

Abstract
Background:
The rise of direct-to-consumer (DTC) orthodontics has caused significant controversy amongst dentists and orthodontists. However, little is known about the actual harm (or benefits) experienced by users of at-home teeth aligners.
Methods:
We designed a 24-item online survey to assess individuals’ experience with at-home aligners. We recruited participants for six months (March-August 2019) on social media platforms (Instagram & Twitter) and online forums related to DTC orthodontics. A total of 470 responses were analyzed.
Results:
The typical respondent was a white, female millennial who purchased aligners to correct crowding. More than half of respondents consulted with a dentist prior to purchasing aligners. In those interactions, the dentist most often recommended an in-office treatment. Though the majority (87.5%) of respondents were satisfied with treatment, 6.6% had to visit their dentist due to the severity of side effects.
Conclusion:
Though many respondents would have preferred traditional treatment from a dentist or orthodontist, they opted for DTC aligners because of cost and convenience.
Practical Implications:
Rather than warning patients wholesale against at-home aligners, it may be more productive for dentists to have frank discussions with them of risks and benefits. In parallel to pushing for increased accountability for DTC orthodontics companies, it may be prudent to consider new ways of co-existing in this altered landscape, such as offering professional oversight of DTC treatments.
Keywords: Dental Devices, Home Care, Dental Industry, Health Policy, Malocclusion, Oral Health, Orthodontic Appliances, Patient Education, Professional Role, Public Policy, Teledentistry
Introduction
Recent years have seen the rise of do-it-yourself (DIY) dentistry and orthodontics, wherein individuals perform aspects of dentistry on themselves outside the supervision of a trained professional.1,2 Though DIY dentistry includes straightening teeth with rubber bands and fishing clips,3 the practice that has generated the most controversy has been the sale of clear plastic aligners directly to public.2,4–11 As of January 2020, there are at least six companies in the United States offering at-home aligners, which are marketed for cosmetic improvement of one’s smile. Some of these companies have storefronts where a technician takes an image of a user’s teeth; in others, the user takes their own impression using a mold kit. Over the course of several months, the user receives new sets of aligners through the mail. By cutting out in-person dental supervision and monitoring, companies offer treatment for thousands of dollars less than a similar in-office procedure.12 Although the American Dental Association (ADA) and the American Association of Orthodontists (AAO) have referred to this phenomenon as DIY dentistry,3,13 here we refer to it as “direct-to-consumer” (DTC) orthodontics.
DTC models of orthodontics have been sharply condemned by dentists and orthodontists. In 2017 the ADA passed a resolution against DIY teeth straightening, and later ran a full-page advertisement in the Wall Street Journal, warning against unsupervised dental treatment.14 The AAO has publicly cautioned against the practice via a consumer alert15 and has filed legal complaints with 36 state dental boards against SmileDirectClub,16 the DTC orthodontics company that has the largest share of the market.17 These public repudiations, however, have not slowed the rise of DTC orthodontics: last year SmileDirectClub had an initial public offering,18 and signed deals with CVS and Walgreens that will allow them to open over a thousand shops in those locations.19 The ongoing turf war—over who has the authority to move teeth and how it should be done—is evident in a clash over language, of what is DIY and what is teledentistry, of who are customers and who are patients, of what is medicine and what is cosmetics.
Proponents of DTC orthodontics argue that the low cost of at-home aligners ($2,000 as compared to approximately $6,000 for Invisalign) makes teeth alignment accessible to a greater number of individuals;4 that it is a form of teledentistry because there is a dentist (albeit one that the consumer never or seldomly meets) who approves the treatment;20 and that objections to their practices can be expected because companies are market “disrupters” like Uber and Airbnb.21 On the other hand, dentists and orthodontists have argued that moving teeth is a medical service that should only be carried out by licensed healthcare professionals who have undergone the requisite training. Underpinning arguments put forth by dentists is that there is a risk to unsupervised teeth alignment. Indeed, the ADA discourages DIY orthodontics because of the “potential for harm to patients,”22 while the AAO’s consumer alert emphasizes that moving teeth can “lead to potentially irreversible and expensive damage such as tooth and gum loss, changed bites, and other issues.”23
To date, however, the notion of damage to health from at-home aligners has not been systematically studied. Aside from occasional media reports,21,24–26 little is known about the actual harm (or benefits) experienced by users of DTC aligners. More broadly, there has been a lack of research on those who use at-home aligners: who they are, why they seek at-home aligners, if they consult with dentists prior to purchasing aligners, and if they are satisfied with treatment. Such information could not only shed light on the social phenomenon of DTC orthodontics, but also help illuminate its potential trajectory and inform how to better engage with the public.
The present study aimed to fill that knowledge gap by conducting the first empirical study of users of at-home teeth aligners. To that end, we designed an online survey about DTC aligners and recruited participants via social media. Our aim was to better understand users’ experiences with at-home aligners, in order to bring empirical data to bear on contemporary debates regarding DTC orthodontics.
Methods
Survey Instrument.
We designed a 24-item Qualtrics online survey to assess subjects’ experiences with at-home aligners. Survey questions assessed how subjects heard about at-home aligners; their primary reason for obtaining aligners; interactions (if any) with a dentist/orthodontist prior to purchasing aligners; past experience with teeth alignment; satisfaction with aligners and side effects; communication with the company; attitudes towards aligners; and sociodemographic information. Questions were informed by a preliminary scoping review of the DTC orthodontics landscape as well as interviews with dentists and orthodontists.
Recruitment.
