

Abstract
Breast cancer is the most prevalent malignancy among Lebanese women, and nearly half of these women are age < 50 years at diagnosis. Despite the current screening guidelines in Lebanon to start mammograms at 40 years of age, monthly self-breast examination, and yearly clinical breast examination, compliance with these recommendations remains low in both Lebanese and Lebanese-American women. This study aimed to examine different factors associated with breast cancer screening compliance in Lebanese and Lebanese-American women and determine and compare factors that predict breast cancer screening for these 2 groups. A cross-sectional study design was used to examine the factors associated with breast cancer screening compliance in Lebanese and Lebanese-American women. A total of 250 Lebanese women and 105 Lebanese-American women completed the questionnaires. Of these, 74.3% of Lebanese-American women and 72.5% of Lebanese women had ever had a mammogram, and 58.4% of Lebanese women had had a clinical breast examination, compared with 84.8% of Lebanese-American women. In both groups, health care provider recommendation was a predictor of having had a mammogram. Although the breast cancer screening practices of both groups are higher than previously reported, they continue to fall below the recommended rate of 81% according to the Healthy People Project. Given the susceptibility of Lebanese women age > 40 years to develop breast cancer, promotional breast cancer screening campaigns must emphasize the importance of adhering to screening guidelines for both Lebanese and Lebanese-American women.
INTRODUCTION
Breast cancer is the most commonly diagnosed cancer in women worldwide.1 In Lebanon, breast cancer is the most prevalent malignancy among Lebanese women,2 accounting for one third of all female cancers.3 Of these, 40% to 43% are women age < 50 years, as compared with 19% to 24% of cases in Western countries.4-7 Younger women generally present with more aggressive forms of breast cancer, thus resulting in poor prognosis and subsequently higher mortality rates. The prevalence of deleterious BRCA mutations is lower than expected in Lebanese women, supporting the hypothesis that other factors contribute to breast cancer in young women.8-11
CONTEXT
Key Objective
To evaluate and compare the perceived fears, barriers, and benefits regarding breast cancer screening between Lebanese and Lebanese- American women.
Knowledge Generated
More than 90% of both Lebanese and Lebanese-American women reported being familiar with breast cancer screening; however, the screening rates for both groups were below the recommended 81%. Physician and health care provider recommendation for breast cancer screening was a predictor of having had breast cancer screening in both groups.
Relevance
Given the susceptibility of Lebanese women age < 50 years to develop breast cancer, it is imperative they undergo breast cancer screening. Health care provider recommendation is a predictor of breast cancer screening for both groups; therefore, health care providers should educate Lebanese and Lebanese-American women on breast cancer risks and benefits of early detection and screening and recommend breast cancer screening.
Early detection of breast cancer can be achieved by mammography, breast self-examination (BSE), and clinical breast examination (CBE) and can lead to lower breast cancer mortality rates.12 In the United States, only mammography is recommended for early detection of breast cancer, with yearly mammography starting at age 45 years and biannual mammography after the age of 55 years.13-15 In Lebanon, however, because of early-age breast cancer occurrences among Lebanese women, the guidelines for breast cancer screening established by the Ministry of Public Health include annual mammography screening, monthly BSE, and yearly CBE.6,16,17
Despite these recommendations, there seem to be disparities in breast cancer screening between Lebanese women and Lebanese-American women. In the United States, it was last reported in 2008 that 28.6% of women of Lebanese descent underwent yearly mammography.18 This number is well below the Healthy People Project goal of 81% and considerably lower than that among Lebanese women in Lebanon, which is estimated to be 45% and 59.1%.19-21 Although the Healthy People program is based in the United States, its health promotion and disease prevention goals can be applied in other countries. Several factors, including but not limited to women’s knowledge and beliefs about breast cancer screening practices, play an important role in the use of breast cancer screening. Because the number of women undergoing breast cancer screening in the United States was found to be lower than that in Lebanon, it is important to determine the factors associated with screening compliance among Lebanese women and compare them with those of Lebanese-American women. This will allow for a better understanding of the similarities and differences in the factors that influence compliance with breast cancer screening in Lebanese and Lebanese-American women. This study aimed to examine different factors associated with breast cancer screening compliance in Lebanese and Lebanese-American women and determine and compare factors that predict breast cancer screening for these 2 groups.
