

Abstract
Objective
The aim of this systematic review and meta-analysis study was to determine the pooled estimate of the effect of antenatal magnesium sulfate (MgSO4) on intraventricular hemorrhage (IVH) in premature infants.
Methods
Two review authors independently searched all randomized clinical trials from international databases, including Medline (PubMed), Web of Sciences, Scopus, Cochrane Central Register of Controlled Trials (CENTRAL), and Research Registers of ongoing trials (ClinicalTrials.gov), from January 1989 to August 2017. Two independent review authors were responsible for data collection. After extracting the necessary information from the evaluated articles, metaanalysis of the data was performed using Stata version 14. Also, sources of heterogeneity among studies were determined by Meta regression.
Results
In this study, among 126 articles that were extracted from primary studies, 7 papers that evaluated the effect of MgSO4 on IVH were eligible for inclusion in the meta-analysis. The results of the meta-analysis showed that pooled relative risk (95% confidence interval [CI]) was 0.80 (95% CI, 0.63 to 1.03) for the effect of MgSO4 on IVH.
Conclusion
Results of this study showed that although MgSO4 had a protective effect on IVH in premature infants, this effect was not statistically significant. Further studies are needed to determine the best dosage, timing, and gestational age to achieve the optimum effect of MgSO4 on IVH.
Systematic Review Registration
International Prospective Register of Systematic Reviews (PROSPERO) Identifier: CRD42019119610
Keywords: Magnesium Sulfate, IVH, Premature infants, Systematic review, Meta-analysis
Introduction
Intraventricular hemorrhage (IVH) consists of bleeding inside or around the ventricles, which are the areas in the brain that contain the cerebral spinal fluid. IVH is a common problem in premature infants, especially in very low birth weight infants (<1,500 g) [1]. Ancel et al. [2] reported that 56 children with normal ultrasound findings accounted for 35% of children with cerebral palsy. In the same study, children with isolated IVH, and those with white matter disease, accounted for 14% and 52% of cerebral palsy cases, respectively [2].
Many factors are involved in the incidence of IVH, the most important of which include respiratory distress, hypoxiainduced damage, ischemia, high or low blood pressure, increased venous blood pressure, pneumothorax, and hypovolemia [3]. Symptoms of IVH are nonspecific and differ according to the severity of the disease [4]. In severe and acute IVH cases, symptoms such as pale skin, acute anemia, respiratory dysfunction, and fontanel bulge can occur. Currently, cerebral ultrasound or magnetic resonance imaging is performed in the first 3 days of life and is repeated two or three times in suspected cases of IVH to assess its severity [5,6]. Bleeding from the germinal matrix around the brain ventricle based on IVH extension in brain ultrasonography is divided into four categories: grade 1 for limited bleeding to germinal matrix; grade 2 for IVH; grade 3 for bleeding with ventricular extension; and grade 4 for extension of bleeding to brain parenchyma. Grades 1 and 2 are automatically removed without any consequence; however, grades 3 and 4 are associated with severe consequences [7]. Given that preterm birth is a major cause of IVH, various methods have been proposed for its prevention [8]. Tocolytic treatments are among the conventional methods; however, there is disagreement about the best treatment method [9]. Magnesium sulfate, prostaglandin inhibitors, calcium channel blockers, and nitric oxide releasing drugs are some of the therapeutic methods in which positive effects have been reported [10,11]. Currently, magnesium sulfate is one of the most common methods used to prevent preterm delivery. Various studies have suggested that magnesium sulfate reduces the risk of brain injury in preterm infants [12-14]. In contrast, there are some studies that do not confirm the effect of magnesium sulphate on risk reduction of IVH, cerebral palsy, and perinatal mortality [15-17]. Therefore, given the controversy in the results of various studies in this field, the aim of this systematic review and meta-analysis study was to determine the effect of antenatal magnesium sulfate (MgSO4) on IVH in premature infants.
Materials and methods
This systematic review was performed according to the Preferred Reporting Items for Systematic Reviews and MetaAnalyses (PRISMA) [18]. The protocol of this study was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42019119610).
1. Search strategy
Two review authors (YM and KM) independently searched all randomized clinical trials from international databases, including Medline (PubMed), Web of Sciences, Scopus, Cochrane Central Register of Controlled Trials (CENTRAL), and Research Registers of ongoing trials (ClinicalTrials.gov), from January 1989 to August 2017. The search was performed based on 11 English phrases and keywords, including “Magnesium Sulfate (MgSO4)”, “Heptahydrate Magnesium Sulfate”, “Tocolysis Preterm”, “Newborn”, “Newborn Infant”, “Newborn Infants”, “Fetal”, “Neonatal”, “Preterm Prelabor Rupture of Membranes (PPROM)”, “Prelabor Rupture of Membranes (PROM)”, “Preterm Birth”, “Premature Births”, “Intraventricular hemorrhage (IVH)”, “Cerebral Intraventricular Hemorrhages”, “Neuroprotection”, “Neuronal Protection”, “Dystonic-Rigid Cerebral Palsy”, “Mixed Cerebral Palsy”, “Rolandic Type Cerebral Palsy”, “Congenital Cerebral Palsy”, “Spastic Diplegia”, “Monoplegic Cerebral Palsy”, “Athetoid Cerebral Palsy”, “Dyskinetic Cerebral Palsy”, “Atonic Cerebral Palsy”, “Hypotonic Cerebral Palsy”, “Diplegic Infantile Cerebral Palsy”, “Spastic Cerebral Palsy”, and “Cerebral Palsy (CP)”. We exported the search results to the End-Note software version 9. The duplicated primary studies were deleted. The primary search results were reviewed based on the inclusion and exclusion criteria, and some of the articles were eliminated after reviewing their title and abstract. Subsequently, we investigated the search results and excluded some studies after full text review (Fig. 1).
