

Abstract
Objective
Here, we investigated whether cytokines in the cervicovaginal fluid (CVF) can be predictive markers of preterm birth (PTB).
Methods
A multi-center prospective cohort study was conducted on 59 singleton pregnant women hospitalized for preterm labor (PTL) and/or preterm premature rupture of membranes (pPROM) between 22 weeks and 36 weeks 6 days of gestation from 2014 to 2015. The levels of 13 inflammatory cytokines (macrophage inflammatory protein [MIP]-1α, MIP-1β, tumor necrosis factor [TNF]-α, interleukin [IL]-1β, IL-6, IL-8, IL-17α, granulocyte colony stimulating factor [G-CSF], IL-7, IL-4, IL-5, IL-10, and IL-13) were measured using a multiplex bead-based immunoassay and that of fetal fibronectin (fFN) was measured using enzyme-linked immunosorbent assay (ELISA). Statistical analyses were performed using Student’s t-test, Mann-Whitney U test, Pearson’s correlation, and receiver operating characteristic (ROC) curve analysis in SPSS version 20.0.
Results
Among the 13 cytokines assessed, the levels of 3 cytokines (MIP-1α, IL-6, and IL-7) were negatively correlated with gestational age at delivery (P=0.028, P=0.002, and P=0.018, respectively). Sensitivities of MIP-1α, IL-6, and IL-17α were 70%, 80%, and 75%, respectively, and their specificities were 57%, 65%, and 69%, respectively. The sensitivity and specificity of fFN were 33% and 95%, respectively.
Conclusion
In symptomatic women diagnosed with PTL and/or pPROM, cytokines from cervicovaginal fluid, especially IL-6 and IL-17α, could be better predictive markers of PTB than fFN.
Keywords: Cytokines, Interleukin-6, Interleukin-17A, Biomarkers, Preterm birth
Introduction
Preterm birth (PTB), defined as birth before 37 weeks of gestation, is a major cause of neonatal morbidity and mortality [1,2]. Over the past decade, the prevalence of preterm births has steadily increased worldwide. Morbidity and mortality of infants born before 34 weeks of gestation are more than those of infants born after 34 weeks. Therefore, antenatal steroid administration is recommended for patients with preterm labor (PTL) and preterm premature rupture of membranes (pPROM). However, prediction methods and therapies for the same are not well studied.
PTB can be classified into two categories: spontaneous and iatrogenic. Spontaneous PTB accounts for up to 75% of all PTBs [3]. About 45% of PTBs are caused by PTL with intact membranes, while 30% are caused by the pre-labor rupture of fetal membranes. Causes of spontaneous PTB include activation of inflammatory reactions in the gestational tissues and secretion of inflammatory cytokines as an immune response to ascending infection of the genital tract and abnormal vaginal microorganisms [4-7].
Many studies aimed at predicting PTB have been conducted. Commonly used screening tests include risk scoring, cervical length measurement, and detection of biochemical markers. Risk scoring involves quantification of risk factors for spontaneous PTB and/or pPROM, including PTB history, cervical conization history, low socioeconomic status, low body mass index, smoking, drug use, anxiety, multifetal gestation, gestational diabetes, and gestational hypertension [6-9]. Tests for fetal fibronectin (fFN) and phosphorylated insulin-like growth factor binding protein-1 (IGFBP1) are now commercially available [10,11]. The level of fFN in cervicovaginal fluid (CVF), leaked due to the disruption of maternal choriodecidual tissues and through matrix remodeling, was used as a diagnostic marker for predicting PTB using a noninvasive method. Lockwood et al. described the clinical utility of fFN to predict spontaneous PTB in symptomatic women with high sensitivity (81.7%) and specificity (82.5%), based on a fFN threshold concentration of ≥50 ng/mL [3,8]. However, its specificity and sensitivity were confounded by unprotected vaginal intercourse, digital examination, bleeding, or contamination with amniotic fluid [1,12]. Cervical length measurement using transvaginal sonograms in patients with PTL and pPROM have also been used to predict PTB; however, it requires a skilled ultrasonographer and shows limited correlation with CVF [13-15].
