

Abstract
Background
Workforce alcohol and drug testing is commonplace but its effect in reducing occupational injuries remains unclear.
Objectives
To assess the effects of alcohol and drug screening of occupational drivers (operating a motorised vehicle) in preventing injury or work‐related effects such as sickness absence related to injury.
Search methods
We searched the following databases up to June 2007 (or up to the latest issue then available): MEDLINE, EMBASE, The Cochrane Library, Cochrane Occupational Health Field's specialised register, DARE, PsychINFO, ERIC, ETOH, CISDOC, NIOSHTIC, TRANSPORT, Zetoc, Science Citation Index and Social Science Citation index and HSELINE. We also searched reference lists, relevant websites and conducted hand searching.
Selection criteria
Randomised controlled trials (RCTs), cluster‐randomised trials, controlled clinical trials, controlled before and after studies (more than three time points to be measured before and after the study) and interrupted time‐series (ITS) studies that evaluated alcohol or drug screening interventions for occupational drivers (compared to another intervention or no intervention) with an outcome measured as a reduction in injury or a proxy measure thereof.
Data collection and analysis
Two review authors independently extracted data and assessed study quality. We contacted authors of the included studies for further information.
Main results
We included two interrupted time‐series studies conducted in the USA. One study was conducted in five large US transportation companies (N = 115,019) that carried passengers and/or cargo. Monthly injury rates were available from 1983 to 1999. In the study company, two interventions of interest were evaluated: mandatory random drug testing and mandatory random and for‐cause alcohol testing programmes. The third study focused only on mandatory random drug testing and was conducted on federal injury data that covered all truck drivers of interstate carriers.
We recalculated the results from raw data provided by the study authors. Following reanalysis, we found that in one study mandatory random and for‐cause alcohol testing was associated with a significant decrease in the level of injuries immediately following the intervention (‐1.25 injuries/100 person years, 95% CI ‐2.29 to ‐0.21) but did not significantly affect the existing long‐term downward trend (‐0.28 injuries/100 person years/year, 95% CI ‐0.78 to 0.21).
Mandatory random drug testing was significantly associated with an immediate change in injury level following the intervention (1.26 injuries/100 person years, 95% CI 0.36 to 2.16) in one study, and in the second study there was no significant effect (‐1.36/injuries/100 person years, 95% CI ‐1.69 to 0.41). In the long term, random drug testing was associated with a significant increase in the downward trend (‐0.19 injuries/100 person years/year, 95% CI ‐0.30 to ‐0.07) in one study, the other study was also associated with a significant improvement in the long‐term downward trend (‐0.83 fatal accidents/100 million vehicle miles/year, 95% CI ‐1.08 to ‐0.58).
Authors' conclusions
There is insufficient evidence to advise for or against the use of drug and alcohol testing of occupational drivers for preventing injuries as a sole, effective, long‐term solution in the context of workplace culture, peer interaction and other local factors. Cluster‐randomised trials are needed to better address the effects of interventions for injury prevention in this occupational setting.
Keywords: Humans; Motor Vehicles; Motor Vehicles/statistics & numerical data; Substance Abuse Detection; Accidents, Occupational; Accidents, Occupational/prevention & control; Accidents, Occupational/statistics & numerical data; Alcoholism; Alcoholism/diagnosis; Substance‐Related Disorders; Substance‐Related Disorders/diagnosis; United States; United States/epidemiology; Workplace; Wounds and Injuries; Wounds and Injuries/epidemiology; Wounds and Injuries/prevention & control
Plain language summary
Alcohol and drug screening for preventing injury among people whose job involves driving
Alcohol and drug abuse are serious public health problems worldwide. Workplace alcohol and drug testing is a common intervention, especially in developed nations, but it is costly and its use is controversial. This systematic review aimed to assess the effects of alcohol and drug screening among occupational drivers for preventing injury.
We conducted a systematic search of the literature on the effects of alcohol and drug screening among occupational drivers for preventing injury. We then appraised the quality of the studies found and assessed their results. We found two time‐series studies conducted in the USA. One was conducted in five large transportation companies, and it examined the effects of two interventions of interest: implementation of legislation for mandatory random drug testing and mandatory random and for‐cause alcohol testing. The other study was conducted using national injury data.
There is limited evidence that in the long term mandatory drug‐testing interventions can be more effective than no intervention in reducing injuries in occupational drivers. For mandatory alcohol testing there was evidence of an immediate effect only.
Given the widespread practice of alcohol and drug testing and the paucity of evaluation studies found, more evaluation studies are needed. Interrupted time‐series is a feasible study design for evaluating interventions that aim at preventing alcohol and drug related injuries. However, time‐series studies of higher quality and of long duration are needed to increase the level of evidence. A cluster‐randomised trial would be the ideal study design to evaluate the effects of interventions for injury prevention in this occupational setting.
Background
Description of the condition
The misuse of alcohol and illicit drugs constitutes a major global public health problem (Rodgers 2004). In recent years, the role of alcohol and drug intoxication in work‐related injuries and work‐related crashes has received increasing attention (Francis 2003; Hope 2005; IIDTW 2004). In some safety‐critical occupations a single mistake could have disastrous consequences in terms of death, injury and impact on public confidence (Francis 2003; IIDTW 2004). Results of some recent surveys of alcohol and drug use provide ample cause for concern. In the United States (US), military personnel service members between the ages 18 and 25 had a twice as high prevalence of heavy drinking in the previous 30 days as civilians in the same age group (Fernandez 2006). In a British Health community postal survey, there was a significant association between illegal drug use and work‐related traffic crashes independent of other associated variables like alcohol, health issues and prescription drug use (Smith 2004). However a study analysing annual reports from 1995‐2000 published by the US Department of Transportation estimated that only less than one crash in 1,000 per year was attributable to employee alcohol use (Cunradi 2005). For drugs the estimate was 4 to 7 crashes annually in 1,000 crashes (Cunradi 2005).
Description of the intervention
Alcohol and drug testing involves the analysis of biological material to detect these substances or their metabolites in the body. Testing may involve analysis of blood, urine, saliva, sweat, hair and breath samples (Francis 2003). The timing of work‐related testing can take a variety of forms, including pre‐employment testing, random testing of employees and post‐accident testing, reasonable suspicion testing, follow‐up and return‐to‐duty testing.
Workforce drug and alcohol testing is extremely controversial and there has been prolonged debate over the effectiveness, cost‐effectiveness, ethics and legality of the practice (IIDTW 2004). In the US an estimated 80% of the large employers currently use some form of alcohol and/or drug testing of employees (Ozminkowski 2003). All Federal government employees and all workers in industries regulated by the Federal government are included in mandatory screening programmes (Spiehler 1994). Mandatory drug testing for safety‐sensitive occupations was announced in 1988 by the United States Department of Transportation Industry (federal law) and implemented in 1990 (Jacobson 2003). There is a relative paucity of research evidence on the nature and extent of workforce drug and alcohol testing outside the US. Legislation and implementation varies between and within countries. In Canada, the United Kingdom and other European countries, workforce testing has been primarily concentrated in safety and security critical industries and professions where it has been argued that the public is entitled to expect the highest standards of safety and probity (Francis 2003; IIDTW 2004). While selective drug‐free workplace programmes have been associated with an industry specific preventive effect, this tends to occur in the construction and service sectors where two key factors are influential: background level of injury risk and prevalence of substance abuse in the workforce (Wickizer 2004).
