commenced immediately after spinal anaesthesia in conjunction with standardised IV coload with warm Hartmann's solution. Initial phenylephrine rate of 60 mL/h for the first 3 min and stopped if SBP was > 120% of the baseline. After the first 3 min, the infusion was continued at the same rate if SBP was between 80% and 100% of baseline, until the time of giving birth; infusion was discontinued if the SBP was more than 100% of baseline value. All women received standardised aspiration prophylaxis and standardised spinal anaesthetic technique and dose. Hypotension requiring intervention: rescue dose of phenylephrine 50 μg if BP decreased to < 80% baseline for 2 consecutive readings, despite phenylephrine infusion. Bradycardia requiring intervention: if bradycardia without hypotension, phenylephrine infusion was discontinued for 1 min; if bradycardia developed with hypotension, IV glycopyrronium 200 μg was administered. |
|
| Outcomes |
Maternal: BP; hypotension; hypertension; bradycardia; total dose of phenylephrine; nausea and vomiting Neonatal: Apgar scores at 1 min and 5 min; umbilical arterial pH and gases |
|
| Notes | Hypotension defined as SBP < 80% baseline Hypertension defined as SBP > 120% baseline Bradycardia defined as heart rate < 50 bpm |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomised" – no further details reported |
| Allocation concealment (selection bias) | Unclear risk | "Closed similar" envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | An anaesthetist who was not involved in case management prepared a 20 mL syringe for phenylephrine infusion with the designated concentration; both women and the anaesthetist in charge of the case were blinded to the concentration of phenylephrine in the syringe |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Not reported, but likely in view of the above. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 11/128 lost to follow‐up (not reported by assigned group):
|
| Selective reporting (reporting bias) | Low risk | Most expected outcomes were reported. |
| Other bias | Unclear risk | Some suggestion of imbalance in randomisation and/or differential losses to follow‐up (54 and 63 women analysed in each group) |
Arora 2015.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 90 women Inclusion criteria: ASA grade I/II, full term (36‐40 weeks' gestation), uncomplicated singleton pregnancy, elective LSCS under spinal anaesthesia Exclusion criteria: fetal distress, antepartum haemorrhage, pregnancy‐induced hypertension, diabetes mellitus, multiple gestation, significant cardiorespiratory disorder or intrapartum cardiomyopathy Setting: India |
|
| Interventions |
Colloid preload versus colloid coload versus crystalloid preload Group 1: 10 mL/kg colloid preload (6% HES administered 20 min prior to SAB) Group 2: 10 mL/kg colloid co‐load (6% HES administered by rapid infusion in 10 min immediately after SAB) Group 3: 10 mL/kg crystalloid preload (Ringer's lactate administered 20 min prior to SAB) All women received the same aspiration prophylaxis, anaesthetic technique and dose, IV cannula. 10 min after induction of spinal anaesthesia, normal saline was given in all 3 groups at rate of 200 mL/h. Hypotension was treated by increasing rate of fluid infusion and IV ephedrine 5 mg until the BP had improved to within 20% of baseline. |
|
| Outcomes | Maternal: incidence of hypotension, dose of ephedrine | |
| Notes | Hypotension was defined as SBP < 80% baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random allocation |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | None reported |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Bhagwanjee 1990.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 24 women Inclusion criteria: healthy, term parturients undergoing elective CS. Exclusion criteria: placental dysfunction, intrauterine growth retardation, abnormal fetal presentation, weight more than 90 kg Setting: South Africa |
|
| Interventions |
Lower limb compression versus control Group 1: legs wrapped with 10 cm Esmarch bandages from ankle to mid‐thigh immediately following spinal with preservation of pedal pulses Group 2: control All women received standardised IV preload with plasmalyte followed by a standardised spinal anaesthetic technique and dose |
|
| Outcomes |
Maternal: hypotension; spinal to birth time; uterine incision to birth time Neonatal: Apgar scores (minus colour) at 2 min and 5 min; umbilical arterial and venous blood gas oxygen tension and saturation |
|
| Notes | Hypotension defined as SBP < 100 mmHg or less than 80% baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding not reported – unlikely due to nature of intervention (leg wrapping) |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: not reported |
| Selective reporting (reporting bias) | Low risk | Most expected outcomes reported |
| Other bias | Low risk | Similar baseline characteristics. None apparent |
Bhardwaj 2013.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 90 women Inclusion criteria: ASA grade I, elective CS under spinal anaesthesia, singleton pregnancy, no fetal abnormalities, no pre‐eclampsia, no cerebrovascular diseases Setting: India |
|
| Interventions |
Phenylephrine infusion versus ephedrine infusion versus metaraminol infusion Group 1: phenylephrine 30 μg/mL (15 μg/min) Group 2: ephedrine 5 mg/mL (2.5 mg/min) Group 3: metaraminol 0.5 mg/mL (0.25 mg/min) Immediately following SAB, patients received 1 mL bolus of study drug and then a infusion at 15 mL/h All women received standardised: aspiration prophylaxis, monitoring, IV cannulation, isotonic saline coload, spinal anaesthetic technique and dose If SBP increased 1.25 times above baseline, infusion was ceased. If SBP dropped 10% below the baseline, 1 mL bolus of study drug given. If maternal heart rate < 60 bpm and SBP < 80% of baseline, or if maternal heart rate < 50 and SBP < 100% of baseline, or if maternal heart rate < 45 regardless of BP, glycopyrrolate 0.2 mg IV given |
|
| Outcomes |
Maternal: incidence of maternal hypotension, incidence of maternal hypertension, heart rate, nausea/vomiting, total dose of vasopressor Neonatal: Apgar scores at 1 min and 5 min, umbilical cord gases |
|
| Notes | Hypotension: SBP < 80% of baseline Hypertension: SBP > 120% of baseline |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomised sequence |
| Allocation concealment (selection bias) | Low risk | Sequentially numbered sealed envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind Study drugs prepared by another anaesthetist not involved in other aspects of the participants' care, into a unlabelled 20 mL syringe |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Below exclusions reported: Group 2 – 1 failed SAB Group 3 – 1 failed SAB Group 1 – 2 pump failures |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Bottiger 2010.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 60 women Inclusion criteria: ASA I/II, elective caesarean delivery Exclusion criteria: none stated Setting: USA |
|
| Interventions |
Crystalloid preload versus colloid preload Group 1: crystalloid preload (1500 mL Ringer's lactate) Group 2: colloid preload (0.5L 6% HES) Women in both groups received 100 μg/min phenylephrine infusion following spinal anaesthesia which continued until uterine incision. The phenylephrine infusion was adjusted according to heart rate and SBP which was maintained at 20% of the baseline. No further information regarding spinal anaesthetic technique/dose etc was provided. |
|
| Outcomes |
Maternal: vasopressor dose, incidence of hypotension, incidence of nausea and vomiting, incidence of bradycardia Neonatal: Apgar score |
|
| Notes | Hypotension was defined as a 20% fall in SBP from baseline. Hypertension was defined as an increase of 20% from baseline. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Method not explicitly stated |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 3 women excluded for unspecified reasons and at an unclear point along the study pathway Additionally, study states "60 patients were included as part of a 90 patient study" |
| Selective reporting (reporting bias) | Low risk | None evident |
| Other bias | Low risk | None evident |
Bouchnak 2012.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 60 women Inclusion criteria: ASA I scheduled for elective CS, singleton term pregnancy Exclusion criteria: chronic or gestational hypertension, cardiac disease, diabetes, known fetal abnormalities, contraindication to spinal anaesthesia Setting: Tunisia |
|
| Interventions |
Colloid preload versus crystalloid preload Group 1: HES 130/0.4 500 mL preload 15 min prior to spinal anaesthesia. Group 2: saline – normal saline solution preload 1000 mL within 15 min prior to spinal anaesthesia All women received standardised anaesthetic technique and dose. Hypotension requiring intervention: 6 mg bolus ephedrine when SBP was < 80% of baseline. |
|
| Outcomes |
Maternal: hypotension; SBP; adverse effects; need for ephedrine; heart rate; tachycardia (> 100 bpm); nausea; vomiting; pruritus Neonatal: umbilical blood gases; Apgar scores ar 1 min and 5 min; birthweight |
|
| Notes | Hypotension defined as SBP < 80% baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Reported only as "randomized" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Not reported |
| Selective reporting (reporting bias) | Unclear risk | Some outcomes not fully (numerically) reported |
| Other bias | Low risk | Similar baseline characteristics |
Calvache 2011.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 80 women Inclusion criteria: ASA I/II women aged 18‐45 years with an uncomplicated singleton pregnancy at term who were scheduled for caesarean under spinal anaesthesia Exclusion criteria: pregnancy‐induced hypertension, cardiac disease, diabetes, fetal complications and women in labour: post hoc exclusions (surgery lasting > 2 h; requirement for perioperative sedation; conversion to general anaesthesia, surgical complications such as intraoperative haemorrhage, protocol violations) Setting: Colombia |
|
| Interventions |
Wedge versus supine position Group 1: wedge after intrathecal injection women were placed from the left lateral position to the supine position, with a right‐lumbar pelvic wedge (wooden, 35 cm long, 20 cm wide and with 20 degrees inclination), placed at the right posterior‐superior iliac crest and lumbar region Group 2: supine: after intrathecal injection, women were placed from the left lateral position to the supine position All women received no premedication, standardised oxygen therapy, standardised spinal anaesthetic technique and dose, and standardised crystalloid co‐load Hypotension was treated with IV boluses of ethylephrine 1 mg until hypotension was corrected. Bradycardia was treated with 0.5 mg atropine. |
|
| Outcomes | Maternal: hypotension BP; vasopressor requirements (median ethylephrine consumption); nausea; vomiting; bradycardia | |
| Notes | Hypotension was defined as a 25% reduction in SBP from baseline. Bradycardia was defined as heart rate < 40 bpm. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated sequence |
| Allocation concealment (selection bias) | Unclear risk | "Randomly allocated" ... "by independent anesthetist"; no further details provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | A single unblinded anaesthetist performed spinal anaesthesia, positioning of women, anaesthetic management and data collection |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Data analysis was blinded, but not mentioned if outcome assessment was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up |
| Selective reporting (reporting bias) | High risk | No neonatal outcomes reported |
| Other bias | Low risk | Similar baseline characteristics |
Cardoso 2004a.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 50 women Inclusion criteria: term singleton pregnancies, ASA I, undergoing caesarean under spinal anaesthesia Exclusion criteria: chronic hypertension, gestation‐induced hypertension, cardiovascular or vascular brain disease, known fetal abnormalities and women with total or partial spinal anaesthesia failure Setting:Brazil |
|
| Interventions |
Colloid versus crystalloid preload: Group 1: received preload of modified fluid gelatin, 10 mL/kg Group 2: received preload of Ringer's lactate, 10 mL/kg All women received a standardised spinal anaesthetic technique and dose and standardised uterine displacement. |
|
| Outcomes |
Maternal: hypotension; nausea; vomiting; vasopressor consumption Neonatal: cord blood (presented as mean and SD); Apgar < 7 at 5 min |
|
| Notes | Hypotension was defined as decreases of more than 10% or more than 20% of baseline SBP. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Randomly allocated": method not described |
| Allocation concealment (selection bias) | Unclear risk | "Drawing of closed envelopes" |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "Double blind" – no further details |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | "Double blind" – no further details |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up |
| Selective reporting (reporting bias) | High risk | Minimal results reporting: outcomes reported as means and SD only |
| Other bias | Low risk | Similar baseline characteristics |
Carvalho 1999a.
| Study characteristics | ||
| Methods | RCT | |
| Participants | N = 80 Inclusion criteria: healthy women undergoing spinal anaesthesia for elective caesarean Exclusion criteria: not specified Setting: Brazil |
|
| Interventions |
Ephedrine (different doses) versus control Group 1: 5 mg ephedrine administered immediately after spinal anaesthesia Group 2: 10 mg ephedrine administered immediately after spinal anaesthesia Group 3: 15 mg ephedrine administered immediately after spinal anaesthesia Group 4: control – no ephedrine Standardised spinal anaesthetic technique and dose |
|
| Outcomes |
Maternal: hypotension; nausea; vomiting; hypertension requiring intervention Neonatal: cord/neonatal blood < 7.2; Apgar < 8 at 5 min |
|
| Notes | Hypotension defined as fall in SAP below 20% baseline Abstract only |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, but method not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Unclear risk | Not reported |
| Other bias | Unclear risk | Not reported |
Carvalho 1999b.
| Study characteristics | ||
| Methods | Randomised trial | |
| Participants | 100 women Inclusion criteria: healthy women undergoing spinal anaesthesia for elective caesarean Exclusion criteria: not specified Setting: Brazil |
|
| Interventions |
Ephedrine infusion (different rates) versus control Group 1: ephedrine infusion 0.5 mg/min administered immediately after spinal anaesthesia Group 2: ephedrine infusion 1 mg/min administered immediately after spinal anaesthesia Group 3: ephedrine infusion 2 mg/min administered immediately after spinal anaesthesia Group 4: ephedrine infusion 4 mg/min administered immediately after spinal anaesthesia Group 5: no ephedrine All women received a standardised anaesthetic technique and dose. |
|
| Outcomes |
Maternal: hypotension; vomiting; hypertension requiring intervention. Neonatal: cord/neonatal blood < 7.2; Apgar < 8 at 5 min |
|
| Notes | Hypotension defined as fall in SAP below 20% baseline Abstract only |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method of randomisation not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Unclear risk | Not reported |
| Other bias | Unclear risk | Not reported |
Carvalho 2000.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 120 women Inclusion/exclusion criteria: not available as whole paper was not translated Setting: Brazil |
|
| Interventions |
Ephedrine bolus + infusion versus ephedrine infusion alone versus rescue bolus of ephedrine only Group 1: ephedrine 10 mg in bolus followed by continuous infusion of 2 mg/min until birth Group 2: ephedrine 8 mg/min for 3 min, followed by 4 mg/min for 2 min, then 2 mg/min until birth Group 3: control: Ringer's lactate preload and rescue bolus of ephedrine in case of hypotension All women received a standardised preload of Ringer's lactate and standardised spinal anaesthetic technique and dose. |
|
| Outcomes |
Maternal: hypotension; nausea; vomiting; hypertension requiring intervention Neonatal: umbilical artery pH; Apgar < 8 at 5 min |
|
| Notes | Hypotension defined as SBP < 80% of baseline Abstract only |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method of randomisation not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses to follow‐up: 2/120 for cord blood pH measurement (in the ephedrine infusion group) |
| Selective reporting (reporting bias) | Unclear risk | Not reported |
| Other bias | Unclear risk | Not reported |
Carvalho 2009.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 46 women Inclusion criteria: women scheduled for caesarean under spinal anaesthesia; age 18‐54 years; weight ≤ 100 kg; height ≥ 150 cm; ASA physical status I or II; uncomplicated term pregnancy Exclusion criteria: pregnancy‐induced hypertension; cardiac disease; diabetes or fetal complications; women in labour Setting: USA |
|
| Interventions |
Colloid preloading versus colloid coloading Group 1: colloid preload: 500 mL 6% hetastarch IV slowly over 20 min before spinal anaesthesia Group 2: colloid coload: 500 mL 6% hetastarch IV as quickly as possible, with the aid of a pressure bag, immediately after spinal anaesthesia All women received standardised aspiration prophylaxis and standardised spinal anaesthetic technique and dose. Hypotension requiring intervention was managed with vasopressor mix of 5 mg/mL ephedrine plus 25 μg/mL phenylephrine given according to a strict predefined algorithm (systolic pressure ≥ 90% of baseline: no vasopressor; 80%‐89% systolic pressure: 1 mL equivalent to ephedrine 5 mg + phenylephrine 25 μg; 79%‐79% systolic pressure: 2 mL equivalent to ephedrine 10 mg + phenylephrine 50 μg; systolic pressure < 70%: 3 mL equivalent to ephedrine 15 mg + phenylephrine 75 μg) |
|
| Outcomes |
Maternal: hypotension; bradycardia; tachycardia; nausea, vomiting; total vasopressor dose Neonatal: umbilical and venous arterial pH; Apgar scores; neonatal weight |
|
| Notes | Hypotension defined as SBP < 90% baseline Bradycardia defined as heart rate < 40 bpm Tachycardia defined as heart rate > 140 bpm |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random numbers generated using MS Excel |
| Allocation concealment (selection bias) | Unclear risk | Sealed, opaque envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible to blind the interventions |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up |
| Selective reporting (reporting bias) | Unclear risk | Most expected outcomes were reported, although some were reported in a form that could not used in this review |
| Other bias | Low risk | Similar baseline characteristics |
Chan 1997.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 46 women Inclusion criteria: healthy parturients with normal pregnancies undergoing elective CS at term Exclusion criteria: not specified Setting: China |
|
| Interventions |
Prophylactic ephedrine versus crystalloid preload Group 1: ephedrine 0.25 mg/kg in 5 mL normal saline over 3 min immediately after spinal injection Group 2: Hartmann's solution 20 mL/kg 10‐15 min prior to spinal injection Standardised spinal anaesthetic technique and dose |
|
| Outcomes |
Maternal: hypotension); level of sensory block; Doppler ultrasound uterine blood flow measurements before and 5 min after spinal injection; nausea and vomiting; shivering; cardiac dysrhythmia; uterine incision‐birth time Neonatal: arterial and venous cord blood gases; Apgar scores at 1 min and 5 min |
|
| Notes | Hypotension defined as a decrease in systolic pressure of > 20% of baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomly assigned": method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Neonatal assessment only (a preoperative Doppler ultrasound of uterine blood flow conducted by obstetrician who was blinded to the "treatment received") – no further details |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Methods not described |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses to follow‐up: none |
| Selective reporting (reporting bias) | Unclear risk | Most expected outcomes reported |
| Other bias | Low risk | Similar baseline characteristics |
Chohedri 2007.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 60 women Inclusion criteria: ASA I‐II ambulatory pregnant women for whom elective caesarean with spinal anaesthesia was planned (no instances of fetal distress) Setting: Iran |
|
| Interventions |
Ephedrine: comparison of different routes of administration Group 1: oral ephedrine, 25 mg administered before spinal Group 2: IM injection of ephedrine, 25 mg, 30 min before spinal Group 3: IV bolus of ephedrine, 25 mg in 2 mL injected over a 1‐min period, immediately after spinal induction All women received a standardised 20 mL/kg preload of Ringer's lactate solution and a standardised spinal anaesthetic technique. The anaesthetic dose was increased from 60 mg lidocaine to 70 mg lidocaine if the woman's height was > 160 cm. Hypotension requiring intervention was managed with 10 mg ephedrine IV bolus increments every min until SBP returned to normal (> 100 mmHg and > 70% baseline). |
|
| Outcomes |
Maternal: hypotension; hypertension (increase of 30% from baseline); heart rate (tachycardia increase of 30% from baseline), nausea Neonatal: Apgar scores |
|
| Notes | Hypertension was defined as an increase in BP by 30% from baseline. Tachycardia was defined as an increase in heart rate of 30% from baseline. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | "[R]andomly divided into three equal groups of 20" |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "Double blind" – no further detail provided |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | "Double blind" – no further detail provided |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | None reported |
| Selective reporting (reporting bias) | Unclear risk | Not all expected outcomes were reported, e.g. only 1 neonatal outcome reported in a way that could not be used in this review |
| Other bias | Low risk | No apparent source of other bias |
Cyna 2010.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 45 women Inclusion criteria: women aged > 18 years, > 34 weeks' gestation, singleton pregnancy presenting for elective CS under spinal anaesthesia Exclusion criteria: women unable to stand or walk for 15 min, with pre‐existing hypertension or pre‐eclampsia, multiple pregnancy or grade 3‐4 placenta praevia Setting: Australia |
|
| Interventions |
Walking versus lying down Group 1: walking: women were asked to walk to the operating theatre for at least 15 min prior to positioning for spinal anaesthesia Group 2: lying: women were taken to theatre on a barouche or trolley; lying with a wedge Spinal anaesthesia technique, IV fluids given, vasopressors given were not reported |
|
| Outcomes | Maternal: incidence of hypotension | |
| Notes | Hypotension defined as fall in SBP 20% from baseline or < 100 mmHg systolic Ephedrine and metaraminol were used to treat hypotension |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated sequence |
| Allocation concealment (selection bias) | Low risk | "Consecutively numbered sealed opaque envelopes" |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants and anaesthetists not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 1 participant's data were lost, leaving 44 women suitable for analysis. Lying group: 3 participants in the lying group has a failed spinal and converted to general anaesthesia; 2 participants withdrew without explanation Walking group: 2 patients had protocol violation (not given 6 mg prophylactic ephedrine) Intention‐to‐treat analyses performed 17 women in lying group and 20 women in walking group were analysed. |
| Selective reporting (reporting bias) | Unclear risk | Exact values of outcomes not reported in abstract |
| Other bias | Low risk | Similar baseline characteristics |
Dahlgren 2005.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 110 women Inclusion criteria: healthy women with normal term singleton pregnancies presenting for elective CS Setting: Sweden |
|
| Interventions |
Crystalloid versus colloid preload Group 1: acetated Ringer's solution, 1000 mL, preceded by 20 mL 15% saline 0.9% IV Group 2: dextran 60 3%, 1000 mL, preceded by 20 mL dextran 1 IV All women received a standardised spinal anaesthetic technique and dose. Hypotension was managed by a standardised regimen of ephedrine dosing. |
|
| Outcomes |
Maternal: hypotension; clinically significant hypotension; severe hypotension ephedrine consumption; blood loss Neonatal: umbilical artery < pH 7.2; pCO2; base deficit |
|
| Notes | Hypotension defined as SAP dropping below 100 mmHg; clinically significant hypotension as drop in SAP > 20% below baseline and severe hypotension defined as SAP < 80 mmHg | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | "Sealed envelope" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "Double‐blinded" – solution prepared and administered by an anaesthetic nurse not otherwise involved in the care of the woman (including the initial injection) |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses: 1/110 – 1 woman from crystalloid group excluded due to protocol violation; 1 woman allocated to crystalloid subsequently found to have received colloid. |
| Selective reporting (reporting bias) | High risk | Not all outcomes listed in the paper were reported |
| Other bias | Low risk | Some baseline differences, e.g. 32% nulliparous in the crystalloid group compared with 21% in the colloid group |
Dahlgren 2007.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 55 women presenting for elective CS Inclusion criteria: healthy women with term singleton normal pregnancies Setting: Sweden |
|
| Interventions |
Colloid versus crystalloid preload Group 1: colloid group: 20 mL of 15% dextran 1, followed by 1000 mL IV infusion of 3% dextran 60. This solution was administered during 20 min immediately preceding intrathecal injection. Group 2: crystalloid group: 20 mL IV injection of 0.9% saline, followed by 1000 mL IV infusion of acetated Ringer's solution. This solution was administered during 20 min immediately preceding intrathecal injection. All women received standardised fasting protocol, no premedication and a standardised spinal anaesthetic technique and dose. Hypotension requiring intervention was managed with ephedrine 5 mg if SBP dropped below 100 mmHg, and repeated as required. |
|
| Outcomes |
Maternal: hypotension – overall, clinically significant or severe Criteria for rescue: if the woman developed discomfort associated with a decrease in SBP of at least 20% from baseline, even if it was above 100 mmHg |
|
| Notes | 'Overall' hypotension defined as a fall in systolic pressure below 100 mmHg 'Clinically significant' hypotension defined as hypotension associated with maternal discomfort (nausea, retching/vomiting, dizziness or chest symptoms) 'Severe' hypotension defined as a reduction of the SAP below 80 mmHg |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Randomly allocated" – method not specified |
| Allocation concealment (selection bias) | Unclear risk | Sealed envelope |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | 'Double‐blind'. The woman, the anaesthesiologist and all other personnel in the operating room were unaware of the study group. The study solutions were prepared and administered by an anaesthetic nurse who was not otherwise involved in the care of the patient, and were covered by a non‐transparent plastic bag. The anaesthesiologist did not enter the operating room until the study solution had been given. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | All personnel were blinded to treatment allocation, except for the anaesthetic nurse who prepared the solutions (who was not involved in the care of the patient). |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 2/55 excluded due to protocol violation (1 was given ephedrine despite a normal BP and the other could not go through the SST because of leg muscle spasm). Not specified which groups they were from |
| Selective reporting (reporting bias) | Low risk | Only maternal outcome reported was hypotension; no infant outcomes were reported |
| Other bias | Low risk | No apparent sources of other bias |
Damevski 2011.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 40 women Inclusion criteria: ASA I, women aged 21‐28 years with normal pregnancies, elective caesarean for breech presentation, cephalopelvic disproportion, re‐operation Exclusion criteria: body weight > 90 kg, women who refused caesarean Setting: Macedonia |
|
| Interventions |
Ephedrine infusion versus crystalloid preload Group 1: ephedrine: continuous fast‐drop infusion of 500 mL Ringer's solution with 50 mL ephedrine, commenced immediately after venous cannulation for spinal anaesthesia, and continued until the umbilical cord was clamped Group 2: crystalloid: 20 mL/kg Ringer's solution, warmed to room temperature, commenced 20‐30 min prior to spinal anaesthesia, and continued until the umbilical cord was clamped All women received a standardised spinal anaesthetic technique and dose, standardised oxygen therapy, and standardised oxytocin regimen. Hypotension requiring intervention received 5 mg IV boluses of ephedrine in group 1 (ephedrine group) and 10 mg IV boluses of ephedrine in group 2 (crystalloid group). |
|
| Outcomes |
Maternal: hypotension; quantity of crystalloid; quantity of ephedrine; nausea and vomiting Neonatal: Apgar scores |
|
| Notes | Hypotension defined as SBP < 100 mmHg | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomised" – no further details reported |
| Allocation concealment (selection bias) | Unclear risk | As above |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up |
| Selective reporting (reporting bias) | Unclear risk | Not all outcomes available (e.g. Apgar scores presented only as medians) |
| Other bias | Low risk | Similar baseline characteristics |
Das Neves 2010.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 120 women Inclusion criteria: physical status ASA I, with an indication for elective CS, singleton term pregnancy Exclusion criteria: history of hypertension or pregnancy‐induced hypertension, cardiovascular or cerebrovascular disease, fetal abnormalities, history of hypersensitivity to the drugs used in the study, and contraindications to spinal block Setting: Brazil |
|
| Interventions |
Phenylephrine: prophylactic infusion versus therapeutic dosing Group 1: continuous IV infusion of phenylephrine, using a 1‐channel "Baxter" volumetric infusion pump (containing a solution of 10 mL of NS with 10 mg phenylephrine (100 μg/mL)), at 0.15 μg/kg/min, which was started immediately after the spinal block Group 2: a single dose of phenylephrine, 50 μg IV, administered immediately after the spinal block. Baxter volumetric infusion pump connected, containing 100 mL NS Group 3: a single dose of phenylephrine, 50 μg IV, administered in case of hypotension, defined as a fall in SBP and/or DBP of up to 20% of mean baseline levels. Baxter volumetric infusion pump connected, containing 100 mL NS All women received a standardised spinal anaesthetic technique and dose followed by a standardised crystalloid infusion and standardised positioning. Hypotension treatment involved a bolus of 30 μg of phenylephrine IV repeated every 2 min if a drop in BP > 20% that was not controlled with the therapeutic regimen used. Bradycardia was treated when associated with hypotension with 0.5 mg of atropine IV. |
|
| Outcomes |
Maternal: hypotension; reactive hypertension; bradycardia; nausea and vomiting Neonatal: Apgar score < 8 at 5 min |
|
| Notes | Hypotension defined as a drop in SBP and/or DBP > 20% of mean baseline levels Reactive hypertension defined as BP 20% > mean baseline levels after the use of the vasopressor Bradycardia defined as heart rate lower than 50 bpm |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated numbers |
| Allocation concealment (selection bias) | Unclear risk | Sequential sealed envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "Double blind." Patients, and physicians responsible for collecting and analysing the data were blinded; anaesthetist administering the anaesthesia was not blinded. This anaesthetist was not involved in data collection and analysis. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Those collecting and analysing the data were blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up occurred |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Unclear risk | No apparent sources of other bias |
Davies 2006.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 70 women Inclusion criteria: ASA physical status I or II, women scheduled for elective CS under spinal anaesthesia, > 37 weeks' gestation Exclusion criteria: pregnancy‐induced hypertension, multiple pregnancy, fetal compromise, diabetes mellitus, polyhydramnios, weight > 100 kg, renal or hepatic disease, anaemia (haemoglobin < 10 g/dL), clotting Setting: UK |
|
| Interventions |
Colloid: 5 mL/kg versus 10 mL/kg preload Group 1: 5 mL/kg pentastarch, volume preload before spinal anaesthesia (infused over 10 min) Group 2: 10 mL/kg pentastarch, volume preload before spinal anaesthesia (infused over 10 min) All women received standardised aspiration prophylaxis, a standardised spinal anaesthetic technique and dose, and standardised positioning. Hypotension requiring intervention was treated with 6 mg increments of ephedrine until resolution; smaller decreases in BP were similarly treated if accompanied by nausea, vomiting or dizziness. |
|
| Outcomes |
Maternal: hypotension; ephedrine use Neonatal: Apgar score at 1 min |
|
| Notes | Hypotension was defined as a decrease in SBP to < 70% baseline or < 90 mmHg | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomisation according to sealed envelopes"; no further details |
| Allocation concealment (selection bias) | Unclear risk | As above |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "A technician prepared the calculated volume of pentastarch and covered it with a black bag to blind the anaesthetist to the volume administered." |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Not reported but probably done |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No losses reported |
| Selective reporting (reporting bias) | Unclear risk | Not all expected outcomes were reported |
| Other bias | Low risk | Similar baseline characteristics |
Doherty 2012.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 69 women Inclusion criteria: ASA physical status I/II; aged 18 years and older; weight 50‐100 kg; height between 150 and 180 cm Exclusion criteria: allergy or hypersensitivity to phenylephrine; hypertension; cardiovascular or cerebrovascular disease; fetal abnormalities; diabetes (excluding gestational diabetes); or contraindications to spinal anaesthesia Setting: Canada |
|
| Interventions |
Phenylephrine infusion versus phenylephrine bolus Group 1: infusion: fixed rate phenylephrine infusion 120 μg/min; infusion was started immediately on completion of intrathecal injection, at a rate of 1 mL/min and continued for a minimum of 2 min, and continued if maternal SBP was equal to or lower than baseline. If maternal BP was higher than baseline, the infusion was discontinued and the BP reassessed after 2 min Group 2: bolus: intermittent phenylephrine bolus of 120 μg; women received 1 mL of bolus solution every time SBP was equal to or lower than baseline. A bolus was not administered when SBP was above baseline All women received an IV infusion of Ringer's lactate started at a minimal rate in the holding area, with subsequent standardised crystalloid coload on administration of spinal anaesthetic. No antiemetic premedication was given. All women received a standardised spinal anaesthetic technique, dose and positioning. Hypotension requiring intervention received rescue dose of 5 mg ephedrine. Bradycardia requiring intervention received 0.6 mg atropine if heart rate < 60 bpm for 2 consecutive readings and SBP equal to or lower than baseline (infusion was discontinued if bradycardia with SBP higher than baseline). |
|
| Outcomes |
Maternal: BP; cardiac output; heart rate, hypotension; hypertension; nausea/vomiting; bradycardia; total dose of phenylephrine Neonatal: umbilical blood gases; neonatal weight; Apgar score at 1 min and 5 min |
|
| Notes | Hypotension was defined as SBP < 80% baseline. Hypertension was defined as SBP > 120% baseline. Bradycardia was defined as heart rate < 60 bpm. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random number table |
| Allocation concealment (selection bias) | Unclear risk | Sealed, opaque envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "Double blind": women and attending anaesthetists were blinded to the group allocation. 2 syringes, 1 20 mL bolus and 60 mL infusion were prepared for each woman. 1 syringe contained 120 μ/mL phenylephrine and the second syringe contained saline. Both syringes were labelled 'phenylephrine/placebo' and 'bolus syringe' and 'infusion syringe' respectively. The anaesthetist then received 1 syringe of infusion solution and 1 syringe of bolus solution (but did not know which syringe contained the phenylephrine). Each was administered according to the protocol for bolus and infusion as described above. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Not specifically stated, but probably done |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 9/69 were lost to follow‐up: 4/35 from the intervention group (3 pump errors; 1 unable to calibrate properly) and 5/35 from the bolus group (2 required additional anaesthesia (ketamine), 2 pump errors and 1 unable to calibrate properly) |
| Selective reporting (reporting bias) | Unclear risk | Most expected outcomes were reported, although blood gases reported only as mean and SD, and not specified if maternal hypertension required intervention |
| Other bias | Low risk | Baseline characteristics were similar |
Dyer 2004.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 50 women Inclusion criteria: less than 90 kg, ASA I and II, singleton pregnancy, presenting for elective caesarean under spinal anaesthesia Exclusion criteria: pre‐eclamptic women Setting: South Africa |
|
| Interventions |
Crystalloid: preload versus rapid infusion Group 1: preload – modified Ringer's lactate, 20 mL/kg preload 20 min before spinal Group 2: coload – rapid infusion of an equivalent volume of modified Ringer's lactate immediately after induction of spinal All women received a standardised spinal anaesthetic technique and dose. Hypotension < 80% of baseline treated with 5 mg boluses of ephedrine; < 70% of baseline treated with 10 mg ephedrine until a return to within 80% of baseline |
|
| Outcomes |
Maternal: hypotension; BP; heart rate; time to block; induction to incision times; incision to birth times; anaesthesia and surgery times; blood loss; urine output; nausea; ephedrine dose Neonatal: birthweight; Apgar scores; umbilical arterial pH; umbilical arterial base deficit |
|
| Notes | Hypotension defined as BP < 80% baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomly allocated" – methods not described |
| Allocation concealment (selection bias) | Unclear risk | "Allocation card contained within a sealed envelope" |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | "Since there were clearly pre‐defined target MAPs for vasopressor administration for each individual, the study was not blinded" |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses to follow‐up: none |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
El‐Mekawy 2012.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 90 women Inclusion criteria: ASA I, singleton pregnancy, term gestation, non‐life‐threatening cause for emergency CS under spinal anaesthesia (prolonged labour or dystocia, failed labour induction or amniotic rupture) Exclusion criteria: patient refusal, fetal distress, known fetal abnormalities, cardiovascular, renal or liver diseases, chronic hypertension or gestational hypertension, coagulation disorders, and those with total or partial spinal anaesthesia failure Setting: Egypt |
|
| Interventions |
Crystalloid co/postload versus colloid co/postload versus ephedrine infusion Group 1: 0.5 mL/kg/min Ringer's lactate via infusion pump: co/post loading started at time of spinal injection and continued after spinal injection with until fetus delivery (clamping of umbilical cord) Group 2: 0.5 mL/kg/min Voluven (6% HES 130/0.4 in isotonic NaCl solution) via infusion pump: co/post loading started at time of spinal injection and continued after it with until fetus delivery Group 3: ephedrine infusion at 1 mg/min via infusion pump commenced immediately after spinal anaesthesia until fetus delivery. Accompanied by infusion of Ringer's lactate at minimal infusion rates required to keep vein open Hypotension treated by 5 mg bolus of IV ephedrine every 2 min until SBP returned to normal value in all groups Bradycardia treated immediately using 0.5 mg atropine IV Nausea and vomiting treated with 10‐20 mg IV metoclopramide when unrelated to hypotension or not corrected by ephedrine bolus alone |
|
| Outcomes |
Maternal: BP, heart rate, adverse effects (nausea, vomiting, dizziness, chest symptoms, dyspnoea, tachypnoea), total IV fluid given, total ephedrine dose, time from spinal anaesthesia to delivery of fetus (clamping of umbilical cord) Neonatal: heart rate was monitored by CTG continuously until delivery; Apgar scores at 1 min and 5 min; arterial blood gas sample taken from umbilical cord for blood gas analysis (pH, pCO2) within 2 min after delivery |
|
| Notes | Hypotension was defined as 20% decrease in SBP from the baseline. Maternal bradycardia was defined as heart rate < 60 bpm. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method of randomisation not reported |
| Allocation concealment (selection bias) | Unclear risk | Closed envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Neither participants nor personnel were blinded, however this was unlikely to have impacted upon the measured results. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessor not blinded; however this was unlikely to have impacted upon the measured results. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | None reported |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | Non apparent |
Eldaba 2015.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 200 women Inclusion criteria: ASA I/II, aged 18‐30 years, elective CS Exclusion criteria: patient refusal, contraindication to spinal anaesthesia, known allergy to granisetron, patients receiving serotonin agonists or antagonists, ischaemic heart disease, chronic hypertension or pregnancy‐induced hypertension Setting: Egypt |
|
| Interventions |
Granisetron versus control Group 1: 1 mg granisetron diluted in 10 mL normal saline IV administered slowly over 1 min, 5 min prior to spinal anaesthesia Group 2: 10 mL normal saline IV administered slowly over 1 min, 5 min prior to spinal anaesthesia (placebo) All women received a crystalloid preload (500 mL Ringer's lactate), standardised positioning, standardised spinal anaesthetic technique and dose, standardised maintenance IVT. Hypotension was managed with a rapid bolus of 100 mL of Ringer's lactate. Vasopressors administered if MABP < 70 mmHg: ephedrine 5 mg IV bolus if heart rate was < 90 bpm, phenylephrine 0.1 mg IV bolus if heart rate > 90 bpm. Bradycardia (if not associated with hypotension) was treated with 0.5 mg atropine. |
|
| Outcomes |
Maternal: incidence of hypotension, heart rate Neonatal: Apgar scores at 1 min and 5 min |
|
| Notes | Hypotension was defined as MAP < 70 mmHg. Bradycardia defined as heart rate < 50 bpm. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐based randomisation |
| Allocation concealment (selection bias) | Unclear risk | Assignment in sealed envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blinded. Syringed were prepared by an anaesthetist who was blinded to the study protocol |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 5 excluded (3 from group 1 and 2 from group 2) due to conversion to GA No statement with respect to 'intention‐to‐treat' |
| Selective reporting (reporting bias) | Low risk | Most expected outcomes reported |
| Other bias | Low risk | None evident |
Embu 2011.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 50 women
Inclusion criteria: ASA I‐II, singleton pregnancy, elective CS under SAB Exclusion criteria: patients with pre‐existing hypertension or pregnancy‐induced hypertension, cardiovascular or cerebrovascular disease, autonomic neuropathy, spinal deformities, infections in the lumbar area, coagulopathies, hypovolaemia from any cause and SBP < 100 mmHg. Patients aged < 18 or > 40 years, weighing < 50 kg or > 100 kg, taller than 180 cm or shorter than 140 cm, and patients with placental complications, cord complications, fetal malformations and those babies whose birthweights were < 2.5 kg or > 4.5 kg by ultrasound Setting: Nigeria |
|
| Interventions |
Colloid preload versus crystalloid preload Group 1: 500 mL HES IV IV 10 min before SAB Group 2: 1000 mL of Ringer's lactate IV 10 min before SAB All patients: standardised preparation, monitoring, positioning, spinal anaesthetic dose and technique, IV fluids, oxygen delivery Hypotension treated with (unspecified) rapid infusion of IV fluids, followed by IV ephedrine 5 mg if not responding |
|
| Outcomes |
Maternal: incidence of hypotension, nausea and vomiting, dizziness and breathlessness, interval between preload‐to‐spinal injection and delivery and uterine incision‐to‐delivery Neonatal: Apgars at 1 min and 5 min |
|
| Notes | Hypotension defined as SBP < 80% of baseline or absolute value of SBP < 100 mmHg | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Patients were randomly allocated by drawing sealed envelopes which were shuffled |
| Allocation concealment (selection bias) | Unclear risk | Sealed envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Bag placed over fluid to conceal identity |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | None apparent |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Farid 2016.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 74 women Inclusion criteria: healthy patients; elective CS Exclusion criteria: patients who experienced complications during the surgery Setting: Pakistan |
|
| Interventions |
Crystalloid preload versus crystalloid coload Group 1 (P): received crystalloid preload 15 mL/kg Hartmann's solution 20 min prior to spinal anaesthesia Group 2 (C): received crystalloid coload 15 mL/kg Hartmann's solution at time of administration of spinal anaesthesia All women received standardised monitoring, standardised cannulation, standardised spinal anaesthetic technique and dose Hypotension was treated with vasopressor (phenylephrine or ephedrine) |
|
| Outcomes | Maternal: incidence of hypotension | |
| Notes | Hypotension was defined as reduction in MAP by > 20% from baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomly assigned by trainee anaesthesia or anaesthetist in charge of case" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | "Patients going into complications during surgery were excluded" – unspecified how many patients (if any) this involved. No further details provided |
| Selective reporting (reporting bias) | Low risk | Not evident |
| Other bias | Low risk | Not evident |
Faydaci 2011.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 90 women
Inclusion criteria: ASA1‐2, elective CS under SAB Exclusion criteria: not stated Setting: Turkey |
|
| Interventions |
Crystalloid preload: different doses Group 1: 10 mL/kg Ringer's lactate Group 2: 15 mL/kg Ringer's lactate Group 3: 20 mL/kg Ringer's lactate All preloads administered over 15 min before SAB with subsequent ephedrine infusion commenced immediately after SAB All women received standardised premedication/fasting, spinal dose and technique, position, monitoring Hypotension was treated with 10 mg IV bolus ephedrine |
|
| Outcomes |
Maternal: incidence of hypotension, nausea and vomiting, total amount ephedrine Neonatal: cord blood gas analysis, Apgars at 1 min and 5 min |
|
| Notes | Hypotension defined as decrease in MAP of > 20% | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random numbers |
| Allocation concealment (selection bias) | Low risk | "Enclosed system" presumably means covered |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Low risk | Not apparent |
| Other bias | Low risk | Not apparent |
French 1999.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 160 women Inclusion criteria: ASA I or II undergoing elective caesarean under spinal anaesthesia |
|
| Interventions |
Colloid preload versus crystalloid preload Group 1: pentastarch 10% in 0.9% saline 15 mL/kg Group 2: Hartmann's solution 15 mL/kg All women received a standardised anaesthetic technique with variable anaesthetic dose, followed by standardised surgical positioning. |
|
| Outcomes |
Maternal: BP; hypotension; block height; uterine incision to birth interval Neonatal: Apgar scores at 1 min and 5 min; cord pH |
|
| Notes | Hypotension was defined as SBP below 90 mmHg or < 70% below baseline. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomisation method not described |
| Allocation concealment (selection bias) | Low risk | Adequate: randomisation code by pharmacy and study drugs "covered with a black plastic bag to ensure blinding" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding: not specifically stated but anaesthetist and women presumably were blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Not reported |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Gomaa 2003.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 90 women Inclusion criteria: healthy pregnant women (25 to 40 years) undergoing elective caesarean under spinal anaesthesia Exclusion criteria: women known to be hypertensive Setting: Egypt |
|
| Interventions |
Ephedrine versus phenylephrine versus control Group 1: ephedrine, 50 mg IM Group 2: phenylephrine, 4 mg IM Group 3: 2 mL saline IM All study drugs given 10 min before spinal anaesthesia All women received a standardised crystalloid preload and a standardised spinal anaesthetic technique and dose followed by standardised surgical positioning. |
|
| Outcomes |
Maternal: hypotension Neonatal: cord/neonatal blood (reported as mean and SD); Apgar < 8 at 5 min (reported as mean and SD) |
|
| Notes | Hypotension was defined as 25% decrease in MAP from baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding: drugs were prepared by an anaesthetic assistant not involved in the study and injected by an anaesthetist not involved in data collection or care of the women |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses to follow‐up: not stated but losses unlikely |
| Selective reporting (reporting bias) | Low risk | Not apparent |
| Other bias | Low risk | Not apparent |
Grubb 2004.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 24 women Inclusion criteria: pregnant women scheduled for elective caesarean |
|
| Interventions |
Ephedrine versus control Group 1: ephedrine, 50 mg IM Group 2: saline IM Study drugs administered prior to spinal anaesthetic All women received standardised volume loading and a standardised spinal anaesthetic technique and dose followed by standardised surgical positioning. |
|
| Outcomes | Maternal: hypotension; nausea | |
| Notes | Hypotension was defined as defined as SBP < 70% baseline or < 90 mmHg | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Methods not described |
| Allocation concealment (selection bias) | Unclear risk | Methods not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding: described as "double‐blind placebo‐controlled" – no further details |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: not stated but losses unlikely |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Gulhas 2012.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 105 women Inclusion criteria: ASA I‐II, aged 18‐45 years, elective CS under SAB Exclusion criteria: contraindication to regional anaesthesia, ASA score III‐IV, < 18 years of age, multiple gestation, < 150 cm tall or > 170 cm tall, pre‐eclampsia, eclampsia, diabetes mellitus, intrauterine anomalities, using medications containing ephedrine or phenylephrine, failed SAB requiring conversion to general anaesthesia Setting: Turkey |
|
| Interventions |
Various doses of ketamine versus control Group 1: 0.25 mg/kg IV ketamine administered immediately following intrathecal injection Group 2: 0.5 mg/kg IV ketamine administered immediately following intrathecal injection Group 3: placebo control: 2 mL physiological saline administered immediately following intrathecal injection All women received a standardised crystalloid preload, a standardised spinal anaesthetic technique and dose), standardised monitoring and standardised surgical positioning. Hypotension was managed with 10 mg ephedrine IV. Atropine was administered if heart rate was < 45 bpm. |
|
| Outcomes |
Maternal: hypotension, ephedrine use, sedation score, shivering, pruritus, nausea and vomiting, hallucinations Neonatal: Apgars, cord blood pH |
|