Subjects were recruited using two methods. The first involved posting recruitment messages to online forums related to at-home teeth aligners. In March 2019, a single message was posted to three of the five Facebook groups related to aligners whose moderators granted us permission (SnapCorrect Members, Smilelove Members, Smile Direct Club Members) and one Reddit.com forum (https://www.reddit.com/r/smiledirectclub/). The second method emerged from our observation that users of aligners often post to social media using specific hashtags, photographically documenting their treatment progression. We conducted preliminary research to identify common hashtags utilized, which resulted in a list of 25 hashtags that were either general (#smilejourney) or specific to the six main companies marketing at-home aligners in the United States at the time of the survey (SmileDirectClub, Candid Co, Smilelove, SnapCorrect, Orthly and Impressions Smile). Next, we systematically searched Instagram and Twitter for these hashtags, and included users if the text and/or image in their posts indicated that they were using aligners. We excluded users if their posts were: (a) in a language other than English; (b) made by any commercial entity; or (c) sponsored by a company or financially motivated (e.g., posts that contained discount codes or mentions of sponsorships). Once eligible users were identified, we sent them a brief recruitment message from our lab’s social media account with a unique link to the survey. From March to August 2019, we contacted a total of 2,366 users via Instagram and 451 via Twitter (see supplementary material).
Ethics approval for the study was obtained from the University of Pennsylvania Institutional Review Board, and all users had to click through an informed consent. After completing the survey, subjects could enter a raffle to win one of ten $50 Amazon e-gift cards. Responses were analyzed using SPSS Statistics V26. Descriptive statistics were used to characterize the composition and properties of the sample, and simple inferential statistics were used to explore significant differences between subgroups.
Results
Response Rate.
Between March and August 2019, 464 respondents completed the survey in its entirety. After reviewing an additional number of partial responses (n=45), we chose to include six respondents who completed all substantive questions but skipped some demographic questions. Thus, in total, 470 responses were included in the final analysis: 76 (16.2%) recruited from the Reddit forum; 158 (33.6%) from Facebook groups; 233 (49.6%) from Instagram, and 3 (0.6%) from Twitter. Messages sent via Instagram yielded a greater response rate (9.9%) than those sent via Twitter (0.7%; see supplemental information).To validate that participants had purchased at-home aligners, at the beginning of the survey, they were asked to select the company that they purchased aligners from. At the end of the survey, they were asked to select a blurred image of an aligner box that most closely resembled the one mailed to them. After reviewing responses from the 3.2% (n=15) “mismatches” (i.e., the company and box did not match) and verifying their internal consistency, we opted to keep them in our analysis.
Sociodemographics.
The typical respondent was a white, female millennial27 who was employed full-time and either married or in a relationship (Table 1). States with the largest number of respondents were California (n=47; 10.0%), Florida (n=37; 7.9%), and Texas (n=35; 7.4%). Compared to the U.S. population, a greater percentage of respondents in our sample held a bachelor’s degree or higher (52.7% as compared to 34.9%).28 In addition, relative to the income distribution of the U.S. population, there were fewer respondents in both higher (>$150,000) and lower (under $24,500) income brackets (Fig. 1).29
Table 1.
Sociodemographic characteristics of respondents (N=470).
| n | % | Value | Range | |
|---|---|---|---|---|
| Gender | ||||
| Female | 391 | 83.2% | ||
| Male | 71 | 15.1% | ||
| Non-binary/prefer not to answer | 8 | 1.7% | ||
| Age, mean (SD) | 32.6 (9.3) | 13-75 | ||
| Age, by generation* | ||||
| Generation Z (22 and under) | 40 | 8.5% | ||
| Millennial (ages 23 to 38) | 329 | 70.0% | ||
| Generation X (39 to 54) | 81 | 17.2% | ||
| Baby boomer (55 to 73) | 16 | 3.4% | ||
| Silent generation (74 to 91) | 1 | 0.2% | ||
| Race or ethnicity | ||||
| White | 363 | 77.2% | ||
| Hispanic | 52 | 11.1% | ||
| Black | 45 | 9.6% | ||
| Asian | 23 | 4.9% | ||
| Other | 25 | 5.3% | ||
| Marital status | ||||
| Married | 181 | 38.5% | ||
| Single | 137 | 29.1% | ||
| In a relationship† | 119 | 25.3% | ||
| Divorced | 22 | 4.7% | ||
| Other | 7 | 1.5% | ||
| Education | ||||
| High school or less | 46 | 9.8% | ||
| Associate’s degree | 56 | 11.9% | ||
| Some college | 115 | 24.5% | ||
| Bachelor’s degree | 159 | 33.8% | ||
| Master’s degree | 66 | 14.0% | ||
| Professional degree | 10 | 2.1% | ||
| Doctoral degree | 13 | 2.8% | ||
| Employment | ||||
| Full time | 298 | 63.4% | ||
| Part time | 41 | 8.7% | ||
| Student | 40 | 8.5% | ||
| Homemaker | 33 | 7.0% | ||
| Self-employed | 32 | 6.8% | ||
| Unemployed | 17 | 3.6% | ||
| Retired | 4 | 0.9% |
Generation categories defined according to Pew Research Center (2019).27
This category encompasses non-married individuals who identify as being in a relationship.
Figure 1.
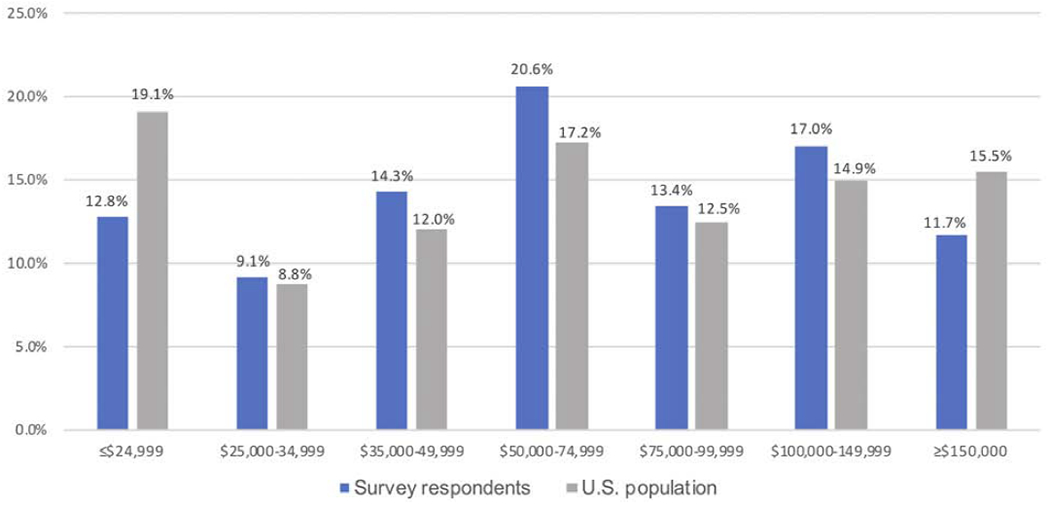
Annual household income of U.S. consumers of at-home teeth aligners compared to the U.S. population.29 N=465 because of five missing responses.
