

Abstract
Background
Worldwide, mother‐to‐child transmission (MTCT) of human immunodeficiency virus type 1 (HIV) represents the most common means by which children acquire HIV infection. Efficacious and effective interventions to prevent in utero and intrapartum transmission of HIV infection have been developed and implemented. However, a large proportion of MTCT of HIV occurs postnatally, through breast milk transmission.
Objectives
The objectives of this systematic review were to collate and assess the evidence regarding interventions to decrease late postnatal MTCT of HIV, and to determine the efficacy of such interventions in decreasing late postnatal MTCT of HIV, increasing overall survival, and increasing HIV‐free survival.
Search methods
Electronic searches were undertaken using PubMed, EMBASE and other databases for 1980‐2008. Hand searches of reference lists of pertinent reviews and studies, as well as abstracts from relevant conferences, were also conducted. Experts in the field were contacted to locate any other studies. The search strategy was iterative.
Selection criteria
Randomized clinical trials assessing the efficacy of interventions to prevent MTCT of HIV through breast milk were included in the analysis. Other trials and intervention cohort studies with relevant data also were included, but only when randomization was not feasible due to the nature of the intervention (i.e., infant feeding modality).
Data collection and analysis
Data regarding HIV infection status and vital status of infants born to HIV‐infected women, according to intervention, were extracted from the reports of the studies.
Main results
Six randomized clinical trials and one intervention cohort study were included in this review. Two trials addressed the issue of shortening the duration of (or eliminating) exposure to breast milk. In a trial of breastfeeding versus formula feeding, formula feeding was efficacious in preventing MTCT of HIV (the cumulative probability of HIV infection at 24 months was 36.7% in the breastfeeding arm and 20.5% in the formula arm [p = 0.001]), but the mortality and malnutrition rates during the first two years of life were similar in the two groups. In a trial of early cessation of breastfeeding, HIV‐free survival was similar between those children who ceased breastfeeding abruptly around four months of age and those who continued breastfeeding. Another trial addressing vitamin supplementation found more cases of HIV infection among children of mothers in the vitamin A arm. Efficacy for other vitamin supplements was not shown. An intervention cohort study evaluated the risk of MTCT by six months of age according to infant feeding modality, and found increased risks of MTCT among breastfed children who also received solids any time after birth (hazard ratio = 10.87, 1.51‐78.00, p = 0.018). Cumulative 3‐month mortality among formula fed infants was higher than among exclusively breastfed infants (hazard ratio = 2.06, 1.00‐4.27, p = 0.051). Three trials evaluated antiretroviral prophylaxis to breastfeeding infants. In one trial conducted in Botswana, mothers received zidovudine prophylaxis beginning at 34 weeks gestation and during labor, and mother and infants were randomized to receive a two‐dose nevirapine regimen or placebo. Infants were randomized to six months of breastfeeding with zidovudine prophylaxis (breastfeeding+zidovudine) or formula feeding with one month of infant zidovudine (formula+zidovudine). Mothers were instructed to initiate and complete weaning between five and six months of age. Breastfeeding+zidovudine (transmission rate = 9.0%) was not as effective as formula+zidovudine (transmission rate 5.6%) in preventing late postnatal HIV transmission (p = 0.04). Breastfeeding+zidovudine and formula+zidovudine had comparable HIV‐free survival rates at 18 months (p = 0.60). Two trials of extended infant nevirapine prophylaxis demonstrated efficacy. In the first (data combined from trials conducted in three different countries), a six‐week course of nevirapine resulted in a lower risk of HIV transmission by six weeks of age (p=0.009), but not at six months of age (p = 0.016). In the second, mothers were counseled to breastfeed exclusively for six months and to consider weaning thereafter. Nevirapine administration until 14 weeks of age (5.2%) or nevirapine with zidovudine until 14 weeks of age (6.4%) resulted in significantly lower risks of MTCT of HIV by 9 months of age than a control regimen of two‐dose nevirapine prophylaxis (10.6%) (p < 0.001). HIV‐free survival was significantly better through the age of 9 months in both extended prophylaxis groups, and through the age of 15 months in the extended nevirapine group.
Authors' conclusions
Complete avoidance of breastfeeding is efficacious in preventing MTCT of HIV, but this intervention has significant associated morbidity (e.g., diarrheal morbidity if formula is prepared without clean water). If breastfeeding is initiated, two interventions 1). exclusive breastfeeding during the first few months of life; and 2) extended antiretroviral prophylaxis to the infant (nevirapine alone, or nevirapine with zidovudine) are efficacious in preventing transmission.
Plain language summary
Transmission of HIV from mother to child through breast milk
Mother‐to‐child transmission (MTCT) of HIV is the primary way that children become infected with HIV. Such transmission can take place when the child is still in the mother’s womb, around the time of birth, or through breastfeeding after birth. Hundreds of thousands of children are infected this way every year, with most of them in developing countries. Major progress has been made in preventing MTCT when the baby is still in the mother’s womb, or around the time the baby is born. In many resource‐rich settings, mothers with HIV infection are counseled not to breastfeed their children, and there are feasible and affordable alternatives to breastfeeding. However, in parts of the world where the vast majority of mothers with HIV infection live, complete avoidance of breastfeeding is often not feasible (for example, because of the lack of availability of clean water and of affordable replacement feeding). Therefore, interventions to prevent transmission of HIV infection through breast milk are urgently needed. The authors found that, in addition to complete avoidance of breastfeeding if safe and affordable, exclusive breastfeeding (where the baby receives only breast milk) for the first few months of life helps prevent transmission (as compared to breastfeeding supplemented by feeding the baby other liquids or solids). Another intervention, giving the baby an anti‐HIV medicine (antiretroviral) while breastfeeding, decreases the risk of transmission of HIV from mother to child. Implementation of such interventions, as well as developing more and better interventions, is essential.
Background
By the end of 2007, approximately 33 million people worldwide, including 2.1 million children under the age of 15 years, were living with human immunodeficiency virus type 1 (HIV) infection or acquired immunodeficiency syndrome (AIDS) (UNAIDS 2008). An estimated 1200 children under the age of 15 years acquire HIV infection each day (420,000 new infections/year) (UNAIDS 2008). The vast majority of HIV‐infected children acquire the infection through mother‐to‐child transmission (MTCT) in utero, around the time of labor and delivery, or postnatally through breastfeeding (Read 2005a).
Evidence of increased mortality among children of HIV‐infected mothers
Children born to HIV‐infected mothers have high rates of mortality, regardless of their own infection status (Newell 2004). In a pooled analysis of randomized trials from sub‐Saharan Africa, children born to mothers in the advanced stages of HIV infection were at considerably higher risk of death when compared to those of mothers who were at a less advanced stage of the disease (irrespective of the child's HIV infection status), and this association was even stronger for uninfected children (Newell 2004). Also, the timing of acquisition of HIV infection was associated with mortality, as children who were infected before four weeks of age were at higher risk of death during the first 12‐24 months after infection than those who acquired infection after four weeks of age (through breastfeeding).
Mother‐to‐child transmission of HIV
An 'umbrella review' of five Cochrane reviews recently examined the evidence for interventions for the prevention of in utero and intrapartum MTCT (Bond 2007). Two interventions have been shown to be efficacious in the prevention of MTCT of HIV during these periods:
Antiretroviral (ARV) prophylaxis: ARVs given to HIV‐infected pregnant women and/or to their infants can prevent MTCT of HIV (Volmink 2007).
Caesarean delivery before labor and before ruptured membranes ('elective' Caesarean section, or ECS): Performing a caesarean section before labor and before ruptured membranes can prevent MTCT of HIV (Read 2005b).
This systematic review will analyze the evidence of interventions for the prevention of late postnatal (breastfeeding) MTCT of HIV.
Late postnatal MTCT of HIV (through breastfeeding)
In 2006, the World Health Organization reaffirmed previous recommendations for all HIV‐infected mothers to receive counseling, including provision of general information about risks and benefits of various infant feeding options, and specific guidance in selecting the feeding option most likely to be suitable for their individual situation. It also called for mothers to be supported in their choices regarding infant feeding (WHO 2006).
The benefits of breastfeeding are well recognized and include significantly decreased infant morbidity and mortality rates by providing optimal nutrition, protecting against common childhood infections (such as gastrointestinal and respiratory tract infections), and promoting child spacing (Pebley 1986; Thapa 1988; Yoon 1996; Cesar 1999; WHO Team 2000; Kramer 2001). Breastfeeding is particularly important in resource‐poor regions of the world, where limited access to clean water increases the risk of diarrhea if replacement feeding is used, and many mothers do not have the means to afford the costs of formula and other breast milk substitutes. However, HIV is transmitted through human milk, leading to the dilemma that the use of replacement feeding in resource‐poor settings, while protecting an infant against HIV infection, also could place the same infant at risk of morbidity and mortality from other infections.
Moreover, mothers opting to feed their children through replacement feeding are stigmatized in many cultures, which greatly complicates adherence to a replacement‐feeding regimen (Rankin 2005). They are often assumed to be infected with HIV, leading to HIV‐associated stigma, where women may be ostracized and expelled from their families in the case of suspected HIV infection. Even in situations where an HIV‐associated stigma does not exist and women have the choice to breastfeed or use replacement feeding, the supplies needed to continually conduct replacement feeding can be sporadic, compromising infant nutrition or resulting in mixed feeding. However, exclusive breastfeeding in itself can be difficult for mothers, especially for those who have responsibilities that take them away from their children during the day. In these instances, a child may receive mixed feedings, i.e., breast milk when with their mothers, and alternative feeding options when being cared for by others.
Shortly after the first report of transmission of HIV through breastfeeding (Ziegler 1985), the U.S. Centers for Disease Control and Prevention (CDC) recommended that HIV‐infected women in the United States of America avoid breastfeeding (MMWR 1985), because replacement feeding in the U.S. is safe, affordable, and culturally acceptable. The CDC and the American Academy of Pediatrics (AAP 1995) have continued to recommend counseling HIV‐infected women in the U.S. not to breastfeed or provide their milk for the nutrition of their own or other infants. Avoidance of breastfeeding remains an important component of efforts to prevent MTCT of HIV in the U.S. (Read 1999) and in other countries. MTCT of HIV has been substantially decreased in the U.S. (Lindegren 1999), in Europe, and elsewhere.
However, in many areas of the world, especially those areas where breastfeeding is the norm and safe replacement feeding generally is not possible, the enormous and unremitting epidemic of MTCT of HIV continues (UNAIDS 2008). Recommendations of the World Health Organization (WHO) are similar to those of the CDC, in that when replacement feeding is acceptable, feasible, sustainable, and safe, HIV‐infected mothers should avoid breastfeeding altogether (WHO 2006). Research efforts focused on the continuing problem of breastfeeding transmission in much of the world have yielded additional information regarding mechanisms of HIV transmission through breastfeeding, as well as the timing of and risk factors for such transmission.
Breastfeeding transmission of HIV
Over more than two decades, the understanding of MTCT of HIV through breastfeeding has increased tremendously. Beginning with the earliest clinical evidence (case reports) of breastfeeding transmission of HIV (Ziegler 1985), additional information regarding breastfeeding transmission has come from numerous descriptive, analytic epidemiologic, and laboratory studies (Read 2003). Risk factors for transmission of HIV through breastfeeding have been identified, including the duration of breastfeeding as well as characteristics of the mother, the infant, the breast milk, and the type of breastfeeding.
Duration of breastfeeding
The contribution of breastfeeding transmission to the overall risk of MTCT of HIV, and the timing of and risk factors for breastfeeding transmission, were analyzed in an individual patient data meta‐analysis of nine clinical trials of HIV‐infected women and their infants, conducted in sub‐Saharan Africa (BHITS 2004). Breastfeeding contributes substantially to overall MTCT of HIV; of children with known timing of infection, as much as 42% of transmission was attributable to breastfeeding. The cumulative probability of transmission increased as the duration of breastfeeding increased (from 1.6% at three months of age to 9.3% at 18 months of age).
Characteristics of the mother and infant
A number of maternal and infant characteristics have been associated with increased risk of breastfeeding transmission of HIV. Maternal factors associated with breastfeeding transmission of HIV include younger maternal age and higher parity (Miotti 1999), recent HIV infection (with concomitantly high viral load) or advanced maternal HIV disease stage, and breast abnormalities. More advanced maternal disease stage, as manifested by low CD4+ cell counts, is a risk factor for late postnatal transmission of HIV (Semba 1999a; Embree 2000; Pillay 2000; BHITS 2004) along with higher maternal peripheral blood or human milk viral load (Semba 1999b; Pillay 2000; Richardson 2003). An early case report of the temporal association of HIV acquisition by the child of an HIV‐infected woman with a breast abscess suggested that the ingestion of inflammatory cells related to the bacterial infection of the breast contributes to breastfeeding transmission of HIV (Van de Perre 1992). Later studies confirmed the association of transmission of HIV through breastfeeding with maternal breast abnormalities such as breast abscesses, mastitis, and nipple lesions. In Kenya, mastitis and breast abscesses were associated with late postnatal transmission of HIV (John 2001). In Malawi, women with increased human milk sodium concentrations consistent with sub‐clinical mastitis had higher human milk viral loads than did women without increased human milk sodium concentrations (Semba 1999a). In another study in Kenya, maternal nipple lesions and mastitis were each associated with an increased risk of late postnatal transmission (Embree 2000). Oral candidiasis before six months of age is associated with late postnatal transmission (Embree 2000), and results of a study in the Ivory Coast suggested maternal breast abscesses and cracked nipples, as well as oral candidiasis in infants, were risk factors for late postnatal transmission of HIV through breastfeeding (Ekpini 1997). Male gender has been associated with breastfeeding transmission of HIV (BHITS 2004).