Fig. 1.
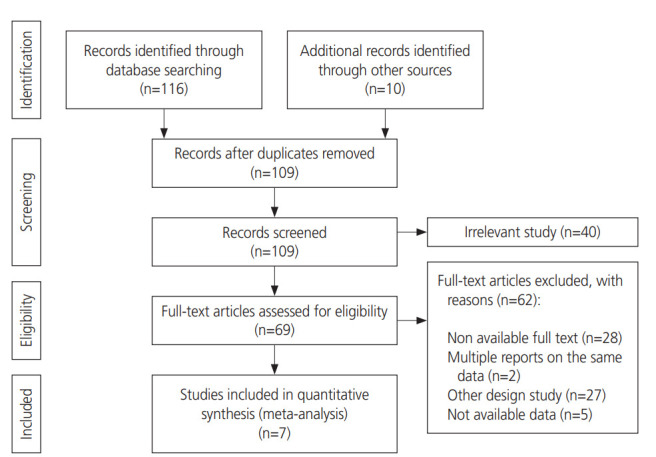
Flow diagram of the literature search and study selection.
2. Inclusion and exclusion criteria
We included all randomized controlled trials (RCTs) which assessed or reported the effect of antenatal magnesium sulfate on IVH in premature infants. Therefore, only articles in which the primary outcome was IVH in premature infants, and gestational age between 24 to 37 weeks, were included in this review. Also, we considered primary studies in which IVH was diagnosed after birth by cranial ultrasound. We excluded duplicate citations, non- peer reviewed, cross-sectional studies, case control studies, review papers, book chapters, conference proceedings, and studies with other primary outcomes.
3. Data extraction and quality assessment
After assessment of the titles, abstracts, and texts, the full text of each selected article was retrieved for detailed analysis. Data were extracted using a data collection form with the name of the first author, date of publication, study title, study design, geographical setting, sample size, type of comorbidities (IVH-related), and main outcome. The entire process, from systematic search to final data extraction, was performed independently by two research experts (Kappa statistic for agreement for quality assessment; 0.75). Two reviewers (KM and ZN) independently evaluated the articles. Any disagreement was assessed by both reviewers, and if a consensus was not reached, a third author (YM) would evaluate the study. Moreover, quality assessment (using CONSORT) was determined by the same data extractor for each study. Risk of bias in the included studies was assessed using the Cochrane Risk of Bias Tool [19]. The bias domains that were assessed included sequence generation, allocation concealment, blinding, outcome data, and outcome reporting. Trials were rated as high risk of bias when the methodological flaw was likely to have affected the true outcome, low risk of bias if the flaw was deemed inconsequential to the true outcome, and unclear risk of bias when insufficient information was provided to permit judgment.
4. Statistical analysis
In this meta-analysis, we used two measures of association measurement: odds ratio (OR) and relative risk (RR). When the frequency of outcome (IVH in premature infants) is relatively low, OR and risk ratio provide similar estimates of RR [20]. We used logarithm and standard error logarithm RR for meta-analysis. The pooled RR with 95% confidence interval (CI) was derived through the DerSimonian and Laird method using random and fixed models [21]. Finally, for the estimated RR, we used the random effects model, since the test for heterogeneity was statistically significant in some analyses. In the present study, we used Cochran’s Q test and I2 statistic, with a significance level set at P-value <0.10 for evaluating statistical heterogeneity between the studies [22]. An I2 <50%, I2 ≥50%, and I2 ≥75% were considered to be evidence of “moderate”, “substantial”, and “considerable” heterogeneity, respectively [19]. In addition, to assess the source of heterogeneity between the studies, the authors conducted a meta regression and subgroup analysis. Publication bias was assessed by funnel plot, Egger and Begg’s test, with a significance level set at P-value<0.10 [23]. The statistical analysis was performed using Stata 14.0 (Stata Corp, College Station, TX, USA) and Review Manager (RevMan), version 5.2 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark).
Results
At the end of the database search, we obtained 126 articles. Among these articles, 17 were removed due to duplication. After reviewing the titles and abstracts of the articles, 40 were excluded due to non-relevance, resulting in 69 articles. After reviewing the full text of these 69 articles, only 7 were eligible for entry in the meta-analysis (Fig. 1).
The total sample size of the included studies in meta-analysis was 8,578 cases [10,24-29], in which 4 studies reported RR with a total sample size of 4,135 [10,26,28,29], and 3 studies reported OR with a total sample size of 4,443 [24,25,27] (Table 1). Table 1 shows the characteristics and results of the studies included in the meta-analysis.
Table 1.