Increased levels of inflammatory cytokines in CVF signify intra-amniotic infection that causes PTB [16]. Several inflammatory cytokines, including interleukin (IL)-1, -2, -4, -6, -8, -10, -12 and -17, tumor necrosis factor-alpha (TNF-α), interferon gamma (INF-γ), regulated on activation, normal T cell expressed and secreted (RANTES), and C-reactive protein (CRP), have been detected in the CVF, amniotic fluid, and blood of asymptomatic and symptomatic pregnant women [3,4,17,18]. IL-6 and matrix metalloproteinase-8 (MMP-8) levels in the amniotic fluid were significantly correlated with pPROM [19,20]. We also found that the levels of cytokines such as IL-1b, IL-6, IL-7, IL-7a, and TNF-α were significantly increased in the amniotic fluid of patients with cervical insufficiency [16]. Thereafter, the objective of our study was to determine whether inflammatory cytokines could be measured using non-invasive methods. Recent studies have shown that IL-6, IL-8, macrophage inflammatory protein (MIP)-1α, and MIP-1β levels in the CVF of patients with pPROM were correlated with those in the amniotic fluid [21]. IL-1β, IL-6, IL-8, and TNF-α levels were also elevated in patients with intact membranes in PTL [22]. There have also been studies in which IL-6 was shown to be a useful marker for predicting preterm delivery.
In the preset study, we expected that the levels of inflammatory cytokines in the CVF would be elevated in patients with PTL and pPROM. We investigated whether the levels of cytokines in the CVF could be a better predictive marker of PTB than that of fFN in CVF.
Materials and methods
1. Study population
A multi-center (Ewha Womans University Mokdong Hospital, Samsung Medical Center, Konkuk University Hospital, Seoul St. Mary’s Hospital, and Seoul Metropolitan GovernmentSeoul National University Boramae Medical Center) prospective cohort study was conducted in singleton pregnant women suffering from complications of PTL and/or pPROM between 22 weeks and 36 weeks 6 days of gestation, from 2014 to 2015. The characteristics (age, parity, and body mass index at admission) of the mother were analyzed. To diagnose pPROM, sterile speculum exam was conducted for detecting amniotic fluid pooling in vaginal cavity and nitrazine test was done. Uterine activity was assessed by cardiotocography. PTL was diagnosed in patients with regular uterine contraction and 4 or more contractions in 20 minutes, or 8 or more in 60 minutes as detected by cardiotocography. A total of 65 women with singleton pregnancies were included in this study. Patients with preeclampsia, hemolysis, elevated liver enzymes, a low platelet count (HELLP) syndrome, incompetent internal os of cervix (IIOC), and placenta previa were excluded. Out of the 59 participants, 19 were diagnosed with pPROM, and the rest with PTL (Fig. 1); no patient was suspected of clinical chorioamnionitis, defined according to the criteria of Gibbs et al. [23], which includes the presence of fever (>37.8°C) and two or more of the following associated clinical findings: uterine tenderness, malodorous vaginal discharge, maternal leukocytosis, maternal tachycardia, and fetal tachycardia. Gestational age was estimated by fetal biometry, assessed using a sonogram during the first trimester. Cervical length was measured at the time of admission by transvaginal ultrasound. Vaginal transducers were placed in the anterior fornix to examine the endocervical canal. Calipers were used to measure the length of the cervical canal from internal to external os. Women with pPROM at less than 35 weeks of gestation were treated with corticosteroids, tocolytics, and antibiotics. After 34 weeks, all patients with pPROM underwent induced delivery, when there was no labor pain, or cesarean section, if it was indicated. Those with PTL were treated with corticosteroids and tocolytics. We checked pregnancy outcome in terms of gestational age at delivery, birth weight, and Apgar score of the newborn at 1 and 5 minutes.
Fig. 1.
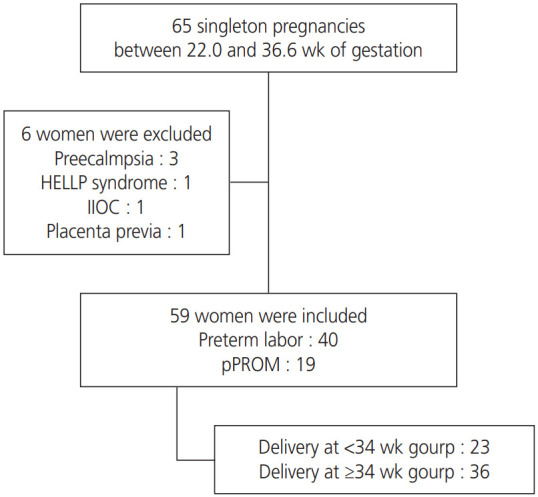
Flow chart of participants in the cohort study. HELLP, hemolysis, elevated liver enzymes, and a low platelet count; IIOC, incompetent internal os of cervix.
2. Cervicovaginal fluid collection and laboratory study
CVF was collected from the posterior vaginal fornix with a sterile cotton swab and stored at −80°C within 30 minutes of collection, until further analysis. The levels of 13 inflammatory cytokines (MIP-1α, MIP-1β, TNF-α, IL-1β, IL-6, IL-8, IL17α, granulocyte-colony stimulating factor [G-CSF], IL-7, IL-4, IL-5, IL-10, and IL-13) in the CVF were measured using the Human Cytokine/Chemokine Magnetic Bead Panel (Merck Millipore, Burlington, MA, USA). The intra-assay and interassay variations of all analyses were less than 10% and 12%, respectively. fFN in CVF was also sampled similarly and measured using a human fFN enzyme-linked immunosorbent assay (ELISA) kit (CUSABIO, Houston, TX, USA).
