

Abstract
Intravitreal anti-vascular endothelial growth factor (VEGF) agents have revolutionized the treatment of retinopathy of prematurity (ROP); however, there are concerns regarding the potential systemic complications caused by those treatments. This study aimed to determine the serum concentrations of cytokines in infants with ROP and to evaluate the changes in serum VEGF concentrations after intravitreal conbercept (IVC). Sixty infants with ROP treated with IVC 0.25 mg were included. Blood samples were collected before treatment as well as 1 week and 4 weeks after treatment. Serum levels of 45 types of cytokines were measured by a multiplex bead assay. We observed that IVC 0.25 mg in ROP patients suppressed the circulating levels of VEGF-A and VEGF-D as of 1 week after injection, and these growth factor levels returned to baseline at 4 weeks. No significant differences were observed in the serum levels of the other cytokines between baseline and 1 or 4 weeks after IVC.
Subject terms: Paediatric research, Clinical trial design, Drug therapy, Adverse effects
Introduction
Retinopathy of prematurity (ROP) is a multifactorial retinal disease that remains a major treatable cause of childhood blindness worldwide1. Especially in developing countries, the prevalence of ROP is growing considerably due to the increased survival rate of low-body-weight preterm infants. Vascular endothelial growth factor (VEGF) is a key proangiogenic factor involved in the pathogenesis of ROP, promoting retinal neovascularization and prompting researchers to explore the effect of anti-VEGF agents in the management of ROP. Recently, the use of anti-VEGF drugs has revolutionized the treatment of ROP, as these agents have several distinct advantages over conventional standard laser photocoagulation therapy, including a simpler procedure and reduced risks of myopia and peripheral visual field defects2. However, given the potential for local and systemic adverse effects from these drugs, there are concerns regarding their use. A few studies have indicated that intravitreal anti-VEGF drugs induce systemic VEGF suppression for weeks to months3–5, although no significant adverse events have been reported to date. There have been occasional reports on the use of conbercept, a novel anti-VEGF agent, for ROP treatment6–8, however, the effect of conbercept on systemic VEGF concentrations in ROP has not yet been reported.
In addition to angiogenesis, an increasing number of studies have demonstrated that inflammation might play an important role in the pathogenesis of ROP. Epidemiological studies have observed elevated rates of ROP in patients with perinatal infections or inflammation, indicating that inflammation may disturb the development of retinal vessels9,10, this observation has been confirmed in animal models11. In addition, eight cytokines were detected to be significantly different in ROP patients in different time periods12. Serum levels of interleukin (IL)-7, monocyte chemotactic protein-1 (MCP-1), macrophage inflammatory protein 1 alpha (MIP-1α), and MIP-1β were significantly elevated in preterm neonates who went on to develop ROP13. In another study, plasma levels of IL-6, IL-8, and tumor necrosis factor-α (TNF-α) were increased in ROP patients14. Holm et al. reported that preterm infants with systemic inflammation in the first postnatal month had an increased risk of prethreshold ROP15. Thus, further studies are required to obtain a better understanding of the molecular mechanisms involved in ROP, guide treatment and identify predictors of ROP.
The aim of this study was to assess the changes in serum levels of VEGF and other cytokines in ROP infants who received intravitreal conbercept (IVC). To our knowledge, this is the first study to present the effect of conbercept on systemic VEGF concentration in ROP patients.
Methods
This study was a case series study approved by the Ethical Committee and Institutional Review Board of Peking University People’s Hospital (Beijing, China). Written informed consent was obtained from the guardian of each participant in accordance with the Declaration of Helsinki. All the examinations, diagnoses and treatments of participants were performed at the Ophthalmology Department of Peking University People’s Hospital. Sixty preterm infants who were diagnosed with ROP and received an intravitreal injection of 0.25 mg conbercept from November 2017 to September 2018 were enrolled in the study group, while the control group consisted of 10 infants diagnosed with congenital cataract.
In the ROP group, we communicated with the participants’ parents regarding the off-label use of IVC and the potential adverse effects of the procedure before initiating treatment. ROP was classified on the basis of the International Classification of Retinopathy of Prematurity (ICROP) as updated in 200516 and was diagnosed by experienced pediatric ophthalmologists (Y.C. and J.L.). The inclusion criteria for the ROP group included (i) a diagnosis of Zone I/II Stage 2/3 ROP with plus disease or aggressive posterior ROP (AP-ROP) with no previous treatment,(ii) the absence of major congenital anomalies,and (iii) no blood transfusion in the 2 weeks preceding blood collection.