Characteristics of studies included by principal outcome evaluated
| Authors | Date of publication | Study name | Study design | Geographical setting | Sample size | Comorbidities (IVH) | Age of Preg- nancy (weeks) | Cases | Doses of intervention | RR (95% Cl) | OR (95% Cl) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Hirtz et al. [24] | 2015 | Antenatal magnesium and cerebral palsy in preterm infants | RCT | US | Intervention group: 953 | Cranial ultrasounds | 24–37 | PPROM/PTL | 6 g loading and 2 g/hr infusion | - | 0.57 (0.37–0.87) |
| Placebo group: 1,026 | |||||||||||
| Mirzamoradi et al. [27] | 2014 | Does magnesium sulfate delay the active phase of labor in women with premature rupture of membranes | RCT | Iran | Intervention group: 46 | Cranial ultrasounds | <34 | PPROM | 4 g loading and 2 g/hr infusion | - | 3.2 (0.4-4.8) |
| Placebo group: 46 | |||||||||||
| Crowther et al. [10] | 2003 | Effect of magnesium sulfate given for neuroprotection before preterm birth | RCT | Australia | Intervention group: 535 | Cranial ultrasounds | <30 | Planned and expected within 24 hr | 4 g loading and 2 g/hr infusion | 1.10 (0.90–1.33) | - |
| Placebo group: 527 | |||||||||||
| Mittendorf et al. [30] | 2002 | Association between maternal serum ionized magnesium levels at delivery and neonatal intraventricular hemorrhage | RCT | US | Intervention group: 72 | Cranial ultrasounds | <34 | PTL | Before active phase (4 g loading and 2 g/hr infusion) | 1.11 (0.53–2.34) | - |
| Placebo group: 72 | After active phase (4 g single dose) | ||||||||||
| Horton et al. [25] | 2015 | The effect of magnesium sulfate administration for neuroprotection on latency in women with preterm premature rupture of membranes | RCT | US | Intervention group: 621 | Cranial ultrasounds | 24–32 | PPROM | 6 g loading and 2 g/hr infusion | - | 0.31 (0.10–0.96) |
| Placebo group: 638 | |||||||||||
| Rouse et al. [29] | 2008 | Magnesium sulfate for the prevention of cerebral palsy | RCT | US | Intervention group: 1,096 | Cranial ultrasounds | 24–31 | PPROM/PTL | 6 g loading and 2 g/hr infusion | 0.91 (0.78–1.08) | - |
| Placebo group: 1,145 | |||||||||||
| Marret et al. [26] | 2006 | Effect of magnesium sulphate on mortality and neurologic morbidity of the verypreterm newborn (of less than 33 weeks) with twoyear neurological outcome: results of the prospective PREMAG trial | RCT | French | Intervention group: 286 | Cranial ultrasounds | <33 | Planned and expected under 30 hr | 4 g single dose | 0.83 (0.62–1.09) | - |
| Placebo group: 278 |
IVH, intraventricular hemorrhage; RR, relative risk; CI, confidence interval; OR, odds ratio; RCT, randomized controlled trial; PPROM, Preterm Prelabor Rupture of Membranes; PTL, preterm labor.
As previously described in the methodology section, when the frequency of outcome (IVH in premature infants) is relatively low, OR and risk ratio provide similar estimates of RR [20]. Therefore, the OR and RR were combined, and the pooled RR was extracted with 95% CI.
1. Quality assessment and risk of bias
The quality assessment of the studies was performed by CONSORT checklist. Table 2 shows quality assessment of included studies according to the CONSORT checklist. As can be seen, the quality of all studies was high based on this checklist, except the study by Mittendorf et al. [30] (Table 2). The risk of bias was also performed for the articles included in the analysis. We considered the probability of the risk of bias according to sequence generation, allocation sequence concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and other potential sources of bias. The results showed that most studies were low risk in terms of random sequence generation (selection bias) and allocation sequence concealment (selection bias). Additional information is provided in Fig. 2. Also, the study by Crowther et al. [10] presented the lowest risk among the studies Fig. 3. The studies did not provide adequate description of their methods, including randomization and blinding, which made it difficult for the researchers to make judgments about the risk of bias among the included studies. Also, outcome data was incomplete in all the included studies, so the risk of selective reporting was high or unclear (Fig. 2).
Table 2.
Quality assessment of included studies according to the CONSORT checklist
| Item No. | Hirtz et al. [24] | Mirzamoradi et al. [27] | Crowther et al. [10] | Mittendorf et al. [30] | Horton et al. [25] | Rouse et al. [29] | Marret et al. [26] |
|---|---|---|---|---|---|---|---|
| 1a | No | Yes | Yes | No | No | Yes | Yes |
| 1b | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 2a | Yes | Yes | Yes | No | Yes | Yes | No |
| 2b | Yes | Yes | No | No | Yes | No | Yes |
| 3a | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 3b | Yes | Yes | Yes | No | Yes | Yes | Yes |
| 4a | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 4b | Yes | Yes | No | Yes | Yes | Yes | Yes |
| 5 | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 6a | Yes | Yes | Yes | Yes | Yes | No | Yes |
| 6b | No | No | No | No | No | No | No |
| 7a | No | Yes | No | Yes | No | Yes | Yes |
| 7b | No | No | Yes | No | No | Yes | Yes |
| 8a | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 8b | No | No | Yes | No | No | No | Yes |
| 9 | No | No | Yes | No | No | No | Yes |
| 10 | No | No | Yes | No | No | No | Yes |
| 11a | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 11b | No | No | No | No | No | Yes | Yes |
| 12a | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 12b | No | No | No | No | No | Yes | No |
| 13a | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 13b | Yes | Yes | No | No | No | No | No |
| 14a | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 14b | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 15 | No | Yes | Yes | Yes | Yes | Yes | Yes |
| 16 | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 17a | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 17b | No | No | No | No | No | No | No |
| 18 | Yes | Yes | No | Yes | No | No | No |
| 19 | No | No | Yes | No | No | No | No |
| 20 | Yes | No | Yes | Yes | Yes | Yes | No |
| 21 | No | No | No | No | No | No | No |
| 22 | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 23 | Yes | No | No | No | No | No | Yes |
| 24 | No | No | No | No | No | Yes | No |
| 25 | No | No | No | No | No | No | No |
| Total | 22 | 23 | 24 | 19 | 20 | 24 | 26 |
Fig. 2.