Characteristics of breast milk
In addition to higher breast milk viral load (both cell‐free and cell‐associated), characteristics of breast milk possibly associated with a higher risk of breastfeeding transmission of HIV include the following: lower concentrations of antiviral substances, such as lactoferrin (Harmsen 1995; Swart 1996), lysozyme, secretory leukocyte protease inhibitor (SLPI) (Hocini 2000), and epidermal growth factor (Donovan 1994), as well as lesser specific, local immune responses to HIV. Interestingly, HIV‐infected women with sub‐clinical mastitis, higher human milk viral loads, and higher rates of MTCT had higher human milk concentrations of lysozyme and SLPI than did HIV‐infected women without sub‐clinical mastitis (Semba 1999b). However, SLPI concentrations in human milk have not been found by other investigators to be associated with HIV transmission through breastfeeding (Becquart 1999). It has been suggested that epidermal growth factor in colostrum helps to make the gastrointestinal tract less permeable to viral infection (Donovan 1994). Higher MTCT of HIV has been associated with lower human milk concentrations of secretory immunoglobulin A and immunoglobulin M during the first several weeks of life in some, (Van de Perre 1993) but not all, studies (Becquart 2000).
Type of infant feeding
The relationship between infant feeding modality, such as exclusive or mixed feeding, and MTCT of HIV also has been evaluated. In South Africa, data from a randomized clinical trial of vitamin A supplementation to prevent MTCT were re‐analyzed to evaluate a possible association between feeding patterns among infants of breastfeeding HIV‐infected mothers and MTCT (Coutsoudis 1999; Coutsoudis 2001). In these analyses, breastfeeding was categorized as exclusive or mixed (i.e., without or with water, other fluids, and food). Women who chose to breastfeed were counseled to consider exclusive breastfeeding. By 15 months of age, children who ever breastfed were more likely to have become HIV‐infected than were children who never breastfed. Of those children who ever breastfed, there was a lower point estimate of transmission for those children who exclusively breastfed until at least three months of age, but no longer than six months of age, as compared to those children with mixed feeding. It has been proposed that feeding of foods other than breast milk in early infancy damages the gastrointestinal tract, with a concomitant increase in the permeability of the gastrointestinal tract to HIV in breast milk (Catassi 1995; Goto 1999). Iliff and colleagues described similar findings from their study in Zimbabwe (Iliff 2005).
Description of the intervention, and how the intervention might work
Because breastfeeding transmission of HIV does occur, and because complete avoidance of breastfeeding is impossible in many settings, identification of risk factors for MTCT of HIV through breastfeeding has been important in order to design interventions to prevent such transmission. There are several potential interventions to prevent breastfeeding transmission of HIV. These include decreasing the duration of exposure to breast milk (e.g., complete avoidance of breastfeeding, early cessation of breastfeeding), decreasing maternal infectivity (e.g., lowering viral load in breast milk through chemical or heat treatment of breast milk, or through ARV prophylaxis to the mother while breastfeeding), addressing factors affecting the transfer of virus from mother‐to‐child (e.g., mixed feeding, infant thrush, maternal nipple bleeding), and improving infant's defenses against HIV (e.g., through passive or active immunization).
Decreasing the duration of exposure to breast milk
Complete avoidance of breastfeeding
Complete avoidance of breastfeeding would be an obvious intervention to prevent HIV transmission through breast milk. However, many issues, including feasibility (clean water), affordability of formula and formula‐feeding supplies, cultural acceptability, and the overall nutritional and immunologic status of the child must be considered.
Early cessation of breastfeeding
In those circumstances where complete avoidance of breastfeeding is not possible, early cessation from breastfeeding would decrease a child's exposure to breast milk and HIV infection. Again, the issues of feasibility, affordability, cultural acceptability, and nutritional status must be considered. Since the risk of morbidity and mortality associated with replacement feeding was believed to decline after a child's first six months of life, it was considered possible to wean a child off of breast milk and supplement his/her diet with other forms of nutrition after this time (VanDerslice 1994). However, several studies in sub‐Saharan Africa have now demonstrated significant morbidity associated with early cessation (Kafulafula 2007, Kourtis 2007, Onyango 2007, Thomas 2008), thus calling for more caution in recommending early cessation of breastfeeding for HIV‐infected women in resource‐poor settings. Thus, the most recent WHO recommendation states: “At six months, if replacement feeding is still not acceptable, feasible, affordable, sustainable and safe, continuation of breastfeeding with additional complementary foods is recommended, while the mother and baby continue to be regularly assessed. All breastfeeding should stop once a nutritionally adequate and safe diet without breast milk can be provided.” (WHO 2006).
Decreasing maternal infectivity (lowering viral load in breast milk)
Studies investigating ways to decrease the viral load in breast milk, either through antiretrovirals for HIV‐infected mothers while breastfeeding, or through the treatment of breast milk with chemical agents or heat, are also underway. Preliminary data from observational or non‐randomized studies suggest maternal antiretroviral prophylaxis while breastfeeding is associated with a decreased risk of MTCT of HIV (Arendt 2007, Giuliano 2007, Kilewo 2008). Ongoing randomized clinical trials are exploring the efficacy of different antiretroviral drugs, administered over varying lengths of time to mothers of breastfeeding infants (Van der Horst 2003; de Vincenzi 2008). Other studies are looking at the treatment of human milk, either through chemical agents (Urdaneta 20055) or heat (Israel‐Ballard 2005) to inactivate HIV. Limited data suggest heat treatment of breast milk does not have major detrimental effects (Israel‐Ballard 2008) but does lower the viral load in the milk (Israel‐Ballard 2005; Israel‐Ballard 2007).
Addressing factors affecting the transfer of virus from mother‐to‐child
The education and counseling of mothers are also important factors in preventing late postnatal MTCT of HIV. Having an understanding of proper breastfeeding techniques can help mothers mitigate or quickly treat breast abnormalities associated with HIV transmission. The same holds true for infant candidiasis. Educating mothers regarding the importance of exclusive breastfeeding in situations where complete avoidance of breastfeeding is not an option appears to be beneficial in terms of initiation and duration of exclusive breastfeeding (Bland 2008; Desmond 2008).
Improving infants' defenses against HIV infection
Improving infants' defenses is yet another potential way to prevent MTCT. It has been hypothesized that passive immunization with HIV immune globulin may decrease MTCT, and a randomized clinical trial is underway in Uganda (Safrit 2004). Other studies are evaluating the safety and immunogenicity of active HIV vaccines in infants (Safrit 2004).
Why it is important to do this review
Major advances have been made in the prevention of MTCT of HIV during the antepartum and intrapartum periods. However, while MTCT of HIV has become rare in the parts of the world where complete avoidance of breastfeeding is feasible, the epidemic of MTCT of HIV, especially transmission through breastfeeding, continues. There is an urgent need to develop and implement effective interventions to prevent such transmission. Therefore, this systematic review was undertaken to assess the available evidence regarding interventions to prevent postnatal MTCT of HIV.
Note (November 2009): Since this review was published in early 2009, several new studies have been published relevant to antiretroviral prophylaxis to prevent HIV transmission during breastfeeding. In light of this new body of evidence, the authors believe that a separate Cochrane review of these interventions is warranted. We anticipate that the new review, titled "Antiretroviral prophylaxis to prevent breast milk transmission of HIV," will be published in Cochrane Library 2010:2. Future updates of the present review will be limited to studies concerned with non‐antiretroviral interventions to prevent breast milk transmission of HIV. The authors plan to prepare a substantive update of the present review sometime in 2010.
Objectives
The objectives of this systematic review are to collate and assess the evidence of interventions to decrease late postnatal MTCT of HIV, and to determine the efficacy of such interventions in decreasing late postnatal MTCT of HIV, increasing overall survival, and increasing HIV‐free survival.
Methods
Criteria for considering studies for this review
Types of studies
Randomized clinical trials of HIV‐infected women and their infants assessing the efficacy of interventions to prevent MTCT of HIV through breast milk were included in the analysis. Other trials and intervention cohort studies with relevant data also were included, but only in those cases where randomization was not feasible due to the nature of the intervention (i.e., infant feeding modality). Studies performed in general or specific populations and in hospitals or clinics were included. Studies performed in any country and published in any language were included. Studies with historical controls and ecological studies were excluded.
Types of participants
HIV‐infected women, pregnant or postpartum, and their children
Types of interventions
Interventions to prevent breast milk transmission of HIV, through decreasing the duration of exposure to breast milk, decreasing maternal infectivity, addressing factors affecting the transfer of virus from mother to child, and improving infants’ defenses against HIV infection
Types of outcome measures
The outcome measures were the following (among children born to HIV‐infected women):
1) HIV infection;
2) overall survival; and
3) HIV‐free survival.
Search methods for identification of studies
See Cochrane HIV/AIDS Group search strategy.
See Table 1 for our strategies in searching Cochrane CENTRAL, EMBASE and PubMed.