METHODS
Design
The study used a descriptive, cross-sectional, comparative study design to evaluate and compare the different factors associated with breast cancer screening compliance in Lebanese and Lebanese-American women.
Sample
The sample size was based on the determination that an equivalence test of means using 2 1-sided tests on data from a parallel-group design with sample sizes of a minimum of 88 in the Lebanese-American group and 88 in the native Lebanese group would achieve 90% power at a 5% significance level when the true difference between the means were 0.00, the standard deviation 10.00, and the equivalence limits −5.00 and 5.00. A convenience sample was recruited from Beirut, Lebanon, and the greater Los Angeles area in the United States. Criteria for inclusion were Lebanon-born Lebanese-American women and Lebanon-born, currently residing in Lebanon, Lebanese women with no history of breast cancer who understand and read English or Arabic.
Instruments
Demographic information was collected using a self-administered questionnaire. The modified Champion’s Health Belief Model Scale (Arabic version) was used to measure health beliefs.22-24 The instrument consist of 42 items designed to measure variables related to breast cancer screening, such as fears, knowledge, barriers, and benefits regarding breast cancer screening. Items are rated on a 5-point Likert scale ranging from strong disagreement (1 point) to strong agreement (5 points). For example, the question “Undergoing mammography can give you confirmation that you are healthy and lessen concern” is 1 of the questions aimed at assessing the participant’s perception of the benefits to having a mammogram. The internal consistency of the Arabic version was previously determined and ranged from .87 to .92.22
Procedure
After institutional review board approvals from the research institutions in Lebanon and the United States, a poster was posted on the announcement bulletin board of the churches and mosques frequently attended by Lebanese women in Beirut, Lebanon, and the greater Los Angeles area requesting their participation in the study. Additionally, study materials, which included the recruitment letter, questionnaire, and researcher-addressed and stamped envelope, were made available in a box near the announcement bulletin boards. The churches and mosques did not sponsor, support, or participate in the promotion of the study. The interested participants completed the questionnaire packet and returned it to the researcher in the provided researcher-addressed and stamped envelope. By filling out the questionnaire, the participants consented to participating in the study. A total of 250 Lebanese women and 105 Lebanese-American women completed the questionnaires and mailed them to the researcher in the envelope provided.
Data Analysis
Descriptive statistics were first conducted on the demographic variables and to determine the scores of the instruments. These were compared between Lebanese and Lebanese-American women using odds ratios (ORs), χ2 and Mann-Whitney U tests, or analyses of variance. Any associations found to be statistically significant (P ≤ .05) between the 2 groups were included in 3 multiple logistic regression models to estimate the odds of each variable for ever having a mammogram (yes v no) or performing a CBE (yes v no) or BSE (yes v no). Likert responses were categorized into high (average > 3) or low average (≤ 3). All tests were 2 sided, and a P value < .05 was considered significant.
RESULTS
Sample Characteristics
The sample comprised 105 Lebanese-American women and 250 Lebanese women. χ2 and t test analyses were conducted to determine differences among the demographic characteristics between the 2 groups (Table 1). There were significantly more Muslim women in the Lebanese-American group compared with the Lebanese group (55.7% v 38.2%, respectively; P = .004). Lebanese-American women were significantly different from Lebanese women in income (P = .006) and age (P = .007).
TABLE 1.