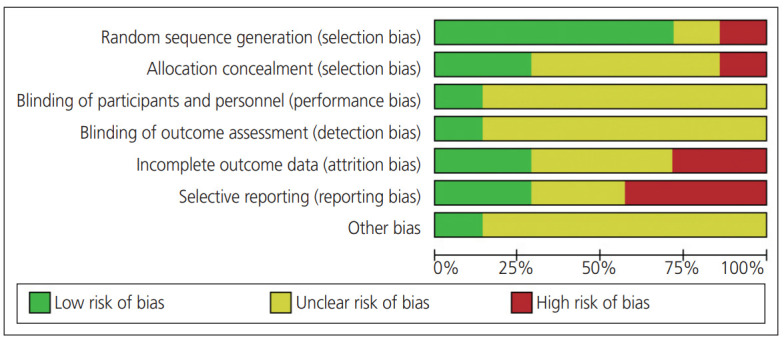
Risk of bias summary: review authors’ judgments about each risk of bias item for each included study.
Fig. 3.
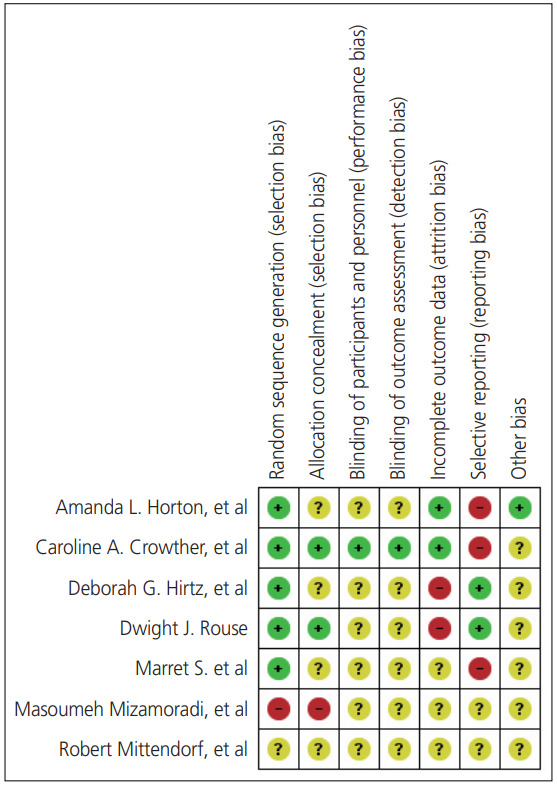
Risk of bias summary (review authors’ judgments about each risk of bias item for each included study).
2. Meta-analysis
The results showed that pooled RR was 0.80 (95% CI, 0.63 to 1.03; I2=63.0%; P=0.013), although MgSO4 had a protective effect on IVH; however, this effect was not statistically significant (Fig. 4). The results also indicated the heterogeneity of the studies; however, bias in the publication of the results was not statistically significant (χ2=3.25; P=0.352; I2=8.2%); however, the CI of the test includes zero (Begg’s test: Z=0.34; P=0.978) (Egger’s test: t=0.10; P=0.930 95% CI, −0.743 to 0.779).
Fig. 4.
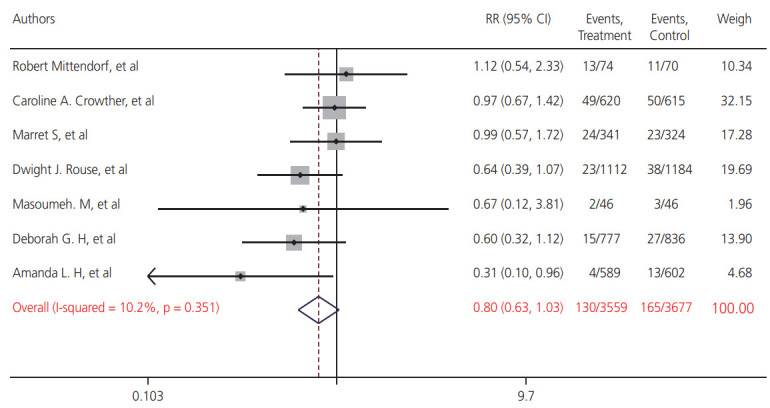
Frost plot for relative risk (RR) and 95% confidence interval (CI) of magnesium sulfate (MgSO4) on intraventricular hemorrhage (IVH).
3. Subgroup analysis
Table 3 shows subgroup analysis by gestational age and MgSO4. The RR for 6 g loading and 2 g/hr regimen of MgSO4 on IVH in premature infants was 0.84 (95% CI, 0.72 to 0.98; I2=42.5%; P=0.345). Also, RR for 4 g loading and 2 g/hr infusion MgSO4 was 1.13 (95% CI, 0.94 to 1.36; I2=27.8%; P=0.250); however, 4-g single dose MgSO4 had a protective effect on IVH in premature infants (RR, 0.86; 95% CI, 0.66 to 1.12; I2=0.0%; P=0.473) (Table 3).
Table 3.