1. Examples of search strategies.
| PubMED: Date range: 1 January 1980 ‐ 15 July 2008 | |
| #11 | Search #3 AND #4 AND #9 |
| #10 | Search #3 AND #4 AND #9 |
| #9 | Search #7 OR #8 |
| #8 | Search (infant feeding) OR (infant nutrition) OR (infant feeding options) OR (exclusive breastfeeding) OR (exclusive breast‐feeding) OR (exclusive breast feeding) OR (formula feeding) OR (early weaning) OR (abrupt weaning) OR (wet nursing) OR (milk bank) OR (milk banks) OR (expressed breast milk) OR (expressed human milk) OR (replacement feeding) |
| #7 | Search #5 AND #6 |
| #6 | Search pasteurization OR pasteurization OR (heat treatment) OR sterilisation OR sterilization OR decontamination |
| #5 | Search (breast milk) OR (breast milks) OR (human milk) |
| #4 | Search (mother‐to‐child transmission) OR (mother to child transmission) OR (adult‐to‐child transmission) OR (adult to child transmission) OR (maternal‐to‐child transmission) OR (maternal to child transmission) OR (breast milk transmission) OR (breast‐milk transmission) OR (vertical transmission) OR (disease transmission, vertical) |
| #3 | Search #1 AND #2 |
| #2 | Search randomized controlled trial [pt] OR controlled clinical trial [pt] OR randomized controlled trials [mh] OR random allocation [mh] OR double‐blind method [mh] OR single‐blind method [mh] OR clinical trial [pt] OR clinical trials [mh] OR ("clinical trial" [tw]) OR ((singl* [tw] OR doubl* [tw] OR trebl* [tw] OR tripl* [tw]) AND (mask* [tw] OR blind* [tw])) OR ( placebos [mh] OR placebo* [tw] OR random* [tw] OR research design [mh:noexp] OR comparative study [mh] OR evaluation studies [mh] OR follow‐up studies [mh] OR prospective studies [mh] OR control* [tw] OR prospectiv* [tw] OR volunteer* [tw]) NOT (animals [mh] NOT human [mh]) |
| #1 | Search HIV Infections[MeSH] OR HIV[MeSH] OR hiv[tw] OR hiv‐1*[tw] OR hiv‐2*[tw] OR hiv1[tw] OR hiv2[tw] OR hiv infect*[tw] OR human immunodeficiency virus[tw] OR human immunedeficiency virus[tw] OR human immuno‐deficiency virus[tw] OR human immune‐deficiency virus[tw] OR ((human immun*) AND (deficiency virus[tw])) OR acquired immunodeficiency syndrome[tw] OR acquired immunedeficiency syndrome[tw] OR acquired immuno‐deficiency syndrome[tw] OR acquired immune‐deficiency syndrome[tw] OR ((acquired immun*) AND (deficiency syndrome[tw])) OR "sexually transmitted diseases, viral"[MESH:NoExp] |
| EMBASE: Date range: 1 January 1980 ‐ 15 July 2008 | |
| #1 | (((('human immunodeficiency virus infection'/exp OR 'human immunodeficiency virus infection') OR ('human immunodeficiency virus infection'/exp OR 'human immunodeficiency virus infection')) OR (('human immunodeficiency virus infection'/exp OR 'human immunodeficiency virus infection') OR ('human immunodeficiency virus infection'/exp OR 'human immunodeficiency virus infection'))) OR ((('human immunodeficiency virus infection'/exp OR 'human immunodeficiency virus infection') OR ('human immunodeficiency virus infection'/exp OR 'human immunodeficiency virus infection')) OR (('human immunodeficiency virus infection'/exp OR 'human immunodeficiency virus infection') OR ('human immunodeficiency virus infection'/exp OR 'human immunodeficiency virus infection')))) OR ((((('human immunodeficiency virus'/exp OR 'human immunodeficiency virus') OR ('human immunodeficiency virus'/exp OR 'human immunodeficiency virus')) OR (('human immunodeficiency virus'/exp OR 'human immunodeficiency virus') OR ('human immunodeficiency virus'/exp OR 'human immunodeficiency virus'))) OR ((('human immunodeficiency virus'/exp OR 'human immunodeficiency virus') OR ('human immunodeficiency virus'/exp OR 'human immunodeficiency virus')) OR (('human immunodeficiency virus'/exp OR 'human immunodeficiency virus') OR ('human immunodeficiency virus'/exp OR 'human immunodeficiency virus'))))) OR (hiv:ti OR hiv:ab) OR ('hiv‐1':ti OR 'hiv‐1':ab) OR ('hiv‐2':ti OR 'hiv‐2':ab) OR ('human immunodeficiency virus':ti OR 'human immunodeficiency virus':ab) OR ('human immuno‐deficiency virus':ti OR 'human immuno‐deficiency virus':ab) OR ('human immunedeficiency virus':ti OR 'human immunedeficiency virus':ab) OR ('human immune‐deficiency virus':ti OR 'human immune‐deficiency virus':ab) OR ('acquired immune‐deficiency syndrome':ti OR 'acquired immune‐deficiency syndrome':ab) OR ('acquired immunedeficiency syndrome':ti OR 'acquired immunedeficiency syndrome':ab) OR ('acquired immunodeficiency syndrome':ti OR 'acquired immunodeficiency syndrome':ab) OR ('acquired immuno‐deficiency syndrome':ti OR 'acquired immuno‐deficiency syndrome':ab) |
| #2 | (random*:ti OR random*:ab) OR (factorial*:ti OR factorial*:ab) OR (cross?over*:ti OR cross?over:ab OR crossover*:ti OR crossover*:ab) OR (placebo*:ti OR placebo*:ab) OR (((doubl*:ti AND blind*:ti) OR (doubl*:ab AND blind*:ab))) OR (((singl*:ti AND blind*:ti) OR (singl*:ab AND blind*:ab))) OR (assign*:ti OR assign*:ab) OR (volunteer*:ti OR volunteer*:ab) OR ((((('crossover procedure'/exp OR 'crossover procedure') OR ('crossover procedure'/exp OR 'crossover procedure')) OR (('crossover procedure'/exp OR 'crossover procedure') OR ('crossover procedure'/exp OR 'crossover procedure'))) OR ((('crossover procedure'/exp OR 'crossover procedure') OR ('crossover procedure'/exp OR 'crossover procedure')) OR (('crossover procedure'/exp OR 'crossover procedure') OR ('crossover procedure'/exp OR 'crossover procedure'))))) OR ((((('double‐blind procedure'/exp OR 'double‐blind procedure') OR ('double‐blind procedure'/exp OR 'double‐blind procedure')) OR (('double‐blind procedure'/exp OR 'double‐blind procedure') OR ('double‐blind procedure'/exp OR 'double‐blind procedure'))) OR ((('double‐blind procedure'/exp OR 'double‐blind procedure') OR ('double‐blind procedure'/exp OR 'double‐blind procedure')) OR (('double‐blind procedure'/exp OR 'double‐blind procedure') OR ('double‐blind procedure'/exp OR 'double‐blind procedure'))))) OR ((((('single‐blind procedure'/exp OR 'single‐blind procedure') OR ('single‐blind procedure'/exp OR 'single‐blind procedure')) OR (('single‐blind procedure'/exp OR 'single‐blind procedure') OR ('single‐blind procedure'/exp OR 'single‐blind procedure'))) OR ((('single‐blind procedure'/exp OR 'single‐blind procedure') OR ('single‐blind procedure'/exp OR 'single‐blind procedure')) OR (('single‐blind procedure'/exp OR 'single‐blind procedure') OR ('single‐blind procedure'/exp OR 'single‐blind procedure'))))) OR ((((('randomized controlled trial'/exp OR 'randomized controlled trial') OR ('randomized controlled trial'/exp OR 'randomized controlled trial')) OR (('randomized controlled trial'/exp OR 'randomized controlled trial') OR ('randomized controlled trial'/exp OR 'randomized controlled trial'))) OR ((('randomized controlled trial'/exp OR 'randomized controlled trial') OR ('randomized controlled trial'/exp OR 'randomized controlled trial')) OR (('randomized controlled trial'/exp OR 'randomized controlled trial') OR ('randomized controlled trial'/exp OR 'randomized controlled trial'))))) OR (allocat*:ti OR allocat*:ab) |
| #3 | #1 AND #2 |
| #4 | 'mother‐to‐child transmission' OR 'mother to child transmission' OR 'adult‐to‐child transmission' OR 'adult to child transmission' OR 'maternal‐to‐child transmission' OR 'maternal to child transmission' OR 'breast milk transmission' OR 'breast‐milk transmission' OR ('vertical transmission'/exp OR 'vertical transmission') OR 'vertical disease transmission' |
| #5 | ('breast milk'/exp OR 'breast milk') OR 'breast milks' OR ('human milk'/exp OR 'human milk') |
| #6 | pasteurisation OR ('pasteurization'/exp OR 'pasteurization') OR ('heat treatment'/exp OR 'heat treatment') OR ('sterilisation'/exp OR 'sterilisation') OR ('sterilization'/exp OR 'sterilization') OR ('decontamination'/exp OR 'decontamination') |
| #7 | #5 AND #6 |
| #8 | ('infant feeding'/exp OR 'infant feeding') OR ('infant nutrition'/exp OR 'infant nutrition') OR 'infant feeding options' OR 'exclusive breastfeeding' OR 'exclusive breast‐feeding' OR 'exclusive breast feeding' OR ('formula feeding'/exp OR 'formula feeding') OR 'early weaning' OR 'abrupt weaning' OR 'wet nursing' OR ('milk bank'/exp OR 'milk bank') OR ('milk banks'/exp OR 'milk banks') OR 'expressed breast milk' OR 'expressed human milk' OR 'replacement feeding' |
| #9 | #7 OR #8 |
| #10 | #3 AND #4 AND #9 |
| Cochrane CENTRAL Controlled Trials Register: Date range: 1 January 1980 ‐ 15 July 2008 | |
| #1 | (HIV INFECTIONS) OR HIV OR HIV OR HIV‐1* OR HIV‐2* OR HIV1 OR HIV2 OR (HIV INFECT*) OR (HUMAN IMMUNODEFICIENCY VIRUS) OR (HUMAN IMMUNEDEFICIENCY VIRUS) OR (HUMAN IMMUNO‐DEFICIENCY VIRUS) OR (HUMAN IMMUNE‐DEFICIENCY VIRUS) OR ((HUMAN IMMUN*) AND (DEFICIENCY VIRUS)) OR (ACQUIRED IMMUNODEFICIENCY SYNDROME) OR (ACQUIRED IMMUNEDEFICIENCY SYNDROME) OR (ACQUIRED IMMUNO‐DEFICIENCY SYNDROME) OR (ACQUIRED IMMUNE‐DEFICIENCY SYNDROME) OR ((ACQUIRED IMMUN*) AND (DEFICIENCY SYNDROME)) OR (VIRAL SEXUALLY TRANSMITTED DISEASES) |
| #2 | (MOTHER‐TO‐CHILD TRANSMISSION) OR (MOTHER TO CHILD TRANSMISSION) OR (ADULT‐TO‐CHILD TRANSMISSION) OR (ADULT TO CHILD TRANSMISSION) OR (MATERNAL‐TO‐CHILD TRANSMISSION) OR (MATERNAL TO CHILD TRANSMISSION) OR (BREAST MILK TRANSMISSION) OR (BREAST‐MILK TRANSMISSION) OR (VERTICAL TRANSMISSION) OR (VERTICAL DISEASE TRANSMISSION) |
| #3 | (BREAST MILK) OR (BREAST MILKS) OR (HUMAN MILK) |
| #4 | PASTEURIZATION OR PASTEURIZATION OR (HEAT TREATMENT) OR STERILISATION OR STERILIZATION OR DECONTAMINATION |
| #5 | (#3 AND #4) |
| #6 | (INFANT FEEDING) OR (INFANT NUTRITION) OR (INFANT FEEDING OPTIONS) OR (EXCLUSIVE BREASTFEEDING) OR (EXCLUSIVE BREAST‐FEEDING) OR (EXCLUSIVE BREAST FEEDING) OR (FORMULA FEEDING) OR (EARLY WEANING) OR (ABRUPT WEANING) OR (WET NURSING) OR (MILK BANK) OR (MILK BANKS) OR (EXPRESSED BREAST MILK) OR (EXPRESSED HUMAN MILK) OR (REPLACEMENT FEEDING) |
| #7 | (#5 OR #6) |
| #8 | (#1 AND #2 AND #7) |
Electronic searches were undertaken using the following databases: CENTRAL, PubMed, EMBASE, and Gateway and AIDSearch. Hand searches of the reference lists of all pertinent reviews and studies found also were undertaken, as well as abstracts from relevant conferences, including the International AIDS Conferences and the annual Conference on Retroviruses and Opportunistic Infections. Experts in the field of HIV prevention were contacted to locate any further studies or relevant conference proceedings not included in the databases to ensure that unpublished studies were included. The search strategy was iterative. There were no restrictions on language.
With regard to the electronic literature search, the optimal sensitive search strategy developed by The Cochrane Collaboration and detailed in the Cochrane Reviewers’ Handbook (Handbook 2008) was used, in conjunction with search terms identified in Table 1, to identify relevant studies from 1 January 1980 to 15 July 2008.
Data collection and analysis
The search for studies was performed with the assistance of the Cochrane HIV/AIDS Group. The authors performed the selection of potentially relevant studies. The titles, abstracts and descriptor terms of all downloaded material from the electronic searches were read and irrelevant reports discarded to create a pool of potentially eligible studies. All citations identified then were inspected independently by JSR, TH, and IMI to establish relevance of the article and whether or not the full article should be acquired. If there was uncertainty, the full article was obtained.
Selection of studies
JSR, TH, and IMI independently applied the inclusion criteria. Studies were reviewed for relevance based on study design, types of participants, exposures and outcome measures. Finally, where resolution was not possible because further information was necessary, attempts were made to contact authors to provide further clarification of data. The method of conflict resolution was by consensus.
Data extraction and management
Using a standardized data extraction form, JSR, TH, and IMI independently extracted data. The following characteristics were extracted from each included study:
Type of intervention
Eligibility criteria for enrollment into the study
Assessment of risk of bias: study design, sequence generation, allocation concealment, blinding, loss to follow‐up, incomplete outcome data, other potential bias
Details regarding the study participants: sample size, population characteristics, country where study performed, HIV diagnostic testing utilized and ages when testing performed
Intervention(s) studied: non‐drug intervention(s), drug intervention(s), comparison groups
Outcome measures: HIV infection status of the child, overall survival, HIV‐free survival
Results
Description of studies
After screening 1349 citations, we identified 17 potentially relevant studies. After reviewing the 17 complete articles for the studies we determined that seven (six randomized clinical trials and one intervention cohort study) met our inclusion criteria (Figure 1). Only the abstract was available for one additional study (SIMBA 2003), as this study has never been published. Authors of the study were contacted, but no further information was obtained. Therefore, we were not able to fully consider this study.
1.
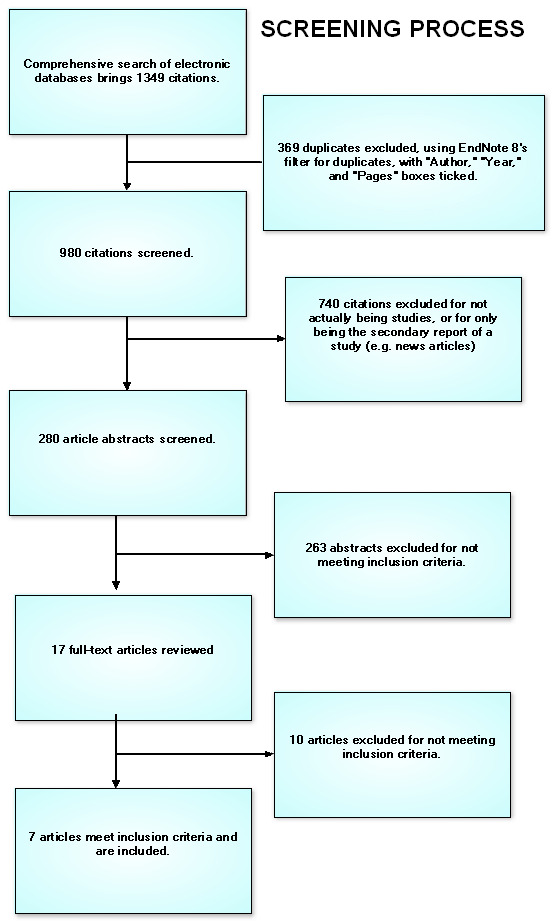
Flowchart of screening process
Studies included in this review: Nduati 2000; Fawzi 2002; Thior 2006; Coovadia 2007Kuhn 2008; Kumwenda 2008; and SWEN 2008. Details of each study are given in the table “Characteristics of included studies” and are noted below:
Randomized clinical trials
The trial conducted in Kenya by Nduati and colleagues (Nduati 2000), prior to the local availability of interventions to prevent MTCT of HIV, was a randomized clinical trial of breastfeeding versus formula feeding for prevention of MTCT. The primary objective of the trial was to determine the efficacy of complete avoidance of breastfeeding (i.e., formula feeding) in prevention of MTCT of HIV, and to compare overall survival and HIV‐free survival in breastfed and formula‐fed infants. HIV‐infected women were eligible for inclusion in the trial if they resided in Nairobi and had access to municipal‐treated water. Women were randomized to breastfeed or formula feed at approximately 32 weeks of gestation. Of 425 women randomized, 401 were followed to delivery and had live born infants. Of 401 infants included in the analysis, 94% were followed to HIV infection or mortality endpoints.