How the intervention might work
Alcohol and drug testing may prevent workplace‐related injuries by deterring the misuse of illicit substances among employees thereby reducing risks to health and safety in the work environment. Other purported benefits of testing include: improved employee welfare, reduced risks to the production process, enhanced public confidence in the organisation and improved medical fitness thereby reducing healthcare costs (Francis 2003, IIDTW 2004).
A recent study of analyses within the construction industry indicated that companies with drug‐testing programmes experienced a 51% reduction in injury incident rates within two years of implementation (Gerber 2002). In contrast to general prevalence data, with a substance misuse testing programme in place in the US Air Force, the overall test positive rates for marijuana and cocaine were very low (Grayson 2004).
Any potential benefits of testing must be weighed against potential harms which include: the fallibility of testing and the consequences associated with false positives (for example, when legally available drugs produce a positive test for illicit substances) and false negatives (the failure to identify persons misusing alcohol or illicit drugs); the initiation of legal proceedings against employers for inappropriately dealing with performance issues or policing the private behaviour of the workforce (Francis 2003; Rothstein 1991). Other potential harms include damaged employer/employee relations and reduced productivity, negative impacts on 'health and safety' arising from underreporting of minor injuries or 'near misses' for fear of triggering testing procedures, stigmatisation of those testing positive and the human resource implications for those who may have tested positive in 'pre‐employment screening' (IIDTW 2004; Rothstein 1991). Furthermore, cost issues and ethical issues have been raised. A sound testing method and test chain process is not standardised internationally.
Why it is important to do this review
Ongoing research, monitoring and analysis of the impact and development of drug testing at work have recently been advocated (IIDTW 2004). Although there have been several reviews written on this topic, no systematic synthesis has previously been carried out of the evidence relating to the benefits and harms of alcohol and drug testing in a workforce that primarily operates vehicles (Francis 2003; French 2004; IIDTW 2004, Levine 2004).
Objectives
To assess the effects of alcohol and drug screening of occupational drivers (operating a motorised vehicle) in preventing injury (or work‐related effects such as sickness absence related to injury).
Methods
Criteria for considering studies for this review
Types of studies
All randomised controlled trials (RCT), cluster‐randomised trials, controlled clinical trials (CCT), controlled before and after studies (CBA) or interrupted time‐series studies (ITS) (with more than three time points to be measured before and after the study) evaluating the effects of alcohol or drug testing in reducing injuries.
Types of participants
We included studies in which the participants were adults whose occupation involved the operation of motorised vehicles for the purpose of transporting persons or goods or services.
The following specific categories of vehicle operator/driver were considered:
Persons operating motorised vehicles in the course of private commercial or public duty designed to carry passengers. This included, but was not limited to, bus drivers (including drivers of school buses), train drivers, taxi drivers, drivers/pilots of aircraft or sea craft.
Persons operating motorised vehicles designed to transport goods or services. This included, but was not limited to, haulers/distributors, postal delivery workers, couriers and sales representatives.
Persons operating motorised vehicles during the course of work that may not have been included under the above categories. This included, but was not limited to, drivers of military vehicles, construction workers, farming workers, oil industry workers, mine/quarry workers and warehouse workers.
Types of interventions
We included studies where the intervention was any form of alcohol and or drug testing administered to the types of participants listed above, with the intention of reducing work(er)‐related injuries. We aimed to categorise interventions according to the timing and purported rationale for testing (pre‐employment, random, post‐incident, reasonable suspicion, return to duty, follow‐up or post‐rehabilitation) and according to the substance that the test was designed to detect (alcohol, cannabinoids, cocaine, amphetamines, opiates, benzodiazepines, phencyclidine or prescription drugs).
Types of outcome measures
Primary outcomes
We included the numbers of:
fatal injuries
non‐fatal injuries
incidents without injury (for example, near miss, loss of driver licence)
Secondary outcomes
Intermediary outcomes (that may lead to a reduction in injuries) and outcomes that measured the consequences of injuries. These included:
behaviour change (that is, participation in treatment programme, or evidence of quitting the substance)
knowledge change regarding alcohol and/or drug misuse within organisational culture or individuals at work, generated by an alcohol and/or drug testing programme
attitude change (that is, within an organisation that may include labour relations, change in working culture or within individuals who are being studied before and after an alcohol and drug screening programme is introduced including stigmatisation)
sickness absence from work related to injury ‐ the change in the average number of sick leave absences
penalty imposed ‐ the change in the number of suspensions from duty or legal outcomes for example, change in the number of driving while intoxicated suspensions
Search methods for identification of studies
We did not restrict the searches by publication status, date, language or country.
Electronic searches
We searched:
MEDLINE (PubMed, 1950 to 28 May 2007)
EMBASE (1966 to 28 May 2007)
CENTRAL (to 29 May 2007)
Cochrane Injuries Group's specialised register (The Cochrane Library Issue 2, 2007)
Cochrane Occupational Health Field's specialised register (The Cochrane Library Issue 2, 2007)
DARE (The Cochrane Library Issue 2, 2007)
Economic Evaluations (The Cochrane Library Issue 2, 2007)
PsychINFO (1967 to 2007/02)
ERIC (1966 to 29 May 2007)
ETOH (1972 to 31 May 2007)
CISDOC/International Labour Organisation (ILO) (1987 to 2006/12)
NIOSH (1900 to 2006/12)
TRANSPORT (1972 to 25 May 2007)
Zetoc (1993 to 1 June 2007)
Science Citation Index and Social Science Citation index (1986 to 28 May 2007)
HSELINE national research register (1987 to 2006/12)
The search strategy for each database is described in Appendix 1.
Searching other resources
We contacted national and international agencies, and the authors of relevant studies, to identify additional studies possibly eligible for inclusion. In addition we hand searched the reference lists of studies screened for inclusion and searched the website of the US Department of Transportation (www.dot.gov) for eligible studies. We also hand searched all issues of Traffic Injury Prevention and Accident Analysis and Prevention up to June 2007. The date of the last search was June 2007.
Data collection and analysis
Selection of studies
The search strategies outlined above were carried out. Two review authors (CC and JR) undertook study selection where the authors screened abstracts and titles for relevance before retrieving the full texts. Both independently assessed whether the studies found met the pre‐defined inclusion criteria. We obtained the full text of all potentially relevant records and obtained further information from authors when a paper contained insufficient information for reaching a decision on eligibility.
Data extraction and management
Two review authors (CC and JR) independently extracted data from the included studies regarding the country where the study was conducted, the type of study design used, characteristics of the study participants (as per study inclusion criteria) and types of interventions and outcomes. A third author (JV) resolved any disagreements.
We intended to extract the following information about specific components of testing methods:
what biological sample was used for the test (e.g. breath, urine, blood, saliva, sweat, hair, nails);
how the test was carried out such as, on‐site testing test (approved protocol, tamper proof seal, chain of custody) or laboratory confirmation (gas chromatography/mass spectrometry);
what substance was tested for such as alcohol, cannabinoids, cocaine, amphetamines, opiates, benzodiazepines, phencyclidine, prescription drugs;
duration of follow‐up (RCT) or data collection in each period (CBA, ITS);
primary outcome measures: the change in number or injury or incidents or deaths;
secondary outcome measures: the change in the average number of sick days, the change in numbers of penalties incurred (for example, at work or by the legal system), change in behaviour, knowledge or attitude change;
cost: information about costs associated with implementing the intervention and relation to outcome(s).