Purchasing aligners.
Most respondents initially heard about at-home aligners through an advertisement (Table 2), and the vast majority had purchased aligners from SmileDirectClub. The main reason for obtaining aligners was to correct crowding or crooked teeth (Table 2). Most respondents were in the midst of treatment at the time they completed the survey (Table 2) because our sampling method recruited users who were posting online about aligners or visiting forums related to them. The majority of respondents rated oral health as somewhat or very important in their decision to purchase aligners (Fig. 2).
Table 2.
Respondents’ (N=470) initial interactions with at-home aligners.
| n | % | |
|---|---|---|
| How respondents first heard about at-home aligners* | ||
| Advertisement | 374 | 79.6% |
| Word of mouth | 53 | 11.3% |
| Social media | 20 | 4.3% |
| Can’t remember | 16 | 3.4% |
| Other | 25 | 5.3% |
| Company from which respondents received at-home aligners | ||
| SmileDirectClub | 407 | 86.6% |
| CandidCo | 20 | 4.3% |
| Smilelove | 18 | 3.8% |
| SnapCorrect | 18 | 3.8% |
| Other | 7 | 1.5% |
| Intended user of at-home aligners | ||
| Self | 462 | 98.3% |
| Child (12-18 years old) | 7 | 1.5% |
| Child: (over 18 years old) | 1 | 0.2% |
| Reasons for obtaining at-home aligners* | ||
| To correct crowded/crooked teeth | 387 | 82.3% |
| To correct gaps between teeth | 121 | 25.7% |
| To correct a bite issue (e.g., overbite, underbite, etc.) | 67 | 14.3% |
| Other | 2 | 0.4% |
| Treatment status at time of survey completion | ||
| Halfway complete or less | 199 | 42.3% |
| More than halfway complete | 154 | 32.8% |
| Finished treatment | 104 | 22.1% |
| Has not started yet | 13 | 2.8% |
Respondents could select more than one option
Figure 2.
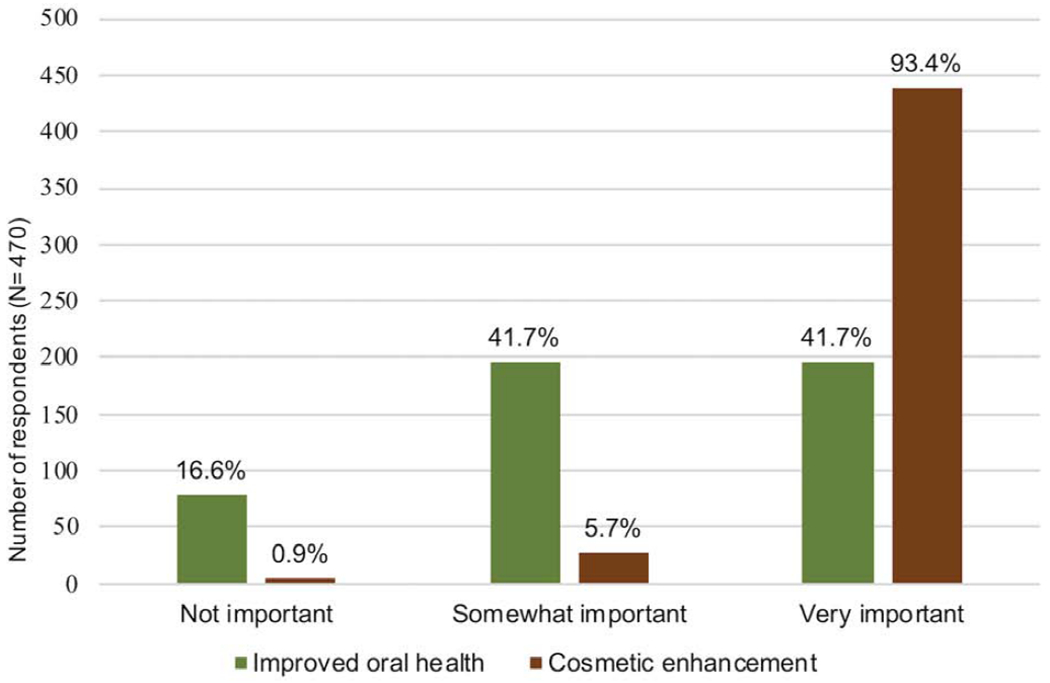
Importance of oral health and cosmetic enhancement in the decision to purchase at-home aligners (N=470).
Interaction with dentists.
Slightly more than half of all respondents consulted with a dentist about teeth alignment before purchasing at-home aligners (Table 3). In those interactions, the dentist most often recommended in-office supervised aligner treatment (Table 3). Further analysis revealed 185 unique respondents for whom the dentist recommended in-office treatment (i.e., aligners or braces), which is 73.1% of all those who consulted with a dentist prior to treatment and 39.4% of our total sample. Nearly all respondents chose an at-home option instead of in-office treatment because of cost, although two-thirds cited convenience as an additional reason (Table 3). The majority of respondents had not received orthodontic treatment in the past (n=324, 68.8%). Of the n=138 who did have past treatment, nearly all (n=130, 94.2%) purchased aligners because they did not wear their retainer post-treatment.