Sample Demographic and Clinical Characteristics

Knowledge of Breast Cancer Screening
Although > 90% of women in both groups were familiar with mammography screening for breast cancer, only 74.3% of Lebanese-American women and 72.5% of Lebanese women had ever had a mammogram. Being familiar with mammography screening significantly increased compliance in Lebanese women (P = .034) but not in Lebanese-American women (P = .228). There were no statistically significant differences between the 2 groups in their familiarity with breast cancer screening. There was a statistically significant difference in the perception of breast cancer screening effectiveness, with Lebanese-American women perceiving all breast cancer screening methods (mammogram, CBE, and SBE) to be significantly more effective than Lebanese women (Table 1).
The 2 groups were not significantly different in ever having had a mammogram (74.3% of Lebanese-American women v 72.8% of Lebanese women); however, the Lebanese-American women had a higher rate of having had a mammogram within a year of completing the survey than the Lebanese women. (67.6% v 51.6%, respectively; P = .006). Despite being familiar with CBE, only 58.4% of Lebanese women had had a CBE, compared with 84.8% of Lebanese-American women (P = .0001). There was no statistically significant difference in performing SBE among the 2 groups (Table 1).
Fears
To compare the differences in the total score of subscale fears, the Mann-Whitney U test was used because the data did not meet the normality assumption of the independent t test. There was a statistically significant difference in the total score of fears between Lebanese-American (median, 2.58) and Lebanese women (median, 3.17; U = 8,791; P = .000). There were also statistically significant differences in individual fears, with Lebanese-American women identifying fear of losing their jobs as a concern, whereas Lebanese women feared saddening family, losing friends, neglecting children, death, suffering, changes in appearance, rumors and gossip, and sexual disturbances (Table 2).
TABLE 2.
Fear of Cancer and Benefits of and Barriers to Cancer Screening

Benefits of Breast Examination and Mammography
To determine if there was a difference between the benefits of breast examination and mammography between the 2 groups, the Mann-Whitney U test was used. The results indicated there was no difference between perceptions about the benefits of breast examination between the Lebanese-American (median, 4.00) and Lebanese women (median, 3.83; U = 10601.5; P = .095). There was also no statistically significant difference between perceptions about the benefits of mammography between the Lebanese-American (median, 4.50) and Lebanese women (median, 4.50; U = 11,961.5; P = .982). There were no statistically significant differences among the individual responses about the benefits of breast examination and mammography between the 2 groups (Table 2).
Barriers to Breast Examination and Mammography
The Mann-Whitney U test was used to determine if there was a difference in perceived barriers for breast examination and mammography between the 2 groups. The results indicated there was a statistically significant difference in the perception of barriers to breast cancer examination between Lebanese-American (median, 2.07) and Lebanese women (median, 2.251; U = 8,821.0; P = .000), with Lebanese women perceiving being uncomfortable looking at their body, worrying something may be discovered, and having a breast examination being pointless because it may be too late as significantly more important than Lebanese-American women (Table 2). There was also a statistically significant difference in the perceptions of barriers to mammography between Lebanese-American (median, 2.07) and Lebanese women (median, 2.52; U = 9,606.00; P = .005). Lebanese women also reported mammograms being more expansive, worrying something will be found, and being too late if something is found as more important barriers than Lebanese-American women (Table 2).
Bivariable Analysis and Predictors of Adherence
Direct logistic regression was performed to identify predictors of performing mammography screening. The models contained 5 independent variables: knowledge of mammography recommendations, knowledge level regarding the effectiveness of mammograms in discovering cancer, history of relatives with cancer, physician-recommended mammogram, and health care provider as the source of mammogram information. The Hosmer and Lemeshow test was used to determine if the models with these predictors were a good fit. For the Hosmer-Lemeshow goodness-of-fit test, a poor fit is indicated by a significance value < .05. The results for members of the Lebanese-American group (χ2 [n = 248] = 6.444; P = .598) and the Lebanese group (χ2 [n = 248] = 6.474) indicated that the models for both Lebanese-American and Lebanese women were a good fit, with a P value > .05.
Additional tests for the usefulness of these models included the Cox and Snell R2 and Nagelkerke R2 tests, which indicated the amount of variation in the dependent variable explained by the models. The results for the Lebanese-American group indicated that between 41.7% and 64.9% of the variance in “Has a history of having a mammogram” was explained by these predictive models. For the Lebanese group, 26.2% to 39.0% of the variance was explained by this set of variables.