| Notes | Hypotension defined as > 20% reduction in SBP from baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated numbers (Excel) by anaesthetist not involved in study |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinded outcome data assessors and "ward staff" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Blinded outcome data assessors and "ward staff" |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 3 patients excluded with failed blocks, flow diagram does not actually make sense from protocol as patients would have received placebo/Ketamine before exclusion |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Gunaydin 2009.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 60 women Inclusion criteria: ASA 2 women undergoing elective CS Exclusion criteria: starch allergies, history of anaphylaxis |
|
| Interventions |
Colloid preload versus crystalloid preload Group 1: IV infusion of 1000 mL Ringer's lactate preloading Group 2: IV infusion of 500 mL colloid Voluven 6% (6% HES 130/0.4 in isotonic NaCl solution) preloading All women received standardised cannulation, aspiration prophylaxis, spinal anaesthesia technique and dose and surgical positioning. Hypotension treated with 10 mg IV ephedrine |
|
| Outcomes |
Maternal: time for block onset and maximum sensory block level, maximum motor block time, block regression time, motor block duration, first analgesic requirement, mobilisation and onset of bowel sounds, the incidence of hypotension, total used ephedrine amount, nausea and vomiting Neonatal: 1 min and 5 min Apgar scores |
|
| Notes | Hypotension defined as a decrease in mean BP to 20% below baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method of sequence generation not specified. Reported as "randomly allocated" |
| Allocation concealment (selection bias) | Unclear risk | Closed envelope method |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Personel were blinded, participants were not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Not data loss, no losses to follow‐up |
| Selective reporting (reporting bias) | Low risk | Not reported |
| Other bias | Low risk | Not reported |
Gunusen 2010.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 120 women Inclusion criteria: healthy women aged 20‐40 years scheduled for elective caesarean delivery under spinal anaesthesia who had uncomplicated singleton, term pregnancy Exclusion criteria: chronic or pregnancy‐induced hypertension, cardiac disease, diabetes mellitus, height < 155 cm, a contraindication to spinal anaesthesia, or known fetal abnormality Setting: Turkey |
|
| Interventions |
Colloid preload versus crystalloid preload versus ephedrine infusion plus crystalloid co‐load Group 1: crystalloid preload: rapid infusion of Ringer's lactate 20 mL/kg, within 15‐20 min of the spinal block. Following anaesthesia, placebo infusion solution administered at a rate of 2.5 mL/min using an infusion pump. Ringer's lactate 1000 mL administered at minimal maintenance rate via 2nd cannula Group 2: colloid preload: 4% succinated gelatine solution (Gelofusine) 500 mL, within 15‐20 min of the spinal block Following anaesthesia, placebo infusion solution administered at a rate of 2.5 mL/min using an infusion pump. Ringer's lactate 1000 mL administered at minimal maintenance rate via 2nd cannula Group 3: ephedrine infusion plus crystalloid co‐load: no fluid preload given Following anaesthesia, infusion solution of ephedrine 50 mg in 100 mL (1.25 mg/mL) administered at rate of 2.5 mL/min using an infusion pump. Ringer's lactate1000 mL, administered rapidly via 2nd cannula All women received standardised aspiration prophylaxis, a standardised spinal anaesthetic technique and dose, standardised surgical positioning and standardised oxytocin administration. Hypotension (requiring intervention) was treated immediately with an IV bolus of ephedrine 5 mg from a separate syringe, repeated when necessary, every 2 min if hypotension persisted or recurred Hypertension treatment: infusion was stopped if the SBP and heart rate increased above the baseline values Bradycardia treatment consisted of IV atropine 0.5 mg. |
|
| Outcomes |
Maternal: moderate hypotension; severe hypotension; maternal bradycardia requiring intervention; maternal tachycardia; hypertension; nausea and vomiting Neonatal: acidosis (cord/neonatal blood with pH < 7.2); neonatal Apgar score < 8 at 5 min |
|
| Notes | Moderate hypotension was defined as a decrease of 20% from baseline, or an SBP < 95 mmHg. Severe hypotension was defined as a decrease of 30% from baseline. Bradycardia was defined as heart rate < 50 bpm. Tachycardia was defined heart rate > 120 bpm. Hypertension was defined as an increase in SBP > 30% above baseline. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation list |
| Allocation concealment (selection bias) | Unclear risk | "Randomly allocated" – concealment method not specified |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Pre‐load fluid in groups CO and CR was administered by an anaesthetic nurse who was not otherwise involved in the care of the patients. Co‐load fluids were prepared by an anaesthetic nurse who was independent of the study. Ringer's lactate in all groups were covered by a similar non‐transparent plastic bag in the perioperative period. The anaesthetist did not enter the operating room until the study solutions had been given, so that those recording data were unaware of the study group allocation. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | "Those recording data were unaware of the study group allocation." Attending paediatrician assessed Apgar scores – unclear if blinded to allocated treatment Umbilical blood samples were taken by the same midwife in the operating room – likely to have been blinded to allocated treatment |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 1/120 – 1 patient in crystalloid preload group was excluded from the study due to an inadequate spinal block |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Hall 1994.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 30 women Inclusion criteria: elective CS, singleton fetus Exclusion criteria: placental pathology, pregnancy exceeded 37 weeks' gestation Setting: UK |
|
| Interventions |
Variable ephedrine infusions versus phenylephrine infusion Group 1: infusion of ephedrine 1 mg/mL at 60 mL/h (1 mg/min) Group 2: infusion of ephedrine 2 mg/mL at 60 mL/h (2 mg/min) Group 3: infusion of phenylephrine at 10 μg/mL at 60 mL/h (10 μg/min) All women received the vasopressor for 30 min via Graseby pump All women received standard aspiration prophylaxis, IV cannulation, crystalloid preloading, surgical positioning, invasive arterial and non‐invasive BP monitoring, and standardised spinal anaesthetic technique and dose. Hypotension was managed with a 2 mL bolus of the vasopressor infusion. If pressure was > 20% above baseline for 3 min, the infusion was stopped. |
|
| Outcomes |
Maternal: incidence of hypotension, time for anaesthesia to reach T4 and maximum height of sensory loss, time between insertion of spinal needle and delivery of fetus, time from uterine incision to delivery of fetus, incidence of complications, total drug dose Neonatal: Apgar score 1 min and 5 min, umbilical arterial and venous blood samples |
|
| Notes | Hypotension was defined as SAP decrease > 20% below baseline Bradycardia was defined as heart rate < 40 bpm |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Anaesthetist who produced infusion not involved in anaesthetic. Blinding: women and anaesthetists blinded to allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: 1 woman excluded from group 2 due to data corruption |
| Selective reporting (reporting bias) | Low risk | None reported |
| Other bias | Low risk | None reported |
Hartley 2001.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 40 women Inclusion criteria: ASA I or II undergoing elective CS Exclusion criteria: weight > 90 kg, height < 150 cm or > 175 cm, multiple pregnancy, diabetes or hypertension |
|
| Interventions |
Lateral versus supine wedged Group 1: right‐lateral position adopted 2 min after spinal injection for 10 min, then turned to supine wedged (right hip) position Group 2: supine‐wedged (right hip) position adopted 1 min after spinal injection and maintained throughout Intervention occurred after spinal injection. All women received a standardised crystalloid preload and anaesthetic technique and dose. Bradycardia was managed with atropine. Hypotension was managed with ephedrine. |
|
| Outcomes | Maternal: hypotension; heart rate; block height; time to maximum block; time to birth; duration of hypotension; nausea/dizziness; ephedrine requirements | |
| Notes | Hypotension was defined as SBP < 80% baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomisation and allocation concealment: sealed envelope |
| Allocation concealment (selection bias) | Unclear risk | Sealed envelope |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses to follow‐up: not stated |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Hasan 2012.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 90 women Inclusion criteria: ASA I‐II, age 20‐35 years, weight 45‐60 kg, height 153‐165 cm Exclusion criteria: pregnancy‐induced hypertension, chronic hypertension, pre‐eclampsia, twin pregnancy, fetal compromise, diabetes mellitus, polyhydramnios, renal, liver or heart disease, coagulopathy Setting: Bangladesh |
|
| Interventions |
Crystalloid preload versus colloid preload versus combination preload Group 1: Ringer's lactate 20 mL/kg preloading Group 2: HES 6% 8 mL/kg preloading Group 3: combination of RL 10 mL/kg and HES 6% 4 mL/kg preloading All women received standardised cannulation, standardised spinal anaesthetic technique and dose, standardised surgical positioning, standardised oxygen therapy and standardised oxytocin dose after delivery Hypotension was treated with IV boluses of ephedrine 5 mg and rapid infusion of Ringer's lactate in all 3 groups |
|
| Outcomes |
Maternal: systolic, diastolic and mean BP measurements; total dose of ephedrine; total volume of IV fluid given Neonatal: Apgar scores |
|
| Notes | Hypotension defined as SBP less than 100 mmHg AND less than 20% of the baseline BP | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Unclear method. "Randomisations were done using card sampling" |
| Allocation concealment (selection bias) | Low risk | Anaesthetist who generated the random sequence infused the allocated fluid behind a screen set, separate from the outcome assessor. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participants and outcome assessors were blinded; however, the personnel who generated the random sequence and infused the fluid were not blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants included in final analysis |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Hwang 2012.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 86 women Inclusion criteria: elective CS Exclusion criteria: pre‐existing hypertension, pre‐eclampsia, cardiovascular disease, diabetes, obesity, multiple pregnancy Setting: South Korea |
|
| Interventions |
(R) lateral positioning versus wedged supine positioning Group 1: maintain the right lateral position for 6 min after spinal anaesthesia before assuming the wedged supine position Group 2: assumed the wedged supine position immediately after the spinal injection Wedging positioning was achieved with an air balloon (1500 mL) was inserted under the right upper buttock in the supine position in both groups. All women received standardised cannulation, standardised crystalloid preload, standardised oxygen therapy and standardised spinal anaesthetic technique and dose. Ephedrine was given if BP decreased > 30% from baseline ("severe hypotension") with increments of 5 mg at 2 min intervals |
|
| Outcomes |
Maternal: hypotension, nausea and vomiting, ephedrine requirement, maximum block height Neonatal: Apgar scores at 1 min and 5 min after birth, umbilical arterial blood gas analysis |
|
| Notes | Hypotension defined as a decrease in MAP of > 20% from baseline Severe hypotension defined as a decrease in MAP of > 30% from baseline |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Block randomisation (6 subjects per block) |
| Allocation concealment (selection bias) | Low risk | Opaque covers – removed immediately after intrathecal injection |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Unable to blind due to different positions but unlikely to affect observation |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Women were in different positions for 6 minutes therefore assessor was unblinded. After the women were put in the supine position, another observer who was blinded to patient group recorded the measurements. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Group 1: 1 excluded due to hypertension at baseline Group 2: 1 excluded due to inadequate block Excluded women not analysed in final results |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Idehen 2014.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 70 women Inclusion criteria: elective CS, ASA I or II Exclusion criteria: multiple pregnancy, weight > 115 kg, height < 150 cm, diabetes mellitus, hypertensive diseases in pregnancy intra‐uterine death, age < 18 years or > 40 years, patients on diuretics, contraindication to central neuraxial blockade Setting: Nigeria |
|
| Interventions |
Combination crystalloid/colloid preload versus crystalloid preload Group 1: 1000 mL crystalloid/colloid (6% pentastarch/Ringer's lactate, 750 mL/250 mL) combination IV preload Group 2: 500 mL colloid (6% pentastarch) IV preload Women in both groups received the same aspiration prophylaxis, IV cannulation, spinal anaesthesia technique and dose. Hypotension treated with 3 mg aliquots of ephedrine and rapid infusion of fluid. |
|
| Outcomes |
Maternal: incidence of hypotension, ephedrine requirement, nausea and vomiting, maximum block height, blood loss, urine output Neonatal: Apgar scores at 1 min and 5 min, birth asphyxia, meconium aspiration |
|
| Notes | Hypotension defined as SBP < 80% of baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Blind balloting |
| Allocation concealment (selection bias) | Unclear risk | Not reported, but double‐blinding |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Syringes were preloaded and wrapped |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Investigator who assessed the outcomes was blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | None reported |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Imam 2012.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 90 women Inclusion criteria: ASA I‐II, elective CS under spinal anaesthesia Setting: Pakistan |
|
| Interventions |
Crystalloid preload versus ephedrine alone versus combination of preload + ephedrine Group 1 (crystalloid group): fluid preload with Ringer's solution 20 mL/kg over 10‐15 min prior to intrathecal injection Group 2 (ephedrine group): IV ephedrine 0.25 mg/kg immediately after intrathecal injection Group 3 (combination group): fluid preload with Ringer's solution 20 mL/kg over 10‐15 min preceding intrathecal injection plus ephedrine 0.25 mg/kg immediately after intrathecal injection Spinal anaesthesia technique was not described. |
|
| Outcomes | Maternal: hypotension, nausea and vomiting | |
| Notes | Hypotension was not defined. It was not clear if they were assessing systolic, diastolic or mean BPs. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | States "randomised" but no elaboration |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | States "blind" but no elaboration |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | States "blind" but no elaboration |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | None reported |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Inglis 1995.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 40 women Inclusion criteria: women who presented for elective CS at term with a singleton pregnancy receiving spinal anaesthesia Exclusion criteria: women less than 150 cm in height, more than 170 cm in height, or whose babies showed evidence of fetal compromise |
|
| Interventions |
Right lateral position versus sitting position during spinal anaesthesia Group 1: right lateral (when anaesthesia induced) Group 2: sitting (when anaesthesia induced) All women received a preload of IV Hartmann's solution (1000 mL), a standardised spinal anaesthetic technique and dose, and standardised surgical positioning. |
|
| Outcomes | Maternal: hypotension; nausea and vomiting; time to block; women's satisfaction; ephedrine requirements | |
| Notes | Hypotension was defined as systolic pressure decreased to < 70% of baseline or < 100 mmHg. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomly allocated" – method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Block assessed by an investigator who was unaware of the women's original position |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 2 from lateral group removed from study (in 1, the spinal needle could not be inserted in the lateral position, but was successfully placed in the sitting position and for the other, a repeat block was needed) |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Jabalameli 2011.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 150 women Inclusion criteria: singleton pregnancy with ASA physical status I or II scheduled for elective caesarean under spinal anaesthesia, without pre‐existing systemic disease or pregnancy‐induced hypertension, preterm labour or signs of onset of labour, known fetal abnormalities, or without contraindications to spinal anaesthesia Exclusion criteria: any significant history of maternal medical or obstetric illness and any fetal compromise in current pregnancy Setting: Iran |
|
| Interventions |
Crystalloids versus colloids versus ephedrine Group1: crystalloid preload: Ringer's lactate solution (15 mL/kg) infused in 30 min before spinal injection. Group 2: colloid preload: colloid solution (Hexamel 7 mg/kg) infused in 30 min before spinal injection. Group 3: ephedrine: ephedrine (15 mg IV bolus) immediately after spinal injection, infused in 45 s. All women received a standardised spinal anaesthetic technique and dose, a standardised crystalloid coload, standardised leg wrapping and standardised surgical positioning. Hypotension (requiring intervention) received rescue boluses of 5 mg ephedrine given each 5 min |
|
| Outcomes |
Maternal: hypotension (SBP); hypotension, bradycardia; BP; heart rate; ephedrine requirement; vomiting; nausea; hypertension Neonatal: Apgar at 1 min and 5 min, umbilical cord blood pH, NACS |
|
| Notes | Hypotension was defined as SBP < 90 mmHg or > 20% below baseline. Bradycardia was defined as heart rate < 50 bpm. Hypertension was defined as SBP > 140 mmHg or > 20% baseline values. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random number table |
| Allocation concealment (selection bias) | Unclear risk | "Randomised" – not further specified except that sampling method was "consecutive" |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Reported that women and all staff involved in the study were blind to the protocol used; however, colloid and crystalloids were preloads while ephedrine was given immediately after the spinal injection. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Nurse assessing the severity of nausea and physician measuring neonatal outcomes were blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up |
| Selective reporting (reporting bias) | Low risk | Most expected outcomes were reported (although nausea was only reported as a continuous measure). |
| Other bias | Low risk | Similar baseline characteristics |
Jacob 2012.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 100 women Inclusion criteria: age 20‐40 years, ASA I‐II, singleton uncomplicated pregnancy, scheduled for elective caesarean under spinal anaesthesia Exclusion criteria: chronic hypertension, pregnancy‐induced hypertension, eclampsia, known cardiovascular disease, haematocrit < 30%, any contraindication to spinal anaesthesia, height < 150 cm Setting: India |
|
| Interventions |
Crystalloid preload versus crystalloid coload Group 1: 15 mL/kg over 20 min before placement of spinal block Group 2: 15 mL/kg of Ringer's lactate over 20 min starting as soon as CSF was tapped All women received standardised aspiration prophylaxis, standardised cannulation, standardised spinal anaesthetic technique and dose, standardised surgical positioning and standardised oxytocin regimen after delivery. Hypotension was treated with crystalloid boluses and 6 mg of ephedrine given intravenously every 3 min until SBP recovered to baseline value. The choice of crystalloid and the volume administered was left to the judgement of the attending anaesthetist. Bradycardia was treated with IV atropine 0.6 mg bolus. |
|
| Outcomes |
Maternal: hypotension, ephedrine requirement for hypotension, nausea and vomiting, pruritus, headache, hypertension, shivering, time from induction‐delivery and uterine incision to delivery, total IV fluid, blood loss Neonatal: Apgar scores at 1 min and 5 min, umbilical artery and vein blood gas measurements |
|
| Notes | Hypotension was defined as decrease in SBP to < 80% of baseline or SBP < 90 mmHg (whichever was lower). Bradycardia was defined as heart rate less than 50 bpm. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random numbers |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Neonatologist blinded Anaesthetist – not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Unclear risk | Not reported |
| Other bias | Unclear risk | Not reported |
James 1973.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 79 women Inclusion criteria: normotensive women undergoing repeat or primary CS for cephalopelvic disproportion |
|
| Interventions |
Lower limb compression versus control Group 1: plastic inflatable boots applied from toes to upper thighs and inflated immediately after spinal Group 2: control All women received a standardised crystalloid preload, a standardised spinal anaesthetic technique with dose adjusted according to subject's height and standardised surgical positioning. |
|
| Outcomes |
Maternal: hypotension Neonatal: Apgar scores at 1 min and 5 min (expressed as mean score) |
|
| Notes | Hypotension was defined as SBP < 100 mmHg | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding: not mentioned |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding: not mentioned |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: not stated |
| Selective reporting (reporting bias) | Unclear risk | Not apparent |
| Other bias | Unclear risk | Not apparent |
Jorgensen 1996.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 30 women Inclusion criteria: healthy, ASA I women undergoing elective CS Exclusion criteria: pre‐eclampsia, pregnancy‐induced hypertension, fetal abnormality, uteroplacental dysfunction |
|
| Interventions |
Lower limb compression versus control
Group 1: compression stockings (pressure equivalent to 54 mmHg) in place before spinal Group 2: control Intervention administered before spinal anaesthetic. All women received a standardised crystalloid preload, a standardised spinal anaesthetic technique with dose adjusted according to subject's height and standardised surgical positioning. |
|
| Outcomes | Maternal: hypotension; nausea; total ephedrine dose Neonatal: Apgar scores at 1 min, 5 min, and 10 min; umbilical cord blood pH (expressed as mean and SD) | |
| Notes | Hypotension was defined as SBP < 100 mmHg or 80% baseline. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation by "lottery", otherwise not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding: not mentioned |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding: not mentioned |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: 2 participants excluded from control group (1 failed spinal, 1 found to have pregnancy‐induced hypertension) |
| Selective reporting (reporting bias) | Unclear risk | Not apparent |
| Other bias | Unclear risk | Not apparent |
Jorgensen 2000.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 120 women Exclusion criteria: pre‐eclampsia, arterial hypertension or multiple pregnancy Setting: Denmark |
|
| Interventions |
Warm versus cold crystalloid preload Group 1: cold (21 degrees centigrade 0.9% saline preload) Group 2: warm (37 degrees centigrade saline preload) All women received a standardised spinal anaesthetic technique and dose as well as 5 mg IV ephedrine after spinal injection. |
|
| Outcomes | Maternal: hypotension; heart rate; arm discomfort; shivering; nausea; vomiting | |
| Notes | Hypotension was defined as < 70% decrease in SAP from baseline or 100 mmHg or less. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation: "computer generation" |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment: "sealed envelopes" |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding: not double‐blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding: not double‐blinded |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: 7/120 women were withdrawn from study, 2 because of failed spinal anaesthesia, 1 because of violation of selection criteria, and 5 because of protocol violations |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Karinen 1995.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 26 women Inclusion criteria: term parturients undergoing elective CS, healthy, uncomplicated singleton, non‐labouring |
|
| Interventions |
Colloid versus crystalloid preload Group 1: 500 mL 6% HES Group 2: 1000 mL Ringer's lactate Study drug infused over 10 min prior to spinal anaesthesia All women received standardised aspiration prophylaxis, standardised spinal anaesthetic technique and dose and standardised crystalloid infusion after spinal anaesthetic. |
|
| Outcomes | Maternal: hypotension; uterine artery pulsatile index; CVP; induction‐delivery time Neonatal: Apgar scores at 1 min, 5 min, and 15 min (incomplete data); umbilical artery pH (expressed as mean and range) | |
| Notes | Hypotension defined as SBP < 80% baseline or < 90 mmHg | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | "Sealed envelopes" – no further details provided |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding: obstetrician performing ultrasound blinded to allocation, other blinding not mentioned |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses to follow‐up: none |
| Selective reporting (reporting bias) | Unclear risk | Not reported |
| Other bias | Low risk | Not apparent |
Khan 2013.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 100 women Inclusion criteria: ASA I‐II, age 20‐35, single pregnancy, elective caesarean under spinal anaesthesia Exclusion criteria: hypertension, congestive cardiac failure, cardiovascular disease, fetal distress, any contraindication to spinal anaesthesia, > 800 mL blood loss in theatre Setting: India |
|
| Interventions |
Crystalloid preload versus crystalloid coload Group 1: preload of 20 mL/kg of Ringer's lactate over 20 min Group 2: coload of 20 mL/kg of Ringer's lactate at the maximal possible rate by pressurise giving set All women received no premedication, standardised cannulation, no further IV fluid except to keep IV line patent, standardised spinal anaesthetic technique and dose and standardised oxytocin postdelivery. Hypotension was treated with boluses of ephedrine 5 mg |
|
| Outcomes |
Maternal: incidence of hypotension, height of sensory block, systolic/diastolic/mean BP, ephedrine requirement Neonatal: Apgar sores at 1 min and 5 min |
|
| Notes | Hypotension was defined as decrease in SBP > 20% from baseline or decrease of systolic pressure to < 90‐100 mmHg | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | No blinding, but protocol well defined and seems unlikely to have affected results |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | No blinding, but protocol well defined and seems unlikely to have affected results |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Not reported |
| Selective reporting (reporting bias) | Low risk | Not apparent |
| Other bias | Low risk | Not apparent |
King 1998.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 30 women Inclusion criteria: undergoing elective CS Exclusion criteria: hypertension, pre‐eclampsia, preterm labour, juvenile diabetes, cocaine and methamphetamine use and cardiac disease |
|
| Interventions |
Ephedrine versus ephedrine + crystalloid versus crystalloid Group 1: ephedrine infusion group: 10 mL saline bolus followed by ephedrine infusion 1 mg/mL, i.e. 20 mg in 12 min Group 2: ephedrine bolus group: 10 mg ephedrine followed by saline infusion 5 mL/min for 2 min followed by 1 mL/min for 10 min Group 3: saline bolus 2 mL followed by infusion 5 mL/min for 2 min followed by 1 mL/min for 10 min All women received a standardised crystalloid preload followed by standardised infusion, a standardised spinal anaesthetic technique and dose and standardised positioning. |
|
| Outcomes |
Maternal: hypotension; time to first ephedrine rescue dose; number of hypotensive participants; total ephedrine dose Neonatal: Apgar scores at 1 min and 5 min |
|
| Notes | Hypotension was defined as SBP < 80% baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Low risk | Adequate: study drugs prepared by a third party (pharmacy) |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding: anaesthetist blinded to interventions |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: not stated |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Kohler 2002.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 100 women Inclusion criteria: healthy women (ASA I or II) scheduled for elective CS under spinal anaesthesia Exclusion criteria: pre‐eclampsia, arterial hypertension, gestational age less than 38 weeks or multiple pregnancy |
|
| Interventions |
Supine versus sitting positioning after spinal anaesthesia Group 1: modified supine (tilted 10 degrees to left) after spinal Group 2: sitting position for 3 min after spinal before modified supine (n = 52) All women received 200‐300 mL isotonic saline given before spinal, then an additional 15 mL/kg after a standardised spinal anaesthetic technique and dose. |
|
| Outcomes |
Maternal: hypotension; BP; nausea; vomiting; pain; level of anaesthesia; rescue with ephedrine; time from injection to birth; time from incision to birth Neonatal: umbilical arterial and venous blood; Apgar scores at 1 min and 5 min; time to sustained respiration; birthweight |
|
| Notes | Hypotension was defined as SBP < 70% of baseline or < 100 mmHg | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated codes |
| Allocation concealment (selection bias) | Low risk | Adequate: "assignments were kept in sealed sequentially‐numbered opaque envelopes" |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding: not mentioned |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Blinding: "haemodynamic data were transferred to a database by a person blind to which group the woman had been allocated" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses to follow‐up: 2/100 – 1 because of electrical power failure and 1 because of violation of selection criteria |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Kohli 2013.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 80 participants Inclusion criteria: age 18‐35 years, ASA I‐II, CS under spinal anaesthesia Exclusion criteria: contraindication to central neuraxial block, chronic hypertension, multiple pregnancy, diabetes mellitus, pregnancy‐induced hypertension, BMI > 30 kg/m² Setting: India |
|
| Interventions |
Mechanical compression versus control Group 1: sequential compression device used. The chambers of the device sequentially inflated from ankle to knee to a maximum pressure of 45‐50 mmHg at the ankle and 35 mmHg at the calf; the duration of compression was 12 s with a 60 s relaxation period between compressions Group 2: no sequential compression device used All women received "adequate" crystalloid preload, standardised monitoring, standardised spinal anaesthetic technique and dose. All women had SCD put on legs, but only group 1 had their SCDs turned on. Hypotension treated with 6 mg boluses of IV ephedrine. |
|
| Outcomes |
Maternal: incidence of hypotension, ephedrine use No neonatal outcomes |
|
| Notes | Hypotension was defined as decrease in SBP by > 20% from baseline. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Unclear risk | Not reported |
| Other bias | Unclear risk | Not reported |
Kuhn 2016.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 120 women Inclusion criteria: healthy pregnant women, term pregnancy, elective caesarean delivery, aged 18‐40 years, height 160‐180 cm, pre‐pregnancy BMI < 31 kg/m² Exclusion criteria: pre‐existing or gestation hypertension/pre‐eclampsia/cardiovascular or cerebrovascular disease/psychiatric or somatic disease (other then well‐treated mild asthma/thyroid hypofunction) or contraindications to spinal anaesthesia Setting: Norway |
|
| Interventions |
Phenylephrine versus leg wrapping versus control Group 1: phenylephrine (initial bolus 0.25 μg/kg followed by infusion 0.25 μg/kg/min) + sham leg‐wrapping Group 2: leg wrapping + IV placebo infusion Group 3: no treatment consisting of sham leg wrapping + IV placebo infusion All women received no premedication or IV prehydration, standardised IV cannulation, standardised monitoring (via LiDCOplus monitor including arterial line), standardised positioning, standardised spinal anaesthesia technique and dose, standardised crystalloid co‐hydration, standardised oxygen therapy, standardised oxytocin regimen. Leg wrapping or sham leg wrapping performed prior to spinal anaesthesia (refer to below for method of blinding) Study medicine infusion commenced at time of spinal anaesthesia, and ceased if SAP > 150 mmHg for > 3 min Hypotension was treated with IV bolus of 30 μg phenylephrine If hypotension was combined with bradycardia, or MAP < 60 mmHg, an IV bolus of 5 mg ephedrine was administered. |
|
| Outcomes |
Maternal: extent of decrease in SBP; change in cardiac output, systemic vascular resistance, stroke volume; heart rate; nausea and vomiting, pruritus Neonatal: umbilical artery and vein pH and BE, Apgar score |
|
| Notes | Hypotension was defined as SAP < 80% of mean SAP or SAP < 90 mmHg Bradycardia was defined as heart rate < 55 bpm |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Hospital pharmacy performed block randomisation into 3 groups of equal size using a pool of sealed and shuffled envelopes |
| Allocation concealment (selection bias) | Low risk | Sealed envelopes for leg wrapping, neutral syringes |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blinded Study medicine prepared in 50 mL syringes containing either phenylephrine or placebo, marked with randomisation number and neutral study information Instructions for therapeutic or sham wrapping placed into a sealed envelope for each patient Leg wrapping performed by specifically trained technical assistants after visual shielding between head of bed and lower extremities. Subsequently, legs were covered prior to positioning in lateral for spinal anaesthesia. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Randomisation codes not revealed until all measurements recorded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Group 1 Ph: 2 excluded (1 GA, 1 low‐quality data) Group 2 LW: 2 excluded (2 low‐quality data) Group 3 Con: 4 excluded (4 low‐quality data) |
| Selective reporting (reporting bias) | Low risk | Most expected outcomes were reported |
| Other bias | Low risk | Funding from South‐Eastern Norway Regional Authority through government research grant |
Kundra 2007.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 90 women Inclusion criteria: ASA physical status I or II, with full‐term singleton pregnancies and scheduled to undergo elective or emergency lower segment CS under subarachnoid block; without maternal or fetal complications Exclusion criteria: essential or pregnancy‐induced hypertension, diabetes, pre‐eclampsia, heart disease, placental abruption, prematurity (< 37 weeks' gestation), obesity, haemoglobin < 7g/dL, intrauterine growth restriction, fetal distress, fetal anomalies Setting: India |
|
| Interventions |
Left lateral tilt versus left manual uterine displacement Group 1: left lateral tilt: women received 15 degree left lateral tilt immediately following administration of anaesthetic Group 2: left manual uterine displacement: women received manual displacement of the uterus immediately following anaesthetic; positioned supine without left lateral tilt All women received standardised aspiration prophylaxis, standardised crystalloid preload, standardised spinal anaesthetic technique and dose. Hypotension (requiring intervention) was treated with IV boluses of ephedrine (6 mg) until SBP was restored to > 90 mmHg. |
|
| Outcomes |
Maternal: hypotension; ephedrine requirement Neonatal: Apgar at 1 min, 5 min, and 10 min |
|
| Notes | Hypotension was defined as SBP < 90 mmHg or < 80% of baseline value Bradycardia defined as heart rate < 60 bpm |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random numbers |
| Allocation concealment (selection bias) | Unclear risk | "Sealed envelope technique." |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "Manual displacement of the uterus was provided by a person other than the attending anaesthetist who was blinded to the haemodynamic parameters being displayed by screen separation." |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Apgar scores were assessed by a clinician who was blinded to group assignment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses reported |
| Selective reporting (reporting bias) | Unclear risk | Not all expected outcomes were reported or reported completely |
| Other bias | Low risk | Baseline characteristics were similar |
Kundra 2008.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 60 women Inclusion criteria: ASA class I and II, single term pregnancies, scheduled for elective caesarean under spinal anaesthesia Exclusion criteria: pre‐existing or pregnancy‐induced hypertension, known cardiovascular disease or contraindications to spinal anaesthesia Setting: India |
|
| Interventions |
Ephedrine versus crystalloid preload Group 1: ephedrine: ephedrine infusion prepared in 0.9% NS (1 mg/mL), started prophylactically at a rate of 5 mg/min for the first 2 min and then at a rate of 1 mg/min for the next 18 min, following administration of spinal anaesthetic Group 2: crystalloid preload: Ringer's lactate 500 mL, infused rapidly over 15‐20 min before institution of spinal anaesthetic All women received a standardised spinal anaesthetic technique and dose followed by a standardised crystalloid infusion. Hypotension requiring intervention received 5 mg IV bolus ephedrine, repeated if necessary. |
|
| Outcomes |
Maternal: hypotension; induction to birth time; total ephedrine dose; adverse effects; heart rate Neonatal: Apgar scores; umbilical venous gases |
|
| Notes | Hypotension was defined as a > 20% fall in SBP | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomly divided into two groups" |
| Allocation concealment (selection bias) | Unclear risk | Sealed envelope |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Described as "single‐blinded" but unlikely that blinding was possible as women in the ephedrine group had 2 separate IV lines established, while those in the crystalloid group had only 1 line |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | None reported |
| Selective reporting (reporting bias) | Unclear risk | Neonatal outcomes not reported in a form that could be used in this review |
| Other bias | Low risk | Similar baseline characteristics |
Lin 1999.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 60 women Inclusion criteria: healthy parturients undergoing primary or repeat CS, gestation 33‐41 weeks, uncomplicated singleton, not in labour, ASA I |
|
| Interventions |
Colloid preload versus crystalloid preload Group 1: 500 mL dextran 40 (n = 30) Group 2: 1000 mL Ringer's lactate (n = 30) Study drug administered over 20 min prior to spinal All women received a standardised spinal anaesthetic technique with variable dose (1.8‐2.2mL 0.5% bupivacaine). |
|
| Outcomes |
Maternal: hypotension; uterine incision‐delivery time; estimated blood loss; urine output; nausea Neonatal: Apgar scores at 1 min and 5 min |
|
| Notes | Hypotension defined as SBP < 70% baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding not mentioned |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding not mentioned |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: not stated |
| Selective reporting (reporting bias) | Unclear risk | Not reported |
| Other bias | Unclear risk | Not apparent |
Loke 2002.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 40 women Inclusion criteria: ASA I women presenting for elective caesarean under spinal anaesthesia |
|
| Interventions |
Head‐down tilt versus control: Group 1: anaesthesia induced in right lateral position (woman's spine inclined at 5 to 6 degrees from horizontal with head slightly lower); anaesthesia induced in right lateral position 10 degree head‐up tilt Group 2: anaesthesia induced in right lateral position (woman's spine inclined at 4 to 5 degrees from horizontal with head slightly higher). All women received a standardised preload of 1 litre crystalloid IV and a standardised spinal anaesthetic technique and dose. |
|
| Outcomes |
Maternal: hypotension; sensory block; ephedrine requirement; nausea; pain Neonatal: Apgar scores at 1 min and 5 min |
|
| Notes | Hypotension defined as SBP < 90 mmHg | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | "Sealed envelope method" |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not mentioned |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Blinding: outcome assessors were only admitted to the operating room once the position of the operating table had been readjusted |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses to follow‐up: none reported but losses unlikely |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Loo 2002.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 40 women Inclusion criteria: undergoing elective CS, ASA I, age 18 to 40 years, height > 150 cm, weight < 100 kg, full‐term singleton fetus with no congenital abnormalities, no polyhydramnios, no intrauterine growth retardation, and estimated fetal weight > 2500 g |
|
| Interventions |
Ephedrine + crystalloid co‐load versus crystalloid preload Group 1: prophylactic ephedrine 6 mg IV and 1000 mL Ringer's lactate commenced immediately after spinal anaesthesia Group 2: preload of 1000 mL Ringer's lactate All women received a standardised spinal anaesthetic technique and dose. |
|
| Outcomes |
Maternal: hypotension (defined as SBP < 100 mmHg); BP; heart rate; time to block; ephedrine dose Neonatal: Apgar scores |
|
| Notes | Hypotension defined as SBP < 100 mmHg | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment: "divided into two groups" |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding: described as "double‐blinded" but no further details provided |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: not stated |
| Selective reporting (reporting bias) | Unclear risk | Unclear reporting |
| Other bias | Low risk | None apparent |
Loughrey 2002.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 67 women (= 68 neonates due to 1 twin pregnancy in the control group) Inclusion criteria: term and peri‐term women presenting for elective CS Exclusion criteria: moderate to severe pre‐eclampsia, history of essential hypertension, contraindication to spinal anaesthesia |
|
| Interventions |
Ephedrine (different doses) versus control Group 1: 6 mg ephedrine Group 2: 12 mg ephedrine Group 3: 0.9% saline IV bolus (control) The study drug was given simultaneously with the anaesthetic. All women received a standardised crystalloid preload and thromboembolic stockings were not worn. All women received a standardised spinal anaesthetic technique and dose. |
|
| Outcomes |
Maternal: hypotension; doses of ephedrine; heart rate; hypertension; nausea or vomiting Neonatal: cord arterial pH; Apgar score at 5 min |
|
| Notes | Hypotension was defined as a reduction in SAP > 30% from baseline or < 90 mmHg. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Computer‐generated" |
| Allocation concealment (selection bias) | Low risk | Adequate: study drugs coded by hospital pharmacy |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding: "double‐blind" – all observers were blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses to follow‐up: 2/67 – 1 woman in the saline group was excluded because an infusion of ephedrine was administered following the spinal injection and another because of administration of IV fentanyl to supplement analgesia |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Loughrey 2005.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 43 women Inclusion criteria: ASA I and II non‐labouring women undergoing scheduled elective caesareans; term uncomplicated singleton pregnancies, women taking only prenatal vitamins and weighing less than 100 kg Exclusion criteria: cardiac, pulmonary or renal diseases or systemic diseases that could influence haemodynamic responses, including pre‐eclampsia, hypertension and diabetes; if women were taking or had a history of taking any medications that could influence haemodynamic responses, including magnesium sulphate, terbutaline or B‐blockers |
|
| Interventions |
Phenylephrine versus control Group 1: 10 mg ephedrine IV Group 2: 40 µg phenylephrine + 10 mg ephedrine The IV bolus of study drug was administered simultaneously with the intrathecal anaesthetic injection. All women received a standardised crystalloid preload, did not wear thromboembolic stockings and received a standardised spinal anaesthetic technique and dose. IV preload with 10 mL/kg of Ringer's lactate; and 10mg IV ephedrine administered simultaneously with study drug For rescue from hypotension, women in the ephedrine only group were given 5 mg ephedrine and women in the ephedrine + phenylephrine group were given 5 mg ephedrine + 20 µg phenylephrine. |
|
| Outcomes |
Maternal: hypotension; heart rate; nausea; rescue boluses; total mean ephedrine dose; total mean phenylephrine dose Neonatal: umbilical artery pH (mean and SD); umbilical vein pH (mean and SD); Apgar scores at 1 min and 5 min |
|
| Notes | Hypotension was defined as SBP < 100 mmHg or a decrease in SBP of 20% from baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | "Sealed envelope" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding: "double‐blinded"; anaesthetist remained blinded to the study solution throughout |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: 3/43 – 1 woman in the ephedrine only group and 2 in the ephedrine/phenylephrine group were excluded from analysis due to improper data collection before unblinding |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Madi‐Jebara 2008.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 120 women Inclusion criteria: non‐labouring ASA I and II women having non‐urgent CS Exclusion criteria: obesity (> 115 kg), height < 152 cm, diabetes, pregnancy‐induced hypertension, chronic hypertension, heart disease, multiple gestation, age < 18 or > 40 years Setting: Lebanon |
|
| Interventions |
Colloid versus crystalloid Group 1: HES (500 mL) Group 2: Ringer's lactate (1000 mL) All women received study fluid administered as preload before spinal. No IV fluids were administered prior to anaesthesia. Standardised spinal anaesthetic technique and dose. Hypotension (requiring intervention) received IV boluses of 3 mg ephedrine; repeated every 2 min if hypotension persisted or recurred |
|
| Outcomes |
Maternal: hypotension; nausea and/or vomiting Neonatal: Apgar scores; umbilical arterial and venous pH |
|
| Notes | Hypotension defined as SBP < 100 mmHg or 20% decrease from baseline. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomly assigned" – no further details given |
| Allocation concealment (selection bias) | Unclear risk | As above |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up |
| Selective reporting (reporting bias) | Unclear risk | None of the neonatal outcomes were reported in a form that could be used in this review. |
| Other bias | Low risk | Baseline characteristics were similar. |
Magalhaes 2009.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 60 women Inclusion criteria: ASA I or II, term pregnancy, of single fetus, indication for CS Exclusion criteria: refusal to participate in study, patients aged < 18 years, pre‐existing or pregnancy‐induced systemic hypertension, presence of cardiovascular or cerebrovascular diseases, fetal abnormalities, history of allergy to drugs used in the study, contraindications to spinal block Setting: Brazil |
|
| Interventions |
Prophylactic ephedrine versus prophylactic phenylephrine Group 1: prophylactic IV dose of 10 mg ephedrine immediately after spinal block Group 2: prophylactic IV dose of 80 μg phenylephrine immediately after spinal block Standardised monitoring and positioning, standardised spinal anaesthetic technique (at L2‐L3 or L3‐L4) and dose, standardised crystalloid coload and maintenance No significant baseline differences between groups Hypotension was managed with a bolus dose of 50% of study drug Bradycardia was treated with 0.75 mg atropine |
|
| Outcomes |
Maternal: level of block, time from blockade at T5 to incision of skin, incision of uterus and removal of fetus was recorded, incidence of maternal hypotension, reactive hypertension, bradycardia, nausea/vomiting, total dose of vasopressor Neonatal: Apgar scores at 1 min and 5 min, pH < 7.2 |
|
| Notes | Hypotension was defined as BP less than or equal to 80% baseline. Reactive hypertension was defined as BP > 20% baseline values after the use of the vasopressor. Bradycardia was defined as heart rate < 50 bpm. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random numbers |
| Allocation concealment (selection bias) | Low risk | Sequential sealed envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "Double blind": syringes of study drugs prepared by a physician who was not involved with data collection and analysis |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | "Result of allocation was ignored by both patients & physicians responsible for collecting & analysing study parameters." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up reported |
| Selective reporting (reporting bias) | Low risk | Most expected outcomes were reported |
| Other bias | Unclear risk | No apparent sources of other bias |
Marciniak 2013.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 60 women Inclusion criteria: ASA I‐II, elective CS Exclusion criteria: patient refusal to participate in study, contraindication to perineural anaesthesia, multiple pregnancies, body weight > 115 kg, height < 152 cm, age < 18 or > 40 years old, diabetes, pregnancy‐induced hypertension, chronic hypertension, heart disease Setting: Poland |
|
| Interventions |
Comparison of 2 different colloid solutions as preload: Voluven versus Tetraspan Women were transfused 1 of the following solutions prior to spinal anaesthesia: Group 1: 500 mL transfusion of 6% HES 130/0.4 with 0.9% NaCl prior to anaesthesia (Voluven) over 15 min Group 2: 500 mL of 6% HES 130/0.42 in a physiological electrolyte solution (Tetraspan) over 15 min All women received standardised aspiration prophylaxis, standardised spinal anaesthetic technique and dose, standardised oxygen therapy and standardised oxytocin administration after delivery. Until the birth of the child, the patient did not receive any further IV fluid. Hypotension was managed with 5‐10 mg of IV ephedrine. During delivery 40% O2 given via mask. 10 units oxytocin IV given after delivery |
|
| Outcomes |
Maternal: BP, time to skin incision/delivery/uterine incision Neonatal: Apgar scores 1, 3, 5, 10 min after birth, pH of venous and arterial umbilical blood |
|
| Notes | Hypotension defined as a drop in SBP of 20% below the baseline pressure (or below 100 mmHg) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Unclear risk | Not reported |
| Other bias | Low risk | 5 patients from Group 1 and 4 patients from Group 2 were removed from the study due to problems with cord blood collection for gaso‐metric tests (e.g. inability to perform dual collection of blood samples from the same vessel or no collection). Successful tests were conducted in the remaining 51 patients (25 in Group 1 and 26 in Group 2) |
Marciniak 2015.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 72 women Inclusion criteria: ASA I/II, elective CS due to cephalopelvic disproportion, post‐C‐section condition, gluteal position, ophthalmic indications and those without medical indications Exclusion criteria: lack of consent, contraindications to spinal anaesthesia, multiple pregnancy, body weight > 155 kg, height < 152 cm, age < 18 years or > 40 years, diabetes mellitus, pregnancy‐induced hypertension, chronic hypertension, cardiac diseases, use of selective serotonin reuptake inhibitors Setting: Poland |
|
| Interventions |