Table 3.
Respondents’ (N=470) considerations prior to beginning at-home aligner treatment.
| n | % | ||||
|---|---|---|---|---|---|
| Spoke to dentist prior to purchasing at-home aligners | |||||
| Yes | 253 | 53.8% | |||
| No | 217 | 46.2% | |||
| If yes, what guidance did the dentist provide?* | n=253 | % | |||
| Recommended in-office supervised aligner treatment (i.e. Invisalign) | 121 | 47.8% | |||
| Recommended braces or another in-office treatment | 98 | 38.7% | |||
| Did not recommend immediate treatment | 29 | 11.5% | |||
| Recommended at-home teeth aligners | 28 | 11.1% | |||
| Advised against at-home teeth aligners | 20 | 7.9% | |||
| Other | 31 | 12.3% | |||
| Had dental insurance when at-home aligner kit was purchased | |||||
| Yes | 310 | 66.0% | |||
| No | 156 | 33.2% | |||
| Not sure | 4 | 0.9% | |||
| If yes, did you think insurance would cover any portion of the cost? | n=310 | % | |||
| Yes | 98 | 31.6% | |||
| No | 164 | 52.3% | |||
| Did not respond to question | 48 | 15.5% | |||
| If yes:† | n=49 | Mean (SD) | |||
| What percentage of the cost did you think insurance would cover? | 48.7% (23.3) | ||||
| What percentage has insurance actually covered? | 23.1% (29.1) | ||||
| Reasons for choosing at-home aligners instead of treatment via a dental provider* | |||||
| Cost | 435 | 92.6% | |||
| Convenience | 307 | 65.3% | |||
| Do not have a dentist/orthodontist | 44 | 9.4% | |||
| Dentist/orthodontist does not provide aligners | 17 | 3.6% | |||
| Other | 19 | 4.0% | |||
Respondents could select more than one option
Responses only shown for the n=49 who reported finishing treatment and for those who reported being more than halfway through treatment.
Experience with aligners.
The vast majority of respondents were very happy or somewhat happy with the results of aligners (Figure 3). Those using aligners for bite issues were more likely to be dissatisfied as compared to those using aligners to correct crowding or gaps [X2 (1, N=457) = 6.40 p < 0.05; Cramer’s V = 0.123]. Satisfaction level did not vary significantly based on how far along respondents were in the treatment process [X2 (1, N=457) = 3.94, p = 0.067]. Table 4 depicts the range of side effects experienced by users. While pain and discomfort can be expected for aligner treatment,30,31 6.6% had side effects serious enough that necessitated a visit to their family dentist. Most respondents did not attempt to contact a company dentist during the course of their treatment. Of those who did, the majority received an online message (Table 4). As shown in Figure 4, although most respondents would recommend at-home aligners to others, a large number (44.5%) would have preferred receiving treatment from a dentist or orthodontist.
Figure 3.
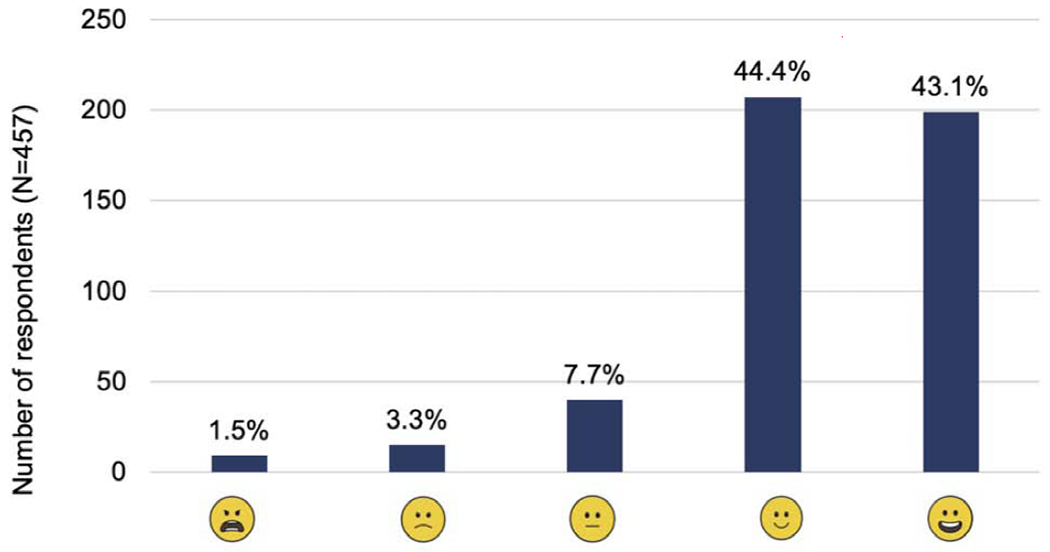
Respondents’ (N=457) happiness level with at-home aligners. Respondents could choose from one of the five emojis depicted above. Only responses of those who have commenced or completed treatment are depicted.
Table 4.