However, only two studies (one of which was reported in two papers) met our inclusion criteria and they included information only on the schedule of data collection and on primary outcomes. One article addressed costs.
Although we contacted the authors for clarification, we were unable to obtain the relevant information about what samples or testing methods were used.
Assessment of risk of bias in included studies
Two review authors (CC and JR) independently assessed the methodological quality of the included studies. The two review authors independently rated the publications describing the included studies with the quality criteria for interrupted time series (ITS) study designs (Ramsay 2004). The two review authors then worked together and performed the rating a second time. All disagreements were resolved by discussion and by jointly clarifying the criteria used for assessment. In cases of persistent disagreement, a third author (JV) was involved in the decision.
The quality criteria for interrupted time series (ITS) study designs consists of an appraisal of studies in eight domains (Ramsay 2004):
Had the intervention occurred independently of other changes over time?
Was the intervention unlikely to affect data collection?
Was the primary outcome assessed blindly or measured objectively?
Was the primary outcome reliable or measured objectively?
Did the composition of the data‐set at each point in time cover at least 80% of the total number of participants in the study?
Was the shape of the intervention effect specified a priori?
Was a rationale for the number and spacing of data points described?
Was the study analysed appropriately using time‐series techniques?
We did not use the tool to derive a summary score of quality; instead we report how the study performed within each domain.
Publication bias
We considered addressing publication bias by means of a funnel plot and checking for asymmetry. However there were less than the required minimum of five studies available to be put in the funnel plot.
Measurement of intervention effect
Outcomes reported in Spicer 2005 were recalculated as number of injuries per 100 person years during a given time period. The scarcity of data reported in Swena 1999 prevented us from recalculating the reported numbers of fatal accidents per 100 million vehicle miles travelled into anything else. The results of the included studies were reanalysed as to both the change in level and change in trend after the intervention as previously described (Ramsay 2004).
Dealing with missing data
We contacted the study authors for any missing data. Additional information regarding study details and statistical data was sought and received from the authors. The results of this review are based on calculations performed using these data.
Data synthesis
For time‐series studies, data from the original papers were reanalysed according to the recommended methods for analysis of interrupted time‐series (ITS) designs for inclusion in systematic reviews (Ramsay 2004). These methods utilise a segmented time‐series regression analysis to estimate the effect of an intervention while taking into account secular time trends and any autocorrelation between individual observations. For each study, a first order autoregressive time‐series model was fit to the data using a modification of the parameterization of Ramsay 2004. Details of the mode specification are as follows:
Y= ß0+ ß1time+ ß2 (time‐p) I(time > p) +ß3 I(time > p)+ E, E˜ N(0, s2)
For time =1,...,T, where p is the time of the start of the intervention, I (time > =p) is a function which takes the value 1 if time is p or later and zero otherwise, and where the errors E are assumed to follow a first‐order autoregressive process (AR1). The parameters ß have the following interpretation: ß1 is the pre‐intervention slope. ß2 is the difference between post and pre‐intervention slopes. ß3 is the change in level at the beginning of the intervention period, meaning that it is the difference between the observed level at the first intervention time point and that predicted by the pre‐intervention time trend.
No pooling of data across studies was carried out because one study used measured data and the other used federal records that didn't show how many drivers the intervention affected.
We used a rating system, based on the Levels of Evidence (van Tulder 2003), to summarise the strength of scientific evidence of the effects of the intervention. The rating system was based on both the quality and the outcome of the studies as follows: I. Strong evidence ‐ consistent findings in multiple high quality RCTs or CCTs; II. Moderate evidence ‐ consistent findings in multiple low quality RCTS, CBAs, ITS and/or one high quality RCT; III. Limited evidence ‐ one low quality RCT or one CBA study or one ITS; IV. Conflicting evidence ‐ inconsistent findings in multiple trials; V. No evidence ‐ no trials.
Subgroup analysis and investigation of heterogeneity
There were insufficient data to perform a subgroup analysis according to the type of intervention (for example, pre‐employment testing, random testing, post‐incident testing).
Sensitivity analysis
We considered conducting sensitivity analyses to determine the impact of excluding studies with lower methodological quality. However, only two studies met the inclusion criteria for this review.
Methods for future updates
The review authors intend to perform a new search for eligible studies every two years and to update the review accordingly.
Results
Description of studies
Results of the search
Approximately 6000 potentially relevant publications were identified and screened for retrieval. Following assessment on the basis of title and abstract only 19 full text article publications were considered for inclusion in this review, and were scrutinised further with regard to our inclusion and exclusion criteria. Sixteen articles were excluded (Messer 1996; Beirness 2004; Taggart 1989; Spicer 2003; Zwerling 1990; Zwerling 1992; Gerber 2001; Lindseth 2001; Seijts 2005; Mumenthaler 2003; Zaloshnja 2006; Zaloshnja 2007; Peek‐Asa 1999; Kraus 2001; Jacobson 2003, Snowden 2007) (see 'Characteristics of excluded studies' table). Therefore, only two studies (Swena 1999 and Spicer 2005, published as two articles) met the inclusion criteria and were included in this review (see 'Characteristics of Included Studies' table and Figure 1).
1.
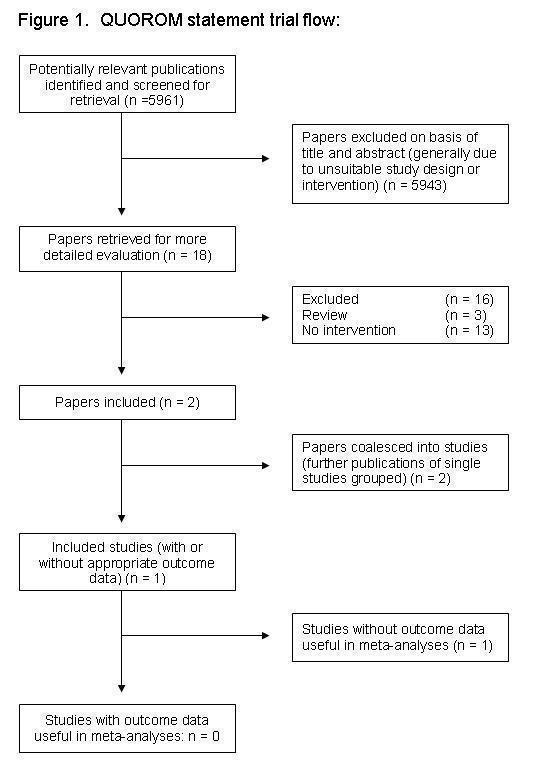
Figure 1 Trial flow.
Included studies
Two studies from the United States, of which one was reported in two publications, were included in this review (Swena 1999 and Spicer 2005).
Design of the study Spicer 2005 is an evaluation of a workplace peer‐focused substance abuse prevention and early intervention program (titled PeerCare) evaluated against the background of federally mandated random drug and alcohol testing in an interrupted time‐series design from 1983 to 1996. Because we were given access to the raw data we could focus our reanalysis on the testing interventions instead of the primary substance abuse prevention intervention. This voided the reported intervention versus control setup and made all study companies part of the intervention group. Spicer 2005 evaluated the effects of the PeerCare and testing interventions, and measured reportable injuries only, whereas another paper that used the same data (Miller 2007) measured both reportable and minor injuries and estimated the cost effectiveness of the PeerCare and testing interventions.