In the Lebanese-American group, the strongest predictor of having had a mammogram was demonstration of knowledge of mammography screening recommendations. The OR for this predictor indicated those with correct answers were 45 times as likely to have had a mammogram compared with those who answered screening recommendations incorrectly (OR, 45.47; 95% CI, 7.01 to 294.85; P = .00). In the Lebanese group, there was no statistically significant difference in having had a mammogram between those who answered correctly and those who answered incorrectly in regard to recommendations for screening.
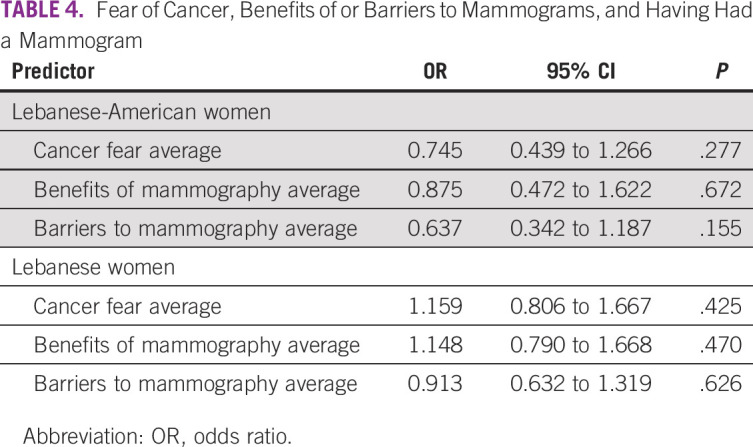
Members of the Lebanese-American group who referred to other sources of information (eg, television, Internet, friends) for mammography recommendations were > 14 times more likely to have had a mammogram than those who received their information from a health care provider (OR, 14.21; 95% CI, 1.90 to 106.14; P = .01). In both groups, there were statistically significant findings for health care provider recommendations for a mammogram. Lebanese-American participants were 14 times as likely to have had a mammogram if recommended by their physician (OR, 13.83; 95% CI, 1.98 to 96.37; P = .01). Lebanese participants had similar results; they were also 14 times as likely to have had a mammogram if recommended by their physician (OR, 14.34; 95% CI, 4.82 to 42.64; P = .00; Table 3). There was no indication that average scores on fear of cancer, benefits of mammograms, or barriers to mammograms were statistically significant predictors of history of having had a mammogram (Table 4).
TABLE 3.
Predictors of Mammography

TABLE 4.
Fear of Cancer, Benefits of or Barriers to Mammograms, and Having Had a Mammogram
DISCUSSION
This exploratory study sought to characterize and compare the prevalence of and factors associated with breast cancer screening in Lebanese and Lebanese-American women. The results of this study indicate that Lebanese and Lebanese-American women do not differ in their rates of mammography screening, despite their significantly different fears associated with a cancer diagnosis and perception of breast cancer screening barriers and benefits. A majority of the Lebanese-American and Lebanese women were familiar with the use of mammogram for detecting cancer, BSE, and CBE. These findings are comparable to the rate of 97.9% of women being familiar with the use of mammogram reported by Elias et al20; however, in our sample, 78.4% and 75.1% Lebanese-American and Lebanese women, respectively, reported having had a mammogram in the past versus the 36.4% of Lebanese-American women and 53.8% Lebanese women reported by Schwarts et al18 and Elias et al, respectively. This may be in part because of the differences in education level among the participants in the studies, with the Lebanese-American and Lebanese women who participated in our study having had more education than the participants in these other studies. The increase in mammography screening among Lebanese-American women could in part be a result of the increased media attention in recent years to breast cancer, as more celebrities have revealed their breast cancer diagnoses than previously, and of their being older than their Lebanese counterparts. The percentages of women with knowledge of CBE and BSE in both groups were much lower than those reported by Doumit et al25 (60.4% of Lebanese women and 59.1% of Lebanese-American women v 83.5% of Lebanese women, respectively). Lebanese-American women were more likely to have had a CBE (84.8%) compared with the Lebanese women in our study (58.4%) and the study by Doumit et al (71%). The percentage of women performing BSE was not different between Lebanese and Lebanese-American women in our study, but it was much lower than previous findings (48.6% of Lebanese-American women and 46% Lebanese women v 63.7% of Lebanese women, respectively).25 This may be in part because of a lack of focus on CBE and SBE, after no benefit was seen for CBE or SBE in detecting cancer or improving survival for women who have breast cancer.