Respondents’ (N=457) experiences with at-home aligners.*
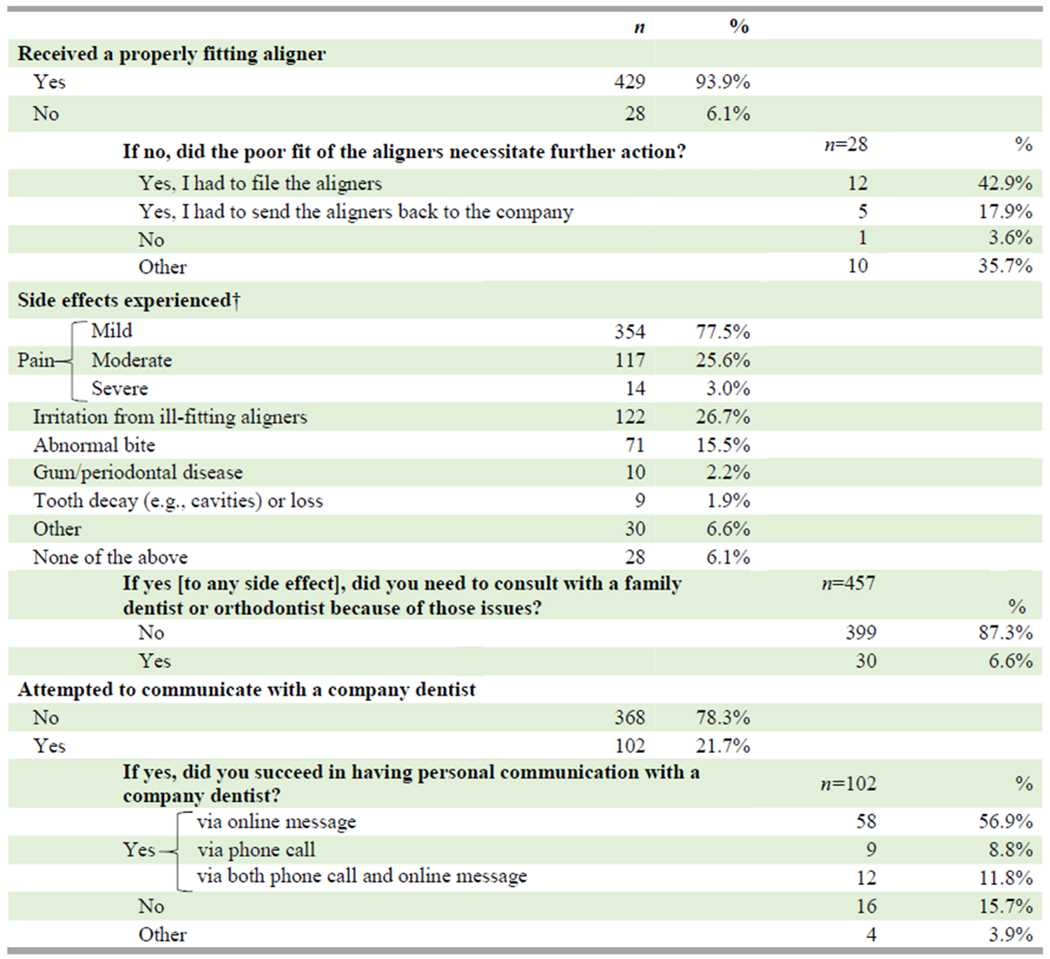 |
N=457 reflects the number of respondents in our sample who had commenced or completed treatment
Respondents could select more than one option.
Figure 4.
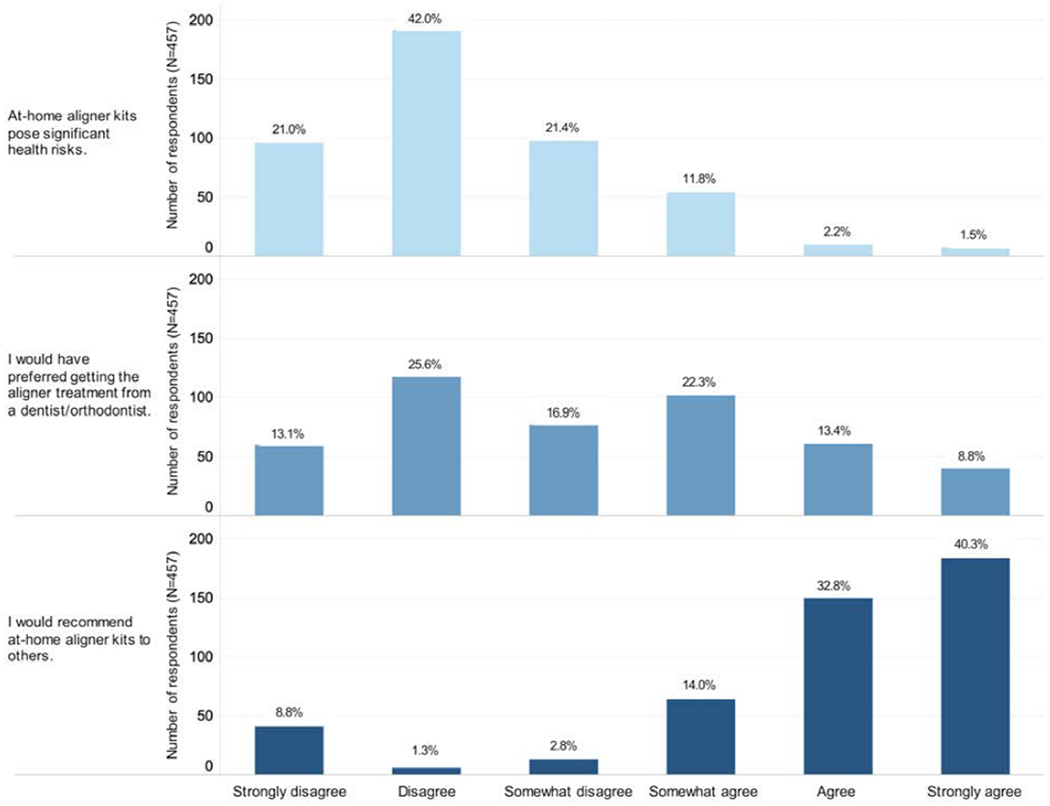
Attitudes of respondents towards risk, treatment modality preference, and likeliness to recommend at-home aligners to others. Only responses of those who have commenced or completed treatment are depicted (N=457).