Swena 1999 is an evaluation of federally mandated random drug testing on fatal truck accidents in an interrupted time‐series design from 1983 to 1997. The data were obtained from the Fatality Analysis Reporting System database which is maintained by the National Highway Traffic Safety Administration.
Participants and duration of study In Spicer 2005, a retrospective analysis was conducted using cross‐sectional time‐series data to examine the association between occupational injury rate and (1) federally mandated drug testing and (2) federally mandated alcohol testing. The study duration was 13 years, from 1983 until 1996. The study population consisted of approximately 115,019 employees in five large interstate transport companies that carried passengers and/or cargo in the USA. The number of occupational injuries reported to the Federal government between January 1983 and June 1996, that were calculated as injuries per 100,000 employee‐hours, was tabulated monthly for the five companies (study and controls). Injuries were reportable to the Federal government if they resulted in (1) death or medical treatment and/or (2) restricted or lost workdays. In Miller 2007, injury data was available until 1999 and included reportable as well as not‐reportable injuries. These were generally minor injuries that were treated by a non‐health professional and did not result in lost work days.
Swena 1999 reports that the number of active truck drivers (i.e. number of participants exposed to the intervention) is not actually known with a sufficient degree of accuracy. The study duration was 14 years, from 1984 to 1997.
Types of interventions In the USA, federally mandated random drug testing for safety‐sensitive occupations in the transportation industry commenced on January 1st 1990 and random and for‐cause alcohol testing on August 15th 1994. Biological sampling and the quality of testing were outlined in the federal testing regulations to be interpreted by management of the employing organisation. The PeerCare intervention that did not fulfil our inclusion criteria was introduced in 1987. It was a union‐management partnership and training activity to recognize and intervene with problem (impaired) workers on‐the‐job, and to change attitudes to substance use in the workplace. In addition, in 1995 there was a safety restructuring procedure that affected one of the study companies.
Types of outcome measures The primary outcome measure in Spicer 2005 was the injury rate per 100,000 employee‐hours. The secondary outcomes were the costs of both program implementation and of occupational injuries. In Swena 1999 the primary outcome measure was the rate of large truck fatal accidents per 100 million vehicle miles travelled. A large truck was defined as weighing over 10,000 pounds gross vehicle weight, including single unit trucks and truck tractors.
Excluded studies
The main reasons for excluding the remaining sixteen identified studies were as follows (see table of 'Characteristics of excluded studies'):
(a) Inappropriate study design (i.e. not a randomised controlled trial (RCT), cluster‐randomised trial, controlled clinical trial (CCT), controlled before and after study (CBA) or interrupted time series studies (ITS) (Kraus 2001; Spicer 2003; Zwerling 1992; Gerber 2001; Peek‐Asa 1999; Taggart 1989; Jacobson 2003, Messer 1996)).
(b) Study did not evaluate the effects of alcohol or drug testing in reducing injuries (Zwerling 1990; Lindseth 2001; Seijts 2005; Beirness 2004; Mumenthaler 2003; Zaloshnja 2006; Zaloshnja 2007, Snowden 2007).
Risk of bias in included studies
Spicer 2005 met four of the quality criteria recommended for interrupted time‐series studies (Ramsay 2004):
The intervention was unlikely to affect data collection. As the main outcome was routinely collected data on injuries to be reported to the federal regulatory agency, it is unlikely that the introduction of drug and alcohol testing impacted on the way the data was collected. The authors indicated that they merged individual records with personnel files with negligible problems.
The primary outcome was assessed blindly or measured objectively. The injury figures were good objective measures of medium to serious injuries as they included only those injuries to be reported to the federal regulatory agency. Reportable injuries were defined by clear criteria (injuries that result in death, medical treatment and/or restricted or lost work days).
The primary outcome was reliable or measured objectively.
The composition of the data set at each point in time covered at least 80% of the total number of events in the study. As monthly official injury statistics were used we assume that these covered close to 100% of all events that happened in the particular month.
Spicer 2005 did not meet the remaining four criteria:
The shape of the intervention effect was not specified a priori. The study lacked specific hypotheses. Neither the expected effect of the random alcohol and drug testing nor the effect of the Peer Care programme were specified in advance.
The intervention had not occurred independently of other changes over time. The introduction of federally mandated drug testing (1990) followed by alcohol testing (1994) overlapped with the Peer Care intervention (1987) making it difficult to differentiate between the effects of the interventions. The workplace culture of the study companies is also likely to have changed in the pre‐intervention period when the US government changed Federal employment culture in 1986 by requiring employees to refrain from the use of illegal drugs. In addition, safety restructuring in one of the study companies in 1995 also overlapped with the drug and alcohol testing.
No rationale for the number and spacing of data points was described. However, the spacing of data points was pre‐set by the monthly injury data reporting and can be considered as sensitive enough to show changes in injuries over time due to the interventions. The period covered was probably long enough to reveal both immediate and long‐term post‐intervention effects on injuries.
The main emphasis of the study was on evaluating the effect of the Peer Care programme rather than random alcohol or drug testing. Therefore the applied analyses were not relevant for isolating the effects of random drug and alcohol testing from the effects of the Peer Care programme.
Weaknesses in the study are indicated by a lack of data on post‐accident drug and alcohol tests from the period prior to the workplace intervention. Separate analysis of subgroups was not possible.
Swena 1999 also met four of the quality criteria recommended for interrupted time‐series studies (Ramsay 2004):
The intervention was unlikely to affect data collection. As the main outcome was routinely collected data on injuries to be reported to the federal regulatory agency it is unlikely that the introduction of drug testing impacted on the way the data was collected.
The primary outcome was assessed blindly or measured objectively. The accident rate figures were good objective measures. Reportable injuries were defined by clear criteria (injuries that result in death).
The primary outcome was reliable or measured objectively.
The composition of the data set at each point in time did cover at least 80% of the total number of events in the study. As monthly official injuries statistics were used we assume that these covered close to 100% of all events that happened in the particular month.
Swena 1999 did not meet the remaining four criteria.
The shape of the intervention effect was not specified a priori. The study lacked specific hypotheses. The expected effect of the random drug testing programme was not specified in advance.
No rationale for the number and spacing of data points was described. The period covered was probably long enough to reveal both immediate and long‐term post‐intervention effects on injuries.
Most likely the intervention did not occur independently of other changes over time because it is not known who were actually affected by the intervention and to what degree. If one assumes that the data represent all large interstate truck drivers then one can also assume that these individuals were also subjected to various limitations, rules, etc. No other influences apart from drug testing were considered in the study.
The study was analyzed appropriately as to the immediate effect but did not take into account the possibility of auto‐correlation of the data. The change in fatality rate per 100 million vehicle miles travelled was modelled by linear regression over the years 1984 to 1989. These were then extrapolated over the following years. In other words, the authors compared the scores following the introduction of the intervention to those that would have been expected based on the scores from before the intervention instead of comparing pre‐intervention scores with post‐intervention scores. There was no analysis of the long‐term effect.