3. Statistical analysis
Statistical analyses were performed using the Statistical Package for Social Sciences (version 20; SPSS Inc., Chicago, IL, USA). Clinical characteristics were compared using Student’s t-test for continuous variables and χ2 test for categorical variables. P<0.05 was considered statistically significant. The relationship between the level of cytokines and gestational age at delivery was analyzed using Pearson’s correlation. The levels of cytokines were analyzed by the Mann-Whitney U test and compared between preterm delivery group (delivery at <34 weeks) and normal controls (delivery at ≥34 weeks). Receiver operating characteristic (ROC) curves of cytokine levels in early preterm birth were generated and the area under the curve (AUC) was determined.
Results
1. Characteristics of the study population
The demographic and clinical data of the study participants are presented in Table 1. The study group consisted of 23 pregnant women who delivered before 34 weeks of gestation and the controls (n=36) delivered after 34 weeks of gestation. There was no significant difference in age, parity, body mass index, and cervical length between the two groups (P=0.519, P=0.730, P=0.487, and P=0.381, respectively). fFN in the CVF showed a significant difference between the two groups (P=0.017). The study group was divided into PTL- and pPROM- subgroups. Frequency analysis was performed at the time of admission using the χ2 test for the diagnosis. There was no statistical difference in the distribution between the two groups, with a P-value of 0.77. Gestational age at the time of diagnosis was significantly different for the two groups (P=0.002). The white blood cell count, birth weight, and Apgar score of the newborns showed significant differences between the two groups (P<0.001).
Table 1.
Clinical characteristics of the study population (n=59)
| Characteristics | Delivery at <34 wk (n=23) | Delivery at ≥34 wk (n=36) | P-valuea) |
|---|---|---|---|
| Maternal age (yr) | 31 (23–38) | 32 (19–46) | 0.519 |
| Nulliparity | 6 (16.7) | 3 (13.0) | 0.730d) |
| BMI (kg/m2) | 24 (20–33) | 25 (18–32) | 0.487 |
| Fetal fibronectin (ng/mL) | 133 (11–699) | 40 (11–142) | 0.017b) |
| WBC (cell/mL) | 13,596 (8,130–24,280) | 10,063 (6,440–16,640) | <0.001c) |
| Cervical length (mm) | 20 (0–44) | 23 (2–69) | 0.381 |
| <25 mm group | 12 (57.1) | 18 (54.5) | >0.990d) |
| ≥25 mm group | 9 (42.9) | 15 (45.5) | |
| Diagnosis at admission | |||
| PTL group | 12 (52.2) | 28 (77.8) | 0.077d) |
| pPROM group | 11 (47.8) | 8 (22.2) | |
| Gestational age at admission (wk) | 28 (22–33) | 31 (20–36) | 0.002b) |
| Gestational age at delivery (wk) | 29 (23–33) | 36 (34–41) | <0.001c) |
| Birth weight (g) | 1,323 (570–2,320) | 2,640 (780–3,740) | <0.001c) |
| Apgar score at 1 min | 6 (0–10) | 8 (4–10) | <0.001c) |
| Apgar score at 5 min | 7 (0–10) | 9 (8–10) | <0.001c) |
Data are expressed as median (range) for continuous variables and number (%) for categorical variables.
BMI, body mass index; WBC, white blood cell; PTL, preterm labor; pPROM, preterm premature rupture of membranes.
Continuous variable were analyzed by Student’s t-test;
Significant difference between 2 group (P<0.05);
Significant difference between 2 group (P<0.001);
Categorical variable was analyzed by χ2 test.