Ondansetron versus control Group 1 (O): 8 mg ondansetron in 10 mL 0.9% NaCl IV Group 2 (P): 10 mL 0.9% NaCl IV Syringe content administered over 1 min, after colloid preload and 5 min prior to spinal anaesthesia. All women received standardised aspiration prophylaxis, standardised monitoring, standardised cannulation and colloid prehydration, standardised spinal anaesthetic technique and dose. Hypotension was managed with fractionated IV ephedrine boluses. Bradycardia was managed with 0.5 mg atropine. |
|
| Outcomes |
Maternal: hypotension, bradycardia Neonatal: Apgar scores at 1 min and 5 min, baby's weight, umbilical vein acid‐base status |
|
| Notes | Hypotension was defined as a 20% decrease in systolic pressure or decrease in systolic pressure < 90 mmHg Bradycardia was defined as heart rate < 60 bpm |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Online randomisation programme |
| Allocation concealment (selection bias) | Low risk | Study drug prepared by anaesthetist otherwise uninvolved in study |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | The anaesthetist preparing the solution was on call, and the anaesthetist administering the solution was blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 2 patients in placebo group received IV opioids due to insufficient analgesia and were thus excluded from the study |
| Selective reporting (reporting bias) | Low risk | Most expected outcomes were reported |
| Other bias | Low risk | None evident |
Mathru 1980.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 87 women Inclusion criteria: healthy parturients undergoing elective caesarean under spinal anaesthesia |
|
| Interventions |
Colloid + crystalloid versus crystalloid versus ephedrine + crystalloid versus ephedrine + colloid + crystalloid Group 1: 5% albumin in Ringer's lactate with 5% dextrose solution (15 mL/kg) Group 2: Ringer's lactate with 5% dextrose solution (15 mL/kg) Group 3: Ringer's lactate with 5% dextrose solution (15 mL/kg) plus ephedrine 25 mg IM Group 4: 5% albumin in Ringer's lactate with 5% dextrose solution (15 mL/kg) plus ephedrine 25 mg IM Fluids were administered as a preload over 15‐20 min before spinal anaesthesia. All women received a standardised anaesthetic technique with variable local anaesthetic dose (6‐8 mg 0.5% hyperbaric tetracaine). |
|
| Outcomes |
Maternal: hypotension; MAP; heart rate Neonatal: Apgar scores |
|
| Notes | Hypotension defined as a decrease in SBP below 90 torr | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding not stated |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding not stated |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: not stated |
| Selective reporting (reporting bias) | Unclear risk | Inadequate reporting |
| Other bias | High risk | Variable dose of local anaesthetic used for spinal anaesthesia |
Mercier 2014.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 167 women Inclusion criteria: ASA I‐II, elective caesarean under spinal anaesthesia, aged > 18 years, weight > 60 kg and < 95 kg, term singleton pregnancy (> 37 weeks' gestation) Exclusion criteria: concomitant diseases (e.g. pregnancy‐induced hypertension, diabetes mellitus, cardiovascular or cerebrovascular disease, coagulation disorders), fetal complications, contraindications to spinal anaesthesia or HES administration, emergency CS, women who received IV fluid prior to admission to theatre Setting: multicentre, France |
|
| Interventions |
Colloid versus crystalloid preload Group 1: HES: 500 mL 6% HES 130/0.4, followed by 500 mL Ringer's lactate Group 2: RL: 500 mL of Ringer's lactate, followed by second infusion of 500 mL Ringer's lactate All women received standardised aspiration prophylaxis, standardised monitoring, standardised anaesthetic technique and dose. Maternal bradycardia treated with atropine 0.5‐1 mg IV Hypotension treatment: SBP > 95% baseline – no treatment, SBP 94‐80% baseline received 50 μg phenylephrine, SBP 79%‐90% of baseline received 100 μg phenylephrine, SBP < 70% of baseline received 150 μg phenylephrine. Sustained nausea and vomiting was treated with ondansetron 4 mg IV. |
|
| Outcomes |
Maternal: incidence of hypotension; time of onset of hypotension; symptomatic hypotension; nausea and vomiting; dizziness; minimum heart rate; bradycardia; atropine and phenylephrine requirement Neonatal: Apgar scores at 1 min and 5 min, umbilical arterial and venous pH |
|
| Notes | Hypotension defined as SBP < 80% of baseline Bradycardia defined as heart rate < 50 bpm |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation sequence using SAS software; blocks of 4 |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind: "study fluids were provided in indistinguishable 500 mL bottles in both groups with randomisation code, as previously pictured." |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Clearly reported in study results 11 protocol violations in HES group, and 10 in the Ringer's group Intention‐to‐treat analysis |
| Selective reporting (reporting bias) | Low risk | Not apparent |
| Other bias | High risk | Fully funded by Fresenius Kabi, the company that produces HES |
Miyabe 1997.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 34 women Inclusion criteria: term parturients undergoing elective CS, ASA I Exclusion criteria: not specified |
|
| Interventions |
Head‐up versus control Group 1: horizontal Group 2: 10 degree head‐down tilt All women received a standardised anaesthetic technique and dose. |
|
| Outcomes |
Maternal: hypotension; block height; fluid; ephedrine doses Neonatal: none stated |
|
| Notes | Hypotension defined as SBP < 100 mmHg | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding not mentioned |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding not mentioned |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: not stated |
| Selective reporting (reporting bias) | Unclear risk | Unclear reporting |
| Other bias | Unclear risk | Unclear reporting |
Mohta 2010.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 60 women Inclusion criteria: ASA I or II women with term uncomplicated pregnancies, scheduled to undergo elective CS under subarachnoid block Exclusion criteria: pregnancy‐induced hypertension, cardiovascular disease, cerebrovascular disease, placental or fetal abnormalities, absolute or relative contraindication to spinal anaesthesia and women with SBP < 100 mmHg Setting: India |
|
| Interventions |
Phenylephrine versus mephentermine Group 1: infusion of phenylephrine (50 μg/mL); administered immediately following spinal anaesthesia, at a rate of 60 mL/h (50 μg/min) Group 2: infusion of mephentermine s (600 μg/mL); administered immediately following spinal anaesthesia, at a rate of 60 mL/h (600 μg/min) All women received a standardised fluid preload and standardised spinal anaesthetic technique. Spinal anaesthetic dose was 2.2 mL of hyperbaric 0.5% bupivacaine unless patient's height was < 150 cm, in which case the dose was 2 mL. Hypotension was managed with a 2 mL bolus dose of respective vasopressor solution (100 μg phenylephrine or 1.2 mg mephentermine). Hypertension was managed with stepwise reduction in infusion by 6 mL/h. Bradycardia was managed with 0.3 mg boluses of atropine. |
|
| Outcomes |
Maternal: hypotension; reactive hypertension; bradycardia; nausea; vomiting; dizziness Neonatal: umbilical arterial and venous blood gases; Apgar scores at 1 min and 5 min |
|
| Notes | Hypotension was defined as fall of ≥ 20% from baseline or an absolute value of < 100 mmHg SBP, whichever was higher. Hypertension was defined as a rise in SBP > 20% above baseline. Bradycardia was defined as heart rate < 50 bpm |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomly divided into two groups of 30 each" |
| Allocation concealment (selection bias) | Unclear risk | "Sealed envelope" |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Described as double‐blind: "the solution of vasopressor for infusion was prepared by an assistant who was not involved in the study, and the investigator, as well as the patient, were thus blinded to the identity of vasopressor used" However, it was not possible for the anaesthetist to be blinded as treatment of hypotension with "the respective vasopressor solution" would have required knowledge of which vasopressor was used. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up |
| Selective reporting (reporting bias) | Low risk | Most expected outcomes were reported |
| Other bias | Low risk | Similar baseline characteristics except for a lower mean baseline heart rate in the phenylephrine group |
Morgan 2000.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 185 women Inclusion criteria: healthy women with uncomplicated term pregnancies undergoing elective CS Exclusion criteria: not specified |
|
| Interventions |
Variable ephedrine infusions versus crystalloid preload alone versus crystalloid preload + variable ephedrine infusions Group 1: ephedrine infusion alone at 1 mg/min from spinal injection until birth Group 2: ephedrine infusion alone at 2 mg/min from spinal injection until birth Group 3: ephedrine infusion alone at 3‐4 mg/min from spinal injection until birth Group 4: Ringer's lactate 1000 mL over 20 min before spinal injection Group 5: Ringer's lactate 1000 mL over 20 min before spinal injection plus ephedrine infused at 1 mg/min from spinal injection until birth Group 6: Ringer's lactate 1000 mL over 20 min before spinal injection plus ephedrine infused at 2 mg/min from spinal injection until birth Group 7: Ringer's lactate 1000 mL over 20 min before spinal injection plus ephedrine infused at 3‐4 mg/min from spinal injection until birth All women received a standardised spinal anaesthetic technique and dose. |
|
| Outcomes |
Maternal: hypotension; heart rate; hypertension Neonatal: umbilical artery pH (expressed as means ± SD), BE |
|
| Notes | Hypotension defined as decrease in SBP > 30% from baseline Tachycardia defined as heart rate > 130 bpm Hypertension defined as SBP > 150 mmHg |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding: "double blinded" – no further details |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: not stated |
| Selective reporting (reporting bias) | Unclear risk | Unclear reporting |
| Other bias | Unclear risk | Unclear reporting |
Moslemi 2015.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 90 recruited, 83 completed analysis Inclusion criteria: healthy pregnancy of gestational age 36 weeks or higher, non‐emergency CS Exclusion criteria: below 36 weeks' gestation, emergence CS, high‐risk pregnancies (multiple gestations, intrauterine growth retardation, pre‐eclampsia, maternal cardiovascular or respiratory diseases), any contraindication of spinal anaesthesia (patient refusal, coagulopathy, haemorrhage or hypovolaemic shock), unexpected events during surgery (haemorrhage, sensory block higher or lower than T4‐T5 after spinal anaesthesia) Setting: Iran |
|
| Interventions |
Phenylephrine versus ephedrine versus crystalloid Group 1: 450 μg phenylephrine in 250 cc normal saline administered over 30 min after preload Group 2: 45 mg ephedrine in 250 cc normal saline administered over 30 min Group 3: 250 cc normal saline infused over 30 min All women received standardised monitoring, standardised crystalloid preload and standardised spinal anaesthetic technique and dose. Hypotension was treated with study vasopressor (clinician blinded to which vasopressor): Group 1 received 50‐100 μg phenylephrine Group 2 and 3 received 5‐10 mg ephedrine. |
|
| Outcomes |
Maternal: incidence and degree of hypotension, heart rate and rhythm, nausea/vomiting, number of vasopressor therapy and total dose, "any other intra or post‐operative complication". Neonatal: arterial blood gas, Apgar at 1 min and 5 min |
|
| Notes | Hypotension defined as drop in BP > 20% baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation list |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Study drugs labelled with numerical codes and investigators were blinded Double‐blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Double‐blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Group 1: 4 excluded due to very high or very low sensory block Group 2: 3 excluded due to very high or very low block |
| Selective reporting (reporting bias) | Low risk | Group 1: 4 excluded due to very high or very low sensory block Group 2: 3 excluded due to very high or very low block |
| Other bias | Low risk | None apparent Funded by: University of Medical Sciences and Women's Reproductive Health Research Centre |
Muzlifah 2009.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 80 women Inclusion criteria: ASA I or II women scheduled for elective CS under spinal anaesthesia, normal singleton pregnancy; > 36 weeks' gestation; BMI 20‐38 kg/m²; height > 145 cm Exclusion criteria: contraindications for spinal anaesthesia and failed spinal necessitating conversion to GA Setting: Malaysia |
|
| Interventions |
Crystalloids: different preload volumes Group 1: low volume crystalloid 10 mL/kg of Ringer's lactate infusion preload Group 2: high volume crystalloid 20 mL/kg of Ringer's lactate infusion preload All women received standardised aspiration prophylaxis, standardised anaesthetic technique and dose, standardised fluid maintenance. Hypotension was managed with 6 mg boluses of ephedrine. |
|
| Outcomes | Maternal: hypotension; BP; ephedrine requirement; nausea; vomiting; oxygen saturation; respiratory rate | |
| Notes | Hypotension was defined as a > 20% fall in MAP from baseline. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Coin toss |
| Allocation concealment (selection bias) | Unclear risk | "Randomly allocated" – no further details reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Described as "single blinded" – no further details reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up reported |
| Selective reporting (reporting bias) | High risk | No neonatal outcomes were reported |
| Other bias | Low risk | Similar baseline characteristics |
Nazir 2012.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 100 women Inclusion criteria: ASA grade I women undergoing elective CS under spinal anaesthesia with a normal singleton pregnancy beyond 36 weeks' gestation Exclusion criteria: pregnancy‐induced hypertension, diabetes, cardiovascular or cerebrovascular disease, fetal abnormalities, contraindication to spinal anaesthesia Setting: India |
|
| Interventions |
Prophylactic ephedrine versus phenylephrine Group 1: prophylactic bolus of ephedrine 10 mg IV 1 min after intrathecal injection Group 2: prophylactic dose of phenylephrine 100 μg IV 1 min after intrathecal injection All women received standardised premedication, a standardised fluid preload, a standardised spinal anaesthetic technique (in either lateral or seated position) and dose, standardised surgical positioning. Hypotension managed with rescue boluses of ephedrine 5 mg IV (group 1) or phenylephrine 50 μg IV (group 2) whenever maternal SBP was recorded as less than 90 mmHg. Bradycardia was treated with atropine 300 μg IV bolus. |
|
| Outcomes |
Maternal: BP (systolic, diastolic, mean); heart rate; need for rescue bolus(es); need for atropine Neonatal: Apgar scores at 1 min and 5 min; umbilical cord blood pH (unclear as to venous or arterial); results for Apgar and pH < 7.2 |
|
| Notes | Definition of hypotension is a SBP measurement < 90 mmHg. Bradycardia was defined as heart rate < 60 bpm. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomly allocated into two groups of 50 each" – method not specified |
| Allocation concealment (selection bias) | Unclear risk | "Randomly allocated into two groups of 50 each" – method not specified |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "Double blind" – the vasopressor solutions were prepared in identical syringes by an anaesthetist or investigator who was not involved in subsequent patient care |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Not reported, but outcomes probably recorded by staff involved in care |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses reported |
| Selective reporting (reporting bias) | Low risk | Most expected outcomes reported |
| Other bias | Low risk | None evident |
Ngan Kee 2000.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 80 women Inclusion criteria: ASA I or II Asian women with term singleton pregnancies having elective CS Exclusion criteria: pre‐existing or pregnancy‐induced hypertension, known cardiovascular or cerebrovascular disease, or contraindications to spinal anaesthesia Setting: Hong Kong, China |
|
| Interventions |
Ephedrine + crystalloid preload (different doses) versus crystalloid preload alone Group1: ephedrine 10 mg Group 2: ephedrine 20 mg Group 3: ephedrine 30 mg Group 4: saline control All were diluted to 10 mL with saline and injected intravenously over 30 s. All women received a standardised crystalloid preload with Ringer's lactate followed by a standardised spinal anaesthetic technique and dose. |
|
| Outcomes |
Maternal: hypotension; hypertension; heart rate; total ephedrine dose; nausea or vomiting; upper sensory level; skin incision to birth and uterine incision to birth time Neonatal: Apgar scores at 1 min and 5 min; umbilical arterial and venous blood gas and pH; cardiotocograph |
|
| Notes | Hypotension defined as SBP < 80% baseline or < 100 mmHg Hypertension defined as SBP > 120% baseline |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Coded, opaque shuffled envelopes – randomisation method not described |
| Allocation concealment (selection bias) | Low risk | Adequate: coded, opaque shuffled envelopes, study drugs were prepared by an anaesthetist not involved in assessing women |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Double‐blind (participants and anaesthetists) – no further details |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: maternal heart rate data lost in 1 woman (out of 20) from 10 mg group; cord blood samples incomplete in 2 each from control (n = 20), 20 mg (n = 20) and 30 mg (n = 20) groups |
| Selective reporting (reporting bias) | Low risk | Appears to report all outcomes |
| Other bias | Low risk | None evident |
Ngan Kee 2004a.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 50 women Inclusion criteria: term singleton pregnancies scheduled for elective caesarean under spinal anaesthesia Exclusion criteria: pre‐existing or pregnancy‐induced hypertension, cardiovascular or cerebrovascular disease, known fetal abnormality or contraindication to spinal anaesthesia Setting: Hong Kong, China |
|
| Interventions |
Phenylephrine versus control Group 1: phenylephrine IV immediately after intrathecal injection; 100 µg/min for 3 min Group 2: control (saline infusion plus rescue IV bolus of phenylephrine (100 µg) when SAP < 80% baseline Note: women in the phenylephrine group were given phenylephrine 100 µg/min whenever SAP was less than baseline. All women received a standardised spinal anaesthetic technique and dose. |
|
| Outcomes |
Maternal: hypotension; BP; nausea and vomiting; bradycardia requiring intervention; phenylephrine dose; incision to birth time Neonatal: umbilical arterial blood gases; umbilical venous blood gases; Apgar scores |
|
| Notes | Hypotension defined as SAP < 80% baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Computer‐generated randomization codes" |
| Allocation concealment (selection bias) | Low risk | "Codes contained in sealed, sequentially numbered envelopes" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "Double blind"; "two identical syringes"; investigators and women were blinded to the contents of the syringes |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses to follow‐up: none (although there was insufficient cord blood to measure pH in 1 neonate) |
| Selective reporting (reporting bias) | Low risk | Appears to report all |
| Other bias | Low risk | None evident |
Ngan Kee 2013a.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 104 participants Inclusion criteria: ASA I‐II, age > 18 years, term singleton pregnancy, elective caesarean under spinal anaesthesia Exclusion criteria: pre‐existing or gestational hypertension, abnormality of fetus, onset of uterine contraction, coagulopathy, thrombocytopenia, cerebrovascular or cardiovascular disease, any contraindication to the use of spinal anaesthesia, height > 180 cm or < 140 cm, weight > 100 kg or < 50 kg Setting: Hong Kong, China |
|
| Interventions |
Prophylactic glycopyrrolate versus control Group 1: single IV bolus of glycopyrrolate 4μg/kg diluted in saline to 2 mL administered at commencement of spinal injection Group 2: single IV bolus 2 mL saline placebo administered at commencement of spinal injection All women received standardised aspiration prophylaxis, standardised monitoring, standardised positioning, standardised cannulation, a standardised spinal anaesthetic technique and dose, and standardised crystalloid coload. BP maintained using infusion of phenylephrine 100 μg/mL using a computer controlled closed‐loop feedback infusion. |
|
| Outcomes |
Maternal: total dose and median rate of phenylephrine infusion, total amount of IV fluid given, number of episodes of hypotension, nausea and vomiting Neonatal: Apgar scores, umbilical cord gases |
|
| Notes | Hypotension was defined as SBP < 80% of baseline. Hypertension was defined as SBP > 120% of baseline. Bradycardia was defined as heart rate < 50 bpm. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random codes |
| Allocation concealment (selection bias) | Low risk | Sealed opaque sequentially numbered envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Yes, both blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Group 1 – 5 excluded due to severe shivering, infusion tubing fault, computer cable fault Group 2 – 6 excluded due to severe shivering, infusion tubing fault |
| Selective reporting (reporting bias) | Low risk | Appears all reported |
| Other bias | Low risk | None evident |
Nishikawa 2007.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 54 women Inclusion criteria: ASA I‐II status women, between 20 to 40 years, undergoing elective caesarean Exclusion criteria: women with BMI > 30 kg/m², anaemia (Hb < 10 g/dL), history of neurological or psychiatric diseases Setting: Japan |
|
| Interventions |
Colloid preload versus colloid coload versus crystalloid alone Group 1: colloid preload: after Ringer's lactate was started at a rate of 5 mL/kg, this was changed to HES 6% (molecular weight 70 kDa, degree of substitution 0.5) and infusion rate was increased to 15 mL/kg for 10 min before spinal anaesthesia. Infusion rate was returned to Ringer's lactate at 5 mL/kg Group 2: colloid coload: after Ringer's lactate was started at a rate of 5 mL/kg, this was changed to HES 6% (molecular weight 70 kDa, degree of substitution 0.5) and infusion rate was increased to 15 mL/kg for 10 min after spinal anaesthesia. Infusion rate was returned to Ringer's lactate at 5 mL/kg Group 3: crystalloid alone: Ringer's lactate at 5 mL/kg All women received standardised leg wrapping, no sedative premedication, and a standardised spinal anaesthetic technique and dose. Hypotension requiring intervention was managed with IV bolus of 4 mg of ephedrine to maintain BP at 80% of baseline. Bradycardia was managed with IV atropine 0.5 mg. |
|
| Outcomes |
Maternal: hypotension; need for ephedrine; BP; bradycardia Neonatal: pH, BE, Apgar scores |
|
| Notes | Hypotension was defined as a decrease in SBP < 80% baseline Bradycardia was defined as heart rate < 50 bpm |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random number tables |
| Allocation concealment (selection bias) | Unclear risk | No method of allocation concealment reported |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "Double‐blind"; "both the patient and the researcher who recorded the data were blinded as to the type of colloid loading" |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up |
| Selective reporting (reporting bias) | Low risk | Most expected outcomes were reported (except for nausea/vomiting) |
| Other bias | Unclear risk | Similar baseline characteristics except that women in the HES coload group had lower mean BMI |
Nivatpumin 2016.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 168 women Inclusion criteria: age > 18 years, ASA I‐II, term singleton pregnancy, elective caesarean delivery under spinal anaesthesia Exclusion criteria: diabetes mellitus other than gestational diabetes, hypertension, BMI > 40 kg/m², complicated pregnancy, allergy to study drugs, long QT syndrome, contraindications to spinal anaesthesia Setting: Thailand |
|
| Interventions |
Ondansetron versus ephedrine versus control Group 1: ephedrine 10 mg IV Group 2: ondansetron 8 mg IV Group 3: normal saline IV Above interventions were diluted in 10 mL 0.9% saline and administered immediately after spinal anaesthesia. All women received the same aspiration prophylaxis, monitoring, crystalloid preload, anaesthetic technique and dose. If hypotension developed, women received ephedrine 5‐10 mg or noradrenalin 4‐8 μg IV (choice of agent was up to the attending anaesthetist). Bradycardia was treated with IV atropine 0.6 mg. |
|
| Outcomes |
Maternal: hypotension, nausea and vomiting, incidence of vasopressor and dose of vasopressor used Neonatal: Apgar scores |
|
| Notes | Hypotension defined as decrease in SBP > 20% of baseline or SBP < 90 mmHg. Bradycardia defined as heart rate < 50 bpm. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation table |
| Allocation concealment (selection bias) | Low risk | Sealed envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Only 2 women were excluded due to protocol violations |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Oh 2014.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 60 women Inclusion criteria: ASA I, elective CS under spinal anaesthesia Exclusion criteria: gestational age < 37 weeks, multiple gestation, fetal distress, pre‐eclampsia, cardiovascular disease, diabetes Setting: South Korea |
|
| Interventions |
Comparison of crystalloid preload versus coload Group 1: rapid infusion of 15 mL/kg Hartmann's preloading Group 2: rapid infusion of 15 mL/kg Hartmann's just after intrathecal injection All women had same monitoring, IV access, spinal anaesthetic technique and dose. Hypotension treated with 5 mg IV ephedrine. |
|
| Outcomes |
Maternal: incidence of hypotension, nausea and vomiting Neonatal: Apgar scores at 1 min and 5 min, umbilical cord gases |
|
| Notes | Hypotension defined as a decrease of SBP > 20% from baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random allocation (block randomisation, block size 4) |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Not blinded, but unlikely to have affected incidence of hypotension |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Not blinded, but unlikely to have affected incidence of hypotension |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Group 1: 1 woman excluded due to surgical delay by other operation Group 2: 1 woman excluded due to inadequate spinal anaesthesia |
| Selective reporting (reporting bias) | Low risk | Not apparent |
| Other bias | Low risk | Not apparent |
Olsen 1994.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 28 women Inclusion criteria: healthy parturients at term scheduled for elective CS due to disproportion or breech presentation |
|
| Interventions |
Prophylactic ephedrine + crystalloid preload versus crystalloid preload alone Group 1: 750 mL isotonic saline plus 20 mL/kg preload Group 2: 750 mL isotonic saline plus 500 mL preload followed by ephedrine bolus (0.15 mg/kg) and ephedrine infusion (0.4 mg/kg/h); ephedrine commenced after spinal anaesthetic All women received standardised positioning, and a standardised spinal anaesthetic technique and dose followed by standardised surgical positioning. |
|
| Outcomes |
Maternal: hypotension; BP; level of block; induction to incision/incision to birth times; ephedrine dose Neonatal: umbilical pH; Apgar scores |
|
| Notes | Hypotension was defined as > 10 mmHg decrease in MAP (reported only as dose of ephedrine) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding not mentioned |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Apgar scores were blinded – no further details |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: 2/28 women were excluded due to technical difficulties with the ephedrine infusion pump and the Dinamap respectively |
| Selective reporting (reporting bias) | Unclear risk | Unclear reporting |
| Other bias | Unclear risk | unclear reporting |
Ortiz‐Gomez 2014.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 128 women Inclusion criteria: ASA I, elective caesarean under spinal anaesthesia Exclusion criteria: patient refusal to participate, contraindication to spinal anaesthesia, age < 20 or > 45 years, BMI > 30 kg/m², history of allergy or side effects to ondansetron Setting: Spain |
|
| Interventions |
Comparison of different doses of prophylactic ondansetron with placebo Group 1: placebo 0.9% saline 10 mL Group 2: 2 mg ondansetron with 0.9% saline to total volume of 10 mL Group 3: 4 mg ondansetron with 0.9% saline to total volume of 10 mL Group 4: 8 mg ondansetron with 0.9% saline to total volume of 10 mL The above 10 mL preparation was injected IV over 60 s, 5 min before the spinal anaesthesia was performed All women received the same IV cannulation, monitoring, spinal anaesthetic technique with dose adjusted according to height, and 8 mL/kg of colloid coloading Hypotension was treated with IV ephedrine 10 mg, or phenylephrine 50 μg if maternal heart rate > 95 beat/min Bradycardia was treated with IV atropine 0.01 mg/kg |
|
| Outcomes | Maternal: incidence of hypotension, adverse effects, need for atropine or ephedrine or phenylephrine | |
| Notes | Hypotension defined as SBP < 75% of baseline Bradycardia was defined as heart rate < 45 beat/min |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomised by local statistical department |
| Allocation concealment (selection bias) | Low risk | Ondansetron/placebo syringes were prepared by the anaesthetic nurse with no label indicating the group allocation |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Double‐blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | None reported |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Ouerghi 2010.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 62 women Inclusion criteria: ASA physical status 1 and 2, term singleton pregnancy undergoing elective CS under spinal anaesthesia Exclusion criteria: pre‐existing or pregnancy‐induced hypertension, women with cardiac, renal or other end‐organ disease, women in active labour, placenta praevia, contraindications to neuraxial block, emergency delivery Setting: Tunisia |
|
| Interventions |
Crystalloid preload versus control Group 1: rapid preload infusion of 20 mL/kg Ringer's lactate, 15 min before the spinal block Group 2: no preload All women received a standardised spinal anaesthetic technique and dose with standardised surgical positioning. Hypotension (requiring intervention) was treated immediately with rapid fluid infusion and ephedrine 6 mg IV and repeated whenever necessary. |
|
| Outcomes |
Maternal: hypotension; nausea; vomiting; pruritus; dizziness; time to hypotension; heart rate Neonatal: Apgar at 1 min and 5 min |
|
| Notes | Hypotension was defined as 20% or more fall below the pre‐induction level, or systolic pressure < 100 mmHg | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomly assigned"; no further details given |
| Allocation concealment (selection bias) | Unclear risk | "Sealed envelope" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | An independent investigator who recorded all variables was blinded to the anaesthetic technique used (however the paper did not report how this blinding was achieved) |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | As above; plus Apgar score was assessed by a paediatrician who was unaware of group assignment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 2/62 – 1 from each group (both due to inadequate sensory level (< T6)) |
| Selective reporting (reporting bias) | Unclear risk | Some maternal outcomes not reported completely; only 1 neonatal outcome reported |
| Other bias | Unclear risk | Similar baseline characteristics |
Ozkan 2004.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 150 women Inclusion criteria: absence of any systemic illness or fetal pathology, undergoing CS under spinal anaesthesia |
|
| Interventions |
Crystalloid preload versus colloid preload versus crystalloid preload + prophylactic ephedrine versus colloid preload + prophylactic ephedrine Group1: Ringer's lactate IV 1000 mL Group 2: Ringer's lactate IV 1000 mL + ephedrine 15 mg Group 3: Ringer's lactate IV 1000 mL + ephedrine 30 mg Group 4: gelatine 500 mL solution Group 5: gelatine 500 mL + ephedrine 15 mg Group 6: gelatine 500 mL + ephedrine 30 mg Unclear whether standardised spinal anaesthetic technique and dose Hypotension treated with additional Ringer's lactate infusions while hypotensive periods longer than 3 min were treated with 5 mg ephedrine IV |
|
| Outcomes |
Maternal: hypotension; heart rate; nausea; vomiting; vasopressor requirement Neonatal: stated that there were no significant differences in neonatal outcomes, but these outcomes were not described |
|
| Notes | Hypotension defined as < 20% of baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding not stated |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding not stated |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up not stated |
| Selective reporting (reporting bias) | Unclear risk | Not apparent, but not well reported |
| Other bias | High risk | Variable dose of local anaesthetic used for spinal anaesthesia |
Perumal 2004.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 40 women Inclusion criteria: healthy term women awaiting elective caesarean under spinal anaesthesia |
|
| Interventions |
Colloid preload versus crystalloid preload Group 1: HES preload, 1000 mL over 15 min Group 2: Ringer's lactate preload, 1500 mL over 15 min All women received a standardised spinal anaesthetic technique and dose. |
|
| Outcomes | Maternal: hypotension; heart rate; Doppler measures; ephedrine use | |
| Notes | Hypotension was defined as 20% reduction in SBP | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Methods not described |
| Allocation concealment (selection bias) | Unclear risk | Methods not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "Double blind" – no further details |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses to follow‐up: none reported but losses unlikely |
| Selective reporting (reporting bias) | Unclear risk | Not apparent, but not well reported |
| Other bias | Unclear risk | Not apparent, but not well reported |
Pouliou 2006.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 60 women Inclusion criteria: ASA I‐II women aged 18‐45 having elective LSCS under spinal anaesthesia No exclusion criteria mentioned in abstract Setting: Greece |
|
| Interventions |
Pre‐spinal anaesthesia IM ephedrine versus delayed IV ephedrine Group 1: ephedrine IM 37.5 mg 15 min before spinal Group 2: ephedrine 15 mg IV 2 min after spinal anaesthesia All women received a standardised crystalloid preload followed by a standardised spinal anaesthetic technique and dose |
|
| Outcomes | Maternal: incidence/severity of hypotension | |
| Notes | Hypotension classified as "mild" (decrease of 20% from baseline) or "severe" (decrease of < 30% from baseline) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Double‐randomised" but no details as to how |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Unable to be blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Unclear risk | Unclear reporting |
| Other bias | Unclear risk | Unclear reporting |
Pouta 1996.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 22 women Inclusion criteria: healthy women undergoing elective CS at term, indications being breech presentation, contracted pelvis or previous CS Exclusion criteria: multiple gestation, fetal and maternal complications and contraindications to spinal anaesthesia, active labour |
|
| Interventions |
Colloid preload versus crystalloid preload Group 1: 500 mL 6% HES prior to spinal anaesthesia Group 2: 1000 mL Ringer's lactate prior to spinal anaesthesia All women received standardised aspiration prophylaxis, standardised crystalloid coload, standardised spinal anaesthetic and dose, and standardised surgical positioning. |
|
| Outcomes |
Maternal: hypotension; data expressed as mean (SD) rather than discrete incidence of hypotension; heart rate; CVP; haematocrit; ANP; endothelin‐1 (ET‐1) assays (central and peripheral); blood loss Neonatal: birthweight; umbilical arterial ANP; ET‐1 assays; pH (expressed as mean (SEM)) |
|
| Notes | Hypotension defined as SBP < 90 mmHg or less than 80% of baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Methods not described |
| Allocation concealment (selection bias) | Unclear risk | Methods not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding not mentioned |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding not mentioned |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up not stated |
| Selective reporting (reporting bias) | Unclear risk | Unclear reporting |
| Other bias | Unclear risk | Unclear reporting |
Ramin 1994.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 32 women Inclusion criteria: healthy pregnant women undergoing elective caesarean at term (38 to 40 weeks' gestation) with spinal anaesthesia Exclusion criteria: women in labour, hypertension, diabetes, platelet counts < 100,000 mm3, prolonged thromboplastin time, fetal distress, cardiac or pulmonary disease, any medical illness, or a known history of drug abuse |
|
| Interventions |
Prophylactic angiotensin versus prophylactic ephedrine versus control Group 1: angiotensin II (1000 ng/mL in 0.9% sodium chloride) Group 2: ephedrine (1 mg/mL) Group 3: control (no prophylactic intervention) All women received a standardised crystalloid preload and a standardised spinal anaesthetic technique with slight variation in spinal anaesthetic doses. |
|
| Outcomes |
Maternal: hypotension (defined as decrease of > 30% from baseline); arterial BP (mean and SD);
angiotensin levels Neonatal: Apgar scores at 1 min and 5 min (mean and SD); pH < 7.2; umbilical artery pH (mean and SD); umbilical venous pH (mean and SD); pCO2; BE |
|
| Notes | Hypotension was defined as a decrease in BP of > 30% from baseline. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomised" but method otherwise not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding not stated |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding not stated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses to follow‐up: 2/32 – 1 woman in the control group with a fetal death; 1 woman (group not specified) gave birth before her scheduled procedure |
| Selective reporting (reporting bias) | Unclear risk | Unclear reporting |
| Other bias | Unclear risk | Unclear reporting |
Rees 2002.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 60 women Inclusion criteria: healthy women undergoing elective caesarean Exclusion criteria: women with symptoms or signs of labour, prematurity (< 37 weeks' gestation), multiple pregnancy, hypertension, pre‐eclampsia, obesity, intrauterine growth retardation, fetal distress or any other factor contraindicating a standard spinal anaesthetic technique Setting: UK |
|
| Interventions |
Left lateral versus left lateral tilt Group 1: full left lateral after spinal Group 2: 15 degree left lateral table tilt from supine after spinal Women remained in the study position for 15 min after spinal anaesthesia; women in the left lateral group were then turned into the 15 degree tilt position. All women received a standardised crystalloid preload, a standardised spinal anaesthetic technique and dose, and 6 mg ephedrine IV immediately after insertion of spinal anaesthetic. |
|
| Outcomes |
Maternal: hypotension; block height; ephedrine dose; nausea; vomiting; bradycardia; maximum percentage decrease in arm SAP; maximum percentage decrease in leg SAP; fetal heart traces Neonatal: Apgar scores (presented as means and ranges); venous cord gases (presented as means only); arterial cord gases (presented as means only) |
|
| Notes | Hypotension was defined as SAP of either less than 100 mmHg or less than 80% of baseline. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Stratified by cephalic or breech presentation (separate random‐number lists) |
| Allocation concealment (selection bias) | Unclear risk | Sealed envelopes prepared in advance by a third party |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding not stated |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding not stated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses to follow‐up: 2/60 – 1 from each group: in 1 woman, the anaesthetist was unable to site the spinal in the lateral position and the spinal was subsequently successfully inserted in the sitting position; another withdrawal (from the lateral group) was due to inadequate spread of spinal blockade |
| Selective reporting (reporting bias) | Unclear risk | Unclear reporting |
| Other bias | Unclear risk | Unclear reporting |
Riley 1995.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 40 women Inclusion criteria: non‐labouring ASA I and II women having non‐urgent CS Exclusion criteria: obesity (weight over 115 kg), height less than 152 cm, diabetes, pregnancy‐induced hypertension, chronic hypertension, heart disease, multiple gestation and age less than 18 or more than 40 years |
|
| Interventions |
Colloid + crystalloid preload versus crystalloid preload Group 1: 500 mL 6% hetastarch administered prior to induction of spinal anaesthesia Group 2: 1000 mL Ringer's lactate administered prior to induction of spinal anaesthesia All women received a standardised crystalloid infusion after the study drug, a standardised spinal anaesthetic technique and dose, and ephedrine 10 mg IV. |
|
| Outcomes |
Maternal: hypotension; heart rate; block height; ephedrine dose; nausea and/or vomiting; additional IV fluid prior to birth. Neonatal: Apgar scores < 7; umbilical arterial and venous blood gas (expressed as mean and SD); pH (expressed as mean and SD). |
|
| Notes | Hypotension was defined as SBP less than 100 mmHg and less than 80% of baseline. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Women and providers blinded – no further details |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up not stated |
| Selective reporting (reporting bias) | Unclear risk | Unclear reporting |
| Other bias | Unclear risk | Unclear reporting |
Romdhani 2014.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 105 patients undergoing elective caesarean section Inclusion criteria: term singleton pregnancies, not in labour, elective caesarean, appropriate for spinal anaesthesia Exclusion criteria: pre‐eclampsia, weight > 110 kg, < 150 cm tall, allergy to HES, known fetal abnormalities, contraindication for spinal anaesthesia, sensitive block height that exceeded T4, haemodynamic instability caused by a surgical complication, failed spinal anaesthesia Setting: Tunisia |
|
| Interventions |
HES vs crystalloid preload Group 1: 500 mL of 6% HES 130/0.4 Group 2: 1500 mL of 9% normal saline solution Both groups received bolus 30 min prior to spinal anaesthesia Both groups received rescue ephedrine |
|
| Outcomes |
Maternal: hypotension; heart rate; dose of ephedrine; nausea and vomiting Neonatal: umbilical blood pH; Apgar at 1 min and 5 min |
|
| Notes | Hypotension defined as a 20% drop in systolic blood pressure from baseline. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not blinded |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Low risk | Most expected outcomes reported |
| Other bias | Low risk | Not apparent |
Rout 1992.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 20 women Inclusion criteria: healthy parturients undergoing elective CS, term, singleton pregnancies, cephalic presentation, not more than 90 kg Exclusion criteria: medical or obstetric complications or evidence of placental dysfunction |
|
| Interventions |
Crystalloid preload: comparison of different rates of infusion Group 1: plasmalyte‐L 20 mL/kg infused over 20 min prior to spinal anaesthesia Group 2: plasmalyte‐L 20 mL/kg infused over 10 min prior to spinal anaesthesia All women received a standardised spinal anaesthetic technique and dose. |
|
| Outcomes |
Maternal: hypotension; heart rate; CVP; spinal to birth time; uterine incision to birth time; block height at 5 min; ephedrine dose Neonatal: Apgar scores (minus colour) at 2 and 5 min; umbilical arterial and venous blood gas and pH (data incomplete) |
|
| Notes | Hypotension was defined as SBP less than 100 mmHg and less than 80% of baseline. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding not mentioned |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding not mentioned |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up not stated |
| Selective reporting (reporting bias) | Unclear risk | Unclear reporting |
| Other bias | Unclear risk | Unclear reporting |
Rout 1993a.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 100 women Inclusion criteria: ASA I parturients undergoing elective repeat CS with uncomplicated singleton pregnancy and weight less than 90 kg at term Exclusion criteria: not specified |
|
| Interventions |
Lower leg compression versus leg elevation versus control Group 1: legs horizontal but wrapped from toe to mid‐thigh with rubber Esmarch bandages with preservation of pedal pulses Group 2: legs elevated on 4 pillows at 30 degrees to horizontal Group 3: control – neither wrapped nor raised All women received a standardised crystalloid preload and a standardised spinal anaesthetic technique and dose. |
|
| Outcomes |
Maternal: hypotension; diastolic BP; heart rate; onset of hypotension; ephedrine dose; spinal to birth time; uterine incision to birth time Neonatal: umbilical arterial and venous blood gas; pH < 7.25; Apgar scores minus colour at 2 min and 5 min |
|
| Notes | Hypotension defined as defined as SBP less than 100 mmHg and less than 80% baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding not mentioned |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding not mentioned |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: 3/100 – 2 women had an inadequate block and 1 woman had a high block (groups not specified) |
| Selective reporting (reporting bias) | Unclear risk | Not apparent |
| Other bias | Unclear risk | Not apparent |
Sahoo 2012.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 56 women Inclusion criteria: ASA I, age 20‐40, elective LSCS Exclusion criteria: contraindications to SAB, patient refusal, unstable haemodynamics, coagulopathy, history of hypersensitivity to ondansetron or local anaesthetic agents, hypertensive disorders of pregnancy, cardiovascular insufficiency, receiving selective serotonin reuptake inhibitors or migraine medications Setting: India |
|
| Interventions |
Pretreatment with ondansetron versus placebo Group 1: IV ondansetron 4 mg diluted in 10 mL of normal saline given over 1 min, 5 min before spinal anaesthesia Group 2: 10 mL of normal saline IV given over 1 min, 5 min before spinal anaesthesia |
|
| Outcomes |
Maternal: hypotension, decrease in BP, decrease in heart rate, nausea and vomiting Neonatal: none |
|
| Notes | Hypotension: SBP < 90 mmHg or DBP < 60 mmHg Bradycardia: heart rate < 50 bpm |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation chart |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Blinded anaesthetist assessing outcomes |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Not apparent |
| Selective reporting (reporting bias) | Low risk | Not apparent |
| Other bias | Low risk | Not apparent |
Selvan 2004.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 60 women Inclusion criteria: healthy women awaiting elective caesarean under spinal anaesthesia |
|
| Interventions |
Colloid vs crystalloid preload Group 1: HES 6% w/v 500 mL Group 2: HES 6% w/v 1000 mL Group 3: Hartmann's solution 1500 mL All women were placed in the left lateral position and fluid was then preloaded over 15 min. All women received a standardised anaesthetic technique and dose. |
|
| Outcomes |
Maternal: hypotension; heart rate; BP; ephedrine use Neonatal: cord gases |
|
| Notes | Hypotension defined as 20% reduction in SBP | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "Double blind" – no further details |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | "Double blind" – no further details |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up not stated |
| Selective reporting (reporting bias) | Unclear risk | Not apparent, but not well reported |
| Other bias | Unclear risk | Not apparent, but not well reported |
Siddik 2000.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 40 women Inclusion criteria: non‐labouring ASA class I and II women scheduled for elective caesarean Exclusion criteria: obesity (> 115 kg), height > 152 cm, diabetes, pregnancy‐induced hypertension, chronic hypertension, heart disease, multiple gestation, breech presentation, age < 18 or > 40 and SBP < 100 mmHg Setting: Lebanon |
|
| Interventions |
Colloid v crystalloid preload Group 1: HES 10%, 500 mL Group 2: Ringer's lactate 1000 mL Preload was administered 10 min before spinal anaesthesia; women were placed in left supine wedged position. All women received a standardised spinal anaesthetic technique and dose. |
|
| Outcomes |
Maternal: hypotension; block height; ephedrine dose; heart rate; BP; nausea; vomiting Neonatal: Apgar scores; venous and arterial blood gases |
|
| Notes | Hypotension was defined as SBP < 80% baseline or < 100 mmHg | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomisation method not described |
| Allocation concealment (selection bias) | Unclear risk | "Drawing shuffled sealed envelopes" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding: nurses placed a brown paper bag over the IV solution to conceal its identity from the anaesthetist |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up not stated |
| Selective reporting (reporting bias) | Unclear risk | Not apparent |
| Other bias | Unclear risk | Not apparent |
Siddik‐Sayyid 2009.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 183 women Inclusion criteria: non‐labouring women, > 37 weeks' gestation, ASA I or II scheduled for elective caesarean Exclusion criteria: pregnancy‐induced hypertension, chronic hypertension, multiple gestation, known fetal compromise, diabetes mellitus, polyhydramnios, weight > 100 kg, major systematic disease, anaemia (haemoglobin concentration < 10 g/dL), or clotting diathesis Setting: Lebanon |
|
| Interventions |
Colloid preload versus colloid coload Group 1: colloid preload: preload of 500 mL HES (6% HES 130/0.4), administered by gravity at a wide open rate over 15‐20 min before spinal anaesthesia Group 2: colloid coload: coload of 500 mL of HES (6% HES 130/0.4) administered using a pressure infusion system at the maximum possible rate, commenced at the time of identification of CSF All women received a standardised spinal anaesthetic technique and dose, a standardised crystalloid infusion after spinal anaesthetic, and a standardised oxytocin regimen after delivery. Hypotension requiring intervention was managed with 6 mg IV bolus of ephedrine if heart rate < 90 bpm or 0.1 mg phenylephrine IV bolus if heart rate > 90 bpm. |
|
| Outcomes |
Maternal: hypotension; minimum SBP; maximum heart rate; time to hypotension; ephedrine dose; phenylephrine dose; nausea and/or vomiting; metoclopramide administration; total Ringer's lactate; duration of infusion; duration of surgery; sensory block level; duration of anaesthesia Neonatal: birthweight; Apgar score; umbilical vein pH, pO2, pCO2, BE; umbilical artery pH, pO2, pCO2, BE |
|
| Notes | Hypotension was defined as the administration of at least 1 dose of vasopressor. Severe hypotension was defined as SBP < 80 mmHg. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated table of random numbers |
| Allocation concealment (selection bias) | Unclear risk | "Randomised" – no further details provided |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Woman, anaesthetist performing the spinal block, collecting the data and treating adverse effects, and the paediatrician assessing neonatal outcomes were all unaware of group allocation. The infusion bag was prepared and hidden behind a drape and administered by a nurse who was not involved in anaesthetic management (and who decided when the woman should sit up for spinal anaesthesia). To maintain blinding, this occurred after completion of colloid administration in the preload group (lasting ~15‐20 min) or 15‐20 min from starting the Ringer's lactate in the coload group. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | See above |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 5/183 women were excluded after randomisation due to protocol violations (2 from the preload group and 3 from the coload group) |
| Selective reporting (reporting bias) | Unclear risk | Most expected outcomes reported but some (all neonatal outcomes) not reported in a form that could be used in this review (e.g. medians, and average for Apgar scores) |
| Other bias | Low risk | No apparent risk of other sources of bias |
Singh 2009.