Effects of interventions
Mandatory alcohol testing versus no alcohol testing
Immediate effect on injury level
In Spicer 2005, mandatory random and for‐cause alcohol testing was associated with a decrease in the level of injuries immediately following the intervention (‐1.25 injuries/100 person years, 95% CI ‐2.29 to ‐0.21)
Long‐term change in time‐trend of injury level
In Spicer 2005, there was no significant change in the already downward trend (‐0.28 injuries/100 person years/year, 95% CI ‐0.78 to 0.21) (see Figure 2).
2.

Figure 2 Injury rate in Spicer 2005.
Mandatory drug testing versus no drug testing
Immediate effect on injury level
In Spicer 2005, mandatory random drug testing was associated with a statistically significant increase in injury level following the intervention (1.26 injuries/100 person years, 95% CI 0.36 to 2.16). In Swena 1999 there was no immediate statistically significant effect for mandatory random drug testing (‐1.36/injuries/100 person years, 95% CI ‐1.69 to 0.41) (see Figure 3).
3.

Figure 3 Rate of large truck fatal accidents in Swena 1999
Long‐term change in time‐trend of injury level
In Spicer 2005, the intervention was associated with a significant decline of the yearly injury rate additional to the already downward trend over time (‐0.19 injuries/100 person years/year, 95% CI ‐0.30 to ‐0.07). Also in Swena 1999 the intervention was associated with a significant further improvement of the downward trend (‐0.83 fatal accidents/100 million vehicle miles/year, 95% CI ‐1.08 to ‐0.58).
Cost‐benefit ratio
Miller 2007 (under Spicer 2005) reported the costs of the drug and alcohol testing interventions and the estimated costs ($US) of the avoided injuries at one transportation company. The drug and alcohol testing interventions cost altogether $35 per employee and together with the peer worker mediated substance abuse program, which cost another $35 per employee, avoided an estimated $1850 in employer injury costs per employee in 1999, corresponding to a benefit‐cost ratio of 1:26.
Discussion
We found no randomised trials of the effects of drug or alcohol testing of drivers for reducing injuries. The two included studies were interrupted time‐series studies conducted in the USA. These studies provide limited evidence that mandatory random drug testing can decrease injuries in the long term although the results in the short term were contradictory. In one study, the effect size of the continuous drop of 0.19 injuries per 100 person years was small although the estimate can be considered as fairly precise with 95% confidence intervals ranging from 0.30 to 0.07. Another study found that mandatory random drug testing can increase the downward trend of the rate of fatal accidents by ‐0.83 fatal accidents per 100 million vehicle miles travelled per year. The immediate drop in level of injuries (1.25 injuries/100 person years) after the implementation of mandatory random and for‐cause alcohol testing in the Spicer 2005 study can be judged as substantial although fairly imprecise. No change in the long‐term slope ‐ additional to the already downward trend ‐ could be shown following this intervention. This could be due to the limited number of measurement points after the implementation of alcohol testing in 1994, thereby compromising statistical power. The change in the long term slope following the implementation of random drug testing in Swena 1999 can only be seen as an approximation of the effect of the intervention because the size of the population represented by this data is not known.
The Spicer 2005 study also assessed the effects of a peer‐worker mediated workplace substance abuse programme (PeerCare) on the background of federally mandated drug and alcohol testing. Because of the overlap of these three interventions the independent effects of the testing interventions are difficult to differentiate.
According to the same study (publication Miller 2007) drug and alcohol testing interventions may also be cost‐effective, at least in the US. However, the figures are based on overall company costs that, according to the authors, did not include some relevant costs like those of a pre‐existing employee assistance program. The authors also do not describe the testing regimes in sufficient detail to allow comparisons with the costs expected in the healthcare systems of other countries. For this reason we did not try to adjust the figures for inflation or currency. Since we did not include in our systematic search strategy items or specialist databases addressing economic evaluation it is possible that we may have overlooked studies and data other than those conducted alongside effectiveness studies. The two included studies were both conducted in the USA and so it is unclear how the results might apply to Europe or to low and middle income countries.
The excluded studies either used ITS study designs that did not satisfy our inclusion criteria (i.e. less than three time points measured before and after the study), or they did not relate substance testing with number of injuries.
A strong aspect of our time‐series analysis is that it adjusted for secular and other cyclical changes in the auto‐regressive time‐series model. This is especially pertinent with this review as the past fifty years have shown a rather steady downward trend in injuries. Nonetheless, a clear drawback of the time‐series design is that it is susceptible to bias as introduced by co‐interventions (interventions that are introduced concurrently), as well as the determination of the point in time where the intervention is introduced and the type of effect the intervention can have over time. Our recalculations of the results consider only one intervention at a time by comparing all data points preceding the intervention to those following it.
It was not possible to assess the extent to which publication bias may have been present due to the small number of included studies. We attempted to reduce the likelihood of language bias by not having language restrictions in the systematic search strategy.
Cluster‐randomised trials are needed to better address the effects of interventions for injury prevention in this occupational setting.
Comparison with other reviews
We found no previous systematic or narrative reviews of the effects of drug or alcohol testing to reduce injuries specifically in drivers. The review by Kraus 2001 about the effects of drug testing to decrease injuries in nonspecific workplaces concluded that: "...the published evidence for effects such as reduced injury or accident rates lacks scientific detail". In another systematic review about injury prevention in a different occupational setting, the construction industry (van der Molen 2007), an intervention aiming at a drug‐free workplace evaluated with an interrupted time‐series design in a large company was shown to be effective in reducing the level and the trend of injuries over time. The interrupted time‐series design therefore seems to be feasible in evaluating interventions that aim to prevent injuries in the workplace. A standardised approach to analysis and reporting is needed to be able to compare and possibly synthesize data across studies.
Authors' conclusions
Implications for practice.
There is insufficient evidence to advise for or against the use of drug and alcohol testing of occupational drivers for preventing injuries as a sole, effective, long‐term solution in the context of workplace culture, peer interaction and other local factors.
Implications for research.
Given the widespread practice of alcohol and drug testing and the paucity of evaluation studies found, more evaluation studies are needed. Interrupted time‐series is a feasible study design for evaluating interventions that aim at preventing alcohol and drug related injuries. However, time‐series studies of higher quality and of sufficient duration are needed to increase the level of evidence. A cluster‐randomised trial would be the ideal study design to evaluate the effects of interventions for injury prevention in this occupational setting.
Acknowledgements
Merja Jauhiainen from the Cochrane Occupational Health Field for conducting most of the database searches. Karen Blackhall from the Cochrane Injuries Group for assistance with database searches.
Appendices
Appendix 1. Search strategy
The search string for randomised controlled trials was based on Robinson 2002.