Venous blood samples from ROP patients were collected in plastic serum separator tubes before IVC as well as 1 week and 4 weeks after IVC, while those of the control group were collected at the time of diagnosis. Samples were then centrifuged at 3,000 rpm for 10 min, and the supernatants were stored in Eppendorf tubes at − 80 °C until assayed. A 45-plex Human Cytokine/Chemokine/Growth Factor Procarta Plex Panel (cat. # EPXR450-12171-901, Invitrogen, Thermo Fisher Scientific) was used to measure the serum concentrations of cytokines via Luminex technology as described previously17, including VEGF-A, VEGF-D, placental growth factor-1 (PlGF-1), platelet-derived growth factor-BB (PDGF-BB), brain-derived neurotrophic factor (BDNF), β-nerve growth factor (β-NGF), epidermal growth factor (EGF), basic fibroblast growth factor (FGF-2), granulocytemacrophage colony stimulating factor (GM-CSF), hepatocyte growth factor (HGF), stem cell factor (SCF), stromal cell derived factor-1α (SDF1α), eotaxin, growth-regulated oncogene α (GROα), interferon gamma (IFN-γ), IFNα, TNF-α, TNF-β, IL-1RA, IL-1β, IL-1α, IL-2, IL-4, IL-5, IL-6, IL-7, IL-8, IL-9, IL-10, IL-12 p70, IL-13, IL-15, IL-17A, IL-18, IL-21, IL-22, IL-23, IL-27, IL-31, interferon-induced protein10 (IP-10), leukemia inhibitory factor (LIF), MCP-1, MIP-1α, MIP-1β, and regulated upon activation normal T cell (RANTES). All measurements were performed in triplicate.
Data are presented as the mean ± standard deviation and were analyzed using SPSS 20.0 for Mac (SPSS, IBM Corp., NY, USA). The Mann–Whitney U test was conducted to compare differences between ROP patients and controls. The Wilcoxon matched-pairs signed rank test was used to compare the cytokine changes in ROP patients before and after IVC injection. A P value less than 0.05 was considered statistically significant.
Results
Clinical data and treatment outcomes of the study population
Sixty patients (27 girls and 33 boys, 117 eyes) with Zone I/II Stage 2/3 ROP with plus disease or AP-ROP were enrolled in the study, and 10 full-term infants (four girls and six boys, 15 eyes) with congenital cataracts were included as the control group. The demographics of the patients are summarized in Table 1. The mean gestational age of infants with ROP was 29.02 ± 1.67 weeks (range 26–34.71 weeks), and their mean birth weight was 1,173.13 ± 316.50 g (range 500–2,100 g). The mean postmenstrual age at initial treatment was 39.70 ± 3.32 weeks (range 33.29–51 weeks). The mean age of the control group was 4.95 ± 2.15 months. Recurrence that required treatment occurred in 9 patients (15 eyes, 12.82%) with ROP, and the mean recurrence interval was 6.28 ± 5.41 weeks (range 2 to 20.5 weeks). The remaining eyes exhibited regression of the disease after one injection. Repeated intravitreal anti-VEGF agent injection or laser photocoagulation was performed for the eyes with recurrence. All patients with ROP were followed up for at least 6 months; the mean length of follow-up was 48.34 ± 11.46 weeks. At the end of the follow-up, no ocular or systemic adverse events were observed in this group, and all the eyes achieved favorable treatment outcomes, with no signs of recurrence or retinal detachment.
Table 1.
Demographicsof study population.
| Characteristic | ROP patients | Controls | P value | |
|---|---|---|---|---|
| No | 60 (117 eyes) | 10 (15 eyes) | ||
| Female, no. (%) | 27 (45%) | 4 (40%) | 0.77a | |
| Age | 39.70 ± 3.32 (weeks) | 4.95 ± 2.15 (months) | < 0.001b | |
| PMA at treatment (weeks) | 39.70 ± 3.32 (33.29–51) | / | ||
| GA (weeks) | 29.02 ± 1.67 (26–34.71) | / | ||
| Birth weight (g) | 1,173.13 ± 316.50 (500–2,100) | / | ||
| Zone, Stage, no. (eyes) | / | / | ||
| I 3 + | 3 | |||
| II 2 + | 13 | |||
| II 3 + | 93 | |||
| AP-ROP | 8 | |||
| Recurrence | 9 (15 eyes) | / | / | |
| Recurrence interval (weeks) | 6.28 ± 5.41 (2.0–20.5) | / | / | |
| Follow-up periods (weeks) | 48.34 ± 11.46 | / | / | |
Data are shown as mean ± SD or number (%).
ROP retinopathy of prematurity, PMA postmenstrual age, GA gestational age, AP-ROP aggressive posteriorretinopathy of prematurity.
aX2 test.
bMann–Whitney U testwas performed to compare age between two groups.
Changes in serum levels of cytokines in ROP patients before and after treatment with conbercept
The mean serum levels of VEGF-A before, 1 week after, and 4 weeks after an injection of 0.25 mg conbercept were 1976.18 ± 982.45 pg/ml (n = 60), 1,388.99 ± 753.27 pg/ml (n = 16), and 1771.53 ± 581.78 pg/ml (n = 8), respectively. The serum VEGF-A level at 1 week after IVC was significantly lower than baseline (P = 0.021). However, no significant difference was detected between baseline and 4 weeks after IVC (P = 0.25) (Fig. 1).
Figure 1.