Open-ended comments:
89 respondents opted to include an additional comment at the end of the survey. Common themes were recognition of the “trade-offs” involved in DTC orthodontics (i.e., that it wouldn’t be perfect, but it would be “adequate”) and the need to employ common sense by seeing a dentist beforehand and not choosing DTC orthodontics to fix serious bite issues. Some emphasized the convenience of DTC aligners (“…as a working mother of two small children, I don’t have time for constant orthodontic appointments”). A number of respondents would not have gotten aligners otherwise due to cost; one emphasized the flexibility of the payment plan ($80/month). Many respondents were frustrated with the customer service provided by companies. Notably, two mentioned significant harm from aligners; one had “lots of damage to fix” costing “$11,500 and counting” and another needed an orthodontist to “fix the bite issues and pain that the at home aligners caused.”
Discussion
During the course of our study, a user we attempted to recruit via Instagram noted that she had signed a non-disclosure agreement (NDA) with a DTC orthodontics company and could not complete our survey. Indeed, various reports have indicated that SmileDirectClub sometimes requires customers to sign an NDA prior to processing a refund, and instructs them to remove negative reviews from social media.25,26,32,33 Although we cannot know how many individuals declined to participate because of NDAs, based on our yearlong, informal observations of online forums related to aligners—where users relate both positive and negative experiences, and discuss the use of NDAs—we estimate that it is likely a small percentage. Still, we note this limitation prominently here as it is important to interpret our results—and in particular, ratings of satisfaction levels—with this caveat.
This study provides the first empirical glimpse of those who use at-home aligners. Most respondents were white, female millennials. Though the prevalence of this demographic may have been due to our social media recruitment method, a report of an unpublished CVS survey noted many millennial users, indicating that this may indeed be the prevalent age demographic.34 With regard to income, there were fewer respondents in the lowest (≤$25,000) and highest (≥$150,000) household income brackets relative to the U.S. population. These findings suggest that the lowest earners may not be able to afford to spend several thousand dollars on a cosmetic procedure, and that the highest earners may be more likely to turn to supervised orthodontic treatment. While cost was the main reason for choosing at-home aligners, convenience was cited by two-thirds of respondents. This finding is not surprising when considered in conjunction with the prevalence of millennials in our study, who have come of age in an era where the Internet provides instantaneous shopping, entertainment, and transportation.
Rather than circumventing the dentist entirely, our results paint a more complex portrait: many sought consultations from a dentist/orthodontist prior to purchasing at-home aligners, but opted for the DTC option after the dentist/orthodontist recommended an in-office treatment. That this scenario occurred for 39.4% (n=185) of all survey respondents should be concerning for dentists, orthodontists, and the public, as it indicates a loss of supervision of dental treatment, particularly amongst younger patients. However, there is also an opportunity: 44.5% of respondents would have preferred traditional treatment from a dentist or orthodontist. Given that cost and convenience were the main reasons for turning to DTC aligners, dentists who provide more affordable aligner treatment with flexible payment plans and a reduced number of in-office visits may be better suited to compete with DTC aligner companies.
Our results highlight the blurred lines between enhancement and treatment in the orthodontic context: while nearly all respondents cited cosmetic enhancement as very important in their decision to purchase aligners reason, a significant portion (41.7%) agreed that improved oral health was also very important in their decision. These results mirror debates in the scholarly literature regarding the extent to which bite correction is cosmetic as opposed to medically necessary.35–37 The muddled boundaries are exemplified by a comment from one user, who stopped DTC aligner treatment because she “was viewed more as a customer than a patient.”
Overall, the results of this study indicate that while the majority of users appear to be satisfied with DTC orthodontics, a small portion have experienced more serious side effects. In particular, those who utilize aligners for bite issues are less satisfied, raising questions about whether those with more significant malocclusions are being adequately excluded from treatment. This is particularly concerning, given that dentists from most DTC orthodontics companies do not review radiographs or other dental records prior to approving treatment. Accountability for DTC orthodontic companies and the dentists who work for them remains a cardinal concern, especially given that many companies do not provide users with a direct line of communication to a dentist. Though the majority of respondents in our sample received an online message when they attempted to contact a company dentist, reports have raised doubts about whether such messages are indeed coming from a dentist.25 In recognition of these concerns, a new California law will require teledentists to review treatment records and provide their full names and license numbers; it will also allow consumers to submit complaints directly to the state dental board irrespective of having signed an NDA.38,39 The impact of this law on the DTC orthodontics market should be watched with great interest.
This study has a number of limitations. First, as mentioned above, users may have declined to participate due to having signed an NDA; thus, satisfaction levels may have skewed positive, and those with negative experiences may have been underrepresented. Second, given that we recruited via online avenues, our sample may not be representative of the population of all users of DTC aligners, but rather only those who have engaged in social media related to aligners. However, given that a report of a CVS survey of users of DTC aligners found a large number of millennial users, and given that the vast majority (86%) of this age demographic utilizes social media,40 it is reasonable to speculate that many users may be engaged with social media related to DTC aligners. Third, it is unclear to what extent there was a nonresponse bias (i.e., how those who completed the survey may have differed from those who did not).
Fourth, many respondents were in the midst of treatment; though we found a slight difference in satisfaction level based on how far along they were in treatment, our sample sizes were small for dissatisfied respondents. It is possible that a larger sample of those who had completed treatment would have yielded different results. Fifth, we had no way of confirming whether consumers purchased aligners. However, by including a unique validation question and monitoring survey links, we took steps to ensure the validity of our data. Finally, survey responses are inherently self-report measures, and users of DTC aligners have limited knowledge of tooth alignment and occlusion. It is possible that users may have been satisfied with treatment without recognizing that their periodontal health may have been compromised, or that tooth alignment and result occlusion may be particularly unstable.