Knowledge of mammography screening recommendations was the strongest predictor of having had a mammogram in Lebanese-American women, followed by recommendation by the physician and the health care provider being the first source of information. Knowledge of mammography screening did not translate into similar findings in Lebanese women. These findings are consistent with those of Alatrash et al,26 who found knowledge to be a significant predictor of mammography screening in Arab American women. Our findings are also contradictory to those of Hassoun et al,27 who reported knowledge as a barrier to breast cancer screening in Lebanese women. The only predictor of having had a mammogram in Lebanese women was mammogram being recommended by their physician. Knowledge regarding the effectiveness of breast cancer screening was statistically significantly higher in Lebanese-American women than in Lebanese women. This indicates that despite the increased efforts to raise awareness about breast cancer in Lebanon, the campaign may not be increasing women’s knowledge about the benefits of screening, which has been shown to be associated with the likelihood of seeking breast cancer screening. The likelihood of practicing breast cancer screening when recommended by the physician confirms previous findings.28-30
Overall fear of cancer and benefits of and barriers to mammograms were not statistically significant predictors of having had a mammogram in either group. This is in contradiction to the findings by Elias et al,20 who reported that the perceived benefits were significantly related to compliance with mammography screening. This is perhaps because the participants in this study relied on physician recommendations to perform the screening.
Limitations of our study include the fact that the sample was not representative of the larger population of Lebanese and Lebanese-American population, because it was conducted in Beirut, Lebanon, and greater Los Angeles, which are metropolitan areas.
In conclusion, the findings of this study indicate that despite acculturation, Lebanese-American women do not seek mammography screening at a higher rate than their Lebanese counterparts. Although the breast cancer screening practices of both groups are higher than previously reported, they continue to fall below the recommended rate of 81% by the Healthy People Project.21 Given the susceptibility of Lebanese women age > 40 years to develop breast cancer, promotional breast cancer screening campaigns must emphasize the importance of adhering to screening guidelines for both Lebanese and Lebanese-American women. In addition, given that < 75% of the mammograms were recommended by physicians, these providers should be educated to better inform them about Lebanese women’s b'reast cancer risk factors, the benefits of early detection and screening or rescreening, and the efficacy of breast cancer screening.
SUPPORT
Supported by a grant from Sigma Theta Tau International Honor Society of Nursing, Chi Alpha Chapter.
AUTHOR CONTRIBUTIONS
Conception and design: Laura Bourdeanu
Collection and assembly of data: Laura Bourdeanu, Manal Alatrash, Nayiri Ketchedjian
Data analysis and interpretation: Laura Bourdeanu, Manal Alatrash, Barbara Pate
Manuscript writing: All authors
Final approval of manuscript: All authors
Accountable for all aspects of the work: All authors
AUTHORS' DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to www.asco.org/rwc or ascopubs.org/go/site/misc/authors.html.
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (Open Payments).
Laura Bourdeanu
Stock and Other Ownership Interests: OncoGambit.com
Patents, Royalties, Other Intellectual Property: Cofounder of OncoGambit.com
Nayiri Ketchedjian
Employment: Whole Foods Market
Stock and Other Ownership Interests: Sientra (I)
No other potential conflicts of interest were reported.