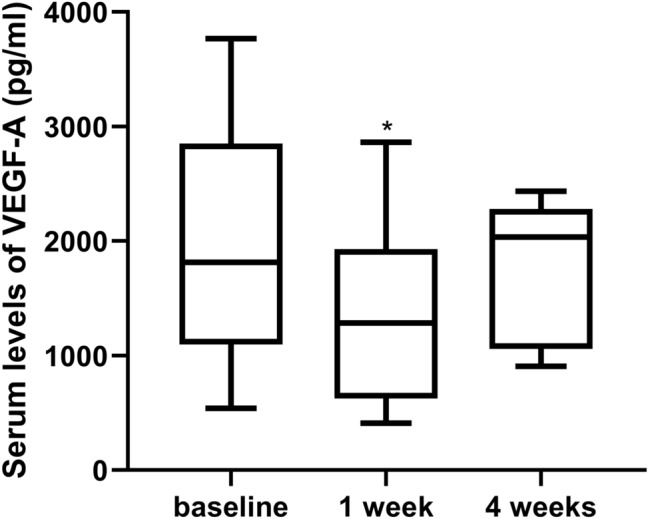
Box plot showing the serum VEGF-A levels of ROP patients before and after IVC. The serum VEGF-A levels at 1 week after IVC were significantly lower than baseline. No significant difference was observed between baseline and 4 weeks after IVC. *P < 0.05.
The mean serum levels of VEGF-D before, 1 week after, and 4 weeks after an injection of 0.25 mg conbercept were 110.23 ± 99.57 pg/ml (n = 60), 87.88 ± 90.34 pg/ml (n = 16), and 111.06 ± 79.99 pg/ml (n = 8), respectively. The serum VEGF-D level at 1 week after IVC was significantly lower than baseline (P = 0.044). However, no significant difference was detected between baseline and 4 weeks after IVC (P = 0.46) (Fig. 2).
Figure 2.
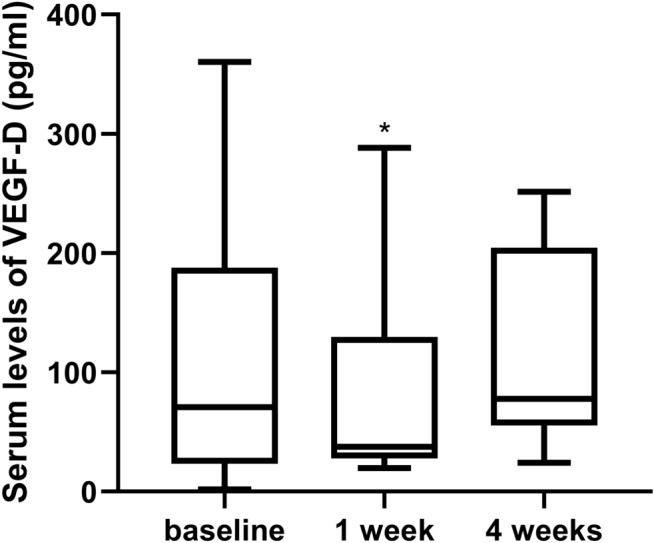
Box plot showing the serum VEGF-D levels of ROP patients before and after IVC. The serum VEGF-D levels at 1 week after IVC were significantly lower than baseline. No significant difference was observed between baseline and 4 weeks after IVC. *P < 0.05.
In this study, 21 cytokines (GM-CSF, IL-1α, IL-1β, IL-2, IL-4, IL-5, IL-7, IL-9, IL-10, IL-12 p70, IL-13, IL-15, IL-17A, IL-21, IL-22, IL-23, IL-27, IL-31, TNF-β, LIF, and IFN-α) had concentrations lower than the minimum detectable levels in more than 50% of the samples. No significant differences were observed in serum levels of the other 22 cytokines between baseline and 1 week or 4 weeks after IVC injection (Supplemental Table 1).
Serum levels of cytokines in infants with ROP
Compared with the control group, patients with ROP had increased levels of the cytokines VEGF-A (P = 0.002), VEGF-D (P = 0.012), MIP-1β (P = 0.009), IP-10 (P = 0.008), RANTES (P = 0.002), eotaxin (P = 0.017), TNF-α (P = 0.019), IL-18 (P = 0.025), EGF (P < 0.001), SCF (P = 0.007), PlGF-1 (P = 0.008), and β-NGF (P = 0.034), along with decreased levels of MCP-1 and HGF (P < 0.001 and P < 0.001, respectively). No significant difference was observed in the concentration of MIP-1α, IL-6, IL-8, SDF-1α, GRO-α, IFN-γ, IL-1RA, FGF-2, PDGF-BB, and BDNF between the two groups. Detailed results are presented in Table 2. The other 21 cytokines mentioned above were not analyzed.
Table 2.
