

Abstract
This short report shares learning from the research and development phase of the national decision support programme in NHS Scotland. It outlines how the programme has adopted an outcomes-focused approach which has guided critical decisions on solution design, engagement of policy sponsors, clinical and management leaders, implementation and evaluation approach, technical architecture and technology development. It discusses how this outcomes-led approach positions decision support as catalyst for a learning health and care system that continuously refreshes the healthcare knowledge base through new insights generated by evaluating impact and outcomes.
Keywords: computer methodologies, information management, medical informatics, patient care
Introduction
Scotland’s national decision support programme has been underway since April 2017. It is led by the Scottish Government Digital Health and Care Directorate, to deliver on a key objective within Scotland’s Digital Health and Care Strategy1—“expand knowledge mobilisation and decision support tools and services for self-management, shared decisions, and frontline practice in health and social care”. Programme management responsibility sits with the Digital Health and Care Institute.
The programme is currently in research and innovation phase. It is building insights and defining direction of travel through iterative development and evaluation. This short overview shares key learning to date.
Methods
Outcomes-focused approach
A guiding light from an early stage has been the need to focus on outcomes rather than technology as the driving force. As outlined below, this outcomes focus has determined our approach to solution design, technical delivery, implementation and evaluation.
It has led us to develop decision support for critical service priorities where national strategy indicates a need to improve care and reduce unwarranted variation, harm and waste. Initial developments are sponsored by policy leads for service transformation programmes in diabetes, polypharmacy resulting from comorbidities, and chronic pain and antimicrobial prescribing. A second phase of work is progressing decision support to deliver other essential outcomes—addressing waiting times through improved referral management in orthopaedics and gastroenterology, and supporting management of palliative care at home.
User-centred design
Engaging with the practitioners and patients who will use our decision support solutions in daily life is of paramount importance for decision support to realise its potential impact. Each decision support development has a designated clinical lead, a product owner and a user reference group.
We use service design principles and participatory design with stakeholders to understand users’ stories and identify the pressure points in care processes where decision support will have maximum effect. We then apply standards for usability, technology design and development, quality management and risk management standards using Agile development methodology. These approaches aim to maximise use of decision support through a consistently good user experience that takes account of human factors and human–computer interaction.
Technology approach
We have learnt that delivering impact at scale, in the complex health and care environment, with rapidly changing technology, requires a whole systems approach. We have therefore started to scope a co-ordinated technology framework to facilitate harmonised, joined up development across partners in health, academia and industry.
Results
Decision support tools
Flagship tools delivered to date include mobile apps and websites for polypharmacy, antimicrobial prescribing and gastrointestinal care pathways, and conversion of elements of chronic pain and polypharmacy guidance into person-specific, intelligent decision support integrated into the context of individual patient records in primary care systems. These are currently being evaluated in operational test environments.
Cross-cutting outcomes supported by all these decision support tools include improving self-management, shared decision-making between patient and professional, and co-ordination of care around individual patient needs. These are all priorities for Realistic Medicine.2
Implementation and evaluation framework
To design decision support solutions and implementation approach to maximise impact, we have developed a sociotechnical evaluation framework to identify the barriers and enablers to implementation.3
To keep implementation focused on impact of decision support on key outcomes, we aim to integrate enablers and barriers into an outcomes chain based on evidence of cause–effect relationships. Indicators are specified for key enablers and outcomes at multiple levels and are measured throughout iterative improvement cycles. This will enable us to continuously improve our decision support tools and implementation approach.
Technology architecture
Key aspects of the co-ordinated national technology architecture developed through the decision support programme to date are illustrated in figure 1:
Figure 1.