| Study characteristics | ||
| Methods | Randomised, quasi‐experimental observational cohort study | |
| Participants | 60 patients
Inclusion criteria: ASA I, elective LSCS Exclusion criteria: pregnancy‐induced high BP, high‐risk pregnancy, fetal distress, moderate to severe anaemia, patient refusal, infection at site of injection, bleeding diathesis, severe hypovolaemia, elevated intracranial pressure, spine deformity and patients with major systemic illness Setting: India |
|
| Interventions |
Crystalloid versus colloid preload Group 1: 20 mL/kg Ringer's lactate preloading over 20 min just prior to SAB Group 2: 10 mL/kg HES 130/0.4 (up to a max 500 mL) preloading over 20 min just prior to SAB All women received standardised premedication, positioning, monitoring, IV cannulation/urinary catheter, SAB and technique, oxygen delivery, intra‐operative fluids, oxytocin. Hypotension treated with IV bolus of crystalloid up to 200 mL, further hypotension treated with mephentermine 3 mg IV bolus every 1 min until SBP> 90 mmHg achieved. Bradycardia treated with atropine 300 μg aliquots. |
|
| Outcomes |
Maternal: haemodynamics/observations, urine output, duration of surgery, uterine incision‐delivery time, SAB complications, "undesirable effects" from HES including "anaphylactoid" reactions, pruritis, bleeding Neonatal: Apgar scores at 1 min and 5 min |
|
| Notes | Hypotension was defined as a fall in SAP > 30% of baseline or SAP < 90 mmHg | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Unclear risk | Not reported |
| Other bias | Unclear risk | Not reported |
Singh 2014.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 60 women Inclusion criteria: singleton uncomplicated pregnancy, ASA I‐II, elective caesarean under spinal anaesthesia Setting: unknown |
|
| Interventions |
Leg wrapping versus no leg wrapping Group 1: no leg wrapping Group 2: leg wrapping with crepe bandage (15 cm width, 4 m stretched length) from ankle to mid‐thigh level over both legs. During wrapping, lower extremities were lifted at a 45 degree angle Crepe bandages were wrapped tightly enough that the woman felt the tightness, yet it was comfortable and not painful. All patients had their legs wrapped by the same person in 3 min to eliminate bias introduced by method or altered force of wrapping. Legs were hidden to ensure blinding. All women received the same aspiration prophylaxis, monitoring, 20 mL/kg IV Ringer's lactate fluid preloading over 15‐20 min prior to spinal anaesthesia, spinal anaesthetic technique and dose. Hypotension was treated with 50 μg IV phenylephrine bolus and an increase in rate of IV fluid infusion. |
|
| Outcomes | Maternal: incidence of hypotension | |
| Notes | Hypotension was defined as a fall in SBP to < 90 mHg. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Generation of random sequence not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Personnel blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Personnel blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | None reported |
| Selective reporting (reporting bias) | Low risk | Not apparent |
| Other bias | Low risk | Not apparent |
Singh 2016.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 50 women Inclusion criteria: primiparous, full‐term parturients, aged 18‐40 years, ASA I, scheduled for elective CS Exclusion criteria: refusal of regional anaesthesia, contraindications to spinal anaesthesia, fetal abnormalities, known allergy to any of the drugs used in the study, pregnancy‐induced hypertension or parturients with SBP > 140 mmHg, history of diabetes mellitus, cardiovascular or cerebrovascular and any chronic diseases Setting: India |
|
| Interventions | Ephedrine versus control Group 1: 1 mL 5 mg ephedrine IV immediately after SAB Group 2: 1 mL 0.9% NaCl IV immediately after SAB All women received standardised monitoring, standardised crystalloid IV fluid, standardised spinal anaesthetic technique and dose. Treatment of hypotension involved rapid infusion of Ringer's lactate and 5 mg IV ephedrine. Bradycardia treated with 0.6 mg IV atropine sulfate. |
|
| Outcomes |
Maternal: incidence of hypotension, reactive hypertension, number of patients requiring rescue ephedrine, total dose of rescue ephedrine (mg), bradycardia, nausea/vomiting, average time to delivery Neonatal: Apgar scores at 1 min and 5 min |
|
| Notes | Hypotension was defined as a decrease in SBP of > 20% Bradycardia was defined as heart rate < 60 bpm Reactive hypertension: SBP > 140 mmHg |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blinded. Study solution prepared by person not involved in the study |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Study staff recorded outcomes |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All patients completed protocol |
| Selective reporting (reporting bias) | Low risk | Not evident |
| Other bias | Unclear risk | None evident |
Sood 1996.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 50 women Inclusion criteria: ASA I or II parturients undergoing elective CS at term Exclusion criteria: history of cardiovascular disease or contraindication to spinal, body weight > 90 kg and/or thigh circumference > 62 cm |
|
| Interventions |
Lower limb compression versus control Group 1: TED stockings applied 1 hour preoperatively from toes to mid‐thigh according to manufacturer's guidelines Group 2: no compression All women received standardised crystalloid preload, standardised spinal anaesthetic technique with dose adjusted according to subject's height. |
|
| Outcomes |
Maternal: hypotension; diastolic BP and MAP; heart rate; SpO2 Neonatal: Apgar scores at 1 min and 5 min |
|
| Notes | Hypotension was defined as a SBP < 90 mmHg or a decrease in SBP more than 20% from baseline. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding not mentioned |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding not mentioned |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up not stated |
| Selective reporting (reporting bias) | Unclear risk | Not apparent |
| Other bias | Unclear risk | Not apparent |
Stein 1997.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 75 women Inclusion criteria: healthy women (55 of whom had experienced at least 1 previous birth) undergoing elective CS during spinal anaesthesia Exclusion criteria: history of nausea and vomiting associated with previous surgery or anaesthesia; nausea or vomiting within 24 h prior to caesarean, history of diabetes mellitus, or morbid obesity |
|
| Interventions |
Acupressure versus metoclopramide versus placebo Group 1: acupressure bands + 2 mL IV saline Group 2: placebo wrist bands + 10 mg metoclopramide Group 3: placebo wrist bands + 2 mL IV saline Acupressure defined as pressure on the Neiguan (P6) acupuncture points of the wrist. All women received a standardised preload of 1500‐2000 mL Ringer's lactate in addition to a standardised spinal anaesthetic technique and dose. |
|
| Outcomes |
Maternal: hypotension; nausea (score > 2); vomiting; anxiety Neonatal: Apgar score < 7 at 5 min |
|
| Notes | Hypotension was defined as a decrease in SBP more than 20% from baseline or < 100 mmHg. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | "Envelope system" – no further details |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding: wrist bands were placed bilaterally by an anaesthetist not directly involved in the women's care. The acupressure bands were lightly covered with gauze and tapes so they could not be distinguished from the placebo bands. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: not stated |
| Selective reporting (reporting bias) | Low risk | Not apparent |
| Other bias | Low risk | Not apparent |
Sujata 2012.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 100 women Inclusion criteria: ASA I‐II, elective CS under SAB Exclusion criteria: contraindication to SAB, peripartum bleeding > 1 L, multiple gestation, polyhydramnios, gestation < 37 weeks, any patient considered at high risk of DVT Setting: India |
|
| Interventions |
Mechanical lower limb compression versus control Group 1: mechanical pump with thigh‐level cuff applied to lower limbs in all subjects and switched on Group 2: mechanical pump with thigh‐level cuff applied to lower limbs in all subjects but not switched on All women received standardised aspiration prophylaxis, standardised monitoring, standardised spinal anaesthetic technique and dose, standardised crystalloid coloading and maintenance, standardised positioning and standardised oxytocic administration. Hypotension was treated with IV ephedrine 6 mg, repeated every 3 min as needed. |
|
| Outcomes |
Maternal: BP, heart rate, SpO2 recorded every 3 min for 1 h. Total volume of IV fluid given, total ephedrine dose Neonatal: Apgar scores |
|
| Notes | Hypotension defined as a decrease in SBP > 20% baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Sealed envelope |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Anaethetist caring for women during caesarean blinded. Possible that blinding may have been broken |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Group 1 – 3 women excluded due to pregnancy‐induced hypertension Group 2 – 5 women excluded due to pregnancy‐induced hypertension |
| Selective reporting (reporting bias) | Low risk | Not apparent |
| Other bias | Low risk | Not apparent |
Sutherland 2001.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 100 women Inclusion criteria: ASA I or II women undergoing elective CS Exclusion criteria: contraindication to spinal anaesthesia or thigh circumference > 64 cm |
|
| Interventions |
Lower limb compression versus control Group 1: TED stockings applied before arrival in theatre and lower limb sequential compression device inflated immediately after spinal injection Group 2: no mechanical prophylaxis All women received a standardised spinal anaesthetic technique with dose adjusted according to subject's height. Hypotension was managed with a standardised ephedrine regimen. |
|
| Outcomes |
Maternal: hypotension; systolic, diastolic and mean BP; level of sensory block; ephedrine requirement; time to first episode of hypotension Neonatal: Apgar scores at 1 min and 5 min (expressed as n with score < 9); umbilical artery pH (expressed as mean (SD)) |
|
| Notes | Hypotension defined as SBP < 100 mmHg or fall of > 20% from baseline Lack of blinding acknowledged Protocol violations acknowledged |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Neither participants nor investigators blinded |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Losses to follow‐up: no dropouts but 46/100 protocol violations (ephedrine administered in error on 17 occasions (9 intervention, 8 control), ephedrine omitted in error on 29 occasions (10 intervention, 19 control) |
| Selective reporting (reporting bias) | Unclear risk | Not apparent |
| Other bias | Unclear risk | Not apparent |
Tawfik 2014.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 210 women Inclusion criteria: elective caesarean, ASA I‐II, singleton pregnancy Exclusion criteria: age < 19 or > 40 years, height < 150 or > 185 cm, weight < 60 or > 100 kg, BMI > 40 kg/m², chronic or pregnancy‐induced hypertension, baseline SBP < 100 or > 140 mmHg, diabetes mellitus, cardiovascular, cerebrovascular or renal disease, haemoglobin < 100g/L, patients in labour, any contraindication to spinal anaesthesia, preterm (< 37 weeks gestation), multiple pregnancy, polyhydramnios or known fetal abnormalities Setting: Egypt |
|
| Interventions |
Colloid preload versus crystalloid coload Group 1: colloid preload – 6% HES 130/0.4 in 0.9% sodium chloride 500 mL within 15 min before induction of spinal anaesthesia Group 2: crystalloid coload – 1000 mL of Ringer's acetate using a pressuriser as rapidly as possible starting at time of intrathecal injection All women received IV cannulation, routine monitoring, a standardised crystalloid infusion after administration of study solution, a standardised spinal anaesthetic technique and dose. Hypotension was treated with IV ephedrine 5 mg bolus. Severe hypotension was treated with 10 mg IV ephedrine. Bradycardia was treated with IV atropine 0.5 mg. |
|
| Outcomes |
Maternal: hypotension, bradycardia, nausea and vomiting Neonatal: Apgar scores at 1 min and 5 min and umbilical cord gases |
|
| Notes | Hypotension defined as SBP < 80% baseline or < 90 mmHg Severe hypotension: SBP < 80 mmHg Maternal bradycardia defined as heart rate < 50 bpm |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random numbers |
| Allocation concealment (selection bias) | Low risk | Sequentially numbered opaque sealed envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blinded. Anaesthetists, women, and neonatologists blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Double‐blinded. Outcomes recorded by anaesthetists and neonatologists |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 5 patients excluded due to failed spinal or protocol violation |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Tercanli 2005.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 22 women Inclusion criteria: healthy women with uncomplicated singleton pregnancies at 36‐40 weeks' gestation, not in labour, undergoing elective caesarean under spinal anaesthesia |
|
| Interventions |
Crystalloid: high versus low volume preload Group 1: 15 mL/kg Ringer's lactate Group 2: 150 mL Ringer's lactate All women received a standardised spinal anaesthetic technique and dose. |
|
| Outcomes |
Maternal: hypotension; ephedrine dose Neonatal: pulsatility indices; pH (mean and SD); Apgar score at 1 min, 5 min, and 10 min (mean and SD); NACS |
|
| Notes | Hypotension was defined as decrease in SBP of more than 20% from baseline. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Low risk | Adequate: drawing of sealed consecutive opaque sealed envelopes a day before surgery |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding not stated |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding not stated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses to follow‐up: not stated but losses unlikely |
| Selective reporting (reporting bias) | Low risk | Not apparent |
| Other bias | Low risk | Not apparent |
Terkawi 2015.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 91 women Inclusion criteria: elective CS Exclusion criteria: diabetes, chronic hypertension, gestational hypertension, pre‐eclampsia, cardiac disease, patients with long QT syndrome and known contraindications to spinal anaesthesia Setting: USA |
|
| Interventions |
Ondansetron versus control Group 1: received 8 mg ondansetron diluted in 10 mL in 0.9% NaCl Group 2: received 10 mL of 0.9% NaCl Study drug was administered over a period of 5 min whilst in sitting position, prior to SAB. All women received standardised aspiration prophylaxis, standardised colloid preload, standardised crystalloid maintenance fluid, standardised monitoring, standardised spinal anaesthetic technique and dose, standardised positioning. Hypotension was managed with boluses of 100 μg of phenylephrine administered incrementally until SBP > 90 mmHg. Bradycardia was managed with 0.4 mg atropine or 0.2 mg glycopyrrolate. |
|
| Outcomes |
Maternal: incidence of hypotension, incidence of bradycardia, amount of vasopressor and anticholinergic agents given, pruritus, nausea and vomiting, extent of sensory block, estimated blood loss, total fluid administered Neonatal: Apgar scores |
|
| Notes | Hypotension was defined as SBP < 90 mmHg or 20% drop in SBP from baseline. Bradycardia was defined as heart rate < 60 bpm. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation |
| Allocation concealment (selection bias) | Unclear risk | Not clear |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Drugs prepared by pharmacist |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | All research personnel were blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Group 1: 4 excluded (3 due to protocol violation, 1 due to failed SAB) Group 2: 1 excluded (due to protocol violation) |
| Selective reporting (reporting bias) | Low risk | Not apparent |
| Other bias | Low risk | None evident |
Torres unpub.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 50 women Inclusion criteria: scheduled for elective CS Exclusion criteria: contraindications to spinal anaesthesia, fetal or maternal pathology and known allergy to the drugs being administered |
|
| Interventions |
Ephedrine versus control Group 1: ephedrine IV 8 mg Group 2: placebo (saline) Study drugs were given at the same time as spinal anaesthetic. All women received a preload of 10 mL/kg Ringer's lactate, a prophylactic dose of 8 mg of ephedrine prior to intrathecal injection, a standardised spinal anaesthetic technique and dose, and standardised positioning for surgery. |
|
| Outcomes |
Maternal: hypotension; dose of local anaesthetic; level of block; surgical time; BP; heart rate; nausea; vomiting; total ephedrine dose; postdural puncture headache Neonatal: Apgar score at 1 min and 5 min |
|
| Notes | Hypotension was defined as decrease in SBP of 20% or more. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Double‐blind but details not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Double‐blind but details not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Not apparent |
| Selective reporting (reporting bias) | Low risk | Not apparent |
| Other bias | Low risk | Not apparent |
Trabelsi 2015.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 80 women Inclusion criteria: ASA I, elective caesarean, primipara, term pregnancy Exclusion criteria: emesis gravidarum, contraindication to spinal anaesthesia (patient refusal, unstable haemodynamic, and coagulation abnormalities), chronic hypertension or pre‐eclampsia, morbid obesity, and/or any study drugs allergy Setting: Tunisia |
|
| Interventions |
Prophylactic ondansetron versus control Group 1: 4 mg IV ondansetron in 10 mL saline, 5 min before spinal puncture Group 2: 10 mL saline, 5 min before spinal puncture All women received the same monitoring, standardised crystalloid preload before spinal anaesthesia, spinal anaesthetic technique and dose. Hypotension was treated with 100 mL crystalloid and 6 mg ephedrine IV. Bradycardia was treated with fluids and ephedrine up to 25 mg, If did not resolve within 30 s of treatment, IV atropine 0.5 mg IV given every 30 s until resolution |
|
| Outcomes |
Maternal: incidence of hypotension, nausea and vomiting Neonatal: Apgar scores, umbilical cord gases |
|
| Notes | Hypotension was defined as a decrease from baseline > 20% in systolic pressure. Bradycardia was defined as 30% drop in heart rate or < 45 bpm. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random sequence generated by website: www.random.org |
| Allocation concealment (selection bias) | Low risk | Anaesthetic nurse prepared solution according to group allocation on above website |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Double‐blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No data loss |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Tsen 2000.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 40 women Inclusion criteria: ASA I and II women not in labour undergoing elective caesarean for term uncomplicated singleton pregnancies, taking only prenatal vitamins and weighing less than 100 kg Exclusion criteria: women with cardiac, pulmonary or renal diseases, or systemic diseases that could influence haemodynamic responses, including pre‐eclampsia, hypertension and diabetes; if women were taking or had a history of taking any medications that could influence haemodynamic responses, including magnesium sulphate, terbutaline or beta‐blockers |
|
| Interventions |
Ephedrine versus control Group 1: ephedrine 2 mL IV (10 mg) given simultaneously with spinal anaesthetic Group 2: saline 2 mL IV given simultaneously with spinal anaesthetic All women received a standardised crystalloid preload and a standardised spinal anaesthetic technique and dose, followed by standardised surgical positioning. Hypotension was treated with 10 mg IV doses of ephedrine. |
|
| Outcomes |
Maternal: hypotension; MAP; heart rate; tachycardia (ephedrine group only); hypertension (ephedrine group only); systemic vascular resistance index; stroke index; cardiac index Neonatal: Apgar score < 8 at 5 min |
|
| Notes | Hypotension was defined as 20% decrease in MAP | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Sealed envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding: double‐blind – Apgar scored by a paediatrician blinded to the study – no further details |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up |
| Selective reporting (reporting bias) | Low risk | Not apparent |
| Other bias | Low risk | Not apparent |
Turkoz 2002.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 30 women Inclusion criteria: healthy women at term undergoing elective CS under spinal anaesthesia Exclusion criteria: active labour, rupture of amniotic membranes, chronic or pregnancy‐induced hypertension, insulin‐dependent diabetes mellitus, multiple gestation, oligohydramnios and preoperative diagnosis of small for gestational age fetus |
|
| Interventions |
Ephedrine infusion versus ephedrine bolus Group 1: ephedrine infusion IV 5 mg/min commenced immediately after intrathecal injection Group 2: control – ephedrine bolus 10 mg administered if hypotension developed All women received standardised positioning, standardised crystalloid preload, a standardised spinal anaesthetic technique with the dose adjusted according to subject's height. |
|
| Outcomes | Maternal: hypotension); nausea and vomiting; BP; heart rate; arterial blood Neonatal: umbilical arterial blood; umbilical venous blood; heart rate; BP | |
| Notes | Hypotension defined as 20% decrease from baseline (measured prior to fluid preload) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Sealed envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding not stated |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding not stated |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: not stated |
| Selective reporting (reporting bias) | Unclear risk | Unclear reporting |
| Other bias | Unclear risk | Unclear reporting |
Ueyama 1992.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 100 women (60 non‐labouring women scheduled for elective caesarean and 40 labouring women for emergency caesarean) Exclusion criteria: women with placenta praevia, abruptio placenta; toxaemia |
|
| Interventions |
Ephedrine (various doses) versus control Group1: ephedrine 5 mg Group 2: ephedrine 10 mg Group 3: no ephedrine Ephedrine was administered with the spinal. All women received a standardised preload of 1000 mL Ringer's lactate, a standardised spinal anaesthetic technique and dose. |
|
| Outcomes | Maternal: hypotension; SAP | |
| Notes | Hypotension was defined as SAP lower than 80 mmHg | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Methods not described |
| Allocation concealment (selection bias) | Unclear risk | Methods not describe |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding not stated |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding not stated |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: not stated |
| Selective reporting (reporting bias) | Unclear risk | Unclear reporting |
| Other bias | Unclear risk | Unclear reporting |
Ueyama 1999.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 36 women Inclusion criteria: healthy full‐term parturients scheduled for elective caesarean during spinal anaesthesia Exclusion criteria: abruptio placenta, placenta praevia, multiple gestation, pre‐eclampsia, or women who were receiving ritodrine or other beta‐tocolytics |
|
| Interventions |
Colloid preload versus crystalloid preload Group 1: 500 mL HES 6% Group 2: 1000 mL HES 6% Group 3: 1500 mL Ringer's lactate All solutions were infused over 30 min before injection of spinal anaesthesia. All women received a standardised spinal anaesthetic technique and dose. |
|
| Outcomes | Maternal: hypotension; blood volume; cardiac output | |
| Notes | Hypotension defined as defined as decrease in SBP to less than 100 mmHg and less than 80% of baseline value | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation by random envelope method |
| Allocation concealment (selection bias) | High risk | No allocation concealment. Infusion bottle shape different between study groups |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: not stated |
| Selective reporting (reporting bias) | Unclear risk | Not apparent, but not well reported |
| Other bias | Unclear risk | Not apparent, but not well reported |
Ueyama 2002.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 20 women Inclusion criteria: healthy women scheduled for elective caesarean during spinal anaesthesia |
|
| Interventions |
Prophylactic ephedrine versus prophylactic phenylephrine Group 1: 40 mg ephedrine Group 2: 250 µg phenylephrine All women were given Ringer's lactate at a rate of 100 mL/hour immediately after ephedrine or phenylephrine. All women received a standardised spinal anaesthetic technique and dose followed by standardised surgical positioning. |
|
| Outcomes | Maternal: hypotension; cardiac output | |
| Notes | Hypotension defined as a drop in SBP of > 20% and < 100 torr | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Methods not described |
| Allocation concealment (selection bias) | Unclear risk | Methods not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding: "in a double‐blind fashion" – no further details |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Not reported |
| Selective reporting (reporting bias) | Low risk | Not apparent |
| Other bias | Low risk | Not apparent |
Unlugenc 2015.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 90 women Inclusion criteria: ASA I/II, singleton uncomplicated pregnancy at full term gestation undergoing elective CS under spinal anaesthesia Exclusion criteria: significant co‐existing disease such as pre‐eclampsia and hepato‐renal disease, pregnancy pre‐induced hypertension, being in active labour or requiring emergency CS, any contraindication to regional anaesthesia such as local infection or bleeding disorders Setting: Turkey |
|
| Interventions |
Rapid crystalloid coload versus rapid colloid coload versus slow crystalloid coload Group 1: 1000 mL Ringer's lactate at maximum rate Group 2: 1000 mL 6% HES at maximum rate Group 3: 1000 mL Ringer's lactate at minimum rate All fluids were commenced immediately after induction of spinal anaesthesia. All women received standardised fasting regimen, standardised monitoring, standardised cannulation, standardised crystalloid coload (10 mL/kg/hour) via a separate cannula, standardised spinal anaesthetic technique and dose, standardised positioning, standardised oxygen therapy. Hypotension was treated with IV ephedrine 10 mg. If heart rate was < 50 bpm, 0.5 mg atropine was administered IV. |
|
| Outcomes |
Maternal: incidence of hypotension, total fluid volumes, ephedrine requirements, bradycardia, hypoxaemia, excessive sedation, pruritis, dizziness, nausea and vomiting Neonatal: umbilical artery pH/PaO2/PaCO2/HCO3‐, Apgar scores at 1 min and 5 min |
|
| Notes | Hypotension was defined as SBP < 80% of baseline (prenatal) or < 90 mmHg. Bradycardia was defined as heart rate < 50 bpm. Hypoxaemia was defined as SpO2 < 95%. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation |
| Allocation concealment (selection bias) | Low risk | Fluid in non‐transparent bag |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Assessors blinded to patient group. "Demographic data (age, height, weight, parity and gravity) and duration of surgery were noted by an observer blinded to the treatment group. Systolic and diastolic blood pressures (SBP, DBP), heart rate and peripheral oxygen saturation (SpO2) were recorded by an anaesthetist blinded to the patient group." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up |
| Selective reporting (reporting bias) | Low risk | Not apparent |
| Other bias | Low risk | None identified |
Upadya 2016.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 50 women Inclusion criteria: non‐labouring ASA I/II undergoing elective CS Exclusion criteria: patients aged < 18 years or > 40 years, weighing > 100 kg, height < 152 cm, associated diabetes mellitus, pregnancy‐induced hypertension, chronic hypertension, heart disease, multiple gestation, breech presentation, SBP < 100 mmHg, patients who had received IV fluids prior to surgery Setting: India |
|
| Interventions |
Crystalloid preload versus colloid preload Group 1 crystalloid preload: 1000 mL Ringer's lactate Group 2 colloid preload: 500 mL 6% hetastarch Fluids were administered 30 min prior to surgery. All women received standardised aspiration prophylaxis, standardised cannulation, standardised monitoring, standardised spinal anaesthetic technique and dose, standardised positioning, standardised oxygen therapy. Hypotension was managed with IV boluses of 5 mg of ephedrine, repeated every 2 min as required. |
|
| Outcomes |
Maternal: incidence of hypotension, nausea/vomiting, interval between spinal injection and delivery Neonatal: Apgar scores |
|
| Notes | Hypotension was defined as SBP < 100 mmHg and < 80% baseline BP | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not specified |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not specified |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not specified |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No evidence of losses to follow‐up |
| Selective reporting (reporting bias) | Low risk | Not evident |
| Other bias | Low risk | None apparent |
Ure 1999.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 50 women Inclusion criteria: singleton pregnancy, ASA I or II, presenting for elective caesarean at term Exclusion criteria: height < 152 cm, multiple pregnancy, pregnancy‐induced hypertension, placenta praevia, diabetes mellitus, maternal refusal, clotting disorder, fixed cardiac output disease, pre‐existing neurological disease, local and systemic sepsis, and allergy to local anaesthetics |
|
| Interventions |
Glycopyrrolate versus control Group 1: glycopyrrolate 200 µg Group 2: saline (placebo) All women received the study drug with a standardised crystalloid preload (15 mL/kg). All women received a standardised spinal anaesthetic technique and dose followed by standardised surgical positioning. |
|
| Outcomes |
Maternal: hypotension; nausea; nausea severity score; nausea episodes per woman; vomiting; ephedrine dose; heart rate; duration of operation; time to block; blood loss Neonatal: birthweight; Apgar score |
|
| Notes | Hypotension defined as decrease in SAP 20% or more from baseline or absolute decrease to less than 100 mmHg | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding: "double‐blind"; "both glycopyrrolate and saline were given as 1 mL of clear fluid and therefore the participant and researcher were blinded to the randomization" |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses to follow‐up: 1 woman in the glycopyrrolate group refused subarachnoid anaesthesia after the study drug had been given |
| Selective reporting (reporting bias) | Low risk | Not apparent |
| Other bias | Low risk | Not apparent |
Wang 2014a.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 150 women Inclusion criteria: primiparous, single fetus, elective caesarean, age 18‐35 years, 37‐40 weeks gestation, ASA I‐II, normal prenatal exam, normal liver and renal function, normal fetal screening, no medical history of heart or lung disease Setting: China |
|
| Interventions |
Comparison of different doses of prophylactic ondansetron versus control 5 min prior to spinal anaesthesia, women were given (all diluted to 5 mL with physiological saline): Group 1: 5 mL physiological saline Group 2: 2 mg ondansetron Group 3: 4 mg ondansetron Group 4: 6 mg ondansetron Group 5: 8 mg ondansetron All women received no premedication, routine monitoring, cannulation, a standardised crystalloid coload, and a standardised spinal anaesthetic technique and dose Treatment of hypotension consisted of administration of IV bolus of 100 μg phenylephrine |
|
| Outcomes |
Maternal: hypotension, treatment for hypotension/bradycardia, nausea and vomiting Neonatal: cord gases, Apgar score at 1 min and 5 min |
|
| Notes | Hypotension defined as systolic pressure < 80% of baseline | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated codes |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Ondansetron and saline solutions were prepared by an anaesthetist who was blinded to this study. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | None reported |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Wang 2014b.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 66 women Inclusion criteria: primiparous, singleton pregnancy, elective caesarean, age 18‐35, 37‐42 weeks' gestation, ASA I‐II, normal prenatal examinations, normal renal and liver function, no medical history of heart or lung disease, no fetal abnormalities Exclusion criteria: hypertension, cardiovascular or cerebrovascular disease, placenta praevia, abnormal fetal development, contraindications to spinal anaesthesia, endocrine disorders, recent administration of 5‐HT reuptake inhibitors or drugs for treatment of migraines Setting: China |
|
| Interventions |
Prophylactic ondansetron versus control 5 min prior to spinal anaesthesia: Group 1: 4 mg IV ondansetron (diluted to 5 mL with physiological saline) Group 2: 5 mL IV physiological saline All women received the same standardised monitoring, cannulation, spinal anaesthetic technique and dose, standardised crystalloid coload and postdelivery oxytocin If hypotension occurred, 100 μg IV phenylephrine was administered, and repeated every 2 min as required until SBP > 80% baseline If bradycardia occurred, 0.5 mg IV atropine was administered If SpO2 < 95%, mask assisted O2 inhalation was given at 3 L/min If nausea or vomiting occurred, 12.5 mg IV promethazine was administered If intractable pain, assisted anaesthetics were added or GA performed and patient was excluded |
|
| Outcomes |
Maternal: incidence of hypotension, bradycardia, nausea and vomiting, peak block height, total consumption of phenylephrine Neonatal: umbilical cord gases, Apgar scores at 1 min and 5 min |
|
| Notes | Hypotension was defined as maternal SBP < 80% baseline Bradycardia was defined as heart rate < 50 bpm Hypertension was defined as SBP > 140 mmHg or DBP > 90 mmHg |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated |
| Allocation concealment (selection bias) | Low risk | Opaque, sealed, sequentially numbered envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Study drugs prepared by anaesthetist not directly involved in the patient scare or assessment. Solutions were in syringes of similar appearance, labelled study drug |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | As above, anaesthetist was blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Group 1: 1 woman excluded from BP analysis due to intractable shivering preventing BP measurement, 2 women excluded from blood gas analysis due to insufficient samples Group 2: 1 woman completely excluded due to failed spinal anaesthesia, 2 women excluded from blood gas analysis because of insufficient samples |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent. Grant from Wuxi Municipal Health Bureau |
Webb 1998.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 40 women Inclusion criteria: parturients receiving spinal anaesthesia for elective CS Exclusion criteria: impalpable lumbar spines, baseline BP > 150/90, coagulopathy, sepsis, hypovolaemia |
|
| Interventions |
Ephedrine versus control Group 1: ephedrine 37.5 mg IM in 1.5 mL saline administered prior to spinal anaesthesia Group 2: placebo 1.5 mL saline IM in deltoid muscle administered prior to spinal anaesthesia All women received a standardised crystalloid preload, and a standardised spinal anaesthetic technique and dose. |
|
| Outcomes |
Maternal: hypotension; hypertension; heart rate Neonatal: Apgar scores at 5 min; umbilical vein pH (expressed as mean and SD) |
|
| Notes | Hypotension was defined as a decrease in SBP < 100 mmHg OR > 70% baseline Hypertension was defined as SBP > 30% above baseline, but no intervention reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding not stated |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding not state |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: not stated |
| Selective reporting (reporting bias) | Unclear risk | Unclear reporting |
| Other bias | Unclear risk | Unclear reporting |
Wilson 1998.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 70 women Inclusion criteria: pregnant women (ASA I or II) undergoing elective CS |
|
| Interventions |
Glucose versus crystalloid preload Group 1: glucose 5% IV Group 2: normal saline IV Administered at 125 mL/h prior to spinal anaesthesia Unclear whether all women received the same anaesthetic technique and dose |
|
| Outcomes |
Maternal: hypotension; total study solution received; total IV preload; glucose levels Neonatal: Apgar scores; umbilical cord gases |
|
| Notes | Hypotension was defined as SBP > 20% decrease | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding: study solutions "were enclosed in an opaque bag to maintain blinding"; "double‐blind" |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: not stated |
| Selective reporting (reporting bias) | Unclear risk | Unclear reporting |
| Other bias | High risk | Variable dose of local anaesthetic used for spinal anaesthesia |
Wilson 1999.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 120 women Inclusion criteria: ASA I‐II singleton pregnancy, able to speak English, undergoing elective CS Exclusion criteria: morbid obesity, glucose intolerance, taking vasoactive medication or that known to alter glucose metabolism |
|
| Interventions |
Comparison of dextrose 5% versus normal saline as a crystalloid preload Group 1: dextrose 5% in normal saline at 125 mL/h IV for 2 hours before surgery Group 2: normal saline at same rate All women received a standardised crystalloid preload after the study drug (normal saline 15 mL/kg) followed by a standardised anaesthetic technique and dose, and standardised surgical positioning |
|
| Outcomes |
Maternal: hypotension; serial blood glucose measurements; preoperative fasting time; total fluid volume administered; block height; spinal‐birth time Neonatal: Apgar scores at 1 min, 5 min, and 10 min; umbilical venous and arterial blood gas; pH; lactate and glucose (generally expressed as mean (SD)) |
|
| Notes | Hypotension defined as a decrease in SBP > 20% or BP less than 100 mmHg | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated table |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding: intervention solutions in opaque bags – participants, anaesthetist and investigator unaware of allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | As above |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses to follow‐up: 1 participant was excluded from saline only group due to incomplete maternal data; and neonatal data were incomplete due to technical problems with umbilical cord blood analysis |
| Selective reporting (reporting bias) | Unclear risk | Unclear reporting |
| Other bias | Unclear risk | Unclear reporting |
Yokoyama 1997.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 30 women Inclusion criteria: healthy women undergoing elective CS under spinal anaesthesia at term Setting: Japan |
|
| Interventions |
Dopamine versus control Group 1: dopamine continuous infusion 5 µg/kg/min Group 2: non‐dopamine infusion All women received a preload of 1000 mL of Ringer's lactate All women received a variable anaesthetic technique (L2‐3 or L3‐4) with variable 0.3% dibucaine doses (1.6‐2.0 mL) |
|
| Outcomes |
Maternal: hypotension; BP; heart rate Neonatal: Apgar scores |
|
| Notes | Hypotension was defined as 90% or less of baseline BP | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Unclear risk | Not apparent, but not well reported |
| Other bias | Unclear risk | Not apparent, but not well reported |
Yorozu 2002.