2. Cytokine levels in the cervicovaginal fluid in the study and control groups
Among the 13 cytokines considered for the study, 9 (MIP-1β, MIP-1α, TNF-α, IL-1β, IL-6, IL-8, IL-17α, G-CSF, IL-7) were detected in the CVF of the 2 groups. Fig. 2 graphically shows the correlation of these 9 cytokines with the gestational age at delivery; 4 of these (MIP-1α, MIP-1β, IL-6, and IL-7) showed a significant negative correlation (P=0.003, P=0.010, P=0.035, and P=0.041, respectively). The levels of these 9 cytokines were compared between the study group and control group and are shown in Table 2. The levels of 3 cytokines (MIP-1α, IL-6, and IL-17α) were significantly higher in patients with PTL and/or pPROM who delivered before 34 weeks of gestation, compared to controls (P=0.028, P=0.002, and P=0.018, respectively). ROC curves were constructed for the 5 cytokines (MIP-1α, MIP-1β, IL-6, IL-7, and IL-17α) showing significant differences between the two groups and AUC values and optimal concentration thresholds for predictive utility were determined. Based on these thresholds, the sensitivities and specificities for the prediction of PTB were determined (Fig. 3 and Table 3). Sensitivities of MIP-1β, MIP-1α, IL-6, IL-17α, and IL-7 were 47%, 70%, 80%, 75%, and 35%, respectively, and their specificities of were 82%, 57%, 65%, 69%, and 94%, respectively; the areas under the ROC curves of these cytokines were 0.676, 0.677, 0.788, 0.715, and 0.643, respectively. The sensitivity and specificity of CVF fFN were 33% and 95%, respectively. Forty patients who were diagnosed with PTL at the time of admission were analyzed. The levels of IL-6 and IL-7 showed significant increase in the study group with P-values of 0.023 and 0.040, respectively (Supplementary Table 1). The ROC curves for these 2 cytokines were constructed and AUC values and optimal concentration thresholds for predictive utility were determined (Supplementary Table 2). Sensitivities of IL-6 and IL-7 were 83% and 83%, respectively, and their specificities were 76% and 64%, respectively. The sensitivity and specificity of CVF fFN were 33% and 70%, respectively. Subgroup analysis of 19 patients who were diagnosed with pPROM at the time of admission compared the cytokines of PTB and control group. IL-1β showed a significant difference with P-value 0.043 (Supplementary Table 3).
Fig. 2.

The relationship between cytokine level and gestational age at delivery. Using Pearson correlation. MIP, macrophage inflammatory protein; TNF, tumor necrosis factor; IL, interleukin; G-CSF, granulocyte colony stimulating factor. a)Significantly negative correlated with the gestational age at delivery (P<0.05).
Table 2.
Cervicovaginal fluid cytokine levels in patients in the study group and control group
| Cytokine | Delivery at <34 wk (n=23) | Delivery at ≥34 wk (n=36) | P-valueb) |
|---|---|---|---|
| MIP-1β | 18.56 (0–375.00) | 2.89 (0–301.56) | 0.067 |
| MIP-1α | 11.62 (0–309.47) | 5.73 (0–130.48) | 0.028a) |
| TNF-α | 0 (0–169.67) | 0 (0–130.66) | 0.661 |
| IL-1β | 65.35 (0–3,321.48) | 67.08 (0–2,990.27) | 0.738 |
| IL-6 | 83.27 (0–1,712.41) | 1.44 (0–956.15) | 0.002a) |
| IL-8 | 3,663.22 (234.78–10,911.85) | 3,007.72 (154.79–10,365.90) | 0.472 |
| IL-17α | 6.54 (1.51–17.97) | 4.17 (0–11.69) | 0.018a) |
| G-CSF | 38.80 (0–1,097.48) | 38.74 (0–818.30) | 0.225 |
| IL-7 | 2.81 (0–18.83) | 0 (0–19.55) | 0.064 |
Data are expressed as the median (range) (pg/mL).
MIP, macrophage inflammatory protein; TNF, tumor necrosis factor; IL, interleukin; G-CSF, granulocyte colony stimulating factor
Significant difference between 2 groups (P<0.05);
Using Mann-Whitney U test.
Fig. 3.
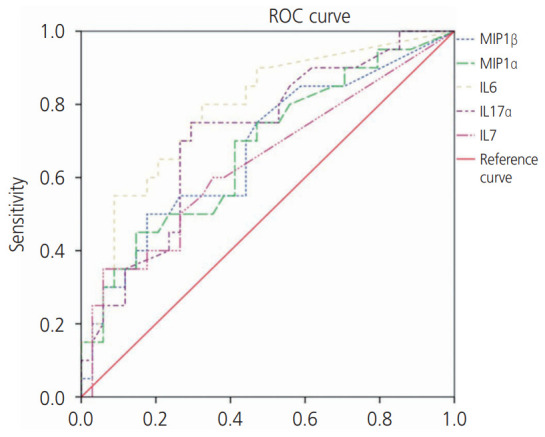
ROC curves of 5 cytokines in the prediction of early preterm birth (delivery at <34 weeks). ROC, receiver operating characteristic; MIP, macrophage inflammatory protein; TNF, tumor necrosis factor; IL, interleukin; G-CSF, granulocyte colony stimulating factor.
Table 3.