Summary relative risk (RR) Estimates (95% confidence intervals [CIs]) for randomized controlled trial studies conducted on the effect of antenatal magnesium sulfate (MgSO4) on intraventricular hemorrhage in premature infants by gestational age, and MgSO4 regimen
| Subgroup | Number of studies (Sample size) | Summery RR (95% CI) | Between studies |
Between subgroups |
||||
|---|---|---|---|---|---|---|---|---|
| I2 | P heterogeneity | Q | Q | P heterogeneity | ||||
| MgSO4 regimen | ||||||||
| 6 g loading and 2 g/h infusion | 3 (6,592)a) | 0.84 (0.72–0.98) | 42.5% | 0.345 | 7.07 | 6.07 | 0.048 | |
| 4 g loading and 2 g/h infusion | 3 (1,298)b) | 1.13 (0.94–1.36) | 27.8% | 0.250 | 2.77 | |||
| 4 g single dose | 2 (832)c) | 0.86 (0.66–1.12) | 0.0% | 0.473 | 0.51 | |||
| Gestational age (wk) | ||||||||
| 24 to 37 | 4 (7,654) | 0.93 (0.83–1.05) | 74.1% | 0.009 | 11.57 | 16.21 | 0.013 | |
| <34 | 3 (1,842) | 0.91 (0.70–1.18) | 56.7% | 0.099 | 4.62 | |||
The results of the subgroup analysis based on gestational age showed that the effect of MgSO4 on IVH in premature infants between 24–37 weeks and <34 weeks were 0.93 (95% CI, 0.83 to 1.05; I2=74.1%; P=0.009) and 0.92 (95% CI, 0.70 to 1.18; I2=56.7%; P=0.099), respectively (Table 3).
4. Meta regression
The results of the meta regression analysis, used to explore the sources of interstudy heterogeneity according to gestational age, indicated that the effect of MgSO4 on risk of IVH is unrelated to gestational age (Q test=2.43, df=2, P-value=0.467).
Discussion
IVH is one of the most common complications in premature infants, and can cause long-term disability, cerebral palsy, mental retardation, seizures, behavioral and cognitive impairment, and death [31,32]. Studies have shown that the immature antioxidant system of the preterm infant can cause damage to the endothelial cells and alter brain hemostasis, can increase the susceptibility to reactive oxygen species, and, finally, increase the risk for IVH [33-35], Furthermore, studies have shown that approximately one third of cerebral palsy cases and IVH occur in premature infants [36]. Therefore, the present systematic review and meta-analysis study was designed to investigate the effect of antenatal MgSO4 on IVH in premature infants.
The results of our study indicate that although MgSO4 had a protective effect on IVH, this effect is not statistically significant (pooled RR, 0.80; 95% CI, 0.63 to 1.03). Although studies have shown MgSO4 being used for the first time in obstetric practice, there is a controversy about its effect on the outcomes of premature infants [37,38]. Indeed, some studies have concluded that MgSO4 is harmful due to increased risk of death and neurological problems for neonates [39-41]. In contrast, other studies have shown that MgSO4 has a protective and beneficial effect on low birth weight infants [42-44]. For example, a study by Nelson et al. showed that the use of MgSO4 can reduce the IVH incidence (OR, 0.14; 95% CI, 0.05 to 0.51) [42]. In a systematic review study conducted by Doyle et al. [45] with the aim of studying the effect of antenatal MgSO4 on neurologic outcomes in preterm infants, the results showed that use of MgSO4 dramatically reduced the risk of cerebral palsy in the children of women at risk of preterm birth (RR, 0.69; 95% CI, 0.54 to 0.87); also, a significant decrease was observed in the rate of substantial gross motor dysfunction (RR, 0.61; 95% CI, 0.44 to 0.85) [45]. In general, there are many reports that show that MgSO4 increases the antioxidant properties of the brain, protects the brain cells against hypoxia and apoptosis, and normalizes platelet aggregation [46-50]. In other words, the MgSO4 is a tocolytic method for preventing preterm labor. Epidemiological studies have shown that MgSO4 in mothers leads to myocardial stability and blood supply in placenta and fetal brain, as well as reduction of the ischemic region and antioxidant effects, with decreased platelet adhesion in the fetus [51-53].
In contrast, some studies concluded that use of MgSO4 had no effect, or had a minor and insignificant effect, on premature infants [16,17].The large RCTs that were conducted using different doses of MgSO4 have shown an insignificant reduction in the combined death, cerebral palsy, or gross motor dysfunction among premature infants [10,26,29]. For example, the results of a clinical trial study by Marret et al. [26] showed that although MgSO4 has a protective effect on IVH, this effect was not statistically significant (OR, 0.83; 95% CI, 0.55 to 1.32). Meanwhile, the study by Crowther et al. [10] showed that magnesium sulfate had a protective effect on the risk of IVH; however, this effect was not statistically significant (OR, 0.83; 95% CI, 0.64 to 1.32). Also, a systematic review by Doyle et al. [45] that studied the effect of antenatal magnesium sulfate on neurologic outcome in preterm infants indicated that antenatal magnesium sulfate therapy has no statistically significant effect on pediatric mortality, or on other neurologic impairments or disabilities, in the early years of life of children (RR, 1.01; 95% CI, 0.82 to 1.23). A study by Petrova and Mehta [54] in 2012 revealed that there was no significant association between the use of magnesium sulfate, IVH, and parenchyma injury. Evidently, the results of these studies are consistent with our results. However, the results among various studies in this field are inconsistent, which may be due to differences in study design, study population or sample size, gestational age, follow-up patterns, and/or different doses of the MgSO4.
There several limitations of this study that should be considered when interpreting the results. First, potential publication bias may exist in the observed results, since only some established electronic literature databases were searched. Second, language bias may threaten the results, given that only published articles in English were reviewed. Third, due to lack of detailed information, the quality assessment of the eligible studies may have been influenced by personal judgment. Finally, the last limitation is heterogeneity among the studies. Indeed, the included studies were not directly comparable with each other due to different methods for outcome assessment and experimental variation.