REFERENCES
- 1. Torre LA, Islami, F, Siegel RL, et al: Global cancer in women: Burden and trends. Cancer Epidemiol Biomarkers Prev 26:444-457, 2017. [DOI] [PubMed]
- 2.Shamseddine A, Saleh A, Charafeddine M, et al. Cancer trends in Lebanon: A review of incidence rates for the period of 2003-2008 and projections until 2018. Popul Health Metr. 2014;12:4. doi: 10.1186/1478-7954-12-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Shamseddine A, Sibai AM, Gehchan N, et al. Cancer incidence in postwar Lebanon: Findings from the first national population-based registry, 1998. Ann Epidemiol. 2004;14:663–668. doi: 10.1016/j.annepidem.2003.12.002. [DOI] [PubMed] [Google Scholar]
- 4. doi: 10.2147/BCTT.S130273. El Chediak A, Alameddine RS, Hakim A, et al: Younger age is an independent predictor of worse prognosis among Lebanese nonmetastatic breast cancer patients: Analysis of a prospective cohort. Breast Cancer (Dove Med Press) 9:407-414, 2017. [DOI] [PMC free article] [PubMed]
- 5.El Saghir NS, Shamseddine AI, Geara F, et al. Age distribution of breast cancer in Lebanon: Increased percentages and age adjusted incidence rates of younger-aged groups at presentation. J Med Liban. 2002;50:3–9. [PubMed] [Google Scholar]
- 6.Lakkis NA, Adib SM, Osman MH, et al. Breast cancer in Lebanon: Incidence and comparison to regional and Western countries. Cancer Epidemiol. 2010;34:221–225. doi: 10.1016/j.canep.2010.02.013. [DOI] [PubMed] [Google Scholar]
- 7.Shamseddine AI, Musallam KM. Cancer epidemiology in Lebanon. Middle East J Cancer. 2010;1:41–44. [Google Scholar]
- 8.Chouchane L, Boussen H, Sastry KSR. Breast cancer in Arab populations: Molecular characteristics and disease management implications. Lancet Oncol. 2013;14:e417–e424. doi: 10.1016/S1470-2045(13)70165-7. [DOI] [PubMed] [Google Scholar]
- 9.El Saghir NS, Zgheib NK, Assi HA, et al. BRCA1 and BRCA2 mutations in ethnic Lebanese Arab women with high hereditary risk breast cancer. Oncologist. 2015;20:357–364. doi: 10.1634/theoncologist.2014-0364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Farra C, Dagher C, Badra R, et al: BRCA mutation screening and patterns among high-risk Lebanese subjects. Hered Cancer Clin Pract 17:4, 2019. [DOI] [PMC free article] [PubMed]
- 11.Jalkh N, Nassar-Slaba J, Chouery E, et al. Prevalance of BRCA1 and BRCA2 mutations in familial breast cancer patients in Lebanon. Hered Cancer Clin Pract. 2012;10:7. doi: 10.1186/1897-4287-10-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Smith RA, Andrews KS, Brooks D, et al. Cancer screening in the United States, 2019: A review of current American Cancer Society guidelines and current issues in cancer screening. CA Cancer J Clin. 2019;69:184–210. doi: 10.3322/caac.21557. [DOI] [PubMed] [Google Scholar]
- 13.Committee on Practice Bulletins—Gynecology Practice bulletin number 179: Breast cancer risk assessment and screening in average-risk women. Obstet Gynecol. 2017;130:e1–e16. doi: 10.1097/AOG.0000000000002158. [DOI] [PubMed] [Google Scholar]
- 14.Oeffinger KC, Fontham ET, Etzioni R, et al. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA. 2015;314:1599–1614. doi: 10.1001/jama.2015.12783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. doi: 10.7326/M15-2886. Siu AL; US Preventive Services Task Force: Screening for breast cancer: US Preventive Services Task Force recommendation statement. Ann Intern Med 164:279-296, 2016 [Erratum: Ann Intern Med 164:448, 2016] [DOI] [PubMed] [Google Scholar]