Receiver operating characteristic curve analysis
| Cytokine | AUC | 95% CI | P-value | Cut-off | Sensitivity | Specificity |
|---|---|---|---|---|---|---|
| MIP-1β | 0.676 | 0.525–0.828 | 0.032 | 17.51 | 47 | 82 |
| MIP-1α | 0.677 | 0.527–0.828 | 0.031 | 6.46 | 70 | 57 |
| IL-6 | 0.788 | 0.661–0.915 | 0.000 | 23.46 | 80 | 65 |
| IL-17α | 0.715 | 0.574–0.857 | 0.009 | 5.53 | 75 | 69 |
| IL-7 | 0.643 | 0.485–0.802 | 0.081 | 0.98 | 35 | 94 |
| Fibronectin | 0.662 | 0.494–0.830 | 0.073 | 74.50 | 33 | 95 |
AUC, area under a receiver operating characteristic curve; CI, confidence interval; MIP, macrophage inflammatory protein; IL, interleukin.
Discussion
Our study showed that elevated levels of multiple cytokines (MIP-1α, MIP-1β, IL-6, IL-7, and IL-17α) in the CVF were associated with PTB. Among these, IL-6 and IL-17α showed better sensitivity than the more commonly used marker fFN. This indicated that IL-6 and IL-17α can be used as predictive markers for PTB.
Fetal fibronectin, involved in maintaining the integrity of the fetal chorion and maternal decidua, predicts spontaneous PTB when detected in CVF between 22 and 34 weeks of gestation. Meta-analysis of Leitich et al. [24], found the sensitivity and specificity of fFN in predicting PTB in mothers with PTL to be 63% and 86%, respectively. In our study, however, fFN showed 33% sensitivity of and 95% specificity as a predictor of PTB. As shown in Table 3, the sensitivities of IL-6 and IL-17α were higher than those of fFN by 80% and 75%, respectively. The AUC of fFN was 0.662, while those of IL-6 and IL-17α were 0.788 and 0.715, respectively. The results for fFN may be confounded by unprotected vaginal intercourse, digital examination, bleeding, or contamination with amniotic fluid [1,12]. We did not consider the amniotic fluid contamination of CVF as a confounding factor and believe that it affected the outcome for pPROM patients. Therefore, in the subgroup analysis, the fFN and cytokine levels of the PTL patients, but not of the pPROM patients, were compared. In subgroup analysis, the sensitivity of IL-6 and IL-7 both were 83%, which was higher than the 33% sensitivity of fFN.
Several protein mediators and cytokines have been studied in the amniotic fluid, blood, urine, and CVF [1,25,26]. Studies considering the association of elevated inflammatory cytokines with chorioamnionitis and PTL were initiated in the amniotic fluid [19]. However, since amniocentesis itself is an invasive method, many studies sought to measure the same non-invasively in the blood, urine, and CVF. The composition of human CVF reflects the local biochemical environment of the gestational tissues. Therefore, CVF proteins, such as fFN, IGFBP1, defensins, lactoferrin, sialidase, granulocyte elastase, human chorionic gonadotropin, IL-1β, IL-6, IL-8, IL-18, IL-1 receptor antagonists, and TNF have been utilized to predict PTB [27-32]. Particularly, IL-6 is strongly associated with intraamniotic inflammation and microbe-associated intra-amniotic inflammation; hence, measurement of IL-6 in CVF can be used as an easy, noninvasive, rapid method for point-of-care assessment [33,34]. IL-6 induces T-lymphocytes to synthesize C-reactive protein and to promote the differentiation of B-cells. It is a pro-inflammatory cytokine seen widely in decidual tissue, placenta, fetal membrane, and amniotic fluid, and regulates immune adaptation to allow the pregnancy to progress. Preterm labor and pPROM are thought be because of the inflammatory condition caused by infection. Our study has showed that IL-6 is superior to conventional fFN assays. IL-17α as a protective cytokine in host defense against bacterial and fungal infections, was shown to be associated with intra-amniotic inflammation [35].No study has analyzed IL-17 in the CVF; however, IL-17α was significantly elevated in the amniotic fluid of patients with cervical insufficiency [16]. MIP-1α and MIP-1β are produced in the macrophages in response to infection and inflammation. They subsequently activate human granulocytes and the level of MIP-1α in the CVF is associated with amniotic fluid infection [21,36,37]. MIP-1α has been studied in the CVF of patients with pPROM, but not PTL. In this study, we found that elevation of the MIP-1α level in the CVF was associated with PTL. IL-7 is a cytokine that can stimulate IL-17 production by cells involved in both innate and adaptive immunity. Elevated serum IL-7 is also associated with PTL [38].
Although our sample size was small, the strength of this study is that it was conducted as a multi-center prospective study in 5 centers in Korea. This study directly compared cytokines and fFN in the CVF from the same cohort of patients. When selecting a patient group, the ones with multiple gestation, gestational diabetes, and gestational hypertension were excluded. However, factors such as cervical conization history, socio-economic status, pre-pregnancy body mass index, smoking, drug use, and anxiety that could be confounding factors could not be excluded. The gestational age at diagnosis is also a confounding factor that may affect the gestational age at delivery, but no analysis has been done to correct this.