| Study characteristics | ||
| Methods | RCT | |
| Participants | 67 women Inclusion criteria: without toxaemia, undergoing caesarean under spinal anaesthesia Setting: Japan |
|
| Interventions |
Colloid preload versus crystalloid preload Group 1: HES starch 1% dextrose (n = 32) Group 2: Ringer's lactate (n = 35) For all women IV infusion was commenced at arrival in the operating room and continued until delivery All women received a standardised spinal anaesthetic technique with dose adjusted according to subject's height, and standardised surgical positioning |
|
| Outcomes |
Maternal: pain; time from incision to birth; hypotension; ephedrine dose; duration of hypotension; level of block; blood loss Neonatal: Apgar score; birthweight; blood pH; pO2; pCO2; BE; blood sugar; haemoglobin |
|
| Notes | Hypotension was defined as SBP < 90 mmHg | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Paediatricians blinded for Apgar scores |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Unclear risk | Not apparent, but not well reported |
| Other bias | Unclear risk | Not apparent, but not well reported |
ANP: atrial natriuretic peptide; ASA: American Society of Anesthesiologists Classification; BE: base excess; BMI: body mass index; BP: blood pressure; bpm: beats per minute; cc: cubic centimetre, equivalent to 1 mL; CS: caesarean section; CSE: combined spinal‐epidural; CSF: cerebrospinal fluid; CTG: cardiotocography; CVP: central venous pressure; DBP: diastolic blood pressure; DVT: deep vein thrombosis; ET‐1: enothelin‐1; GA: general anaesthetic; HES: hydroxyethyl starch; IDC: in‐dwelling catheter (urinary catheter); IVT: intravascular transfusion; IM: intramuscular; IV: intravenous; LSCS: lower segment caesarean section; MAP: mean arterial pressure; NACS: neurologic and adaptive capacity score; NICU: neonatal intensive care unit; NS: normal saline; pO2: partial pressure of oxygen; pCO2: partial pressure of carbon dioxide; RCT: randomised controlled trial; SAB: sub‐arachnoid block; SAP: systolic arterial pressure; SBP: systolic blood pressure; SCD: sequential compression device; SD: standard deviation; SEM: standard error of mean; SpO2/SaO2: oximetry; SST: supine stress test; TED: thromboembolic deterrent; w/v: weight/volume; 0.9% NaCl/ 0.9% NS: 0.9% sodium chloride, normal saline.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Adekanye 2007 | Examines effect on combined spinal‐epidural (not spinal anaesthesia alone) |
| Adigun 2010 | Prevention of hypotension was not a study outcome, instead it examined effect of the interventions on restoration of BP. Aim was treatment not prophylaxis |
| Akhtar 2011 | Inadequate information on number of women allocated to each group |
| Alahuhta 1994 | Intervention aimed to treat hypotension not prevent |
| Amponsah 2011 | Investigated prevention of hypotension resulting from combined spinal‐epidural anaesthesia |
| Aragao 2014 | Intervention aimed to treat hypotension not prevent |
| Arai 2008 | Combined spinal‐epidurals performed |
| Arboleda 2012 | Investigated treatment, rather than prevention, of hypotension |
| Armstrong 2010 | Inadequate reporting of study method. It is unclear if patients received spinal versus epidural versus combined spinal‐epidural |
| Ashpole 2005 | Phenylephrine and ephedrine used to maintain systolic arterial pressure (treating hypotension) |
| Atalay 2010 | Anaesthetic regimen differed between groups |
| Atashkhoyi 2012 | Investigated treatment, rather than prevention, of hypotension |
| Ayorinde 2001 | Combined spinal epidural anaesthesia performed |
| Aziz 2013 | Quasi‐randomised study |
| Bach 2002 | Intervention aimed to treat hypotension not prevent |
| Balcan 2011 | Pharmacological treatment of maternal hypotension was studied. Prophylaxis was not studied |
| Basuni 2016 | Comparison of different anaesthetic techniques |
| Belzarena 2006 | Ephedrine or ethylphenylephrine (etilfrine) were used for treating, not preventing, hypotension |
| Benhamou 1998 | Compared different spinal techniques – intervention was adding clonidine or fentanyl to bupivacaine |
| Bhar 2011 | Incidence of hypotension not reported |
| Bhattarai 2010 | Phenylephrine, ephedrine or mephentermine were used for treating, not preventing hypotension |
| Bjornestad 2009 | Participants received epidural, not spinal anaesthesia |
| Borgia 2002 | Participants underwent combined epidural‐spinal anaesthesia |
| Bouchnak 2006 | Compared different spinal anaesthetic techniques – different rates of anaesthetic administration |
| Bouslama 2012 | Dose of the anaesthetic into spinal was not standardised between the study groups (low dose versus high dose). Comparisons between different anaesthetics techniques not included in this review |
| Bryson 2007 | Compared different spinal anaesthetic techniques – different doses of local anaesthetic. |
| Butwick 2007 | Incidence of hypotension not reported |
| Cai 2016 | Combined spinal‐epidurals performed |
| Campbell 1993 | Compared different spinal anaesthetic techniques – intervention compared 2 different needles |
| Cardoso 2004b | Metaraminol was used to maintain BP |
| Cardoso 2005 | Phenylephrine or metaraminol were used for treating, not preventing, hypotension |
| Carvalho 2015 | Not a prospective randomised controlled trial (control group was retrospectively collected from case notes). Also incidence of hypotension not reported. |
| Cesur 2008 | This study evaluated different anaesthetic techniques – hyperbaric bupivacaine alone versus sequential subarachnoid injection of plain bupivacaine followed by hyperbaric bupivacaine |
| Chanimov 2006 | Investigation of effect of fluid preload on neonatal acid‐base status (not maternal hypotension) |
| Choi 2005 | Comparison of different anaesthetic techniques |
| Chung 1996 | Compared different spinal anaesthetic techniques – intervention was volume of anaesthetic |
| Clark 1980 | Dopamine was used for treating, not preventing, hypotension |
| Cohen 2002 | Investigated prevention of hypotension for combined spinal‐epidural anaesthesia for caesarean section |
| Cooper 2002 | Phenylephrine and ephedrine used to maintain systolic arterial pressure (treating hypotension) |
| Cooper 2004 | Phenylephrine and ephedrine used to maintain systolic arterial pressure (treating hypotension) |
| Cooper 2007 | Intervention aimed to treat hypotension not prevent |
| Coppejans 2006 | Combined spinal‐epidurals performed |
| Das 2011 | Inadequate data. This study investigates both the prevention and management of hypotension using a infusion which is commenced prior to spinal injection and then titrated according to BP using a predetermined algorithm. It is the initial prevention of hypotension (prior to titration of the vasopressor infusion) that this Cochrane review examines, however, this is impossible to examine based on the published data in this paper. |
| Datta 1982 | Not randomised (allocated according to BP levels) |
| Davemski 2007 | Intervention aimed to treat hypotension not prevent |
| Defossez 2007 | Treatment rather than prevention |
| Desalu 2005 | Ephedrine or saline used to maintain systolic arterial pressure (treating hypotension) |
| Doherty 2011 | Investigated treatment, rather than prevention, of hypotension. Also incidence of hypotension was not reported |
| Dua 2013 | Investigated treatment of hypotension, not prevention of hypotension |
| Dyer 2009 | Phenylephrine and ephedrine used to maintain systolic arterial pressure (treating hypotension) |
| El‐Hakeem 2011 | Incidence of hypotension not reported |
| Evron 2007 | Investigated prevention of hypotension following combined spinal‐epidural anaesthesia (not spinal anaesthesia alone) |
| Fabrizi 1998 | Inadequate data on specific numbers for incidence of hypotension in each group |
| Farber 2015 | Techniques to prevent incidence of hypotension following spinal anaesthesia for caesarean section not investigated |
| Forkner 2012 | Combined spinal‐epidural anaesthesia performed |
| Foss 2014 | Incidence of hypotension not reported |
| Frikha 2008 | Inadequate data. The number of participants in each study group was not reported. |
| Frolich 2001 | Study not adequately controlled with respect to fluid administration. Methods to prevent maternal hypotension was not a study outcome |
| Fuzier 2005 | Treatment, not prevention, of hypotension |
| Gallo 1996 | Compared different spinal anaesthetic techniques – 2 doses of bupivacaine |
| Gambling 2015 | Combined spinal‐epidural anaesthesia performed |
| Garrison 2005 | Intervention was early identification of signs of hypotension so that women received prompt treatment |
| George 2015 | Treatment, rather than prevention, of hypotension |
| Goudie 1988 | Participants not randomised ('sequential allocation') |
| Guasch 2010 | Investigated different anaesthetic techniques in prevention of maternal hypotension |
| Guillon 2010 | Incidence of hypotension not reported |
| Gulec 2012 | Investigated different doses of levobupivacaine into a combined spinal‐epidural anaesthetic |
| Gulhas 2013 | Only women who developed hypotension were randomised |
| Gunda 2010 | Ephedrine or phenylephrine were used to treat, not prevent, hypotension |
| Gupta 2012 | Women given combined spinal epidural anaesthesia |
| Gutsche 1976 | No mention of randomisation |
| Hahn 1998 | BP 'maintained', thus not prevention |
| Hamzei 2015 | Different anaesthetic agent doses for spinal anaesthesia were compared |
| Hanss 2006 | Quasi‐randomised trial |
| Haruta 1987 | Investigated treatment of hypotension; no definition of hypotension; no evidence of randomisation |
| Hennebry 2009 | Combined spinal‐epidurals performed |
| Higgins 2015 | Investigated treatment of hypotension, not prevention |
| Housni 2004 | Studied the effect of the rate of injection of bupivacaine on haemodynamic changes in elective caesarean |
| Husaini 1998 | Hypotension treated not prevented ‐ ephedrine manually regulated to keep BP in normal range |
| Iwama 2002 | 2 different anaesthetics used ‐ not a randomised trial |
| Jackson 1995 | BP was maintained by ephedrine infusion as well as treated according to rescue criteria for hypotension |
| Jain 2008 | Maintenance, not prevention of hypotension |
| James 1996 | Interventions were differing needle orientations |
| Javed 2014 | Comparison of different anaesthetic techniques |
| John 2013 | Inadequate data – incidence of hypotension following spinal anaesthesia was not reported |
| Kamrul 2012 | Investigated methods of preventing oxytocin induced hypotension by co‐administration of phenylephrine. Preventing of spinal anaesthesia induced hypotension was not investigated. |
| Kang 1982 | BP 'maintained', thus not prevention |
| Kang 1996 | Epidural anaesthesia used |
| Kangas‐Saarela 1990 | Despite adequate definition of hypotension, any fall in BP was treated with ephedrine boluses – not prevention |
| Kansal 2005 | BP 'maintained', thus not prevention |
| Kaya 2007 | Combined spinal epidural anaesthesia performed |
| Keera 2016 | Different anaesthetic techniques compared |
| Kinsella 2012 | Incidence of hypotension not reported |
| Ko 2007 | Combined spinal‐epidurals performed |
| Kumar 2013 | Treatment rather than prevention of spinal hypotension was investigated |
| Kutlesic 2012 | Different anaesthetic techniques investigated |
| Lal 2015 | Intervention aimed to treat hypotension, not prevent |
| Langesaeter 2008 | Combined spinal‐epidurals performed |
| LaPorta 1995 | Comparison of pressors used to treat hypotension, not prevention |
| Law 2003 | Incidence of hypotension not reported |
| Lee 2005 | Intervention aimed to treat hypotension not prevent. |
| Lee 2008 | Investigated prevention of hypotension in combined spinal‐epidural anaesthesia |
| Lee 2012 | Prevention of hypotension was not investigated |
| Lee 2015 | Combined spinal‐epidural anaesthesia performed |
| Lee 2016 | Combined spinal‐epidural anaesthesia performed |
| Lewis 2004 | Ephedrine and/or fluid used to maintain BP |
| Liu 2010 | Epidural anaesthesia used |
| Luo 2016 | Treatment, rather than prevention, of hypotension |
| Madi‐Jebara 2007 | Intervention aimed to treat hypotension not prevent |
| Mahajan 2009 | Study meets criteria for inclusion but unable to interpret data/results presented in paper. Attempted to contact to resolve but no response. |
| Matorras 1998 | Anaesthetist made decision of whether women had general anaesthetic or spinal anaesthesia. Different anaesthetic techniques used therefore excluded |
| Matsota 2013 | Group allocation was not reported. It was not reported to be a "randomised" study |
| Matsota 2015 | Combined spinal‐epidural anaesthesia performed |
| McDonald 2011 | Combined spinal‐epidurals performed |
| McLeod 2010 | Prevention of hypotension following spinal anaesthesia was not investigated. |
| Mebazaa 2010 | This study investigates different spinal anaesthetic doses (i.e. reduction in bupivacaine dose) effect on incidence of hypotension |
| Mendonca 2003 | Combined spinal‐epidurals performed |
| Mercier 2001 | Investigated treatment of hypotension |
| Miller 2000 | Unclear how many women were allocated to each study group |
| Mitra 2014 | This RCT was included in comparison 7 (colloid versus crystalloid) in the Cyna 2017 updated review. However, this study has since been retracted by the Saudi Journal of Anaesthesia and we have now reclassified this study from included to excluded. |
| Mohta 2008 | Dose‐finding comparison between ephedrine and phenylephrine, not a randomised trial |
| Mohta 2015 | Investigated treatment rather than prevention of hypotension |
| Mohta 2016 | Treatment, rather than prevention, of hypotension |
| Moore 2000 | Investigates effect of speed of spinal local anaesthetic injection on incidence of hypotension |
| Moore 2014 | Different anaesthetic agent doses for spinal anaesthesia were compared |
| Moran 1991 | Comparison of pressors used to maintain BP, not used for prevention |
| Mowbray 2002 | Phenylephrine and ephedrine were used for treating, not preventing, hypotension |
| Narejo 2012 | Investigated 2 different types of local anaesthetic used in intrathecal injection and their effects on the incidence of hypotension |
| Nasir 2005 | Comparison of different anaesthetic regimens |
| Negron 2010 | Combined spinal‐epidural anaesthesia performed |
| Ngan 2016 | Treatment, rather than prevention, of hypotension |
| Ngan Kee 2001a | Metaraminol was used for treating, not preventing, hypotension |
| Ngan Kee 2001b | Metaraminol was used for treating, not preventing, hypotension |
| Ngan Kee 2001c | Metaraminol was used for treating, not preventing, hypotension |
| Ngan Kee 2004b | Thresholds of systolic arterial pressure randomised rather than prophylactic interventions |
| Ngan Kee 2005 | Phenylephrine was used to maintain systolic arterial pressure (treating hypotension) |
| Ngan Kee 2008a | Treatment, not prevention |
| Ngan Kee 2008b | Treatment, not prevention |
| Ngan Kee 2009 | Phenylephrine and ephedrine were used to maintain systolic arterial pressure (treating hypotension) |
| Ngan Kee 2011 | Methods to maintain maternal BP was investigated, not methods to prevent hypotension |
| Ngan Kee 2013b | Methods to maintain maternal BP was investigated, not methods to prevent hypotension |
| Ngan Kee 2015 | Investigated treatment of hypotension |
| Nishikawa 2004 | Results not reported for all women who were randomised (5 emergency caesareans not reported in the groups to which they were randomised) |
| Norris 1987 | Crystalloids used for maintaining BP |
| Norris 1989 | Incidence of hypotension not reported |
| Nutangi 2013 | This study investigates the efficacy of vasopressors in treatment (not prevention) of postspinal hypotension. |
| Nze 2003 | Incidence of hypotension not reported |
| Ocio 2013 | Combined spinal‐epidural anaesthesia performed |
| Okutan 2006 | Incidence of hypotension not reported |
| Osseyran 2011 | Anaesthetic techniques varied among participants: spinal anaesthetic is not controlled and position of patient variable (variable bupivicaine dose according to height of patient, ± fentanyl, positioned in supine or side‐lying for SAB). |
| Park 1996 | Study was uncontrolled with respect to haemodynamics – "...ephedrine and additional fluid were given at the discretion of the anesthesiologist ... to maintain a systolic BP > 100 mmHg or 80% of baseline" |
| Peng 2013 | Combined spinal‐epidural anaesthesia conducted, not spinal anaesthesia alone |
| Pickford 2000 | Despite adequate definition of hypotension, rescue ephedrine was also given for nausea and hypotension was not reported |
| Prakash 2010 | Phenylephrine and ephedrine were used to treat, not prevent, hypotension |
| Quan 2013 | Incidence of hypotension not reported |
| Quan 2014 | Combined spinal epidurals performed |
| Quan 2015 | Different anaesthetic agents for spinal anaesthesia were compared |
| Quan 2016 | Different anaesthetic techniques compared |
| Quiney 1995 | Study not adequately controlled – BP maintained within 20% of preoperative value of baseline by adjusting infusion rate of ephedrine in Hartmann's solution |
| Rashad 2013 | Investigated treatment of hypotension |
| Reed 2006 | Intervention aimed to manage hypotension not prevent |
| Rehman 2011 | This study investigated the efficacy of prophylactic ephedrine given soon after spinal block compared to those women who were given treatment boluses of ephedrine only after they developed hypotension |
| Rewari 2015 | Number of women allocated to each study group not reported |
| Ronenson 2014 | Intervention was using different doses of anaesthetic |
| Rout 1993b | Quasi‐randomised study |
| Rout 2000 | Unclear definition of hypotension |
| Rucklidge 2002 | Combined spinal‐epidurals performed |
| Rucklidge 2005 | Combined spinal‐epidurals performed |
| Rumboll 2015 | Prevention of oxytocin‐induced hypotension rather than prevention of spinal‐induced hypotension |
| Russell 2002 | Combined spinal‐epidurals performed |
| Sahin 2015 | Number of women allocated to each study group not reported |
| Sakr 2014 | Combined spinal epidurals performed |
| Sanwal 2008 | Investigated effects of intrathecal midazolam in addition to bupivacaine on post‐spinal hypotension |
| Saravanan 2006 | Combined spinal‐epidurals performed |
| Schofield 2011 | Intervention aimed to treat hypotension not prevent |
| Seltenrich 2001 | Comparison of injection rates of spinal anaesthetic |
| Seyedhejazi 2007 | Investigated the effect of different doses of bupivacaine‐fentanyl on postspinal hypotension |
| Sherif 2013 | Investigated treatment not prevention of hypotension in women having spinal anaesthesia for caesarean section |
| Shifman 2007 | Epidurals performed |
| Siddik‐Sayyid 2013 | Not reported as a randomised study |
| Siddik‐Sayyid 2014 | Techniques to treat, rather than prevent, hypotension |
| Siddiqui 2016 | Compared different anaesthetic doses/regimens |
| Simon 1999 | Compared fast and slow injection rates; no mention of randomisation |
| Sivevski 2006 | Investigated effect of plain bupivacaine versus lower dose bupivacaine with fentanyl on the incidence of hypotension |
| Sng 2013 | Investigated treatment, not prevention of hypotension |
| Sng 2014 | Techniques to treat, rather than prevent, hypotension |
| Sprague 1976 | Not randomised – allocation was sequential |
| Stewart 2010 | Combined spinal‐epidurals performed |
| Stewart 2011 | Investigated the effect of differing rates of phenylephrine infusions (used for the treatment of maternal hypotension) on the incidence of maternal reactive hypertension |
| Stoneham 1999 | Compared different spinal anaesthetic techniques – spinal given in different positions |
| Sumikura 2009 | Investigated the effect of preloading with lactated or bicarbonate Ringer's solutions on fetal acid base balance. Maternal BP was not reported |
| Szmuk 2008 | Treatment, not prevention |
| Tamilselvan 2009 | Combined spinal‐epidurals performed |
| Tanaka 2007 | Not a randomised controlled trial |
| Tanaka 2008 | Phenylephrine dose finding study, not randomised trial |
| Tang 2015 | Combined spinal‐epidural performed; compared different anaesthetic techniques |
| Tekyeh 2013 | Different doses of spinal local anaesthetic compared |
| Teoh 2009 | Not prophylaxis – arterial BP was maintained at 90% to 100% of baseline values |
| Thomas 2001 | Thresholds of systolic arterial pressure randomised rather than prophylactic interventions |
| Thomas 2004 | Given as treatment not prophylaxis |
| Thomas 2006 | Treatment given as baby was born |
| Tolia 2008 | Compared different spinal anaesthetic techniques – different doses of anaesthetics |
| Turker 2011 | Incidence of hypotension not reported |
| Vallejo 2015 | Incidence of hypotension not reported |
| Van Bogaert 1998 | The method by which hypotension was treated was not clearly reported, and potentially inconsistent between study participants |
| Vercauteren 1996 | Investigated CSE technique |
| Vercauteren 2000 | Combined spinal‐epidurals performed |
| Vincent 1998 | Study not adequately controlled – BP maintained at 90% – 100% of baseline by adjusting infusions of intervention pressor |
| Vuffray 2005a | Treatment, rather than prevention, of hypotension |
| Vuffray 2005b | Treatment, rather than prevention, of hypotension |
| Wang 2011 | Intervention aimed to treat hypotension not prevent |
| Wang 2015 | Combined spinal epidurals performed |
| Williamson 2009 | Comparison of different spinal anaesthetic techniques |
| Wojciechowski 2008 | Incidence of hypotension not reported |
| Wollman 1968 | No mention of randomisation of study participants. 'Control group' included 5 parturients having vaginal birth |
| Xiao 2015a | Combined spinal epidurals performed |
| Xiao 2015b | Combined spinal epidurals performed |
| Xu 2012 | Not a randomised trial. This study aimed to determine the median effective volume of crystalloid in preventing hypotension in women undergoing caesarean delivery with spinal anaesthesia. |
| Xu 2014 | Combined spinal‐epidural anaesthesia performed |
| Yadav 2012 | Intervention aimed to treat hypotension not prevent |
| Yentis 2000 | Combined spinal‐epidurals performed |
| Yokoyama 2004 | Variable bupivicaine dosing was used: "The amount of 0.5% bupivacaine hyperbaric solution to be administered was adjusted to aim for a level of anaesthesia of T4, at 2.5ml, with reference to the weight of the patient." |
| Yoon 2012 | Incidence of hypotension not reported |
| Young 1996 | Intervention aimed to treat hypotension not prevent |
| Yun 1998 | Combined spinal‐epidurals performed |
| Yurtlu 2012 | Investigated effect of hyperbaric, isobaric and combinations of bupivacaine for spinal anaesthesia |
| Zakowski 1992 | Comparison of pressors to treat, not prevent, hypotension |
| Zasa 2015 | Only randomised women at high risk of developing hypotension |
| Zhou 2008 | Combined spinal‐epidurals performed |
BP: blood pressure; CSE: combined spinal‐epidural; SBP: systolic blood pressure.
Characteristics of studies awaiting classification [ordered by study ID]
Abedinzadeh 2010.
| Methods | RCT |
| Participants | Women undergoing caesarean section Inclusion criteria: aged 20‐40 years, ASA physical status I and II, single pregnancy, elective caesarean, gestational age ≥ 37 weeks Exclusion criteria: hypovolaemia, deformity of spinal column, increase of intracranial pressure, coagulopathy, infection of skin or soft tissue and dissatisfaction of patient |
| Interventions |
Atropine versus ephedrine versus phenylephrine Group 1: 0.5 mg atropine (IV) before spinal anaesthesia (single dose) Group 2: 5 mg ephedrine before spinal anaesthesia (single dose) Group 3: 100 µg phenylephrine (mucosal) before spinal anaesthesia (single dose) All women receive 500 mL Ringer's lactate before spinal anaesthesia |
| Outcomes |
Maternal: blood pressure; heart rate; oxygen saturation Neonatal: — |
| Notes | Full report published in 2012, in Arabic, abstract is in English Awaiting translation |
Alday 2011.
| Methods | RCT |
| Participants | 80 women undergoing caesarean section Inclusion criteria: absence of uterine activity or fetal risk Exclusion criteria: not specified |
| Interventions |
Ephedrine vs phenylephrine after spinal block Group 1: IV bolus of 0.1 mg/kg plus continuous infusion at a rate of 0.5 mg/kg/h Group 2: IV bolus of 0.5 µg/kg plus continuous infusion at a rate of 1.5 µg/kg/min |
| Outcomes |
Maternal: hypotension; hypertension; bradycardia Neonatal: umbilical cord blood parameters (pH, pCO2, HCO3); Apgar scores |
| Notes | Original article in Spanish Only abstract in English Awaiting translation; unclear if this intervention is for treatment or prevention of hypotension |
Amiri 2013.
| Methods | RCT |
| Participants | 100 pregnant women undergoing elective caesarean section Inclusion criteria: not specified Exclusion criteria: not specified |
| Interventions |
Phenylephrine vs ephedrine post spinal anaesthesia Group 1: 100 μg bolus dose Group 2. 10 mg bolus dose |
| Outcomes |
Maternal: heart rate; BP Neonatal: umbilical cord blood gases |
| Notes | Original article in Arabic Only abstract in English Awaiting translation |
Ashpole 2006.
| Methods | RCT |
| Participants | 40 women undergoing caesarean section Inclusion criteria: not specified Exclusion criteria: not specified |
| Interventions |
Ephedrine versus phenylephrine Group 1: 5 mg/min ephedrine infusions Group 2: 100 μg/min phenylephrine infusions |
| Outcomes |
Maternal: incidence of hypotension; incidence of hypertension; duration of infusion; spinal delivery Neonatal: fetal acidosis |
| Notes | Unclear whether intervention is for treatment or prevention of hypotension – first author contacted 26/06/2017, awaiting response. |
Bennasr 2014.
| Methods | RCT |
| Participants | 120 women undergoing elective caesarean section Inclusion criteria: ASA I and II Exclusion criteria: not specified |
| Interventions |
HES vs normal saline Group 1: 500 mg of HES 130/0.4 (Voluven (R)) Group 2: 500 mL normal saline Both groups received ephedrine for hypotension |
| Outcomes |
Maternal: hypotension; ephedrine requirement and consumption; nausea and vomiting; headache Neonatal: Apgar scores; umbilical blood gases |
| Notes | Original version in French Only abstract available in English Awaiting translation |
Boswell 2008.
| Methods | RCT |
| Participants | 105 women undergoing elective caesarean section |
| Interventions | Group 1: received a 1‐mg/min ephedrine infusion from the time of injection of the spinal solution until uterine incision Group 2: received a 9‐mg ephedrine bolus at the time of injection of the spinal solution. Group 3: received no prophylactic ephedrine |
| Outcomes |
Maternal: time of hypotension; volume of rescue fluid; dose of rescue ephedrine Neonatal: Apgar scores |
| Notes | If SBP fell below IBP, a 250‐mL rescue bolus of normal saline and ephedrine 6 mg were given. If, after 2 min the SBP was still < IBP, a further 6‐mg bolus of ephedrine was given. If, after a further 2 min, the SBP remained < IBP, another 250‐mL bolus of saline with ephedrine 6 mg was given. This 4‐min cycle would be repeated until the SBP was > IBP. The study continued until uterine incision. Abstract only. Unclear whether intervention is for treatment or prevention of hypotension – first author's institution contacted 26 June 2017, awaiting response |
Bright 2003.
| Methods | RCT |
| Participants | 40 women undergoing elective caesarean section |
| Interventions |
Ephedrine vs placebo Group 1: ephedrine 30 mg Group 2: placebo Identical capsules taken by mouth 1 h before institution of the spinal anaesthetic. All participants then received Hartmann's solution 15 mL/kg before subarachnoid injection of 0.5% heavy bupivacaine 2.5 mL and diamorphine 0.25 mg, using a 25‐gauge pencil‐point needle with the patient in the sitting position on the operation table |
| Outcomes |
Maternal: — Neonatal: — |
| Notes | Women were given bolus injections of rescue ephedrine 6 mg on each occasion their systolic blood pressure was less than 80% of that recorded before the spinal injection. Abstract only. Insufficient information to assess risk of bias – unable to find contact details of author |
Golmohammadi 2013.
| Methods | RCT |
| Participants | 112 women undergoing elective caesarean section Inclusion criteria: ASA I and II Exclusion criteria: not specified |
| Interventions |
HES prior to spinal anaesthesia vs HES after spinal anaesthesia Both groups received 500 mg of 6% HES Both groups received rescue dose of combined ephedrine 5 mg/mL with phenylephrine 25 µg/mL |
| Outcomes |
Maternal: hypotension; vVasopressor consumption Neonatal: not specified |
| Notes | Original article in Arabic Only abstract available in English Awaiting translation |
Gonzalez 2014.
| Methods | RCT |
| Participants | 26 women undergoing caesarean section Inclusion criteria: not specified Exclusion criteria: age < 18 years, non‐elective CS, BMI > 40 kg/m², hypertension, multiple pregnancy, high‐risk patients, sepsis, insulin – dependent diabetes mellitus, spinal block level > T5, ongoing epidural anaesthesia |
| Interventions |
Intermittent pneumatic compression system (IPCS) versus control Group 1: IPCS applied to legs Group 2: crystalloid cohydration with 0.9% saline 500 mL (given to women in both groups) |
| Outcomes |
Maternal: diastolic, mean and diastolic arterial pressure; umbilical cord blood gas values; phenylephrine boluses and total dose; haemoglobin levels Neonatal: Apgar scores at 1 min and 5 min |
| Notes | Abstract only; unclear whether intervention is for treatment or prevention of hypotension – unable to find contact details of authors |
Higgins 2009.
| Methods | Not known |
| Participants | Women undergoing caesarean section Inclusion criteria: not specified Exclusion criteria: not specified |
| Interventions |
Coload with colloid versus crystalloid solutions Group 1: 500 mL of Ringer's lactate Group 2: 1000 mL of Ringer's lactate Group 3: 500 mL of 6% hydroxyethyl starch All solutions given over 15 minutes immediately following intrathecal administration of hyperbaric bupivacaine 12 µg with fentanyl 15 mg and morphine 150 µg. |
| Outcomes |
Maternal: hypotension; heart rate; stroke volume; cardiac index; systemic vascular resistance Neonatal: — |
| Notes | Abstract only. Insufficient information to assess risk of bias – first author contacted 26 June 2017, awaiting response |
Hwang 1994.
| Methods | RCT |
| Participants | 21 women undergoing elective caesarean section Inclusion criteria: ASA I Exclusion criteria: not specified |
| Interventions |
Crystalloid 20 min vs crystalloid 10 min prior to spinal Both groups received 20 mL/kg |
| Outcomes |
Maternal: CVP; hypotension Neonatal: not specified |
| Notes | Original article in Korean Only abstract available in English Awaiting translation |
Jain 2013.
| Methods | RCT |
| Participants | 92 women undergoing caesarean section Inclusion criteria: undergoing spinal anesthesia for emergency cesarean delivery indicated due to acute fetal compromise Exclusion criteria: not specified |
| Interventions | Ephedrine versus phenylephrine Group 1: received prophylactic infusions of ephedrine at the rate of 2.5 mg/min Group 2: received prophylactic infusions of phenylephrine at the rate of 30 µg/min |
| Outcomes |
Maternal: systolic blood pressure; umbilical artery pH; need for immediate resuscitation; haemodynamics; intra‐operative nausea/vomiting Neonatal: cord blood gases; incidence of fetal acidosis; Apgar score |
| Notes | Abstract only. Unclear whether intervention is for treatment or prevention of hypotension – first author contacted 26/06/2017, awaiting response. |
Jung 2006.
| Methods | RCT |
| Participants | 900 women undergoing elective caesarean section Inclusion criteria: not specified Exclusion criteria: not specified |
| Interventions |
Ephedrine vs phenylephrine vs ephedrine plus phenylephrine Group 1: ephedrine 2 mg/min infusion with 6 mg bolus Group 2: phenylephrine 33.3 µg/min infusion with 50 µg bolus Group 3: ephedrine plus phenylephrine combined at half the infusion doses and bolus |
| Outcomes |
Maternal: number of boluses given; hypotension; bradycardia Neonatal: umbilical blood gas; Apgar score |
| Notes | Original article in Korean Only abstract available in English Awaiting translation; unclear if intervention is for treatment or prevention |
Kashiwagi 2012.
| Methods | RCT |
| Participants | A non‐specified number of women undergoing elective caesarean section Inclusion criteria: not specified Exclusion criteria: not specified |
| Interventions |
Left 15 degrees tilt vs uterine displacement by hand Ephedrine (4 mg IV) administered in either case for hypotension, nausea or vomiting Group 1: following spinal injection patients turn to 15 degrees left lateral supine position Group 2: following spinal injection patient had uterine displacement by hand |
| Outcomes |
Maternal: arm systolic BP; leg systolic BP; mean ephedrine requirement Neonatal: Apgar scores; umbilical artery pH |
| Notes | Original article in Japanese Only abstract available in English Awaiting translation |
Kiss 2012.
| Methods | RCT |
| Participants | 102 women undergoing caesarean section Inclusion criteria: not specified Exclusion criteria: fetal distress, severe comorbidities, urgent caesarean section for any cause |
| Interventions | Ringer's lactate versus balanced Ringer's solution |
| Outcomes |
Maternal: mean arterial pressure; heart rate; oxygen saturation Neonatal: — |
| Notes | Abstract only. Unclear if intervention is treatment or prevention of hypotension – unable to find contact details of authors |
Lang 1996.
| Methods | RCT |
| Participants | 38 women undergoing caesarean section Inclusion criteria: not specified Exclusion criteria: not specified |
| Interventions | Ringer's lactate versus albumin solution Group 1: 50 mL/kg of Ringer's lactate before spinal anaesthesia with 12 mg of bupivacaine Group 2: 15 mL/kg of 5% albumin solution before spinal anaesthesia with 12 mg of bupivacaine |
| Outcomes |
Maternal: mean arterial pressure; umbilical cord blood gases; arterial natriuretic peptide; cardiac output Neonatal: Apgar scores; fetal biochemical profiles |
| Notes | Abstract only. Insufficient information to assess risk of bias – unable to find contact details of authors |
Lee 2011.
| Methods | Not known |
| Participants | 45 women undergoing caesarean section Inclusion criteria: not clear Exclusion criteria: not clear |
| Interventions | Prehydration versus Wrapping of legs Group 1: prehydration with 10 mL/kg Group 2: prehydration with 10 mL/kg and wrapping of the legs Group 3: prehydration with 5 mL/kg and wrapping of the legs |
| Outcomes |
Maternal: incidence of hypotension; systolic arterial pressure Neonatal: — |
| Notes | Full report is in Chinese while the abstract is in English Awaiting translation |
Osazuwa 2015.
| Methods | RCT |
| Participants | Women undergoing caesarean section Inclusion criteria: not specified Exclusion criteria: not specified |
| Interventions | Colloid versus crystalloid versus combination of both preloads Group 1: 500 mL of Ringer's lactate, preload, before spinal anaesthesia Group 2: 500 mL of 6% pentastarch, preload, before spinal anaesthesia Group 3: combination of 250 mL of 6% pentastarch and 750 mL of Ringer's lactate intravenous fluid preload, before spinal anaesthesia |
| Outcomes |
Maternal: hypotension Neonatal: not specified |
| Notes | Abstract only. Insufficient information to assess risk of bias – first author contacted 26/06/2017, awaiting response. |
Rahmoune 2009.
| Methods | RCT |
| Participants | 62 women undergoing caesarean section Inclusion criteria: women with ASA I status Exclusion criteria: not specified |
| Interventions |
Colloid versus control Group 1: preloading with 500 mL of a gelatine modified fluid (Gelofusine 4%) over 10 min before spinal anaesthesia Group 2: no preload |
| Outcomes |
Maternal: systolic arterial blood pressure; incidence of nausea and vomiting; allergic reactions Neonatal: Apgar scores at 1 min and 5 minutes; cord blood gases |
| Notes | Abstract only. Insufficient information to assess risk of bias – unable to find contact details for authors. |
Sahoo 2011.
| Methods | RCT |
| Participants | 40 women undergoing caesarean section Inclusion criteria: full‐term pregnant women of ASA grade I and II, posted for cesarean section Exclusion criteria: not specified |
| Interventions |
Phenylephrine versus colloids (hydroxyethyl starch) Group 1: women received phenylephrine at 60 µg/min for 2 min unless SBP was > 120% of baseline immediately after intrathecal injection Group 2: women received rapid colloid infusion (12 mL/kg of hydroxyethyl starch 6%) immediately after intrathecal injection |
| Outcomes |
Maternal: blood pressure; fall in BP below 80% of baseline; umbilical artery pH Neonatal: — |
| Notes | Abstract only. Unclear if intervention is for treatment or prevention of hypotension – first author's institution contacted 26 June 2017, awaiting response |
Sakuma 2010.
| Methods | RCT |
| Participants | 32 patients undergoing caesarean delivery Inclusion criteria: not specified Exclusion criteria: not specified |
| Interventions |
Phenylephrine vs ephedrine Both groups received drug after spinal Group 1: phenylephrine continuous infusion – details not specified in abstract Group 2: ephedrine continuous infusion – details not specified in abstract |
| Outcomes |
Maternal: block height; haemodynamic changes Neonatal: umbilical artery pH |
| Notes | Original article in Japanese Only abstract available in English Awaiting translation; unclear if intervention is for treatment or prevention of hypotension |
Soltani 2009.
| Methods | RCT |
| Participants | 300 women undergoing caesarean section Inclusion criteria: not specified Exclusion criteria: not specified |
| Interventions | Combination of 2 interventions Group 1: crystalloid and colloid: Ringer's lactate (15 mL/kg) and Hemaxel (7ml/kg) – both given before spinal anaesthesia (SA) Group 2: crystalloid and ephedrine: Ringer's lactate (15 mL/kg) given before SA and ephedrine 15 mg IV, after SA Group 3: crystalloid and bandage: Ringer's lactate (15 mL/kg) and lower limb bandage Group 4: colloid and ephedrine: hydroxyethyl starch (7ml/kg) given before SA, and ephedrine 15 mg IV, after SA Group 5: colloid and bandage: hydroxyethyl starch (7ml/kg) given before SA, and lower limb bandage Group 6: ephedrine and bandage: ephedrine 15 mg, IV after SA, and lower limb bandage |
| Outcomes |
Maternal: pulse rate; systolic blood pressure Neonatal: Apgar score; neurological and adaptive capacity score (NACS) |
| Notes | Abstract only. Insufficient information to assess risk of bias – first author contacted 26 June 2017, awaiting response |
Van Bogaert 2000.
| Methods | RCT |
| Participants | 68 women undergoing caesarean section Inclusion criteria: not specified Exclusion criteria: not specified |
| Interventions |
Hip flexion versus no flexion Immediately after the administration of subarachnoid injection, women were placed in Fowler's position (30 degree raised head and shoulders, 15 degree lateral tilt) Group 1: hip flexed at 45 degree for 5 minutes Group 2: legs were straight |
| Outcomes |
Maternal: systolic arterial pressure; incidence of hypotension Neonatal: Apgar scores |
| Notes | Brief communication only. Insufficient information to assess risk of bias – first author contacted 26 June 2017, email bounced, unable to find other contact |
Van Treese 1996.
| Methods | RCT |
| Participants | 60 women undergoing caesarean section Inclusion criteria: ASA physical status I and II Exclusion criteria: pregnancy‐induced hypertension; pre‐eclampsia or eclampsia; illegal drug use; fetal distress; nausea and vomiting; maternal coagulopathy; high/low blood pressure; diabetes |
| Interventions | All women in both the groups received 15‐20 mL/kg Ringer's lactate 20‐30 minutes prior to subarachnoid block (SAB), left uterine displacement (LUD), and ephedrine as needed Group 1: TED compression prior to fluid loading and SAB, and fluids Group 2: TED compression and foam wedge that elevates leg to 30 degree within 5 minutes following SAB prior to fluid loading and SAB, and fluids Group 3: received only fluids |
| Outcomes |
Maternal: incidence of hypotension; blood loss Neonatal: not specified |
| Notes | Abstract only. Insufficient information to assess risk of bias – unable to find contact details. |
Yoon 2009.
| Methods | RCT |
| Participants | 32 women undergoing caesarean section Inclusion criteria: not specified Exclusion criteria: not specified |
| Interventions | Ephedrine versus phenylephrine versus combination of both infusions |
| Outcomes |
Maternal: systolic blood pressure; pulse rate; systolic vascular resistance index; cardiac index; stroke volume index; nausea and vomiting scores; total fluid intake; phenylephrine rescues; umbilical vein pH Neonatal: Apgar scores |
| Notes | Full report is available in Korean Awaiting translation. Unclear if intervention is for treatment or prevention of hypotension. |
BMI: body mass index; BP: blood pressure; CVP: central venous pressure; HES: hydroxyethyl starch solution; IBP: invasive blood pressure; IM: intramuscular; IV: intravenous; RCT: randomised controlled trial; SAB: sub‐arachnoid block; TED: thromboembolic deterrent.
Characteristics of ongoing studies [ordered by study ID]
NCT01891175.
| Study name | Prevention of maternal hypotension during elective caesarean section performed with spinal anaesthesia, through intermittent pneumatic compression system in the lower extremities |
| Methods | RCT |
| Participants |
Inclusion criteria: age > 18 years; elective caesarean section Exclusion criteria: emergency caesarean; epidural anaesthesia; caesarean section of multiple pregnancies; obstetric pathology (pre‐eclampsia, eclampsia, HELLP syndrome (haemolysis elevated liver enzymes low platelet count), small‐for‐gestational age, preterm (< 32 weeks); valvular heart disease; hypertension; sepsis; BMI > 40 kg/m²; insulin dependent diabetes mellitus; block level achieved with spinal anaesthesia > T5; patients that cannot meet the study protocol |
| Interventions | Phenylephrine infusion vs phenylephrine infusion with intermittent pneumatic compression |
| Outcomes |
Maternal: vasopressor dose required; effectiveness of intermittent pneumatic compression system to decrease requirement of vasopressors Neonatal: not specified |
| Starting date | — |
| Contact information | — |
| Notes | Information obtained from trial registry |
BMI: body mass index; RCT: randomised controlled trial.
Differences between protocol and review
In this update (2017), the criteria for considering studies for this review were changed to exclude:
quasi‐randomised, cluster or cross‐over studies;
studies in which women received combined spinal‐epidural anaesthesia or epidural anaesthesia.
Primary and secondary outcomes were specified from the main and other outcomes.
We reported Apgar scores as they were reported by trialists. This meant that as well as Apgar scores of less than 7 or 8 at five minutes, we reported Apgar scores of less than 9 at five minutes.
We only performed assessment of publication bias through funnel plots for the primary outcome, as it was likely caused by the large amount of small trials that contributed to all the analyses.
Contributions of authors
Planning review: Allan Cyna, Scott Simmons. Writing protocol: Allan Cyna, Scott Simmons. Revising protocol: Allan Cyna, Richard Emmett, Scott Simmons. Retrieving papers for review: Richard Emmett. Extracting data from reviewed papers: Cheryl Chooi, Julia Cox, Richard Lumb. Writing draft review: Richard Emmett, Allan Cyna. Revising original review: Scott Simmons, Allan Cyna, Richard Emmett. First update and amendments: Allan Cyna, Richard Emmett, Philippa Middleton. Second update (2006) and amendments: Allan Cyna and Philippa Middleton, with comments from the other review authors. Third update (2017) and amendments: Cheryl Chooi, Julia Cox, Richard Lumb.
Sources of support
Internal sources
Discipline of Obstetrics and Gynaecology, The University of Adelaide, Australia
Department of Health and Ageing, Australia
External sources
No sources of support supplied
Declarations of interest
Cheryl Chooi: none known. Richard S Lumb: none known. Julia J Cox: none known. Richard S Emmett: none known. Philippa Middleton: none known. Scott W Simmons: none known. Mark Chemali: none known. Allan M Cyna: is also an author of one of the included studies (Cyna 2010). CC and RSL extracted data from this study.
Edited (no change to conclusions)
References
References to studies included in this review
Adsumelli 2003 {published data only}
- Adsumelli RSN, Steinberg ES, Schabel JE, Saunders TA, Poppers PJ. Sequential compression device with thigh-high sleeves supports mean arterial pressure during caesarean section under spinal anaesthesia. British Journal of Anaesthesia 2003;91(5):695-8. [DOI] [PubMed] [Google Scholar]
Alahuhta 1992 {published data only}
- Alahuhta S, Rasanen J, Jouppila P, Jouppila R, Hollmen AI. Ephedrine and phenylephrine for avoiding maternal hypotension due to spinal anaesthesia for caesarean section. International Journal of Obstetric Anesthesia 1992;1(3):129-34. [DOI] [PubMed] [Google Scholar]
Alimian 2014 {published data only}
- Alimian M, Mohseni M, Safaeian R, Faiz SH, Majedi MA. Comparison of hydroxyethyl starch 6% and crystalloids for preloading in elective caesarean section under spinal anesthesia. Medical Archives (Sarajevo, Bosnia and Herzegovina) 2014;68(4):279-81. [DOI] [PMC free article] [PubMed] [Google Scholar]
Allen 2010 {published data only}
- Allen TK, George RB, White WD, Muir HA, Habib AS. A double-blind, placebo-controlled trial of four fixed rate infusion regimens of phenylephrine for hemodynamic support during spinal anesthesia for cesarean delivery. Anesthesia & Analgesia 2010;111(5):1221-9. [DOI] [PubMed] [Google Scholar]
Amaro 1998 {published data only}
- Amaro AR, Capelli EL, Cardoso MMSC, Rosa MCR, Carvalho JCA. Manual left uterine displacement or modified Crawford's edge. A comparative study in spinal anesthesia for cesarean delivery [Deslocamento uterino manual ou cunha de crawford modificada? Estudo comparativo em raquianestesia para cesarianas]. Revista Brasileira de Anestesiologia 1998;48(2):99-104. [Google Scholar]
Ansari 2011 {published data only}
- Ansari T, Hashem M, Razek A, Gamassy A, Saleh A. Comparison of two doses of phenylephrine with crystalloid cohydration for prevention of spinal anaesthesia-induced hypotension during elective caesarean section: a double-blind randomised controlled study. International Journal of Obstetric Anesthesia 2009;18(Suppl 1):S37. [Google Scholar]
- Ansari T, Hashem MM, Hassan AA, Gamassy A, Saleh A. Comparison between two phenylephrine infusion rates with moderate co-loading for the prevention of spinal anaesthesia-induced hypotension during elective caesarean section. Middle East Journal of Anesthesiology 2011;21(3):361-6. [PubMed] [Google Scholar]
Arora 2015 {published data only}
- Arora P, Singh RM, Kundra S, Gautam PL. Fluid administration before caesarean delivery: Does type and timing matter? Journal of Clinical and Diagnostic Research 2015;9(6):UC01-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bhagwanjee 1990 {published data only}
- Bhagwanjee S, Rocke DA, Rout CC, Koovarjee RV, Brijball R. Prevention of hypotension following spinal anaesthesia for elective caesarean section by wrapping of the legs. British Journal of Anaesthesia 1990;65(6):819-22. [DOI] [PubMed] [Google Scholar]
Bhardwaj 2013 {published data only}
- Bhardwaj N, Jain K, Arora S, Bharti N. A comparison of three vasopressors for tight control of maternal blood pressure during cesarean section under spinal anesthesia: effect of maternal and fetal outcome. Journal of Anaesthesia and Clinical Pharmacology 2013;29(1):26-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bottiger 2010 {published data only}
- Bottiger B, Bezinover D, Dalal P, Prozesky J, Vaida S. Comparison of phenylephrine infusion with colloids vs. crystalloids for reduction of spinal induced hypotension during cesarean delivery preliminary results. In: Society for Obstetric Anesthesia and Perinatology (SOAP) 42nd Annual Meeting; 2010 May 12-16, San Antonio, USA. soap.org/display_2010_abstract.php?id=114: Society for Obstetric Anesthesia and Perinatology, 2010. [Abstract no 114]
- NCT00846651. Spinal anesthesia induced hypotension during cesarean section [Comparison of phenylephrine infusion with colloids vs. crystalloids for reduction of spinal-induced hypotension during cesarean section]. clinicaltrials.gov/show/NCT00846651 (first received 18 February 2009).
Bouchnak 2012 {published data only}
- Bouchnak M, Magouri M, Abassi S, Khemiri K, Tlili F, Troudi H, et al. Preloading with HES 130/0.4 versus normal saline solution to prevent hypotension during spinal anaesthesia for elective caesarean section [Préremplissage par HEA 130/0,4 versus sérum salé isotonique dans la prévention de l'hypotension au cours de la rachianesthésie pour césarienne programmée]. Annales Françaises d'Anesthésie et de Réanimation 2012;31:523-7. [DOI] [PubMed] [Google Scholar]
Calvache 2011 {published data only}
- Calvache JA, Munoz MF, Baron F. Hemodynamic effects of a right lumbar-pelvic wedge during spinal anesthesia for cesarean section. British Journal of Anaesthesia 2012;108(Suppl 2):ii96. [DOI] [PubMed] [Google Scholar]
- Calvache JA, Munoz MF, Baron FJ. Hemodynamic effects of a right lumbar-pelvic wedge during spinal anesthesia for cesarean section. International Journal of Obstetric Anesthesia 2011;20(4):307-11. [DOI] [PubMed] [Google Scholar]
Cardoso 2004a {published data only}
- Cardoso MMSC, Bliacheriene S, Freitas CRC, Cesar DS, Torres MLA. Preload during spinal anesthesia for cesarean section: comparison between crystalloid and colloid solutions. Revista Brasileira de Anestesiologia 2004;54(6):781-7. [DOI] [PubMed] [Google Scholar]
Carvalho 1999a {published data only}
- Carvalho JCA, Cardoso MMSC, Capelli EL, Amaro AR, Rosa MCR. Prophylactic ephedrine during cesarean delivery spinal anesthesia: dose-response study of bolus and continuous infusion administration [Efedrina profilatica durante raquianestesia para cesariana: estudo dose-resposta da administracao em bolus e em infusao continua]. Revista Brasileira de Anestesiologia 1999;49(5):309-14. [Google Scholar]
Carvalho 1999b {published data only}
- Carvalho JCA, Cardoso MMSC, Capelli EL, Amaro AR, Rosa MCR. Prophylactic ephedrine during cesarean delivery spinal anesthesia: dose-response study of bolus and continuous infusion administration [Efedrina profilatica durante raquianestesia para cesariana: estudo dose-resposta da administracao em bolus e em infusao continua]. Revista Brasileira de Anestesiologia 1999;49(5):309-14. [Google Scholar]
Carvalho 2000 {published data only}
- Carvalho JCA, Cardoso MMSC, Lorenz E, Amaro AR, Rosa MCR. Prophylactic ephedrine during spinal anesthesia for cesarean section: bolus followed by continuous infusion in fixed doses or continuous infusion in decreasing doses. Revista Brasileira de Anestesiologia 2000;50(6):425-30. [Google Scholar]
Carvalho 2009 {published data only}
- Carvalho B, Mercier FJ, Riley ET, Brummel C, Cohen SE. Hetastarch co-loading is as effective as pre-loading for the prevention of hypotension following spinal anesthesia for cesarean delivery. International Journal of Obstetric Anesthesia 2009;18(2):150-5. [DOI] [PubMed] [Google Scholar]
Chan 1997 {published data only}
- Chan WS, Irwin MG, Tong WN, Lam YH. Prevention of hypotension during spinal anaesthesia for caesarean section: ephedrine infusion versus fluid preload. Anaesthesia 1997;52(9):908-13. [DOI] [PubMed] [Google Scholar]
Chohedri 2007 {published data only}
- Chohedri AH, Khojeste L, Shahbazi S, Alahyari E. Ephedrine for prevention hypotension; comparison between intravenous, intramuscular and oral administration during spinal anesthesia for elective cesarean section. Professional Medical Journal 2007;14(4):610-5. [Google Scholar]
Cyna 2010 {published data only}
- ACTRN12606000391572. Walking versus lying to prevent hypotension following spinal anaesthesia for caesarean section [Walking versus lying to prevent hypotension following spinal anaesthesia for caesarean section: a randomised controlled trial]. anzctr.org.au/Trial/Registration/TrialReview.aspx?id=81583 (first received 5 September 2006).