Fawzi and colleagues (Fawzi 2002) conducted a randomized trial of vitamin supplements. Pregnant women presenting to public antenatal clinics in Dar es Salaam between 12 and 27 weeks of gestation, who resided in and intended to stay in the city until at least one year after delivery, were enrolled. Participants were randomly assigned in a two‐by‐two factorial design to receive a daily oral dose of one of four regimens beginning at enrollment and continuing throughout pregnancy and during breastfeeding: 1) vitamin A alone (30 mg beta‐carotene plus 5000 IU preformed vitamin A); 2) multivitamins excluding vitamin A (20 mg B1, 20 mg B2, 25 mg B6, 100 mg niacin, 50 micrograms B12, 500 mg vitamin C, 30 mg vitamin E, 0.8 mg folic acid); 3) multivitamins including vitamin A in the same doses as above; and placebo. At delivery, women in groups 1 and 3 received an additional oral dose of vitamin A (200,000 IU), and women in groups 2 and 4 received placebo.
As part of a clinical trial in Botswana, 1200 HIV‐infected women were randomized to breastfeeding with infant zidovudine prophylaxis for six months versus formula feeding plus infant zidovudine for one month to reduce mother‐to‐child HIV transmission (Thior 2006). Zidovudine 4 mg/kg every 12 hours from birth until one month of age was given to all infants, and discontinued at one month of age in the formula‐fed group. For the breastfed plus zidovudine group, infant zidovudine prophylaxis continued from 1‐2 months of age at 4 mg/kg every 8 hours, and from 2‐6 months of age (while still breastfeeding) at 6 mg/kg every 8 hours. All mothers received zidovudine 300 mg orally twice daily from 34 weeks gestation and during labor). Mothers and infants were randomized to receive single‐dose nevirapine or placebo. Eligibility criteria for the mothers included being between 33‐35 weeks gestation, having a positive HIV ELISA on 2 separate samples, being aged 18 years or older, having levels of hemoglobin at 80 g/L or above, absolute neutrophil counts of 1000 or more cells/mm, alanine aminotransferase and aspartate aminotrasferase at 10 or less times the upper limit of normal, and creatinine 1.5 mg/dL (132.6 micromol/L) or less, and not having known intolerance to zidovudine or nevirapine. The primary efficacy (HIV infection by age 7 months and HIV‐free survival by age 18 months) and safety (occurrence of infant adverse events by 7 months of age) end points were evaluated in 1179 infants.
Kuhn et al (Kuhn 2008) evaluated the effects of early, abrupt cessation of breastfeeding on HIV‐free survival of children in Zambia. HIV‐infected women were recruited from antenatal clinics in Lusaka, Zambia that offered HIV counseling and testing, and the two‐dose nevirapine regimen for prevention of MTCT of HIV. Women (at less than 38 weeks of gestation) could volunteer if they intended to breastfeed for any length of time, accepted nevirapine prophylaxis, and agreed to be randomized. Exclusion criteria were severe pregnancy complications, previous cesarean delivery, and HIV‐related conditions requiring hospitalization. Participants were randomly assigned to one of two groups. Women assigned to the intervention group were encouraged to breastfeed exclusively to four months, and then to stop breastfeeding abruptly, or as rapidly as possible. Women assigned in the control group were encouraged to breastfeed exclusively for six months, and then to gradually introduce complementary foods and to continue to breastfeed for as long as they chose.
A trial of extended infant prophylaxis with nevirapine was conducted in Malawi (Kumwenda 2008). All infants received a single oral dose of nevirapine (2 mg/kg) plus oral zidovudine (4 mg/kd) twice daily for one week. Drugs for infants in the two extended prophylaxis groups were dispensed beginning at the 1‐week study visit. In Arm 1, the single dose of nevirapine with the one week course of zidovudine was given to the infant (control regimen). In Arm 2, the control regimen PLUS daily nevirapine (2 mg/kg once daily during week 2, then 4 mg/kg once daily during weeks 3‐14) was administered. In Arm 3, the control regimen PLUS daily nevirapine with zidovudine (4 mg/kg twice daily during weeks 2‐5, 4 mg/kg three times daily during weeks 6‐8, and 6 mg/kg three times daily during weeks 9‐14) was given. HIV‐infected pregnant women were eligible for enrollment into the study, except if the HIV infection was not identified until after they delivered (late presenters). Other eligibility criteria for the women were: at least 18 years of age (although women < 18 years of age could be enrolled if they consented and a guardian gave permission), pregnant or had given birth within the previous 24 hours at one of the study clinics, a resident of the study area, willing to return for postnatal follow‐up visits for up to 2 years, and intended to breastfeed. Infants with life‐threatening conditions requiring immediate care were excluded. The women received intrapartum nevirapine prior to the randomization of the infants.
Three separate but coordinated randomized controlled trials were conducted in Ethiopia, India, and Uganda (SWEN 2008). Data from these trials were analyzed together. In Arm 1 (control arm) of the trials, 200 mg nevirapine was provided to women in labor and 2 mg/kg to infants shortly after birth. In Arm 2 of the trials, this two‐dose nevirapine regimen was provided in addition to infant dosing of 5 mg nevirapine each day starting at age 7 days through six weeks of life. The risk of HIV infection and death at 6 weeks and 6 months of age in infants who were HIV‐uninfected at birth was estimated. The analysis included data for 1887 infants.
Intervention cohort study
A study to assess the risk of HIV transmission and survival associated with exclusive breastfeeding and other types of infant feeding was conducted by Coovadia and colleagues (Coovadia 2007) in South Africa. Women were enrolled into a non‐randomized intervention cohort study if they were 16 years of age or older, planned to stay in the study area for at least three months after delivery, and provided written informed consent. HIV‐infected women and their infants were offered two‐dose nevirapine prophylaxis, and a six‐month supply of infant formula was offered free at any time in the first 12 months of the infant’s life. Antenatal counseling regarding infant feeding options was provided, as were home visits 3‐4 times during the first two weeks of life and every two weeks thereafter until the infant was six months old. Infants who were exclusively breastfed were compared to those receiving mixed breastfeeding and those receiving replacement feeding.
Risk of bias in included studies
2.
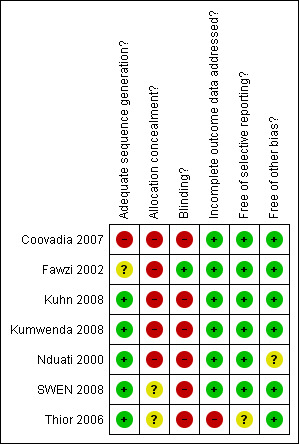
Risk of bias table. Green = low risk of bias; red = high risk of bias; yellow = bias risk is unclear.
3.
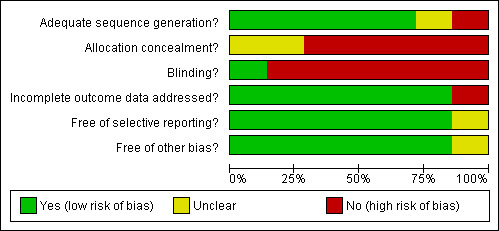
A plot of the distribution of judgements (Yes, Unclear and No) across studies for each risk of bias item.
Effects of interventions
Decreasing the duration of exposure to breast milk
In terms of decreasing the duration of exposure to breast milk, one randomized clinical trial compared MTCT of HIV and mortality among children of HIV‐infected women who were breastfed or formula fed (Nduati 2000). The trial demonstrated the efficacy of complete avoidance of breastfeeding (formula feeding) for the prevention of MTCT of HIV. The cumulative probability of HIV infection at 24 months was 36.7% (95% CI: 29.4‐44.0%) in the breastfeeding arm and 20.5% (95%CI: 14.0‐27.0%) in the formula arm (p = 0.001). Although the 2‐year mortality rates in both arms were similar [breastfeeding arm: 24.4% (95%CI: 18.2‐30.7%) vs. formula feeding arm: 20.0% (95%CI: 14.4‐25.6%); p = 0.30], the rate of HIV‐free survival at two years was significantly lower in the breastfeeding arm than in the formula feeding arm (58.0% vs. 70.0%, respectively, p = 0.02). Another randomized clinical trial evaluated early cessation of breastfeeding (Kuhn 2008). Child mortality rates were similar by 24 months in the two groups (23.9% in the intervention group and 24.6% in the control group (p = 0.96)). There was no significant difference in HIV‐free survival at 24 months of age between the two groups according to the intention‐to‐treat analysis (intervention group: 68.4%, control group: 64.0%; p = 0.13). Among uninfected children who were still being breastfed at 4 months, there was no significant difference between the groups in HIV‐free survival at 24 months (intervention group: 83.9%, control group: 80.7%; p = 0.27). Between 4 and 24 months, rates of postnatal HIV transmission were similar (6.2% in the intervention group and 8.8% in the control group, p = 0.19), as was mortality among uninfected children (10.7% in the intervention group and 11.7% in the control group; p = 0.71).
Decreasing maternal infectivity One clinical trial evaluated micronutrient supplementation for prevention of MTCT of HIV (Fawzi 2002). Multivitamins excluding vitamin A had no effect on the overall risk of HIV transmission (RR = 1.04; 95%CI: 0.82‐1.32; p = 0.76). Multivitamins were associated with non‐statistically significant reductions in transmission through breastfeeding. Vitamin A increased the risk of transmission (RR=1.38; 95%CI: 1.09‐1.76; p = 0.009). Multivitamins were associated with non‐statistically significant reduction in mortality by 24 months among infants with HIV infection and still alive at 6 weeks.
Modifying factors affecting the transfer of virus from mother to infant
One intervention cohort study evaluated the risk of MTCT according to infant feeding modality (Coovadia 2007). Of 1276 infants with complete feeding data, breastfed children who also received solids during the first six months of life were significantly more likely to become HIV‐infected than were exclusively breastfed children (HR 10.87; 95%CI = 1.51‐78.00; p=0.018). Cumulative 3‐month mortality in exclusively breastfed infants was 6.1% (4.74‐7.92) vs. 15.1% (7.63‐28.73) in infants given replacement feeds (HR 2.06; 1.00‐4.27, p=0.051).
Increasing infant defenses
Three trials evaluated antiretroviral prophylaxis to the breastfeeding infant for prevention of MTCT of HIV (Thior 2006, Kumwenda 2008, SWEN 2008).
Thior 2006: Breastfeeding with zidovudine prophylaxis during the first six months of life, with mothers instructed to initiate and complete weaning when the infant was between five and six months of age, was not as efficacious as formula feeding in preventing postnatal HIV transmission; the 7‐month HIV infection rates were 5.6% (32 infants in the formula fed group) vs. 9.0% (51 infants in the breastfed plus zidovudine group) (P = 0.04). Breastfeeding with zidovudine prophylaxis was associated with a lower mortality rate at 7 months, but both strategies had comparable HIV‐free survival at 18 months (despite a lower rate of HIV transmission with formula feeding). Cumulative mortality or HIV infection rates at 18 months were 80 infants (13.9%, formula fed) vs. 86 infants (15.1% breastfed plus zidovudine) (P = 0.60). Cumulative infant mortality at 7 months was significantly higher for the formula‐fed group than for the breastfed plus zidovudine group (9.3% vs. 4.9%; p = 0.003), but this difference diminished beyond month 7 such that the time‐to‐mortality distributions through age 18 months were not significantly different (P = 0.21).
Kumwenda 2008: Of 3016 infants, 255 were found to have HIV infection. Among infants who were not infected at birth, the control group had consistently higher rates of HIV infection between the ages of 6 weeks and 18 months, as compared with both extended‐prophylaxis groups. At 9 months, the estimated rate of HIV infection (primary end point) was 10.6% in the control group, 5.2% in the extended nevirapine group (P < 0.001), 6.4% in the extended dual prophylaxis group (P = 0.002). In this trial, mothers were counseled to breastfeed exclusively for six months and to consider weaning thereafter. There were no significant differences in terms of transmission between the two extended‐prophylaxis groups. There were no statistically significant differences in mortality by study arm.