In conclusion, the results of this review showed that although MgSO4 had a protective effect on IVH in neonates, this effect is not statistically significant. However, based on the heterogeneity in study population, sample sizes, gestational age, magnesium sulfate dosage, and follow-up patterns among the included studies, further investigation is needed to evaluate the best dosage, timing and gestational age for the optimum effect of magnesium sulfate on IVH.
Acknowledgments
This study was financially supported by the Deputy of Research and Technology of Iran University of Medical Sciences, Tehran, Iran (Grant No. 13281).
Footnotes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Ethical approval The study is applicable to Institutional Review Board (IRB: IR.IUMS.REC.1397.830).
Patient consent There is no need for patient consent in this review article.
References
- 1.Delbos F, Bertrand G, Croisille L, Ansart-Pirenne H, Bierling P, Kaplan C. Fetal and neonatal alloimmune thrombocytopenia: predictive factors of intracranial hemorrhage. Transfusion. 2016;56:59–66. doi: 10.1111/trf.13274. [DOI] [PubMed] [Google Scholar]
- 2.Ancel PY, Livinec F, Larroque B, Marret S, Arnaud C, Pierrat V, et al. EPIPAGE Study Group Cerebral palsy among very preterm children in relation to gestational age and neonatal ultrasound abnormalities: the EPIPAGE cohort study. Pediatrics. 2006;117:828–35. doi: 10.1542/peds.2005-0091. [DOI] [PubMed] [Google Scholar]
- 3.Ibishi VA, Isjanovska RD. Prelabour rupture of membranes: mode of delivery and outcome. Open Access Maced J Med Sci. 2015;3:237–40. doi: 10.3889/oamjms.2015.037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Perlman JM, Goodman S, Kreusser KL, Volpe JJ. Reduction in intraventricular hemorrhage by elimination of fluctuating cerebral blood-flow velocity in preterm infants with respiratory distress syndrome. N Engl J Med. 1985;312:1353–7. doi: 10.1056/NEJM198505233122104. [DOI] [PubMed] [Google Scholar]
- 5.Ahmann PA, Lazzara A, Dykes FD, Brann AW, Jr, Schwartz JF. Intraventricular hemorrhage in the high-risk preterm infant: incidence and outcome. Ann Neurol. 1980;7:118–24. doi: 10.1002/ana.410070205. [DOI] [PubMed] [Google Scholar]
- 6.Bada HS, Korones SB, Perry EH, Arheart KL, Ray JD, Pourcyrous M, et al. Mean arterial blood pressure changes in premature infants and those at risk for intraventricular hemorrhage. J Pediatr. 1990;117:607–14. doi: 10.1016/s0022-3476(05)80700-0. [DOI] [PubMed] [Google Scholar]
- 7.Papile LA, Munsick-Bruno G, Schaefer A. Relationship of cerebral intraventricular hemorrhage and early childhood neurologic handicaps. J Pediatr. 1983;103:273–7. doi: 10.1016/s0022-3476(83)80366-7. [DOI] [PubMed] [Google Scholar]
- 8.Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr. 1978;92:529–34. doi: 10.1016/s0022-3476(78)80282-0. [DOI] [PubMed] [Google Scholar]
- 9.Stark MJ, Hodyl NA, Andersen CC. Effects of antenatal magnesium sulfate treatment for neonatal neuro-protection on cerebral oxygen kinetics. Pediatr Res. 2015;78:310–4. doi: 10.1038/pr.2015.96. [DOI] [PubMed] [Google Scholar]
- 10.Crowther CA, Hiller JE, Doyle LW, Haslam RR, Australasian Collaborative Trial of Magnesium Sulphate (ACTOMg SO4) Effect of magnesium sulfate given for neuroprotection before preterm birth: a randomized controlled trial. JAMA. 2003;290:2669–76. doi: 10.1001/jama.290.20.2669. [DOI] [PubMed] [Google Scholar]
- 11.Conde-Agudelo A, Romero R. Antenatal magnesium sulfate for the prevention of cerebral palsy in preterm infants less than 34 weeks' gestation: a systematic review and metaanalysis. Am J Obstet Gynecol. 2009;200:595–609. doi: 10.1016/j.ajog.2009.04.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Killion MM. Magnesium sulfate for neuroprotection. MCN Am J Matern Child Nurs. 2015;40:394. doi: 10.1097/NMC.0000000000000187. [DOI] [PubMed] [Google Scholar]
- 13.Bozkurt O, Eras Z, Canpolat FE, Oguz SS, Uras N, Dilmen U. Antenatal magnesium sulfate and neurodevelopmental outcome of preterm infants born to preeclamptic mothers. J Matern Fetal Neonatal Med. 2016;29:1101–4. doi: 10.3109/14767058.2015.1035641. [DOI] [PubMed] [Google Scholar]
- 14.Bano S, Chaudhary V, Garga UC, Yadav S, Singh SK. Chapter 1. Intracranial hemorrhage in the newborn. In: Chaudhary V, editor. Intracerebral Hemorrhage. London: IntechOpen Limited; 2014. [Google Scholar]
- 15.Kimberlin DF, Hauth JC, Goldenberg RL, Bottoms SF, Iams JD, Mercer B, et al. The effect of maternal magnesium sulfate treatment on neonatal morbidity in < or = 1000-gram infants. Am J Perinatol. 1998;15:635–41. doi: 10.1055/s-2007-994082. [DOI] [PubMed] [Google Scholar]