Looking ahead, it is likely that some form of DTC orthodontics is here to stay. This is underscored both by the high satisfaction levels reported in this survey, as well as the increasing partnerships of companies like SmileDirectClub with retailers34 and insurance companies.41 Importantly, the challenges posed by at-home aligners are not unique: fields such as genetics, psychiatry, neurology, and cardiology are all experiencing similar disruptions due to the advent of DTC health products.42 Some scholars have argued that in today’s world of expanded patient access to DTC tests and interventions, physicians will need to “reconceptualize their role,” occasionally acting as consultants or advisors, instead of the sole gatekeepers of treatment.43 Thus, in parallel to pushing for increased accountability for DTC orthodontics companies, it may be prudent to consider new ways of co-existing in this altered landscape, such as offering professional oversight of DTC treatments. Doing so might help achieve the ultimate goal: improving the oral health of millions of Americans.
Supplementary Material
Acknowledgements:
This study was supported by the Office of the Director, National Institutes of Health (NIH), grant number DP5OD026420.
Thanks to Dr. Chaim Wexler, DDS, for comments on the survey design and manuscript draft. Thanks to Qian (Erin) Huang, MPH, for assistance with analysis.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Disclosure. None of the authors reported any disclosures.
References
- 1.Kravitz ND, Burris B, Butler D, Dabney WC. Teledentistry, Do-It-Yourself Orthodontics, and Remote Treatment Monitoring. JCO. 2016;L(12):718–726. [PubMed] [Google Scholar]
- 2.Schneider SA. The Role and Implications of “Do It Yourself” Tooth Movement. Dent Hypotheses. 2016;7(4):157–159. doi: 10.4103/2155-8213.195977 [DOI] [Google Scholar]
- 3.American Association of Orthodontists. Orthodontists Report Uptick in Number of Patients Attempting DIY Teeth Straightening. 2017. “https://www.aaoinfo.org/1/press-room/orthodontists-report-uptick-in-number-of-patients-attempting-diy-teeth-straightening” Accessed Dec. 27, 2019.
- 4.Ackerman M, Burris B. The way it was, the way it ought to be, the way it is, and the way it will be. Am J Orthod Dentofac. 2018;153(2):165–166. doi: 10.1016/j.ajodo.2017.09.010 [DOI] [PubMed] [Google Scholar]
- 5.Behrents RG. Do-it-yourself impressions and clear retainers: A fairy tale. Am J Orthod Dentofac. 2016;150(2):205–207. doi: 10.1016/j.ajodo.2016.06.010 [DOI] [PubMed] [Google Scholar]
- 6.Frazier MC. The sky is not the limit! Am J Orthod Dentofac. 2018;154(1):6–8. doi: 10.1016/j.ajodo.2018.04.016 [DOI] [PubMed] [Google Scholar]
- 7.Hughes J The way it really is. Am J Orthod Dentofac. 2018; 154(1):5–6. doi: 10.1016/j.ajodo.2018.04.002 [DOI] [PubMed] [Google Scholar]
- 8.Rigsbee OH. Thoughts about “The way it was ….” Am J Orthod Dentofac. 2018;154(1):4–5. doi: 10.1016/j.ajodo.2018.04.001 [DOI] [PubMed] [Google Scholar]
- 9.Spencer GW. What we have to offer. Am J Orthod Dentofac. 2018;154(1):8–9. doi: 10.1016/j.ajodo.2018.05.005 [DOI] [PubMed] [Google Scholar]
- 10.Greco PM. When the patient is his own doctor …. Am J Orthod Dentofac. 2018;154(6):757. doi: 10.1016/j.ajodo.2018.10.003 [DOI] [PubMed] [Google Scholar]
- 11.Sandler J Patients… or “profit centres”? JWFO. 2018;7(1):2–5. [Google Scholar]
- 12.Dickey M Tech startups want to go inside your mouth. 2018. “https://techcrunch.com/2018/01/27/tech-startups-want-to-go-inside-vour-mouth/” Accessed Aug. 8, 2018.
- 13.Burger D ADA discourages DIY orthodontics through resolution. 2017. “https://www.ada.org/en/publications/ada-news/2017-archive/november/ada-discourages-diy-orthodontics-through-resolution” Accessed Aug. 22, 2018.
- 14.Solana K ADA launches public awareness campaign discouraging DIY dentistry. 2018. “https://www.ada.org/en/publications/ada-news/2018-archive/august/ada-launches-public-awareness-campaign-discouraging-diy-dentistry” Accessed Aug. 9, 2018.
- 15.American Association of Orthodontists. Consumer Alert from the AAO: Questions to Consider When Researching Direct-To-Consumer Orthodontic Companies. n.d. “https://www.aaoinfo.org/1/online-orthodontic-companies” Accessed Sep. 10, 2019.
- 16.American Association of Orthodontists. American Association of Orthodontists Discusses Patient Health And Safety Information Regarding Direct-To-Consumer Orthodontics. 2019. “https://www.prnewswire.com/news-releases/american-association-of-orthodontists-discusses-patient-health-and-safety-information-regarding-direct-to-consumer-orthodontics-300878975.html” Accessed Dec. 27, 2019.
- 17.Reinicke C Wall Street is overwhelmingly bullish on SmileDirectClub even after it had the worst US IPO in 12 years. Here’s what analysts are saying. 2019. “https://markets.businessinsider.com/news/stocks/smiledirectclub-stock-ratings-analysts-targets-from-maior-wall-street-firms-2019-10-1028581163#1-jpmorgan-we-see-a-clear-path-to-sustained-top-line-growth-1 ” Accessed Jan. 4, 2020.
- 18.Trainer D What Investors Need to Know About SmileDirectClub’s (SDC) IPO. 2019. https://www.forbes.com/sites/greatspeculations/2019/09/11/what-investors-need-to-know-about-smiledirectclubs-sdc-ipo/#7c63bd6b55b1” Accessed Sep. 12, 2019.
- 19.Toy S SmileDirectClub went public: 5 things to know about the teeth-straightening startup. 2020. “https://www.marketwatch.com/storv/smiledirectclub-is-going-public-5-things-to-know-about-the-teeth-straightening-startup-2019-08-21” Accessed Dec. 12, 2019.
- 20.SmileDirectClub. How It Works. “https://smiledirectclub.com/how_it_works/” Accessed Dec. 31, 2019.