HIV‐free survival was significantly better through the age of 9 months in both extended prophylaxis groups, and through the age of 15 months in the extended nevirapine group.
SWEN 2008: At six weeks of age, more children in the control group (one dose of nevirapine) than the extended‐dose nevirapine group were infected (relative risk: 0.54; 0.34‐0.86; p=0.009). However, at six months of age, the risk of transmission was similar (relative risk 0.80; 0.58‐1.10; p=0.16). HIV‐free survival was higher in the extended prophylaxis arm, at both six weeks (p = 0.008) and six months (p = 0.03).
Discussion
Summary of main results
Six randomized clinical trials and one intervention cohort study were included in this review. Complete avoidance of breastfeeding is efficacious in preventing MTCT of HIV. If breastfeeding is initiated, two interventions are efficacious in preventing transmission: 1) exclusive breastfeeding; and 2) extended antiretroviral prophylaxis.
Specifically, breastfed children who also received solids had higher rates of MTCT of HIV as well as higher three‐month mortality rates (compared to exclusive breastfeeding). With regard to antiretroviral prophylaxis, in a population of HIV‐infected women counseled to breastfeed exclusively for six months and to consider weaning thereafter, administration of nevirapine alone or nevirapine with zidovudine until the age of 14 weeks prevents more transmission by 9 months of age than a short‐course of antiretrovirals (one dose of nevirapine and one week of zidovudine). HIV‐free survival was significantly better through the age of 9 months in both extended prophylaxis groups, and through the age of 15 months in the extended nevirapine group.
Authors' conclusions
Implications for practice.
To date, three interventions have been identified for the prevention of late postnatal (breastfeeding) transmission of HIV: complete avoidance of breastfeeding, exclusive breastfeeding, and antiretroviral prophylaxis to the breastfeeding infant. Morbidity associated with complete avoidance of breastfeeding (e.g., diarrheal and respiratory disease), in addition to the cost of purchasing formula or other replacement milk and the stigma associated with not breastfeeding, are significant, and in many situations make this intervention infeasible.
Counseling and support for exclusive breastfeeding have increased the proportion of women who pursue this modality of infant feeding. However, this is time and resource intensive, and will require investment of significant resources in order to have a significant effect in terms of decreasing MTCT of HIV and/or increasing HIV‐free survival.
Infant nevirapine prophylaxis for six weeks or 14 weeks (among infants of mothers who were counseled to breastfeed exclusively for six months and to consider weaning thereafter) has shown promise with regard to prevention of MTCT of HIV and for improvement in HIV‐free survival. Such infant antiretroviral prophylaxis was well‐tolerated. However, the implications of the studies to date are that antiretroviral prophylaxis to the breastfeeding infant must continue for the duration of breastfeeding (since the efficacy observed with administration for six or 14 weeks dissipates after prophylaxis is discontinued). Nevirapine resistance among those infants who fail prophylaxis and become infected while receiving nevirapine (Arrive 2007) warrants further evaluation.
Implications for research.
Efficacious interventions for the prevention of late postnatal MTCT of HIV through breastfeeding have been developed, but additional research is needed. It is important to characterize more completely the mechanism(s) of breast milk transmission of HIV, and to conduct operational research regarding the implementation of efficacious interventions. Possible limitations of existing interventions (e.g., nevirapine resistance among those infants who fail prophylaxis and become infected while receiving nevirapine) need to be evaluated and understood, the safety profile of available interventions needs to be evaluated further, and new and better interventions developed.
What's new
| Date | Event | Description |
|---|---|---|
| 9 November 2009 | Amended | Notice that this review will be split, and that future updates to this review will be of a different scope. |
History
Protocol first published: Issue 3, 2007 Review first published: Issue 1, 2009
| Date | Event | Description |
|---|---|---|
| 10 December 2008 | Amended | Corrected one of the additional references (changed one to Safrit 2004); added author contributions; made a few subtle edits for clarity. |
Acknowledgements
Valériane Leroy and Francois Dabis, Institut de Santé Publique, Epidémiologie et Développement (ISPED), Bordeaux Cedex, France
Nathan A. Smith, Global Health Sciences, University of California, San Francisco
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Coovadia 2007.
| Methods | Non‐randomized intervention cohort study | |
| Participants | HIV‐infected and uninfected pregnant women attending antenatal clinics in KwaZulu Natal were enrolled into a non‐randomized intervention cohort study if they were 16 years of age or older, planned to stay in the study area for at least 3 months after delivery, and provided written informed consent. Uninfected women were included to establish the effect of HIV status on adherence to exclusive breastfeeding and other infant feeding practices. | |
| Interventions | Exclusive breastfeeding (antenatal counseling regarding infant feeding options, home visits 3‐4 times during first 2 weeks of life, and every 2 weeks thereafter until the infant was 6 months old. | |
| Outcomes | HIV status: 1276 infants with complete feeding data. 14.1 (95%CI: 12.0‐16.4) of exclusively breastfed infants infected with HIV by age 6 weeks and 19.5% (17.0‐22.4) by 6 months; the risk was significantly associated with maternal CD4 cell counts below 200 cells/mm3 (adjusted HR 3.79; 2.35‐6.12) and birth weight < 2500 grams (1.81; 1.07‐3.06). Breast infants who also received solid food during their first six months of life were significantly more likely to acquire infection than were exclusively breastfed children (HR 10;87; 1.51‐78.00; p=0.018), as were infants who at 12 weeks received both breast milk and formula milk (1.82; 0.98‐3.36; p=0.057). Mortality: Cumulative 3‐month mortality was15.1% (7.63‐28.73) in infants given replacement feeds vs. 6.1% (4.74‐7.92) among exclusively breastfed infants (HR 2.06; 1.00‐4.27, p=0.51). |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | High risk | Not a randomized controlled trial |
| Allocation concealment? | High risk | Not a randomized controlled trial |
| Blinding? All outcomes | High risk | This study was not blinded. |
| Incomplete outcome data addressed? All outcomes | Low risk | "Data for nevirapine uptake and ingestion were inconsistent and are not included in any analysis." |
| Free of selective reporting? | Low risk | No problems apparent |
| Free of other bias? | Low risk | No problems apparent |
Fawzi 2002.
| Methods | Randomized controlled trial | |
| Participants | Pregnant women presenting to public antenatal clinics (in the era before interventions to prevent MTCT of HIV were available locally) between 12 and 27 weeks gestation who resided in Dar es Salaam, Tanzania, and who intended to stay in the city until after delivery and for at least 1 year thereafter were enrolled. Median age ˜24 years; CD4 count ˜ 420 | |
| Interventions | Eligible women were randomly assigned in a two‐by‐two factorial design to receive a daily oral dose of one or four regimens from enrolment and throughout the pregnancy and lactation periods:
At delivery, women in groups 1 and 3 received an additional oral dose of vitamin A (200,000 IU), and women in groups 2 and 4 received placebo. Those infants whose mothers received multivitamins were compared to infants whose mothers did NOT receive multivitamins. Similarly, those infants whose mothers received vitamin A were compared to infants whose mothers did NOT receive vitamin A. |
|
| Outcomes | HIV infection status: Multivitamins (vitamins B, C, and E) had no effect on the overall risk of HIV transmission (RR = 1.04; 95%CI: 0.82‐1.32; p = 0.76). Multivitamins were associated with non‐statistically significant reductions in transmission through breastfeeding. More cases of HIV infection were observed among children of mothers in the vitamin A arm compared with those who did not receive vitamin A (RR=1.38; 95%CI: 1.09‐1.76; p = 0.009). Mortality: Multivitamins (vitamins B, C, and E) had a modest and not statistically significant reduction in mortality by 24 months or the combined risks of infection and mortality among children. |
|
| Notes | Not all study details were provided in this publication. "Details of the study design have been published [9,10]" (referring to Fawzi 2000 and Fawzi 1998). Fawzi 2000 says: "Details of the study design have been published elsewhere (10,11)" (referring to Fawzi 1999 and Fawzi 1998). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Unclear risk | "We assigned women randomly to receive a daily oral dose." (From Fawzi 1999) |
| Allocation concealment? | High risk | Not addressed |
| Blinding? All outcomes | Low risk | "We realized that unblinding, whether real or based on an impression or perception that may develop among subjects or staff, is more likely to occur if regimens are color‐coded or bear simple numeric codes. To minimize this risk, we provided the regimen in bottles labeled with the subjects’ names and identification numbers, and made active tablets and placebo indistinguishable, so that neither the subjects nor the investigators could identify which subjects were randomized to the same regimen." (From Fawzi 1999) |
| Incomplete outcome data addressed? All outcomes | Low risk | "We also developed a system for tracking the survival of all women not in active follow‐up, by visiting their homes regularly and asking questions of neighbors, relatives, and friends. Through these methods, we have kept loss to follow‐up down to about 5% per year. We anticipated these inevitable losses, and other losses due to mortality, and factored them in our sample‐size calculation." (From Fawzi 1999) |
| Free of selective reporting? | Low risk | No problems apparent. |
| Free of other bias? | Low risk | No problems apparent. |
Kuhn 2008.
| Methods | Randomized controlled trial | |
| Participants | HIV‐infected women were recruited from two antenatal clinics in Lusaka, Zambia that offered VCT and the two dose nevirapine prophylaxis regimen (one dose to mother, one dose to infant) prophylaxis. Pregnant women (less than 38 weeks gestation) were recruited. Women could volunteer if they intended to breastfeed for any length of time, accepted treatment with nevirapine, and agreed to be randomly assigned to the intervention or control group. Exclusion criteria were severe pregnancy complications (e.g., pre‐eclampsia), previous cesarean delivery, and HIV‐related conditions requiring hospitalization. Median CD4 count of mothers at baseline was ˜330 cells/mm3. The maternal plasma viral load (median) was about 36,000‐41,000 copies/mL. Slightly over a third of the women were eligible for antiretroviral therapy. The mean age was 26 years. 84‐85% were married. Over half of mothers had no schooling or only primary school education. 3216 women and 3276 infants were enrolled, and infants underwent randomization at birth; of 3276 infants assigned an intervention, 3106 were included in the primary analysis; of these, 2389 reached the HIV infection endpoint OR did not have HIV infection and were under follow‐up or completed follow‐up. Median maternal age was ˜26 years. ˜2/3 had < grade 8 education; median CD4 count was ˜400; ˜2/3 presented early (>4 hours before delivery) |
|
| Interventions | Early, abrupt weaning Participants were randomly assigned to one of two groups. The experimental intervention encouraged women to breastfeed exclusively to 4 months and then to stop breastfeeding abruptly, or as rapidly as possible. Women in the control group were encouraged to breastfeed exclusively to 6 months, gradually introduce complementary foods, and continue to breastfeed for a duration of their own choice (standard practice). |
|
| Outcomes | Child mortality rates were similar by 24 months in the two groups: 23.9% in the intervention group and 24.6% in the control group (p = 0.96). There was no significant difference in HIV‐free survival between the two groups according to the intention‐to‐treat analysis: at 24 months of age, 68.4% of children in the intervention group and 64.0% in the control group were alive and not infected with HIV (p = 0.13) Among uninfected children who were still being breastfed at 4 months, there was no significant difference between the groups in HIV‐free survival at 24 months: 83.9% of the children in the intervention group survived to 24 months without HIV infection, as compared with 80.7% in the control group (p = 0.27). Between 4 and 24 months, rates of postnatal HIV transmission were not significantly different (6.2% in the intervention group and 8.8% in the control group, p = 0.19), and mortality among uninfected children was similar in the two groups (0.7% in the intervention group and 11.7% in the control group, p = 0.71). |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Low risk | Use of a computer algorithm with randomized permuted block design within each site |
| Allocation concealment? | High risk | "Participants were informed of their assignment at the next (usually second‐month) visit to ensure sufficient time for preparation." |
| Blinding? All outcomes | High risk | This study was not blinded. |
| Incomplete outcome data addressed? All outcomes | Low risk | "Home‐visit teams tracked the participants who did not return for appointments. Information about children’s deaths was sought from hospital and clinic records and from interviews with caretakers and health care personnel. The circumstances of all deaths were reviewed to identify the causes of death." |
| Free of selective reporting? | Low risk | No problems apparent |
| Free of other bias? | Low risk | No problems apparent |
Kumwenda 2008.