- Barnard A, Newman M, Cyna AM. Walking versus lying to prevent hypotension following spinal anaesthesia for caesarean section - a randomised controlled trial. Anaesthesia and Intensive Care 2010;38(4):769-70. [Google Scholar]
Dahlgren 2005 {published data only}
- Dahlgren G, Granath F, Pregner K, Rosblad PG, Wessel, Irestedt L. Colloid vs. crystalloid preloading to prevent maternal hypotension during spinal anaesthesia for elective cesarean section. Acta Anaesthesiologica Scandinavica 2005;49(8):1200-6. [DOI] [PubMed] [Google Scholar]
Dahlgren 2007 {published data only}
- Dahlgren G, Granath F, Wessel H, Irestedt L. Prediction of hypotension during spinal anesthesia for cesarean section and its relation to the effect of crystalloid or colloid preload. International Journal of Obstetric Anesthesia 2007;16(2):128-34. [DOI] [PubMed] [Google Scholar]
Damevski 2011 {published data only}
- Damevski V, Damevska G, Krivasija M, Nojkov J, Sivevski A. Caesarean section in isobaric spinal anesthesia with and without direct preoperative hydration with crystalloids. Bratislava Medical Journal 2011;112(8):459-62. [PubMed] [Google Scholar]
Das Neves 2010 {published data only}
- Das Neves JFNP, Monteiro GA, Almeida JR, Sant'Anna RS, Bonin HB, Macedo CF. Phenylephrine for blood pressure control in elective cesarean section: therapeutic versus prophylactic doses. Revista Brasileira de Anestesiologia 2010;60(4):391-8. [DOI] [PubMed] [Google Scholar]
Davies 2006 {published data only}
- Davies P, French GW. A randomised trial comparing 5 ml/kg and 10 ml/kg of pentastarch as a volume preload before spinal anaesthesia for elective caesarean section. International Journal of Obstetric Anesthesia 2006;15(4):279-83. [DOI] [PubMed] [Google Scholar]
Doherty 2012 {published data only}
- Doherty A, Ohashi Y, Downey K, Carvalho JCA. Phenylephrine infusion versus bolus regimens during cesarean delivery under spinal anesthesia: a double-blind randomized clinical trial to assess hemodynamic changes. Anesthesia & Analgesia 2012;115(6):1343-50. [DOI] [PubMed] [Google Scholar]
Dyer 2004 {published data only}
- Dyer RA, Farina Z, Joubert IA, Du Toit P, Meyer M, Torr G, et al. Crystalloid preload versus rapid crystalloid administration after induction of spinal anaesthesia (coload) for elective caesarean section. Anaesthesia and Intensive Care 2004;32(3):351-7. [DOI] [PubMed] [Google Scholar]
Eldaba 2015 {published data only}
- Eldaba AA, Amr YM. Intravenous granisetron attenuates hypotension during spinal anesthesia in cesarean delivery: a double-blind, prospective randomized controlled study. Journal of Anaesthesiology, Clinical Pharmacology 2015;31(3):329-32. [DOI] [PMC free article] [PubMed] [Google Scholar]
El‐Mekawy 2012 {published data only}
- El-Mekawy NM. Comparative study between ephedrine infusion vs. CO/post loading of fluids for prevention of hypotension in emergency cesarean section under spinal anesthesia. Egyptian Journal of Anaesthesia 2012;28(3):193-8. [Google Scholar]
Embu 2011 {published data only}
- Embu HY, Isamade ES, Nuhu SI, Ishaku LA. Prevention of spinal hypotension during caesarean section: comparison of 6% hydroxyethyl starch and ringer's lactate. African Journal of Anaesthesia and Intensive Care 2011;11(1):1-5. [Google Scholar]
Farid 2016 {published data only}
- Farid Z, Mushtaq R, Ashraf S, Zaeem K. Comparative efficacy of crystalloid preloading and co-loading to prevent spinal anesthesia induced hypotension in elective caesarean section. Pakistan Journal of Medical and Health Sciences 2016;10(1):42-5. [Google Scholar]
Faydaci 2011 {published data only}
- Faydaci F, Gunaydin B. Different preloading protocols with constant ephedrine infusion in the prevention of hypotension for elective cesarean section under spinal anesthesia. Acta Anaesthesiologica Belgica 2011;62(1):5-10. [PubMed] [Google Scholar]
French 1999 {published data only}
- French GWG, White JB, Howell SJ, Popat M. Comparison of pentastarch and Hartmann's solution for volume preloading in spinal anaesthesia for elective caesarean section. British Journal of Anaesthesia 1999;83(3):475-7. [DOI] [PubMed] [Google Scholar]
- French GWG, White JB, Popat M. Volume preloading with pentastarch in elective caesarean section: a prospective, randomized double-blind trial. International Journal of Obstetric Anesthesia 1998;7:207-8. [Google Scholar]
Gomaa 2003 {published data only}
- Gomaa GA, Elewa SA. Prophylactic use of vasopressors for reduction of spinal anaesthesia-induced hypotension during caesarean section. Egyptian Journal of Anaesthesia 2003;19(1):45-50. [Google Scholar]
Grubb 2004 {published data only}
- Grubb CT, Balestrieri PJ, Durieux ME. Effects of intramuscular ephedrine during subarachnoid block for cesarean delivery [abstract]. Anesthesiology 2004;101 Suppl:A1184. [Google Scholar]
Gulhas 2012 {published data only}
- Gulhas N, Ozgul U, Erdil F, Sanli M, Nakir H, Yologlu S, et al. The effect of low-dose ketamine on ephedrine requirement following spinal anesthesia in cesarean sections: a randomised controlled trial. HealthMED 2012;6(8):2870-6. [Google Scholar]
Gunaydin 2009 {published data only}
- Gunaydin B, Camgoz N, Polat GA. [Comparison of maternal and neonatal effects of fixed volume of crystalloid or colloid preloading for elective cesarean sections before spinal anesthesia] [Sezaryen operasyonlarinda spinal anestezi oncesi sabit volumde kristalloid veya kolloid onyuklemesinin maternal ve neonatal etkileri nin karsilastirilmasi]. Anestezi Dergisi 2009;17(4):205-10. [Google Scholar]
Gunusen 2010 {published data only}
- Gunusen I, Karaman S, Ertugrul V, Firat V. Effects of fluid preload (crystalloid or colloid) compared with crystalloid co-load plus ephedrine infusion on hypotension and neonatal outcome during spinal anaesthesia for caesarean delivery. Anaesthesia and Intensive Care 2010;38(4):647-53. [DOI] [PubMed] [Google Scholar]
Hall 1994 {published data only}
- Hall PA, Bennett A, Wilkes MP, Lewis M. Spinal anaesthesia for caesarean section: comparison of infusions of phenylephrine and ephedrine. British Journal of Anaesthesia 1994;73(4):471-4. [DOI] [PubMed] [Google Scholar]
Hartley 2001 {published data only}
- Hartley H, Ashworth H, Kubli M, O'Sullivan G, Seed PT, Reynolds F. Spinal anesthesia for cesarean section: a comparison of the effects of right lateral and supine-wedged positions on blood pressure. Anesthesiology 2000;92(Suppl):A91. [Google Scholar]
- Hartley H, Seed PT, Ashworth H, Kubli M, O'Sullivan G, Reynolds F. Effect of lateral versus supine wedged position on development of spinal blockade and hypotension. International Journal of Obstetric Anesthesia 2001;10(3):182-8. [DOI] [PubMed] [Google Scholar]
Hasan 2012 {published data only}
- Hasan AB, Mondal MK, Badruddoza NM, Bhowmick DK, Islam MS, Akhtaruzzaman KM, et al. Comparison of three fluid regimens for preloading in elective caesarean section under spinal anaesthesia. Mymensingh Medical Journal: MMJ 2012;21(3):533-40. [PubMed] [Google Scholar]
Hwang 2012 {published data only}
- Hwang JW, Oh AY, Song IA, Na HS, Ryu JH, Park HP, et al. Influence of a prolonged lateral position on induction of spinal anesthesia for cesarean delivery: a randomized controlled trial. Minerva Anestesiologica 2012;78(6):646-52. [PubMed] [Google Scholar]
Idehen 2014 {published data only}
- Idehen HO, Amadasun FE, Ekwere IT. Comparison of intravenous colloid and colloid-crystalloid combination in hypotension prophylaxis during spinal anesthesia for cesarean section. Nigerian Journal of Clinical Practice 2014;17(3):309-13. [DOI] [PubMed] [Google Scholar]
Imam 2012 {published data only}
- Imam SM, Ali CA, Hussain S. The efficacy of prophylactic combination therapy using ephedrine iv along with fluid preload as compared to fluid preloading alone or IV ephedrine alone in prevention of maternal hypotension during spinal anesthesia for caesarean section. Pakistan Journal of Medical and Health Sciences 2012;6(3):573-6. [Google Scholar]
Inglis 1995 {published data only}
- Inglis A, Daniel M, McGrady E. Maternal position during induction of spinal anaesthesia for caesarean section: a comparison of right lateral and sitting positions. Anaesthesia 1995;50(4):363-5. [DOI] [PubMed] [Google Scholar]
- Inglis A, Daniel M, McGrady EM. Single-shot spinal anaesthesia for caesarean section: a comparison of right lateral and sitting positions. International Journal of Obstetric Anesthesia 1994;3(3):180-1. [Google Scholar]
Jabalameli 2011 {published data only}
- Jabalameli M, Soltani AH, Hashemi J, Behdad S, Soleimani B. A randomized comparative trial of combinational methods for preventing post-spinal hypotension at elective cesarean delivery. Journal of Research in Medical Sciences 2011;16(9):1129-38. [PMC free article] [PubMed] [Google Scholar]
Jacob 2012 {published data only}
- Jacob JJ, Williams A, Verghese M, Afzal L. Crystalloid preload versus crystalloid coload for parturients undergoing cesarean section under spinal anesthesia. Journal of Obstetric Anaesthesia and Critical Care 2012;2(1):10-5. [Google Scholar]
James 1973 {published data only}
- James FM, Greiss FC. The use of inflatable boots to prevent hypotension during spinal anesthesia for cesarean section. Anesthesia & Analgesia 1973;52:246-51. [PubMed] [Google Scholar]
Jorgensen 1996 {published data only}
- Jorgensen J, Christensen PK, Sonnenschein CH. Compression stockings as prevention of hypotension in cesarean section during spinal anesthesia. Ugeskrift for Laeger 1996;158(11):1526-9. [PubMed] [Google Scholar]
Jorgensen 2000 {published data only}
- Jorgensen HS, Bach LF, Helbo-Hansen HS, Nielsen PA. Warm or cold saline for volume preload before spinal anaesthesia for caesarean section? International Journal of Obstetric Anesthesia 2000;9(1):20-5. [DOI] [PubMed] [Google Scholar]
Karinen 1995 {published data only}
- Karinen J, Rasanen J, Alahuhta S, Jouppila R, Jouppila P. Effect of crystalloid and colloid preloading on uteroplacental and maternal haemodynamic state during spinal anaesthesia for caesarean section. British Journal of Anaesthesia 1995;75(5):531-5. [DOI] [PubMed] [Google Scholar]
Khan 2013 {published data only}
- Khan M, Waqar-ul-Nisai, Farooqi A, Ahmad N, Qaz S. Crystalloid co-load: a better option than crystalloid pre-load for prevention of postspinal hypotension in elective caesarean section. Internet Journal of Anesthesiology 2013;32(1).
King 1998 {published data only}
- King SW, Rosen MA. Prophylactic ephedrine and hypotension associated with spinal anesthesia for cesarean delivery. International Journal of Obstetric Anesthesia 1998;7(1):18-22. [DOI] [PubMed] [Google Scholar]
Kohler 2002 {published data only}
- Kohler F, Sorensen JF, Helbo-Hansen HS. Effect of delayed supine positioning after induction of spinal anaesthesia for caesarean section. Acta Anaesthesiologica Scandinavica 2002;46(4):441-6. [DOI] [PubMed] [Google Scholar]
Kohli 2013 {published data only}
- Kohli M, Arora S. Evaluation of efficacy of sequential compression device for prevention of hypotension after spinal anaesthesia in caesarean section. International Journal of Obstetric Anesthesia 2013;22(Suppl 1):S30. [Google Scholar]
Kuhn 2016 {published data only}
- Kuhn JC, Hauge TH, Rosseland LA, Dahl V, Langesaeter E. Continuous hemodynamic monitoring during caesarean delivery: phenylephrine infusion versus lower extremity compression. A randomized, double-blinded, placebo-controlled study. In: Society for Obstetric Anesthesia and Perinatology (SOAP) 47th Annual Meeting; 2015 May 13-17; Colorado, USA. 2015:O2-02.
- Kuhn JC, Hauge TH, Rosseland LA, Dahl V, Langesaeter E. Hemodynamics of phenylephrine infusion versus lower extremity compression during spinal anesthesia for cesarean delivery: a randomized, double-blind, placebo-controlled study. Anesthesia & Analgesia 2016;122(4):1120-9. [DOI] [PubMed] [Google Scholar]
Kundra 2007 {published data only}
- Kundra P, Khanna S, Habeebullah S, Ravishankar M. Manual displacement of the uterus during caesarean section. Anaesthesia 2007;62(5):460-5. [DOI] [PubMed] [Google Scholar]
Kundra 2008 {published data only}
- Kundra S, Abraham V, Afzal L. Prevention of hypotension during spinal anaesthesia for caesarean section: ephedrine infusion versus crystalloid preloading. Journal of Anaesthesiology Clinical Pharmacology 2008;24(4):433-6.
Lin 1999 {published data only}
- Lin CS, Lin TY, Huang CH, Lin YH, Lin CR, Chan WH, et al. Prevention of hypotension after spinal anesthesia for cesarean section: dextran 40 versus lactated Ringer's solution. Acta Anaesthesiologica Sinica 1999;37(2):55-9. [PubMed] [Google Scholar]
Loke 2002 {published data only}
- Loke GPY, Chan EHY, Sia ATH. The effect of 10 (degree) head-up tilt in the right lateral position on the systemic blood pressure after subarachnoid block for caesarean section. Anaesthesia 2002;57(2):169-72. [DOI] [PubMed] [Google Scholar]
Loo 2002 {published data only}
- Loo C, Qah T. Prophylactic intravenous ephedrine and spinal anaesthesia for cesarean section. Anesthesia & Analgesia 2002;94:S189. [PubMed] [Google Scholar]
Loughrey 2002 {published data only}
- Loughrey J, Walsh F, Gardiner J. Prophylactic intravenous bolus ephedrine in spinal anaesthesia for elective caesarian section [abstract]. British Journal of Anaesthesia 1997;78(Suppl 1):109. [DOI] [PubMed] [Google Scholar]
- Loughrey JPR, Walsh F, Gardiner J. Prophylactic intravenous bolus ephedrine for elective caesarean section under spinal anaesthesia. European Journal of Anaesthesiology 2002;19(1):63-8. [DOI] [PubMed] [Google Scholar]
Loughrey 2005 {published data only}
- Loughrey JPR, Yao N, Datta S, Segal S, Pian-Smith M, Tsen LC. Hemodynamic effects of spinal anesthesia and simultaneous intravenous bolus of combined phenylephrine and ephedrine versus ephedrine for cesarean delivery. International Journal of Obstetric Anesthesia 2005;14(1):43-7. [DOI] [PubMed] [Google Scholar]
Madi‐Jebara 2008 {published data only}
- Madi-Jebara S, Ghosn A, Sleilaty G, Richa F, Cherfane A, Haddad F, et al. Prevention of hypotension after spinal anesthesia for cesarean section: 6% hydroxyethyl starch 130/0.4 (Voluven) versus lactated ringer's solution. Lebanese Medical Journal 2008;56(4):203-7. [PubMed] [Google Scholar]
- Madi-Jebara SN, Ghosn A, Cherfane A, Antakly MC, Yazigi A. Prevention of hypotension after spinal anesthesia for cesarean section: Voluven* (6% hydroxyethyl starch 130/0.4) versus lactated ringer's solution [abstract]. Anesthesiology 2004;101(Suppl):A1197. [PubMed] [Google Scholar]
Magalhaes 2009 {published data only}
- Magalhaes E, Goveia CS, Araujo Ladeira LC, Nascimento BG, Kluthcouski SM. Ephedrine versus phenylephrine: prevention of hypotension during spinal block for cesarean section and effects on the fetus. Revista Brasileira de Anestesiologia 2009;59(1):15-20. [DOI] [PubMed] [Google Scholar]
Marciniak 2013 {published data only}
- Marciniak A, Wujtewicz M, Owczuk R. The impact of colloid infusion prior to spinal anaesthesia for caesarean section on the condition of a newborn--a comparison of balanced and unbalanced hydroxyethyl starch 130/0.4. Anestezjologia Intensywna Terapia 2013;45(1):14-9. [DOI] [PubMed] [Google Scholar]
Marciniak 2015 {published data only}
- Marciniak A, Owczuk R, Wujtewicz M, Preis K, Majdylo K. The influence of intravenous ondansetron on maternal blood haemodynamics after spinal anaesthesia for caesarean section: a double-blind, placebo-controlled study. Ginekologia Polska 2015;86(6):461-7. [DOI] [PubMed] [Google Scholar]
Mathru 1980 {published data only}
- Mathru M, Rao TLK, Kartha RK, Shanmugham M, Jacobs HK. Intravenous albumin administration for prevention of spinal hypotension during cesarean section. Anesthesia & Analgesia 1980;59(9):655-8. [PubMed] [Google Scholar]
Mercier 2014 {published data only}
- Mercier FJ, Diemunsch P, Ducloy-Bouthors AS, Mignon A, Fischler M, Malinovsky JM, et al. 6% Hydroxyethyl starch (130/0.4) vs Ringer's lactate preloading before spinal anaesthesia for caesarean delivery: the randomized, double-blind, multicentre CAESAR trial. British Journal of Anaesthesia 2014;113(3):459-67. [DOI] [PubMed] [Google Scholar]
Miyabe 1997 {published data only}
- Miyabe M, Sato S. The effect of head-down tilt position on arterial blood pressure after spinal anesthesia for cesarean delivery. Regional Anesthesia 1997;22(3):239-42. [DOI] [PubMed] [Google Scholar]
Mohta 2010 {published data only}
- Mohta M, Janani SS, Sethi AK, Agarwal D, Tyagi A. Comparison of phenylephrine hydrochloride and mephentermine sulphate for prevention of post spinal hypotension. Anaesthesia 2010;65:1200-5. [DOI] [PubMed] [Google Scholar]
Morgan 2000 {published data only}
- Morgan D, Philip J, Sharma S, Gottumukkala V, Perez B, Wiley J. A neonatal outcome with ephedrine infusions with or without preloading during spinal anesthesia for cesarean section. Anesthesiology 2000;92(Suppl):A5. [Google Scholar]
Moslemi 2015 {published data only}
- Moslemi F, Rasooli S. Comparison of prophylactic infusion of phenylephrine with ephedrine for prevention of hypotension in elective cesarean section under spinal anesthesia: a randomized clinical trial. Iranian Journal of Medical Sciences 2015;40(1):19-26. [PMC free article] [PubMed] [Google Scholar]
Muzlifah 2009 {published data only}
- Muzlifah KB, Choy YC. Comparison between preloading with 10 ml/kg and 20 ml/kg of Ringer's lactate in preventing hypotension during spinal anaesthesia for caesarean section. Medical Journal of Malaysia 2009;64(2):114-7. [PubMed] [Google Scholar]
Nazir 2012 {published data only}
- Nazir I, Bhat MA, Qazi S, Buchh VN, Gurcoo SA. Comparison between phenylephrine and ephedrine in preventing hypotension during spinal anesthesia for cesarean section. Journal of Obstetric Anaesthesia and Child Care 2012;21(2):92-7. [Google Scholar]
Ngan Kee 2000 {published data only}
- Ngan Kee W, Khaw K, Lee BB, Lau TK. Prophylactic intravenous ephedrine during spinal anaesthesia for caesarean section [abstract]. Anaesthesia and Intensive Care 2000;28(1):107. [Google Scholar]
- Ngan Kee WD, Shaw KS, Lee BB, Lau TK, Gin T. A dose-response study of prophylactic intravenous ephedrine for the prevention of hypotension during spinal anesthesia for cesarean delivery. Anesthesia & Analgesia 2000;90(6):1390-5. [DOI] [PubMed] [Google Scholar]
Ngan Kee 2004a {published data only}
- Ngan Kee WD, Khaw KS, Ng FF, Lee BB. Prophylactic phenylephrine infusion for preventing hypotension during spinal anesthesia for cesarean delivery. Anesthesia & Analgesia 2004;98(3):815-21. [DOI] [PubMed] [Google Scholar]
Ngan Kee 2013a {published data only}
- Ngan Kee WD, Lee SW, Khaw KS, Ng FF. Haemodynamic effects of glycopyrrolate pre-treatment before phenylephrine infusion during spinal anaesthesia for caesarean delivery. International Journal of Obstetric Anesthesia 2013;22(3):179-87. [DOI] [PubMed] [Google Scholar]
Nishikawa 2007 {published data only}
- Nishikawa K, Yokoyama N, Saito S, Goto F. Comparison of effects of rapid colloid loading before and after spinal anesthesia on maternal hemodynamics and neonatal outcomes in cesarean section. Journal of Clinical Monitoring and Computing 2007;21(2):125-9. [DOI] [PubMed] [Google Scholar]
Nivatpumin 2016 {published data only}
- Nivatpumin P, Thamvittayakul V. Ephedrine versus ondansetron in the prevention of hypotension during cesarean delivery: a randomized, double-blind, placebo-controlled trial. International Journal of Obstetric Anaesthesia 2016;27:25-31. [DOI] [PubMed] [Google Scholar]
Oh 2014 {published data only}
- Oh AY, Hwang JW, Song IA, Kim MH, Ryu JH, Park HP, et al. Influence of the timing of administration of crystalloid on maternal hypotension during spinal anesthesia for cesarean delivery: preload versus coload. BMC Anesthesiology 2014;14:36. [DOI] [PMC free article] [PubMed] [Google Scholar]
Olsen 1994 {published data only}
- Olsen KS, Feilberg VL, Hansen CL, Rudkjobing O, Pedersen T, Kyst A. Prevention of hypotension during spinal anaesthesia for caesarean section. International Journal of Obstetric Anesthesia 1994;3:20-4. [DOI] [PubMed] [Google Scholar]
Ortiz‐Gomez 2014 {published data only}
- Ortiz-Gomez JR, Palacio-Abizanda FJ, Morillas-Ramirez F, Fornet-Ruiz I, Lorenzo-Jimenez A, Bermejo-Albares ML. The effect of intravenous ondansetron on maternal haemodynamics during elective caesarean delivery under spinal anaesthesia: a double-blind, randomised, placebo-controlled trial. International Journal of Obstetric Anesthesia 2014;23(2):138-43. [DOI] [PubMed] [Google Scholar]
Ouerghi 2010 {published data only}
- Ouerghi S, Bougacha MA, Frikha N, Mestiri T, Ben Ammar MS, Mebazaa MS. Combined use of crystalloid preload and low dose spinal anesthesia for preventing hypotension in spinal anesthesia for cesarean delivery: a randomized controlled trial. Middle East Journal of Anesthesiology 2010; 20(5):667-72. [PubMed] [Google Scholar]
Ozkan 2004 {published data only}
- Ozkan T, Eker A, Karadeniz M, Haker N, Korap N, Tugrul M. Maternal and neonatal effects of different fluid and ephedrine combinations for prehydration before spinal anesthesia for cesarean section [abstract]. Regional Anesthesia and Pain Medicine 2004;29(Suppl 2):16. [Google Scholar]
Perumal 2004 {published data only}
- Perumal T, Fernando R, Bray J, Coloumb M. Maternal hemodynamic parameters after crystalloid vs colloid preloading for cesarean section under spinal anesthesia: a supra sternal doppler comparison [abstract]. Anesthesiology 2004;101 Suppl:A1233. [Google Scholar]
Pouliou 2006 {published data only}
- Pouliou A, Kiskia O, Kolotoura A, Hapsa H, Andreotti B, Emexidis TH. Prevention of hypotension caused during spinal anaesthesia for caesarean section. Intramuscular or intravenous ephedrine [abstract]. Regional Anesthesia and Pain Management 2006;31(5 Suppl 1):17. [Google Scholar]
Pouta 1996 {published data only}
- Pouta AM, Karinen J, Vuolteenaho OJ, Laatikainen TJ. Effect of intravenous fluid preload on vasoactive peptide secretion during caesarean section under spinal anaesthesia. Anaesthesia 1996;51:128-32. [DOI] [PubMed] [Google Scholar]
Ramin 1994 {published data only}
- Ramin SM, Ramin KD, Cox K, Magness RR, Shearer VE, Gant NF. Comparison of prophylactic angiotensin II versus ephedrine infusion for prevention of maternal hypotension during spinal anesthesia. American Journal of Obstetrics and Gynecology 1994;171(3):734-9. [DOI] [PubMed] [Google Scholar]
Rees 2002 {published data only}
- Rees SG, Thurlow JA, Gardner IC, Scrutton MJ, Kinsella SM. Comparison of true 15 degree table tilt vs full lateral position after induction of spinal anesthesia for cesarean section [abstract]. Anesthesiology 2001;94(1A):A82. [Google Scholar]
- Rees SGO, Thurlow JA, Gardner IC, Scrutton MJL, Kinsella SM. Comparison of true 15 degree table tilt vs. full lateral position after induction of spinal anaesthesia for caesarean section. International Journal of Obstetric Anesthesia 2001;10:210. [Google Scholar]
- Rees SGO, Thurlow JA, Gardner IC, Scrutton MJL, Kinsella SM. Maternal cardiovascular consequences of positioning after spinal anaesthesia for caesarean section: left 15 degree table tilt vs. left lateral. Anaesthesia 2002;57(1):15-20. [DOI] [PubMed] [Google Scholar]
Riley 1995 {published data only}
- Riley ET, Cohen SE, Rubenstein AJ, Flanagan B. Prevention of hypotension after spinal anesthesia for cesarean section: six percent hetastarch versus lactated Ringer's solution. Anesthesia & Analgesia 1995;81(4):838-42. [DOI] [PubMed] [Google Scholar]
Romdhani 2014 {published data only}
- Romdhani C, Trabelsi W, Lebbi A, Naas I, Elaskri H, Gharsallah H, et al. Lower incidence of hypotension following spinal anesthesia with 6% hydroxyethyl starch preload compared to 9% saline solution in caesarean delivery [Incidence de l'hypotension apres une anesthesie rachidienne avec 6% d'amidon hydroxyethyle compare au serum sale a 9% dans les cesariennes]. Tunisie Medicale 2014;92(6):406-10. [PubMed] [Google Scholar]
Rout 1992 {published data only}
- Rout CC, Akoojee SS, Rocke DA, Gouws E. Rapid administration of crystalloid preload does not decrease the incidence of hypotension after spinal anaesthesia for elective caesarean section. British Journal of Anaesthesia 1992;68:394-7. [DOI] [PubMed] [Google Scholar]
Rout 1993a {published data only}
- Rout CC, Rocke DA, Gouws E. Leg elevation and wrapping in the prevention of hypotension following spinal anaesthesia for elective caesarean section. Anaesthesia 1993;48(4):304-8. [DOI] [PubMed] [Google Scholar]
Sahoo 2012 {published data only}
- Sahoo T, SenDasgupta C, Goswami A, Hazra A. Reduction in spinal-induced hypotension with ondansetron in parturients undergoing caesarean section: a double-blind randomised, placebo-controlled study. International Journal of Obstetric Anesthesia 2012;21(1):24-8. [DOI] [PubMed] [Google Scholar]
Selvan 2004 {published data only}
- Selvan T, Fernando R, Bray J, Sodhi M, Columb M. Suprasternal Doppler estimation of cardiac output following intravenous fluid preloading for caesarean section under spinal anaesthesia. International Journal of Obstetric Anesthesia 2004;13(3):S8. [Google Scholar]
Siddik 2000 {published data only}
- Siddik SM, Aouad MT, Kai GE, Sfeir MM, Baraka AS. Hydroxyethylstarch 10% is superior to ringer's solution for preloading before spinal anesthesia for cesarean section. Canadian Journal of Anaesthesia 2000;47(7):616-21. [DOI] [PubMed] [Google Scholar]
Siddik‐Sayyid 2009 {published data only}
- Siddik-Sayyid SM, Nasr VG, Taha SK, Zbeide RA, Shehade JM, Al Alami AA, et al. A randomized trial comparing colloid preload to coload during spinal anesthesia for elective cesarean delivery. Anesthesia & Analgesia 2009;109(4):1219-24. [DOI] [PubMed]
- Siddik-Sayyid SM, Zbeidy RA. Colloid prehydration versus colloid cohydration during spinal anesthesia for cesarean delivery. Anesthesiology 2008;109:A1128. [Google Scholar]
Singh 2009 {published data only}
- Singh U, Saha U. Prevention of hypotension following spinal anaesthesia for caesarean section-comparison of volume preloading with ringer lactate & 6% hydroxyethyl starch (HES 130/0.4). Journal of Anaesthesiology Clinical Pharmacology 2009;25(1):54-8. [Google Scholar]
Singh 2014 {published data only}
- Singh K, Payal YS, Sharma JP, Nautiyal R. Evaluation of hemodynamic changes after leg wrapping in elective cesarean section under spinal anesthesia. Journal of Obstetric Anaesthesia and Critical Care 2014;4(1):23-8. [Google Scholar]
Singh 2016 {published data only}
- Singh TH, Thokchom RS, Sinam M, Nongthonbam R, Devi MB, Singh KM. Prophylactic intravenous ephedrine for prevention of hypotension in cesarean section during spinal anesthesia: a comparative study. JMS - Journal of Medical Society 2016;30(2):116-20. [Google Scholar]
Sood 1996 {published data only}
- Sood PK, Cooper PJF, Michel MZ, Wee MYK, Pickering RM. Thromboembolic deterrent stockings fail to prevent hypotension associated with spinal anaesthesia for elective caesarean section. International Journal of Obstetric Anesthesia 1996;5(3):172-5. [DOI] [PubMed] [Google Scholar]
- Sood PK, Cooper PJF, Michel MZ, Wee MYK. Do TED (thrombo-embolic deterrent) stockings prevent or attenuate hypotension of spinal anaesthesia for elective caesarean section? International Journal of Obstetric Anesthesia 1994;3:177-8. [DOI] [PubMed] [Google Scholar]
Stein 1997 {published data only}
- Stein DJ, Birnbach DJ, Danzer BI, Kuroda MM, Grunebaum A, Thys DM. Acupressure versus intravenous metoclopramide to prevent nausea and vomiting during spinal anaesthesia for cesarean section. Anesthesia & Analgesia 1997;84:342-5. [DOI] [PubMed] [Google Scholar]
Sujata 2012 {published data only}
- Panigrahi BP, Namiath S, Arora D, Das S. Use of a sequential compression mechanical device to prevent spinal hypotension in elective cesarean section. In: American Society of Anesthesiologists (ASA) 2011 Annual Meeting; 2011 October 15-19; Illinois, Chicago. 2011.
- Sujata N, Arora D, Panigrahi BP, Hanjoora VM. A sequential compression mechanical pump to prevent hypotension during elective cesarean section under spinal anesthesia. International Journal of Obstetric Anesthesia 2012;21(2):140-5. [DOI] [PubMed] [Google Scholar]
Sutherland 2001 {published data only}
- Sutherland PD, Wee MYK, Weston-Smith P, Skinner T, Thomas P. The use of TED stockings and sequential compression device to prevent spinal hypotension during caesarean section [abstract]. International Journal of Obstetric Anesthesia 1999;8:193. [DOI] [PubMed] [Google Scholar]
- Sutherland PD, Wee MYK, Weston-Smith P, Skinner T, Thomas P. The use of thromboembolic deterrent stockings and a sequential compression device to prevent spinal hypotension during caesarean section. International Journal of Obstetric Anesthesia 2001;10(2):97-102. [DOI] [PubMed] [Google Scholar]
Tawfik 2014 {published data only}
- Tawfik MM, Hayes SM, Jacoub FY, Badran BA, Gohar FM, Shabana AM, et al. Comparison between colloid preload and crystalloid co-load in cesarean section under spinal anesthesia: a randomized controlled trial. International Journal of Obstetric Anesthesia 2014;23(4):317-23. [DOI] [PubMed] [Google Scholar]
Tercanli 2005 {published data only}
- Tercanli S, Schneider M, Visca E, Hosli I, Troeger C, Peukert R, et al. Influence of volume preloading on uteroplacental and fetal circulation during spinal anaesthesia for caesarean section in uncomplicated singleton pregnancies. Fetal Diagnosis and Therapy 2002;17(3):142-6. [DOI] [PubMed] [Google Scholar]
Terkawi 2015 {published data only}
- Terkawi AS, Mehta SH, Hackworth JH, Tiouririne M. Ondansetron dose not attenuates hypotension in patients undergoing elective cesarean delivery under spinal anesthesia: a double-blinded, placebo-controlled randomized trial. Anesthesia & Analgesia 2014;118(Suppl 1):S-194. [Google Scholar]
- Terkawi AS, Tiouririne M, Mehta SH, Hackworth JM, Tsang S, Durieux ME. Ondansetron does not attenuate hemodynamic changes in patients undergoing elective cesarean delivery using subarachnoid anesthesia. A double blind, placebo-controlled, randomized trial. Regional Anesthesia and Pain Medicine 2015;40(4):344-8. [DOI] [PubMed] [Google Scholar]
Torres unpub {unpublished data only}
- Torres D. Untitled manuscript (as supplied prior to 18 July 2017). Data on file .
Trabelsi 2015 {published data only}
- Trabelsi W, Romdhani C, Elaskri H, Sammoud W, Bensalah M, Labbene I, et al. Effect of ondansetron on the occurrence of hypotension and on neonatal parameters during spinal anesthesia for elective caesarean section: a prospective, randomized, controlled, double-blind study. Anesthesiology Research and Practice 2015;2015:158061. [DOI] [PMC free article] [PubMed] [Google Scholar]
Tsen 2000 {published data only}
- Tsen LC, Boosalis P, Segal S, Datta S, Bader A. Hemodynamic effects of simultaneous administration of intravenous ephedrine and spinal anesthesia for cesarean delivery. Journal of Clinical Anesthesia 2000;12:378-82. [DOI] [PubMed] [Google Scholar]
Turkoz 2002 {published data only}
- Turkoz A, Togal T, Gokdeniz R, Toprak H, Ersoy O. Effectiveness of intravenous ephedrine infusion during spinal anaesthesia for cesarean section based in maternal hypotension, neonatal acid base status and lactate levels. Anaesthesia and Intensive Care 2002;30(3):316-20. [DOI] [PubMed] [Google Scholar]
- Turkoz A, Togal T, Toprak HI, Gokdeniz R, Pelik F, Ersoy O. Prophylactic intravenous ephedrine during spinal anaesthesia for cesarean section. British Journal of Anaesthesia 1999;82 Suppl:161. [Google Scholar]
Ueyama 1992 {published data only}
- Ueyama H, Tanigami H, Nishimua M, Tashiro C. Prophylactic intravenous administration for cesarean section during spinal anesthesia in laboring and nonlaboring patients [abstract]. Anesthesiology 1992;77(3A):A975. [Google Scholar]
Ueyama 1999 {published data only}
- Ueyama H, He YL, Tanigami H, Mashimo T, Yoshiya I. Effects of crystalloid and colloid preload on blood volume in the parturient undergoing spinal anesthesia for elective cesarean section. Anesthesiology 1999;91:1571-6. [DOI] [PubMed] [Google Scholar]
Ueyama 2002 {published data only}
- Ueyama H, Hiuge Y, Takashina M, Mashimo T. Maternal cardiovascular effects of prophylactic ephedrine and phenylephrine for elective caesarean section undergoing spinal anaesthesia. Anesthesiology 2002;96 Suppl:A1051. [Google Scholar]
Unlugenc 2015 {published data only}
- Unlugenc H, Turktan M, Evruke IC, Gunduz M, Burgut R, Yapicioglu-Yildizdas H, et al. Rapid fluid administration and the incidence of hypotension induced by spinal anesthesia and ephedrine requirement: the effect of crystalloid versus colloid coloading. Middle East Journal of Anaesthesiology 2015;23(3):273-81. [PubMed] [Google Scholar]
Upadya 2016 {published data only}
- Upadya M, Bhat S, Paul S. Six percent hetastarch versus lactated ringer's solution - for preloading before spinal anesthesia for cesarean section. Anesthesia, Essays and Researches 2016;10(1):33-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ure 1999 {published data only}
- Ure D, James KS, McNeill M, Booth JV. Glycopyrrolate reduces nausea during spinal anaesthesia for caesarean section without affecting neonatal outcome. British Journal of Anaesthesia 1999;82(2):277-9. [DOI] [PubMed] [Google Scholar]
Wang 2014a {published data only}
- Wang M, Zhuo L, Wang Q, Shen MK, Yu YY, Yu JJ, et al. Efficacy of prophylactic intravenous ondansetron on the prevention of hypotension during cesarean delivery: a dose-dependent study. International Journal of Clinical and Experimental Medicine 2014;7(12):5210-6. [PMC free article] [PubMed] [Google Scholar]
Wang 2014b {published data only}
- Wang Q, Zhuo L, Shen MK, Yu YY, Yu JJ, Wang M. Ondansetron preloading with crystalloid infusion reduces maternal hypotension during cesarean delivery. American Journal of Perinatology 2014;31(10):913-21. [DOI] [PubMed] [Google Scholar]
Webb 1998 {published data only}
- Webb AA, Shipton EA. Re-evaluation of i.m. ephedrine as prophylaxis against hypotension associated with spinal anaesthesia for caesarean section. Canadian Journal of Anaesthesia 1998;45(4):367-9. [DOI] [PubMed] [Google Scholar]
Wilson 1998 {published data only}
- Wilson DJ, Heid R, Douglas MJ, Rurak DW. The effects of preoperative glucose administration on spinal-induced hypotension in elective C/S delivery. Anesthesiology 1998;88(4 Suppl):A12. [Google Scholar]
- Wilson DJ, Heid R, Douglas MJ, Rurak DW. The effects of preoperative glucose administration on spinal-induced hypotension in elective C/S delivery. Canadian Journal of Anaesthesia 1998;45(5 Pt 2):A61. [Google Scholar]
Wilson 1999 {published data only}
- Wilson D, Douglas J, Heid R, Rurak D. Preoperative dextrose does not affect spinal-induced hypotension in elective cesarean section. Canadian Journal of Anaesthesia 1999;46(11):1024-9. [DOI] [PubMed] [Google Scholar]
Yokoyama 1997 {published data only}
- Yokoyama H, Kubota N, Toda K. Continuous infusion of dopamine to maintain stable arterial pressure during spinal anaesthesia for caesarean section. European Journal of Anaesthesiology 1997;14:72-3. [Google Scholar]
Yorozu 2002 {published data only}
- Yorozu T, Morisaki H, Kondoh M, Zenfuku M, Shigematsu T. Comparative effect of 6% hydroxyethyl starch (containing 1% dextrose) and lactated Ringer's solution for cesarean section under spinal anesthesia. Journal of Anesthesia 2002;16(3):203-6. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Adekanye 2007 {published data only}
- Adekanye O, Sivasankar R, Collis RE. Hypotension following low-dose combined spinal-epidural anaesthesia for caesarean section: left lateral versus supine tilted position [abstract]. International Journal of Obstetric Anesthesia 2007;16(Suppl 1):S9. [Google Scholar]
Adigun 2010 {published data only}
- Adigun TA, Amanor-Boadu SD, Soyannwo OA. Comparison of intravenous ephedrine with phenylephrine for the maintenance of arterial blood pressure during elective caesarean section under spinal anaesthesia. African Journal of Medicine and Medical Sciences 2010;39(1):13-20. [PubMed] [Google Scholar]
Akhtar 2011 {published data only}
- Akhtar FM, Kazi WA, Rizvi A, Mushtaq R, Alia A. Prevention of hypotension in caesarean delivery under spinal anaesthesia; new modified supine wedged position. Anaesthesia, Pain and Intensive Care 2011;15(2 Suppl 1):157. [Google Scholar]
Alahuhta 1994 {published data only}
- Alahuhta S, Karinen J, Lummet R, Jouppila R, Hollmen AI, Jouppila P. Uteroplacental haemodynamics during spinal anaesthesia for caesarean section with two types of uterine displacement. International Journal of Obstetric Anesthesia 1994;3(4):187-92. [DOI] [PubMed] [Google Scholar]
Amponsah 2011 {published data only}
- Amponsah AP, Cohen S, Lasalle S, Shah S, Daley W. Can hypotension from intrathecal ropivacaine for cesarean section (C/S) be prevented with 6% hetastarch more effectively than prophylactic IV ephedrine? Regional Anesthesia and Pain Medicine 2011;36(5):510. [Google Scholar]
Aragao 2014 {published data only}
- Aragao FF, Aragao PW, Martins CA, Salgado Filho N, Barroqueiro Ede S. Comparison of metaraminol, phenylephrine and ephedrine in prophylaxis and treatment of hypotension in cesarean section under spinal anesthesia. Revista Brasileira de Anestesiologia 2014;64(5):299-306. [DOI] [PubMed] [Google Scholar]
Arai 2008 {published data only}
- Arai YC, Kato N, Matsura M, Ito H, Kandatsu N, Kurokawa S, et al. Transcutaneous electrical nerve stimulation at the PC-5 and PC-6 acupoints reduced the severity of hypotension after spinal anaesthesia in patients undergoing caesarean section. British Journal of Anaesthesia 2008;100(1):78-81. [DOI] [PubMed] [Google Scholar]
Arboleda 2012 {published data only}
- Arboleda DPB, Ruiz NJF, Mejia GAM, Garcia NIS, Penuela EJG. Etilefrine vs phenylephrine for hypotension during spinal anesthesia for cesarean section: clinical trial controlled multicenter randomized, double blind. In: Society for Obstetric Anesthesia and Perinatology (SOAP) 44th Annual Meeting; 2015 May 2-5; Monterey, USA. 2012:TW-2.
Armstrong 2010 {published data only}
- Armstrong SL, Fernando R, Jones TL, Columb M. Positioning for obstetric anaesthesia and its effects on maternal cardiac output and fetal wellbeing. International Journal of Obstetric Anesthesia 2010;19(Suppl 1):S10. [Google Scholar]
Ashpole 2005 {published data only}
- Ashpole K, Fernando R, Tamilselvan P, Columb M. Maternal cardiac output changes with phenylephrine and ephedrine infusions after spinal anaesthesia for elective caesarean section. International Journal of Obstetric Anesthesia 2005;14(Suppl 1):S5. [Google Scholar]
- Ashpole KJ, Tamilselvan P, Fernando R, Columb M. Maternal cardiac output changes occurring with phenylephrine and ephedrine infusions after spinal anesthesia for elective cesarean section. Anesthesiology 2005;102(Suppl 1):9. [Google Scholar]
Atalay 2010 {published data only}
- Atalay C, Aksoy M, Aksoy AN, Dogan N, Kursad H. Combining intrathecal bupivacaine and meperidine during caesarean section to prevent spinal anaesthesia-induced hypotension and other side-effects. Journal of International Medical Research 2010;38(5):1626-36. [DOI] [PubMed] [Google Scholar]
Atashkhoyi 2012 {published data only}
- Atashkhoyi S, Fardiazar Z, Hatami MP, Torab R. Comparison the effect of ephedrine and phenylephrine in treatment of hypotension after spinal anesthesia during cesarean section. Open Journal of Obstetrics and Gynecology 2012;2:192-6. [Google Scholar]
Ayorinde 2001 {published data only}
- Ayorinde B, Brown J, Buczkowski P, Shah J, Buggy DJ. Prevention of spinal anaesthesia-induced hypotension during caesarian section: comparative study of pre-emptive vasopressors. British Journal of Anaesthesia 2000;84:277P-278P. [DOI] [PubMed] [Google Scholar]
- Ayorinde BT, Buczkowski P, Brown J, Shah J, Buggy DJ. Evaluation of pre-emptive intramuscular phenylephrine and ephedrine for reduction of spinal anaesthesia-induced hypotension during caesarean section. British Journal of Anaesthesia 2001;86(3):372-6. [DOI] [PubMed] [Google Scholar]
- Heidemann BH, Clark VA. Use of pre-emptive vasopressors for spinal anaesthesia-induced hypotension during caesarean section. British Journal of Anaesthesia 2001;87(2):320-1. [PubMed] [Google Scholar]
Aziz 2013 {published data only}
- Aziz N, Bangash R, Khan P. Comparison between ephedrine and phenylephrine in the prevention of post spinal hypotension during elective cesarean section. Journal of Medical Sciences (Peshawar) 2013;21(1):27-30. [Google Scholar]
Bach 2002 {published data only}
- Bach PS, Kamani A, Douglas J, Esler M, Gunka V. Incidence of hypotension after spinal for cesarean section. Canadian Journal of Anaesthesia 2002;49(6 Suppl):A55. [Google Scholar]
- Bach PS, Kamani A, Douglas J, Gunka V, Esler M. The impact of a tightly controlled trial on the incidence of hypotension after spinal for cesarean section [abstract]. Anesthesiology 2002;96:A1029. [Google Scholar]
- Bach PS, Kamani AA, Douglas JM, Gunka V, Esler M. The importance of methodological variables in the study of hypotension after spinal anesthesia for cesarean section: pentastarch vs. normal saline. Anesthesiology 2002;96(Suppl 1):GM-6. [Google Scholar]
Balcan 2011 {published data only}
- Balcan A, Cindea I, Gherghina V, Nicolae G. Spinal anaesthesia for caesarean section: Comparison of maternal and neonatal effects of bolus administration of ephedrine and phenylephrine. European Journal of Anaesthesiology 2011;28 Suppl:160. [Google Scholar]
Basuni 2016 {published data only}
- Basuni AS. Addition of low-dose ketamine to midazolam and low-dose bupivacaine improves hemodynamics and postoperative analgesia during spinal anesthesia for cesarean section. Journal of Anaesthesiology Clinical Pharmacology 2016;32(1):44-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Belzarena 2006 {published data only}
- Belzarena SD. Ephedrine and etilefrine as vasopressor to correct maternal arterial hypotension during elective cesarean section under spinal anesthesia. Comparative study [Estudo comparativo entre efedrina e etilefrina como vasopressor para correcao da hipotensao arterial materna em cesarianas eletivas com raquianestesia]. Revista Brasileira de Anestesiologia 2006;56(3):223-9. [DOI] [PubMed] [Google Scholar]
Benhamou 1998 {published data only}
- Benhamou D, Thorin D, Brichant J-F, Dailland P, Milon D, Schneider M. Intrathecal clonidine and fentanyl with hyperbaric bupivacaine improves analgesia during cesarean section. Anesthesia & Analgesia 1998;87(3):609-13. [DOI] [PubMed] [Google Scholar]
Bhar 2011 {published data only}
- Bhar D, Bharati S, Halder PS, Mondal S, Sarkar M, Jana S. Efficacy of prophylactic intramuscular ephedrine in prevention of hypotension during caesarean section under spinal anaesthesia: a comparative study. Journal of the Indian Medical Association 2011;109(5):300-3, 307. [PubMed] [Google Scholar]
Bhattarai 2010 {published data only}
- Bhattarai B, Bhat SY, Upadya M. Comparsion of bolus phenylephrine, ephedrine and mephentermine for maintenance of arterial pressure during spinal anesthesia in cesarean section. Journal of Nepal Medical Association 2010;49(177):23-8. [PubMed] [Google Scholar]
Bjornestad 2009 {published data only}
Borgia 2002 {published data only}
- Borgia ML, Pinto R, Meloncelli S, Ferri F, Berritta C, Panella I, et al. Influence of the position during combined spinal-epidural anesthesia for caesarean section delivery [Effetti della posizione materna durante l'induzione di anestesia subarachnoidea - epidurale combinata nel parto cesareo]. Acta Anaesthesiologica Italica 2002;52:143-8. [Google Scholar]
Bouchnak 2006 {published data only}
- Bouchnak M, Belhadj N, Chaaoua T, Azaiez W, Hamdi M, Maghrebi H. Spinal anaesthesia for caesarean section: does injection speed have an effect on the incidence of hypotension? [Rachianesthesie pour cesarienne: la vitesse d'injection a-t-elle une influence sur l'incidence de l'hypotension?]. Annales Francaises d Anesthesie et de Reanimation 2006;25(1):17-9. [DOI] [PubMed] [Google Scholar]
Bouslama 2012 {published data only}
- Bouslama MA, Ghaddab A, Khouadja H, Beji T, Tarmiz K, Ben Jazia K. No benefice of low-dose bupivacaine (7.5mg) in spinal anaesthesia for caesarean delivery to prevent hypotension. European Journal of Anaesthesiology 2012;29:168. [Google Scholar]
Bryson 2007 {published data only}
- Bryson GL, MacNeil R, Jeyaraj LM, Rosaeg OP. Small dose spinal bupivacaine for cesarean delivery does not reduce hypotension but accelerates motor recovery. Canadian Journal of Anaesthesia 2007;54(7):531-7. [DOI] [PubMed] [Google Scholar]
Butwick 2007 {published data only}
- Butwick A, Carvalho B. Effects of crystalloid and colloid preloads on coagulation assessed by thromboelastography in parturients prior to elective cesarean section [abstract]. International Journal of Obstetric Anesthesia 2006;15 Suppl 1:S4. [Google Scholar]
- Butwick A, Carvalho B. The effect of colloid and crystalloid preloading on thromboelastography prior to cesarean delivery. Canadian Journal of Anaesthesia 2007;54(3):190-5. [DOI] [PubMed] [Google Scholar]
- Butwick AJ, Starre P, Carvalho B. Effects of crystalloid and colloid preloads on coagulation assessed by thromboelastography in parturients prior to elective cesarean section [abstract]. Anesthesiology 2006;104(Suppl 1):9. [Google Scholar]
Cai 2016 {published data only}
- Cai YX, Zeng K, Ni J, Huang W. [The effect of different positions on block plane of isobaric bupivacaine for caesarean section with combined spinal-eqidural analgesia]. Journal of Sichuan University. Medical Science Edition 2016;47(2):283-6. [PubMed] [Google Scholar]
Campbell 1993 {published data only}
- Campbell DC, Douglas J, Pavy TJG, Merrick P, Flanagan ML, McMorland GH. Comparison of the 25-gauge Whitacre with 24-gauge Sprotte spinal needle for elective caesarean section: cost implications. Canadian Journal of Anaesthesia 1993;40(12):1131-5. [DOI] [PubMed] [Google Scholar]
Cardoso 2004b {published data only}
- Cardoso MMSC, Santos MM, Yamaguchi ET, Hirahara JT, Amaro AR. Fluid preload in obstetric patients. How to do it? Revista Brasileira de Anestesiologia 2004;54(1):13-9. [DOI] [PubMed] [Google Scholar]
Cardoso 2005 {published data only}
- Cardoso MM, Yamaguchi ET, Amaro AR, Mezzetti R, Torres MA. Fetal and maternal effects of bolus of phenylephrine or metaraminol during spinal anesthesia for cesarean delivery [abstract]. Anesthesiology 2005;102(Suppl 1):31. [Google Scholar]
Carvalho 2015 {published data only}
- Carvalho B, Mangum K, Wang R, Drover D. Ondansetron does not prevent spinal hypotension but reduces total vasopressor requirements in women undergoing caesarean delivery. In: Society for Obstetric Anesthesia and Perinatology (SOAP) 47th Annual Meeting; 2015 May 13-17; Colorado, USA. 2015:T-10.