Serum concentrations (pg/ml) (mean ± SD) of cytokines in ROP patients (study group) and subjects with congenital cataract (control group).
| Cytokines | ROP patients | Controls | P value |
|---|---|---|---|
| VEGF-A | 1976.18 ± 982.45 | 683.0 ± 452.8 | 0.002 |
| VEGF-D | 110.23 ± 99.57 | 26.1 ± 48.1 | 0.012 |
| MIP-1β | 194.64 ± 146.67 | 66.0 ± 74.3 | 0.009 |
| Eotaxin | 29.72 ± 24.13 | 10.6 ± 9.3 | 0.017 |
| IP-10 | 136.99 ± 111.45 | 37.9 ± 29.2 | 0.008 |
| RANTES | 27.50 ± 17.30 | 9.1 ± 11.8 | 0.002 |
| IL-18 | 48.97 ± 41.92 | 16.8 ± 32.5 | 0.025 |
| TNF-α | 14.30 ± 8.10 | 7.8 ± 5.6 | 0.019 |
| MCP-1 | 232.96 ± 255.37 | 560.6 ± 280.7 | < 0.001 |
| EGF | 50.31 ± 39.13 | 2.6 ± 4.2 | < 0.001 |
| SCF | 23.50 ± 15.91 | 9.3 ± 2.6 | 0.007 |
| PlGF-1 | 45.62 ± 37.48 | 11.3 ± 21.7 | 0.008 |
| β-NGF | 22.31 ± 16.00 | 10.7 ± 10.4 | 0.034 |
| HGF | 113.47 ± 113.59 | 678.0 ± 419.3 | < 0.001 |
| SDF-1α | 268.55 ± 204.30 | 221.6 ± 56.7 | 0.48 |
| GRO-α | 28.26 ± 35.30 | 7.1 ± 2.4 | 0.07 |
| BDNF | 62.75 ± 78.73 | 12.6 ± 16.1 | 0.05 |
| IFN-γ | 58.74 ± 59.31 | 19.2 ± 43.3 | 0.05 |
| IL-8 | 16.32 ± 29.74 | 14.2 ± 8.4 | 0.83 |
| IL-6 | 14.31 ± 10.50 | 24.3 ± 33.9 | 0.12 |
| MIP-1α | 17.26 ± 23.20 | 10.7 ± 3.5 | 0.39 |
| IL-1RA | 892.19 ± 1,388.95 | 585.1 ± 257.8 | 0.49 |
| FGF-2 | 16.63 ± 8.73 | 17.7 ± 6.9 | 0.71 |
| PDGF-BB | 243.53 ± 388.90 | 23.0 ± 41.3 | 0.08 |
Data are shown as mean ± SD. Mann–Whitney U test.
ROP retinopathy of prematurity, VEGF vascular endothelial growth factor, MIP macrophage inflammatory protein, IP-10 interferon-induced protein10, RANTES regulated upon activation normal T cell, IL interleukin, TNF-α tumor necrosis factor-alpha, MCP monocyte chemotactic and activatingfactor, EGF epidermal growth factor, SCF stem cell factor, PIGF-1 placental growth factor-1, NGF nerve growth factor, HGF hepatocyte growth factor, SDF1α stromal cell derived factor-1α, GROα growth-regulated oncogene α, BDNF brain-derived neurotrophic factor, IFN-γ interferon gamma, IL-1Ra interleukin-1 receptor antagonist, FGF-2 basic fibroblast growth factor, PDGF-BB platelet-derived growth factor-BB.
Discussion
In this study, we observed that 1) serum VEGF-A and VEGF-D levels were suppressed at 1 week after IVC and returned to baseline at 4 weeks, while no significant differences were observed in the serum levels of other cytokines between baseline and 1 week or 4 weeks after IVC injection; 2) compared with the control group, ROP patients had significantly different serum concentrations of several angiogenic, inflammatory, and chemotactic factors, indicating that those factors may be associated with ROP.
The main concerns of anti-VEGF therapies, a set of recently emerged treatments for ROP recently, are potential side effects of systemic VEGF suppression. A few studies have indicated that intravitreal anti-VEGF drugs induce systemic VEGF suppression for weeks to months. Sato et al.3 reported that serum VEGF levels significantly decreased 1 week after 0.5 mg intravitreal bevacizumab (IVB) in 4 patients. Wu et al.18 found that serum VEGF levels were suppressed at 1 day after IVB in 3 patients and still measurable in 1 patient at 8 weeks. In a later study by the same group, serum VEGF levels significantly decreased from baseline over a follow-up period of up to 8 weeks in 6 patients with ROP after IVB, while there was no significant difference in 4 patients who underwent intravitreal ranibizumab (IVR) treatment5. Hong et al.19 found that plasma VEGF was significantly reduced at 1 week and 2 weeks after IVB in 6 patients and returned to baseline at 8 weeks. Our previous study demonstrated that plasma VEGF was suppressed 1 day after IVR and normalized 1 week after injection20. Recently, Chen et al.21 found that serum VEGF levels were suppressed for at least 1 week after IVR. Only one case report found that the serum level of VEGF remained normalized until 4 weeks after IVR4. In another study, serum VEGF levels were significantly reduced in 9 patients after IVB and 5 patients after intravitreal aflibercept (IVA) up to 12 weeks, and the serum levels of VEGF were more suppressed in the IVB group than in the IVA group22.