- 21.Subbaraman N This Companv Is Trving To Disrupt The Braces Industrv And Dentists Are Fighting Back. 2017. “https://www.buzzfeednews.com/article/nidhisubbaraman/braces-wars-dentists-are-warning-that-mail-order” Accessed Nov. 10, 2018.
- 22.American Dental Association. ADA discourages DIY orthodontics through resolution. 2017. “https://www.ada.org/en/publications/ada-news/2017-archive/november/ada-discourages-diy-orthodontics-through-resolution” Accessed Aug. 22, 2018.
- 23.Behrents RG. Consumer alert on the use of elastics as “gap bands.” Am J Orthod Dentofac. 2014;146(3):271–272. doi: 10.1016/j.ajodo.2014.07.003 [DOI] [PubMed] [Google Scholar]
- 24.Sleiman J Inside the battle between Smile Direct Club and ‘organized dentistry.’ 2019. “https://whyy.org/segments/inside-the-battle-between-smile-direct-and-organized-dentistry/” Accessed Jan. 4, 2020.
- 25.Research H SmileDirectClub: Moving Fast and Breaking Things in People’s Mouths – 85% Downside. 2019. “https://hindenburgresearch.com/smiledirectclub-moving-fast-and-breaking-things-in-peoples-mouths/” Accessed Jan. 2, 2020.
- 26.Damiano M Mail order teeth aligners are controversial. Now they have an unlikely promoter at Boston Children’s. 2019. “https://www.bostonglobe.com/metro/2019/12/21/they-cheap-and-convenient-but-mail-order-teeth-aligners-are-also-controversial-now-they-have-unlikely-promoter-children-hospital/HsMWMhsLQibOzoAz0Cx5lO/story.html” Accessed Jan. 4, 2020.
- 27.Dimock M Defining generations: Where Millennials end and Generation Z begins. 2019. “https://www.pewresearch.org/fact-tank/2019/01/17/where-millennials-end-and-generation-z-begins/” Accessed Nov. 8, 2019.
- 28.Census Bureau US. Educational Attainment in the United States: 2018. 2019. “https://www.census.gov/data/tables/2018/demo/education-attainment/cps-detailed-tables.html” Accessed Dec. 20, 2019.
- 29.Census Bureau U HINC-01. Selected Characteristics of Households by Total Money Income. “https://www.census.gov/data/tables/time-series/demo/income-poverty/cps-hinc/hinc-01.html” Accessed Dec. 20, 2019.
- 30.Fujiyama K, Honjo T, Suzuki M, Matsuoka S, Deguchi T. Analysis of pain level in cases treated with Invisalign aligner: comparison with fixed edgewise appliance therapy. Prog Orthod. 2014;15(1):64. doi: 10.1186/s40510-014-0064-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Malament K How to Deal with Invisalign® Discomfort. 2019. “https://www.bostonprosthodontics.com/blog/2019/01/25/how-to-deal-with-invisalign-196045” Accessed Jan. 6, 2020.
- 32.Linnane C SmileDirectClub stock slides 13% as California Gov. Newsom signs law to change ‘teledentistry’ rules. 2019. “https://www.marketwatch.com/story/smiledirectclub-stock-slides-10-as-california-gov-newsom-signs-law-to-change-teledentistry-rules-2019-10-14” Accessed Jan. 4, 2020.
- 33.Griffith E, Eavis P. This Company Says It Will Fix Your Smile. It May Shush You if It Doesn’t. 2020. https://www.nytimes.com/2020/01/21/technology/smiledirectclub-smile-nda.html Accessed Jan. 21, 2020.
- 34.Thomas L, LaVito A. CVS will bring hundreds of SmileDirectClub shops to its stores, offering a cheaper way to straighten teeth. 2019. “https://www.cnbc.com/2019/04/25/cvs-is-opening-up-hundreds-of-smiledirectclub-shops-in-its-stores.html” Accessed Dec. 30, 2019.
- 35.Ackerman M Selling orthodontic need: innocent business decision or guilty pleasure? J Med Ethics. 2010;36(5):275. doi: 10.1136/jme.2009.033761 [DOI] [PubMed] [Google Scholar]
- 36.Hunt O, Hepper P, Johnston C, Stevenson M, Burden D. Professional perceptions of the benefits of orthodontic treatment. Eur J Orthodont. 2001;23(3):315–323. doi: 10.1093/ejo/23.3.315 [DOI] [PubMed] [Google Scholar]
- 37.Burden DJ. Oral Health-Related Benefits of Orthodontic Treatment. Semin Orthod. 2007;13(2):76–80. doi: 10.1053/j.sodo.2007.03.002 [DOI] [Google Scholar]
- 38.Low E California Assembly Bill No. 1519. 2019. “https://leginfo.legislature.ca.gov/faces/billNavClient.xhtm?bill_id=201920200AB1519” Accessed Jan. 4, 2020.
- 39.Versaci M California passes law strengthening teledentistry requirements. 2019. “https://www.ada.org/en/publications/ada-news/2019-archive/october/california-passes-law-strengthening-teledentistry-requirements” Oct. 19, 2019.
- 40.Vogels EA. Millennials stand out for their technology use, but older generations also embrace digital life. 2019. https://www.pewresearch.org/fact-tank/2019/09/09/us-generations-technology-use/” Accessed Jan. 22, 2020.
- 41.SmileDirectClub. Insurance. n.d. “https://smiledirectclub.com/insurance/” Accessed Jan. 2, 2020.
- 42.Wexler A, Joffe S. 5 ways to address the challenges of direct-to-consumer health products. 2019. “https://www.statnews.com/2019/04/02/address-challenges-direct-to-consumer-health-products/” Accessed Jan. 4, 2020.
- 43.Kilbride MK, Joffe S. The New Age of Patient Autonomy. Jama. 2018;320(19):1973–2. doi: 10.1001/jama.2018.14382 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.