Cesur 2008 {published data only}
- Cesur M, Alici HA, Erdem AF, Borekci B, Silbir F. Spinal anesthesia with sequential administration of plain and hyperbaric bupivacaine provides satisfactory analgesia with hemodynamic stability in cesarean section. International Journal of Obstetric Anesthesia 2008;17(3):217-22. [DOI] [PubMed] [Google Scholar]
Chanimov 2006 {published data only}
- Chanimov M, Gershfeld S, Cohen ML, Sherman D, Bahar M. Fluid preload before spinal anaesthesia in caesarean section: the effect on neonatal acid-base status. European Journal of Anaesthesiology 2006;23(8):676-9. [DOI] [PubMed] [Google Scholar]
Choi 2005 {published data only}
- Choi DH, Ko JS, Cho CH. Prevention of hypotension with crystalloid versus colloid dural spinal or low-dose combined spinal-epidural anesthesia for cesarean delivery [abstract]. Regional Anesthesia and Pain Medicine 2005;30(5 Suppl 1):74. [Google Scholar]
- Kim CS, Ahn HJ, Shin SH, Choi DH. Prevention of hypotension with crystalloid versus colloid during spinal or combined spinal-epidural anesthesia for cesarean delivery. Korean Journal of Anesthesiology 2004;46(4):408-13. [Google Scholar]
Chung 1996 {published data only}
- Chung CJ, Bae SH, Chae KY, Chin YJ. Spinal anaesthesia with 0.25% hyperbaric bupivacaine for caesarean section: effects of volume. British Journal of Anaesthesia 1996;77(2):145-9. [DOI] [PubMed] [Google Scholar]
Clark 1980 {published data only}
- Clark RB, Brunner JA. Dopamine for the treatment of spinal hypotension during caesarean section. Anesthesiology 1980;53(6):514-7. [DOI] [PubMed] [Google Scholar]
Cohen 2002 {published data only}
- Cohen S, Denenberg H, Alptekin B, Ginsberg S, Bokhari F, Burley E, et al. Is 6% hetastarch preferred over prophylactic IV ephedrine for prevention of hypotension from intrathecal ropivacaine for C/S? Anesthesiology 2002;96 Suppl 1:Abstract no: P-88. [Google Scholar]
Cooper 2002 {published data only}
- Cooper DW, Carpenter M, Mowbray P, Desira W, Ryall DM, Kokri MS. Fetal and maternal effects of phenylephrine and ephedrine during spinal anesthesia for cesarean delivery. Anesthesiology 2002;97(6):1582-90. [DOI] [PubMed] [Google Scholar]
- Cooper DW, Schofield L. Is a relatively high pre-spinal heart rate associated with reduced efficacy of prophylactic vasopressor during spinal anaesthesia for caesarean section? International Journal of Obstetric Anesthesia 2011;20(3):268-9. [DOI] [PubMed] [Google Scholar]
Cooper 2004 {published data only}
- Cooper DW, Jeyaraj L, Hynd R, Thompson R, Meek T, Ryall D, et al. Intravenous vasopressors can affect rostral spread of spinal anaesthesia in pregnancy. International Journal of Obstetric Anesthesia 2004;13(3):S5. [DOI] [PubMed] [Google Scholar]
- Cooper DW, Jeyaraj L, Hynd R, Thompson R, Meek T, Ryall DM, et al. Evidence that intravenous vasopressors can affect rostral spread of spinal anesthesia in pregnancy. Anesthesiology 2004;101(1):28-33. [DOI] [PubMed] [Google Scholar]
Cooper 2007 {published data only}
- Cooper DW, Gibb SC, Meek T, Owen S, Kokri MS, Malik AT, et al. Effect of intravenous vasopressor on spread of spinal anaesthesia and fetal acid-base equilibrium. British Journal of Anaesthesia 2007;98(5):649-56. [DOI] [PubMed] [Google Scholar]
- Cooper DW, Gibb SC, Meek T, Owen S, Kokri MS, Malik AT, et al. Effect of intravenous vasopressor on spread of spinal anaesthesia for caesarean section and fetal acid-base equilibrium. Anaesthesia 2008;63:902. [DOI] [PubMed] [Google Scholar]
Coppejans 2006 {published data only}
- Coppejans HC, Hendrickx E, Goossens J, Vercauteren MP. The sitting versus right lateral position during combined spinal-epidural anesthesia for cesarean delivery: block characteristics and severity of hypotension. Anesthesia & Analgesia 2006;102(1):243-7. [DOI] [PubMed] [Google Scholar]
Das 2011 {published data only}
- Das S, Mukhopadhyay S, Mandal M, Mandal S, Basu SR. A comparative study of infusions of phenylephrine, ephedrine and phenylephrine plus ephedrine on maternal haemodynamics in elective caesarean section. Indian Journal of Anaesthesia 2011;55(6):578-83. [DOI] [PMC free article] [PubMed] [Google Scholar]
Datta 1982 {published data only}
- Datta S, Alper MH, Ostheimer GW, Weiss JB. Method of ephedrine administration and nausea and hypotension during spinal anesthesia for cesarean section. Anesthesiology 1982;56(1):68-70. [DOI] [PubMed] [Google Scholar]
Davemski 2007 {published data only}
- Davemski V, Davemska G, Krivasija M, Nojkov O, Sivevski A. Cesarean section in isobaric spinal anesthesia with and without direct preoperative hydration with crystalloids - a comparative clinical study. Anaesthesiology and Intensive Care 2007;34(2):3-8. [Google Scholar]
Defossez 2007 {published data only}
- Defossez T, Lauwers M, Camu F. A comparison of ephedrine and phenylephrine boluses versus continuous infusion of ephedrine and phenylephrine during spinal anaesthesia for caesarean delivery. Acta Anaesthesiologica Belgica 2007;58(1):66. [Google Scholar]
Desalu 2005 {published data only}
- Desalu I, Kushimo OT. Is ephedrine infusion more effective at preventing hypotension than traditional prehydration during spinal anaesthesia for caesarean section in African parturients? International Journal of Obstetric Anesthesia 2005;14:294-9. [DOI] [PubMed] [Google Scholar]
Doherty 2011 {published data only}
- Doherty A, Ohashi Y, Downey K, Carvalho JC. Hemodynamic changes during spinal anaesthesia assessed with non-invasive bioreactance: a randomized controlled trial of bolus and infusion regimens of phenylephrine to prevent hypotension. Canadian Journal of Anesthesia 2011;58(Suppl 1):S62. [Google Scholar]
Dua 2013 {published data only}
- Dua M, Sharma R, Jain R. Comparative evaluation of phenylephrine and ephedrine for treatment of spinal-induced hypotension in caesarean section. Journal of Obstetric Anaesthesia and Critical Care 2013;3(1):54. [Google Scholar]
Dyer 2009 {published data only}
El‐Hakeem 2011 {published data only}
- El-Hakeem EE, Kaki AM, Almazrooa AA, Al-Mansouri NM, Alhashemi JA. Effects of sitting up for five minutes versus immediately lying down after spinal anesthesia for Cesarean delivery on fluid and ephedrine requirement; a randomized trial. Canadian Journal of Anaesthesia 2011;58(12):1083-9. [DOI] [PubMed] [Google Scholar]
Evron 2007 {published data only}
- Evron S, Gorodinsky L, Sadan O, Golan A, Ezri. Hemodynamic effects of preventive administration of ephedrine and phenylephrine during combined spinal-epidural anesthesia for cesarean delivery. American Journal of Obstetrics and Gynecology 2007;197(6 Suppl 1):S113, Abstract no: 370. [Google Scholar]
Fabrizi 1998 {published data only}
- Fabrizi A, Crochetiere CT, Roy L, Villeneuve E, Lortie L. Prevention of side-effects during caesarean (sic) section under spinal anaesthesia. Canadian Journal of Anaesthesia 1998;45(5 Pt 2):A62. [Google Scholar]
- Fabrizi A, Crochetiere CT, Roy L, Villeneuve E, Lortie L. Prevention of side-effects during cesarean section under spinal anesthesia. Regional Anesthesia 1998;23(3):44. [Google Scholar]
Farber 2015 {published data only}
- Farber MK, Schultz R, Lugo L, Liu X, Huang C, Tsen LC. The effect of co-administration of intravenous calcium chloride and oxytocin on maternal hemodynamics and uterine tone following cesarean delivery: a double-blinded, randomized, placebo-controlled trial. International Journal of Obstetric Anesthesia 2015;24(3):217-24. [DOI] [PubMed]
Forkner 2012 {published data only}
- Forkner IF, Lazar O, Gershon RY, Lynde GC. Compression stockings: Does placement immediately prior to spinal administration reduce hypotension? In: Society for Obstetric Anesthesia and Perinatology (SOAP) 44th Annual Meeting; 2015 May 2-5; Monterey, USA. 2012:S-45.
Foss 2014 {published data only}
- Foss VT, Christensen R, Rokamp KZ, Nissen P, Secher NH, Nielsen HB. Effect of phenylephrine vs. ephedrine on frontal lobe oxygenation during caesarean section with spinal anesthesia: an open label randomized controlled trial. Frontiers in Physiology 2014;5(81):1-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Frikha 2008 {published data only}
- Frikha N, Ouerghi S, Mestiri T, Mebazaa MS, Ammar MSB. Volume preload in prevention of hypotension during spinal anaesthesia for elective caesarean section. Anesthesiology 2008;109:A1328. [Google Scholar]
Frolich 2001 {published data only}
- Froelich MA. Atrial natriuretic peptide (ANP) and hydration prior to spinal anesthesia (SA) for cesarean section (CS). Anesthesiology 2000;92 Suppl:A8. [Google Scholar]
- Frolich MA. Role of the atrial natriuretic factor in obstetric spinal hypotension. Anesthesiology 2001;95(2):371-6. [DOI] [PubMed] [Google Scholar]
Fuzier 2005 {published data only}
- Fuzier R, Decramer I, Fuzier V, Desprats R, Samli K. Is the combination ephedrine-phenylephrine useful for the treatment of established hypotension after spinal anesthesia for cesarean section? [abstract]. Regional Anesthesia and Pain Medicine 2005;30(5 Suppl 1):76. [Google Scholar]
Gallo 1996 {published data only}
- Gallo F, Alberti A, Fongaro A, Negri MG, Carlot A, Altafina L, Valenti S. Spinal anesthesia for cesarian (sic) section: 1% versus 0.5% hyperbaric bupivacaine [Anestesia spinale nel taglio cesareo: confronto tra bupivacaina iperbarica all'1% ed allo 0,5%]. Minerva Anestesiologica 1996;62(1-2):9-15. [PubMed] [Google Scholar]
Gambling 2015 {published data only}
- Gambling DR, Bender M, Faron S, Glaser D, Farrell TR. Prophylactic intravenous ephedrine to minimize fetal bradycardia after combined spinal-epidural labour analgesia: a randomized controlled study. Canadian Journal of Anaesthesia 2015;62(11):1201-8. [DOI] [PubMed] [Google Scholar]
Garrison 2005 {published data only}
- Garrison R, Wiley J, Philip J, Sharma S. Prevention of hypotension following spinal anesthesia for caesarean section using noninvasive transthoracic electrical impedance cardiography [abstract]. Anesthesiology 2005;102(Suppl 1):8. [Google Scholar]
George 2015 {published data only}
- George RB, McKeen DM, Allen TK, Polin CM, Habib AS. A double blind randomized controlled trial of a prophylactic phenylephrine infusion versus bolus phenylephrine for the treatment of spinal induced hypotension in obese parturients. In: Society for Obstetric Anesthesia and Perinatology (SOAP) 47th Annual Meeting; 2015 May 13-17; Colorado, USA. 2015:T-64.
Goudie 1988 {published data only}
- Goudie TA, Winter AW, Ferguson DJM. Lower limb compression using inflatable splints to prevent hypotension during spinal anaesthesia for caesarean section. Acta Anaesthesiologica Scandinavica 1988;32(7):541-4. [DOI] [PubMed] [Google Scholar]
Guasch 2010 {published data only}
- Guasch E, Gilsanz F, Diez J, Alsina E. Maternal hypotension with low doses of spinal bupivacaine or levobupivacaine and epidural volume expansion with saline for cesarean section. Revista Española de Anestesiología y Reanimación 2010;57(5):267-74. [DOI] [PubMed] [Google Scholar]
Guillon 2010 {published data only}
- Guillon A, Leyre S, Remerand F, Taihlan B, Perrotin F, Fusciardi J, et al. Modification of Tp-e and QTc intervals during caesarean section under spinal anaesthesia. Anaesthesia 2010;65(4):337-42. [DOI] [PubMed] [Google Scholar]
Gulec 2012 {published data only}
- Gulec H, Degerli S, Ozayar E, Bercin F, Sahin S. The effects of 7 mg levobupivacaine on maternal hemodynamics with side effects in combined spinal-epidural anaesthesia for cesarean section. Anaesthesia, Pain and Intensive Care 2012;16(2):127-30. [Google Scholar]
Gulhas 2013 {published data only}
- Gulhas N, Tekdemir D, Durmus M, Yucel A, Erdil FA, Yologlu S, et al. The effects of ephedrine on maternal hypothermia in caesarean sections: a double blind randomized clinical trial. European Review for Medical and Pharmacological Sciences 2013;17(15):2051-8. [PubMed] [Google Scholar]
Gunda 2010 {published data only}
- Gunda CP, Malinowski J, Tegginmath A, Suryanarayana VG, Chandra SBC. Vasopressor choice for hypotension in elective Cesarean section: ephedrine or phenylephrine? Archives of Medical Science 2010;6(2):257-63. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gupta 2012 {published data only}
- Gupta S, Naithani U, Sinha N, Doshi V, Surendran K, Bedi V. Comparison of hydroxyethyl starch versus normal saline for epidural volume extension in combined spinal anesthesia for cesarean section. Journal of Obstetric Anaesthesia and Critical Care 2012;2(1):16-22. [Google Scholar]
Gutsche 1976 {published data only}
- Gutsche BB. Prophylactic ephedrine preceding spinal analgesia for cesarean section. Anesthesiology 1976;45(4):462-5. [DOI] [PubMed] [Google Scholar]
Hahn 1998 {published data only}
- Hahn RG, Resby M. Volume kinetics of Ringer's solution and dextran 3% during induction of spinal anaesthesia for caesarean section. Canadian Journal of Anaesthesia 1998;45(5):443-51. [DOI] [PubMed] [Google Scholar]
Hamzei 2015 {published data only}
- Hamzei A, Nazemi SH, Alami A, Gochan ADM, Kazemi A. Comparing different epinephrine concentrations for spinal anesthesia in cesarean section: a double-blind randomized clinical trial. Iranian Journal of Medical Sciences 2015;40:302-8. [PMC free article] [PubMed]
Hanss 2006 {published data only}
- Hanss R, Bein B, Francksen H, Scherkl W, Bauer M, Doerges V, et al. Heart rate variability-guided prophylactic treatment of severe hypotension after subarachnoid block for elective cesarean delivery. Anesthesiology 2006;104(4):635-43. [DOI] [PubMed] [Google Scholar]
Haruta 1987 {published data only}
- Haruta M, Funato T, Saeki N, Naka Y, Shinkai T. Ephedrine administration for cesarean section under spinal anesthesia. Acta Obstetrica et Gynaecologica Japonica 1987;39(2):207-14. [PubMed] [Google Scholar]
Hennebry 2009 {published data only}
- Hennebry MC, Stocks GM, Belavadi P, Barnes J, Wray S, Columb MO, et al. Effect of i.v. phenylephrine or ephedrine on the ED50 of intrathecal bupivacaine with fentanyl for caesarean section. British Journal of Anaesthesia 2009;102(6):806-11. [DOI] [PubMed] [Google Scholar]
Higgins 2015 {published data only}
- Higgins N, McCarthy RJ, Wong CW. Phenylephrine versus ephedrine for the management of spinal anesthesia-induced hypotension in preeclamptic patients during cesarean delivery. In: Society for Obstetric Anesthesia and Perinatology (SOAP) 47th Annual Meeting; 2015 May 13-17; Colorado, USA. 2015:O2-03.
- NCT00458003. Phenylephrine in spinal anesthesia in preeclamptic patients [Phenylephrine versus ephedrine to treat spinal anesthesia-induced hypotension in preeclamptic patients during cesarean delivery]. clinicaltrials.gov/show/NCT00458003 (first received 4 April 2007).
Housni 2004 {published data only}
- Housni B, Miguil M. Hypotension during spinal anaesthesia for caesarean section: comparison of two rates of injection [Hypotension arterielle au cours de rachianesthesie pour cesarienne: comparaison de deux vitesses d'injection]. Cahiers D'Anesthesiologie 2004;52(5):345-8. [Google Scholar]
Husaini 1998 {published data only}
- Husaini SW, Russell IF. Volume preload: lack of effect in the prevention of spinal-induced hypotension at caesarean section. International Journal of Obstetric Anesthesia 1998;7:76-81. [DOI] [PubMed] [Google Scholar]
Iwama 2002 {published data only}
- Iwama H, Ohmizo H, Furuta S, Ohmori S, Watanabe K, Kaneko T. Spinal anesthesia hypotension in elective cesarean section in parturients wearing extra-strong compression stockings. Archives of Gynecology and Obstetrics 2002;267(2):85-9. [DOI] [PubMed] [Google Scholar]
Jackson 1995 {published data only}
- Jackson R, Reid JA, Thorburn J. Volume preloading is not essential to prevent spinal-induced hypotension at caesarean section. British Journal of Anaesthesia 1995;75(3):262-5. [DOI] [PubMed] [Google Scholar]
- Reid JA, Jackson R, Thorburn J. Volume preloading is not essential to prevent spinal induced hypotension at caesarean section. International Journal of Obstetric Anesthesia 1995;4:63. [DOI] [PubMed] [Google Scholar]
Jain 2008 {published data only}
- Jain K, Bharadwaj N. Fetal and maternal outcome after control of maternal blood pressure during cesarean section under spinal anaesthesia: comparison of three vasopressors. Regional Anesthesia and Pain Medicine 2008;33(5 Suppl 1):130. [Google Scholar]
James 1996 {published data only}
- James KS, Stott SM, McGrady EM, Pearsall FJ, Frame WT, Russell D. Spinal anaesthesia for Caesarean section: effect of Sprotte needle orientation. British Journal of Anaesthesia 1996;77(2):150-2. [DOI] [PubMed] [Google Scholar]
Javed 2014 {published data only}
- Javed K, Ishrat Z, Akhtar N, Ijaz B. Comparative study of intrathecal 0.5% isobaric versus 0.5% hyperbaric bupivacaine in same volume and dose to assess the quality of spinal anaesthesia and haemodynamic changes occurring during cesarean section. Pakistan Journal of Medical and Health Sciences 2014;8(2):407-10. [Google Scholar]
John 2013 {published data only}
- John JR. A prospective study comparing preemptive intramuscular ephedrine versus intravenous ephedrine to prevent hypotension during spinal anaesthesia for caesarean delivery. Journal of Obstetric Anaesthesia and Critical care 2013;3(2):119. [Google Scholar]
Kamrul 2012 {published data only}
- Kamrul Hasan ABM, Kulkarni AH, Durairajan S, Lim KH, Latif Z, Kaul HL. Prevention of oxytocin induced hypotension in caesarean delivery by co-administration of phenylephrine. International Journal of Obstetric Anesthesia 2012;21:S19. [Google Scholar]
Kang 1982 {published data only}
- Kang YG, Abouleish E, Caritis S. Prophylactic intravenous ephedrine infusion during spinal anesthesia for cesarean section. Anesthesia & Analgesia 1982;61:839-42. [PubMed] [Google Scholar]
Kang 1996 {published data only}
- Kang YS, Kim YM, Jeon TW, Cho KH. The effect of crystalloid administration on blood pressure and heart rate change during epidural anesthesia in cesarean section. Korean Journal of Anesthesiology 1996;31(6):706-12. [Google Scholar]
Kangas‐Saarela 1990 {published data only}
- Kangas-Saarela T, Hollmen AI, Tolonen U, Eskelinen P, Alahuhta S, Jouppila R, et al. Does ephedrine influence newborn neurobehavioural responses and spectral EEG when used to prevent maternal hypotension during caesarean section? Acta Anaesthesiologica Scandinavica 1990;34(1):8-16. [DOI] [PubMed] [Google Scholar]
Kansal 2005 {published data only}
- Kansal A, Mohta M, Sethi AK, Tyagi A, Kumar P. Randomised trial of intravenous infusion of ephedrine or mephentermine for management of hypotension during spinal anaesthesia for caesarean section. Anaesthesia 2005;60(1):28-34. [DOI] [PubMed] [Google Scholar]
Kaya 2007 {published data only}
- Kaya S, Karaman H, Erdogan H, Akyilmaz A, Turhanoglu S. Combined use of low-dose bupivacaine, colloid preload and wrapping of the legs for preventing hypotension in spinal anaesthesia for caesarean section. Journal of International Medical Research 2007;35(5):615-25. [DOI] [PubMed] [Google Scholar]
Keera 2016 {published data only}
- Keera AAI, Elnabtity AMA. Two syringe spinal anesthesia technique for cesarean section: a controlled randomized study of a simple way to achieve more satisfactory block and less hypotension. Anesthesia, Essays and Researches 2016;10(2):312-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kinsella 2012 {published data only}
- Kinsella SM, Harvey NL. A comparison of the pelvic angle applied using lateral table tilt or a pelvic wedge at elective caesarean section. Anaesthesia 2012;67(12):1327-31. [DOI] [PubMed] [Google Scholar]
Ko 2007 {published data only}
- Ko JS, Kim CS, Cho HS, Choi DH. A randomized trial of crystalloid versus colloid solution for prevention of hypotension during spinal or low-dose combined spinal-epidural anesthesia for elective cesarean delivery. International Journal of Obstetric Anesthesia 2007;16(1):8-12. [DOI] [PubMed] [Google Scholar]
Kumar 2013 {published data only}
- Kumar R. Comparison of intravenous phenylephrine with intravenous mephentermine for management of post spinal hypotension in caesarean section and effects on neonate. Journal of Obstetric Anaesthesia and Critical Care 2013;3(1):57. [Google Scholar]
Kutlesic 2012 {published data only}
- Kutlesic M, Kutlesic R. The impact of the type of anaesthesia on neonatal acid-base status. Regional Anesthesia and Pain Medicine 2012;37(5 Suppl 1):E277. [Google Scholar]
Lal 2015 {published data only}
- Lal SK. Comparison of phenylephrine versus ephedrine for management of hypotension during spinal anaesthesia for elective caesarean section. Indian Journal of Public Health Research and Development 2015;6(1):34-9. [Google Scholar]
Langesaeter 2008 {published data only}
- Langesaeter E, Rosseland LA, Stubhaug A. Continuous invasive blood pressure and cardiac output monitoring during cesarean delivery: a randomized, double-blind comparison of low-dose versus high-dose spinal anesthesia with intravenous phenylephrine or placebo infusion. Anesthesiology 2008;109(5):856-63. [DOI] [PubMed] [Google Scholar]
- NCT00199784. Hemodynamic measurements during cesarean section with spinal anesthesia. clinicaltrials.gov/show/NCT00199784 (first received 13 September 2005).
LaPorta 1995 {published data only}
- LaPorta RF, Arthur GR, Datta S. Phenylephrine in treating maternal hypotension due to spinal anaesthesia for caesarean delivery: effects on neonatal catecholamine concentrations, acid base status and Apgar scores. Acta Anaesthesiologica Scandinavica 1995;39(7):901-5. [DOI] [PubMed] [Google Scholar]
Law 2003 {published data only}
- Law AC, Lam KK, Irwin MG. The effect of right versus left lateral decubitus positions on induction of spinal anesthesia for cesarean delivery. Anesthesia & Analgesia 2003;97(6):1795-9. [DOI] [PubMed] [Google Scholar]
Lee 2005 {published data only}
- Lee SJ, Ok SY, Lee JS, Kim SI. The effect of fluid preloading and ephedrine administration for prevention of hypotension during spinal anesthesia for cesarean delivery. Korean Journal of Anesthesiology 2005;49(2):199-205. [Google Scholar]
Lee 2008 {published data only}
- Lee SY, Choi DH, Park HW. The effect of colloid co-hydration on the use of phenylephrine and hemodynamics during low-dose combined spinal-epidural anesthesia for cesarean delivery. Korean Journal of Anesthesiology 2008;55:685-90. [Google Scholar]
Lee 2012 {published data only}
- Lee SW, Khaw KS, Ngan Kee WD, Leung TY, Critchley LA. Haemodynamic effects from aortocaval compression at different angles of lateral tilt in non-labouring term pregnant women. British Journal of Anaesthesia 2012;109(6):950-6. [DOI] [PubMed] [Google Scholar]
Lee 2015 {published data only}
- Lee MH, Kim EM, Bae JH, Park SH, Chung MH, Choi YR, et al. Head elevation in spinal-epidural anesthesia provides improved hemodynamics and appropriate sensory block height at caesarean section. Yonsei Medical Journal 2015;56(4):1122-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lee 2016 {published data only}
- Lee HM, Kim SH, Hwang BY, Suh DG, Koh WU, Jang DM, et al. The effects of prophylactic bolus phenylephrine on hypotension during low-dose spinal anesthesia for cesarean section. International Journal of Obstetric Anesthesia 2016;25:17-22. [DOI] [PubMed] [Google Scholar]
Lewis 2004 {published data only}
- Lewis NL, Downer JP, Ritchie EL, Nel MR. Left lateral versus supine wedged position for onset of spinal block, following combined spinal-epidural anesthesia for caesarean section. International Journal of Obstetric Anesthesia 2002;11 Suppl:2. [Google Scholar]
- Lewis NL, Ritchie EL, Downer JP, Nel MR. Left lateral vs. supine, wedged position for development of block after combined spinal-epidural anaesthesia for caesarean section. Anaesthesia 2004;59(9):894-8. [DOI] [PubMed] [Google Scholar]
Liu 2010 {published data only}
- Liu F. The effects of colloid and crystalloid solution for volume preloading on maternal hemodynamics. Guizhou Medical Journal 2010;34(9):791-3. [PubMed] [Google Scholar]
Luo 2016 {published data only}
- Luo XJ, Zheng M, Tian G, Zhong HY, Zou XJ, Jian DL. Comparison of the treatment effects of methoxamine and combining methoxamine with atropine infusion to maintain blood pressure during spinal anesthesia for cesarean delivery: a double blind randomized trial. European Review for Medical and Pharmacological Sciences 2016;20(3):561-7. [PubMed] [Google Scholar]
Madi‐Jebara 2007 {published data only}
- Madi-Jebara S, Ghosn A, Karim N, Yazigi A, Yazbeck P. Hypotension after spinal anesthesia for cesarean section: effects of lactated ringer's cohydration. Anesthesiology 2007;107:Abstract no: A676. [Google Scholar]
Mahajan 2009 {published data only}
- Mahajan L, Anand LK, Gombar KK. A randomized double-blinded comparison of ephedrine, phenylephrine and mephentermine infusions to maintain blood pressure during spinal anaesthesia for cesarean delivery: the effects on fetal acid-base status and haemodynamic control. Journal of Anaesthesiology Clinical Pharmacology 2009;25(4):427-32. [Google Scholar]
Matorras 1998 {published data only}
- Matorras R, Tacuri C, Anibal N, Gutierrez de Teran G, Cortes J. Lack of benefits of left tilt in emergent cesarean sections: a randomized study of cardiotocography, cord acid-base status and other parameters of the mother and the fetus. Journal of Perinatal Medicine 1998;26(4):284-92. [DOI] [PubMed] [Google Scholar]
Matsota 2013 {published data only}
- Matsota P, Karakosta A, Pandazi A, Niokou D, Christodoulaki K, Kostopanagiotou G. The effect of 6% hydroxyethyl starch 130/0.42 vs lactated Ringer's preload on the haemodynamic status of parturients undergoing spinal anaesthesia for elective caesarean delivery using arterial pulse contour analysis. European Journal of Anaesthesiology 2013;30:166. [DOI] [PubMed] [Google Scholar]
Matsota 2015 {published data only}
- Matsota P, Karakosta A, Pandazi A, Niokou D, Christodoulaki K, Kostopanagiotou G. The effect of 0.5 L 6% hydroxyethyl starch 130/0.42 versus 1 L Ringer's lactate preload on the hemodynamic status of parturients undergoing spinal anesthesia for elective cesarean delivery using arterial pulse contour analysis. Journal of Anesthesia 2015;29(3):352-9. [DOI] [PubMed] [Google Scholar]
McDonald 2011 {published data only}
- McDonald S, Fernando R, Ashpole K, Columb M. Maternal cardiac output changes after crystalloid or colloid cohydration following spinal anaesthesia for elective caesarean section [abstract]. International Journal of Obstetric Anesthesia 2007;16(Suppl 1):S8. [Google Scholar]
- McDonald S, Fernando R, Ashpole K, Columb M. Maternal cardiac output changes after crystalloid or colloid coload following spinal anesthesia for elective cesarean delivery: a randomized controlled trial. Anesthesia Analgesia 2011;113(4):803-10. [DOI] [PubMed] [Google Scholar]
- McDonald S, Fernando R, Ashpole K, Columb M. Maternal cardiac output changes following crystalloid or colloid cohydration with spinal anesthesia for elective cesarean section [abstract]. Anesthesiology 2007;106(Suppl 1):50. [Google Scholar]
McLeod 2010 {published data only}
- McLeod G, Munishankar B, MacGregor H, Murphy DJ. Maternal haemodynamics at elective caesarean section: a randomised comparison of oxytocin 5-unit bolus and placebo infusion with oxytocin 5-unit bolus and 30-unit infusion. International Journal of Obstetric Anesthesia 2010;19(2):155-60. [DOI] [PubMed] [Google Scholar]
Mebazaa 2010 {published data only}
- Mebazaa MS, Ouerghi S, Ben Meftah R, Ben Cheikh M, Mestiri T, Ben Ammar MS. Reduction of bupivacaine dose in spinal anaesthesia for caesarean section may improve maternal satisfaction by reducing incidence of low blood pressure episodes. Middle East Journal of Anesthesiology 2010;20(5):673-8. [PubMed] [Google Scholar]
Mendonca 2003 {published data only}
- Mendona C, Griffiths J, Ateleanu B, Collis R. Hypotension after spinal anaesthesia for caesarean section: supine tilt v full lateral position. International Journal of Obstetric Anesthesia 2002;11 Suppl:19. [Google Scholar]
- Mendonca C, Griffiths J, Ateleanu B, Collis RE. Hypotension following combined spinal-epidural anaesthesia for caesarean section; left lateral position vs. supine position. Anaesthesia 2003;58(5):428-31. [DOI] [PubMed] [Google Scholar]
Mercier 2001 {published data only}
- Mercier FJ, Riley ET, Frederickson WL, Benhamou D, Cohen SE. Phenylephrine added to prophylactic ephedrine infusion during spinal anethesia for elective cesarean section. Anesthesiology 2000;93(3A):A1057. [DOI] [PubMed] [Google Scholar]
- Mercier FJ, Riley ET, Frederickson WL, Rodger-Christoph S, Benhamou D, Cohen SE. Phenylephrine added to prophylactic ephedrine infusion during spinal anesthesia for elective cesarean section. Anesthesiology 2001;95(3):668-74. [DOI] [PubMed] [Google Scholar]
Miller 2000 {published data only}
- Levin A, Datta S, Segal S. The effect of posture on hypotension after spinal anesthesia after cesarean section. Anesthesiology 1998;88(4 Suppl):A10. [Google Scholar]
- Miller A, Levin A, Datta S, Tsen L, Segal S. Effect of posture prior to spinal anesthesia for cesarean section on maternal angiotensin II, aldosterone, and blood pressure. Anesthesiology 2000;92 Suppl:A3. [Google Scholar]
Mitra 2014 {published data only}
- Mitra T, Das A, Majumdar S, Bhattacharyya T, Mandal RD, Hajra BK. Prevention of altered hemodynamics after spinal anesthesia: a comparison of volume preloading with tetrastarch, succinylated gelatin and ringer lactate solution for the patients undergoing lower segment caesarean section. Saudi Journal of Anaesthesia 2014;8(4):456-62. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
Mohta 2008 {published data only}
- Mohta M, Agarwal D, Gupta LK, Tyagi A, Gupta A, Sethi AK. Comparison of potency of ephedrine and mephentermine for prevention of post-spinal hypotension in caesarean section. Anaesthesia and Intensive Care 2008;36(3):360-4. [DOI] [PubMed] [Google Scholar]
Mohta 2015 {published data only}
- Mohta M, Harisinghani P, Sethi AK, Agarwal D. Effect of different phenylephrine bolus doses for treatment of hypotension during spinal anaesthesia in patients undergoing elective caesarean section. Anaesthesia and Intensive Care 2015;43(1):74-80. [DOI] [PubMed] [Google Scholar]
Mohta 2016 {published data only}
- Mohta M, Aggarwal M, Sethi AK, Harisinghani P, Guleria K. Randomized double-blind comparison of ephedrine and phenylephrine for management of post-spinal hypotension in potential fetal compromise. International Journal of Obstetric Anesthesia 2016;27:32-40. [DOI] [PubMed] [Google Scholar]
Moore 2000 {published data only}
- Moore B, McKeating MK. Slow administration of intrathecal anaesthetic for caesarean section reduces maternal hypotension [abstract]. Anaesthesia and Intensive Care 2000;28(2):215. [Google Scholar]
Moore 2014 {published data only}
- Moore A, Bourrassa-Blanchette S, El Mouallem E, Kaufman I, El-Bahrawy A, Li-Pi-Shan W, et al. The median effective seated time for hypotension induced by spinal anesthesia at Cesarean delivery with two doses of hyperbaric bupivacaine: a randomized up-down sequential allocation study. Canadian Journal of Anaesthesia 2014;61(10):916-21. [DOI] [PubMed] [Google Scholar]
Moran 1991 {published data only}
- Moran DH, Perillo M, LaPorta RF, Bader AM, Datta S. Phenylephrine in the prevention of hypotension following spinal anesthesia for cesarean delivery. Journal of Clinical Anesthesia 1991;3(4):301-5. [DOI] [PubMed] [Google Scholar]
Mowbray 2002 {published data only}
- Mowbray P, Cooper DW, Carpenter M, Ryall DM, Desira WR, Kokri MS. Phenylephrine, ephedrine and fetal acidosis at caesarean delivery under spinal anaesthesia. International Journal of Obstetric Anesthesia 2002;11 Suppl:1. [Google Scholar]
Narejo 2012 {published data only}
- Narejo AS, Memon GN, Wagan F, Wagan MA, Khawaja RA. A study to assess the quality of spinal anesthesia and to observe hemodynamic changes occuring during cesarean section with spinal anesthesia, comparing 0.5% isobaric bupivacaine and 0.75% hyperbaric bupivacaine in same volume and dose. Medical Channel 2012;18(1):58-62. [Google Scholar]
Nasir 2005 {published data only}
- Nasir KK, Shahid E, Shahani AS. Use of hyperbaric and isobaric bupivacaine in elective cesarean section: a comparison. Annals of Pakistan Institute of Medical Sciences 2005;1(1):40-4. [Google Scholar]
Negron 2010 {published data only}
- Negron M, Cohen S, Rianto A, Sylviana B, Patel P. Does the addition of phenylephrine to prophylactic IV ephedrine further reduce the incidence of hypotension from intrathecal ropivacaine for C/S. In: Society for Obstetric Anesthesia and Perinatology (SOAP) 42nd Annual Meeting; 2010 May 12-16; San Antonio, USA. 2010.
Ngan 2016 {published data only}
- Ngan Kee WD, Khaw KS, Tam YH, Ng FF, Lee SW. Performance of a closed-loop feedback computer-controlled infusion system for maintaining blood pressure during spinal anaesthesia for caesarean section: a randomized controlled comparison of norepinephrine versus phenylephrine. Journal of Clinical Monitoring and Computing 2016 [Epub ahead of print]. [DOI] [PubMed]
Ngan Kee 2001a {published data only}
- Ngan Kee WD, Khaw KS, Lee BB, Wong MM, Ng FF. Metaraminol infusion for maintenance of arterial blood pressure during spinal anesthesia for cesarean delivery: the effect of a crystalloid bolus. Anesthesia & Analgesia 2001;93(3):703-8. [DOI] [PubMed] [Google Scholar]
Ngan Kee 2001b {published data only}
- Ngan Kee WD, Lau TK, Khaw KS, Lee BB. Comparison of metaraminol and ephedrine infusions for maintaining arterial pressure during spinal anesthesia for elective cesarean section. Anesthesiology 2001;95(2):307-13. [DOI] [PubMed] [Google Scholar]
Ngan Kee 2001c {published data only}
- Ngan Kee W, Khaw K, Lee B, Wong M, Ng F. Randomized controlled study of colloid preload before spinal anaesthesia for caesarean section [abstract]. Anesthesiology 2001;95 Suppl:A1054. [DOI] [PubMed] [Google Scholar]
- Ngan Kee WD, Khaw KS, Lee BB, Ng FF, Wong MMS. Randomized controlled trial of colloid preload before spinal anaesthesia for caesarean section. British Journal of Anaesthesia 2001;87(5):772-4. [DOI] [PubMed] [Google Scholar]
Ngan Kee 2004b {published data only}
- Ngan Kee WD, Khaw KS, Ng FF. Comparison of phenylephrine infusion regimens for maintaining maternal blood pressure during spinal anaesthesia for caesarean section. British Journal of Anaesthesia 2004;92(4):469-74. [DOI] [PubMed] [Google Scholar]
Ngan Kee 2005 {published data only}
- Ngan Kee WD, Khaw KS, Ng FF. Prevention of hypotension during spinal anesthesia for cesarean delivery: an effective technique using combination phenylephrine infusion and crystalloid cohydration. Anesthesiology 2005;103:744-50. [DOI] [PubMed] [Google Scholar]
Ngan Kee 2008a {published data only}
- Ngan Kee WD, Lee A, Khaw KS, Ng FF, Karmakar MK, Gin T. A randomized double-blinded comparison of phenylephrine and ephedrine infusion combinations to maintain blood pressure during spinal anaesthesia for cesarean delivery: the effects on fetal acid-base status and hemodynamic control. Anesthesia & Analgesia 2008;107(4):1295-302. [DOI] [PubMed] [Google Scholar]
Ngan Kee 2008b {published data only}
- Ngan Kee WD, Khaw KS, Lau TK, Ng FF, Chui K, Ng KL. Randomised double-blinded comparison of phenylephrine vs ephedrine for maintaining blood pressure during spinal anaesthesia for non-elective caesarean section. Anaesthesia 2008;63(12):1319-26. [DOI] [PubMed] [Google Scholar]
Ngan Kee 2009 {published data only}
Ngan Kee 2011 {published data only}
- Ngan Kee WD, Khaw KS, Tam YH, Ng FF. Comparison of closed-loop feedback computer-controlled and manual-controlled phenylephrine infusions during spinal anaesthesia for caesarean section. International Journal of Obstetric Anesthesia 2011;20(Suppl 1):S17. [Google Scholar]
Ngan Kee 2013b {published data only}
- Ngan Kee WD, Khaw KS, Ng FF, Tam YH. Randomized comparison of closed-loop feedback computer-controlled with manual-controlled infusion of phenylephrine for maintaining arterial pressure during spinal anaesthesia for caesarean delivery. British Journal of Anaesthesia 2013;110(1):59-65. [DOI] [PubMed] [Google Scholar]
Ngan Kee 2015 {published data only}
- Ngan Kee WD, Lee SW, Ng FF, Tan PE, Khaw KS. Randomized double-blinded comparison of norepinephrine and phenylephrine for maintenance of blood pressure during spinal anesthesia for cesarean delivery. Anesthesiology 2015;122(4):736-45. [DOI] [PubMed] [Google Scholar]
- Ngan Kee WD, Lee SWY, Ng FF, Tan PE, Khaw KS. Randomized evaluative study of phenylephrine or norepinephrine for maintenance of blood pressure during spinal anaesthesia for caesarean delivery: the RESPOND study. International Journal of Obstetric Anesthesia 2014;23(Suppl 1):S10. [Google Scholar]
Nishikawa 2004 {published data only}
- Nishikawa K, Yakoyama N, Saito S, Goto F. Comparison of the effects of colloid and crystalloid solution for volume preloading on maternal hemodynamics and neonatal outcome in spinal anesthesia for caesarean section [abstract]. Anesthesiology 2004;101 Suppl:A1201. [PubMed] [Google Scholar]
Norris 1987 {published data only}
- Norris MC, Leighton BL, DeSimone CA, Goodman DA, Gorman RM. Influence of the choice of crystalloid solution on neonatal acid-base status at cesarean section [abstract]. Anesthesiology 1987;67(3A):A458. [Google Scholar]
Norris 1989 {published data only}
- Norris MC, Leighton BL, Desimone CA, Palmer CM. Does the choice of crystalloid affect maternal and neonatal glucose homeostasis at caesarean section? Anesthesia & Analgesia 1989;68:S212. [Google Scholar]
Nutangi 2013 {published data only}
- Nutangi V, Thatte WS, Velankar PM. Comparison of intravenous phenylephrine, ephedrine and mephentermine for management of post spinal hypotension in cases of cesarean section and effects of these drugs on neonates. Journal of Obstetric Anaesthesia and Critical Care 2013;3(2):115. [Google Scholar]
Nze 2003 {published data only}
- Nze PUN. Effect of pre-medication with atropine on the blood pressure of parturient undergoing caesarian section under spinal anaesthesia. Orient Journal of Medicine 2003;15(1&2):1-4. [Google Scholar]
Ocio 2013 {published data only}
- Ocio LP, Arevalo EG, Alsina E, Brogly N, Dominguez A, Gilsanz F. Can we get maternal hypotension "0" with low dose using a combined spinal epidural technique? A randomized controlled trial. In: Society for Obstetric Anesthesia and Perinatology (SOAP) 45th Annual Meeting; 2013 April 24-28; San Juan, Puerto Rico. 2013:Abstract no: F29.