However, serum VEGF concentrations varied broadly among different studies. Generally, systemic VEGF suppression seems to be more pronounced in IVB than IVR, but no studies have reported changes in serum VEGF concentration in ROP patients after IVC. In this study, we observed that serum concentrations of VEGF-A and VEGF-D were initially suppressed at 1 week after IVC and returned to baseline at 4 weeks. Conbercept is an engineered fusion protein with a molecular weight of 143 kDa that binds to all VEGF-A isoforms and the related VEGFR-1 ligands VEGF-B and PlGF. This drug has 50 times the VEGF binding affinity of bevacizumab or ranibizumab and washes out according to first-order kinetics in ocular tissues23. Systemic VEGF suppression after intravitreal anti-VEGF drugs is associated with the drug dosage, drug-free intervals, half-life, molecular size and presence of Fc function24. The vitreous half-life of conbercept is 4.2 days in rabbits, while those of aflibercept, bevacizumab and ranibizumab are 4.79 days, 6.61 days and 2.88 days, respectively25–27. The serum level of conbercept in 6 patients was undetectable within 1–2 days after injection in a previous study28. In our previous comparative study in adult patients with age-related macular degeneration29, serum VEGF concentrations were significantly decreased at 1 day and 1 week after intravitreal injection of 0.5 mg conbercept, while no significant effect was observed at 4 weeks; however, in the IVR group, no significant difference was observed at any of the observed time points, indicating that conbercept might have a longer systemic VEGF suppression time than IVR. The same results were detected in ROP patients. Our previous study demonstrated that plasma VEGF was suppressed at 1 day after IVR and normalized at 1 week after injection20. In this study, the dose of conbercept was reduced to 0.25 mg per eye, which is half the adult dosage for ROP, and 57 patients received a total of 0.5 mg conbercept. Serum concentrations of VEGF-A and VEGF-D were initially suppressed 1 week after IVC and returned to baseline at 4 weeks. Three patients were injected in only one eye, and we were unable to statistically analyze whether this affected systemic VEGF levels. Considering the suggestion from our previous study that 0.15 mg IVC was effective for Zone II Stage 2/3 ROP with plus disease,6 reducing the doses of the anti-VEGF agents appears to be a safer choice that reduces serum VEGF suppression. Moreover, there was no difference in serum VEGF concentrations between ROP patients with recurrence and other patients before or after IVC treatment. Overall, this study found no prolonged systemic VEGF suppression after IVC in ROP patients.
In this study, recurrence that required treatment occurred in 9 patients (15 eyes, 12.82%) with ROP. Our previous studies6,7 of conbercept demonstrated similar ROP recurrence rates (6/38 and 3/20, respectively), which were consistent with a study from another team in South China (8/48).8 In our comparative study,7 the recurrence rate was lower with conbercept than with ranibizumab (15/28, 53.6%). Our previous study found a similar recurrence rate (45.45%) of ranibizumab.20 Recently, another study found that 26.2% (18/42) of eyes had a recurrence of ROP after the initial IVR treatment in South China.21 Overall, it seems that conbercept is associated with a lower clinical recurrence rate than ranibizumab. At the end of the follow-up, no ocular or systemic adverse events were observed in this group.
In addition, no significant differences were observed in the serum levels of other cytokines between baseline and 1 week or 4 weeks after IVC injection. Conbercept can bind to PlGF, and a previous study reported that retinal PlGF levels were decreased significantly in the conbercept (KH902)-treated group in an oxygen-induced retinopathy model.30 However, the serum level of PlGF was not suppressed in this study.
Furthermore, this study showed that the levels of several cytokines were significantly different between ROP patients and the control group, adding information on the pathogenesis of ROP. The key role of VEGF in the pathogenesis of ROP has been well illustrated in many animal models as well as in humans. Previous studies detected no difference in cord blood VEGF concentrations at birth between preterm and term infants,31 between preterm infants who later developed ROP and those who did not develop this disease in a gestational age-matched case–control study,32 or between ROP and non-ROP infants at 32 or 36 weeks.33 In this study, circulatory VEGF-A and VEGF-D concentrations in ROP patients were significantly higher than those in infants with congenital cataract. The pathogenesis of ROP is considered to involve two phases. Phase I is characterized by downregulation of growth factors, and phase II is marked by overproduction of VEGF, leading to vasoproliferation. In our study, the ROP patients were in phase II, and so their VEGF concentrations were higher than those of the control group, consistent with other studies.34,35
In addition, the serum levels of MIP-1β, IP-10, RANTES, eotaxin, TNF-α, and IL-18 were significantly higher in ROP patients than in controls, while the opposite was true of MCP-1 levels, suggesting that inflammation is involved in the development of ROP. MIP-1β, TNF-α and IL-18 are proinflammatory factors that can compromise the blood–retinal barrier, exacerbate retinal ischemia, modulate angiogenesis, and induce the progression of ROP. Chemotactic cytokines, such as RANTES, IP-10, and eotaxin, chemoattract various inflammatory cells such as natural killer cells and monocytes, stimulating inflammatory cascades in many diseases.36,37 MCP-1 has been detected in neurons and astrocytes and is involved in the development of the brain and neuroretina.38 In a gestational age-matched case–control study, the serum level of MIP-1β was significantly higher in ROP patients than in healthy preterm neonates and was negatively correlated with birthweight.13 Several studies observed high plasma levels of TNF-α in association with an increased risk of ROP,14,15 while BDNF levels were negatively correlated with ROP risk.15 A large cohort study suggested that RANTES and IL-18 might be involved in the pathogenesis of ROP.12 In another study, vitreous levels of IP-10, eotaxin, and RANTES were significantly higher in ROP eyes than in non-ROP eyes39. Elevated aqueous levels of eotaxin, IFN-γ, IP-10, MIP-1β, and TNF-α were detected in ROP patients, and MIP-1β levels were independently correlated with ROP retreatment.40 These data were consistent with our findings.