- 16. doi: 10.1016/S0140-6736(11)61351-2. Forouzanfar MH, Foreman KJ, Delossantos AM, et al: Breast and cervical cancer in 187 countries between 1980 and 2010: A systematic analysis. Lancet. 378:1461-1484, 2011. [DOI] [PubMed] [Google Scholar]
- 17.Youlden DR, Cramb SM, Dunn NA, et al. The descriptive epidemiology of female breast cancer: An international comparison of screening, incidence, survival and mortality. Cancer Epidemiol. 2012;36:237–248. doi: 10.1016/j.canep.2012.02.007. [DOI] [PubMed] [Google Scholar]
- 18.Schwartz K, Fakhouri M, Bartoces M, et al. Mammography screening among Arab American women in metropolitan Detroit. J Immigr Minor Health. 2008;10:541–549. doi: 10.1007/s10903-008-9140-8. [DOI] [PubMed] [Google Scholar]
- 19.El Asmar M, Bechnak A, Fares J, et al. Knowledge, attitudes and practices regarding breast cancer amongst Lebanese females in Beirut. Asian Pac J Cancer Prev. 2018;19:625–631. doi: 10.22034/APJCP.2018.19.3.625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Elias N, Bou-Orm IR, Adib SM. Patterns and determinants of mammography screening in Lebanese women. Prev Med Rep. 2016;5:187–193. doi: 10.1016/j.pmedr.2016.12.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Office of Disease Prevention and Health Promotion: Healthy People 2020. https://www.healthypeople.gov/2020/topics-objectives/topic/cancer/objectives.
- 22. Azaiza F, Cohen M: Health beliefs and rates of breast cancer screening among Arab women. J Womens Health (Larchmt) 15:520-30, 2006. [DOI] [PubMed]
- 23.Champion VL. Instrument development for health belief model constructs. ANS Adv Nurs Sci. 1984;6:73–85. doi: 10.1097/00012272-198404000-00011. [DOI] [PubMed] [Google Scholar]
- 24.Champion VL. Revised susceptibility, benefits, and barriers scale for mammography screening. Res Nurs Health. 1999;22:341–348. doi: 10.1002/(sici)1098-240x(199908)22:4<341::aid-nur8>3.0.co;2-p. [DOI] [PubMed] [Google Scholar]
- 25. Doumit M, Arevian M, Fares S: Knowledge, attitude and practice of Lebanese women towards breast cancer, breast self-examination and mammography. Presented at the 43rd Biennial Convention for Sigma Theta Tau International Honor Society, Las Vegas, NV. November 7-11, 2015. [Google Scholar]
- 26.Alatrash M. Prevalence, perceived benefits, and perceived barriers regarding breast cancer screening among three Arab American women subgroups. J Transcult Nurs. 2020;31:242–249. doi: 10.1177/1043659619859058. [DOI] [PubMed] [Google Scholar]
- 27.Hassoun Y, Dbouk H, Aldin E, et al. Barriers to mammography screening: How to overcome them. Mid East J Canc. 2015;6:243–251. [Google Scholar]
- 28.Elobaid YE, Aw TC, Grivna M, et al. Breast cancer screening awareness, knowledge, and practice among arab women in the United Arab Emirates: A cross-sectional survey. PLoS One. 2014;9:e105783. doi: 10.1371/journal.pone.0105783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Leslie NS, Deiriggi P, Gross S, et al. Knowledge, attitudes, and practices surrounding breast cancer screening in educated Appalachian women. Oncol Nurs Forum. 2003;30:659–667. doi: 10.1188/03.ONF.659-667. [DOI] [PubMed] [Google Scholar]
- 30.Ravichandran K, Al-Hamdan NA, Mohamed G. Knowledge, attitude, and behavior among Saudis toward cancer preventive practice. J Family Community Med. 2011;18:135–142. doi: 10.4103/2230-8229.90013. [DOI] [PMC free article] [PubMed] [Google Scholar]