PubMed search strategy (to 28.5.2007)
#1 drug* OR cannabi* OR opia* OR cocaine OR amphetamine* OR phencyclidine* OR benzodiazepine* OR alcohol OR medication* OR prescription* OR medicament* OR pharmaceutical* OR sedative* OR intoxicat* OR drunk* OR drink* OR "substance abuse" OR marijuana OR DUI OR DWI #2 (lorry OR lorries OR truck OR trucks OR bus OR buses OR van OR vans OR tram OR trams OR train OR trains OR railroad OR railroads OR taxi OR taxis) AND (driver*) #3 (lorry OR lorries OR truck OR trucks OR bus OR buses OR van OR vans OR tram OR trams OR train OR trains OR railroad OR railroads OR taxi OR taxis) AND (driving) #4 captain OR seafarer* OR sailor* OR seaman #5 pilot* AND (airline* OR aviation OR airplane* OR aircraft OR aeroplane* OR airship*) #6 pilots #7 commercial* AND (drive* OR driving) #8 (driver* OR driving) AND (worker* OR working* OR occupation*) #9 #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 #10 #1 AND #9 #11 randomized controlled trial [pt] OR controlled clinical trial [pt] OR randomized controlled trials [mh] OR random allocation [mh] OR double‐blind method [mh] OR single‐blind method [mh] OR clinical trial [pt] OR clinical trials [mh]) OR ("clinical trial" [tw]) OR ((singl* [tw] OR doubl* [tw] OR trebl* [tw] OR tripl* [tw]) AND (mask* [tw] OR blind* [tw])) OR (placebos [mh] OR placebo* [tw] OR random* [tw] OR research design [mh:noexp] OR comparative study OR evaluation studies [mh] OR follow‐up studies [mh] OR prospective studies [mh]) NOT (animals [mh] NOT human [mh]) #12 (effect* [tw] OR control* [tw] OR evaluation* [tw] OR program* [tw]) #13 #11 OR #12 #14 #10 and #13
EMBASE (to 28.5.2007)
#1 randomized controlled trial/exp OR randomization/exp OR clinical trial/exp OR clinical trials/exp OR controlled study/exp OR double blind procedure/exp OR single blind procedure/exp OR ((singl* OR doubl* OR trrbl* OR tripl*) AND (mask* OR blind*)) OR placebo*OR comparative study/exp OR research design/exp OR evaluation study OR evaluation studies/exp OR follow up/exp OR prospective study/exp OR effect* OR control* OR evaluation/exp OR program* #2 drug/exp OR drugs/exp OR cannabi* OR opia* OR cocaine* OR amphetamine* OR phencyclidine* OR benzodiapine* OR alcohol/exp OR medication* OR presciption* OR medicament* OR pharmaceutical* OR sedative* OR intoxicat* OR drunk* OR drink* OR "substance abuse"/exp OR marijuana/exp OR dui OR dwi #3 (lorry OR lorries OR truck OR trucks OR bus OR buses OR van OR vans OR tram OR trams OR train/exp OR trains OR railroad/exp OR railroads/exp OR taxi OR taxis OR commercial* OR worker* OR working OR occupation*) AND (driver* OR driving) OR ((pilot* AND (airline* OR aviation/exp OR airplane* OR aircraft* OR aeroplane* OR airship*)) OR captain* OR seafarer* OR sailor' OR seaman/exp OR pilots* #4 nonmedical occupations/exp #5 #1 AND #2 OR #3 OR #4 #6 #5 LIMIT humans AND LIMIT/embase
SCI & SSCI (Web of Science) (to 28.5.2007)
#1 random* OR "controlled clinical" OR "clinical trial*" OR "double blind*" OR "single blind*" OR ((singl* OR doubl* OR trebl* OR tripl*) AND (mask* OR blind*)) OR placebo* OR "research design" OR comparativ* OR evaluation* OR "follow up" OR prospectiv* OR effect* OR control* OR evaluation* OR program* #2 drug OR drugs OR cannabi* OR opia* OR cocaine* OR amphetamine* OR phencyclidine* OR benzodiazepine* OR alcohol* OR medication* OR prescription* OR medicament* OR pharmaceutical* OR sedative* OR intoxicat* OR drunk* OR drink* "substance abuse" OR marijuana OR dui OR dwi) #3 (lorry OR lorries OR truck OR trucks OR bus OR buses OR van OR vans OR tram OR trams OR train/exp OR trains OR railroad/exp OR railroads/exp OR taxi OR taxis OR commercial* OR worker* OR working OR occupation*)) AND (driver OR drivers OR driving) OR captain* OR seafarer* OR sailor' OR seaman/exp OR pilots* #5 #1 AND #2 AND #3
NIOSHTIC2, CISDOC and HSELINE (Silverplatter) (to 28.5.2007)
#1 random* or control* or allocation or double‐blind or single‐blind or clinical or "research design" or "follow up" or ((singl* or doubl* or trebl* or tripl*) and (blind* or mask*)) or placebo* or comparativ* or evaluation or follow‐up or prospectiv* or effect* or control* or evaluation* or program* #2 drug or drugs or cannabi* or opia* or cocaine* or amphetamine* or phencyclidine* or benzodiazepine* or alcohol* or medication* or prescription* or pharmaceutical* or sedative* or intoxicat* or drunk* or drink* or marijuana or dui or dwi or "substance abuse" #3 captain* or seafarer* or sailor* or seaman or pilots or ((drive* or driving) and (lorry or lorries or truck or trucks or bus or buses or van or vans or tram or trams or train or trains or railroad* or taxi or taxis or commercial* or worker* or working or occupation*)) or ((pilot* and (airline* or aviation or airplane* or aircraft* or aeroplane* or airship*)) #4 #1 AND #2 AND #3
PschINFO (Silverplatter) (to 29.5.2007)
#1 random* or control* or "clinical trial" or "clinical trials" or "double blind" or "single blind" or ((singl* or doubl* or trebl* or tripl*) and (mask* or blind*)) or placebo* or "research design" or comparativ* or "follow up" or prospectiv* or effect* or control* or evaluation* or program* #2 drug or drugs or cannabi* or opia* or cocaine* or amphetamine* or phencyclidine* or benzodiazepine* or alcohol* or medication* or prescription* or medicament* or pharmaceutical* or sedative* or intoxicat* or drunk* or drink* or "substance abuse" or marijuana or dui or dwi #3 captain* or seafarer* or sailor* or seaman or pilots or ((driver* or driving) and (lorry or lorries or truck or trucks or bus or buses or van or vans or tram or trams or train or trains or railroad* or taxi or taxis or commercial* or worker* or working or occupation*)) #4 #1 AND #2 AND #3
Cochrane Library (Wiley InterScience) (to 29.5.2007)
#1 (drug or drugs or cannabi* or opia* or cocaine* or amphetamine* or phencyclidine* or benzodiazepine* or alcohol* or medication* or prescription* or medicament* or pharmaceutical* or sedative* or intoxicat* or drunk* or drink* or "substance abuse" or marijuana or dui or dwi ):tw,ab,kw. #2 ((driver* or driving) and (lorry or lorries or truck or trucks or bus or buses or van or vans or tram or trams or train or trains or railroad* or taxi or taxis or commercial* or worker* or working or occupation*)) or captain* or seafarer* or sailor* or seaman or pilots or ((pilot* and (airline* or aviation* or airplane* or aircraft* or aeroplane* or airship*)) #3 #1 AND #2
ERIC (ProQuest CSA) (to 29.5.2007)
#1 random* or clinical* or allocation or placebo* or ((singl* or doubl* or trebl* or tripl*) and (blind* or mask*)) or comparativ* or evaluation or follow‐up or prospectiv* or effect* or control* or evaluation* or program* #2 drug* or cannabi* or opia* or cocaine* or amphetamine* or phencyclidine* or benzodiazepine* or alcohol* or medication* or prescription* or medicament* or pharmaceutical* or sedative* or intoxicat* or drunk* or drink* or "substance abuse" or marijuana or dui or dwi #3 (driver* or driving) and (lorry or lorries or truck or trucks or bus or buses or van or vans or tram or trams or train or trains or railroad* or taxi or taxis or commercial* or worker* or working or occupation* or commercial)) or captain* or seafarer* or sailor* or seaman or pilots or ((pilot* or driver* or driving) and (airline* or aviation* or airplane* or aircraft* or aeroplane* or airship*)) #4 #1 and #2 and #3
ETOH (etoh.niaa.nih.gov) (to 31.5.2007)
Because of the limitations of the interface each term had to be searched separately from this database.