Moreover, serum levels of EGF, SCF, PlGF-1, and β-NGF were significantly higher in ROP patients than in controls in this study. A previous study demonstrated that EGF receptor inhibitors prevented insulin-induced retinal vascular leakage in mice,41 and inhibition of PlGF-1 reduced pathological vascular leakage in a mouse retinopathy model.42 SCF was observed to be upregulated by hypoxia, directing the migration of neural progenitor cells and promoting angiogenesis.43 NGF has been found in the adult and developing rodent retina in association with associated with retinal degeneration.44 The vitreous level of NGF was significantly elevated in diabetic retinopathy patients.45 The role of these cytokines in ROP has not been established, and further studies are needed to achieve a better understanding of the pathogenesis of ROP. In summary, it seems that cytokines are intricately interrelated with the development of ROP.
Our study has several limitations that must be mentioned. The sample size was small, and the serum levels of several cytokines varied widely. In addition, the serum concentration of VEGF did not necessarily reflect the levels in the retina,46 and it varied in different studies, probably as a result of different patient selection criteria, stages of ROP, samples, and test methods. Moreover, the control group of this study included full-term infants with congenital cataract, and there was a significant difference in age. Thus, the differences in cytokine levels between the two groups may have been interfered with by gestational age and postmenstrual age.
Conclusion
In conclusion, IVC for ROP patients induced circulatory VEGF suppression at 1 week after injection, and this effect fully subsided at 4 weeks. IVC is an effective treatment for ROP patients, but its safety profile needs further investigation.
Supplementary information
Acknowledgements
The present study was supported by Beijing Bethune Charitable Foundation (Grant No. 2018-Z-08).
Author contributions
Involved in study design and conduct (Y.C., J.H.L.); data collection, management, analysis (Y.C., X.M.Z., D.D.L.H,J.H.L.), and interpretation (X.M.Z., Y.S.X., J.H.L.); and manuscript preparation, review, or approval (Y.C.,X.M.Z., J.H.L.).
Data availability
The original data used to support the findings of this study are available from the corresponding author upon request.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
These authors contributed equally: Yong Cheng and Xuemei Zhu.
Supplementary information
is available for this paper at 10.1038/s41598-020-69684-7.
References
- 1.Gilbert C. Retinopathy of prematurity: a global perspective of the epidemics, population of babies at risk and implications for control. Early Hum. Dev. 2008;84:77–82. doi: 10.1016/j.earlhumdev.2007.11.009. [DOI] [PubMed] [Google Scholar]
- 2.Lepore D, et al. Follow-up to age 4 years of treatment of type 1 retinopathy of prematurity intravitreal bevacizumab injection versus laser: fluorescein angiographic findings. Ophthalmology. 2018;125:218–226. doi: 10.1016/j.ophtha.2017.08.005. [DOI] [PubMed] [Google Scholar]
- 3.Sato T, et al. Serum concentrations of bevacizumab (avastin) and vascular endothelial growth factor in infants with retinopathy of prematurity. Am. J. Ophthalmo. 2012;153:327–333. doi: 10.1016/j.ajo.2011.07.005. [DOI] [PubMed] [Google Scholar]
- 4.Hoerster R, et al. Serum concentrations of vascular endothelial growth factor in an infant treated with ranibizumab for retinopathy of prematurity. Acta Ophthalmol. 2013;91:e74–75. doi: 10.1111/j.1755-3768.2012.02469.x. [DOI] [PubMed] [Google Scholar]
- 5.Wu WC, et al. Serum vascular endothelial growth factor after bevacizumab or ranibizumab treatment for retinopathy of prematurity. Retina. 2017;37:694–701. doi: 10.1097/IAE.0000000000001209. [DOI] [PubMed] [Google Scholar]
- 6.Cheng Y, Meng Q, Linghu D, Zhao M, Liang J. A lower dose of intravitreal conbercept effectively treats retinopathy of prematurity. Sci. Rep. 2018;8:10732. doi: 10.1038/s41598-018-28987-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Jin E, Yin H, Li X, Zhao M. Short-term outcomes after intravitreal injections of conbercept versus ranibizumab for the treatment of retinopathy of prematurity. Retina. 2018;38:1595–1604. doi: 10.1097/IAE.0000000000001763. [DOI] [PubMed] [Google Scholar]
- 8.Bai Y, et al. Efficacy of intravitreal conbercept injection in the treatment of retinopathy of prematurity. Br. J. Ophthalmol. 2018 doi: 10.1136/bjophthalmol-2017-311662. [DOI] [PubMed] [Google Scholar]