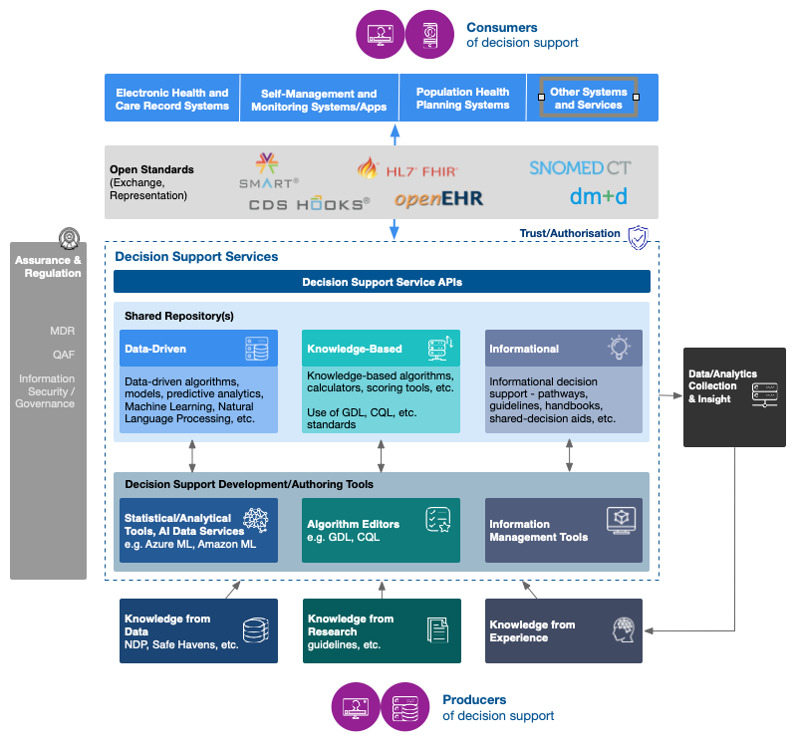
Emerging thinking around a co-ordinated technical architecture, underpinned by assurance for safety, quality, ethics, information governance and information security. This brings together decision support from dispersed organisations to deliver consistent high-quality care to individual patients across all stages of their journey. For example, a patient with low back pain may need knowledge-based decision support for self-management, prescribing, other therapies and referral management in primary care, as well as rules-based imaging requesting and data-driven AI decision support to interpret imaging results in secondary care.
(1) Shared, open repository of quality assured decision support models, algorithms and content. This will provide a ‘once for Scotland’ single source of truth for decision support. Algorithms can be shared, re-used, localised, combined, and integrated into different clinical systems and applications through an integrated service layer. A national co-ordinating framework has been developed which outlines the intention to converge over time on open digital standards for decision support.
(2) A spectrum of decision support tools—informational to intelligent. The existing evidence base indicates that maximum impact is delivered by intelligent, knowledge-based expert systems. These integrate decision support algorithms with electronic health record systems and proactively push patient-specific calls to action to the user.4
At the same time, learning from developments so far indicates that it is important to continue to support freestanding and informational solutions such as mobile apps and websites. These simpler solutions are quicker to implement at scale and NHS Scotland survey results indicate that they are widely used in health and care services. For the medium-term to long-term future, we are also exploring next-generation data-driven artificial intelligence methods where the potential is great and the evidence still emergent.
(3) A self-service model. To enable health and care services to build quality-assured decision support solutions to support outcomes identified as priorities in their own organisations. These tools are currently being piloted in early adopter organisations, accompanied by skills training for key staff.
Discussion—the way forward
The outcomes-led approach which has evolved through the research and innovation phase of the decision support programme lays foundations for progressing towards a learning health and care system.5 As shown in the lowest layer of the architecture in figure 1, this learning system combines classic research knowledge with real-world knowledge from service data and practitioner and patient experience.
The commitment within the decision support programme to continuous evaluation and improvement enables capture of real-world outcomes data generated by decision support tools. This helps us to refine our knowledge base so that we can progress towards the ultimate goal of personalised decision-making centred on individual patient needs.
Footnotes
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Patient consent for publication: Not required.
Provenance and peer review: Commissioned; externally peer reviewed.
References
- 1. Scottish Government Scotland’s Digital Health and Care Strategy; Enabling, Connecting, Empowering. Edinburgh: Scottish Government, 2018. https://www.gov.scot/publications/scotlands-digital-health-care-strategy-enabling-connecting-empowering/ [Google Scholar]
- 2. Scottish Government Personalising Realistic Medicine: Chief Medical Officer for Scotland's Annual Report 2017–2018, 2019. Available: https://www.gov.scot/publications/personalising-realistic-medicine-chief-medical-officer-scotland-annual-report-2017-2018/ [Accessed Nov 2019].
- 3. Cresswell K, Callaghan M, Mozaffar H, et al. NHS Scotland’s decision support platform: a formative qualitative evaluation. BMJ Health Care Inform 2019;26:e100022. 10.1136/bmjhci-2019-100022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Van de Velde S, Heselmans A, Delvaux N, et al. A systematic review of trials evaluating success factors of interventions with computerised clinical decision support. Implement Sci 2018;13:114. 10.1186/s13012-018-0790-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. The Institute of Medicine Digital infrastructure for the learning health system: the foundation for continuous improvement in health and health care. Washington: Institute of Medicine, 2011. https://www.nap.edu/catalog/12912/digital-infrastructure-for-the-learning-health-system-the-foundation-for [Google Scholar]