- 16.Paneth N, Jetton J, Pinto-Martin J, Susser M, The Neonatal Brain Hemorrhage Study Analysis Group Magnesium sulfate in labor and risk of neonatal brain lesions and cerebral palsy in low birth weight infants. Pediatrics. 1997;99:E1. doi: 10.1542/peds.99.5.e1. [DOI] [PubMed] [Google Scholar]
- 17.Grether JK, Hoogstrate J, Walsh-Greene E, Nelson KB. Magnesium sulfate for tocolysis and risk of spastic cerebral palsy in premature children born to women without preeclampsia. Am J Obstet Gynecol. 2000;183:717–25. doi: 10.1067/mob.2000.106581. [DOI] [PubMed] [Google Scholar]
- 18.Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6:e1000100. doi: 10.1371/journal.pmed.1000100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane handbook for systematic reviews of interventions. Version 5.0.1. London: The Cochrane Collaboration; 2008. [Google Scholar]
- 20.Greenland S. Quantitative methods in the review of epidemiologic literature. Epidemiol Rev. 1987;9:1–30. doi: 10.1093/oxfordjournals.epirev.a036298. [DOI] [PubMed] [Google Scholar]
- 21.DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–88. doi: 10.1016/0197-2456(86)90046-2. [DOI] [PubMed] [Google Scholar]
- 22.Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21:1539–58. doi: 10.1002/sim.1186. [DOI] [PubMed] [Google Scholar]
- 23.Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34. doi: 10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hirtz DG, Weiner SJ, Bulas D, DiPietro M, Seibert J, Rouse DJ, et al. Antenatal MAGNESIUM AND CEREBRAL PALSY IN PRETERM INFANTS. J Pediatr. 2015;167:834–839. doi: 10.1016/j.jpeds.2015.06.067. e3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Horton AL, Lai Y, Rouse DJ, Spong CY, Leveno KJ, Varner MW, et al. Effect of magnesium sulfate administration for neuroprotection on latency in women with preterm premature rupture of membranes. Am J Perinatol. 2015;32:387–92. doi: 10.1055/s-0034-1387930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Marret S, Marpeau L, Follet-Bouhamed C, Cambonie G, Astruc D, Delaporte B, et al. Effect of magnesium sulphate on mortality and neurologic morbidity of the very-preterm newborn (of less than 33 weeks) with two-year neurological outcome: results of the prospective PREMAG trial. Gynecol Obstet Fertil. 2008;36:278–88. doi: 10.1016/j.gyobfe.2008.01.012. [DOI] [PubMed] [Google Scholar]
- 27.Mirzamoradi M, Behnam M, Jahed T, Saleh-Gargari S, Bakhtiyari M. Does magnesium sulfate delay the active phase of labor in women with premature rupture of membranes? A randomized controlled trial. Taiwan J Obstet Gynecol. 2014;53:309–12. doi: 10.1016/j.tjog.2013.06.014. [DOI] [PubMed] [Google Scholar]
- 28.Mittendorf R, Dambrosia J, Dammann O, Pryde PG, Lee KS, Ben-Ami TE, et al. Association between maternal serum ionized magnesium levels at delivery and neonatal intraventricular hemorrhage. J Pediatr. 2002;140:540–6. doi: 10.1067/mpd.2002.123283. [DOI] [PubMed] [Google Scholar]
- 29.Rouse DJ, Hirtz DG, Thom E, Varner MW, Spong CY, Mercer BM, et al. A randomized, controlled trial of magnesium sulfate for the prevention of cerebral palsy. N Engl J Med. 2008;359:895–905. doi: 10.1056/NEJMoa0801187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Mittendorf R, Dammann O, Lee KS. Brain lesions in newborns exposed to high-dose magnesium sulfate during preterm labor. J Perinatol. 2006;26:57–63. doi: 10.1038/sj.jp.7211419. [DOI] [PubMed] [Google Scholar]
- 31.Pinto Cardoso G, Houivet E, Marchand-Martin L, Kayem G, Sentilhes L, Ancel PY, et al. Association of intraventricular hemorrhage and death with tocolytic exposure in preterm infants. JAMA Netw Open. 2018;1:e182355–182355. doi: 10.1001/jamanetworkopen.2018.2355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Braun A, Xu H, Hu F, Kocherlakota P, Siegel D, Chander P, et al. Paucity of pericytes in germinal matrix vasculature of premature infants. J Neurosci. 2007;27:12012–24. doi: 10.1523/JNEUROSCI.3281-07.2007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.McCrea HJ, Ment LR. The diagnosis, management, and postnatal prevention of intraventricular hemorrhage in the preterm neonate. Clin Perinatol. 2008;35:777–92. doi: 10.1016/j.clp.2008.07.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Folkerth RD, Haynes RL, Borenstein NS, Belliveau RA, Trachtenberg F, Rosenberg PA, et al. Developmental lag in superoxide dismutases relative to other antioxidant enzymes in premyelinated human telencephalic white matter. J Neuropathol Exp Neurol. 2004;63:990–9. doi: 10.1093/jnen/63.9.990. [DOI] [PubMed] [Google Scholar]