- 9.Lee J, Dammann O. Perinatal infection, inflammation, and retinopathy of prematurity. Semin. Fetal neonatal Med. 2012;17:26–29. doi: 10.1016/j.siny.2011.08.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Klinger G, et al. Outcome of early-onset sepsis in a national cohort of very low birth weight infants. Pediatrics. 2010;125:e736–740. doi: 10.1542/peds.2009-2017. [DOI] [PubMed] [Google Scholar]
- 11.Hong HK, et al. Neonatal systemic inflammation in rats alters retinal vessel development and simulates pathologic features of retinopathy of prematurity. J. Neuroinflamm. 2014;11:87. doi: 10.1186/1742-2094-11-87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Sood BG, et al. Perinatal systemic inflammatory response syndrome and retinopathy of prematurity. Pediatr. Res. 2010;67:394–400. doi: 10.1203/PDR.0b013e3181d01a36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Yu H, et al. Serum concentrations of cytokines in infants with retinopathy of prematurity. APMIS. 2014;122:818–823. doi: 10.1111/apm.12223. [DOI] [PubMed] [Google Scholar]
- 14.Silveira RC, Fortes Filho JB, Procianoy RS. Assessment of the contribution of cytokine plasma levels to detect retinopathy of prematurity in very low birth weight infants. Investig. Ophthalmol. Vis. Sci. 2011;52:1297–1301. doi: 10.1167/iovs.10-6279. [DOI] [PubMed] [Google Scholar]
- 15.Holm M, et al. Systemic inflammation-associated proteins and retinopathy of prematurity in infants born before the 28th week of gestation. Invest. Ophthalmol. Vis. Sci. 2017;58:6419–6428. doi: 10.1167/iovs.17-21931. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.16International Committee for the Classification of Retinopathy of, P. The International Classification of Retinopathy of Prematurity revisited. Arch. Ophthalmol.123, 991–999, 10.1001/archopht.123.7.991 (2005). [DOI] [PubMed]
- 17.Cheng Y, et al. Analysis of aqueous humor concentrations of cytokines in retinoblastoma. PLoS ONE. 2017;12:e0177337. doi: 10.1371/journal.pone.0177337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wu WC, et al. Serum levels of vascular endothelial growth factor and related factors after intravitreous bevacizumab injection for retinopathy of prematurity. JAMA Ophthalmol. 2015;133:391–397. doi: 10.1001/jamaophthalmol.2014.5373. [DOI] [PubMed] [Google Scholar]
- 19.Hong YR, et al. Plasma concentrations of vascular endothelial growth factor in retinopathy of prematurity after intravitreal bevacizumab injection. Retina. 2015;35:1772–1777. doi: 10.1097/IAE.0000000000000535. [DOI] [PubMed] [Google Scholar]
- 20.Zhou Y, Jiang Y, Bai Y, Wen J, Chen L. Vascular endothelial growth factor plasma levels before and after treatment of retinopathy of prematurity with ranibizumab. Graefe's Arch. Clin. Exp. Ophthalmol. 2016;254:31–36. doi: 10.1007/s00417-015-2996-0. [DOI] [PubMed] [Google Scholar]
- 21.Chen X, et al. Serum vascular endothelial growth factor levels before and after intravitreous ranibizumab injection for retinopathy of prematurity. J. Ophthalmol. 2019;2019:2985161. doi: 10.1155/2019/2985161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Huang CY, et al. Changes in systemic vascular endothelial growth factor levels after intravitreal injection of aflibercept in infants with retinopathy of prematurity. Graefe's Arch. Clin. Exp. Ophthalmol. 2018;256:479–487. doi: 10.1007/s00417-017-3878-4. [DOI] [PubMed] [Google Scholar]
- 23.Lu X, Sun X. Profile of conbercept in the treatment of neovascular age-related macular degeneration. Drug design, Dev. Therapy. 2015;9:2311–2320. doi: 10.2147/DDDT.S67536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Fogli S, et al. Clinical pharmacology of intravitreal anti-VEGF drugs. Eye. 2018;32:1010–1020. doi: 10.1038/s41433-018-0021-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Li H, et al. Pharmacokinetics of a long-lasting anti-VEGF fusion protein in rabbit. Exp. Eye Res. 2012;97:154–159. doi: 10.1016/j.exer.2011.09.002. [DOI] [PubMed] [Google Scholar]
- 26.Stewart MW, Rosenfeld PJ. Predicted biological activity of intravitreal VEGF Trap. Br. J. Ophthalmol. 2008;92:667–668. doi: 10.1136/bjo.2007.134874. [DOI] [PubMed] [Google Scholar]
- 27.Sinapis CI, et al. Pharmacokinetics of intravitreal bevacizumab (Avastin(R)) in rabbits. Clin. Ophthalmol. 2011;5:697–704. doi: 10.2147/OPTH.S19555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Zhang M, et al. A phase 1 study of KH902, a vascular endothelial growth factor receptor decoy, for exudative age-related macular degeneration. Ophthalmology. 2011;118:672–678. doi: 10.1016/j.ophtha.2010.08.008. [DOI] [PubMed] [Google Scholar]