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Spicer 2005.
| Methods | Time‐series study with control. | |
| Participants | 115,019 employees in five large interstate transport companies that carried passengers and/or cargo. | |
| Interventions | 1986 Change in employment requirements for federal employees. 1987 Peer‐worker mediated substance abuse program (Peercare) introduced. 1990 Federal mandate for random drug testing. 1994 Federal mandate for random and for‐cause alcohol testing introduced. 1995 Safety restructuring in one study company. |
|
| Outcomes | Injuries per 100,000 employee hours. | |
| Notes | Same study as Miller 2007 but with slightly different variables. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | High risk | |
Swena 1999.
| Methods | Retrospective time‐series study on large truck drivers' fatal accident data obtained from the Federal Highway Administration. | |
| Participants | The number of active truck drivers that were subjected to the intervention is not known. | |
| Interventions | Random drug testing. | |
| Outcomes | Fatality rate per 100 million vehicle miles travelled. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | High risk | |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Beirness 2004 | Review about the effectiveness of alcohol ignition interlock programs. |
| Gerber 2001 | Prevalence study. |
| Jacobson 2003 | Prevalence study. |
| Kraus 2001 | Review about the effectiveness of drug testing interventions in mixed occupational settings. |
| Lindseth 2001 | No control group. |
| Mumenthaler 2003 | Comparison of specific psychoactive drugs on pilot performance; Intermediate measure used as outcome (flight simulator tests). |
| Peek‐Asa 1999 | Review about the effectiveness of randomly stopping and breath testing drivers to deter from drinking and driving. |
| Seijts 2005 | Review of perceptions toward testing. |
| Snowden 2007 | Case ‐ control study. |
| Spicer 2003 | Prevalence study. |
| Taggart 1989 | Interrupted time‐series study without three measurements before the introduction of the intervention. |
| Wickizer 2004 | Quasi‐ experimental; not specific for drug/alcohol intervention. |
| Zaloshnja 2006 | Cost estimate study. |
| Zaloshnja 2007 | Cost estimate study. |
| Zwerling 1990 | Cost estimate study. |
| Zwerling 1992 | Cost estimate study. |
Differences between protocol and review
The inclusion criteria and the instrument for judging study quality were changed.
In the protocol we stated that we would include interrupted time‐series (ITS) studies only when they used a control group. When conducting the review proper, we soon realised this was contradictory to our initial intention of including properly conducted ITS studies. According to our definition, ITS studies have been conducted properly when they have conducted at least three outcome measurements before and after the intervention. The inclusion of a control group is therefore of less importance. The idea behind ITS studies is to compare the situation before an intervention to the situation following its implementation (rather than intervention vs. control). We implemented this correction to the review inclusion criteria before we had an idea what this would do to the results. Therefore ITS studies without a control group, but with three outcome measurements before and after the intervention, were included.
From other reviews using ITS studies (van der Molen 2007) we learned that there was a better instrument for judging quality (Ramsay 2004) and that we should use that instrument instead of the one we had chosen (Downs 1998). The Downs 1998 checklist was initially chosen because in addition to randomised controlled trials it could also be applied to (non‐randomised) controlled clinical trials. Since no randomised controlled trials or controlled clinical trials were included in the review we don't think this biased the results.
Contributions of authors
Clodagh Cashman conceptualised the review, took the lead in writing the protocol and wrote the sections collaborating with Jos Verbeek, Jani Ruotsalainen, Birgit Greiner and Paul Beirne.
Jos Verbeek and Jani Ruotsalainen designed the systematic search strategies in collaboration with the Cochrane Occupational Health Field and Karen Blackhall of the Cochrane Injuries Group.
Sources of support
Internal sources
University College Cork, Ireland.
External sources
Health Research Board, Ireland.
Finnish Institute of Occupational Health, Finland.
Declarations of interest
None known.
New
References
References to studies included in this review
Spicer 2005 {published data only}
- Miller TR, Zaloshnja E, Spicer RS. Effectiveness and benefit‐cost of peer‐based workplace substance abuse prevention. Accident; analysis and prevention 2007;39(3):565‐73. [DOI] [PubMed] [Google Scholar]
- Spicer RS, Miller TR. Impact of a workplace peer‐focused substance abuse prevention and early intervention program. Alcoholism, clinical and experimental research 2005;29(4):609‐11. [DOI] [PubMed] [Google Scholar]
Swena 1999 {published data only}
- Swena DD. Effect of Random Drug Screening on Fatal Commercial Truck Accident Rates. International Journal of Drug Testing 1999;2:1‐13. [Google Scholar]
References to studies excluded from this review
Beirness 2004 {published data only}
- Beirness DJ, Marques PR. Alcohol ignition interlock programs. Traffic injury prevention 2004;5(3):299‐308. [DOI] [PubMed] [Google Scholar]
Gerber 2001 {published data only}
- Gerber JK, Yacoubian GS. An assessment of drug testing within the construction industry. Journal of drug education 2002;32(1):53‐68. [DOI] [PubMed] [Google Scholar]
Jacobson 2003 {published data only}
- Jacobson M. Drug testing in the trucking industry: the effect on highway safety. Journal of Law and Economics 2003;XLVI:131‐56. [Google Scholar]
Kraus 2001 {published data only}
- Kraus JF. The effects of certain drug‐testing programs on injury reduction in the workplace: an evidence‐based review. International journal of occupational medicine and environmental health 2001;7(2):103‐8. [DOI] [PubMed] [Google Scholar]
Lindseth 2001 {published data only}
- Lindseth PD, Vacek JJ, Lindseth GN. Urinalysis drug testing within a civilian pilot training program: did attitudes change during the 1990's?. Aviation, Space and Environmental Medicine 2001;72(7):647‐51. [PubMed] [Google Scholar]
Mumenthaler 2003 {published data only}
- Mumenthaler MS, Yesavage JA, Taylor JL, O'Hara R, Friedman L, Lee H, Kraemer HC. Psychoactive drugs and pilot performance: a comparison of nicotine, donepezil, and alcohol effects. Neuropsychopharmacology 2003;28(7):1366‐73. [DOI] [PubMed] [Google Scholar]
Peek‐Asa 1999 {published data only}
- Peek‐Asa C. The effect of random alcohol screening in reducing motor vehicle crash injuries. American journal of preventive medicine 1999;16(1 Suppl):57‐67. [DOI] [PubMed] [Google Scholar]