In conclusion, CVF cytokines, especially IL-6, IL-17α, could be useful predictive markers of PTB in patients with PTL and/or pPROM; however, studies with larger cohort will be required for validation of these findings.
Acknowledgments
This research was supported by the Ministry of Health and Welfare of the Republic of Korea (Grant Number: HI18C0378) through the Korea Health Industry Development Institute.
We would like to thank Editage (www.editage.co.kr) for English language editing.
Footnotes
No potential conflict of interest relevant to this article was reported.
Ethical approval: This study was approved by the Institutional Review Board Committee of Ewha Womans University Mokdong Hospital (certificate No. EUMC 2014-06-010).
Patient consent: The patients provided written informed consent for the publication and the use of their images.
Supplementary materials
Supplementary Tables associated with this article can be found online at https://doi.org/10.5468/ogs.19131.
Cervicovaginal fluid cytokine levels in preterm labor patients in the study group and control group
Receiver operating characteristic curve analysis in preterm labor patients
Cervicovaginal fluid cytokine levels in preterm premature rupture of membranes patients in the study group and control group
References
- 1.Heng YJ, Liong S, Permezel M, Rice GE, Di Quinzio MK, Georgiou HM. Human cervicovaginal fluid biomarkers to predict term and preterm labor. Front Physiol. 2015;6:151. doi: 10.3389/fphys.2015.00151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Yoo JY, You YA, Kwon EJ, Park MH, Shim S, Kim YJ. Differential expression and methylation of integrin subunit alpha 11 and thrombospondin in the amnion of preterm birth. Obstet Gynecol Sci. 2018;61:565–74. doi: 10.5468/ogs.2018.61.5.565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Chan RL. Biochemical markers of spontaneous preterm birth in asymptomatic women. BioMed Res Int. 2014;2014:164081. doi: 10.1155/2014/164081. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Amabebe E, Chapman DR, Stern VL, Stafford G, Anumba DO. Mid-gestational changes in cervicovaginal fluid cytokine levels in asymptomatic pregnant women are predictive markers of inflammation-associated spontaneous preterm birth. J Reprod Immunol. 2018;126:1–10. doi: 10.1016/j.jri.2018.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Jefferson KK. The bacterial etiology of preterm birth. Adv Appl Microbiol. 2012;80:1–22. doi: 10.1016/B978-0-12-394381-1.00001-5. [DOI] [PubMed] [Google Scholar]
- 6.Dekker GA, Lee SY, North RA, McCowan LM, Simpson NA, Roberts CT. Risk factors for preterm birth in an international prospective cohort of nulliparous women. PLoS One. 2012;7:e39154. doi: 10.1371/journal.pone.0039154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Son KA, Kim M, Kim YM, Kim SH, Choi SJ, Oh SY, et al. Prevalence of vaginal microorganisms among pregnant women according to trimester and association with preterm birth. Obstet Gynecol Sci. 2018;61:38–47. doi: 10.5468/ogs.2018.61.1.38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kim YJ, Lee BE, Park HS, Kang JG, Kim JO, Ha EH. Risk factors for preterm birth in Korea: a multicenter prospective study. Gynecol Obstet Invest. 2005;60:206–12. doi: 10.1159/000087207. [DOI] [PubMed] [Google Scholar]
- 9.Baer RJ, McLemore MR, Adler N, Oltman SP, Chambers BD, Kuppermann M, et al. Pre-pregnancy or first-trimester risk scoring to identify women at high risk of preterm birth. Eur J Obstet Gynecol Reprod Biol. 2018;231:235–40. doi: 10.1016/j.ejogrb.2018.11.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Conde-Agudelo A, Papageorghiou AT, Kennedy SH, Villar J. Novel biomarkers for the prediction of the spontaneous preterm birth phenotype: a systematic review and meta-analysis. BJOG. 2011;118:1042–54. doi: 10.1111/j.1471-0528.2011.02923.x. [DOI] [PubMed] [Google Scholar]
- 11.Paternoster DM, Muresan D, Vitulo A, Serena A, Battagliarin G, Dell’avanzo M, et al. Cervical phIGFBP-1 in the evaluation of the risk of preterm delivery. Acta Obstet Gynecol Scand. 2007;86:151–5. doi: 10.1080/00016340600935730. [DOI] [PubMed] [Google Scholar]