- 35.Ma S, Li X, Fang Q, Ross MG, Chao CR. Influence of fetal to neonatal transition on nitric oxide synthase expression in the nucleus tractus solitarius in sheep. Brain Res Dev Brain Res. 1999;118:119–27. doi: 10.1016/s0165-3806(99)00137-6. [DOI] [PubMed] [Google Scholar]
- 36.Winter S, Autry A, Boyle C, Yeargin-Allsopp M. Trends in the prevalence of cerebral palsy in a population-based study. Pediatrics. 2002;110:1220–5. doi: 10.1542/peds.110.6.1220. [DOI] [PubMed] [Google Scholar]
- 37.Fox NS, Gelber SE, Kalish RB, Chasen ST. Contemporary practice patterns and beliefs regarding tocolysis among U.S. maternal-fetal medicine specialists. Obstet Gynecol. 2008;112:42–7. doi: 10.1097/AOG.0b013e318176158e. [DOI] [PubMed] [Google Scholar]
- 38.Lewis DF. Magnesium sulfate: the first-line tocolytic. Obstet Gynecol Clin North Am. 2005;32:485–500. doi: 10.1016/j.ogc.2005.03.002. [DOI] [PubMed] [Google Scholar]
- 39.Mittendorf R, Pryde PG. A review of the role for magnesium sulphate in preterm labour. BJOG. 2005;112(Suppl1):84–8. doi: 10.1111/j.1471-0528.2005.00592.x. [DOI] [PubMed] [Google Scholar]
- 40.Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. N Engl J Med. 2020;382:1199–207. doi: 10.1056/NEJMoa2001316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Mittendorf R, Besinger R, Santillan M, Gianopoulos J. When used in the circumstance of preterm labor, is there a paradoxical effect of varying exposures to magnesium sulfate (MgSO4) on the developing human brain? Am J Obstet Gynecol. 2005;193:S65. [Google Scholar]
- 42.Nelson KB, Grether JK. Can magnesium sulfate reduce the risk of cerebral palsy in very low birthweight infants? Pediatrics. 1995;95:263–9. [PubMed] [Google Scholar]
- 43.You C, Deng Y, Hu W, Sun J, Lin Q, Zhou F, et al. Estimation of the time-varying reproduction number of COVID-19 outbreak in China. Lancet. doi: 10.2139/ssrn.3539694. 2020 Feb 20 [Epub]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Schendel DE, Berg CJ, Yeargin-Allsopp M, Boyle CA, Decoufle P. Prenatal magnesium sulfate exposure and the risk for cerebral palsy or mental retardation among very low-birth-weight children aged 3 to 5 years. JAMA. 1996;276:1805–10. [PubMed] [Google Scholar]
- 45.Doyle LW, Crowther CA, Middleton P, Marret S. Antenatal magnesium sulfate and neurologic outcome in preterm infants: a systematic review. Obstet Gynecol. 2009;113:1327–33. doi: 10.1097/AOG.0b013e3181a60495. [DOI] [PubMed] [Google Scholar]
- 46.Golan H, Kashtuzki I, Hallak M, Sorokin Y, Huleihel M. Maternal hypoxia during pregnancy induces fetal neurodevelopmental brain damage: partial protection by magnesium sulfate. J Neurosci Res. 2004;78:430–41. doi: 10.1002/jnr.20269. [DOI] [PubMed] [Google Scholar]
- 47.Gulczynska E, Gadzinowski J, Wilczynski J, Zylinska L. Prenatal MgSO4 treatment modifies the erythrocyte band 3 in preterm neonates. Pharmacol Res. 2006;53:347–52. doi: 10.1016/j.phrs.2006.01.002. [DOI] [PubMed] [Google Scholar]
- 48.Sameshima H, Ikenoue T. Long-term magnesium sulfate treatment as protection against hypoxic-ischemic brain injury in seven-day-old rats. Am J Obstet Gynecol. 2001;184:185–90. doi: 10.1067/mob.2001.108343. [DOI] [PubMed] [Google Scholar]
- 49.Thordstein M, Bågenholm R, Thiringer K, Kjellmer I. Scavengers of free oxygen radicals in combination with magnesium ameliorate perinatal hypoxic-ischemic brain damage in the rat. Pediatr Res. 1993;34:23–6. doi: 10.1203/00006450-199307000-00006. [DOI] [PubMed] [Google Scholar]
- 50.Türkyilmaz C, Türkyilmaz Z, Atalay Y, Söylemezoglu F, Celasun B. Magnesium pre-treatment reduces neuronal apoptosis in newborn rats in hypoxia-ischemia. Brain Res. 2002;955:133–7. doi: 10.1016/s0006-8993(02)03395-4. [DOI] [PubMed] [Google Scholar]
- 51.Mittendorf R, Pryde PG. An overview of the possible relationship between antenatal pharmacologic magnesium and cerebral palsy. J Perinat Med. 2000;28:286–93. doi: 10.1515/JPM.2000.035. [DOI] [PubMed] [Google Scholar]
- 52.Garnier Y, Middelanis J, Jensen A, Berger R. Neuroprotective effects of magnesium on metabolic disturbances in fetal hippocampal slices after oxygen-glucose deprivation: mediation by nitric oxide system. J Soc Gynecol Investig. 2002;9:86–92. doi: 10.1016/s1071-5576(01)00161-7. [DOI] [PubMed] [Google Scholar]
- 53.Elimian A, Verma R, Ogburn P, Wiencek V, Spitzer A, Quirk JG. Magnesium sulfate and neonatal outcomes of preterm neonates. J Matern Fetal Neonatal Med. 2002;12:118–22. doi: 10.1080/jmf.12.2.118.122. [DOI] [PubMed] [Google Scholar]
- 54.Petrova A, Mehta R. Magnesium sulfate tocolysis and intraventricular hemorrhage in very preterm infants. Indian J Pediatr. 2012;79:43–7. doi: 10.1007/s12098-011-0440-y. [DOI] [PubMed] [Google Scholar]