- 29.Jin E, et al. Serum levels of vascular endothelial growth factor before and after intravitreal injection of ranibizumab or conbercept for neovascular age-related macular degeneration. Retina. 2017;37:971–977. doi: 10.1097/IAE.0000000000001274. [DOI] [PubMed] [Google Scholar]
- 30.Zhou AY, et al. Placental growth factor expression is reversed by antivascular endothelial growth factor therapy under hypoxic conditions. World J. Pediatr. 2014;10:262–270. doi: 10.1007/s12519-014-0502-0. [DOI] [PubMed] [Google Scholar]
- 31.Galazios G, et al. Umbilical cord serum vascular endothelial growth factor (VEGF) levels in normal pregnancies and in pregnancies complicated by preterm delivery or pre-eclampsia. Int. J. Gynaecol. Obstet. Off. Organ Int. Federation Gynaecol. Obstet. 2004;85:6–11. doi: 10.1016/j.ijgo.2003.08.009. [DOI] [PubMed] [Google Scholar]
- 32.Woo SJ, et al. The relationship between cord blood cytokine levels and perinatal factors and retinopathy of prematurity: a gestational age-matched case-control study. Investig. Ophthalmol. Vis. Sci. 2013;54:3434–3439. doi: 10.1167/iovs.13-11837. [DOI] [PubMed] [Google Scholar]
- 33.Pieh C, et al. VEGF-A, VEGFR-1, VEGFR-2 and Tie2 levels in plasma of premature infants: relationship to retinopathy of prematurity. Br. J. Ophthalmol. 2008;92:689–693. doi: 10.1136/bjo.2007.128371. [DOI] [PubMed] [Google Scholar]
- 34.Zhao M, et al. Expression of total vascular endothelial growth factor and the anti-angiogenic VEGF 165 b isoform in the vitreous of patients with retinopathy of prematurity. Chin. Med. J. 2015;128:2505–2509. doi: 10.4103/0366-6999.164937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Velez-Montoya R, et al. Intraocular and systemic levels of vascular endothelial growth factor in advanced cases of retinopathy of prematurity. Clin. Ophthalmol. 2010;4:947–953. doi: 10.2147/OPTH.S11650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Sullivan SE, et al. Circulating concentrations of chemokines in cord blood, neonates, and adults. Pediatr. Res. 2002;51:653–657. doi: 10.1203/00006450-200205000-00018. [DOI] [PubMed] [Google Scholar]
- 37.Luo Y, et al. RANTES stimulates inflammatory cascades and receptor modulation in murine astrocytes. Glia. 2002;39:19–30. doi: 10.1002/glia.10079. [DOI] [PubMed] [Google Scholar]
- 38.Yao Y, Tsirka SE. Monocyte chemoattractant protein-1 and the blood-brain barrier. Cell. Mol. Life Sci. CMLS. 2014;71:683–697. doi: 10.1007/s00018-013-1459-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Sato T, Kusaka S, Shimojo H, Fujikado T. Simultaneous analyses of vitreous levels of 27 cytokines in eyes with retinopathy of prematurity. Ophthalmology. 2009;116:2165–2169. doi: 10.1016/j.ophtha.2009.04.026. [DOI] [PubMed] [Google Scholar]
- 40.Lyu J, et al. Aqueous cytokine levels associated with severity of type 1 retinopathy of prematurity and treatment response to ranibizumab. Graefe's Arch. Clin. Exp. Ophthalmol. 2018;256:1469–1477. doi: 10.1007/s00417-018-4034-5. [DOI] [PubMed] [Google Scholar]
- 41.Sugimoto M, et al. Inhibition of EGF signaling protects the diabetic retina from insulin-induced vascular leakage. Am. J. Pathol. 2013;183:987–995. doi: 10.1016/j.ajpath.2013.05.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Luttun A, et al. Loss of placental growth factor protects mice against vascular permeability in pathological conditions. Biochem. Biophys. Res. Commun. 2002;295:428–434. doi: 10.1016/S0006-291X(02)00677-0. [DOI] [PubMed] [Google Scholar]
- 43.Han ZB, et al. Hypoxia-inducible factor (HIF)-1 alpha directly enhances the transcriptional activity of stem cell factor (SCF) in response to hypoxia and epidermal growth factor (EGF) Carcinogenesis. 2008;29:1853–1861. doi: 10.1093/carcin/bgn066. [DOI] [PubMed] [Google Scholar]
- 44.Garcia TB, Hollborn M, Bringmann A. Expression and signaling of NGF in the healthy and injured retina. Cytokine Growth Factor Rev. 2017;34:43–57. doi: 10.1016/j.cytogfr.2016.11.005. [DOI] [PubMed] [Google Scholar]
- 45.Boss JD, et al. Assessment of neurotrophins and inflammatory mediators in vitreous of patients with diabetic retinopathy. Investig. Ophthalmol. Vis. Sci. 2017;58:5594–5603. doi: 10.1167/iovs.17-21973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Modanlou HD, et al. Ontogeny of VEGF, IGF-I, and GH in neonatal rat serum, vitreous fluid, and retina from birth to weaning. Invest. Ophthalmol. Vis. Sci. 2006;47:738–744. doi: 10.1167/iovs.05-1046. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The original data used to support the findings of this study are available from the corresponding author upon request.