Seijts 2005 {published data only}
- Seijts, G.H, O'Farrell, G. Urine Collection Jars Versus Video Games: Perceptions of Three Stakeholder Groups toward Drug Testing and Impairment Testing Programs. Journal of Drug Issues 2005;35:885‐916. [Google Scholar]
Snowden 2007 {published data only}
- Snowden C, Miller TR, Waehrer GM, Spicer RS. Random alcohol testing reduced alcohol‐involved fatal crashes of drivers of large trucks. Journal of Studies on Alcohol and Drugs 2007;68(5):634‐40. [DOI] [PubMed] [Google Scholar]
Spicer 2003 {published data only}
- Spicer RS, Miller TR, Smith GS. Worker substance use, workplace problems and the risk of occupational injury: a matched case‐control study. Journal of studies on alcohol 2003;64(4):570‐8. [DOI] [PubMed] [Google Scholar]
Taggart 1989 {published data only}
- Taggart RW. Results of the drug testing program at Southern Pacific Railroad. NIDA research monograph 1989;91:97‐108. [PubMed] [Google Scholar]
Wickizer 2004 {published data only}
- Wickizer T, Kopjar B, Franklin G, Joesch J. Do drug‐free workplace programs prevent occupational injuries? Evidence from Washington State. Health Services Research 2004;39(1):91‐110. [DOI] [PMC free article] [PubMed] [Google Scholar]
Zaloshnja 2006 {published data only}
- Zaloshnja E, Miller T. The employer costs of motor vehicle crashes. International journal of injury control and safety promotion 2006;13(3):145‐50. [DOI] [PubMed] [Google Scholar]
Zaloshnja 2007 {published data only}
- Zaloshnja E, Miller TR, Hendrie D, Galvin D. Employer costs of alcohol‐involved injuries. American journal of industrial medicine 2007;50(2):136‐42. [DOI] [PubMed] [Google Scholar]
Zwerling 1990 {published data only}
- Zwerling, C. Ryan, J. Orav, E. J. The efficacy of preemployment drug screening for marijuana and cocaine in predicting employment outcome. Journal of the American Medical Association. 1990;264(20):2639‐43. [PubMed] [Google Scholar]
Zwerling 1992 {published data only}
- Zwerling C, Ryan J, Orav EJ. Costs and benefits of preemployment drug screening. Journal of the American Medical Association 1992;267(1):91‐3. [PubMed] [Google Scholar]
Additional references
Cunradi 2005
- Cunradi CB, Ragland DR, Greiner B, Klein M, Fisher JM. Attributable risk of alcohol and other drugs for crashes in the transit industry. Injury Prevention 2005;11(6):378‐82. [DOI] [PMC free article] [PubMed] [Google Scholar]
Downs 1998
- Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non‐randomised studies of health care interventions. Journal of epidemiology and community health 1998;52(6):377‐84. [PUBMED: 9764259] [DOI] [PMC free article] [PubMed] [Google Scholar]
Fernandez 2006
- Fernandez WG, Hartman R, Olshaker J. Brief interventions to reduce harmful alcohol use among military personnel: lessons learned from the civilian experience. Military Medicine 2006;171(6):538‐43. [DOI] [PubMed] [Google Scholar]
Francis 2003
- Francis P, Hanley N, Wray D. A literature review on the international state of knowledge of drug testing at work with particular reference to the US on behalf of the Independent Inquiry on Drug Testing at Work. University of Northumbria 2003.
French 2004
- French MT, Roebuck MC, Kebreau Alexandre P. To test or not to test: do workplace drug testing programs discourage employee drug use?. Social Science Research 2004;33:45‐63. [DOI] [PubMed] [Google Scholar]
Gerber 2002
- Gerber JK, Yacoubian GS Jr. An assessment of drug testing within the construction industry. Journal of Drug Education 2002;1:53‐68. [DOI] [PubMed] [Google Scholar]
Grayson 2004
- Grayson JK, Gibson RL, Shanklin SL, Neuhauser KM, McGhee. Trends in Positive Drug Tests, United States Air Force, Fiscal Years 1997‐1999. Military Medicine 2004;169(7):499‐504. [DOI] [PubMed] [Google Scholar]
Higgins 2005
- Higgins JPT, Green S editors. Cochrane Handbook for Systematic Reviews of Interventions 4.2.5 [updated May 2005] issue 3. The Cochrane Library. Chichester, UK: John Wiley & Sons, Ltd, 2005. [Google Scholar]
Hope 2005
- Hope A, Gill A, Costello G, Sheehan J, Brazil E, Reid V. Alcohol and injuries in the accident and emergency department – a national perspective. Dublin: Department of Health and Children, 2005. [Google Scholar]
IIDTW 2004
- Independent Inquiry into Drug Testing at Work. Drug testing in the workplace: The report of the Independent Inquiry into Drug Testing at Work. Joseph Rowntree Foundation 2004.
Levine 2004
- Levine MR, Rennie WP. Pre‐employment urine drug testing of hospital employees: future questions and review of current literature. Occupational and Environmental Medicine 2004;61:318‐24. [DOI] [PMC free article] [PubMed] [Google Scholar]
Messer 1996
- Messer, D. An empirical evaluation of the legal assumptions underlying workplace‐based drug and alcohol testing: results from a comparison of random and non‐random testing programs at a large transportation agency. UMI Dissertation Services, Ann Arbor, Michigan;. UMI Company, Ann Arbor, MI, 1996.
Ozminkowski 2003
- Ozminkowski RJ, Mark TL, Goetzel RZ, Blank D, Walsh JM, Cangianelli L. Relationships between urinalysis testing for substance use, medical expenditures, and the occurrence of injuries at a large manufacturing firm. American Journal of Drug and Alcohol Abuse 2003;29(1):151‐67. [DOI] [PubMed] [Google Scholar]
Ramsay 2004
- Ramsay C, Matowe L, Grilli R, Grimshaw J, Thomas R. Interrupted times series designs in health technology assessment: lessons from two systematic reviews of behavior change strategies. International Journal of Technology Assessment in Health Care 2003;19(04):613‐23. [DOI] [PubMed] [Google Scholar]
Robinson 2002
- Robinson KA, Dickersin K. Development of a highly sensitive search strategy for the retrieval of reports of controlled trials using PubMed. International Journal Epidemiology 2002;31(1):150‐3. [DOI] [PubMed] [Google Scholar]
Rodgers 2004
- Rodgers A, Ezzati M, Vander Hoorn S, Lopez AD, Lin RB, Murray CJ, Comparative Risk Assessment Collaborating Group. Distribution of major health risks: findings from the Global Burden of Disease study. Public Library of Science Medicine. Epub 2004;1(1):e27. [DOI] [PMC free article] [PubMed] [Google Scholar]
Rothstein 1991
- Rothstein M. Workplace drug testing: a case study in the misapplication of technology. Harvard Journal of Law and Technology 1991;5:65‐93. [Google Scholar]
Smith 2004
- Smith A, Wadsworth E, Moss S, Simpson S. The scale and impact of illegal drug use by workers. Health and Safety Executive, London 2004.
Spiehler 1994
- Spiehler V. Drug screening in the USA. Bandolier 1994; Vol. 5.
van der Molen 2007
- Molen HF, Lehtola MM, Lappalainen J, Hoonakker PL, Hsiao H, Haslam R, et al. Interventions for preventing injuries in the construction industry. Cochrane Database of Systematic Reviews 2007, Issue 4. [DOI: 10.1002/14651858.CD006251.pub2] [DOI] [PubMed] [Google Scholar]