| Methods | Randomized controlled trial | |
| Participants | Pregnant women who presented for either antenatal or delivery services at specific health centers in Blantyre, Malawi were offered HIV counseling and testing. All women with HIV infection, except those late presenters whose HIV infection was not identified until after they gave birth, received a single intrapartum dose of nevirapine. Women could be enrolled in the trial if they had HIV infection, were at least 18 years of age (although women <18 years of age could be enrolled if they consented and a guardian gave permission), were pregnant or had given birth within the previous 24 hours at one of the study clinics, were a resident of the study area, were willing to return for postnatal follow‐up visits for up to 2 years, and intended to breastfeed. The study excluded infants with life‐threatening conditions requiring immediate care. Mothers were counseled to breastfeed exclusively for six months and to consider weaning thereafter. | |
| Interventions | Arm 1: single dose nevirapine PLUS 1 week of zidovudine (control regimen) Arm 2: control regimen PLUS daily nevirapine starting at age 7 days until the age of 14 weeks Arm 3: control regimen PLUS daily nevirapine with zidovudine starting at age 7 days until the age of 14 weeks The control regimen was single dose nevirapine PLUS 1 week of zidovudine. (Those women who enrolled early enough received one dose of intrapartum nevirapine; some women (approximately 30%) presented too late to receive intrapartum nevirapine.) |
|
| Outcomes | HIV infection status: Of 3016 infants, 255 were found to have HIV infection (242 confirmed and 13 presumptive). Among infants who were not infected at birth, between the ages of 6 weeks and 18 months, the control group had consistently higher rates of HIV infection, as compared with both extended‐prophylaxis groups. At 9 months, the estimated rate of HIV infection (primary end point) was 10.6% in the control group, 5.2% extended nevirapine group (P < 0.001), 6.4% in extended dual prophylaxis group (P = 0.002). There were no significant differences between the two extended‐prophylaxis groups. The estimated protective efficacy of the extended prophylaxis regimens were: 6 weeks:
14 weeks:
6 months:
9 months:
Mortality: No statistically significant differences in mortality by study arm. HIV‐free survival was significantly better through the age of 9 months in both extended prophylaxis groups, and through the age of 15 months in the extended nevirapine group. |
|
| Notes | Adverse effects: Infants receiving nevirapine + zidovudine prophylaxis had a significant increase in the number of adverse events (primarily neutropenia) deemed possibly related to a study drug. There was no difference in adverse events between the control group and the nevirapine only prophylaxis group. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Low risk | "Randomization procedures employed permutated block algorithms of sizes 9 and 12, stratified by study clinic. A computer generated randomization list assigned infants to the appropriate treatment arms using a 1:1:1 allocation ratio. Randomization numbers were placed in sequentially labeled and sealed envelopes." (From Kumwenda 2008) |
| Allocation concealment? | High risk | Not addressed |
| Blinding? All outcomes | High risk | This study was not blinded. |
| Incomplete outcome data addressed? All outcomes | Low risk | "All Grade 3‐4 toxicities, rashes Grade 2B or higher and ALT levels Grade 2 or higher were considered serious. Serious adverse events, including deaths and hospitalizations, were reported to the University of Malawi, Johns Hopkins University, and CDC Institutional Review Boards (IRBs). Abnormal clinical and laboratory findings were followed until resolution to Grade 2 or lower. Infants discontinued from study drug(s) were followed for the study duration." (From Kumwenda 2008 Supplement) |
| Free of selective reporting? | Low risk | No problems apparent |
| Free of other bias? | Low risk | No problems apparent. |
Nduati 2000.
| Methods | Randomized controlled trial | |
| Participants | Pregnant women attending 4 Nairobi antenatal clinics (in the era before interventions to prevent MTCT of HIV were available locally) were offered counseling and serologic testing for HIV. Seropositive women were invited to attend the research clinic at Kenyatta National Hospital. Women were eligible if they resided in Nairobi and had access to municipal‐treated water. Women were randomized to breastfeed or formula feed at about 32 weeks. Of 2315 HIV seropositive women, 1708 (74%) returned to receive their results. Of these, 425 (25%) were enrolled (18% of all seropositive pregnant women). Median age of enrolled women = 23 years. 61% of women living in a 1‐room home, 74% sharing a toilet with other households, 5% owning a refrigerator. All women had access to clean water, 76% had access to flush sanitation. At 32 weeks gestation, 47/381 women (12%) had CD4 < 200 cells/mm3. Median plasma viral load at this visit was 42,360 copies/mL. |
|
| Interventions | Formula feeding instead of breastfeeding. Those randomized to formula feeding were compared to those randomized to breastfeeding. | |
| Outcomes | HIV status: The cumulative probability of HIV infection at 24 months was 36.7% (95% CI: 29.4‐44.0%) in the breastfeeding arm and 20.5% (95%CI: 14.0‐27.0%) in the formula arm (p = 0.001). Morbidity: Mbori‐Ngacha 2001 addresses morbidity: Of 401 live born, singleton or first‐born twin infants of randomized HIV‐seropositive mothers, 371 were included in the analysis of morbidity and mortality. Incidence of diarrhea during the 2 years of follow‐up was similar in formula and breastfeeding arms (155 vs 149 per 100 person‐years, respectively). The incidence of pneumonia was identical in the 2 groups (62/100 person years). There were no significant differences in incidence of other recorded illnesses. Mortality The 2‐year mortality rates in both arms were similar: (breastfeeding arm: 24.4% (95%CI: 18.2‐30.7%) vs. formula feeding arm: 20.0% (95%CI: 14.4‐25.6%); p = 0.30 The rate of HIV‐free survival at 2 years was significantly lower in the breastfeeding arm than in the formula feeding arm (58.0% vs. 70.0%, respectively, p = 0.02). |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Low risk | "Women were randomized to breastfeed or formula feed at about 32 weeks using computer‐generated block randomization." |
| Allocation concealment? | High risk | Not applicable |
| Blinding? All outcomes | High risk | This study was not blinded. |
| Incomplete outcome data addressed? All outcomes | Low risk | "We did not present secondary analyses of self‐reported feeding behavior and HIV transmission or mortality, because feeding practices may be associated with confounding variables that affect primary study outcomes." |
| Free of selective reporting? | Low risk | No problems apparent |
| Free of other bias? | Unclear risk | "Because more than one quarter of women in the formula arm admitted to noncompliance with feeding modality, our estimated breast milk transmission rate is an underestimate." |
SWEN 2008.
| Methods | Randomized controlled trial | |
| Participants | Pregnant women who presented to antenatal and delivery facilities in Addis Ababa, Ethiopia, Pune, India, and Kampala, Uganda, who were identified as HIV‐infected, were offered the local standard of care for prevention of MTCT of HIV and provided infant feeding counseling, consistent with WHO/UNICEF guidelines. Women were eligible for study enrolment if they indicated an intention to breastfeed their infants and provided informed consent. | |
| Interventions | In Arm 1 (control arm) of the trials, 200 mg nevirapine was provided to women in labor and 2 mg/kg to infants shortly after birth. In Arm 2 of the trials, this two‐dose nevirapine regimen was provided in addition to infant dosing of 5 mg nevirapine each day starting at age 7 days through six weeks of life. The risk of HIV infection and death at 6 weeks and 6 months of age in infants who were HIV‐uninfected at birth was estimated. The analysis included data for 1887 infants. | |
| Outcomes | At six weeks of age, more children in the single‐dose nevirapine group than the extended‐dose nevirapine group were infected (relative risk: 0.54; 0.34‐0.86; p=0.009). However, at six months of age, the risk of transmission was similar (relative risk 0.80; 0.58‐1.10; p=0.16). HIV‐free survival was higher in the extended prophylaxis arm, at both six weeks (p = 0.008) and six months (p = 0.03). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Low risk | "For all three countries, block randomisation was used with treatment assignments generated by computer at a central data coordinating centre at Johns Hopkins University. The randomisation list was provided to study pharmacists only in each country." |
| Allocation concealment? | Unclear risk | "Study products were administered by pre‐filled amber oral syringes in Ethiopia and Uganda and by opaque dropper bottles in India, after training of mothers by study pharmacists .A number of specific study procedures were implemented to introduce some degree of masking of study staff and care givers. Specifically, none of the study investigators or staff, with the exception of the study pharmacists and a member of the central data management team, had access to the randomization assignments for study participants." Because study pharmacists knew the randomization assignments, however, and worked directly with the mothers, it is possible that allocation was not sufficiently well concealed. |
| Blinding? All outcomes | High risk | "This study was not blinded"; However, "[t]he reliability of the HIV PCR results were assessed through a centralised quality assurance programme, coordinated by the laboratory of one of the authors (JBJ) at Johns Hopkins School of Medicine, which included blinded retesting of samples from HIV‐infected infants and a random sample of HIV‐uninfected infants. Final infant infection status was assigned for each country by a blinded study investigator and results from all three countries were subsequently reviewed by a fourth blinded investigator (JBJ) to ensure consistency across the countries. |
| Incomplete outcome data addressed? All outcomes | Low risk | "Since many infant deaths occurred at home or outside of the study clinics, information about the cause of these deaths was limited to verbal autopsy interviews of mothers and other family members. Thus, HIV status at the time of death was not available for infants who could have become HIV positive between their last study visit and their death. 38 (72%) of the deaths occurred among infants for whom their last HIV screening test was negative by HIV PCR. However, the mean time from this last study visit until death was 13·8 (SD 17·7) days, decreasing the likelihood that we failed to identify HIV‐infected infants before their death. We assessed the distribution of mortality by sex, because of an imbalance between study groups at baseline, but there was no significant difference between males and females in terms of the distribution of overall mortality (data not shown). We found no differences between groups in other factors that might be associated with infant mortality, including maternal age, maternal CD4 cell count, maternal viral load (available in India and Uganda), maternal education level, parity, gravidity, and gestational age at enrolment (data not shown)." |
| Free of selective reporting? | Low risk | No problems apparent. |
| Free of other bias? | Low risk | No problems apparent. |
Thior 2006.
| Methods | Randomized controlled trial | |
| Participants | 1200 HIV‐infected women were randomized. Primary efficacy (HIV infection by age 7 months and HIV‐free survival by age 18 months) and safety (occurrence of infant adverse events by 7 months of age) end points were evaluated in 1179 infants. Median maternal age = 26.78 years; 55% had water tap in the yard, 37% used communal standpipe; 74% cited private latrine/house as the most used sanitation facility; 24% had electricity in the home; the maternal baseline CD4 count was 366 cells/mm3 and the median maternal baseline plasma viral load was 4.35 log10 copies/mL | |
| Interventions | Mothers were instructed to initiate and complete weaning when the infant was between five and six months of age. Infants were randomized to 6 months of breastfeeding plus prophylactic infant zidovudine (breastfed plus 6 months of zidovudine) or formula feeding plus 1 month of infant zidovudine (formula fed). Infants received zidovudine syrup 4 mg/kg/12 hours from birth until 1 month of age in all infants, and discontinued at 1 month in the formula‐fed group. For the breastfed plus zidovudine group, infant zidovudine prophylaxis continued from 1 to 2 months of age at 4 mg/kg/8 hours, and from 2 to 6 months of age (while still breastfeeding) at 6 mg/kg/8 hours. (All mothers received zidovudine 300 mg orally twice daily from 34 weeks gestation and during labor.). Mothers and infants were randomized to receive single‐dose nevirapine or placebo. |
|
| Outcomes | Morbidity: The rates of grade 3 or higher signs or symptoms (17.6% vs. 13.1%; P = 0.03) and of hospitalization (20.3% vs. 15.6%, P = 0.04) by 7 months were significantly higher among infants in the formula‐fed group than in the breastfed plus zidovudine group. Mortality: Cumulative mortality or HIV infection rates at 18 months were 80 infants (13.9%, formula fed) vs. 86 infants (15.1% breastfed plus zidovudine) (P = 0.60). Cumulative infant mortality at 7 months was significantly higher for the formula‐fed group than for the breastfed plus zidovudine group (9.3% vs. 4.9%; p = 0.003), but this difference diminished beyond month 7 such that the time‐to‐mortality distributions through age 18 months were not significantly different (P = 0.21). Therefore, breastfeeding with zidovudine prophylaxis for six months was associated with a lower mortality rate at 7 months, but both strategies had comparable HIV‐free survival at 18 months. |
|
| Notes | Adverse effects: The rate of grade 3 or higher laboratory abnormality associated with zidovudine toxicity was significantly higher in the breastfed plus zidovudine group than in the formula‐fed group (24.7% vs. 14.8%) (P < 0.001). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Low risk | Centralized randomization to both part 1 and part 2 groups occurred at study enrolment (34 weeks gestation), using permuted blocks of size 8 within each site. |
| Allocation concealment? | Unclear risk | Probably done, but exactly how is unclear. |
| Blinding? All outcomes | High risk | This study was not blinded. |
| Incomplete outcome data addressed? All outcomes | High risk | Not addressed. |
| Free of selective reporting? | Unclear risk | Possibly some post‐randomization selection bias. |
| Free of other bias? | Low risk | No problems apparent. |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Becquet 2006 | Not a randomized clinical trial (prospective cohort study); mothers had received antiretrovirals perinatally. |
| Becquet 2008 | Not a randomized clinical trial (open‐labeled cohort study); mothers had received antiretrovirals perinatally. |
| Bobat 1997 | Not a randomized clinical trial (prospective cohort study). |
| Dabis 1999 | This study addressed in utero/intrapartum transmission (not a trial addressing prevention of late postnatal transmission) |
| Embree 2000 | Not a randomized clinical trial (longitudinal observational cohort study). |
| Gray 2005 | This study addresses prevention of peripartum transmission of HIV. Was not designed (and did not address) late postnatal/breastfeeding transmission of HIV. |
| Guay 1999 | This study addressed in utero/intrapartum transmission (not a trial addressing prevention of late postnatal transmission) |
| Iliff 2005 | This is analysis of data regarding infant feeding (data came from a randomized trial addressing a different topic), i.e., this is an analysis of prospectively collected data regarding infant feeding modalities and infant HIV infection status. |
| Kilewo 2008 | Not a randomized clinical trial (prospective cohort study). |
| Miotti 1999 | Not a randomized clinical trial (prospective cohort study). |
| SIMBA 2003 | Abstract only ‐ manuscript was never published. Authors of the study were contacted, but no further information was obtained. |
Contributions of authors
Tara Horvath screened abstracts, selected studies, abstracted data, assessed the risk of bias, reviewed the manuscript, and managed the project. Banyana Madi drafted a related, earlier version of the review, contributed to the protocol of the present review, and reviewed the manuscript. Irene Iuppa screened abstracts, selected studies, abstracted data, and reviewed the manuscript. Gail Kennedy and George Rutherford also contributed to the protocols design, and reviewed the manuscript. Jennifer Read screened abstracts, selected studies, abstracted data, and wrote most of the manuscript.