Okutan 2006 {published data only}
- Okutan M, Kocamanoglu IS, Sener B, Karakaya D, Sarihasan B, Tur A. Prevention of hypotension related to spinal anaesthesia for cesarean section. Turk Anesteziyoloji ve Reanimasyon Dernegi Dergisi 2006;34(1):27-34. [Google Scholar]
Osseyran 2011 {published data only}
- Osseyran Samper F, Errando CL, Plaza Lloret M, Diaz Cambronero O, Garcia Gregorio N, Andres Ibanez J. Prophylaxis for hypotension during cesarean section under spinal anesthesia: a randomized trial comparing hydroxyethyl starch 130/0.4 to ephedrine [Prevencion de la hipotensión arterial en cesareas con antesia subaracnoidea. Estudio prospectivo, aleatorizado comparativo entre hidroxietilalmidon 130/0,4 y efedrina]. Revista Española de Anestesiología y Reanimación 2011;58(1):17-24. [DOI] [PubMed] [Google Scholar]
Park 1996 {published data only}
- Park GE, Hauch MA, Curlin F, Datta S, Bader AM. The effects of varying volumes of crystalloid administration before cesarean delivery on maternal hemodynamics and colloid osmotic pressure. Anesthesia & Analgesia 1996;83(2):299-303. [DOI] [PubMed] [Google Scholar]
Peng 2013 {published data only}
- Peng X, Liu H, Xi L, Wang H, Li R, Shuai B. Effects of colloid preload on placenta stereology and cord blood S100beta protein during cesarean section under spinal anesthesia. Journal of Southern Medical University 2013;33(2):161-5. [PubMed] [Google Scholar]
Pickford 2000 {published data only}
- Pickford A, Tucker V, Barnes N, Pilkington S, Eldridge J. The effect of position on haemodynamic stability during spinal anaesthesia. Anesthesiology 2000;92 Suppl:A10. [Google Scholar]
Prakash 2010 {published data only}
Quan 2013 {published data only}
- Quan Z, Tian M, Chi P, Cao Y, Li X, Peng K. Influence of phenylephrine or ephedrine on maternal hemodynamics upon umbilical cord clamping during cesarean delivery. International Journal of Clinical Pharmacology and Therapeutics 2013;51(11):888-94. [DOI] [PubMed] [Google Scholar]
Quan 2014 {published data only}
- Quan ZF, He HL, Tian M, Chi P, Li X. Influence of lateral decubitus positioning after combined use of hyperbaric and hypobaric ropivacaine on hemodynamic characteristics in spinal anesthesia for caesarean section. International Journal of Clinical and Experimental Medicine 2014;7(12):5669-74. [PMC free article] [PubMed] [Google Scholar]
Quan 2015 {published data only}
- Quan Z, Tian M, Chi P, Li X, He H, Luo C. Combined use of hyperbaric and hypobaric ropivacaine significantly improves hemodynamic characteristics in spinal anesthesia for caesarean section: a prospective, double-blind, randomized, controlled study. Plos One 2015;10(5):e0125014. [DOI] [PMC free article] [PubMed] [Google Scholar]
Quan 2016 {published data only}
- Quan Z-F, Li X, Tian M, Chi P, He H, Luo C. Combined use of hyperbaric and hypobaric ropivacaine for caesarean section: A prospective, double-blind, randomized, controlled study. International Journal of Clinical and Experimental Medicine 2016;9(4):7438-44. [Google Scholar]
Quiney 1995 {published data only}
- Quiney NF, Murphy PG. The effect of pretreatment with glycopyrrolate on emetic and hypotensive problems during caesarean section conducted under spinal anaesthesia. International Journal of Obstetric Anesthesia 1995;4(1):66-7. [Google Scholar]
Rashad 2013 {published data only}
- Rashad MM, Farmawy MS. Effects of intravenous ondansetron and granisetron on hemodynamic changes and motor and sensory blockade induced by spinal anesthesia in parturients undergoing cesarean section. Egyptian Journal of Anaesthesia 2013;29:369-74. [Google Scholar]
Reed 2006 {published data only}
- Reed L, Garrison R, Sharma S. A combination of phenylephrine and ephedrine infusion maintains systematic vascular resistance and prevents post-spinal hypotension in cesarean delivery [abstract]. Anesthesiology 2006;104(Suppl 1):40. [Google Scholar]
Rehman 2011 {published data only}
- Rehman A, Baig H, Rajput MZ, Zeb H. Comparison of prophylactic ephedrine vs prn ephedrine during spinal anesthesia for caesarian sections. Anaesthesia, Pain and Intensive Care 2011;15(1):21-4. [Google Scholar]
Rewari 2015 {published data only}
- Rewari V, Singhal D, Ramachandran R, Trikha A, Chandralekha, Singh N. Crystalloid versus colloid coload with phenylephrine infusion during spinal anaesthesia for elective caesarean delivery: the effects on maternal haemodynamics and foetal acid-base status. Anesthesia & Analgesia 2015;120(3 Suppl 1):S197. [Google Scholar]
Ronenson 2014 {published data only}
- Ronenson AM, Sitkin SI, Savel'eva IuV. Effecting of intra-abdominal pressure in parturient on level of spina block and frequency of hypotension during cesarean section. Anesteziologiia I Reanimatologiia 2014;59(4):26-9. [PubMed] [Google Scholar]
Rout 1993b {published data only}
- Rout CC, Rocke DA, Levin J, Gouws E, Reddy D. A reevaluation of the role of crystalloid preload in the prevention of hypotension associated with spinal anesthesia for elective cesarean section. Anesthesiology 1993;79(2):262-9. [DOI] [PubMed] [Google Scholar]
Rout 2000 {published data only}
- Rout CC, Rocke DA, Stienstra R. Hypotension and postural haemodynamic changes following caesarean section. Effects of glycopyrrolate 0.4mg iv with spinal anaesthesia. Anesthesiology 2000;92 Suppl:A71. [Google Scholar]
Rucklidge 2002 {published and unpublished data}
- Rucklidge M, Durbridge J, Barnes PK, Yentis SM. Glycopyrronium for prevention of hypotension following CSE for elective caesarean section. International Journal of Obstetric Anesthesia 2001;10:225. [Google Scholar]
- Rucklidge MWN, Durbridge J, Barnes PK, Yentis SM. Glycopyrronium and hypotension following combined spinal-epidural anaesthesia for elective caesarean section in women with relative bradycardia. Anaesthesia 2002;57(1):4-8. [DOI] [PubMed] [Google Scholar]
Rucklidge 2005 {published data only}
- Rucklidge MWM, Paech MJ, Lain J, Evans S, Yentis SM. A comparison of lateral, sitting and Oxford positions for CSE anaesthesia for elective caesarean section [abstract]. International Journal of Obstetric Anesthesia 2003;12:194. [Google Scholar]
- Rucklidge MWM, Paech MJ, Yentis SM. A comparison of the lateral, Oxford and sitting positions for performing combined spinal-epidural anaesthesia for elective caesarean section. Anaesthesia 2005;60(6):535-40. [DOI] [PubMed] [Google Scholar]
Rumboll 2015 {published data only}
- Rumboll CK, Dyer RA, Lombard CJ. The use of phenylephrine to obtund oxytocin-induced hypotension and tachycardia during caesarean section. International Journal of Obstetric Anesthesia 2015;24(4):297-302. [DOI] [PubMed] [Google Scholar]
Russell 2002 {published data only}
- Russell R, Popat M, Richards E, Burry J. Combined spinal epidural anaesthesia for caesarean section: a randomised comparison of Oxford, lateral and sitting positions. International Journal of Obstetric Anesthesia 2002;11:190-5. [DOI] [PubMed] [Google Scholar]
Sahin 2015 {published data only}
- Sahin L, Cesur M, Sahin M, Kilic E, Sen E. Maintenance of the parturient in the left lateral position after spinal anesthesia with plain levobupivacaine for cesarean section reduces hypotension: a randomized study. Regional Anesthesia and Pain Medicine 2015;40(5 Suppl 1):e132. [PubMed] [Google Scholar]
Sakr 2014 {published data only}
- Sakr A, Cohen S, Ramos D, Rah K, Syed S, Syed S, et al. Is 6% hetastarch preferred over prophylactic IV ephedrine for prevention of hypotension from intrathecal ropivacaine for cesarean section? Anesthesia & Analgesia 2014;118(Suppl 1):S-186. [Google Scholar]
Sanwal 2008 {published data only}
- Sanwal MK, Jain A, Vazifdar H. Optimum dose of bupivacaine with midazolam in spinal anesthesia to prevent hypotension in c-section. Anesthesiology 2008;109:A617. [Google Scholar]
Saravanan 2006 {published data only}
- Saranavan S, Columb M, Wilson RC, Watkins EJ, Lyons GR. Equivalent dose of ephedrine and phenylephrine in the prevention of post-spinal hypotension. International Journal of Obstetric Anesthesia 2004;13(3):S4. [Google Scholar]
- Saravanan S, Kocarev M, Wilson RC, Watkins E, Columb MO, Lyons G. Equivalent dose of ephedrine and phenylephrine in the prevention of post-spinal hypotension in caesarean section. British Journal of Anaesthesia 2006;96(1):95-9. [DOI] [PubMed] [Google Scholar]
Schofield 2011 {published data only}
- Schofield L. Is a relatively high pre-spinal heart rate associated with reduced efficacy of prophylactic vassopressor during spinal anaesthesia for caesarean section? Regional Anesthesia and Pain Medicine 2011;36(5 Suppl 2):E242. [DOI] [PubMed] [Google Scholar]
Seltenrich 2001 {published data only}
- Seltenrich M, Kamani A, Gunka V, Douglas J. The effect of injection rate on hypotension during spinal anesthesia for elective cesarean section [abstract]. Anesthesiology 2001;94(1A):A5. [Google Scholar]
- Seltenrich M, Kamani A, Gunka V, Douglas J. The effect of injection rate on hypotension during spinal anesthesia for elective cesarean section [abstract]. Anesthesiology 2001;95:A1042. [Google Scholar]
Seyedhejazi 2007 {published data only}
- Seyedhejazi M, Madarek E. The effect of small dose bupivacaine-fentanyl in spinal anesthesia on hemodynamic nausea and vomiting in cesarean section. Pakistan Journal of Medical Sciences 2007;23(5):747-50. [Google Scholar]
Sherif 2013 {published data only}
- Sherif N, Mokhtar A. Phenylephrine versus ephedrine usage in management of hypotension induced spinal anaesthesia in pre-eclamptic patients undergoing caesarean section. Journal of Perinatal Medicine 2013;41(Suppl 1):Abstract no:835. [Google Scholar]
Shifman 2007 {published data only}
- Shifman E, Got I. A comparison of different solutions for volume preloading: prevention of hypotension during epidural anaesthesia for caesarean section [abstract]. International Journal of Obstetric Anesthesia 2007;16(Suppl 1):S26. [Google Scholar]
Siddik‐Sayyid 2013 {published data only}
- Siddik-Sayyid S, Aouad M. Crystalloid coload combined with variable rate phenylephrine infusion for prevention of hypotension during spinal anesthesia for elective cesarean delivery vs crystalloid coload alone. European Journal of Anaesthesiology 2013;30:166-7. [Google Scholar]
Siddik‐Sayyid 2014 {published data only}
- Siddik-Sayyid SM, Taha SK, Kanazi GE, Aouad MT. A randomized controlled trial of variable rate phenylephrine infusion with rescue phenylephrine boluses versus rescue boluses alone on physician interventions during spinal anesthesia for elective cesarean delivery. Anesthesia & Analgesia 2014;118(3):611-8. [DOI] [PubMed] [Google Scholar]
Siddiqui 2016 {published data only}
- Siddiqui KM, Ali MA, Ullah H. Comparison of spinal anesthesia dosage based on height and weight versus height alone in patients undergoing elective cesarean section. Korean Journal of Anesthesiology 2016;69(2):143-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Simon 1999 {published data only}
- Simon L, Boulay G, Ziane AF, Hamza J. Effect of injection rate in hypotension associated with spinal anaesthesia for caesarean section. British Journal of Anaesthesia 1999;82 Suppl 1:161. [DOI] [PubMed] [Google Scholar]
Sivevski 2006 {published data only}
- Sivevski A. Spinal anaesthesia for cesarean section with reduced dose of intrathecal bupivacaine plus fentanyl. Makedonska Akademija na Naukite i Umetnostite Oddelenie Za Bioloshki i Meditsinski Nauki Prilozi 2006;27(2):225-36. [PubMed] [Google Scholar]
Sng 2013 {published data only}
- Sng BL, Tan HS, Sia A. Closed-loop double-pump automated system versus manual boluses to treat hypotension during spinal anaesthesia for caesarean section: randomised controlled trial. In: Australian and New Zealand College of Anaesthetists Annual Meeting; 2013 May 4-8; Melbourne, Australia. 2013.
Sng 2014 {published data only}
- Sng BL, Tan HS, Sia AT. Closed-loop double-vasopressor automated system vs manual bolus vasopressor to treat hypotension during spinal anaesthesia for caesarean section: a randomised controlled trial. Anaesthesia 2014;69(1):37-45. [DOI] [PubMed] [Google Scholar]
Sprague 1976 {published data only}
- Sprague D. Effects of position and uterine displacement on spinal anesthesia for caesarean section. Anesthesia and Anesthesiology 1976;44(2):164-6. [DOI] [PubMed] [Google Scholar]
Stewart 2010 {published data only}
- Stewart A, Fernando R, McDonald S, Hignett R, Jones T, Columb M, et al. Dose-dependent effects of phenylephrine for elective caesarean section under spinal anaesthesia: implications for the compromised fetus? International Journal of Obstetric Anesthesia 2008;17(Suppl 1):S9. [Google Scholar]
- Stewart A, Fernando R, McDonald S, Hignett R, Jones T, Columb M. The dose-dependent effects of phenylephrine for elective cesarean delivery under spinal anesthesia. Anesthesia & Analgesia 2010;111(5):1230-7. [DOI] [PubMed] [Google Scholar]
Stewart 2011 {published data only}
- Stewart A, Fernando R, McDonald S, Hignett R, Jones T, Colomb M. Can phenylephrine infusions cause reactive hypertension during elective caesarean section? International Journal of Obstetric Anesthesia 2011;20(Suppl 1):S7. [Google Scholar]
Stoneham 1999 {published data only}
- Stoneham M, Eldridge J, Popat M, Russell R. Oxford positioning technique improves haemodynamic stability and predictability of block height of spinal anaesthesia for elective caesarean section. International Journal of Obstetric Anesthesia 1999;8(4):242-8. [DOI] [PubMed] [Google Scholar]
- Stoneham M, Eldridge J, Popat M, Russell R. The wedged supine position predisposes to haemodynamic instability and unpredictable block height during onset of obstetric spinal anaesthesia [abstract]. International Journal of Obstetric Anesthesia 1998;7:199-200. [Google Scholar]
Sumikura 2009 {published data only}
- Sumikura H, Ohashi Y, Akai R, Irikoma S, Oshima M. Fetal acid base balance after preloading with lactated or bicarbonated ringers for cesarean section. In: American Society of Anaesthesiologists Annual Meeting; 2009 Oct 17-21; New Orleans, USA. 2009.
Szmuk 2008 {published data only}
- Szmuk P, Khazin V, Gorodinski L, Ezri T, Evron S. Preventive phenylephrine vs. ephedrine during cesarean delivery under spinal-epidural anesthesia. Anesthesiology 2008;109:A1334. [Google Scholar]
Tamilselvan 2009 {published data only}
Tanaka 2007 {published data only}
- Tanaka M, Balki M, Parkes R, Carvalho J. ED95 of phenylephrine to prevent hypotension and nausea/vomiting after spinal anesthesia for cesarean section. Anesthesiology 2007;106(Suppl 1):55. [Google Scholar]
Tanaka 2008 {published data only}
- Tanaka M, Balki M, Parkes RK, Carvalho JCA. ED95 of phenylephrine to prevent spinal-induced hypotension and/or nausea at elective cesarean delivery. International Journal of Obstetric Anesthesia 2009;18(2):125-30. [DOI] [PubMed] [Google Scholar]
Tang 2015 {published data only}
- Tang WX, Li JJ, Bu HM, Fu ZJ. Spinal anaesthesia with low-dose bupivacaine in marginally hyperbaric solutions for caesarean section. European Journal of Anaesthesiology 2015;32(7):493-8. [DOI] [PubMed] [Google Scholar]
Tekyeh 2013 {published data only}
- Tekyeh SMM, Tabari M, Jahanian V. Investigation the effects and side effects of different dosage of bupivacaine in combination with sufentanil for spinal anesthesia in cesarean section. Iranian Journal of Obstetrics, Gynecology and Infertility 2013;16(66):1-9. [Google Scholar]
Teoh 2009 {published data only}
- Teoh WH, Sia AT. Colloid preload versus coload for spinal anesthesia for cesarean delivery: the effects on maternal cardiac output. Anesthesia and Analgesia 2009;108(5):1592-8. [DOI] [PubMed] [Google Scholar]
- Teoh WHL, Sia ATH, Loh MH. To preload or coload? USCOM evaluation of the timing of colloid expansion on preventing spinal hypotension at cesarean delivery [abstract]. Regional Anesthesia and Pain Management 2006;31(5 Suppl 1):52. [Google Scholar]
Thomas 2001 {published data only}
- Thomas DG, Mowbray P. Comparison of thresholds for giving phenylephrine during spinal anaesthesia for caesarean section. British Journal of Anaesthesia 2001;87(4):658P. [Google Scholar]
Thomas 2004 {published data only}
- Thomas DG, Gardner S. Comparison of the time to peak pressor effect of phenylephrine and ephedrine during spinal anaesthesia for caesarean section. International Journal of Obstetric Anesthesia 2004;13(3):S4. [DOI] [PubMed] [Google Scholar]
Thomas 2006 {published data only}
- Thomas JS, Koh SH, Cooper GM. Haemodynamic effects of intravenous bolus or infusion of oxytocin in women undergoing caesarean section [abstract]. International Journal of Obstetric Anesthesia 2006;15 Suppl 1:S13. [Google Scholar]
Tolia 2008 {published data only}
- Tolia G, Kumar A, Jain A, Pandey M. Low dose intrathecal bupivacaine with fentanyl for cesarean delivery. Journal of Anaesthesiology Clinical Pharmacology 2008;24(2):201-4.
Turker 2011 {published data only}
- Turker G, Yilmazlar T, Basagan E, Gurbet A, Dizman S, Gunay H. The effects of colloid pre-loading on thromboelastography prior to caesarean delivery: hydroxyethyl starch 130/0.4 versus succinylated gelatine. Journal of International Medical Research 2011;39(1):143-9. [DOI] [PubMed] [Google Scholar]
Vallejo 2015 {published data only}
- Vallejo MC, Elzamzamy OM, Attaallah AF, Parsons JR, Shapiro R, Ranganathan. Comparison of continuous intravenous phenylephrine vs. norepinephrine infusions in prevention of spinal hypotension during cesarean delivery: assessment of hemodynamic parameters and outcomes. In: Society for Obstetric Anesthesia and Perinatology (SOAP) 47th Annual Meeting; 2015 May 13-17; Colorado, USA. 2015:GM-06.
Van Bogaert 1998 {published data only}
- Van Bogaert LJ. Prevention of post-spinal hypotension at elective cesarean section by wrapping of the lower limbs. International Journal of Gynecology & Obstetrics 1998;61(3):233-8. [DOI] [PubMed] [Google Scholar]
Vercauteren 1996 {published data only}
- Vercauteren MP, Hoffmann V, Coppejans HC, Van Steenberge AL, Adriaensen HA. Hydroxyethylstarch compared with modified gelatin as volume preload before spinal anaesthesia for caesarean section. British Journal of Anaesthesia 1996;76(5):731-3. [DOI] [PubMed] [Google Scholar]
Vercauteren 2000 {published data only}
- Vercauteren MP, Coppejans HC, Hoffmann VH, Mertens E, Adriaensen HA. Prevention of hypotension by single 5-mg dose of ephedrine during small-dose spinal anesthesia in prehydrated cesarean delivery patients. Anesthesia & Analgesia 2000;90(2):324-7. [DOI] [PubMed] [Google Scholar]
Vincent 1998 {published data only}
- Vincent RD Jr, Werhan CF, Norman PF, Shih GH, Chestnut DH, Ray T, et al. Prophylactic angiotensin II infusion during spinal anesthesia for elective cesarean delivery. Anesthesiology 1998;88(6):1475-9. [DOI] [PubMed] [Google Scholar]
Vuffray 2005a {published data only}
- Vuffray A, Crochetiere C, Bureau N , Villeneuve E, Lacroix J. Ephedrine and phenylephrine in spinal induced hypotension: myth and reality [abstract]. Regional Anesthesia and Pain Medicine 2005;30(5 Suppl 1):73. [Google Scholar]
Vuffray 2005b {published data only}
- Vuffray A, Crochetiere C, Bureau N , Villeneuve E, Lacroix J. Ephedrine and phenylephrine in spinal induced hypotension: myth and reality [abstract]. Anesthesiology 2005;102(Suppl 1):51. [Google Scholar]
Wang 2011 {published data only}
- Wang M, Han CB, Qian YN. Comparison of effects in puerpera and fetus with ephedrine and phenylephrine during a cesarean delivery. Chinese Medical Journal 2011;91(31):2195-8. [PubMed] [Google Scholar]
- Wang M, Qian Y. Effects of ephedrine and phenylephrine on fetal heart rate during spinal anesthesia for cesarean delivery. Anesthesia & Analgesia 2011;112:S-289. [Google Scholar]
Wang 2015 {published data only}
- Wang X, Xu JM, Zhou F, He L, Cui YL, Li ZJ. Maternal position and development of hypotension in patients undergoing cesarean section under combined spinal-epidural anesthesia of intrathecal hyperbaric ropivacaine. Medical Science Monitor 2015;21:52-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Williamson 2009 {published data only}
- Williamson W, Burks D, Pipkin J, Burkard JF, Osborne LA, Pellegrini JE. Effect of timing of fluid bolus on reduction of spinal-induced hypotension in patients undergoing elective cesarean delivery. AANA Journal 2009;77(2):130-6. [PubMed] [Google Scholar]
Wojciechowski 2008 {published data only}
- Wojciechowski KG, McCarthy RJ, Toledo P, Sullivan JT. The effect of fluid co-administration strategies on maternal hypotension following spinal anesthesia. Anesthesiology 2008;109:A1115. [Google Scholar]
Wollman 1968 {published data only}
- Wollman SB, Marx GF. Acute hydration for prevention of hypotension of spinal anesthesia in parturients. Anesthesiology 1968;29(2):374-80. [CN-00235365] [DOI] [PubMed] [Google Scholar]
Xiao 2015a {published data only}
- Xiao W, Duan QF, Fu WY, Chi XZ, Wang FY, Ma DQ, et al. Goal-directed fluid therapy may improve hemodynamic stability of parturient with hypertensive disorders of pregnancy under combined spinal epidural anesthesia for cesarean delivery and the well-being of newborns. Chinese Medical Journal 2015;128(14):1922-31. [DOI] [PMC free article] [PubMed]
Xiao 2015b {published data only}
- Xiao W, Duan Q, Zhao L, Chi X, Wang F, Ma D, et al. Goal-directed fluid therapy may improve hemodynamic stability in parturient women under combined spinal epidural anesthesia for cesarean section and newborn well-being. Journal of Obstetrics and Gynaecology Research 2015;41(10):1547-55. [DOI] [PubMed] [Google Scholar]
Xu 2012 {published data only}
- Xu S, Wu H, Zhao Q, Shen X, Guo X, Wang F. The median effective volume of crystalloid in preventing hypotension in patients undergoing cesarean delivery with spinal anesthesia. Revista Brasileira de Anestesiologia 2012;62(3):312-24. [DOI] [PubMed] [Google Scholar]
Xu 2014 {published data only}
- Xu T, Li Y, Zhou J, Shuai B, Li Y, Mai W, et al. Stereological study of the placenta in patients receiving different vasopressors for hypotension during cesarean section. Journal of Southern Medical University 2014;34(8):1154-7. [PubMed] [Google Scholar]
Yadav 2012 {published data only}
- Yadav U, Bharat K. A clinical comparative study of prophylactic infusions of phenylephrine and ephedrine on maternal hemodynamics and fetal acidosis in elective caesarean section. International Journal of Pharmaceutical Sciences and Research 2012;3(12):5056-61. [Google Scholar]
Yentis 2000 {published data only}
- Yentis SM, Jenkins CS, Lucas DN, Barnes PK. The effect of prophylactic glycopyrrolate on maternal haemodynamics following spinal anaesthesia for elective caesarean section. International Journal of Obstetric Anesthesia 2000;9(3):156-9. [DOI] [PubMed] [Google Scholar]
Yokoyama 2004 {published data only}
- Yokoyama N, Nishikawa K, Saito Y, Saito S, Goto F. Comparison of the effects of colloid and crystalloid solution for volume preloading on maternal hemodynamics and neonatal outcome in spinal anesthesia for cesarean section. Masui - Japanese Journal of Anesthesiology 2004;53(9):1019-24. [PubMed] [Google Scholar]
Yoon 2012 {published data only}
- Yoon HJ, Cho HJ, Lee IH, Jee YS, Kim SM. Comparison of hemodynamic changes between phenylephrine and combined phenylephrine and glycopyrrolate groups after spinal anesthesia for cesarean delivery. Korean Journal of Anesthesiology 2012;62(1):35-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Young 1996 {published data only}
- Young S, Reid JA, Thorburn J. Spinal-induced hypotension at caesarean section reduced to 3.3% [abstract]. International Journal of Obstetric Anesthesia 1996;5:210-1. [DOI] [PubMed] [Google Scholar]
Yun 1998 {published data only}
- Yun E, Marx GF, Santos AC. The effects of maternal position during induction of combined spinal-epidural anesthesia for cesarean delivery. Anesthesia & Analgesia 1998;87(3):614-8. [DOI] [PubMed] [Google Scholar]
Yurtlu 2012 {published data only}
- Yurtlu BS, Hanci V, Okyay RD, Bostankolu SE, Erdogan G, Hakimoglu S, et al. Effects on hypotension incidence: hyperbaric, isobaric, and combinations of bupivacaine for spinal anesthesia in cesarean section [Hipotansiyon insidansi uzerine etkiler: sezaryen icin spinal anestezide hiperbarik, isobarik bupivakain ve kombinasyonlari]. Turkish Journal of Medical Sciences 2012;42(2):307-13. [Google Scholar]
Zakowski 1992 {published data only}
- Zakowski M, Otto T, Baratta J, Ramanathan S, Turndorf H. Phenylephrine for hypotension in high risk parturients during cesarean section. Anesthesiology 1992;77:A973. [Google Scholar]
Zasa 2015 {published data only}
- Zasa M, Conci E, Marchignoli A, Pini R, Passeri L, Fanelli G, et al. Comparison of two different approaches to hypotension following spinal anaesthesia for caesarean delivery: effects on neonatal and maternal wellbeing. Acta Bio-Medica: Atenei Parmensis 2015;86(1):45-52. [PubMed] [Google Scholar]
Zhou 2008 {published data only}
- Zhou ZQ, Shao Q, Zeng Q, Song J, Yang JJ. Lumbar wedge versus pelvic wedge in preventing hypotension following combined spinal epidural anaesthesia for caesarean delivery. Anaesthesia and Intensive Care 2008;36(6):835-9. [DOI] [PubMed] [Google Scholar]
References to studies awaiting assessment
Abedinzadeh 2010 {published data only}
- Abedinzadeh MR, Noorian C, Kheire S, Nejat Z. Pharmaceutical effects of ephedrine, atropine and mucosal phenylephrine on hemodynamic alterations of women during spinal anesthesia in caesarean section. Journal of Gorgan University of Medical Sciences 2012;13(4):27-34. [Google Scholar]
- IRCT138902213912N1. Comparison of the effects of ephedrine, atropine and mucosal phenylephrine perfusion in preventing hypotension during spinal anesthesia for cesarean section. en.search.irct.ir/view/3081 (first received 15 June 2010).
Alday 2011 {published data only}
- Alday Munoz E, Palacio Abizanda F, De Diego Pdel R, Gilsanz Rodriguez F. Ephedrine vs. phenylephrine by intravenous bolus and continuous infusion to prevent hypotension secondary to spinal anesthesia during cesarean section: a randomized comparative trial. Revista Española de Anestesiología y Reanimación 2011;58(7):412-6. [DOI] [PubMed] [Google Scholar]
Amiri 2013 {published data only}
- Amiri HA, Banihashem N, Naziri F, Rabiee M, Ghasemi A, Shirkhani Z, et al. The effects of phenylephrine and ephedrine on maternal hemodynamic changes and neonatal acid-base status during spinal anesthesia for cesarean delivery. Journal of Mazandaran University of Medical Sciences 2013;23(107):123-31. [Google Scholar]
Ashpole 2006 {published data only}
- Ashpole K, Fernando R, Tamilselvan P, Columb M. Fetal pH after phenylephrine or ephedrine infusion titrated to maintain systolic blood pressure at caesarean section under spinal anaesthesia [abstract]. International Journal of Obstetric Anesthesia 2006;15 Suppl 1:S6. [Google Scholar]
- Ashpole KJ, Fernando R, Tamilselvan P, Columb M. Fetal pH after phenylephrine infusion titrated to maintain systolic blood pressure at cesarean section under spinal anesthesia [abstract]. Anesthesiology 2006;104(Suppl 1):38. [Google Scholar]
Bennasr 2014 {published data only}
- Bennasr L, Ben Marzouk S, Ajili Z, Riahi A, Jarraya MA, Massoudi S, et al. Prevention of hypotension during spinal anesthesia for elective caesarean section: coloading with HAE 130/0.4 vs normal saline solution. Annales Francaises D'anesthesie et de Reanimation 2014;33(12):643-7. [DOI] [PubMed] [Google Scholar]
Boswell 2008 {published data only}
- Boswell O, Eldridge J, Taylor I, Tucker V. A prospective, double-blinded randomised controlled trial of ephedrine infusions and ephedrine boluses during spinal anaesthesia for caesarean section. International Journal of Obstetric Anesthesia 2008;17(Suppl 1):S53. [Google Scholar]
- ISRCTN26979860. Prophylactic ephedrine and hypotension during spinal anaesthesia for elective caesarean section. isrctn.com/ISRCTN26979860 (first received 12 September 2003).
Bright 2003 {published data only}
- Bright E, Brownlow H, Gande R, Underhill H, Wise H, Swayne P. Prophylactic oral ephedrine: effect on hypotension after subarachnoid block for caesarean section - a double-blind, controlled, randomised trial [abstract]. International Journal of Obstetric Anesthesia 2003;12:196. [Google Scholar]
Golmohammadi 2013 {published data only}
- Golmohammadi M, Mansuri P, Jafari M, Khalkhali HR, Aghdashi M. Comparison of the effects of colloid loading before and after spinal anesthesia to prevent maternal hypotension in cesarean section. Journal of Zanjan University of Medical Sciences and Health Services 2013;21(89):1-9. [Google Scholar]
Gonzalez 2014 {published data only}
- Gonzalez I, Marti A, Moret E, Manrique S, Suescun M, Trillo L. An intermittent pneumatic compression system in lower extremities reduces vasoconstrictor requirements during elective caesarean section under spinal anesthesia: a preliminary study. International Journal of Obstetric Anesthesia 2014;23(Suppl 1):S29. [Google Scholar]
Higgins 2009 {published data only}
- Higgins N, Grewal GK, Toledo P, Sullivan JT, McCarthy RJ. Hemodynamic changes with spinal anesthesia during co-load with colloid vs crystalloid solutions. In: American Society of Anaesthesiologists Annual Meeting; 2009 Oct 17-21; New Orleans, USA. 2009.
Hwang 1994 {published data only}
- Hwang HS, Lee KC, Song YK, Yoon JS, Kim TY. Effects of the speed of crystalloid preload in preventing of hypotension during spinal anesthesia for caesarean section. Korean Journal of Anesthesiology 1994;27(11):1660-5.
Jain 2013 {published data only}
- Jain K, Makkar JK, Subramani S, Gainder S. A randomised trial comparing prophylactic phenylephrine and ephedrine infusion during spinal anesthesia for emergency cesarean delivery in cases of acute fetal compromise. Journal of Obstetric Anaesthesia and Critical Care 2013;3(2):119. [DOI] [PubMed] [Google Scholar]
Jung 2006 {published data only}
- Jung SW, Kim EJ, Min BW, Ban JS, Lee SG, Lee JH. Comparison of maternal and fetal affects of ephedrine and phenylephrine infusion during spinal anesthesia for cesarean section. Korean Journal of Anesthesiology 2006;51(3):335-42. [Google Scholar]
Kashiwagi 2012 {published data only}
- Kashiwagi K, Kataoka K, Wakabayashi S, Kumagawa Y, Morimoto E, Maeda T, et al. Prevention of spinal hypotension associated with cesarean section by aortocaval compression - left 15 degree table tilt vs. uterine displacement by hand. Japanese Journal of Anesthesiology 2012;61(2):177-81. [PubMed] [Google Scholar]
Kiss 2012 {published data only}
- Kiss K, Zimanyi M, Agocs S, Bodonovits A, Orvos H, Molnar Z. Ringer's lactate (RL) and balanced Ringer's solution (BR) during elective caesarean delivery in spinal anaesthesia: Effects on neonatal homeostasis. European Journal of Anaesthesiology 2012;29:168. [Google Scholar]
Lang 1996 {published data only}
- Lang J, Jayasinghe C, Woodson L, Ahmad M, Mathru M. Failure to prevent hypotension after spinal anaesthesia for elective cesarean section despite crystalloid or colloid preload augmentation is probably mediated by atrial natriuretic peptide. Anesthesiology 1996;85(3A):A904. [Google Scholar]
Lee 2011 {published data only}
- Kang H, Lee JW, Choi JY, Kim YJ. Wrapping of the lower limbs for prevention of post spinal hypotension in cesarean section under spinal anesthesia. Regional Anesthesia and Pain Medicine 2011;36(5 Suppl 2):E164-5. [Google Scholar]
- Lee J, Kang H, Baek SK, Choi J. Wrapping of the lower limbs for prevention of post spinal hypotension during cesarean section under spinal anesthesia. Anesthesia and Pain Medicine 2011;6(2):173-7. [Google Scholar]
Osazuwa 2015 {published data only}
- Osazuwa IH, Ebague A. Crystalloid preload shows transient superiority over colloid, or their combination in spinal anaesthesia-induced hypotension prophylaxis for caesarean section. Nigerian Journal of Medicine 2015;24(2):137-43. [PubMed] [Google Scholar]
Rahmoune 2009 {published data only}
- Rahmoune FC, Saadelli A, Yahiaoui H, Bouzenacha A, Ouchtati M. A randomized controlled study evaluating colloid preload to prevent maternal hypotension after spinal anaesthesia for caesarean section. In: Annual Meeting of the Obstetric Anaesthetists' Association; 2009 May 21-22; Jersey. 2009:P15.
Sahoo 2011 {published data only}
- Sahoo AL, Shidhaye RV, Badhe VK, Divekar DS. Prevention of hypotension following spinal anesthesia for caesarean section: comparison between prophylactic phenylephrine infusion and colloid co-hydration. Journal of Obstetric Anaesthesia and Critical Care 2011;1(2):104. [Google Scholar]
Sakuma 2010 {published data only}
- Sakuma T, Sato M, Sato K, Yokoi M. Effects of intravenous vasopressor on spread of spinal anesthesia with 0.5% hyperbaric bupivacaine for caesarean delivery. Masui - Japanese Journal of Anesthesiology 2010;59(6):691-5. [PubMed] [Google Scholar]
Soltani 2009 {published data only}
- Soltani H, Jabalameli M, Hashemi SJ, Behdad S, Soleimani B. Combinatorial approaches to prevent spinal induced hypotension in CS. Canadian Journal of Anaesthesia 2009;56(Suppl 1):S65. [Google Scholar]
Van Bogaert 2000 {published data only}
- Van Bogaert LJ. Lumbar lordosis and the spread of subarachnoid hyperbaric 0.5% bupivacaine at cesarean section. International Journal of Gynecology & Obstetrics 2000;71(1):65-6. [DOI] [PubMed] [Google Scholar]
Van Treese 1996 {published data only}
- Van Treese PA, Dosch MP, Ernst AM. Effect of leg elevation and/or lower limb compression to prevent hypotension during spinal anesthesia for cesarean section. Journal of the American Association of Nurse Anesthetists 1996;64:456-7. [Google Scholar]
Yoon 2009 {published data only}
- Jee SY, Yoon HJ, Oh JI, Kim SM, Lee IH. Comparison of maternal hemodynamic effects of ephedrine, phenylephrine, and combination infusion during spinal anesthesia for cesarean delivery. In: Society for Obstetric Anesthesia and Perinatology (SOAP) 41st Annual Meeting; 2009 April 29-May 1, Washington, USA. 2009.
- Yoon HJ, Jee YS, Lee IH, Kim SM, Jang CH. Comparison of maternal and fetal effects of ephedrine, phenylephrine, and combination infusion during spinal anesthesia for cesarean delivery. Anesthesia and Pain Medicine 2009;4(2):161-5. [Google Scholar]
References to ongoing studies
NCT01891175 {published data only}
- NCT01891175. Prevention of maternal hypotension during elective caesarean section performed with spinal anaesthesia, through intermittent pneumatic compression system in the lower extremities. clinicaltrials.gov/show/NCT01891175 (first received 24 May 2013).
Additional references
Atlee 1999
- Atlee JL. Complications in Anesthesia. Philadelphia: W.B. Saunders, 1999. [Google Scholar]
Clark 2005
- Clark VA, Sharwood-Smith GH, Stewart AVG. Ephedrine requirements are reduced during spinal anaesthesia for caesarean section in preeclampsia. International Journal of Obstetric Anesthesia 2005;14(1):9-13. [DOI] [PubMed] [Google Scholar]
Cluver 2013
- Cluver C, Novikova N, Hofmeyr GJ, Hall DR. Maternal position during caesarean section for preventing maternal and neonatal complications. Cochrane Database of Systematic Reviews 2013, Issue 3. [DOI: 10.1002/14651858.CD007623.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Gao 2015
- Gao L, Zheng G, Han J, Wang Y, Zheng J. Effects of prophylactic ondansetron on spinal anesthesia-induced hypotension: a meta-analysis. International Journal of Obstetric Anaesthesia 2015;24(4):335-43. [DOI] [PubMed] [Google Scholar]
Glosten 2000
- Glosten B. Anesthesia for obstetrics. In: Miller RD, editors(s). Anesthesia. 5th edition. Vol. 2. Philadelphia: Churchill Livingstone, 2000:2024-68. [ISBN 0-443-07988-9] [Google Scholar]
Hawkins 1997
- Hawkins JL, Koonin LM, Palmer SK, Gibbs CP. Anesthesia-related deaths during obstetric delivery in the United States, 1979-1990. Anesthesiology 1997;86(2):277-84. [DOI] [PubMed] [Google Scholar]
Hibbard 1996
- Hibbard BM, Anderson MM, Drife JO, Tighe JR, Gordon G, Willatts S, et al. Deaths associated with anaesthesia. In: Rubery E, Bourdillon P, editors(s). Report on Confidential Enquiries into Maternal Deaths in the United Kingdom 1991-1993. Norwich: HMSO, 1996:87-102. [ISBN 0 11 321983 0] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane-handbook.org.
Hollmen 1978
- Hollmen AI, Jouppila R, Koivisto M, Maatta L, Pihlajaniemi R, Puukka M, et al. Neurologic activity of infants following anesthesia for cesarean section. Anesthesiology 1978;48(5):350-6. [DOI] [PubMed] [Google Scholar]
Lapins 2001
- Lapins E. Hypotension during spinal anaesthesia for caesarean section. International Journal of Obstetric Anesthesia 2001;10:226. [DOI] [PubMed] [Google Scholar]
Lucas 1999
- Lucas DN, Ciccone GK, Yentis SM. Extending low-dose epidural analgesia for emergency caesarean section. A comparison of three solutions. Anaesthesia 1999;54(12):1173-7. [DOI] [PubMed] [Google Scholar]
May 1995
- Lyons G, May A. Epidural is an outmoded form of regional anaesthesia for elective caesarean section. International Journal of Obstetric Anesthesia 1995;4(1):34-9. [Accession No:95028271] [DOI] [PubMed] [Google Scholar]
Mercier 2013
- Mercier FJ, Auge M, Hoffmann C, Fischer C, Le Gouez A. Maternal hypotension during spinal anesthesia for caesarean delivery. Minerva Anestesiologica 2013;79(1):62-73. [PubMed] [Google Scholar]
MIMS 1995
- MIMS Annual. 19th edition. MIMS, 1995. [Google Scholar]
Morgan 1994
- Morgan P. The role of vasopressors in the management of hypotension induced by spinal and epidural anaesthesia. Canadian Journal of Anesthesia 1994;41(5):404-13. [DOI] [PubMed] [Google Scholar]
Ngan Kee 2006
- Ngan Kee WD, Khaw KS. Vasopressors in obstetrics: what should we be using? Current Opinion in Anesthesiology 2006;19(3):238-43. [DOI] [PubMed] [Google Scholar]
Ousley 2012
- Ousley R, Egan C, Dowling K, Cyna AM. Assessment of block height for satisfactory spinal anaesthesia for caesarean section. Anaesthesia 2012;67(12):1356-63. [DOI] [PubMed] [Google Scholar]
Perel 2013
- Perel P, Roberts I, Ker K. Colloids versus crystalloids for fluid resuscitation in critically ill patients. Cochrane Database of Systematic Reviews 2013, Issue 2. [DOI: 10.1002/14651858.CD000567.pub6] [DOI] [PubMed] [Google Scholar]
Rasmussen 1994
- Rasmussen GE, Malinow AM. Toward reducing maternal mortality: the problem airway in obstetrics. In: Rocke DA, editors(s). International Anesthesia Clinics: Shaping Future Obstetric Anesthesia Practice. Vol. 32. Boston: Little, Brown and Company, 1994:83-101. [ISSN 0020-5907] [PubMed] [Google Scholar]
Reisner 1999
- Reisner LS, Lin D. Anesthesia for cesarean section. In: Chestnut DH, editors(s). Obstetric Anesthesia. 2nd edition. St. Louis: Mosby, 1999:465-92. [ISBN 0-3230-0383-4] [Google Scholar]
RevMan 2014 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Rippoles 2015
- Ripollés Melchor J, Espinosa Á, Martínez Hurtado E, Casans Francés R, Navarro Pérez R, Abad Gurumeta A, et al. Colloids versus crystalloids in the prevention of hypotension induced by spinal anesthesia in elective cesarean section. A systematic review and meta-analysis. Minerva Anestesiologica 2015;81(9):1019-30. [PubMed] [Google Scholar]
Roberts 1995
- Roberts SW, Leveno KJ, Sidawi JE. Fetal acidemia associated with regional anesthesia for caesarean section. Obstetrics & Gynecology 1995;85:79. [DOI] [PubMed] [Google Scholar]
Robson 1992
- Robson SC, Boys RJ, Rodeck C, Morgan B. Maternal and fetal haemodynamic effects of spinal and extradural anaesthesia for elective caesarean section. British Journal of Anaesthesia 1992;68(1):54-9. [DOI] [PubMed] [Google Scholar]
Rocke 1995
- Rocke DA, Rout CC. Volume preloading, spinal hypotension and caesarean section. British Journal of Anaesthesia 1995;75(3):257-9. [MEDLINE: ] [ISSN 0007-0912] [DOI] [PubMed] [Google Scholar]
Russell 1995
- Russell IF. Levels of anaesthesia and intraoperative pain at caesarean section under regional block. International Journal of Obstetric Anesthesia 1995;4:71. [DOI] [PubMed] [Google Scholar]
Sharma 1999
- Sharma SK, Lechner RB. Hematologic and coagulation disorders. In: Chestnut DH, editors(s). Obstetric Anesthesia: Principles and Practice. 2nd edition. St. Louis, Missouri: Mosby Inc, 1999:852. [ISBN 0-3230-0383-4] [Google Scholar]
Sharwood‐Smith 1999
- Sharwood-Smith G, Clark V, Watson E. Regional anaesthesia for caesarean section in severe preeclampsia: spinal anaesthesia is the preferred choice. International Journal of Obstetric Anesthesia 1999;8:85-9. [DOI] [PubMed] [Google Scholar]
Shibli 2000
- Shibli KU, Russell IF. A survey of anaesthetic techniques used for caesarean section in the UK in 1997. International Journal of Obstetric Anesthesia 2000;9(3):160-7. [DOI] [PubMed] [Google Scholar]
Wickham 1996
- Wickham EA. Potential transmission of BSE via medicinal products [Editorial]. BMJ 1996;312(7037):988-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to other published versions of this review
Cyna 2006
- Cyna AM, Andrew M, Emmett RS, Middleton P, Simmons SW. Techniques for preventing hypotension during spinal anaesthesia for caesarean section. Cochrane Database of Systematic Reviews 2006, Issue 4. [DOI: 10.1002/14651858.CD002251.pub2] [DOI] [PubMed] [Google Scholar]
Cyna 2017
- Chooi C, Cox JJ, Lumb RS, Middleton P, Chemali M, Emmett RS, Simmons SW, Cyna AM. Techniques for preventing hypotension during spinal anaesthesia for caesarean section. Cochrane Database of Systematic Reviews 2017, Issue 8. [DOI: 10.1002/14651858.CD002251.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]