- 12.Liong S, Di Quinzio MK, Fleming G, Permezel M, Rice GE, Georgiou HM. New biomarkers for the prediction of spontaneous preterm labour in symptomatic pregnant women: a comparison with fetal fibronectin. BJOG. 2015;122:370–9. doi: 10.1111/1471-0528.12993. [DOI] [PubMed] [Google Scholar]
- 13.Son M, Miller ES. Predicting preterm birth: cervical length and fetal fibronectin. Semin Perinatol. 2017;41:445–51. doi: 10.1053/j.semperi.2017.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Chandiramani M, Seed PT, Orsi NM, Ekbote UV, Bennett PR, Shennan AH, et al. Limited relationship between cervico-vaginal fluid cytokine profiles and cervical shortening in women at high risk of spontaneous preterm birth. PLoS One. 2012;7:e52412. doi: 10.1371/journal.pone.0052412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.DeFranco EA, Lewis DF, Odibo AO. Improving the screening accuracy for preterm labor: is the combination of fetal fibronectin and cervical length in symptomatic patients a useful predictor of preterm birth? A systematic review. Am J Obstet Gynecol. 2013;208:233.e1–6. doi: 10.1016/j.ajog.2012.12.015. [DOI] [PubMed] [Google Scholar]
- 16.Son GH, You YA, Kwon EJ, Lee KY, Kim YJ. Comparative analysis of midtrimester amniotic fluid cytokine levels to predict spontaneous very pre-term birth in patients with cervical insufficiency. Am J Reprod Immunol. 2016;75:155–61. doi: 10.1111/aji.12451. [DOI] [PubMed] [Google Scholar]
- 17.Gulati S, Agrawal S, Raghunandan C, Bhattacharya J, Saili A, Agarwal S, et al. Maternal serum interleukin-6 and its association with clinicopathological infectious morbidity in preterm premature rupture of membranes: a prospective cohort study. J Matern Fetal Neonatal Med. 2012;25:1428–32. doi: 10.3109/14767058.2011.638952. [DOI] [PubMed] [Google Scholar]
- 18.Curry AE, Vogel I, Skogstrand K, Drews C, Schendel DE, Flanders WD, et al. Maternal plasma cytokines in early- and mid-gestation of normal human pregnancy and their association with maternal factors. J Reprod Immunol. 2008;77:152–60. doi: 10.1016/j.jri.2007.06.051. [DOI] [PubMed] [Google Scholar]
- 19.Chaemsaithong P, Romero R, Docheva N, Chaiyasit N, Bhatti G, Pacora P, et al. Comparison of rapid MMP-8 and interleukin-6 point-of-care tests to identify intraamniotic inflammation/infection and impending preterm delivery in patients with preterm labor and intact membranes. J Matern Fetal Neonatal Med. 2018;31:228–44. doi: 10.1080/14767058.2017.1281904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Musilova I, Bestvina T, Hudeckova M, Michalec I, Cobo T, Jacobsson B, et al. Vaginal fluid IL-6 concentrations as a point-of-care test is of value in women with preterm PROM. Am J Obstet Gynecol; 2016. Forthcoming. [DOI] [PubMed] [Google Scholar]
- 21.Lee SM, Park KH, Jung EY, Kook SY, Park H, Jeon SJ. Inflammatory proteins in maternal plasma, cervicovaginal and amniotic fluids as predictors of intra-amniotic infection in preterm premature rupture of membranes. PLoS One. 2018;13:e0200311. doi: 10.1371/journal.pone.0200311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Coleman MA, Keelan JA, McCowan LM, Townend KM, Mitchell MD. Predicting preterm delivery: comparison of cervicovaginal interleukin (IL)-1beta, IL-6 and IL-8 with fetal fibronectin and cervical dilatation. Eur J Obstet Gynecol Reprod Biol. 2001;95:154–8. doi: 10.1016/s0301-2115(00)00450-4. [DOI] [PubMed] [Google Scholar]
- 23.Gibbs RS, Blanco JD, St Clair PJ, Castaneda YS. Quantitative bacteriology of amniotic fluid from women with clinical intraamniotic infection at term. J Infect Dis. 1982;145:1–8. doi: 10.1093/infdis/145.1.1. [DOI] [PubMed] [Google Scholar]
- 24.Leitich H, Kaider A. Fetal fibronectin--how useful is it in the prediction of preterm birth? BJOG. 2003;110 Suppl 20:66–70. [PubMed] [Google Scholar]
- 25.Goldenberg RL, Iams JD, Mercer BM, Meis PJ, Moawad A, Das A, et al. The Preterm Prediction Study: toward a multiple-marker test for spontaneous preterm birth. Am J Obstet Gynecol. 2001;185:643–51. doi: 10.1067/mob.2001.116752. [DOI] [PubMed] [Google Scholar]