Sources of support
Internal sources
Global Health Sciences, University of California, San Francisco, USA.
External sources
No sources of support supplied
Declarations of interest
None of the authors have any conflict of interest.
Edited (no change to conclusions)
References
References to studies included in this review
Coovadia 2007 {published data only}
- Coovadia HM, Rollins NC, Bland RM, Little K, Coutsoudis A, Bennish ML, et al. Mother‐to‐child transmission of HIV‐1 infection during exclusive breastfeeding in the first 6 months of life: an intervention cohort study. Lancet 2007;369(9567):1107‐16. [PUBMED: 17398310] [DOI] [PubMed] [Google Scholar]
Fawzi 2002 {published data only}
- Fawzi WW, Msamanga GI, Hunter D, Renjifo B, Antelman G, Bang H, et al. Randomized trial of vitamin supplements in relation to transmission of HIV‐1 through breastfeeding and early child mortality. AIDS 2002;16(14):1935‐44. [PUBMED: 12351954] [DOI] [PubMed] [Google Scholar]
Kuhn 2008 {published data only}
- Kuhn L, Aldrovandi GM, Sinkala M, Kankasa C, Semrau K, Mwiya M, et al. Effects of early, abrupt weaning on HIV‐free survival of children in Zambia. N Engl J Med 2008;359(2):130‐41. [PUBMED: 18525036] [DOI] [PMC free article] [PubMed] [Google Scholar]
Kumwenda 2008 {published data only}
- Kumwenda NI, Hoover DR, Mofenson LM, Thigpen MC, Kafulafula G, Li Q, et al. Extended antiretroviral prophylaxis to reduce breast‐milk HIV‐1 transmission. N Engl J Med 2008;359(2):119‐29. [PUBMED: 18525035] [DOI] [PubMed] [Google Scholar]
Nduati 2000 {published data only}
- Nduati R, John G, Mbori‐Ngacha D, Richardson B, Overbaugh J, Mwatha A, et al. Effect of breastfeeding and formula feeding on transmission of HIV‐1: a randomized clinical trial. JAMA 2000;283(9):1167‐74. [PUBMED: 10703779] [DOI] [PubMed] [Google Scholar]
SWEN 2008 {published data only}
- Bedri A, Gudetta B, Isehak A, Kumbi S, Lulseged S, Mengistu Y, et al. Extended‐dose nevirapine to 6 weeks of age for infants to prevent HIV transmission via breastfeeding in Ethiopia, India, and Uganda: an analysis of three randomized controlled trials. Lancet 2008;372(9635):300‐13. [PUBMED: 18657709] [DOI] [PubMed] [Google Scholar]
Thior 2006 {published data only}
- Thior I, Lockman S, Smeaton LM, Shapiro RL, Wester C, Heymann SJ, et al. Breastfeeding plus infant zidovudine prophylaxis for 6 months vs formula feeding plus infant zidovudine for 1 month to reduce mother‐to‐child HIV transmission in Botswana: a randomized trial: the Mashi Study. JAMA 2006;296(7):794‐805. [PUBMED: 16905785] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Becquet 2006 {published data only}
- Becquet R, Leroy V, Ekouevi DK, Viho I, Castetbon K, Fassinou P, et al. Complementary feeding adequacy in relation to nutritional status among early weaned breastfed children who are born to HIV‐infected mothers: ANRS 1201/1202 Ditrame Plus, Abidjan, Cote d'Ivoire. Pediatrics 2006;117(4):e701‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
Becquet 2008 {published data only}
- Becquet R, Ekouevi DK, Menan H, Amani‐Bosse C, Bequet L, Viho I, et al. Early mixed feeding and breastfeeding beyond 6 months increase the risk of postnatal HIV transmission: ANRS 1201/1202 Ditrame Plus, Abidjan, Cote d'Ivoire. Preventive Medicine 2008;47(1):27‐33. [PUBMED: 18190955] [DOI] [PubMed] [Google Scholar]
Bobat 1997 {published data only}
- Bobat R, Moodley D, Coutsoudis A, Coovadia H. Breastfeeding by HIV‐1‐infected women and outcome in their infants: a cohort study from Durban, South Africa. AIDS 1997;11(13):1627‐33. [DOI] [PubMed] [Google Scholar]
Dabis 1999 {published data only}
- Dabis F, Msellati P, Meda N, Welffens‐Ekra C, You B, Manigart O, et al. 6‐month efficacy, tolerance, and acceptability of a short regimen of oral zidovudine to reduce vertical transmission of HIV in breastfed children in Cote d'Ivoire and Burkina Faso: a double‐blind placebo‐controlled multicentre trial. DITRAME Study Group. DIminution de la Transmission Mere‐Enfant. Lancet 1999;353(9155):786‐92. [DOI] [PubMed] [Google Scholar]
Embree 2000 {published data only}
- Embree JE, Njenga S, Datta P, Nagelkerke NJ, Ndinya‐Achola JO, Mohammed Z, et al. Risk factors for postnatal mother‐child transmission of HIV‐1. AIDS 2000;14(16):2535‐41. [DOI] [PubMed] [Google Scholar]
Gray 2005 {published data only}
- Gray GE, Urban M, Chersich MF, Bolton C, Niekerk R, Violari A, et al. A randomized trial of two postexposure prophylaxis regimens to reduce mother‐to‐child HIV‐1 transmission in infants of untreated mothers. AIDS 2005;19(12):1289‐97. [DOI] [PubMed] [Google Scholar]
Guay 1999 {published data only}
- Guay LA, Musoke P, Fleming T, et al. Intrapartum and neonatal single‐dose nevirapine compared with zidovudine for prevention of mother‐to‐child transmission of HIV‐1 in Kampala, Uganda: HIVNET 012 randomized trial. Lancet 1999;354(9181):795‐802. [DOI] [PubMed] [Google Scholar]
Iliff 2005 {published data only}
- Iliff PJ, Piwoz EG, Tavengwa NV, Zunguza CD, Marinda ET, Nathoo KJ, et al. Early exclusive breastfeeding reduces the risk of postnatal HIV‐1 transmission and increases HIV‐free survival. AIDS 2005;19(7):699‐708. [DOI] [PubMed] [Google Scholar]
Kilewo 2008 {published data only}
- Kilewo C, Karlsson K, Massawe A, Lyamuya E, Swai A, Mhalu F, et al. Prevention of mother‐to‐child transmission of HIV‐1 through breast‐feeding by treating infants prophylactically with lamivudine in Dar es Salaam, Tanzania: the Mitra Study. J Acquir Immune Defic Syndr 2008;48(3):315‐23. [PUBMED: 18344879] [DOI] [PubMed] [Google Scholar]
Miotti 1999 {published data only}
- Miotti PG, Taha TE, Kumwenda NI, Broadhead R, Mtimavalye LA, Hoeven L, et al. HIV transmission through breastfeeding: a study in Malawi. JAMA 1999;282(8):744‐9. [DOI] [PubMed] [Google Scholar]
SIMBA 2003 {published data only}
- Vyankandondera J, Luchters S, Hassink E, et al. Reducing risk of HIV‐1 transmission from mother to infant through breastfeeding using antiretroviral prophylaxis in infants (SIMBA study) [abstract # LB7]. Paper presented at: the 2nd International AIDS Society Conference on HIV Pathogenesis and Treatment; 2003.
Additional references
AAP 1995
- American Academy of Pediatrics, Committee on Pediatric AIDS. Human milk, breastfeeding, and transmission of human immunodeficiency virus in the United States. Pediatrics 1995;96 977 –979. [PubMed] [Google Scholar]
Arendt 2007
- Arendt V, Ndimubanzi P, Ndayabisa G, Muganda J, Courteille O, Rudanga C, et al. AMATA Study: effectiveness of antiretroviral therapy in breastfeeding mothers to prevent post‐natal vertical transmission in Rwanda [Abstract TuAX102]. Paper presented at the 4th International AIDS Society Conference on HIV Pathogenesis, Treatment and Prevention, 2007.
Arrive 2007
- Arrivé E, Newell ML, Ekouevi DK, Chaix ML, Thiebaut R, Masquelier B, et al. Prevalence of resistance to nevirapine in mothers and children after single‐dose exposure to prevent vertical transmission of HIV‐1: a meta‐analysis. Int J Epidemiol 2007 Oct;36(5):1009‐21. [DOI] [PubMed] [Google Scholar]
Becquart 1999
- Becquart P, Gressenguet G, Hocini H, Kazatchkine MD, Belec L. Secretory leukocyte protease inhibitor in colostrum and breast milk is not a major determinant of the protection of early postnatal transmission of HIV. AIDS 1999;13 2599–2602. [DOI] [PubMed] [Google Scholar]
Becquart 2000
- Becquart P, Hocini H, Levy M, Sepou A, Kazatchkine MD, Belec L. Secretory anti‐human immunodeficiency virus (HIV) antibodies in colostrum and breast milk are not a major determinant of the protection of early postnatal transmission of HIV. J Infect Dis 2000;181 532 –539. [DOI] [PubMed] [Google Scholar]
BHITS 2004
- Breastfeeding and HIV International Transmission Study Group. Late postnatal transmission of HIV‐1 in breast‐fed children: An individual patient data meta‐analysis. J Infect Dis 2004;189:2154‐2166. [DOI] [PubMed] [Google Scholar]
Bland 2008
- Bland RM, Little KE, Coovadia HM, Coutsoudis A, Rollins NC, Newell ML. Intervention to promote exclusive breast‐feeding for the first 6 months of life in a high HIV prevalence area. AIDS 2008;22(7):883‐91. [PUBMED: 18427207] [DOI] [PubMed] [Google Scholar]
Bond 2007
- Bond K, Horváth T, Harvey K, Wiysonge CS, Read JS. The Cochrane Library and mother‐to‐child transmission of HIV: an umbrella review. Evidence‐Based Child Health: A Cochrane Review Journal 2007;2(1):4‐24. [Google Scholar]
Catassi 1995
- Catassi C, Bonucci A, Coppa GV, Carlucci A, Giorgi PL. Intestinal permeability changes during the first month: effect of natural versus artificial feeding. J Pediatr Gastroenterol Nutr 1995 Nov;21(4):383‐86. [DOI] [PubMed] [Google Scholar]
Cesar 1999
- Cesar JA, Victora CG, Barros FC, Santos IS, Flores JA. Impact of breast feeding on admission for pneumonia during postneonatal period in Brazil nested case‐control study. BMJ 1999;318 1316 –1320. [DOI] [PMC free article] [PubMed] [Google Scholar]
Coovadia 2007
- Coovadia HM, Rollins NC, Bland RM, Little K, Coutsoudis A, Bennish ML, Newell ML. Mother‐to‐child transmission of HIV‐1 infection during exclusive breastfeeding in the first 6 months of life: an intervention cohort study. Lancet 2007;369:1107‐16. [DOI] [PubMed] [Google Scholar]
Coutsoudis 1999
- Coutsoudis A, Pillay K, Spooner E, Kuhn L, Coovadia HM. Influence of infant‐feeding patterns on early mother‐to‐child transmission of HIV in Durban, South Africa a prospective cohort study. South African Vitamin A Study Group. Lancet 1999;354 471 –476. [DOI] [PubMed] [Google Scholar]
Coutsoudis 2001
- Coutsoudis A, Pillay K, Kuhn L, Spooner E, Tsai WY, Coovadia HM. Method of feeding and transmission of HIV from mothers to children by 15 months of age prospective cohort study from Durban, South Africa. South African Vitamin A Study Group. AIDS 2001;15 379 –387. [DOI] [PubMed] [Google Scholar]
de Vincenzi 2008
- de Vincenzi I and the Kesho Bora Study Group. HIV‐free survival at 12 months among children born to HIV‐infected women receiving antiretrovirals from 34‐36 weeks of pregnancy [abstract # 638]. Paper presented at the15th Conference on Retroviruses and Opportunistic Infections (CROI), 2008.
Desmond 2008
- Desmond C, Bland RM, Boyce G, Coovadia HM, Coutsoudis A, Rollins N, et al. Scaling‐up exclusive breastfeeding support programmes: the example of KwaZulu‐Natal. PLoS ONE 2008;3(6):e2454. [PUBMED: 18560596] [DOI] [PMC free article] [PubMed] [Google Scholar]
Donovan 1994
- Donovan SM, Odle J. Growth factors in milk as mediators of infant development. Annu Rev Nutr 1994;14 147 –167. [DOI] [PubMed] [Google Scholar]
Ekpini 1997
- Ekpini ER, Wiktor SZ, Satten GA, et al. Late postnatal mother‐to‐child transmission of HIV in Abidjan, Côte d’Ivoire. Lancet 1997;349 1054 –1059. [DOI] [PubMed] [Google Scholar]
Embree 2000
- Embree JE, Njenga S, Datta P, et al. Risk factors for postnatal mother‐child transmission of HIV. AIDS 2000;14:2535 –2541. [DOI] [PubMed] [Google Scholar]
Fawzi 1998
- Fawzi WW, Msamanga GI, Spiegelman D, Urassa EJ, McGrath N, Mwakagile D, et al. Randomised trial of effects of vitamin supplements on pregnancy outcomes and T cell counts in HIV‐1‐infected women in Tanzania. Lancet 1998;351(9114):1477‐82. [PUBMED: 9605804] [DOI] [PubMed] [Google Scholar]
Fawzi 1999
- Fawzi WW, Msamanga GI, Spiegelman D, Urassa EJ, Hunter DJ. Rationale and design of the Tanzania Vitamin and HIV Infection Trial. Controlled Clinical Trials 1999;20(1):75‐90. [PUBMED: 10027501] [DOI] [PubMed] [Google Scholar]
Fawzi 2000
- Fawzi WW, Msamanga G, Hunter D, Urassa E, Renjifo B, Mwakagile D, et al. Randomized trial of vitamin supplements in relation to vertical transmission of HIV‐1 in Tanzania. J Acquir Immune Defic Syndr 2000;23(3):246‐54. [PUBMED: 10839660] [DOI] [PubMed] [Google Scholar]
Giuliano 2007
- Giuliano M, Guidotti G, Andreotti M, Pirillo MF, Villani P, Liotta G, et al. Triple antiretroviral prophylaxis administered during pregnancy and after delivery significantly reduces breast milk viral load: a study within the Drug Resource Enhancement Against AIDS and Malnutrition Program. J Acquir Immune Defic Syndr 2007;44(3):286‐91. [PUBMED: 17146372] [DOI] [PubMed] [Google Scholar]
Goto 1999
- Goto K, Chew F, Torún B, Peerson JM, Brown KH. Epidemiology of altered intestinal permeability to lactulose and mannitol in Guatemalan infants. Pediatr Gastroenterol Nutr 1999 Mar;28;3:282‐90. [DOI] [PubMed] [Google Scholar]
Handbook 2008
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions. Chichester (UK): Wiley‐Blackwell, 2008. [Google Scholar]
Harmsen 1995
- Harmsen MC, Swart RJ, Bethune MP, et al. Antiviral effects of plasma and milk proteins lactoferrin shows potent activity against both human immunodeficiency virus and human cytomegalovirus replication in vitro. J Infect Dis 1995;172 380 –388. [DOI] [PubMed] [Google Scholar]
Hocini 2000
- Hocini H, Becquart P, Bouhlal H, Adle‐Biassette H, Kazatchkine MD, Belec L. Secretory leukocyte protease inhibitor inhibits infection of monocytes and lymphocytes with human immunodeficiency virus type 1 but does not interfere with transcytosis of cell‐associated virus across tight epithelial barriers. Clin Diagn Lab Immunol 2000;7:515 –518. [DOI] [PMC free article] [PubMed] [Google Scholar]
Israel‐Ballard 2005
- Israel‐Ballard K, Chantry C, Dewey K, Lonnerdal B, Sheppard H, Donovan R, et al. Viral, nutritional, and bacterial safety of flash‐heated and pretoria‐pasteurized breast milk to prevent mother‐to‐child transmission of HIV in resource‐poor countries: a pilot study. J Acquir Immune Defic Syndr 2005;40(2):175‐81. [PUBMED: 16186735] [DOI] [PubMed] [Google Scholar]
Israel‐Ballard 2007
- Israel‐Ballard K, Donovan R, Chantry C, Coutsoudis A, Sheppard H, Sibeko L, et al. Flash‐heat inactivation of HIV‐1 in human milk: a potential method to reduce postnatal transmission in developing countries. J Acquir Immune Defic Syndr 2007;45(3):318‐23. [PUBMED: 17514015] [DOI] [PubMed] [Google Scholar]
Israel‐Ballard 2008
- Israel‐Ballard KA, Abrams BF, Coutsoudis A, Sibeko LN, Cheryk LA, Chantry CJ. Vitamin content of breast milk from HIV‐1‐infected mothers before and after flash‐heat treatment. J Acquir Immune Defic Syndr 2008;48(4):444‐9. [PUBMED: 18614920] [DOI] [PMC free article] [PubMed] [Google Scholar]
John 2001
Kafulafula 2007
- Kafulafula G, Thigpen M, Hoover D, et al. Post‐weaning gastroenteritis and mortality in HIV‐uninfected African infants receiving antiretroviral prophylaxis to prevent MTCT of HIV‐1 [abstract # 773]. Paper presented at the 14th Conference on Retroviruses and Opportunistic Infections (CROI), 2007.
Kourtis 2007
- Kourtis A, et al. Diarrhea in Uninfected Infants of HIV‐infected Mothers Who Stop Breastfeeding at 6 Months: The BAN Study Experience [abstract #772]. Paper presented at presented at the 14th Conference on Retroviruses and Opportunistic Infections (CROI), 2007.
Kramer 2001
Kumwenda 2008 Supplement
Lindegren 1999
Mbori‐Ngacha 2001
- Mbori‐Ngacha D, Nduati R, John G, Reilly M, Richardson B, Mwatha A, et al. Morbidity and mortality in breastfed and formula‐fed infants of HIV‐1‐infected women: A randomized clinical trial. JAMA 2001;286(19):2413‐20. [PUBMED: 11712936] [DOI] [PMC free article] [PubMed] [Google Scholar]
Miotti 1999
MMWR 1985
- Centers for Disease Control and Prevention. Recommendations for assisting in the prevention of perinatal transmission of human T‐lymphotropic virus type IIIlymphadenopathy‐associated virus and acquired immunodeficiency syndrome. MMWR Morb Mortal Wkly Rep. 1985; Vol. 34 721 –726, 731–732. [PubMed]
Newell 2004
- Newell ML, Coovadia H, Cortina‐Borja M, Rollins N, Gaillard P, Dabis F, Ghent International AIDS Society (IAS) Working Group on HIV Infection in Women and Children. Mortality of infected and uninfected infants born to HIV‐infected mothers in Africa: a pooled analysis. Lancet. 2004 Oct 2‐8; Vol. 364, issue 9441:1236‐43. [DOI] [PubMed]
Onyango 2007
- Onyango C, et al. Early Breastfeeding Cessation among HIV‐exposed Negative Infants and Risk of Serious Gastroenteritis: Findings from a Perinatal Prevention Trial in Kampala, Uganda [abstract # 775]. Paper presented at the 14th Conference on Retroviruses and Opportunistic Infections (CROI) 2007.
Pebley 1986
- Pebley AR, Millman S. Birthspacing and child survival. Int Fam Plann Perspect. 1986; Vol. 12 71 –79.
Pillay 2000
Rankin 2005
- Rankin W, Brennan S, Schell E, et al. The Stigma of Being HIV‐Positive in Africa. PLoS Medicine August 2005;2(8):247‐249. [DOI] [PMC free article] [PubMed] [Google Scholar]
Read 1999
- Read JS. Preventing mother‐to‐child transmission of HIV the USA experience. Prenat Neonatal Med. 1999; Vol. 4 391 –397.
Read 2003
- Read JS. American Academy of Pediatrics Committee on Pediatric AIDS. Human milk, breastfeeding, and transmission of human immunodeficiency virus type 1 in the United States. Pediatrics 2003; 112;1196‐1205. [DOI] [PubMed] [Google Scholar]
Read 2005a
- Read JS. Prevention of mother‐to‐child transmission of HIV. In: Zeichner SL, Read JS editor(s). Textbook of Pediatric HIV Care. Cambridge, England: Cambridge University Press, 2005. [Google Scholar]
Read 2005b
- Read JS, Newell ML. Cesarean section for preventing mother‐to‐child transmission of HIV infection. Cochrane Database of Systematic Reviews 2005;4. [DOI] [PubMed] [Google Scholar]
Richardson 2003
- Richardson BA, John‐Steward GC, Hughes JP, et al. Breast‐milk infectivity in human immunodeficiency virus type 1‐infected mothers. J Infect Dis. 2003; Vol. 187 736 –740. [DOI] [PMC free article] [PubMed]
Safrit 2004
- Safrit JT, Ruprecht R, Ferrantelli F, Xu W, Kitabwalla M, Rompay K, et al. Immunoprophylaxis to prevent mother‐to‐child transmission of HIV‐1. J Acquir Immune Defic Syndr 2004 Feb 1;35(2):169‐77. [DOI] [PubMed] [Google Scholar]
Semba 1999a
- Semba RD, Kumwenda N, Hoover DR, et al. Human immunodeficiency virus load in breast milk, mastitis, and mother‐to‐child transmission of human immunodeficiency virus type 1. J Infect Dis 1999;180:93‐98. [DOI] [PubMed] [Google Scholar]
Semba 1999b
- Semba RD, Kumwenda N, Taha TE, et al. Mastitis and immunological factors in breast milk of human immunodeficiency virus‐infected women.. J Hum Lact 1999;15 301 –306. [DOI] [PubMed] [Google Scholar]
Swart 1996
Thapa 1988
Thomas 2008
- Thomas T, et al. Rates of diarrhea associated with early weaning among infants in Kisumu, Kenya [abstract # 774]. Paper presented at the 15th Conference on Retroviruses and Opportunistic Infections (CROI) 2008.
UNAIDS 2008
- Joint United Nations Programme on HIV/AIDS. 2007 AIDS Epidemic Update. Geneva, Geneva: 2008.
Urdaneta 2005
- Urdaneta S, Wigdahl B, Neely EB, Berlin CM Jr, Schengrund CL, Lin HM, Howett MK. Inactivation of HIV‐1 in breast milk by treatment with the alkyl sulfate microbicide sodium dodecyl sulfate (SDS). Retrovirology 2005 Apr 29;2(28). [DOI] [PMC free article] [PubMed] [Google Scholar]
Van de Perre 1992
- Perre P, Hitimana DG, Simonon A, et al. Postnatal transmission of HIV associated with breast abscess. Lancet 1992;339:1490 –1491. [DOI] [PubMed] [Google Scholar]
Van de Perre 1993
- Perre P, Simonon A, Hitimana DG, et al. Infective and anti‐infective properties of breastmilk from HIV‐infected women.. Lancet 1993;341 914 –918. [DOI] [PubMed] [Google Scholar]
Van der Horst 2003
- Horst C, Fiscus S, Piwoz E, Corneli A, Moses A, Jones D, et al. Prevention of mother to infant transmission of HIV through breastfeeding and reduction of morbidity and mortality of the breastfeeding mothers: a study in Malawi. Antiviral Therapy 2003;8 (Suppl 1):S4777. [Google Scholar]
VanDerslice 1994
- VanDerslice J, Popkin B, Briscoe J. Drinking‐water quality, sanitation, and breast‐feeding: their interactive effects on infant health.. Bull World Health Organ 1994;72:589–601. [PMC free article] [PubMed] [Google Scholar]
Volmink 2007
- Volmink J, Siegfried NL, Merwe L, Brocklehurst P. Antiretrovirals for reducing the risk of mother‐to‐child transmission of HIV infection. Cochrane Database Syst Rev 2007;1. [DOI] [PubMed] [Google Scholar]
WHO 2006
- WHO HIV, Infant Feeding Technical Consultation. held on behalf of the Inter‐agency Task Team (IATT) on Prevention of HIV Infections in Pregnant Women, Mothers, their Infants. Geneva, October 25‐27, 2006.
WHO Team 2000
- WHO Collaborative Study Team on the Role of Breastfeeding on the Prevention of Infant Mortality. Effect of breastfeeding on infant and child mortality due to infectious diseases in less developed countries: a pooled analysis. Lancet 2000;355:451‐455. [PubMed] [Google Scholar]
Yoon 1996
- Yoon PW, Black RE, Moulton LH, Becker S. Effect of not breastfeeding on the risk of diarrheal and respiratory mortality in children under 2 years of age in Metro Cebu, The Philippines.. Am J Epidemiol 1996;143 1142 –1148. [DOI] [PubMed] [Google Scholar]
Ziegler 1985
- Ziegler JB, Cooper DA, Johnson RO, Gold J. Postnatal transmission of AIDS‐associated retrovirus from mother to infant. Lancet 1985;1 896 –898. [DOI] [PubMed] [Google Scholar]