- 26.Heng YJ, Di Quinzio MK, Permezel M, Rice GE, Georgiou HM. Interleukin-1 receptor antagonist in human cervicovaginal fluid in term pregnancy and labor. Am J Obstet Gynecol. 2008;199:656.e1–7. doi: 10.1016/j.ajog.2008.06.011. [DOI] [PubMed] [Google Scholar]
- 27.Kekki M, Kurki T, Kärkkäinen T, Hiilesmaa V, Paavonen J, Rutanen EM. Insulin-like growth factor-binding protein-1 in cervical secretion as a predictor of preterm delivery. Acta Obstet Gynecol Scand. 2001;80:546–51. [PubMed] [Google Scholar]
- 28.Lockwood CJ, Senyei AE, Dische MR, Casal D, Shah KD, Thung SN, et al. Fetal fibronectin in cervical and vaginal secretions as a predictor of preterm delivery. N Engl J Med. 1991;325:669–74. doi: 10.1056/NEJM199109053251001. [DOI] [PubMed] [Google Scholar]
- 29.Rizzo G, Capponi A, Rinaldo D, Tedeschi D, Arduini D, Romanini C. Interleukin-6 concentrations in cervical secretions identify microbial invasion of the amniotic cavity in patients with preterm labor and intact membranes. Am J Obstet Gynecol. 1996;175:812–7. doi: 10.1016/s0002-9378(96)80004-4. [DOI] [PubMed] [Google Scholar]
- 30.Jacobsson B, Holst RM, Mattsby-Baltzer I, Nikolaitchouk N, Wennerholm UB, Hagberg H. Interleukin-18 in cervical mucus and amniotic fluid: relationship to microbial invasion of the amniotic fluid, intra-amniotic inflammation and preterm delivery. BJOG. 2003;110:598–603. [PubMed] [Google Scholar]
- 31.Tanaka Y, Narahara H, Takai N, Yoshimatsu J, Anai T, Miyakawa I. Interleukin-1β and interleukin-8 in cervicovaginal fluid during pregnancy. Am J Obstet Gynecol. 1998;179:644–9. doi: 10.1016/s0002-9378(98)70058-4. [DOI] [PubMed] [Google Scholar]
- 32.Sanchez-Ramos L, Mentel C, Bertholf R, Kaunitz AM, Delke I, Loge C. Human chorionic gonadotropin in cervicovaginal secretions as a predictor of preterm delivery. Int J Gynaecol Obstet. 2003;83:151–7. doi: 10.1016/s0020-7292(03)00273-x. [DOI] [PubMed] [Google Scholar]
- 33.Kacerovsky M, Musilova I, Jacobsson B, Drahosova M, Hornychova H, Janku P, et al. Cervical fluid IL-6 and IL-8 levels in pregnancies complicated by preterm prelabor rupture of membranes. J Matern Fetal Neonatal Med. 2015;28:134–40. doi: 10.3109/14767058.2014.908179. [DOI] [PubMed] [Google Scholar]
- 34.Ashford K, Chavan NR, Wiggins AT, Sayre MM, McCubbin A, Critchfield AS, et al. Comparison of serum and cervical cytokine levels throughout pregnancy between preterm and term births. AJP Rep. 2018;8 doi: 10.1055/s-0038-1656534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kiefer DG, Peltier MR, Keeler SM, Rust O, Ananth CV, Vintzileos AM, et al. Efficacy of midtrimester short cervix interventions is conditional on intraamniotic inflammation. Am J Obstet Gynecol. 2016;214:276.e1–6. doi: 10.1016/j.ajog.2015.09.006. [DOI] [PubMed] [Google Scholar]
- 36.Romero R, Gomez R, Galasso M, Munoz H, Acosta L, Yoon BH, et al. Macrophage inflammatory protein-1 alpha in term and preterm parturition: effect of microbial invasion of the amniotic cavity. Am J Reprod Immunol. 1994;32:108–13. doi: 10.1111/j.1600-0897.1994.tb01101.x. [DOI] [PubMed] [Google Scholar]
- 37.Lee SM, Park KH, Jung EY, Cho SH, Ryu A. Prediction of spontaneous preterm birth in women with cervical insufficiency: comprehensive analysis of multiple proteins in amniotic fluid. J Obstet Gynaecol Res. 2016;42:776–83. doi: 10.1111/jog.12976. [DOI] [PubMed] [Google Scholar]
- 38.Herrera-Muñoz A, Fernández-Alonso AM, Fischer-Suárez N, Chedraui P, Pérez-López FR. Maternal serum cytokine levels in pregnancies complicated with threatened preterm labour. Gynecol Endocrinol. 2017;33:408–12. doi: 10.1080/09513590.2017.1284786. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Cervicovaginal fluid cytokine levels in preterm labor patients in the study group and control group
Receiver operating characteristic curve analysis in preterm labor patients
Cervicovaginal fluid cytokine levels in preterm premature rupture of membranes patients in the study group and control group